
Abstract
Background:
Traumatic injuries are the most common cause of finger amputations. Therapeutic amputations are less common but may be essential in some patients with congenital malformations of digits.
Case description and methods:
A 21-year-old female patient reported for esthetic management of malformed middle and ring finger of right hand. Examination revealed clino-syndactyly with unusual dermatoglyphics. She was successfully rehabilitated by collaborative efforts of plastic surgeon and prosthodontist, by therapeutic amputation with surgical recontouring and fabrication of somatoprosthesis.
Findings and outcomes:
The patient was satisfied with esthetics of the prosthesis and somatoprosthesis improved function. At 6-month recall, no alterations or repair of prosthesis was required.
Conclusion:
Individualized treatment planning with integration of modifications involving a multidisciplinary approach is required to meet needs of patients with congenital digital malformations. The duplication of unusual dermatoglyphics made the prosthesis more realistic.
Clinical relevance
An individualized treatment plan with modifications to conventional techniques is required to cater to rehabilitative needs of patients with congenital digital malformations.
Introduction
Amputation of any part of a body is a triple threat. It involves loss of function, sensation, and body image. 1 Finger or partial finger amputations are most frequently encountered defects requiring somatoprosthesis. Such defects cause loss of grasp, reduce ability to perform activities with hands, and result in marked psychological trauma. The most common cause is traumatic injury. 2 Therapeutic amputations are less common but may be essential in some patients with congenital malformations of digits that include syndactyly, polydactyly, clinodactyly, camptodactyly, and so on. 3 Such malformations may be isolated or occur in association with syndromes such as Apert syndrome, Crouzon Syndrome, Orofaciodigital syndrome, Freeman–Sheldon syndrome, otopalatodigital syndrome, and so on.3,4
Surgical reattachment may be an option to salvage amputated segment in case of traumatic finger amputation. However, whenever therapeutic digital amputation is planned, microvascular reconstruction techniques such as toe-to-finger transfers, lengthening procedures, and osteo-cutaneous flaps are the only feasible surgical options available. Usually, multiple surgical procedures are required to achieve the desired end result. 5 But despite good functional results achieved by surgical reconstruction, cosmetic outcomes may be unsatisfactory. Almost none of the reconstruction procedures offer an appealing solution to the patient, as all involve long convalescing times. Most such amputees therefore tend to shy away from reconstructive surgical procedures and try to live with their deformity. 5
Also, patients’ willingness to undergo costly procedures like micro-surgical grafting and implants may preclude them. It is in this group of patients, where prosthetic rehabilitation holds a definite edge over surgical procedures. At times the maxillofacial prosthodontist may be called upon to help make a somatoprosthesis for such physically disabled patients. 6 This article presents a case of a 21-year-old female with congenital clino-syndactyly of middle and ring finger of right hand and unusual digital dermatoglyphics, who was successfully rehabilitated by collaborative efforts of plastic surgeon and prosthodontist.
Case description and methods
A 21-year-old female patient reported to the Department of Prosthodontics, for esthetic management of her malformed middle and ring finger of right hand (Figures 1 and 2). Anamnesis revealed that her fingers were malformed since birth and she never sought any treatment before. The psychological status, concerns, and expectations of patient regarding the treatment were evaluated. She was found to be more concerned about esthetics rather than function. Family history was negative and systemic examination ruled out any syndromic association. Physical examination revealed simple 3 (involving only skin and fibrous tissue), incomplete (interconnection not encompassing the entire length of adjacent digits) syndactyly involving proximal phalanges of middle and ring finger (resulting in obliteration of third web space) with clinodactyly involving distal phalanges of middle and ring finger of right hand (Figures 1 and 2). Another noteworthy feature was unusual dermatoglyphics in the form of increased number of creases on palmer aspect of all fingers.
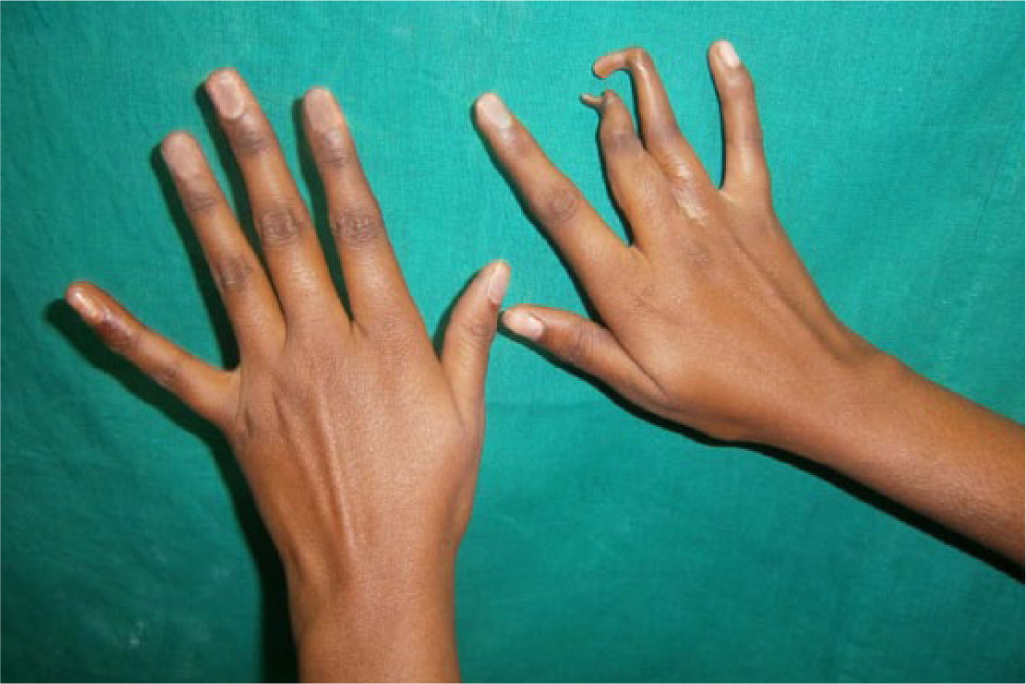
Pre-surgical photograph showing clino-syndactyly—Dorsal aspect.

Pre-surgical photograph showing clino-syndactyly—Palmar aspect.
Due to extreme curvature of distal phalanges, it was not possible to provide a somatoprosthesis over natural fingers. Therefore, the patient was referred to a plastic surgeon for separation of fused proximal phalanges followed by therapeutic amputation to the junction of middle and proximal phalange, with surgical recontouring of residual stumps to facilitate prosthetic rehabilitation. Due to financial constraints, patient disagreed to implant placement following amputation. After a healing period of 8 weeks, patient’s residual stumps were evaluated (Figure 3) and consent obtained for making photographic records.

Post-surgical photograph.
The rehabilitation process was initiated by making impression of the residual stumps (Figure 4) using irreversible hydrocolloid impression material (Alginate; Aramex Trading Co.), which was poured with dental stone (Kalstone; Kalabhai Pvt Ltd) to obtain the working cast. Stumps on the working cast were reduced 1 mm all around the designated area of contact, using depth orientation grooves (horizontal and vertical grooves) (Figure 4), for uniform reduction, while preventing over reduction. This ensured that vascular supply was not compromised. Scoring the stump ensured enhanced retention by creating suction and vacuum, 7 to provide snug-fit to wax patterns and future prosthesis.

Cast of remaining stumps with depth orientation grooves.
An impression of patient’s left middle and index fingers was also made, in a slightly flexed position. Melted modeling wax (Link dental modeling wax no.2; MDM Corporation) was poured into hydrocolloid molds and prepared stumps (lubricated with petrolatum) were inserted immediately into these molds, to duplicate the natural phalanges. Donor technique 8 (in which impression of corresponding fingers of siblings are made to obtain wax patterns) would have been of limited use, as this would not have replicated the unusual dermatoglyphic pattern.
The wax patterns were separated from prepared stumps after cooling of wax and re-adapted to stumps by merging the borders with area adjacent to defect (Figure 5). The anatomic crease lines were accentuated to improve esthetics and provide a natural appearance. Then, the wax patterns were tried on the patient’s residual stumps (Figure 6). The fit, emergence, and orientation of the pattern were evaluated along shape and size.

Adjusted wax patterns on cast.

Wax pattern trial.
The pattern was invested using lost wax technique to obtain a two-piece mold after dewaxing. The two-component system high-temperature vulcanized (HTV) maxillofacial silicone material (M511 maxillofacial silicone; Technovent) was pigmented with intrinsic colors according to the skin color of the patient. Color matching of the palmer surface was done first as this tends to be lighter than the top surface. Appropriately shade matched silicone material was packed and molds were closed followed by the curing process according to manufacturer’s instructions. After sufficient cooling of molds, the prostheses were removed, trimmed, and finished. The shade was evaluated on the patient. As precise coloration is crucial, extrinsic coloring was carefully done to match the color of patient’s skin. The nail was fabricated using transparent and pink self-polymerizing acrylic resin (Trevalon; Dentsply India Pvt Ltd). To achieve an enhanced realistic appearance, the nail and nail bed were shaped with trimmer according to the nails of the natural fingers and it was placed into the nail bed. After making the necessary adjustments, the nail was attached to the prosthesis with a primer (A-330-G Gold Primer; Factor II, Inc.).
The prostheses were inserted (Figure 7) and evaluated. The slight scraping of the stumps on the cast provided enough grip of the prosthesis to not require adhesive use. Decorative rings were used to hide the margins of prosthesis. Instructions for home care were given, including skin care and prosthesis maintenance. On 6 months recall appointment, the prosthesis was found to be satisfactory not requiring repairs. The patient was satisfied with esthetics of the prosthesis. Somatoprostheses improved the function of digits by restoring the normal shape and length besides helping in writing, grasping and holding of light objects.

Finger prosthesis in situ—Dorsal aspect.
Discussion
Rehabilitation of patients with congenital digital malformations is more difficult and challenging compared to rehabilitation of patients with traumatic/acquired defects because of presence of associated variable syndromic associations and presentations. Conventional procedures cannot be used without modifications to achieve desired outcome in such complex cases. In this case, therapeutic amputations of malformed digits were done to enhance outcome of somatoprosthesis. Such amputations are rarely required as most patients seeking digital prosthetic rehabilitation usually suffer from traumatic amputations.
Wax pattern fabrication for patients with unusual dermatoglyphics poses a challenge for the prosthodontist as the conventional donor technique cannot be used. Also, patient’s fingers of normal hand need to be modified carefully to produce positive patterns of affected fingers. Utilizing the residual stump in an effective manner is of paramount importance in cases where implants have not been placed. Modifying the residual stump by uniformly reducing it within physiological limits creates suction and enhances retention of definitive prosthesis, eliminating the need for adhesive. Besides improving patient compliance, this also prevents inadvertent skin reactions due to the use of adhesives and reduces maintenance cost for the patient.
Loss of even a small part of a single digit produces profound effect upon the amputee’s body image, self-esteem, and psychological status. 1 The young amputees usually suffer from crisis in terms of identity, sexuality, and social acceptance. In cases where reconstruction is not advisable, partially successful, or unfeasible such as in case discussed above, somatoprosthesis can be provided which may offer great psychological help. 8 Prosthetic rehabilitation is quick, reversible with no medical compromise, and allows the site to be closely monitored. 9 However, it is necessary to determine the patient’s motivation for obtaining prosthesis and whether there is a realistic understanding of its advantages and disadvantages. If the patient is appropriately informed about the limitations of prosthesis, he or she is better prepared to accept it. Individualized treatment plan with modifications in conventional techniques, involving multidisciplinary team approach, are required to cater the complex needs of such patients. Prosthesis form, coloration, and texture must be as indiscernible as possible from the surrounding natural tissues. The duplication of usual dermatoglyphics in somatoprosthesis, as done in the present case, made the prosthesis realistic, blending it into the normal anatomy.
Conclusion
Individualized treatment plan with integration of modifications in conventional techniques, involving multidisciplinary team approach, is required to cater to the complex needs of patients with congenital digital malformations vis-a-vis traumatic amputations. Although the prosthetic digital prosthesis lacks the sensation of a normal digit, it does provide a myriad of functions unattainable with malformed digits such as holding a pen or grasping a paper. Modified silicone finger somatoprosthesis fabricated for such patients as described should fulfill esthetic and psychological needs of amputees and help them overcome embarrassment in public.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.