
Abstract
Background:
Transverse-plane foot deformities are a frequently encountered issue in children with neurological disorders. They are the source of many symptoms, such as pain and walking difficulties, making their prevention very important.
Objectives:
We aim to describe the use and tolerability of a side pole static ankle foot orthosis used to prevent transverse-plane foot deformities in children with neurologic disorders.
Study design:
Monocentric, retrospective, observational study.
Methods:
Medical data were collected from 103 children with transverse-plane foot deformities in one or both feet caused by a neurological impairment. All children were braced between 2001 and 2010.
Results:
Unilateral orthosis was prescribed for 32 children and bilateral orthosis for 71. Transverse-plane foot deformities were varus in 66% of the cases and an equinus was associated in 59.2% of the cases. Mean age for the first prescription was 8.6 years. For the 23 patients present at the 4-year visit, 84.8% still wore the orthosis daily, and 64.7% wore the orthosis more than 6 h per day. The rate of permanent discontinuation of wearing the orthosis was 14.7%.
Conclusion:
The side pole static ankle foot orthosis is well tolerated with very few side effects, which promotes regular wearing and observance.
Clinical relevance
Side pole static ankle foot orthoses are well tolerated and can be safely used for children with foot abnormalities in the frontal plane that have a neurological pathology origin.
Background
Ankle and foot deformities are common in patients with neurological disorders such as cerebral palsy (CP), neuromuscular disorders (NMD), or meningomyelocele, because neurological deficits can lead to immobility, locomotor system abnormalities, and joint contractures.
For instance, in CP, foot and ankle deformities are reported in 93% of the patients 1 with equinus being the most common foot deformity, followed by planovalgus and equinovarus.1–5 In meningomyelocele, almost all patients experience problems with foot deformities, which may present as transverse or sagittal plane deformities or a combination of both.6,7 In NMD, incidence and type of foot deformity varies depending on the disease, for example, in Charcot–Marie–Tooth diseases (CMT), almost all patients will experience cavovarus, 8 while in Duchenne muscular dystrophy (DMD), an equinovarus deformity is typically acquired as weakness progresses and the ability to walk is lost.9,10
Equinus is a sagittal plane deformity involving the contraction of the gastrocnemius or the gastrocnemius–soleus muscle tendon complex (triceps surae). In contrast, valgus and varus are the transverse-plane deformities involving the tibialis or peroneus muscles which may interfere with the walking process. In CP, varus causes instability during the support phase and difficulties of the foot in the swing phase, 11 while valgus causes excessive ankle eversion and plantar flexion, reduced ankle flexion range of motion, and increased midfoot joint dorsiflexion and pronation. 12 In DMD, equinovarus deformities are recognized as a major cause of disability, playing a role in the loss of ambulation 13 and are sources of skin injuries caused by abnormal support after the ability to walk is lost. 14 In addition, foot deformities can lead to painful calluses on pressure areas, esthetic issues, and make wearing worse shoes uncomfortable.15–17
While there is extensive literature on the management of equinus by operative and non-operative measures in CP,3,4,18,19 no consensus has been found for the management of varus and valgus in this condition. Different treatment options can include the use of orthoses, the use of botulinum toxin, or surgical correction of secondary contractures. Surgical correction remains difficult and is not always successful. 5 In CP, particularly for non-ambulant children or children under 8 years of age, a failure rate of 65% is reported for equinovarus surgery (failure was defined as the need for new foot surgery or the appearance of a varus or valgus of 10° or more). 20 In DMD, foot deformities resulting from musculotendinous contractures are mostly due to fibroadipose degeneration of the muscle fibers. Controversy exists regarding the long-term evolution after foot surgery in DMD, some authors recommend early surgical treatment (transfer of the posterior tibialis, lengthening of the Achilles tendon, and flexor tenotomy for toes) in order to maintain dorsiflexion which would delay the loss of ambulation. 21 Others, on the contrary, promote the use of orthoses by showing an annual delay of 23% in the development of ankle contractures in boys wearing a night posture orthosis. 14
In all cases, it seems important to prevent the occurrence of transverse-plane foot deformities and to limit their development with regard to the high risk of morbidity. In order to prevent such deformities, a side pole static ankle foot orthosis (SPS AFO) has been used in our department since 2001 in children with a neurological disorder predisposing such deformities. Here, we will describe the use, tolerability, and potential side effects of this orthosis that was used during our study, which took place over a 10-year period.
Methods
Study design
The study was a retrospective, monocentric, observational study.
Ethics
This research obtained ethical approval by an ethics committee (Comité de protection des personnes CPP Lyon Sud Est II: IRB number: 00009118).
Subjects and setting
Patients included in the study were (1) less than 17 years of age; (2) regularly followed up in the Pediatric Physical Medicine and Rehabilitation Department (Service de Médecine Physique et de Réadaptation Pédiatrique, L’Escale) in Lyon, France; (3) presented at least a unilateral transverse-plane foot deformity; (4) within the context of a neurological disorder; and (5) and had a first prescription of SPS AFO between December 2001 and December 2011.
SPS AFO
SPS AFO is a side pole axis (internal or external) orthosis allowing correction of transverse-plane foot deformities. This orthosis is a static orthosis, worn mostly at night for ambulatory patients. First, the foot is positioned on the foot module respecting the degree of equinus. In other words, the equinus deformity is respected in order to allow an adequate correction of the transverse-plan deformity.
Second, the side pole axis is brought closer to the leg to correct the transverse-plane deformity. Depending on the tolerance of the patient, the correction could be made progressively by acting on the position of the axis. The closer the axis to the leg, the more complete is the correction.
For correcting valgus feet, the pressure zone is located just above the medial malleolus and the areas of the counterforce zone are located at the level of the posterior external tuberosity of the calcaneus and the outer face of the fifth metatarsal. The tibialis pole is medial and stops just below the tibial plateau. The degree of misalignment is more or less significant depending on the degree of valgus and the correction to be achieved (Figure 1).

Application of the side pole static ankle foot orthosis on a valgus foot.
For correcting varus feet, the pressure zone is located just above the external malleolus and the counterforce zone is located at the inner face of the first metatarsal and the internal posterior of the calcaneus. The pole is lateral (Figure 2).

Application of the side pole static ankle foot orthosis on a varus foot.
For children who can maintain the sitting position, the molding is performed while seated with hip and knee flexed at 90°. For hypotonic children who cannot maintain a sitting position, the molding is performed while the foot is in a maximum plantar support and not resting on the heel. Varus or valgus is first corrected by maintaining the foot in plantar flexion. The search for dorsal flexion occurs only in a second step and is stopped just before the foot switches to varus or valgus. When the orthosis is delivered, instructions for the set-up are given to the child and their parents to ensure observance and tolerance of the orthosis.
Follow-up visits
The baseline visit consisted of the fitting of the orthosis. Follow-up visits consisted of controls to ensure adequate tolerance and adaptation of the orthoses. These visits were carried out in the Pediatric Physical Medicine and Rehabilitation Department, L’Escale by a physiotherapist and a pedorthotist at 3, 6, and every 6 months thereafter.
Data collection
Data were collected from the patients’ medical records.
The following information was collected on the day of the first delivery of SPS AFO: (1) pathology, (2) age, (3) walking abilities (autonomous walking capacity was defined as the ability of the child to complete 10 steps without technical assistance), (4) type of deformity (varus or valgus and unilateral or bilateral), (5) associated with an equinus, and (6) if the prescription was first intention or not, and if not, what type of orthopedic correction the children previously had.
At each follow-up visit, the following information was collected: (1) frequency and duration of wearing the SPS AFO, (2) side effects such as skin problems, pain, or discomfort reported by the parents and/or the child during a specific interview with the health professional, (3) eventual causes for stopping wearing the orthosis, and (4) existence of foot surgery.
Statistical analysis
Quantitative variables were expressed as means ± standard deviation and qualitative variables as number and percentage. Microsoft Office Excel 2011 software was used to perform the analysis.
Results
The main characteristics of the study population are given in Table 1. A total of 103 patients (57 males and 46 females) with a neurological disorder, aged between 1.2 and 16.2 years with a deformity in the frontal plane of one or both feet were included in the study (Table 1). Among them, 34 children had CP, 34 a NMD, and 10 a meningomyelocele. Other patients included presented epileptic encephalopathies, 7 metabolic diseases, 4 leukodystrophies, 3 and arthrogryposis. 3 At the time of first SPS AFO prescription, 51 children were able to walk and almost all patients (96.7%) had motor physiotherapy, with a mean frequency of 2.6 sessions a week.
Characteristics of patients at baseline.
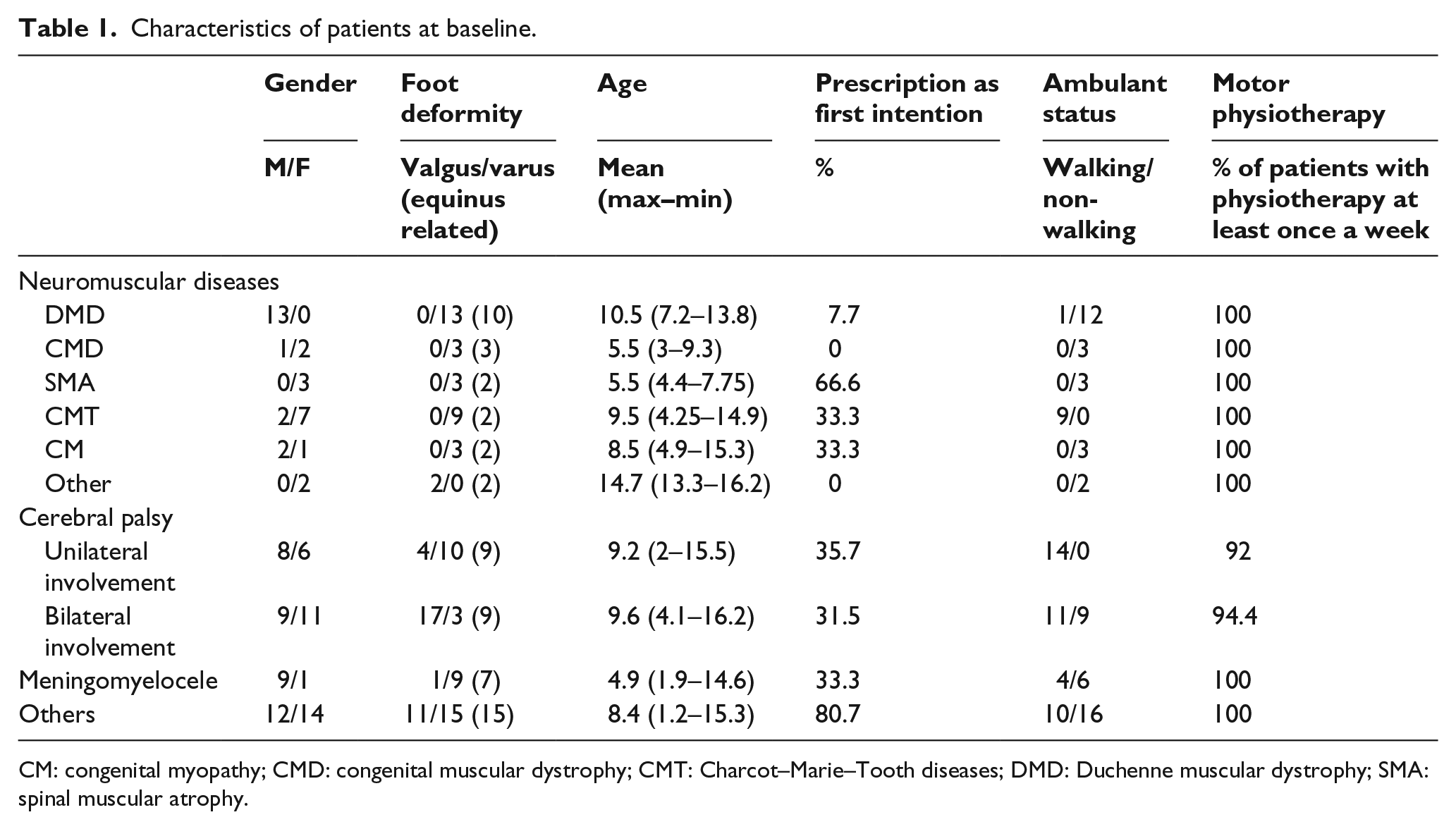
CM: congenital myopathy; CMD: congenital muscular dystrophy; CMT: Charcot–Marie–Tooth diseases; DMD: Duchenne muscular dystrophy; SMA: spinal muscular atrophy.
SPS AFO prescription
Between December 2001 and December 2011, 32 children had a prescription for a unilateral SPS AFO and 71 for a bilateral SPS AFO. In the majority of cases, the deformities were varus feet (66% of prescription). An equinus was associated with 59.2% of cases. Mean age at first SPS AFO prescription was 8.6 ± 2.9 years (min: 1.2 years–max: 16.2 years) (Table 1).
The SPS AFO was prescribed as first orthosis in 38% of cases (Table 1). When prescribed after a first orthosis, the previous orthosis was a postural posterior ankle foot orthosis in 93.5% of cases. The average number of renewals was 1.57 ± 0.88 (min: 1–max: 4) (data not shown).
Description of follow-up
Data concerning the wearing of SPS AFO could be analyzed for 88 patients. Indeed, of the patients whose data were removed from the analysis, eight had insufficient data in their medical records, four died during follow-up (one DMD, one Spinal Muscular Atrophy type II, and two metabolic diseases), and three were lost to follow-up. Mean follow-up duration for the 88 patients was 2.75 years (min: 3 months–max: 8.75 years).
Very little difference was observed with regard to the length of time wearing the orthosis, with 84.8% patients still wearing the SPS AFO every day after 4 years of follow-up. In addition, a very low number of patients wore the SPS AFO only once a week and this remained stable throughout the study (3% at 4 year visit) (Table 2). In contrast, the duration of wearing sessions tended to decrease with time. SPS AFO was worn between 6 and 12 h by 70.8% of the patients at the 3-month visit and by 58.8% at the 4-year visit. In contrast, 21.3% wore SPS AFO less than 6 h per session at the 3-month visit versus 35.3% at the 4-year visit.
Frequency and duration of SPS AFO wearing reported during visits at 3 months, 1 year, 2 years, and 4 years.
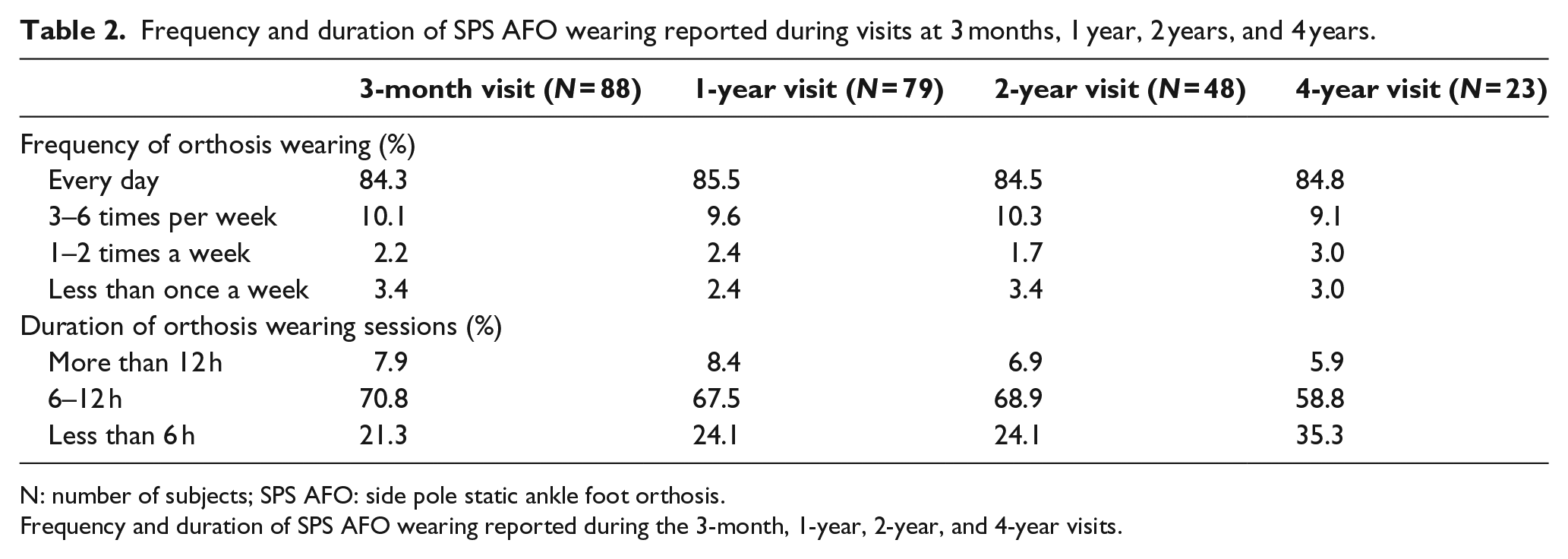
N: number of subjects; SPS AFO: side pole static ankle foot orthosis.
Frequency and duration of SPS AFO wearing reported during the 3-month, 1-year, 2-year, and 4-year visits.
Occurrences of reported side effects over the 4-year period are shown in Figure 3. They mainly concern transient skin problems and painful phenomena (22 and 9, respectively). Side effects occurred mainly during the first months of wearing (18 were reported between fitting and the 3-month follow-up visit vs 7 reported between the 3-month and the 1-year visits).
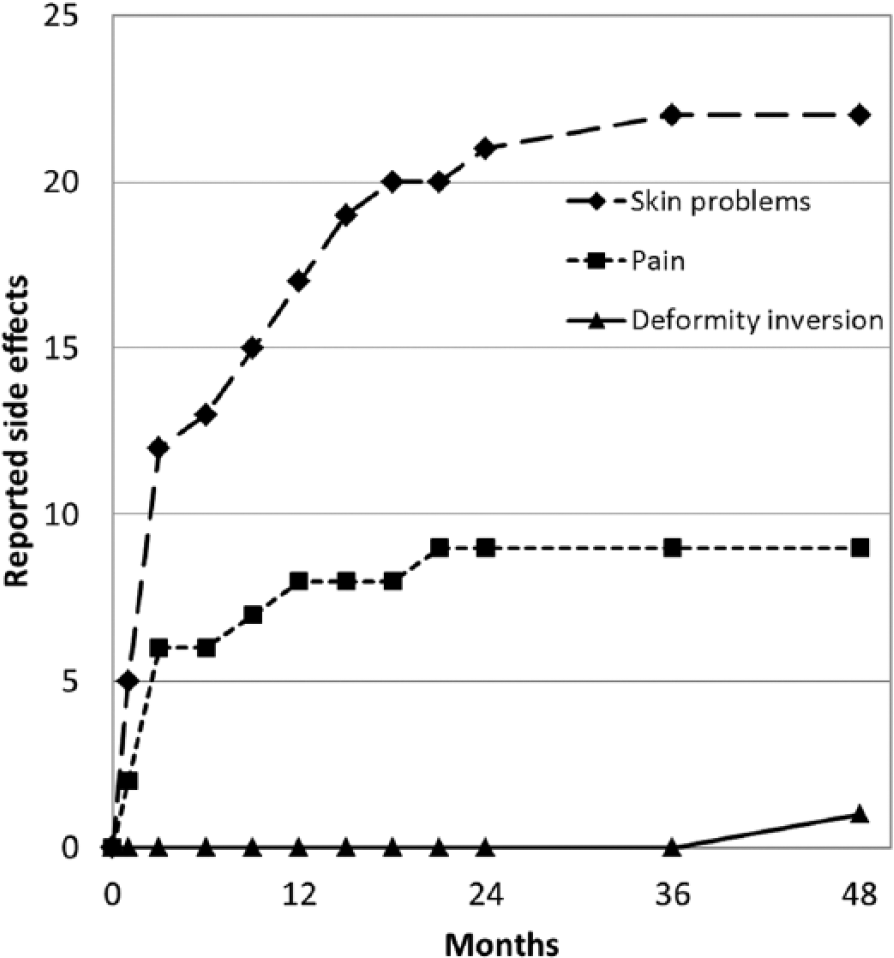
Accumulated number of side effects related to the wearing of the SPS AFO reported by parents and/or children during follow-up visits after SPS AFO fitting.
Two patients presented skin lesions (i.e. bedsores) and stopped wearing the orthosis for a few days while awaiting recovery. Reasons for permanent discontinuation are shown in Table 3. Only 13 patients permanently discontinued the use of the SPS AFO in the 10-year period of the study. Three discontinuations were due to a change in the type of the orthosis, two were due to a correction of the deformity, two were due to foot surgery, one was due to an inversion of the foot deformity, and five were due to side effects. Permanent discontinuations were mainly observed after the 1-year visit (four were reported before the 1-year visit vs nine between the 1-year visit and the 4-year visit).
Causes of permanent discontinuation of wearing the SPS AFO.
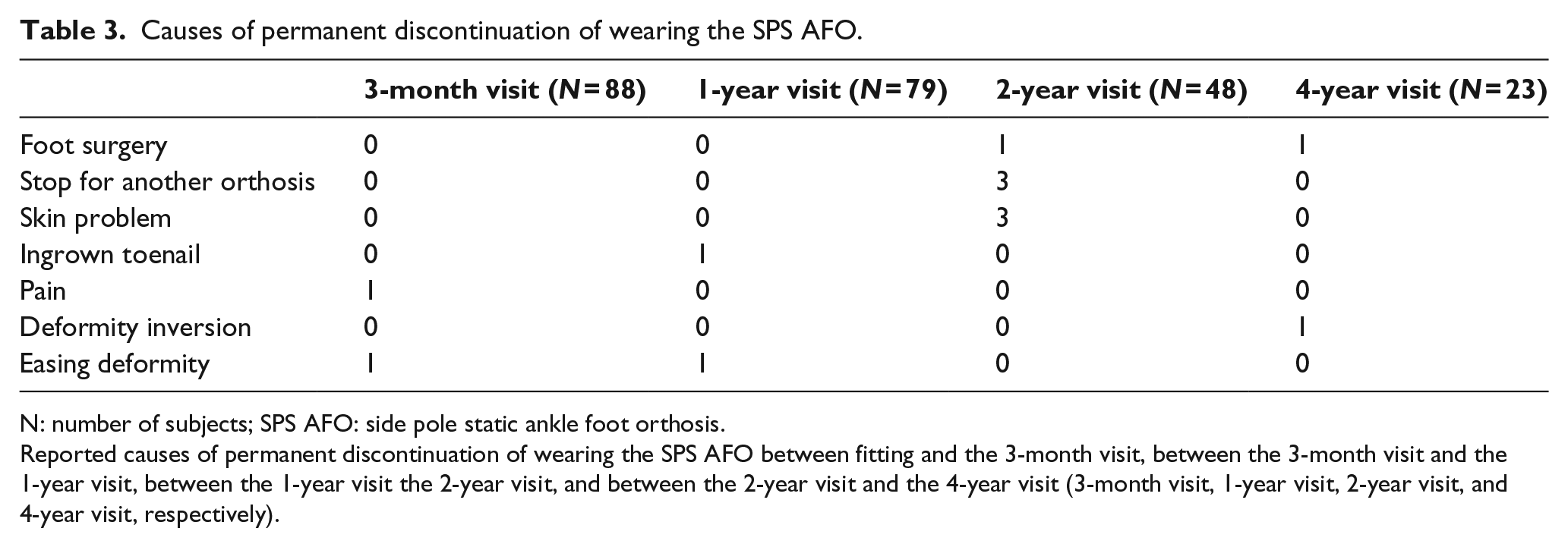
N: number of subjects; SPS AFO: side pole static ankle foot orthosis.
Reported causes of permanent discontinuation of wearing the SPS AFO between fitting and the 3-month visit, between the 3-month visit and the 1-year visit, between the 1-year visit the 2-year visit, and between the 2-year visit and the 4-year visit (3-month visit, 1-year visit, 2-year visit, and 4-year visit, respectively).
Discussion
Considering the controversy of the surgical management of transverse-plane foot deformities in children with neurological origins,5,14,20–22 it is important to develop preventative therapies. For this reason, our pediatric rehabilitation department developed a side pole static orthosis in collaboration with an orthosist to prevent the onset of these disorders and to delay their progression by keeping a maximum flexibility in the foot. In this study, we present the use of this orthosis in our department over a 10-year period.
The orthosis is most often prescribed after failure of a classic ankle foot orthosis (posterior pole) that does not prevent the onset of the transverse-plane deformity. However, this practice has changed with time as prescription as first orthosis has increased over the years: 2 prescriptions out of 9 were a first-intention prescription in 2002 versus 9 out of 20 in 2008.
The orthosis may be prescribed early in the course of the disease; the youngest child in our study was 14 months old. Tolerability of the orthosis by the family and the child appears to be good as it was worn on a regular basis by most children (according to the 4-year visit, 84.8% of patients wore it every day) and over a long period (6–12 h for 58.8% of children, based on the 4-year visit). Walking children wore their orthosis mostly during the night and non-walking children wore their orthosis preferably during the day (all patients who wore the SPS AFO more than 12 h a day were non-walking children).
The total number of children who stopped wearing it is rather low (13 patients), and rarely it was due to adverse events. Indeed, adverse events were mostly transient, with only five cases resulting in a definitive discontinuation of use. To promote observance, SPS AFOs were controlled every 3 months, which allowed the rapid adaptation of the orthosis and adequate following of the growth of the child. With regard to the side effect, bedsores occurred in two children with sensory disorders (meningomyelocele): one child with low communication skills (severe epileptic encephalopathy) and the other with DMD. The second most frequent side effect was pain (nine cases). In two-thirds of these cases, pain occurred in the first 3 months (six cases) after the implementation of the orthosis in patients with a neuromuscular disease (DMD, SMA, or CMT).
In the specific case of DMD, no child underwent orthopedic surgery of the lower limbs during this 10-year period. Indeed, with this condition, orthoses are required upon the occurrence of a varus, which is quite early in the course of the deformities. The regular use of an orthosis may help to maintain a flexibility of the foot which avoids the need for surgery. 22
Unfortunately, due to the retrospective nature of the data collection, footwear could not be studied as this information was rarely specified in the files. The low number of stoppages due to surgery, worsening of equinus, and the use of another orthosis (six in total) suggest a good effectiveness of our device. However, assessment of effectiveness requires a prospective study using objective criteria such as range of motion or radiological assessments and comparison with other best practice treatments.
Conclusion
A SPS AFO may be prescribed early in children with neurological disorders with a transverse-plane deformity (varus or valgus). This orthosis seems safe and well tolerated by children considering the low rate of adverse events and its permanent discontinuation wearing.
Footnotes
Acknowledgements
We acknowledge J Bonin, from the Deage society (Lyon, France), who braced all patients and participated in all control visits during our study.
Author contribution
C.V., C.D., and C.B. contributed to the study design; C.V., C.D., I.P., J.-P.V., and F.M. contributed to the data collection; C.V., C.D., and P.R. contributed to the data analysis; C.V., C.D., P.R., F.M., J.-P.V., C.B., and IP contributed to the manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.