
Abstract
Background:
After amputation patients are more likely to injure their residual limb. An injury of a previously amputated limb, especially if the residuum is not anatomically normal, poses a dilemma for management.
Case Description and Methods:
This case report discusses a femoral fracture sustained proximal to a through-knee amputation.
Findings and outcomes:
The fracture was at the site of a malunited fracture. A shortening osteotomy with bone graft was undertaken to improve alignment and prosthetic fit and remove poor-quality bone. This was stabilised using an intramedullary nail, supplemented with an anti-rotation plate. This fracture went on to uneventful union, and the patient was able to comfortably use a prosthesis with increased functionality compared with prior to the recent injury.
Discussion:
This management enabled quick healing of the fracture without the need to resort to a more proximal amputation.
Conclusion:
In these unusual cases, careful planning is necessary to ensure all aspects of the problem is dealt with. Each case should be treated on its own merits.
Clinical relevance
This case demonstrates the difficulty in care of complex limb trauma and offers a solution for management of similar cases. Excellent results are possible when all surgical options are considered.
Background
The rate of major limb amputation is around 5.1 per 100,000 population in the United Kingdom and has remained unchanged in recent years. 1 Noteworthy, 2%–13% of all amputations in United Kingdom and European countries are due to trauma. 2 When deciding on the level of an amputation, many factors must be taken into account, including the severity of the injury, patient comorbidities and required function post-operatively. Mortality rates for all major amputations range from 3% to 18%, with more proximal level of amputation correlating with an increased mortality. 3 However, this finding is likely heavily influenced by patient comorbidities as the data include those requiring amputation for reasons other than trauma.
With regard to functional capacity, improved post-operative function has consistently been reported with more distal site of amputation. Energy demands following transtibial amputation are less than those following trans-femoral, with through-knee amputation demands being between those of transfemoral and transtibial amputations. 4 The probability of daily prosthetic use has been shown to increase with a more distal amputation site, 96% of transtibial amputations having daily prosthetic wear compared to 76% through knee and 50% transfemoral, 5 likely indicative of increased ease of use, better function and acceptability.
Through-knee amputations in general have their own specific problems and advantages. Historically, revision rates have been high, reported as nearly 10% in 1979 and 13% in 1988. 6 Long flaps are necessary to close the amputation leading to a theoretical poorer wound healing than with an transfemoral amputation. These reasons have led to the operation falling out of favour. More recent series, however, have reported primary healing rates to be around 80%, 7 compared to a healing rate of 90% in above-knee amputations. Through-knee amputations are performed more rarely than amputations at other levels, and this may lead to problems of inadequate experience both intra-operatively and in post-operative care, particularly with prosthesis fitting, all of which can lead to soft tissue complications. Therefore, while functional outcome is consistently reported to be better in through- than above-knee amputation, in those where a consistent predictable result is important, an transfemoral amputation is probably preferred. This particularly includes those with medical comorbidities in whom multiple revision procedures might be dangerous. The nature of a through-knee amputation means that the prosthetic articulation will be lower than the contralateral natural knee, leading to the knee on the amputated side being more prominent in the sitting position and the knee joints not being in line. 8 This not only leads to poor cosmesis but also can cause discomfort to the patient, difficulty sitting and problems with gait. However, compared to an transfemoral amputation, a through-knee provides greater muscle control of the limb and allows use of a total end-bearing prosthetic, thereby avoiding the ischial pressure needed in an transfemoral amputation. 9 Moreover, it offers the potential to wear a prosthetic without suspensory belt.
Amputees are at increased risk of suffering fractures due to decreased bone density, increased risk in osteoporosis and poorer mobility than the general population with increased propensity to fall. Injury to an amputation stump could be a challenge even to most experienced surgeons. 10 Overall, fracture management has been shown in general to yield good results, but subsequent function may be lessened, with 97% of transtibial amputees resuming prosthesis use and 82% transfemoral amputees resuming prosthetic use after sustaining a fracture of the residual limb. 11 As far as the authors are aware, there is no report detailing results of a fracture occurring through a previous malunited fracture in an amputated limb at the through-knee level.
In this case report, we will describe a patient with a through-knee amputation and a re-fracture through an area of poor-quality bone in a deformed residual femur due to previous malunion. This is an unusual problem not well detailed in literature.
Case description and methods
This report describes the case of a 55-year-old man admitted to hospital in February 2013 with a right-sided femoral fracture following a fall from standing. The fracture was situated at the distal third of the femur at the site of a previous malunited fracture. The previous fracture was an open distal femoral fracture sustained in 1984 in a road traffic collision, which at the same time resulted in a severe open tibial injury which was felt at the time to be non-reconstructible. A right through-knee amputation was therefore undertaken early following injury as the trauma was too proximal to preserve the knee. The original femoral fracture was treated with skeletal traction, with wound healing by secondary intent. The patient had had no problems with the wound or femoral segment soft tissues since and achieved good function with a knee disarticulation prosthesis. He had a past medical history of a triple heart bypass in 2000, chronic depression, osteoarthritis and angina.
On admission, the patient was otherwise well. The femoral fracture was displaced and unstable; it was therefore felt unsuitable for non-operative management. Plain radiographs revealed a pre-existing apex anterior deformity at the fracture site with an area of thinned, sclerotic, poor-quality surrounding bone (Figure 1). Computed tomography (CT) scanning was used to confirm the femoral morphology and fracture configuration for pre-op planning. Magnetic resonance imaging (MRI) scanning showed no signs of infection.
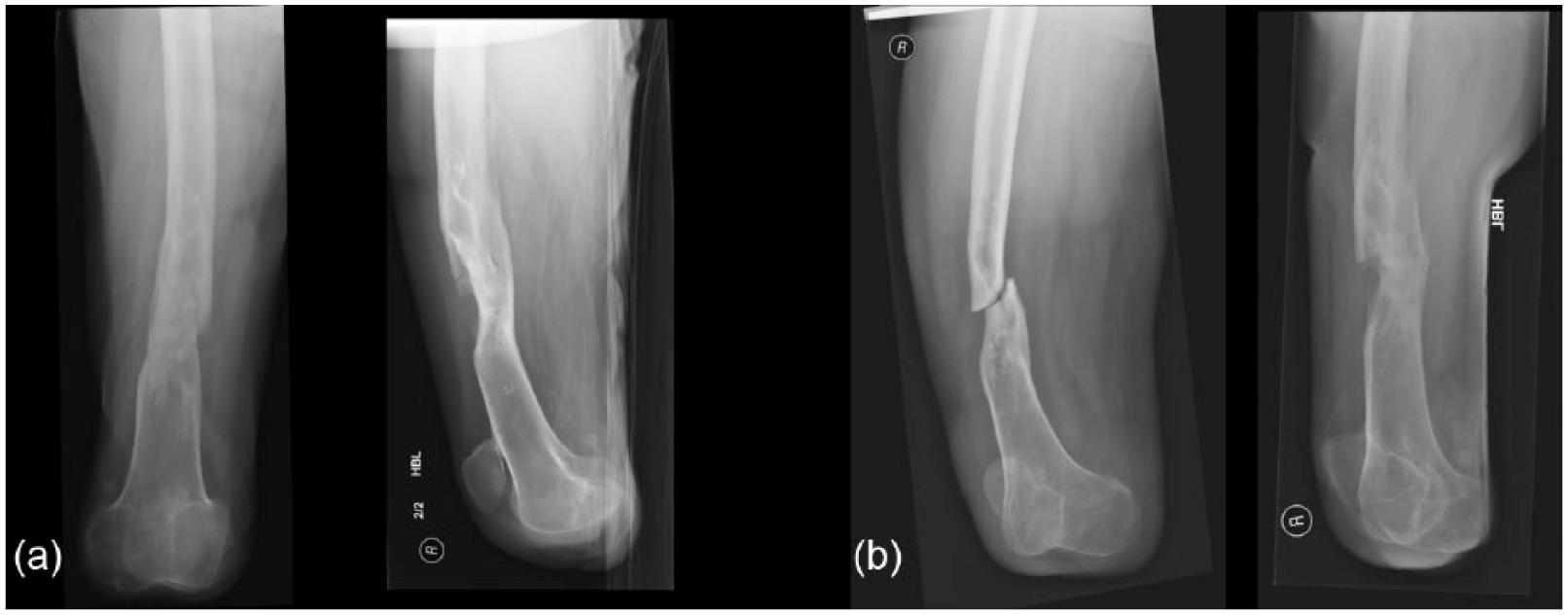
(a) Initial radiographs following injury and (b) following initial attempts at non-operative management showing fracture displacement and instability. Note previous malunion and poor-bone quality in the region of the fracture making standard operative management difficult.
The procedure performed for the femoral fracture was an acute shortening, closing wedge osteotomy and intermedullary nailing. The sclerotic segment including the fracture was resected as an anterior closing wedge. An 11 × 400-mm intramedullary femoral nail was introduced and locked distally with compression of the fracture leading to acute shortening. This was augmented with an anti-rotation locking plate to help neutralise torsional stresses in the transverse osteotomy with short distal segment (Figure 2). Tissue and bone samples were sent for microbiological analysis, and no organisms were subsequently cultured. Autologous bone graft (harvested from the contralateral femur using the reamer–irrigator–aspirator (RIA; DePuy Synthes) and biological adjuncts (bone morphogenic protein-7 (BMP-7), bone marrow aspirate (BMA) (bone marrow aspirate concentrate (BMAC)) and a calcium phosphate graft expander) were introduced to the fracture site to stimulate the osteotomy site in this area of relatively inert previously injured bone according to the principles of the diamond concept for bone repair. 12
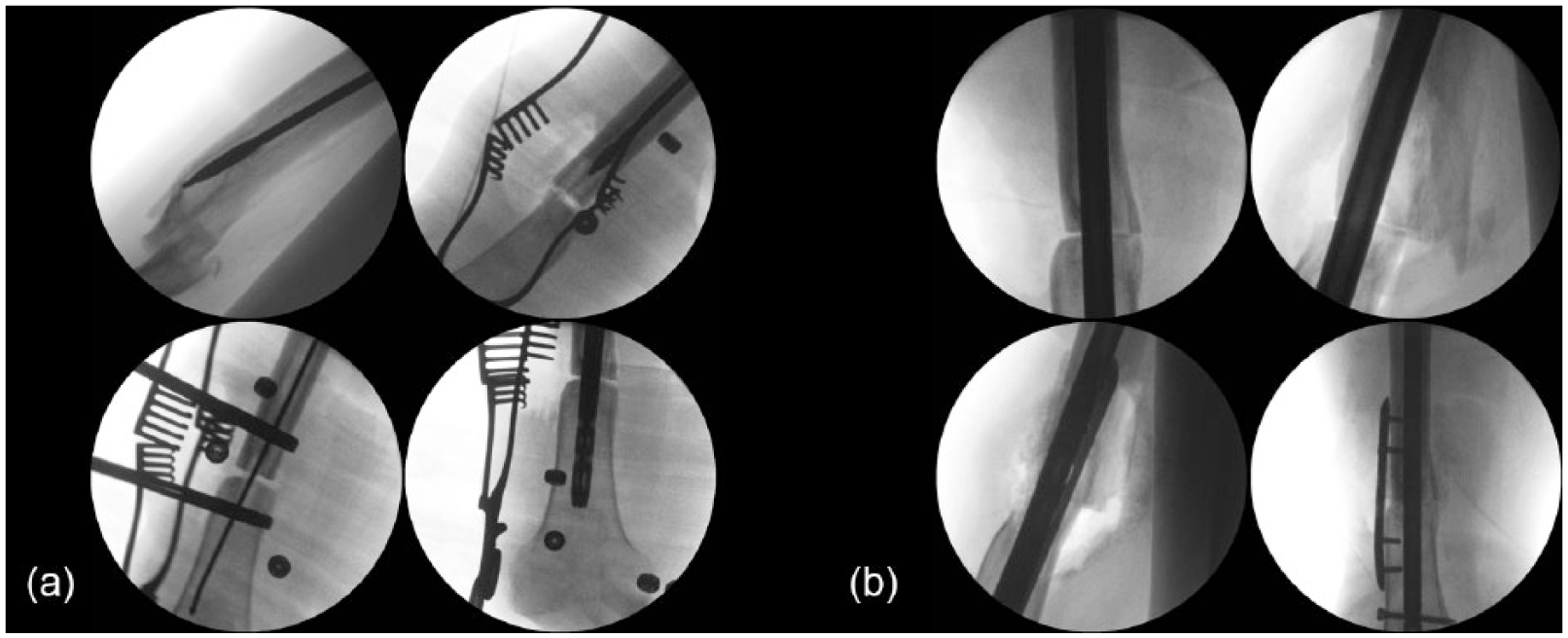
Intraoperative radiographs: (a) initial reamer passage reveals extent of deformity. Shortening closing wedge osteotomy performed removing areas of poor-quality sclerotic bone and improving alignment allows passage of antegrade femoral nail and (b) nail has been passed. Unicortical anti-rotation locking plate added to supplement fixation given transverse distal nature of osteotomy. Site has been augmented with autologous bone graft and bone morphogenic protein-7 (BMP-7).
Post-operatively, the patient underwent an uneventful recovery, initially mobilising without his prosthesis. At clinic, 2 weeks later, the patient had made good early progress, his wounds were healed with no sign of infection and he was pleased with the new shape of his residuum. He remained non-weight-bearing for 6 weeks and then began partially weight-bearing for a further 6 weeks, having been referred to the limb fitting service for a new prosthesis.
Findings and Outcomes
The patient was able to use his new prosthesis comfortably and felt that this fitting was improved compared to his pre-operative prosthesis 3 months post-operatively (Figure 3). In the longer term (6 months onwards), the patient reported improved function compared with that prior to the injury, more regular (daily) prosthetic use and less problems with prosthetic fit. He was happier with the appearance and function now that his knees were at a slightly more equal (though still not identical) level. The fracture appeared radiographically fully consolidated at 6 months (Figure 4). At 2 years post surgery, the patient’s mobility status had been stabilised with no irritation of the soft tissues and full consolidation of the fracture without formation of heterotopic ossification.

Clinical photographs showing the soft tissues post-operatively. New scars have been marked with arrows.

Post-operative radiographs at last follow-up showing good evidence of fracture site consolidation and remodelling and good restoration of overall alignment.
Discussion
This report focuses on the difficulties of tackling a new insult to an already anatomically abnormal femur in the context of previous amputation and the requirement for prosthetic use. The treatment of the initial fracture resulting from the road traffic collision was skeletal traction. Contemporary standard treatment of this type of injury would be intramedullary nailing. The reason skeletal traction was used in this case is unknown but was probably due to the severity of other injuries sustained in the road traffic collision (RTC); it is also important to note that the initial injury occurred in 1984 when skeletal traction was more commonly in use than in current practice.
After the new fracture, several techniques were employed to ensure successful healing. To impart strength to the femur and allow early weight-bearing, intramedullary nailing was used; this may also protect from subsequent fracture. The literature suggests that in the normal femur, antegrade and retrograde nailing have similar outcomes in terms of fracture union. 13 Antegrade nailing is more likely to cause subsequent problems with the hip and retrograde nailing is more likely to cause complications to the knee. Typically, more distal fractures, as in this case, are easier to control using a retrograde technique. However, in this case, an antegrade nail was used. This avoided soft tissue damage to the end of the residuum in the weight-bearing area, reduced the risk of prominent metalware in that area and minimised possible complications in this critical region. Multi-planar locking bolts were used distally 14 due to the fracture being metaphyseal, and this was achievable by the addition of an anterior-posterior (AP) locking bolt. Usually, an AP locking bolt cannot be used with an antegrade femoral nail, as this would impinge during patella motion; in this case, this did not pose a problem as the patella does not move.
As bone had been resected resulting in a transverse defect, an anti-rotation locking plate was used at the fracture site to increase torsional stability. An open approach had been used for bone resection, so no further soft tissue damage was needed for this. Bone graft and bone synthetic materials according to the diamond concept principle of fracture healing were used to induce osteogenesis and replace the defect left by bone resection. 12 Due to the previous injury, there were generally poor bone and poor soft tissues at the fracture site; therefore, synthetic agents were used to maximise the chance of union at the first procedure. 15
The resection led to a shortening of the length of the femur. With the prosthesis in place, this brought the patient’s prosthetic knee more in line with his contralateral native knee, which increased his satisfaction with his prosthesis wearing after healing of the residuum. The above management of the fracture enabled quick healing of the fracture site without need for converting to a more proximal amputation site. In patients with a post-traumatic amputation that also has an injured residuum, an individualised approach is necessary as seen in the herein case.
Conclusion
This case is multifaceted and required a variety of methods to manage. It demonstrates the complexities and challenges of managing amputees with subsequent injury to the residual limb and shows that careful planning is needed to ensure that the cause of problems is dealt with effectively. The management of the femoral fracture in this way allowed the previous issues of the malunion of the femoral fracture and the discrepancy in joint level to be solved, providing the patient with a complete answer to the new and old femoral abnormalities in a single operation.
Footnotes
Acknowledgements
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.