
Abstract
Background:
One of the treatments prescribed for musculoskeletal patients is orthopedic shoe. The use of an orthopedic shoe is thought to produce a more typical ground reactive force pattern.
Objectives:
This study was designed to determine the influence of three heel designs of an orthopedic shoe on the ground reaction forces during walking in healthy subjects.
Study design:
Quasi-experimental.
Method:
In total, 30 healthy adults (12 males, 18 females) walked at a self-selected pace for six trials in each of the three shoe conditions having three different heels which included the following: standard heel, beveled heel, and positive posterior heel flare. For each trial, ground reaction force parameters were recorded using a force plate.
Results:
Repeated measures analysis of variance indicated that the impact force was significantly reduced for the positive posterior heel flare condition by 8% and 13% compared with standard and beveled heels, respectively (p < 0.001). The first peak of vertical force showed a significant reduction in the beveled heel by 5% and 4% compared with the standard heel and the positive posterior heel flare, respectively (p < 0.001). Loading rate was significantly reduced in the beveled heel and the positive posterior heel flare conditions (p < 0.05).
Conclusion:
Positive posterior heel flare reduced impact force due to its geometry flexibility, while a beveled heel reduced first peak of vertical force. The findings of this study show that the shape of the heel therefore has the potential to modify impact loads during walking.
Clinical relevance
This study provides new evidence that by changing shape in the heel of orthopedic shoe impact loads are reduced during walking. Thus, these findings indicate that use of heel design may be beneficial for various musculoskeletal disorders, including key public health problems.
Background
Ground reaction forces (GRFs) act between the ground and the foot during weight-bearing activities (i.e. walking or running). Forces applied to the body are multidirectional resulting in forces in the vertical, anterior/posterior, and from medial/lateral directions. 1 The natural cyclic events related to walking can produce high vertical forces on the body, particularly at initial contact. These forces are large in magnitude ranging between 1.0 and 1.2 times body weight (BW) during the double-stance phase.2,3 High loading rates have been associated with cartilage damage, 4 generalized knee pain, 5 and knee osteoarthritis. 6 In addition, high impact force magnitudes have been associated with anterior cruciate ligament injury 7 and lower limb overuse injuries. 8 Increase and repetition of both high force magnitude and loading rate are considered to have potentially deleterious effects upon the musculoskeletal system.2,3,9 The body has several intrinsic structures to attenuate the subsequent shock-waves that occur during weight-bearing activities. These structures include articular cartilage, intervertebral disks, and menisci and are commonly referred to as shock absorbers. 10 However, as with all biological tissues, at times when conditions favor exceeding the physiological threshold of these shock absorbers, they are unable to withstand the forces of walking. With repetitive, high forces, fatigue or failure can be experienced. 3 Given the potential damaging effects of impact-related loading during the gait, ergonomic interventions in the structure of shoe and insole can be designed to reduce these loads and are considered desirable. Furthermore, lower impact-related loading during walking is associated with superior participant perceived comfort ratings. 11 Previous research has demonstrated that there are a variety of methods used for decreasing the vertical forces while walking. These include using an insole in the footwear2,12,13 or changing the structure of the outsole and heel in the footwear.14,15
While footwear is primarily used to protect the foot from cutaneous injury, it plays a crucial role as a therapeutic device. Orthopedic footwear and footwear adaptations are frequently used within rehabilitation to accommodate joint deformities, modify plantar pressure distribution, alter gait patterns and improve stability and balance. 16 Orthopedic shoes when compared to ordinary shoe can have certain benefits in producing a more typical ground reactive force pattern by improving the alignment of the foot. 17 Small changes in the structure of orthopedic shoe can have a great impact on GRFs, and the moments created on the knee and ankle joints when contact with the ground is made. These changes are typically applied on the outsole or on the heel. The heel is one of the common corrections for the orthopedic shoe and can change the pattern of mechanical loading on the lower limb in the stance phase of walking. 18 Different shapes of heels can have noticeable impacts on the treatment of orthopedic conditions 17 and decrease the imposed loading on the lower limb. 19 A previous study has shown how a beveled heel with a 10° slope compared with a standard heel decreased the vertical ground reaction force (vGRF) in patients who had suffered a stroke by increasing the contact level in the loading response phase. 19 Queen et al. 15 also showed that a positive posterior heel flare (PPHF) with a 11° ± 1° angle compared to a PPHF with a 2° ± 1° angle posteriorly reduced the loading rate and posterior GRF during running. Menz et al. 20 noted that PPHF compared with standard heel and beveled heel increased flexibility at heel contact, therefore the PPHF took comparatively longer to grip the surface when vertical force was applied.
Moreover, while the effect of heel use upon forces between the foot and the ground have been reported, there are little data regarding the effect of the structure and the different heel shapes of the shoe upon the forces exerted. Previous investigations, however, have typically been limited to the influence of material21–23 and the height of the heel12,14 upon the GRFs. Moreover, use of the different designs of the heel is typically prescribed in the orthopedic clinics. There is limited scientific evidence to support heel modificaitons and the justification for prescribing this type of shoe correction is based on experimental theories and observations. Thus, study of the influence of heel shape on the GRFs is merited and should be considered. The purpose of this study was to determine the effects of the standard and beveled heels as well as the PPHF in the orthopedic shoe on the GRFs while walking in healthy individuals. Due to the fact that orthopedic conditions also influence GRFs, this research was carried out on healthy subjects to separate the effect of heel shape from other factors. This study could provide some guidance for prescription of orthopedic shoes.
Methods
In total, 30 healthy subjects (12 males and 18 females) volunteered for this experimental study, and all presented with no current musculoskeletal complaint and no previous history of major lower limb injury or disease. Ethical approval was sought and obtained from the author’s institute ethical approval board and prior to participation; all subjects provided written informed consent. The mean and standard deviation (SD) of age, weight, height, and body mass index of participants was 26 (3.5) years, 62.15 (8.72) kg, 166.4 (8.2) cm, and 22.40 (2.50) kg/m2 respectively. A random sampling method was used among the students and staff of University of Social Welfare and Rehabilitation Science (USWR). This study was conducted at the USWR facility during a 5-month period.
The shoe used in this study was an orthopedic shoe made in the Tehran Red Crescent Society for women and men by an experienced orthotist with 20 years of experience. The main difference among these shoes was the design of the heel: a standard heel, a beveled heel, and a PPHF. Each participant received three shoe conditions: (1) orthopedic shoe with standard heel, (2) orthopedic shoe with beveled heel, and (3) orthopedic shoe with PPHF. The standard heel in this study was a square-edged heel in which the posterior edge was perpendicular to the ground 20 as shown in Figure 1. Beveled heel was a heel with the posterior edge rounded off. The bevel began 1 cm from the bottom of the heel and extended forward 3.5 cm from the posterior edge of the heel, creating an angle with the floor of approximately 10° 24 as shown in Figure 2, and the PPHF is structured so that shoes’ midsole material is inclined at 30° posteriorly away from the posterior aspect of the shoe 20 as shown in Figure 3. The hardness and height of all the heels for each size were constructed equally. The material used for construction of the shoe was leather for the upper portion and the outer sole and heels were constructed of ethylene-vinyl acetate rubber. The average height for the orthopedic shoes was 25 mm 18 and the heel height was 25 mm.

Orthopedic shoe with standard heel used in this study: (a) lateral view and (b) posterior view.

Orthopedic shoe with beveled heel used in this study: (a) lateral view and (b) posterior view.
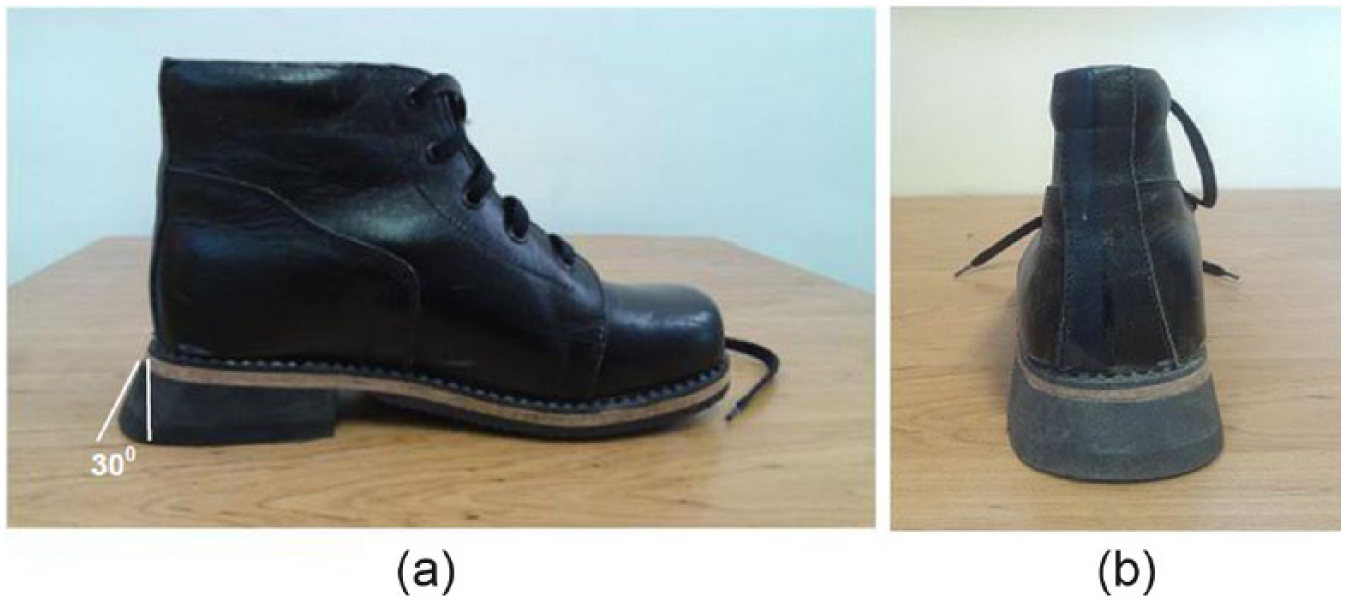
Orthopedic shoe with PPHF used in this study: (a) lateral view and (b) posterior view.
The Kistler Force Plate model 9286A was used to process the clinical data collected, sampling at the rate of 100 Hz, in the ergonomic laboratory located in USWR. In the middle of an 8 m walkway, two Kistler Force Plates were recessed in series.
The process of testing was entirely explained to the participants, and at the completion of the orientation, the participants who consented to participate in the trial were examined and tested. The subjects were asked to walk at a normal pace in the laboratory environment for 5 min so as to adapt to each shoe prior to testing each of the test conditions. Before testing, weight of each individual was determined using the force plate. Right leg data were extracted for final analysis. Three conditions were tested in a randomized order: (1) walking with orthopedic shoe having standard heel, (2) walking with orthopedic shoe having beveled heel, and (3) walking with orthopedic shoe having PPHF. Subjects were asked to rest for 5 min between each trial. The subjects walked two steps before striking the first force plate. Participants were asked to walk at a normal and self-selected pace. The speed of the subjects was measured by a chronometer and trials of over 5% speed difference were eliminated.2,25 The data were then collected from the six successful trials in each test condition.
The primary variables of interest were as follows: impact force (Fz0), the vGRF first peak in the phase of loading response (Fz1), time of the vGRF first peak (T1), loading rate, minimum vGRF in the phase of midstance (Fz2), the vGRF second peak (Fz3), maximum posterior–anterior GRF, and stance time (Figures 4 and 5). Data of GRFs were normalized to percentage of BW and T1 was normalized by subject’s total-stance time. The impact force is seen as a short spike of force (typically occuring within the first 50 ms), superimposed on the upslope of the GRF, immediately following initial contact of the foot.
9
Stance time was defined as time of total-stance phase from the initial contact to the toe-off phase. In this research, the loading rate was measured from the division of the first peak magnitude of vGRF within loading response phase by the time between the initial contact and the time of occurrence of the vGRF first peak (
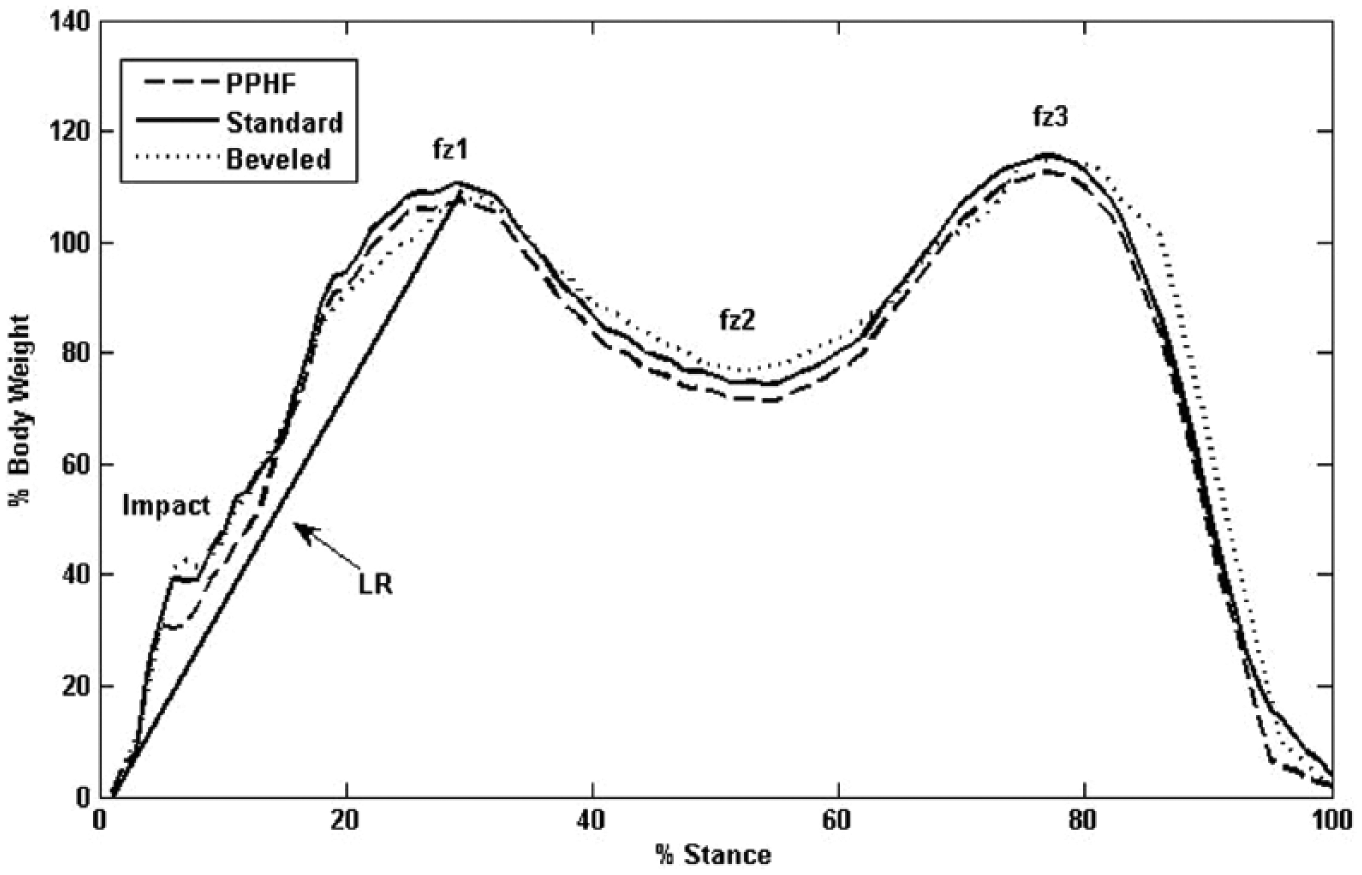
Vertical ground reaction curve demonstrating the impact force, which occurs shortly after foot strike; and vGRF first peak (Fz1), which occurs during the double-stance phase. The loading rate (LR) is the slope of the line from initial contact to vGRF first peak.
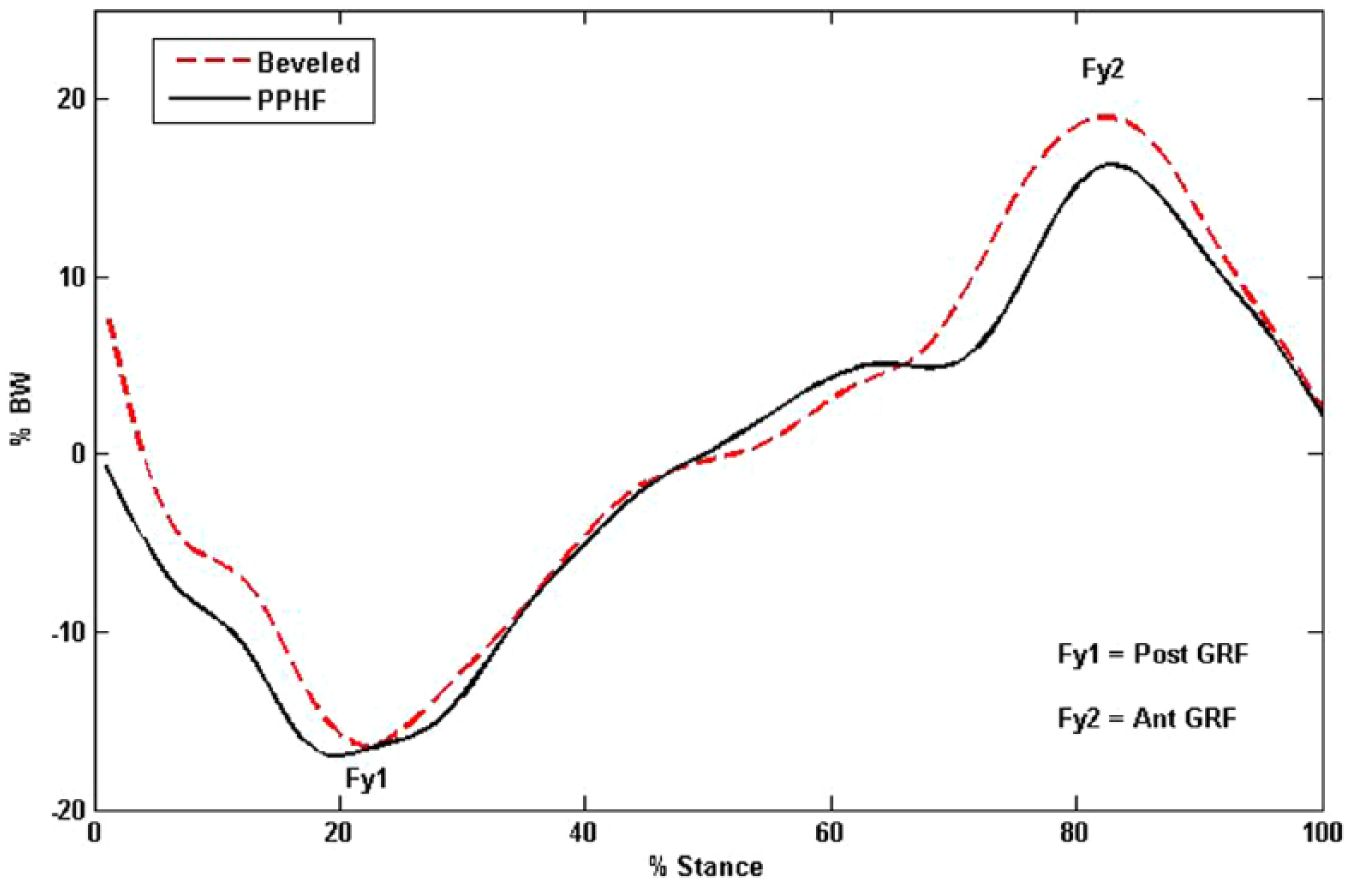
Posterior–anterior component of the GRF (fore- and aft shear). The posterior force (Fy1) occurs at heel strike for making slow the forward progression of the body and anterior force (Fy2) occurs at toe off for propelling the body forward.
Results
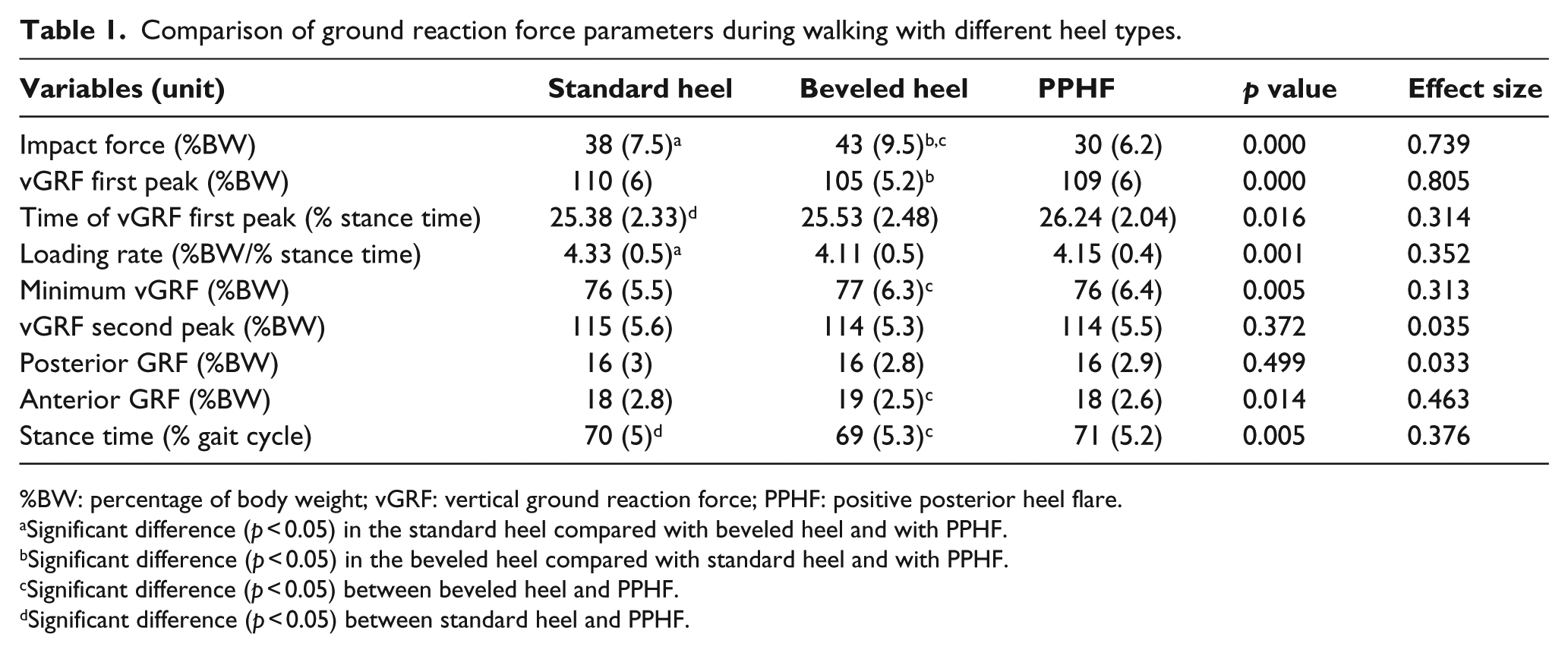
Using orthopedic shoes with different shapes of the heel had a significant effect upon GRFs during normal gait. The results demonstrated that with the PPHF, the impact force was significantly lower than both the standard heel and beveled heel (8% and 13%, respectively). The impact force was significantly increased by 5% in the beveled heel compared with the standard heel (p < 0.001).
Evaluation of the GRFs showed that vGRF first peak with the beveled heel was significantly lower than that with both the standard heel and PPHF (5% and 4%, respectively).
The loading rate in the beveled heel and PPHF was significantly decreased in comparison with standard heel (0.22% and 0.18%, respectively). The time of vGRF first peak significantly increased in PPHF compared to standard heel (p < 0.05). No differences were observed in the posterior GRF with differing heel shapes (p > 0.05). Anterior GRF was significantly reduced with the PPHF when compared to the beveled heel (p < 0.05). There was no significant difference in the anterior GRF between the standard heel and the beveled heel or between the standard heel and PPHF (p > 0.05). Stance time, however, was significantly increased with the PPHF in comparison with the beveled heel. The mean, SD, and p values for GRF parameters in the stance phase of walking are indicated in Table 1.
Comparison of ground reaction force parameters during walking with different heel types.
%BW: percentage of body weight; vGRF: vertical ground reaction force; PPHF: positive posterior heel flare.
Significant difference (p < 0.05) in the standard heel compared with beveled heel and with PPHF.
Significant difference (p < 0.05) in the beveled heel compared with standard heel and with PPHF.
Significant difference (p < 0.05) between beveled heel and PPHF.
Significant difference (p < 0.05) between standard heel and PPHF.
Discussion
The present data demonstrate the influence of three heel shapes of orthopedic shoe on the GRFs in the stance phase of the gait in the young healthy subjects. Reducing the dynamic loads acting upon the lower limb is important for various reasons including minimizing the risk of overuse injuries, 8 low back pain, 27 and osteoarthritis of the knee.28,29 These findings suggest that altering the characteristics of footwear, such as restructuring the heel, might have a substantial influence on the impact-related loading during normal ambulation.
Based on the results, the PPHF was effective in reducing the impact force between the foot and the ground in comparison with the standard heel or beveled heel. It appears that because the flare extended posteriorly, flexibility of the outsole is increased, 20 and as a result, the impact force dissipation at heel contact is decreased. The standard heel and beveled heel had less flexibility than the PPHF and increased impact forces were observed. In all probability, due to the shape of the beveled heel, and it is not having an edge and a large level contact area with the ground at the instant contact, 30 it causes less pressure to the foot, therefore understanding that the subjects’ exerted force to the foot is reduced, he (she) may exert greater force to the ground. The efficacy of the beveled heel in reducing impact force has not previously been demonstrated. Furthermore, additional studies are required to examine and confirm the geometrical shape of the beveled heel and the impact force exerted.
These data indicated that the beveled heel lowered the vGRF first peak as compared with the standard heel and PPHF. The beveled trailing edge on the shoe’s heel most likely allows the foot to roll forward in its step, softening the movement. Furthermore, less muscle strain potentially means less discomfort, 31 and as a consequence, the vGRF first peak is decreased. In an earlier study, it was demonstrated that the beveled heel more so than the standard heel in stroke patients could be used to decrease the loading of the limb at the loading response phase. 19 The beveled heel alters position of the GRF relative to the ankle joint axis and facilitates the forward progression of the center of pressure. This may reduce the demand on the quadriceps by decreasing the external flexor moment acting at the knee during the loading response phase. 32 Conversely, a PPHF can increase the lever arm of the GRF on the ankle joint between initial contact and the loading response phase, requiring an increased effort from the anterior compartment muscles and potentially giving rise to the anterior shin splints.15,31 Based on this result, a beveled heel would be recommended over a standard heel and a PPHF to reduce vGRF first peak during the gait in a young and otherwise healthy population.
A PPHF increased time of vGRF first peak as compared to the standard heel. However, the normal gait cycle requires some knee flexion in the loading phase. 33 The use of the PPHF creates a knee-extensor moment at heel contact, 18 and thus, it is possible that PPHF needs some time to reach the normal knee flexion. The effect of the PPHF in increasing time of vertical force has previously been demonstrated. Menz et al. 20 stated that a PPHF compared with the standard heel and the beveled heel increased outsole flexibility at heel contact; thus, the shoe took comparatively longer to grip the surface when vertical force was applied. Queen et al. 15 showed that a PPHF by increasing dorsiflexion angle at heel strike was most likely the result of the subjects contacting a more posterior portion of the shoe sooner during the swing phase, and subjects could have also chosen to contact the ground earlier, thus they increased the contact time between the foot and the ground.
In this study, the use of PPHF led to reduction in the loading rate in comparison with the standard heel. It is possible that a heel flare increases the surface area for weight-bearing enabling the ground reaction force to be dissipated over a larger region, thereby altering somatosensory feedback from the sole of the foot 34 and reducing the loading rate to the body. Regarding the formulation of loading rate, significant decrease in the time of the vGRF first peak in the PPHF than that of the standard heel decreased loading rate. Queen et al. showed that a PPHF with 11° ± 1° angle compared to a PPHF with 2° ± 1° angle posteriorly reduced the loading rate during running. They stated that the decrease in the slope of the vGRF first peak may have resulted from the subjects landing in more dorsiflexion, with greater dorsiflexion excursion resulting in the vGRF being applied over a longer time, thereby decreasing the slope of the vGRF first peak. 15
The loading rate with the beveled heel as compared with the standard heel significantly decreased. Regarding the formulation of the loading rate, most likely due to a significant decrease in the vGRF first peak in the beveled heel, the loading rate demonstrated a significant decrease. Moreover, the forward rolling motion of the beveled heel used less muscular force, thus the loading rate was decreased and the movement was softer. 31 Choi 35 stated that shoes with rounded outsoles and a mild slope in the heel decreased the vGRF first peak and the loading rate in the healthy subjects because of having a softness in motion. Orthopedic shoes with a beveled heel in this study had a mild slope in the heel which was similar to the results of Choi’s study in decreasing the loading rate.
These results showed that the beveled heel increased the minimum vGRF compared to the PPHF. It appears likely that geometrical shape of the beveled heel due to its rocker curve allows the foot to roll forward in its step. Therefore, a greater force is applied to the ground in the midstance phase; as a result, minimum vGRF increased with the beveled heel.
These data indicated that no differences in the posterior GRF were observed among the three heels. This result is in contrast to the results of Queen et al. 15 that demonstrated that a PPHF with 11° ± 1° angle in comparison with a PPHF with 2° ± 1° angle reduced posterior GRF. This contrast could likely be due to the gait speed, differences in the type of shoes, angles of heels, or test conditions.
Based on the results collected in this trial, the PPHF reduced the anterior GRF significantly as compared to the beveled heel results. It appears likely that the heel flaring by increasing the base of support and increasing the time interval from the initial contact to the occurrence of the toe-off increases stance time. As a result, the body is momentarily decelerated and in essence, the anterior GRF is reduced. However, the beveled heel due to its rocker curve propels the body forward and the findings of this study showed that stance time was decreased. As a consequence, the body is momentarily accelerated forward, as a cause of an anteriorly directed GRF.
There are some limitations to this study. First, the present data pertain to a young healthy population wearing orthopedic shoes. Since age 36 and pathological status 6 can all influence impact-loading characteristics during the gait, the effect of the orthopedic shoe use with different shapes of the heel in different populations may not be consistent with the findings in this study. Second, the immediate biomechanical effect of the heel shape on GRFs was investigated and the longer term effects are unknown. In future studies, it is recommended that a wider range of heels are explored in various patient groups. This should be coupled with the exploration of other areas of gait analysis that could include electromyography, kinematic analysis, and kinetic analysis of ankle (i.e. plantar flexor moment and ankle power).
Conclusion
Based on the findings of this study, it is considered that due to the beveled heel in the orthopedic shoe changes the location of the GRF relative to the ankle joint axis, can facilitate first rocker. As a result, a beveled heel can be useful for subjects who have weak ankle motion control and can also decrease the vGRF first peak and loading rate. In addition, the PPHF in the orthopedic shoe due to its flexibility can reduce the impact force during the heel strike. Heel design is likely to be responsible for the observed reductions in vertical forces and should be considered as part of shoe design for patients with associated lower limb conditions where impact forces need to be minimized.
Footnotes
Acknowledgements
This manuscript is a part of a dissertation entitled “Examining the effects of standard heel, positive posterior heel flare and beveled heel in orthopedic shoe on the GRFs during walking in healthy subjects” that has been conducted by the support of Iran University of medical science and University of Social Welfare and Rehabilitation Science. We also appreciate the clinic of orthopedic shoe of the center of Tehran Red Crescent Society and the students and staff who participated in this study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.