
Abstract

0012
Zeshan Zahid (1) presenting
Rawalpindi Medical College, Rawalpindi, Pakistan (1)
Clinical Trials of newly designed APPNA Orthopedic Rehabilitation Institute (AORI) Foot Abduction Brace and comparison with DENNIS Brown Splint
Clubfoot is commonest congenital deformity in babies. More than 100,000 babies born worldwide each year with clubfoot. The main goal is to achieve a functional, pain free, planti-grade foot with good mobility. Treatment of idiopathic CTEV is serial gentle manipulations and after casting, splinting/bracing to maintain the correction. The main reason of relapse of deformity after correction is non-compliance to bracing program as it is a lengthy process.
The aim of study is to develop a standard, light weight & cost effective Foot Abduction Brace to address the issues of non-compliance and to check its effectiveness.
It was 3 years non randomized interventional study from April 2011 to March 2014 with convenient sampling. Sample size was 110 patients using Dennis Brown and AORI Foot Abduction Brace were divided in study and control group. 30 patients using AORI Foot Abduction Brace were included in study group where as 80 patients using Dennis Brown Splint was included in control group. Study was performed at Department of Orthotics & Prosthetics of Benazir Bhutto Hospital Rawalpindi.
Deformity relapsed in 15% of patients in control group no relapsed was reported in study group where P-value was <.05 that is significant. Skin damage occurred in almost 50% of patients in control group it was reported about 20% in study group with P-value = <.05 which is significant. Residual adduction was reported in >50% of patients in control group and it was reported 0% in study group with P-value = <.001 which is highly significant. Fabrication Cost of AORI Foot Abduction Brace was is almost half of the DB Splint. No leather and steel work is required so that an Orthotist can make it easily. It can also industrialize and easily adjustable by the families.
Clinical trials of AORI FAB showed very good results in maintenance of corrected CTEV as the families are more compliant with AORI FAB because it is light in weight have dynamic effects for Dorsi-flexion while Dennis Brown splint is relatively heavy and found poor to maintain Dorsi-flexion that leads to the relapse of equinus. Skin damage is also less in AORI FAB and it is cost effective with ease to fabricate without extensive work.
0015
Malik Oleiwi (1) presenting
Medical institution / Baghdad, Baghdad / al baldyat .box 287, Iraq (1)
A alternative adjustable socket brim design for Ischial Containment Socket for Trans Femoral amputees
This research explains the process carried out to design and use of alternative adjustable socket brim design if (ICAB) ischial containment socket for (TF) transfeomral amputee, by using locally available material. The study was carried out in three stages. The first one was to design and fabricate ischial containment adjustable brim (ICAB) out of locally available material. In the second stage, casting took place using the ICAB, the third stage, two subjects were fitted with ICAB socket only and one subject was fitted with prosthesis.
This study was to design and fabricate the adjustable ischial containment brim as an alternative method of taking cast of Trans femoral amputee.
The experimental study, based on convenient sampling was conducted at Tanzania Training Centre for Orthopaedic Technologists (TATCOT) at Kilimanjaro Christen medical Centre (KCMC). Six respondents participated. The inclusion criteria were related to age, proximal circumferences of the stump, gender, good stump condition and experienced prosthetic user. This resulted the sample size of six subjects who were secondary user of prosthesis out of which 66.6% (4/6) were males and 33.4% (2/6) were females. After the delivery of the prosthesis, the subject was followed after period of two months.
The IC adjustable socket brim was fabricated for three out of six (3/6) subjects, three out of six (3/6) were taken for the casting of IC socket by the adjustable IC brims. Two out of three (2/3) fitted with IC transfemoral socket, one out of three (1/3) was fitted with the prosthesis using the IC adjustable socket brim method for taken cast with the new method of taking cast, 90% (2/3) subject indicated that fitting was good and they did not experience any problems during fitting and weight bearing. However 10% (1/3) of the subject indicated that, the shape of the proximal brim is slightly different because previously he was using Quad socket and he was familiar with that.
While there was a limitation of number of subject and the time duration of using the prosthesis, all users participating in the study confirmed good fit and mainly the considerable reduced time during casting. This study suggest that the use of three locally manufactured ICAB is cost effective but might also be an appropriate tool for less experienced practitioners leading to adequate ischial containment socket fit.
Bennett–-Wilson, A.(1968) Recent Advances in Above–-Knee Prosthetics. Artificial Limbs. [online] Available from: http://www.oandplibrary.org/al/pdf/1968_02_001.pdf. [Accessed on 3 June 2013].
Czerniecki, J. (2006) Rehabilitation after Traumatic Brain. Lower Extremity Amputation.
In Robinsson, L.R. (2006) Trauma Rehabilitation. Philadelphia. Lippincott Williams & Wilkings.
Kaphingst,n A. and Raabd, W. (2001) Prosthetic Information for the Rehabilitation Team. VIETCOT Guideline for Prosthetic Management Lower Extremity Amputations.
Hanoi, Ministry of Culture and Information.
Kapp, S., Miller, J.A. (2009) Care of the Combat Amputee. Washington. TMM Publications.
Lusardi, M. M., Nielsen, C.C. (2012) Orthotics and Prosthetics in Rehabilitation. Elsevierinc. Missouri.
Gottshalk, F. (1996) Transfemoral amputation. Biomechanics and Surgery. Clinical Orthop 361:15–-22
Hampton, F. (1966) Suspension Casting for Below–-Knee, Above–-Knee, and Syme’s Amputations. Artificial Limbs.10(2), pp: 5–-26
Hoyt C, Littig D, Lundt J, Staats T. (1987) The Ischial Containment Above–-Knee Prosthesis: Course Manual. 3rd ed. Version 1.3.Los Angeles, Calif: UCLA Prosthetics Education and Research Program.
0018
Heather Batten (1,2) presenting Allison Mandrusiak (2) Suzanne Kuys (5,6) Steven McPhail (3,4)
Princess Alexandra Hospital, Brisbane, Queensland, Australia (1) The University of Queensland, Brisbane, Queensland, Australia (2) Centre for Functioning and Health Research, Brisbane, Queensland, Australia (3) Queensland University of Technology, Brisbane, Queensland, Australia (4) The Prince Charles Hospital, Brisbane, Queensland, Australia (5) Griffith University, Gold Coast, Queensland, Australia (6)
Ability of gait speed to predict prosthetic walking potential following lower limb amputation; a descriptive study
Gait speed has been shown to be a reliable predictor of functional ability, future health status including functional decline, hospitalisation and institutionalisation, and death in neurological conditions. Gait speed is a quick and efficient assessment method; yet, to date, there has been little investigation of its potential use in predicting outcomes in populations with lower limb amputation.
To determine gait speed of a large cohort of unilateral lower limb amputees (transtibial level or higher amputation) at discharge from inpatient rehabilitation and to investigate relationships between gait speed, prosthetic potential (as classified by K-level) and functional independence.
A retrospective cohort study was conducted of 111 individuals admitted to inpatient rehabilitation following lower limb amputation from 2005 to 2011 who were prescribed a prosthesis. Measures included gait speed, Functional Independence Measure motor subscale (FIM-Motor) and prosthetic potential, measured using K-level. Median and interquartile ranges (IQR) were used to describe gait speed and FIM-motor for each of the ordinal K-levels (K1-4); which were not normally distributed. Spearman’s correlation coefficient was used to examine the strength of association between K-level, gait speed, and FIM-Motor.
Median (IQR) gait speed for each K-level was: K1, 0.17 (0.15-0.19) m/s, K2, 0.38 (0.25-0.54) m/s, K3, 0.63 (0.50-0.71) m/s and 1.06 (0.95-1.18) m/s for K4. Median (IQR) FIM-Motor scores for K-level 1-4 were 82 (69-84), 83 (79-84), 85 (83-87) and 87 (86-89), respectively. K-level was positively correlated with discharge gait speed (rho=0.64, p<0.001), and discharge FIM-Motor (rho=0.50, p<0.001). Discharge gait speed was also weakly correlated with FIM-Motor (rho=0.36, p<0.001).
People classified at higher K-levels walked faster than those with lower K-levels. However, gait speeds observed across all K-levels indicated high risk of morbidity and mortality. The relatively narrow range of FIM-Motor scores observed across the four K-levels is likely attributed to the requirements for safe and independent discharge from hospital being satisfied. Once people are sufficiently independent (regardless of K-level), they are usually discharged from hospital to continue rehabilitation as an outpatient. Despite this ceiling effect, a moderate correlation was still evident between K-level and FIM-Motor score.
Rehabilitation programs should address factors contributing to slower gait speeds and incorporate gait speed training during prosthetic rehabilitation. Further research is required to investigate whether gait speed changes post discharge from hospital, and what influence further rehabilitation post hospital discharge may have on gait speed.
0019
Suci Anatasia (1) presenting
Politeknik Kesehatan Kementrian Kesehatan Jakarta I (JSPO), DKI Jakarta, Indonesia (1) Exceed (Jakarta), DKI Jakarta, Indonesia (2) ISPO Indonesia, DKI Jakarta, Indonesia (3)
Prevalence of Depression and Anxiety of Upper and Lower Limb Amputees at KCMC in Moshi, MOI and CCBRT in Dar es Salaam, Tanzania
Depression and anxiety may develop at anytime during the period surrounding the amputation, it may affect amputees’ recovery and independence (Carroll; 2006).
Prosthetists should be aware of the psychological issues that may influence patients’ rehabilitation. It may help to facilitate appropriate referrals and enhance the collaborative process of multidisciplinary team work (Desmond; 2002).
To assess the prevalence of depression and anxiety of upper and lower limb amputees at KCMC in Moshi, MOI and CCBRT in Dar es Salaam, Tanzania.
Study design of this research is a descriptive cross-sectional study. Sample population was taken from inpatients and outpatients within a sampled area of two hospitals and one center with orthopedic clinic in Moshi and Dar es Salaam, Tanzania.
Subjects available during study time were (n=47) and was assessed with HADS (Hospital Anxiety Depression Scale) that has been translated into Swahili. Respondents should be unilateral upper and lower limb major amputation, newly amputees to 6 years time since amputation, has no psychiatric historical background and in range of age 6 – 65 years old. The data processed with help of statistician by means of SPSS software.

Various levels of anxiety and depression influenced by many variables. Table above shows us relationship between depression, prosthetic use and trauma as the cause of amputation. In terms of anxiety level, marital status had significant result where married ones appeared to be much more affected than singles (
This study also suggested that occurrence of anxiety and depression last for a period of 2 years after amputation. These findings propped of study done by Hawamdeh (2008), Atherton (2006), Darnall (2005) and Adnan (2003).
This study has pretty similar result with other reported studies. Owing to time limitation, data collection has limited sample width and it may contribute to the lack of statistical significance.
In conclusion, various level of anxiety and depression in Moshi and Dar es Salaam influenced by many socio-demographic factors. Solid multidisciplinary team work and follow up is needed, remembering the result revealed that anxiety and depression exists at some period of time following amputation.
(Hawamdeh; 2008 Pubmed), (Atherton; 2006 Disability and Rehabilitation), (Carroll; 2006 Prosthetics and patient management), (Darnall; 2005 Achieves of physical medicine and rehabilitation), (Adnan; 2003 Military Medicine).
0020
Kadhim Resan (1) presenting Shireen Challoob (1) Yasir Ibrahim (1) Al-mustansiriyah, Urfally, Baghdad, Iraq (1)
Study the influence of stress relaxation on the below knee socket materials from creep test
Polymer and polymer-based composite materials are known to be viscoelastic. This makes the time-dependent behaviour a most important factor in the analysis and design of structures made of such materials. The time-dependency is significantly influenced by various environmental conditions. This study evaluated mechanical properties of the materials used to fabricate prosthetic sockets. Stress relaxation, the time-dependent property, was evaluated from creep test for different types of socket materials by using viscoelastic model.
This research studied the effect of stress relaxation and creep with time on the two types of socket materials and how socket materials deform with time as a result of the effect of stress relaxation .
This research used polypropylene sheet and composite material which are used in large scale in rehabilitation centersthen the creep test of specimens was used to to evaluate the properties of viscoelastic materials. The dimensions of a standard creep test specimen which is selected according to the ASTM-D2990, also the interface pressure was measure by F-socket method, The analysis of socket models was done by FEM software to compute the equivalent modulus stress and temperature. the patient socket was drawing at autocade program and then exported the drawing to ANSYS program to illustrate the effect of the decreasing of stress relaxation modulus in a structure element to determine the deformation in the two type of socket .
The theoretical and experimental calculations depend on the mechanical properties of the material and creep test ; The pressure resulted by patient on socket is determined by F-socket device as shown in Figure (1). the distrubution of this stress and deformation have been determined by using a ANSYS program

A although the materials tested at same conditions, material of polypropylene socket has lower resistance to creep than composite materials socket. And all materials affected by stress relaxation, the stress relaxation modulus of the material of polyproplene has high decreasing rate with time than another type .
Nicholas Herbert, David Simpson,William D. Spence,William Ion, “A preliminary investigation into the development of 3-D printing of prosthetic sockets” JRRD, Volume 42, Number 2, 2005.
Kadhim. K. Resan “Analysis and Design Optimization of Prosthetic Below Knee” Ph.D. thesis, Mechanical Engineering Department, University of Technology, Baghdad, 2007.
0022
Adam Goodworth (1) Diana Veneri (1) Daniel Lee (1) presenting John Burger (2)
University of Hartford, West Hartford, CT, USA (1) New England Orthotic & Prosthetic Systems, Middlebury, CT, USA (2)
Preliminary Design and Evaluation of a Knowledge Based Outcome Measure for Patients with a Lower Limb Prosthesis
Patient education and reliable outcome measures are critical for success in any prosthetic clinic. However, current validated outcome measures are restricted to assessments of mobility, self-efficacy, or self-assessed quality of life. Yet it is clear that patients with a new prosthesis must have competency in domains of knowledge because patients need proficiency in problem solving and cognitive skills related to donning/doffing, skin care, fitting, emergency management, cleaning, and rehabilitation. Knowledge is especially needed in areas with limited access to clinics.
The current study had two goals: to develop a knowledge outcome measure for prosthetics (KOMP) and to perform preliminary field testing of this tool in the US and East Africa.
The KOMP was initially developed as a 36-question yes/no quiz based on literature reviews and interviews with 10 prosthetists with international experience. The KOMP was written at a 6th grade reading level. The KOMP was distributed and evaluated amongst a total of 35 patients with lower limb amputation: 16 in the USA and 19 in Uganda and Kenya. All but 2 patients had experience wearing their prosthesis for at least 6 months. The KOMP was also tested amongst 26 non-amputee “controls” in the US. Usefulness of the KOMP was inferred through open-ended feedback and performance on the quiz. Repeated-measures ANOVA and post hoc testing was performed to determine which questions had significantly different scores. T-tests were used to determine if scores differed between controls and patients.
We anticipated scores to range between 50%-100% because 50% represented random guessing whereas 100% represented a perfect score. Patients were correct on ~87% of questions (74% above random) whereas control subjects were ~77% (54% above random), which was a statistically significant difference. This difference indicates that the KOMP was sensitive to knowledge obtained from experience with prosthetic use. The average East African score was similar to US, but time constraints prevented us from testing all questions in East Africa. Our pilot testing also revealed that some questions were ambiguous and some had answers that were too obvious.
The present study is the first development and field testing of a knowledge-based outcome measure. Best practice indicates that including the target population in the process is a key component of success.1 Our preliminary results led to several modifications to reduce ambiguity and obvious answers. The current KOMP is 21 questions and is undergoing reliability and validity testing for US applications following the National Institute for Health’s PROMIS system (Patient reported Outcomes Measurement Information System) of scientific standards. We have also developed an illustrated question-answer education tool for international use that contains minimal words and compliments the KOMP. Our field testing was performed in collaboration with a larger prosthetics education project in partnership with LIMBS International.
1Dowse, R., Ehlers, M. (2001) Patient Educ Couns,
0024
Lena Gudmundson (1) presenting Hanna Löwén (1)
Bräcke diakoni, Stockholm, Sweden (1)
Rehabilitation and Outcomes of Patients with Lower Limb Amputation
The walking school at Rehabcenter Sfären, Bräcke diakoni (former Red Cross Hospital) is an outpatient unit that serves the entire Stockholm County Council. As a specialist center for people with lower limb amputation there is an average over the last three years of 246 patients and 2662 visits/year. The main goal is to offer patients the opportunity to develop their ability to walk and move with prosthesis and increase their independence.
The aim of this report was to describe rehabilitation and outcomes of patients with bilateral transtibial amputation (BTA) and compare the outcomes with a control group (CG) consisting of patients with unilateral transtibial amputation (UTA).
This is a retrospective data register report. All patients with BTA that underwent rehabilitation during the time period of 2011-01-01- 2014-06-30 were included n=30, 10 women/20 men, mean age 65 years. Cause of amputation was vascular disease without diabetes in 9 cases, diabetes in 12 cases, 5 with infection and 4 due to trauma. The control group consisted of 30 patients with UTA rehabilitated at the same period, 11 women/19 men, mean age 72 years. Cause of amputation was vascular disease without diabetes in 10 cases, diabetes in 10 cases, 2 with infection, 5 due to trauma and 3 due to tumor. Functional outcome of the rehabilitation was evaluated by the physiotherapist’s assessment of how patients managed to stand up and walk both indoors and outdoors. Two alternatives were given: with personal assistance or independently.
All patients, 60 persons, were able to stand up with prosthesis. In the bilateral group 73 % were independent compared to 77 % in the CG. 63 % of the bilateral amputees were independent in walking indoors compared to 73 % in the CG. 37 % of the bilateral amputees were able to walk outdoors independently compared to 57 % in the CG.
We were surprised over the positive outcome for the BTA group and that the difference between the groups was not greater. Prosthetics improves not only the patients seating comfort but also gives them better balance and support area and decreases the risk of falls from wheelchair. It also enables the patients to transfer safely and independently from wheelchair to bed without the need of help from caregivers or lift. Being able to stand up and walk also decreases the risk of decubitus and improves the blood circulation.
Prosthetic supply can play an important role for BTA, as well as for UTA regarding locomotion. This can mean the difference in being independent and being able to participate in daily life activities or not.
0026
Øyvind Bernhardsen (1) presenting
University of Tromsø, Tromsø, Norway (1)
The Amputee Mobility Predictor; translation into Norwegian and inter-rater reliability
The Amputee Mobility Predictor is an instrument designed to measure ambulatory potential of lower-limb amputees with (AmpPro) and without (AmpNoPro) the use of a prosthesis. The instrument has never before been translated into Norwegian and inter-rater reliability of the Norwegian version has therefore not yet been examined.
The aim of this study was to translate the Amputee Mobility Predictor into Norwegian, and to assess the between raters (inter-rater) reliability of the Norwegian version of instrument based on video recordings of the test performances.
The translation process consists of three stages: translation, back-translation and comparison with the original version.
Twenty-four adult lower-limb amputees were recruited and classified according to ability to ambulate. The Amputee Mobility Predictor performance of participants was filmed. All participants were tested with and without prosthesis. The exception was two subjects that only were tested without prosthesis since they did not use one, and two bilateral amputees that only were tested with their prosthesis since testing without was not possible. Seven raters then scored the film once. For total scores on The Amputee Mobility Predictor, relative reliability was investigated for calculating Intraclass correlation coefficients (ICC1.1 and ICC3.1).
For individual items, Cohen’s kappa (k) and percentages agreement were calculated. Bland-Altman Plot was used to verify the consistency of measurements graphically.
The back-translated version was found to be in good accordance with the original version when it came to contents.
The study showed that the Norwegian version of The Amputee Mobility Predictor had excellent inter-rater reliability. Respectively ICC1.1=0.98-0.99 an ICC3.1=0.98-0.99 for assessment without prosthesis and ICC1.1=0.94-0.99 and ICC3.1=0.94-0.99 for assessment with a prosthesis. Kappa values for the individual items ranged between 0.11-1.00. The majority of items, 77,2 %, showed very good or good agreement (k≥0.61).
Results should not be generalized to individuals with cognitive impairments, as they were not included in this study.
This study showed a very high inter-rater reliability of The Amputee Mobility Predictor on lower limb amputees tested both with and without prosthesis. The majority of the individual items showed very good or good agreement, some moderate and one item slight agreement.
The study indicates that the Norwegian version is a reliable instrument for lower limb amputees with different function scored by physiotherapist with diverse working experience.
0028
Ahmad Aziz (1) presenting
PIPOS, Peshawar, Pakistan (1)
Correlation between psychosocial issues and noncompliance in spinal Orthosis in patients with adolescent idiopathic scoliosis
AIS is treated in skeletally immature patients conservatively with spinal orthosis, and has proved its efficacy to decrease or prevent the curve progression4, 5, with full time compliance (20-23 hrs/day) 6, 7. Orthotic management of scoliosis is a disturbing experience for adolescent clients and families8, 9 with an ongoing problem of compliance10.
The aim of this study is to find a correlation between psychosocial issues and noncompliance in spinal orthosis, in patients with adolescent idiopathic scoliosis.
The brace questionnaire (BrQ) was used to collect the quantitative data. All the questions were answered according to the likert scale in the following five responses, “Always”, “Most of the times”, “Some times”, “Almost Never” and “Never”. Descriptive statistical analyses were done and a correlation coefficient test was applied to get the results.
The total numbers of participants were 11 (04 boys and 07 girls) with mean age of 11

In contrast to many researchers we found that young clients fitted with SO were not using special clothing (63.6%). The average negative psychosocial impact was 52.4%
The difference in results of this study to previously published material may be due to the different demographics and culture in which the study was performed. Psychosocial counseling of adolescents with AIS along with orthotic treatment may improve compliance and therefore, the outcome.
Allington, N.J., & Bowen, J.R.(1996). Adolescent Idiopathic Scoliosis: Treatment with Wilmington Brace. A Comparison of Full-Time and Part-Time Use. J. Bone Joint Surg. Am. 78, 1056-62.
Amato, C.R., Griggs, S., & McCoy, B. (2001). Nighttime Bracing with the Providence Brace in Adolescent Girls with Idiopathic Scoliosis. Spine. 26(18), 2006-2012.
Climent, J.M., & Sanchez, J. (1999). Impact of the Type of Brace on the Quality of Life of Adolescents With Spine Deformities. Spine. 24(18), 1903-1908.
0029
Nizar Akhtar (1) presenting Kevin Murray (1)
Pakistan Institute of Prosthetic and Orthotic Sciences, Peshawar, Pakistan (1)
Functional outcomes and the influence of secondary complications in prosthetic rehabilitation of children with acquired amputation or congenitally deficient limbs… A literature review
Children with limb amputations or congenital deficiencies come across a lifetime of functional restrictions. Most of the amputee children are fitted with prostheses or ortho-prostheses to make them able to perform daily activities and reach to the milestones. Common secondary complications like bony over growth, phantom sensation and phantom pain are mainly responsible to influence the functional aspects of children with limb loss. None of the included literature has mentioned the influence of these complications on prosthetic functional outcomes except to some extent by Vannah et al. (1999).
The objective of this literature review is to describe the effectiveness of prostheses and the influence of secondary complications on the functional restoration of children with amputations.
A comprehensive review of literature was conducted on prosthetic functional outcomes, impact of post amputation complications e.g. bony overgrowth, phantom sensation and phantom pain in children with congenital or acquired upper, lower or both extremities amputation. A systematic search was conducted for literature review using several databases. Fourteen studies were included in this review. Selected studies were summarized in tabulated form in terms of Study, Study design, Sample size, Age, Variables measured, outcome measure, Prosthetic Functional Outcomes and Secondary Complications. The literature available till date has rarely studied the impact of post amputation complications on functional outcomes of artificial limbs.
Generally the literature revealed that the functional abilities of children with LL or UL deficiencies were satisfactory. In almost all included studies, the Independence in walking, sports and other physical functions were improved between 80 to 90% except in Vannah et al. (1999) study in which just over 50% of LL deficient children were able to participate in sports related activities. Conversely, three studies argued that prostheses did not appear to develop the functional abilities of children with UL deficiencies.
Bony overgrowth is mentioned in only three studies and none of the studies have measured its effect on prosthetic functional outcomes. Although, 20% of LL prostheses rejection is because of pain but it is not mentioned to how much extent physical triggers of phantom sensation accounted for cessation of prostheses.
Eight studies reported substantial improvement in prosthetic functional outcomes. However, only one study has shown low score in regards of ADL and sports activities. Generally, only three studies have mentioned to some extent the influence of secondary complications in prostheses outcomes. The interventions and variable measurement methods were considerably different in these studies. Similarly, some studies were conducted with very small sample sizes because of which these studies have low score in internal and external validity. Research to identify factors that affect the effectiveness of prosthesis in children and adolescents with acquired or congenital deficiencies needs to be done.
1. Aitken (1963). JBJS
2. Boonstra (2005). POI
3. Buffart (2005) Conference Proceedings MyoEletric Controls/ Powered Prosthetics Symposium.
4. Melzack (1997). Brain
5. Pruitt (1999). Archives of Physical Medicine and Rehabilitation
6. Sener (2001). POI
7. Kuyper (2001).POI
8. Vannah (1999). POI
9. Korkmaz (2012). Acta Orthop Traumatol Turc
10. O’Neal (1996). JPO
11. Vocke (2000). Archives of Orthopedic trauma and Surgery
12. Huizing (2010). POI
13. Wilkins (1998). Pain
14. James (2006). JBJS
0030
Jennifer Langford (1) presenting Alana Stonehouse (1)
Royal Melbourne Hospital, Parkville, Victoria, Australia (1)
The Rehabilitation Pathway of a Quadrilateral Amputee
A patient was admitted to Royal Melbourne Hospital following bilateral transradial and transtibial amputations secondary to streptococcal A. There is limited literature available regarding the rehabilitation pathway of a quadrilateral amputee.
To describe the multidisciplinary rehabilitation pathway of a quadrilateral amputee.
The rehabilitation pathway for the patient was compared to the standard Melbourne Health and Veterans Affairs pathways for unilateral amputees including: goal identification in line with the International Classification of Functioning, Disability and Health (ICF); timing and sequencing of milestones; barriers and solutions to rehabilitation goals; prosthetic prescription and outcome measure selection.
The patient was motivated to return to her previous level of appearance, mobility, function and community participation. Due to her four amputated limbs, she identified both upper and lower limb as well as prosthetic and non-prosthetic goals. These consisted of: cosmetically pleasing prostheses; independent feeding, toileting and dressing; independently using ipad/iphone; independent mobility +/- prostheses and returning to community activities. Timing of rehabilitation milestones were delayed due to slow healing lower limb wounds. Initial focus was on non-prosthetic mobility and upper limb prosthetic rehabilitation. Cosmesis and independent donning was an indication for choosing myoelectric prostheses. She was discharged home having achieved a level of independence with her upper limb prostheses. She was readmitted three months later for intensive lower limb prosthetic training. Extensive scarring determined prosthetic prescription to prevent skin breakdown. The patient was unable to use her transradial prostheses to grip the rails for gait training so alternative gait aids were used. The patient was discharged home independently mobilising with her four prostheses and two crutches. The patient made significant clinical improvements on all the outcome measures completed during her rehabilitation admissions as outlined in Table 1.
Functional and Mobility Outcome Measures taken during Mrs M’s rehabilitation

Note. *P = average performance out of 10. *S = average satisfaction out of 10
In this case goal setting in line with the ICF significantly helped the team and the patient to determine the focus of rehabilitation. While the patient’s goals were similar to other amputees, her goals needed to include upper limbs and lower limbs as well as prosthetic and non-prosthetic goals. The team encountered several barriers including: scarring; strong preference for cosmesis; inability to grip rails with upper limb prostheses and a fractured patella. Throughout the inpatient rehabilitation no one outcome measure captured all aspects of the patient’s progress and therefore a selection of outcome measures was required. Future research documenting complex amputee cases would be beneficial to guide clinicians working in amputee rehabilitation.
0032
James Hawkins (1) Siamak Noroozi (1) Mihai Dupac (1) Philip Sewell (1) presenting
Bournemouth University, Poole, Dorset, UK (1)
An Investigation of the Ground Contact Point and Sagittal Plane Displacement of Energy Storage and Return (ESR) Composite Lower-Limb Prosthetic Feet during Running
Energy storage and return (ESR) feet are designed for active amputees [1]. Their design appears to be carried out on a trial and error basis [2]. It has also been recognised there is little compelling scientific evidence to guide the clinical prescription of ESRs [3].
The aim of this study is to provide insight into the dynamic behaviour of ESR prosthetic feet by investigating the effect of increased velocity on the ground contact point and foot displacement.
Sagittal plane displacement (utilising a displacement sensor attached between the proximal and distal end of the foot) and ground contact point (utilising a linear array of four piezo-electric ground force sensors on the metatarsal region) were recorded from an Ossur Flex-Run ESR foot attached to a highly active unilateral transtibial amputee while carrying out a series of running trials.
The data collected was analysed to provide information on and relationships between: stride cadence; ground contact time; swing phase time; timing and amplitude of maximum displacement; progression of the ground contact point.

The figure shows the average sagittal plane displacement from ten full strides of the Flex-Run foot while the amputee ran at velocities of 8kmh-1, 13kmh-1 and 18kmh-1 on a treadmill. These results show that maximum deflection of the foot increased minimally as the running velocity increased from 8 and 18kmh-1. In addition, ground contact time (280ms@8kmh vs. 180ms@18kmh) and stride time (750ms@8kmh vs. 560ms@18kmh) were found to decrease. An increase of force at the posterior sensor was found as the running velocity increased; indicating that the ground contact point of the foot progressed towards the rear of the foot at increased velocity.
Previous studies have assumed that a prosthetic foot and amputee forms a spring/mass system and therefore the ground contact duration at different running velocities should be comparable. This research concludes that ground contact duration decreases at increased velocity. This has been found to be due to the measured shift in ground contact point rearwards along the metatarsal region at heel-strike stiffening the foot spring rate, resulting in a shorter stride duration. Further research is now needed to generalise the relationship between the key variables to provide quantitative data to inform ESR foot prescription.
[1] Kobayashi, T. et al.; 2014; Clin. Biomech.
[2] Strike, S. et al.; 2000; Proc. Inst. Mech. Eng. H J. Eng.
[3] Hafner, B. et al.; 2011; J. Rehabil. Res. Dev.
0033
Gohar Abbas (1) Nizar Akhtar (1) presenting
PIPOS, Peshawar, Pakistan (1)
Effectiveness of Ponseti Technique in treatment of children with congenital Talipes Equino varus in PIPOS Rehab Services Program (PRSP, Pakistan
Most of the studies agreed that CTEV should be initially treated through conservative techniques, although the preferred technique is still controversial. Among the conservative techniques the success rate of ponseti approach is significantly higher and has fewer complications compared to other techniques like kite and Lovell or French physical therapy methods. On the other hand, several studies preferred surgical treatment to be favorable to get good results in short term follow up while Franke (1987) and Lehman (1994) reported disappointing results of surgical treatment in long term follow up. Because of the disappointing results of surgical treatment, clinicians have adopted interest in the ponseti method. The purpose of the study is to see the outcome of children with CTEV treated by Ponseti method in PRSP Pakistan.
The main objective of this study is to view the effectiveness of Ponseti technique in different club foot clinics of PIPOS to get functional and plantigrade foot.
Between February 2012 and January 2013, a total of 39 clubfeet children with 57 clubfeet (30 males, 9 females) were treated in the clubfoot clinic in PIPOS Rehabilitation services Program (PRSP). We analyzed the records retrospectively under the supervision of senior physiotherapist and senior Orthotist. Ethical approval was obtained from review board of Pakistan Institute of Prosthetic and Orthotic Sciences (PIPOS) and ethical committee of Khyber Medical University (KMU). Scoring was done as per guide lines of Pirani scale by the senior Physiotherapist and Orthotist.
Out of the total 21(54%) Were unilateral and 18(46%) were bilateral. Initially, 27(69%) clubfeet children were less than six months of age and 12(31%) were above six months. The average number of serial cast was about 6. Thirty-five (90%) children with clubfoot deformity had percutaneous tendoachilles tenotomy. None of the included patients was advised extensive corrective surgery by the treating orthopedic surgeon. The clubfoot correction was achieved in about 60% of patients by means of serial casting. There were only 3 (8%) relapses reported after the initial successful correction of the clubfeet deformities through ponseti method. Patients with relapses were again corrected by means of second series of casting followed by foot abduction brace.
Various non-surgical techniques have been in practice but the treatment outcomes were different and confusing for each technique. Various researchers have practiced Ponseti technique and consistently better outcomes were achieved. Colburn and Williams (2003) reported 94% response rate while Lehman et al. (2003) produced 92% response rate. We also found the same response rate as Lehman et al. (2003). Moreover Morcuende et al. (2004) produced better response rate of 98%. Our results clearly indicated that ponseti method has less relapse rate and better outcome in achieving the functional and plantigrade foot.
0034
Andreas Hahn (1,2) Michael Lang (2,1) presenting
Otto Bock Healthcare Products GmbH, Vienna, Austria (1) Otto Bock HealthCare GmbH, Duderstadt, Germany (2)
C-Leg Trial Fittings in Germany
Trial fitting is a standard procedure conducted prior to the prescription of C-Leg. In Germany approval requires demonstration of the utilization functional benefits offered by C-Leg. First results on an evaluation of 1200+ C-Leg trial fittings were presented earlier.
We investigate the relationship between subject’s capability to exhibit functional benefit and factors such as mobility grade, age and amputation etiology.
Data on 1223 C-Leg trial fittings conducted between May 2006 and June 2010 were analysed retrospectively.
83% of the subjects were male, mean age 55.6±15.1. Mean age at amputation was 38.1 ±20.6. Amputation etiology includes trauma [44%], vascular disease [24%], tumor [14%], infection [6%], combat trauma [4%], malformation [2%] and others [6%]. In 13.4% of the total population amputation etiology was not specified.
Most trials (90%) were conducted within one day. Data Analysis: Rates for responsiveness were evaluated. Kendall’s tau was used to investigate correlations of age, mobility grade and/or amputation etiology with respect to the capacity to show individual functional benefits, To quantify effect sizes the Logit multiple regression model was used.
Responder rates for functional benefits were 83% for increase in “safety”, 95% for “relieve of the sound leg”, 94% for “divided attention”, 95% for “gait pattern harmonization”, 93% for “variable gait speed”, 88% for an “overall reduction of effort” and 23% for a “reduction in walking aids”.
Stratification for Age, Mobility Grade (MOBIS) and amputation cause (vascular disease (VD)) showed to either not to correlate (safety, sound. leg, gait harmonization) or weakly correlate.
The calculated probabilities for predicting an individual’s potential of exhibiting a functional benefit based on age, MOBIS and/or VD range from 0.7% (gait harmonization) to 9% (variable cadence).
About 50% of subjects rated MOBIS 2 at baseline were rerated MOBIS 3 after trial fitting (95% CI [45%, 54%]).
The rate of responsiveness is comparable to those reported by e.g. Berry 2009 or Drerup 2008. No or only weak correlations could be found with respect to age, mobility grade and amputation etiology. The multiple regression showed, that age, mobility grade and/or amputation etiology possess very little power to predict individual functional benefit. The MOBIS reclassification after test fitting suggests that technology to a large extend influences mobility grade rating.
035
Amit Saraf (1) presenting
Saraswati institute of medical sciences, Ghaziabad, U.P., India (1)
Effect of postoperative ambulation level on the quality of life in a trans-tibial amputee
Quality of life of a trans-tibial (TT) amputee is not only determined by his functional rehabilitation but also social, economical and psychological rehabilitation. A number of studies have analyzed the influence of lower limb amputation on these factors. This study analysed the effect of functional recovery on other parameters of quality of life in a TT amputee.
To assess the influence of level of ambulation postoperatively on the socioeconomic and psychological aspects in a transtibial amputee.
This was a 10 years retrospective and 2 years prospective study. A total of 160 patients of trans-tibial amputation were followed. Their postoperative ambulatory status was calculated using Pinzur’s ambulatory level. Their quality of life was determined on the basis of answers to a five point questionnaire which included their social, economic and psychological aspects. These parameters were correlated to assess the influence of functional recovery on the quality of life.
All the amputees with Pinzur’s 0-1 level of ambulation suffered loss of income consequent to loss of job. All of them felt increased level of depression and anxiety after amputation. 50% of the patients with postoperative 0-1 level of ambulation felt socially neglected. Comparatively much less percentage of amputees with 5-6 level of ambulation suffered economic, social and psychological crisis.
Quality of life of a TT amputee is determined not only by his functional rehabilitation but also social, economical and psychological factors. From this study we concluded that post operative functional outcome significantly affects the quality of life of an amputee. An amputee with better ambulation level fares better economically, psychologically and socially in comparison to an amputee with poor ambulatory outcome.

Pinzur, M.S., Larsen, J., Smith, D. (1993). Functional outcome of BK amputation in peripheral vascular insufficiency. Clin Orthop Relat Res, 286, 247- 249.
0036
Rashi Gupta (1) presenting G. Pandian (1)
PDU Institute for the Physically Handicapped, Delhi University, New Delhi, India (1)
Introspective Study on Socio- Economical Issues Related to Lower Limb Amputees
Disability creates the major impact in life. Psychological problems were very much high which leads to various healths related issues. Very few people can able to adapt this loss. India stands very high in road traffic accidents and amputations. The amputees feels huge amount of unsaid and undescribed problems. Hence an extensive survey was conducted for the first time in India to find the solutions for their social and economical related issues.
The main motive behind conducting this survey is to explore the problems in their daily life both in society and at home. The outcome of this survey brought out the problems into limelight so that their issues can be addressed in a proper manner, because apart from limb fitting, care about their socio-economic related issues is also equally important.
A detailed questionnaire was made addressing almost all the issues related to psycho-social aspects of amputees. Most of the questions were objective with few questions - “Yes or No”.
All types of lower limb amputees those who are using prosthesis were taken in to consideration. The users were selected from conventional to high-tech prosthetic users. To explore the real and different issues, the patients were selected from - Government institutions, NGOs, private practitioners, and outreached programmes. All the participants were directly interacted face to face by the survey team by travelling into various parts of India.
Amputees with no prosthesis, less than 15 years of age, upper limb amputees are not taken into consideration.
The outcome of the study reflects various issues which we never come across, majority of the participants expressed their concern that the post amputation life have changed their normal life upside down. Huge number of participants expressed that, their personal life with family members were not up to the expectations like standard of living, education of their kids, carry out essential works, actively involving with the family members, relatives and friends. Apart from above, almost one out of three patients had a suicidal tendency before overcoming their problems, at the same time the equal number of patients have shown courage in adjusting their lives according to the circumstances and feel more responsible citizen in the society. During this study, the team met various types of participants from extreme painful life to extreme happy life.
All the results are purely based on the real life complications of the participants and it reflects their changes occur in socio-economic relations with respect to their personal and social life. Most of the issues faced by the participants were not been either addressed or the general public and rehabilitation professionals aware of issues. Though this type of research study has not been conducted by any of the Institutions or Organisations in India, hence result outcome cannot be compared with any previous finding.
0037
Marie THOMAS-POHL (1) presenting David ROGEZ (1) Hélène PILLET (3) Joseph BASCOU (4) François GENET (1,2) Eric LAPEYRE (1)
Military Hospital of Percy, CLAMART, France (1) Raymond Poincaré Hospital, GARCHES, France (2) Ecole Nationale Supérieure d’Arts et Métiers, PARIS, France (3) CERAH, PARIS, France (4)
Coupled analysis of the kinetic data of gait and functional MRI of the amputee. A case of brain plasticity and late acquisition of gait from a patient with congenital lower limbs atrophy
In France, 7800 new cases of amputation have been identified in 2005, with a small proportion of congenital amputations. Most of the patients reach adulthood either having been taken care in rehabilitation or using prosthesis. Mapping fMRI acquisition of an adult who never walked has seldom been studied in the literature.
- first, describe the modifications of the cortical representation with functional MRI (fMRI) during the gait learning with prostheses of a patient with congenital lower limb atrophy
- then, correlate these modifications with kinetic and kinematic parameters of gait analysis
Patient : a 17-year-old African girl, with congenital lower limbs atrophy, who underwent a double distal trans-femoral amputation at 15 years old. Without any reeducation nor prosthesis, she moves inside on her two stumps or with a manual wheelchair.
Materials and methods : fMRI and gait analysis before prosthesis (M0) and 6 months after (M6).
All motor sequences (active movement) of the initial fMRI present an activation of central regions and the supplementary motor area. This activation is predominant in the cortex contralateral to the stimulation side. Somatosensory stimulation activates the post-central region. Mental imagery activates areas similar to those activated during active movement. However, the activation is more intense in the supplementary motor area and there is an additional activation of the parietal, left frontal and left temporal cortex.
At 6 months, fMRI active (motor sequences) regains activation of the same areas as the one of the initial fMRI i.e. the motor contralateral cortex slightly more intense and extensive, the AMS and the premotor cortex.
Kinetic and kinematic parameters of gait were improved between M0 and M6.
For traumatic amputees, the representation of the lost limb is still part of the body schema, the corresponding motor cortex reorganizes incomplete and the contiguous zone expands. For the agenesics as for our patient, the activation is substantially identical to the healthy subjects, without reorganization or telescoping areas.
At M6, the kinetic and kinematic data of gait and fMRI show the acquisition of learning to walk by the improvement of the parameters of the quantitative analysis of walking and the concomitant activation of frontal and prefrontal areas and the increased activation of motor, premotor and supplementary motor areas of lower limbs.
Reilly KT, Sirigu A. Motor cortex representation of the upper-limb in individuals born without a hand. PLos ONE 2011;6(4):e18100.
0039
Eitan Raveh (1) presenting Sigal Portnoy (1)
Tel Aviv University, Tel Aviv, Israel (1)
Effects of adding vibrotactile sensory feedback on performance and visual attention during a dual-task assignment using a pseudo-prosthetic hand

1.Dudkiewicz I, Gabrielov R, Siev-Ner I, Zelig G, Heim M. Evaluation of prosthetic usage in upper limb amputees, Disabil Rehabil, 261:60-63, 2004.
2.Blank A, Okamura AM, Kuchenbecker KJ. Identifying the role of proprioception in upper-limb prosthesis control- Studies on targeted motion. ACM Trans Appl Percept 73, 2010.
0043
Akram Jamali (1) Saeed Forghany (1,2) presenting Christopher Nester (2)
Musculoskeletal Research Centre, Isfahan University of Medical Sciences, Isfahan, Iran (1) Centre for Health Sciences Research, School Health Sciences, University of Salford, Manchester, Iran (2)
The effect of three different insoles on ankle movement variability in athletes with functional ankle instability
Increased ankle movement variability has been reported in people with functional ankle instability (FAI). It is said to be due to mechanoreceptor injuries and neuromuscular impairments. Textured insole may improve variability by increasing tactile sensitivity in the plantar surface of the feet and lateral wedge may effect on the variability by decreasing inversion in people with FAI.
Therefore the purpose of this study was to investigate the effect of textured insole, lateral wedge and textured lateral wedge insole on ankle movement variability in athletes with FAI.
21 athletes with clinically diagnosed FAI participated in this study. Three-dimensional ankle kinematic data was collected by a seven camera Qualysis Proreflex system during four conditions (5 trials per condition): 1) Flat EVA base insole 2) Textured flat EVA insole 3) lateral heel and sole wedge insole (Salford insole) 4) Textured lateral heel and sole wedge. The analysis of ankle movement variability was conducted during stance phase and, 200ms before heel strike to 200ms after heel strike, using the coefficient of multiple correlations (CMC) to investigate pattern variability and Intra-class correlation (ICC) to investigate variability at the points of interest (i.e.: 200ms before heel strike, heel strike and 200ms after heel strike) .
In terms of pattern variability, during both time periods and in most planes, wearing textured lateral wedge increased CMC compared to other insoles. However, statistically significant differences were observed only in frontal plane during stance phase (p<0.05). There were no statistically significant effects from other insoles. The second highest mean CMC value in all planes was for textured flat EVA except for transverse plane rotation during 200ms before and after heel strike.
In terms of variability at the points of interest, in the frontal plane and in all points of interest, wearing textured lateral wedge increased ICC compared to other insoles. The effects of other insoles on ankle movement variability were inconsistent
The results of this study showed that texture has the potential to decrease variability and use of texture with lateral wedge may more improve variability in athletes with FAI
0044
Paula Wijdenes (1) presenting Michael Brouwers (2) Corry van der Sluis (1)Musculoskeletal
Universital Medical Center Groningen, Groningen, Groningen, The Netherlands (1) Rehabilitation center De Hoogstraat, utrecht, Utrecht, The Netherlands (2)
PPP-Arm: the implementation of a national Prosthesis Prescription Protocol
Patients with an acquired or congenital upper limb defect need highly specialized care from multidisciplinary teams. In the Netherlands, various rehabilitation centers had their own method of treatment. Standardized care for these patients was necessary, especially when prescribing prostheses.
To create and implement a national digital protocol, which should be used when prescribing upper limb prostheses.
The Prosthesis Prescription Protocol of the upper limb (PPP-Arm) has been developed in the previous 4 years and is a tool to structure, underpin and evaluate the prescription of upper limb prostheses. The protocol is based on WHO’s criteria of the International Classification of Functioning (ICF).
The protocol consists of the following layers:
Establishing patient’s demands
Establishing device requirements
Preparation of treatment requirements
Selection, try-out and final decision
Delivery of the device
Instructions and training
Evaluation
The protocol has been created through the collaboration of several patients, rehabilitation teams, orthopedic workshops and insurance companies, collaborating in the working group PPP-Arm.
Implementation started in four rehabilitation teams in the Netherlands. After one year another six rehabilitation teams started using the protocol. In each team a knowledge broker was appointed, who was responsible for the implementation within his own center. A national project coordinator maintained contacts with all parties involved, collected questions and problems when using the protocol, organized activities and meetings to develop the protocol further and to stimulate using the protocol.
Advantages of the protocol are: complete and structured, user-friendly, using the same ICF terminology, applied nationally, digital reporting, workplace independent login possibilities for all team members, a prescription report is generated for the insurance company, patients gain more insight in their own treatment process, the protocol contributes to building a national database for research.
Disadvantage of the protocol is: time investment is needed to learn using the protocol.
The nationwide implementation project PPP-Arm was successful, since all participating centers use the protocol. By developing PPP-Arm we have managed to create a national uniform and structured method to advise and evaluate the prescription of upper limb prostheses, which might be interesting for other countries as well.
0045
Soikat Ghosh Moulic (1) presenting Riyaz Hussain (1) Adit Ganguly (1)
Mobility India, Bangalore, Karnataka, India (1)
Effectiveness of monitoring tools for the fabrication process of prosthetics and orthotic devices
Perceptions of quality control measures and protocols are varied across the P&O fraternity. Quality has a direct impact on the effective use of assistive devices. There are various quality control check outs available but having a monitoring tools for the fabrication process is not available.
To understand the effectiveness of the developed monitoring tools in provision of P&O devices.
In December 2011, Mobility India and Christian Medical College, Vellore, with support of ICRC- Special Fund for the Disabled (SFD) and ISPO, organised a consensus seminar on the development of monitoring tools to check the fabrication steps for prosthetics and orthotics appliances. All major schools and rehab professionals from the south east Asia were involved. Internal auditing of monitoring tools used for services provision of P&O devices between Jan 2012 and Jan 2014 was conducted. 364 files audited for four types of devices at our centre in India. Analysis was done for 20 transfemoral prostheses, 53 transtibial prostheses, 77 KAFOs, 214 AFOs using the monitoring tools for each of the fabrication stages.
Transfemoral-10% rectification identified in negative cast stage, assembly and bench alignment stage, 5% in the stages of molding and pre-checkouts
Transtibial- 6% rectification identified in negative cast, 7.5% in fitting and static alignment and 4% rectification in dynamic alignment stages.
KAFO- All stages rectifications identified. More significant need in trial fittings (30%). 14% needed in cast rectification and checkouts and 12% in negative casting.
AFO-. More significant rectification found in trial fittings (20%), negative casting (15%), cast rectification (12.5%), final check outs (10%)
The results reflects the effectiveness of the monitoring system to identify the areas of rectifications in particular stages of fabrication process of P&O devices.
If we interpret the results evaluated items are interrelated and interdependent. The supervisor should have essential sound professional and practical judgment skills. This tool helps in monitoring the stages of fabrications and control over possible errors. It assists in capacity buildings of rehab professionals in specific stages.
Even though the prosthetic devices sample size was small, the clinical relevance was significant. The monitoring tool has to be further tested for validity, reliability and sensitivity in different geographical and clinical set ups.
Utilising the systematic method of monitoring fabrication stages help to determine whether standard of comfort, function and cosmesis have been met and if not provide a basis for further corrective actions ensuring appropriate quality of services.
Lower Limb Prosthetics. Prosthetics and Orthotics Publications, New York, reprinted 2001, (157)
0046
AMIT SARAF (1) presenting
Saraswati institute of medical sciences, ghaziabad, U.P., India (1)
Diabetes Mellitus : a synonym to functional hypoparathyroidism
Poor control of blood glucose levels in patients of Diabetes Mellitus often results in low bone mineral density. The reason for this decrease in bone mass is at present uncertain. In this study, we evaluated correlation of calcium metabolism with blood glucose levels and normal renal function.
To study the effect of blood glucose level on calcium metabolism in the body
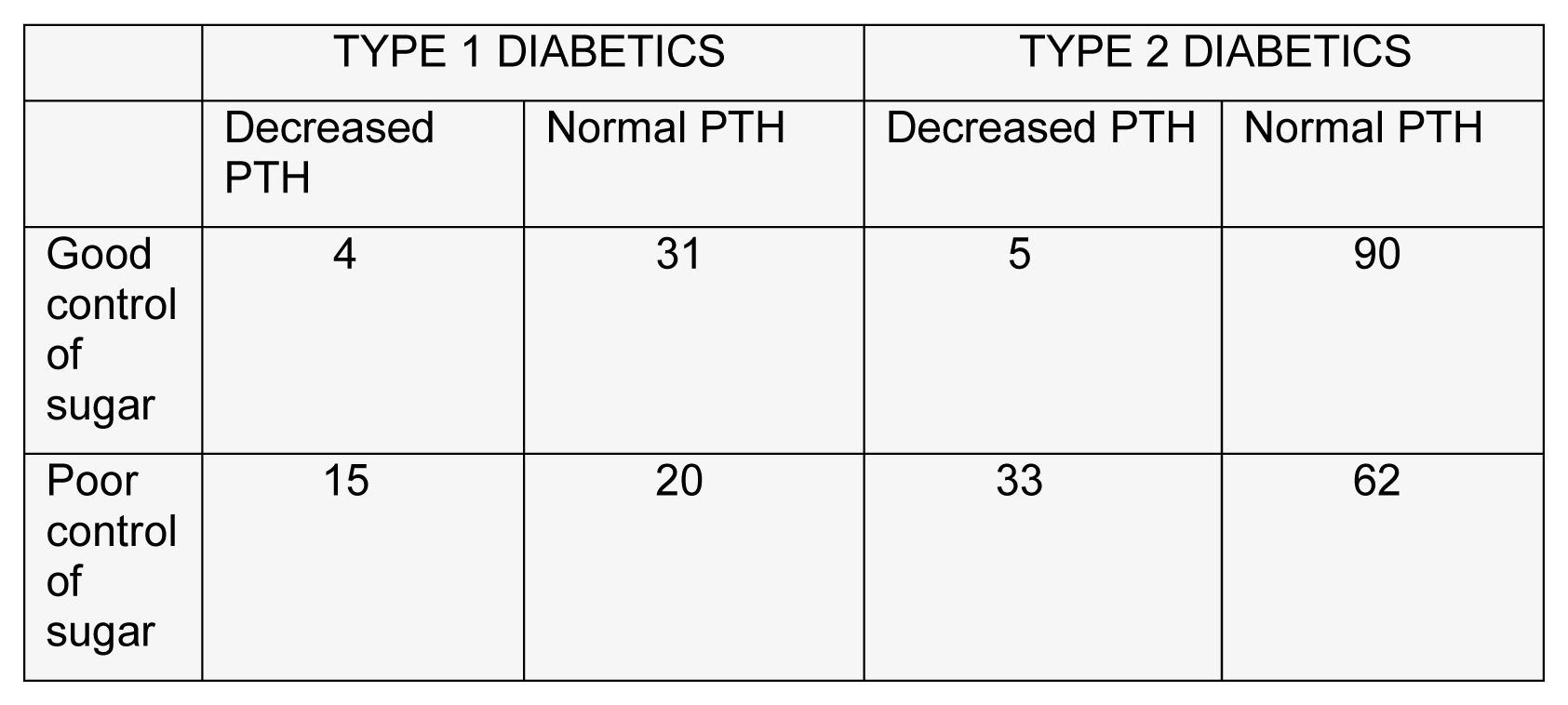
A total of 130 diabetic patients (35 Type 1, 95 Type 2) were enrolled in this study. In all patients plasma calcium (Ca), serum phosphate (PO4), serum parathyroid hormone (PTH), and 24-h urinary calcium (uCa) were determined under both poor and improved control (for at least 7 days) as ascertained by four blood glucose determinations daily.
Improvement of blood glucose level was associated with reduction of uCa both in Type 1 (6.7 +/- 1 vs 5.0 +/- 0.9 mmol/day) and in Type 2 patients (4.3 +/- 0.4 vs 3.1 +/- 0.4 mmol/day). It was also found that considerably more Type 1 patients (15 out of 35) had PTH values below the detection limit (1.5 pmol/l) during poor than during improved control (4 out of 35). Type 2 patients also showed this difference but to a lesser extent. 33 out of 95 type 2 patients had PTH level below detection limit during poor control as compared to only 5 patients during good control. Comparison between the two types of diabetes showed that in Type 1 under poor control, Ca and PTH were lower, while uCa was higher, and after improved control, only uCa continued to be higher.
Nagasaka S, Murakami T, Uchikawa T, Ishikawa SE, Saito T. Effect of glycemic control on calcium and phosphorus handling and parathyroid hormone level in patients with non-insulin- dependent diabetes mellitus. Endocr J. 1995 Jun; 42(3):377-83.
0047
CARLOS GUTIERREZ (1) presenting
INNOVACION ORTOPEDICA, SANTO DOMINGO, Dominican Republic (1)
The Magic Bar II: For Orthotics
This is a low cost system by which we get excellent results in alignment in a bar above the knee braces. In this method we have a similar technique as the one used in the magic bar by which we get duplicate the alignment of dynamics in the lower limb prosthesis. We want to remind you that article of Magic Bar of prosthesis was published in November 2011 in the E-Update ISPO on the technical notes section.
We wish to teach this system in order to make perfect alignment of bars in a lower limb orthotics above the knee without need for sophisticated and expensive equipment.
During the procedure of making the mold, record the patient toe-out in the form of action. Assemble, align the Mold, move, adjust and set on block ankle. Proceed to modify the positive mold. Replace the mold in a bench press. Put a bar plaster (magic bar II) at the end of the toes. This bar should be plumb line of progression to registred in the toe-out. Making another place bar and knee in an parallel to left foot. Another place bar in the back of negative mold to the same height to stand in the knee bar. Proceed to align the joint assemble boxes. Process bars to fold.
This system is an option for the orthoticsthat has given our patients with great results in the DominicanRepublic. We have been using this method for about 600 patients during 2014.

We wish to share this idea for the benefit of all orthesist worlwide. This new system we call « Magic Bar II » for orthotics due to relief or reference incorporated in positive mold located in the distal portion of the foot.
Plaster, laser level, plastic thermo disc, plastic pipe clamp, bench press.
0048
Rashida Begum (1) Zia Ur Rehman (2) presenting Shazia Asif (3)
Pakistan Institute of Prosthetic and Orthotic Sciences, Peshawar, Pakistan (1) Institute of Management Sciences, Peshawar, Pakistan (2) Fauji Foundation Hospital, Rawapindi, Pakistan (3)
Prevalence of post-traumatic stress disorder (PTSD) in physically challenged persons in Khyber Pukhtoonkhuwa, Pakistan
Post-traumatic stress disorder (PTSD) is a highly prevalent and harmful mental health problem with important expenses to the individual and society.
Khyber Pukhtoonkhuwa population is more prone to these traumatic events, because of strategic location in the war zone.
According to the study conducted by
No study had been conducted of persons with disability in Khyber Pukhtoonkhuwa. Therefore, it was the core aim for conducting such study on physically challenged persons.
To assess and determine the level of PTSD symptoms in physically challenged persons. To measure all the categories of PTSD in physically challenged persons. To developed evidence on the base of this study.
The study was conducted in two rehabilitation centres of Khyber Pakhtoonkhuwa, Paraplegic centre and PIPOS Hayatabad, this was cross-sectional descriptive quantitative study. Subjects were randomly sampled in two centres. The sample size was 100 out which 80 were male and 20 were females. PTSD check list civilian version (PCL) was used for measurement of PTSD symptoms and Impact of Event Scale – Revised was used for categorized these symptoms in three categories. The sample comprises both in-patients and out-patients. Symptom profiles of male and female sufferers of PTSD were compared using the chi-squared statistical test.
Data was processed and analysed through SPSS version 16 software.
Main symptoms of PTSD were present in more than 30% of sufferers. Symptom frequencies for anxiety, insomnia, physical reaction (e.g., heart pounding, trouble breathing, sweating) flashback imagery and intrusive thoughts, irritability, poor concentration and avoidance behaviour were found above 70%. Some symptoms (such as inability to recall parts of the trauma and restricted affect) occurred in no more than 35% of sufferers.

Chi-square =60.84 df = 1 P-value = 0.00,(0.05)
There is significant difference between PTSD and Non-PTSD for physically challenged people, at 5% level of significant.
The study result indicated that physically challenged persons are more likely to suffer from PTSD than general population. Out of 100 patients, 89 were found symptomatic and 11 of them were non-symptomatic. Men and women both significantly suffered with PTSD (p < 0.05) Symptoms tend to follow an acute stress reaction, occurred earlier and persisted for many months.
It is important that adequate strategies should be made for physical and psychological management of the patients.
0049
Alex Dickinson (1) presenting Joshua Steer (1) Christopher Woods (1) Peter Worsley (1)
University of Southampton, Southampton, UK (1)
Imaging and analysis of residual limb shape in below knee amputees
Successful prosthetic adoption and rehabilitation following lower-limb amputation is dependent on a safe and comfortable socket-residual limb interface. This interface is designed to maximise comfort whilst providing stable transfer of biomechanical loads. Current practice predominantly utilises subjective, iterative cast rectification to establish socket shape, requiring multiple prosthetist visits. Residuum volume can be measured with high repeatability [1-3] but shape is another key factor [4].
This study proposes a methodology by which residual limb shape data is collected and analysed for high-resolution, objective shape measurement. The aim was to assess its accuracy and reliability.
A computer programme was written to extract automatic, objective measurement of limb volume, cross-section area, and width profiles in the sagittal and coronal planes, from shape scan data:
Data: 1) A 3D printed CAD ‘phantom’ residuum was scanned with three digitisers on ten occasions. 2) Twenty male residuum casts were scanned by two observers, and ten were repeat-scanned on a second occasion. The scan files were aligned spatially, and geometric measurements were extracted automatically.
Measures: 1) mean, S.D. and maximum scan height error between repeat phantom scans and the CAD phantom print geometry; scan vs. CAD volume. 2) Intraclass Correlation (ICC) coefficients and Bland-Altman plots of paired scan volumes; pairwise RMS and absolute error ranges of scan area, and sagittal and coronal width profiles. ‘Max’ denotes 95% C.I.

1) scanner height error ranged from mean (±S.D.) 0.105mm ±0.063mm to 0.884mm ±0.297mm for the most and least expensive scanners, respectively. This gave max 4.66ml to 41.57ml volume magnitude errors. 2) Volume ICC coefficients ranged from 0.993 to 0.999 (intra-rater) and 0.990 to 0.998 (inter-rater). Bland-Altman plots showed max variance ranges of ±77.14ml (inter-rater) and ±43.4ml (intra-rater), and no variance bias with stump volume. Pairwise RMS errors in residuum width profiles ranged from 0.1mm to 1.7mm, and in area profiles from 9.7 mm2 to 116.9mm2.
Two of three scanners produced sub-millimetre accuracy when digitising the phantom. All three scanners produced more repeatable volume measurements than contact methods [1,2]. The scanning and measurement process was also shown to be highly repeatable for residuum casts, within and between observers, with ICCs exceeding a 0.9 threshold for clinical relevance.
The technique provides clinical researchers and prosthetists the capability to establish their own quantitative, objective, multi-patient datasets, enabling long-term patient follow up and, alongside inter-patient functional evaluation, decision support.
[1] Bolt et al 2010, AmJPMR
[2] de Boer-Wilzing et al 2011, APMR
[3] Sanders & Fatone 2011, JRRD
[4] Persson & Liedberg 1983, POI
0051
Edmond Lou (1,2) presenting Miranda Grotski (1) Fraaz Kamal (1) Duc Nguyen (1) Douglas Hill (1,2)
University of Alberta, Edmonton, Alberta, Canada (1) Alberta Health Services, Edmonton, Alberta, Canada (2)
A Bluetooth Orthotic Compliance Monitor for Patients with Adolescent Idiopathic Scoliosis
Orthotic treatment is the most effective non-surgical method to treat children who have adolescent idiopathic scoliosis. Its goal is to stop further curve progression. Four factors affect orthotic treatment outcome: a) growth or curve based risk, b) the in-brace correction, c) the amount of time that the brace is worn (quantity of brace wear or dosage), and d) the wear tightness relative to the prescribed level.
This study aims to develop and report a BluetoothTM compliance monitor that can be easily used by orthotists to understand how patients use their spinal orthoses during their treatment period.
A BluetoothTM orthotic compliance monitor consisting of temperature and low profile force sensors was developed to log the dosage and tightness of brace wear during the treatment period. Custom software was developed for the orthotic monitor to communicate with any iOS, Android or Windows operating portable devices which have built-in Bluetooth v4.0TM function. Analysis and report software were incorporated into the custom software to simplify the analysis process. The logged information could be downloaded wirelessly within 2 minutes. Health professionals at the scoliosis clinic could use the report to objectively understand how patients use their orthoses.
The dimensions and the weight of the compliance monitor (Figure 1a) were 2.5 cm x 5 cm x 1.4 cm, and 8 g, respectively. The compliance monitor could be embedded underneath the major pressure pad (figure 1b) to sense the interface pressure between the orthosis and the body. After installation and setup to acquire data at 1 sample per minute, the monitor logs the temperature and force information automatically. The battery power and memory capacities could last for 9 months without requiring any attention. The accuracy of the temperature and the force sensors were ±1.5oC and ±0.15N, respectively. The reliability of a test on 3 volunteers over 56 hours of the wear time was over 99% when combining temperature and force information.

Using a temperature sensor alone may overestimate complaince in a hot climate and misrepresent dosage, but using a force sensor alone may underestimate the complaince if the user wears their orthosis loosely. This monitor combined force and temperature sensors to measure both time and dosage of brace wear. at99% accuracy.
0052
Edmond Lou (1,2) presenting Andreas Donauer (2) Melissa Tilburn (2) Douglas Hill (1,2)
University fo Alberta, Edmonton, Alberta, Canada (1) Alberta Health Services, Edmonton, Alberta, Canada (2)
Using Ultrasound Imaging and Pressure Measurement System to Optimize TLSO Design for the Treatment of Scoliosis

The standing radiograph (left), standing ultrasound (middle) and simulated in-orthosis ultrasound (right).
In the control group, 5 of 10 (50%) subjects needed a total of 8 brace adjustments requiring a total of 18 in-brace radiographs (average 1.8 radiographs per subject). Some subjects required multiple adjustments. The average in-orthosis Cobb angle correction measured from radiographs at the acceptable orthosis configuration was 53±32%. In the intervention group, 1 subject needed minor adjustment while the remaining 9 had acceptable Cobb angle correction (average 1.1 radiographs per subjects). The average axilla, thoracic and lumbar pressure at the best stimulated in-orthosis configuration were 42±22, 79±27 and 71±30 mmHg, respectively. During the fitting clinic, the average major pad interface pressure at thoracic region prescribed by the orthotists was 82±30 mmHg resulting with the average in-orthosis Cobb angle correction of 51±21% at the follow up clinic.
The use of the ultrasound system provided a radiation-free real-time imaging method that can assist to determine the optimum pressure level and location to obtain the best stimulated in-orthosis correction during brace casting. Using ultrasound imaging to optimize orthosis casting significantly reduces the number of orthosis adjustments and radiographs which demonstrates an improvement over the standard practice.
0055
AMIT SARAF (1) presenting
Saraswati institute of medical sciences, ghaziabad U.P., India (1)
Influence of type of incision on rehabilitation in below knee amputation
Below knee amputation is required in patients with advanced critical limb ischaemia or diabetic foot sepsis in whom no other treatment option is available. Till date there is no consensus as to which surgical closure achieves the maximum rehabilitation potential. In this study we assessed the effects of different types of incision on the outcome of below knee amputation in people with lower limb ischaemia or diabetic foot sepsis, or both. The main focus was to assess the relative merits of skew flap amputation versus Burgess flap (long posterior flap) closure.
To compare the rehabilitative outcome of skew flap versus Burgess flap closure in below knee amputation
This was a ten years retrospective and 2 years prospective study. A total of 144 patients were include of which 76 (53%) patients had Burgess closure while 59 (41%) had skew flap closure. 9 patients underwent atypical closure or skin grafting. These groups were compared on the basis of stump healing time, rate of infection, time for prosthetic fitting and compliance with prosthesis with either of the flaps made.
Below knee amputation using skew flaps conferred no advantage over the well established Burgess flap closure. 76% stumps after Burgess closure and 71.4% after Skew flap closure healed well in time which was insignificant (p>0.05). Primary stump healing was 58% for skew flaps and 55% for burgess flap . The result was not significant. Of the total 144 patients, 72.2% had prosthetic fitting. 60% of them underwent prosthetic fitting within 3 months in both the groups after closure. 66.8% of Burgess flap closure patients and 71% of Skew flap closure were happy with their prosthesis which was not significant.

Stump healing time, rate of infection, time of prosthetic fitting and prosthetic compliance was similar in both the groups. We thus conclude that there is no benefit of one type of incision over another. The choice of amputation technique can, therefore, be a matter of surgeon preference taking into account factors such as previous experience of a particular technique, the extent of non-viable tissue, and the location of pre-existing surgical scars.
Tisi PV, Callam MJ. Type of incision for below knee amputation. Cochrane Database Syst Rev. 2004;(1):CD003749.
0056
AMIT SARAF (1) presenting
Saraswati institute of medical sciences, ghaziabad U.P., India (1)
Mobilization status of diabetics versus non-diabetics after below knee amputation: A comparison
Mobility following below knee amputation has a direct impact on the quality of life. Early and independent mobilization develops confidence in the below knee amputee. This helps the patient to become psychologically, socially and economically independent. In this study we compared mobilization status of diabetics versus non-diabetics amputees. We also prepared a note of type of supports used and duration of prosthetic usage by both the groups postoperatively.
To compare rehabilitative outcome after below knee amputation in diabetics versus non diabetics on the basis of prosthetics and orthotics used by them
This was a 2 years prospective and 10 years retrospective study. A total of 144 below knee amputees using various supports for mobilization were included in this study of which 63 were diabetics and 81 non diabetics. They were followed for a minimum period of 1 year. On follow up they were observed for the type of support used for mobilization.
Of 144 amputees, 92 patients initially used crutches for mobilization. 40 patients used walker, 7 used wheelchair and 5 remained bed ridden before they died. It was observed that of 92 patients who were using crutches, 22 were in diabetic group and 70 in non diabetic group. 31 patients of diabetes and 9 patients of non diabetic group used walker. 5 patients in diabetic group and 2 patients in non diabetic group could mobilize only on a wheelchair. All 5 bedridden patients were in diabetic group. 104 patients started using prosthesis for mobilization once their stumps had healed adequately of which 30 were in diabetic group and 74 in non diabetic. The result was statistically significant. Of 104 prosthesis users, 43 were using it for less than 6 hours per day, 55 were using 6-12 hours per day and 6 patients were using it for > 12 hours per day.

Non diabetics preferred crutches and prosthesis for mobilization in comparison to diabetics. More diabetics were bedridden or on wheel chair after amputation. Non diabetics were using prosthesis for longer time in comparison to diabetics. Major causes for this difference was preoperative lower ambulatory grading in diabetics, weaker muscle mass, old age, co-morbid conditions, increased incidence of infection and prolonged stump healing time.
Basu NN.
0058
Sandeep Uppal (1) presenting
New Zealand Artificial Limb Services, Wellington, New Zealand (1)
Most recent effective post-operative amputee stump management as preparation for prosthesis fitting
The most common cause of amputation worldwide is poor blood circulation because of damage to the blood vessels causing peripheral arterial disease. As a result of this disease, the affected tissue starts to die and infection may ensue. Other causes for amputation include accidental injury, serious burn, tumours in muscle or bone, neuroma (thickening of nerve tissue) and diabetes. In healthcare and nursing practice, hospital staff especially nurses are responsible for managing the stump after amputation. To prevent infection and prepare the stump for proper prosthesis fitting, evidence based practice is important.
This study describes the most recent effective post-operative amputee stump management as preparation for prosthesis fitting and provides recommendations for healthcare and nursing practice obtained from evidence based studies. The process used to find research articles is described and the similarities and differences of each study analysed. The guidelines and their relevance to New Zealand practice are examined.
The method used for this study is Evidence based practice(EBP). Literature for most effective post-operative stump management as a preparation for prosthetic fitting was gained by searching electronic, academic and professional journal databases. The databases accessed were CINAHL, e-links such as Pro Quest, Cochrane Library, Journals and internet sources with full text as well. The databases were first searched using the key terms ‘ amputation, stump management’, ‘prosthesis fitting’, ‘post-operative care’,’ infection’, ‘ dressing’, ‘pain management’, ‘amputation and nursing care’. The results from each term were looked at individually and then as a combination of terms. To gain a wider understanding of the topic, the key terms ‘ Post-operative stump management’, ‘ preparation of stump for prosthesis fitting’, ‘role of nurses for amputee stump care’ were used and as the study was related specifically to nursing practice. The search parameters were limited to dates between 2005- 2013 to ensure the collection of recent work.
Results based on five different studies for post-operative management of stump. All five studies conclude that rigid/ semi rigid dressings are more effective than soft dressings giving faster healing and less oedema (Sanders and Fatone, 2011; Vermeulen et al., 2012; Payne et al., 2010; Nawijn et al., 2005; Deutsch et al., 2005). That recommendation is evidence of level I. However there are differences recommended in what is used next to skin inside the plaster or RRD. Vermeulen et al. (2012) recommend a silicon insert or gel sock inside the rigid dressing and use of a shrinker after healing, but Deutsch et al. (2005) also suggests that rigid dressings may help prevent damage from falls lower chance of further surgery. Only one study looked at use of antibiotics (Payne et al., 2010). This study also recommended the use of rigid dressings.
Use of proper dressings such as semi-rigid/ rigid are very important to prevent maintain the shape of stump and control residual limb volume (prevent oedema). According to the studies, there are some clear guidelines for nurses to provide the best care to the amputee patient. NZALS also has clear guidelines for New Zealand hospitals for amputee patients. An area which requires further study is the use of post-operative antibiotics. Clear communication between the surgeon and the nursing team is emphasized as being very important to ensure consistent patient care. Literature also provide information about complications such as oedema and how can be avoided and provide no. of recommendations.
Basco, M. (2008).Clinical procedures in Prosthetics II [Power point Presentation]. Retrieved from https://docs.google.com/viewer?a=v&q=cache:qUVWbPKPDrsJ:xa.yimg.com/kq/groups/20848158/1340482900/name/Clinical%2520Procedures%2520in%2520Prosthetics%2520II.ppt+stump+management+as+preparation+for+prosthesis+fitting&hl=en&gl=nz&pid=bl&srcid=ADGEESjpNJfNG4_CFtRcAocd6hBf2sce2XWC84ahqtEICzRWfjqqQmvlFzi61d9SbjiLgaLxe9Lt4EEq1RuizOICLYrZrV3gwtcpuXZ_2EPgH2cd3xNiWRDhwaQXJQzTAgVhYNvnqFLh&sig=AHIEtbTikMuQLry8lqXaY1ufmcGqVMYzvA
Chatterjee, R. (2012). Amputation overview. Retrieved from http://www.webmd.com/a-to-z-guides/definition-amputation
Department of Rehabilitation Services. (2011). Standard of care: Lower extremity amputation. Retrieved from http://www.brighamandwomens.org/patients_visitors/pcs/rehabilitationservices/physical%20therapy%20standards%20of%20care%20and%20protocols/general%20-%20le%20amputation.pdf
Deutsch, A., English, R., Vermeer, T., Murray, P., & Condous, M. (2005). Removable rigid dressings versus soft dressings: A randomized, controlled study with dysvascular, trans-tibial amputees. Prosthetics and Orthotics International, 29(2): 193 – 200. doi: 10.1080/03093640500224295
Fitzsimons, T., Clark, A., Symonds, A., Navarrete, M., Saad, N., Lees, P.,… Forde, M. (2006) Physiotherapy following lower limb amputation protocols and reference material 2006. Retrieved from http://www.geocities.ws/nswpar/AmputationManual1.pdf
Harker, J.(2006). Wound healing complications associated with lower limb amputation. Retrieved from http://www.worldwidewounds.com/2006/september/Harker/Wound-Healing-Complications-Limb-Amputation.html
Health Leaders Media, (2012) Evidence based practice. Retrieved from http://www.healthleadersmedia.com/search_results.cfm?q=evidence+based+practice
Hockley, D. (2005). Design & implementation of interdisciplinary care guidelines for hospital management of amputees in Christchurch. Retrieved from https://docs.google.com/gview?url=http://nzals.govt.nz//assets/Resources/Amputee-care/Amputee-care-guidelines/DebbieHockleyCareGuidelinesReport.pdf&pli=1
Kalapatapu, V. (2012). Lower extremity amputation. Retrieved from http://www.uptodate.com/contents/lower-extremity-amputation
Lee, M., & Moroz, A. (2009). Leg Amputation Rehabilitation. Retrieved From http://www.merckmanuals.com/professional/special_subjects/rehabilitation/leg_amputation_rehabilitation.html
Leimkuehler, P. (2012). Postoperative management of the lower extremity amputation. Retrieved from http://www.oandp.org/olc/lessons/html/SSC_02/09ampspec.asp?frmCourseSectionId=E4648351-EF8C-4EB4-BB35-8BC07B891B9C
Nawijn, S., Linde, H., Emmelot, C., & Hofstad, C. (2005). Stump management after trans-tibial amputation: A systematic review. Prosthetics and Orthotics International, 29 (13). doi: 10.1080/17461550500066832
New Zealand Artificial Limb Board. (2012). Treatment and care. Retrieved from http://nzals.govt.nz/amputee-services/treatment-and-care/
New Zealand Artificial Limb Service. ( 2012). A manual for the new amputee. Retrieved from http://nzals.govt.nz/assets/Resources/Amputee-care/Amputee-care-guidelines/KiaKaha1.pdf
Overholt, E., Melnyk, B., Stillwell, S., & Willianson, K. (2010). Critical appraisal of the evidence: Part I, An introduction to gathering, evaluating, and recording the evidence. American Journal of Nursing 110 (7): 47-52 doi: 10.1097/01.NAJ.0000390503.92404.e6.
Payne, K., Sheikh, N., Andrabi, S., El-Tahir, A. (2010) Lower limb amputation wound care: Is there a consensus on wound management? Are post-operative instructions clear?. The Internet Journal of Surgery 2010, 25 (1). doi: 10.5580/27c0
Polit, D., & Beck, C. (2012). Nursing research: Generating and assessing evidence for nursing practice (9th ed.). Philadelphia, MA: Lippincott Williams & Wilkins.
Sanders, J. E., & Fatone, S. (2011). Residual limb volume change: Systematic review of measurement and management. Journal of Rehabilitation Research & Development, 48(8), 949-986. doi:10.1682/JRRD.2010.09.0189.
Schaffer, E. (2010). Skin care of the stump. Retrieved from http://www.merckmanuals.com/professional/special_subjects/limb_prosthetics/skin_care_of_the_stump.html
Vermeulen, H., Ubbink, T, Goossens, A., de Vos, R., Legemate, A., Westerbos, J. (2012).Dressings and topical agents for surgical wounds healing by secondary intention (Review). The Cochrane Library, 2012 (4) doi: 10.1002/14651858.CD003554.pub2
0059
Atefe Aboutorabi (1) presenting Mokhtar Arazpour (1) Maryam Mekial (1) Stephen William Hutchins (2) Sarah Curran (3)
university of social welfare & rehabilitation sciences, Tehran, Iran (1) Faculty of Health & Social Care, IHSCR, University of Salford, Salford, UK (2) Cardiff School of Health Sciences, Cardiff Metropolitan University, South Glamorgan, UK (3)
A review of efficacy of foot orthoses on alteration to center of pressure displacement in flatfoot subjects
Flat foot in children is a common deformity in which the medial longitudinal arch is reduced or eliminated. Foot orthoses are prescribed to prevent further collapse of the medial longitudinal arch or pronation.
The purpose of this review was to evaluate and compare the effect of foot orthoses on center of pressure (CoP) displacement in healthy patients and those with flat foot.
The search strategy was based on the Population Intervention Comparison Outcome (PICO) method. A search was performed in PubMed, Science Direct, Google scholar and ISI web of knowledge databases by using selected keywords. Seventeen articles were selected for final evaluation. The procedure was followed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) method.
The normal CoP excursion has been reported as being 4.01±1/06mm in adults, but in subjects with flexible flat foot this mean was demonstrated to be 4.3mm. results of the literature review demonstrated that there is lack of evidence to show that FOs improve CoP displacement in subjects with flat foot.
FOs are effective in controlling CoP path and maybe move to an abnormal path of CoP toward a more normal trajectory in flat foot subjects. there is no consistent evidence to prove the efficacy of FOs on altering CoP displacement in healthy subjects but in those with flat foot, FOs decreased CoP excursion. The main variables which need to be measured in any future studies should be CoP velocity with FOs. In this review, it was noted that only one study evaluated this parameters.
1. Paton JS, Spooner SK. Effect of extrinsic rearfoot post design on the lateral-to-medial position and velocity of the center of pressure. J Am Podiatr Med Assoc 2006;96:383–92.
2. Xu H, Akai M, Kakurai S, et al. Effect of shoe modifications on center of pressure and in-shoe plantar pressures1. Am J Phys Med Rehab 1999;78:516–24.
3. Van Gheluwe B, Dananberg HJ. Changes in plantar foot pressure with in-shoe varus or valgus wedging. J Am Podiatr Med Assoc 2004;94:1–11.
4. Janin M, Dupui P. The effects of unilateral medial arch support stimulation on plantar pressure and center of pressure adjustment in young gymnasts. Neurosci Lett 2009;461:245–8.
0060
Judy Scopes (1) presenting Marietta van der Linden (1) Nigel Gleeson (1)
Queen Margaret University, Edinburgh, UK (1)
Responsiveness of functional outcome measures used with lower limb amputees during early prosthetic rehabilitation
Knowledge of the responsiveness of an Outcome Measure (OM) is key to the correct interpretation of the results especially following interventions such as rehabilitation programmes or change in prosthetic components.
A survey of Allied Health Professionals (AHPs) working with lower limb amputees in the UK revealed that the most common OMs measuring physical function were: 2 Minute Timed Walk Test (2MWT), Timed up and Go (TUG), Locomotor Capability Index-5 (LCI-5) and the SIGAM Mobility Grades.
To establish the responsiveness of four functional OMs commonly used with lower limb amputees when assessing change during early prosthetic rehabilitation.
Fourteen adult unilateral amputees at trans-tibial or trans-femoral level were recruited following delivery of their primary prosthesis. Score changes in the four commonly-used functional OMs were analysed separately using ANOVA with Repeated Measures and post-hoc tests or their appropriate non-parametric equivalents. Cohen’s d values for the three time intervals were also computed.
Time interval 1: baseline visit (1 week following delivery of primary prosthesis) to 2 weeks later. Time interval 2: just prior to discharge from hospital (at an average of 3 weeks post-limb delivery) to the post-discharge clinic appointment (usually after 6 weeks).
Time interval 3: baseline visit to the post-discharge clinic appointment.
Except for the TUG, positive values indicate an improvement in function. Statistically significant differences (p<0.05) were found amongst absolute scores for all three time intervals for the 2MWT and TUG and for the time intervals 1 and 3 for the LCI-5 and SIGAM. Cohen’s d effect sizes were medium (>0.5) or large (>0.7) effect sizes for all OMs for all time intervals, except the 2MWT and SIGAM for time interval 2 which were smaller.

Although no comparator or gold standard OM was available to confirm improvements during the study period, it was anticipated from clinical experience that the performance of the amputees’ would improve during early prosthetic rehabilitation. These initial results confirm this expectation showing moderate to high effect sizes and significant differences between the baseline assessment and the post-discharge clinic and showing that all OMs are responsive to change over this time interval.the self-reported measures.
0061
Jon Batzdorff (2,3) presenting
San Francisco Prosthetic Orhotic Service, Inc., San Francisco, USA (1) ProsthetiKa, Santa Rosa, Califormia, USA (2) US ISPO, Ohio, USA (3)
Ethical Considerations in Providing Prosthetic/Orthotic Assistance in Developing Countries
There is an ever-increasing number of organizations offering prosthetic and orthotic assistance in developing countries. US ISPO was asked by its neighbors in Latin America to work together to develop a Code of Conduct for such organizations in order raise the awareness of policies and activities that would be considered unethical and unwelcome.
A Code of Conduct was drafted and published on line by US ISPO. The Code was presented to organizations offering P and O assistance in developing countries and they were requested to sign it if they agree to the terms. Signing and adhering to the Code is voluntary and is intended to raise the awareness of the issues as well as providing public accountability on line. The draft was intended as a work in progress which can be refined as needs require.
A committee was formed by US ISPO. Several drafts were created and submitted for approval by the Board of Directors of US ISPO. Once the draft was approved, it was published on the US ISPO website and organizations were invited to sign up. 13 organization signed on to the Code. After five years a follow up discussion was planned and conducted at a meeting in Ecuador. The Code was discussed along with goals and critical and constructive suggestions. The Code will be modified as planned and changes will be made with consideration of the critical suggestions.
13 Organizations signed up to the Code of Conduct. At the five year review of the Code of Conduct held in Ecuador,suggestons were made to expand the Code to include the coduct of P and O schools, and of private for profit orgainzationsas well. The existing provisions as well as possible future provisions of the Code were discussed in addition to enforcement options. It was agreed to continue to discuss and expand the Code to keep it responsive to the current issues.
The Code of Conduct addresses such ethical issues as creating dependency, use of appropriate materials, componenets, and technology, competition with local practitioners and providing free services vs use of a sliding fee schedule. A total of 9 paragraphs are included in the US ISPO Code of Conduct and more areas have been suggested and presented.
0062
Monireh Ahmadi Bani (1) presenting Mokhtar Arazpour (1) Farzam Farahmand (2,3) Shahryar Sefati (2) Mina Bani Asad (2,3) Stephen W Hutchins (4) Reza Vahab Kashani (1) Mohammad-Ebrahim Mousavi (1)
Department of Orthotics and Prosthetics, University of Social Welfare and Rehabilitation Science, Tehran, Iran (1) Mechanical Engineering Department, Sharif University of Technology, Tehran, Iran (2) Research Center of Biomedical Technology and Robotics, Tehran University of Medical Sciences, Tehran, Iran (3) University of Salford, IHSCR, Faculty of Health and Social Care, University of Salford, Salford, UK (4)
Analysis of new medial reciprocal linkage using lower limb paralysis simulator
The simplest approach for orthotic intervention in patients with spinal cord injury (SCI) is the use of mechanical orthoses; the most effective of which are reciprocating gait orthoses (RGOs) and medial linkage orthoses (MLOs). RGOs improve gait parameters and decrease energy expenditure due to the reciprocating motion they provide. MLOs improve cosmesis and functional independency. Although these two types of mechanical orthoses are commonly used by SCI patients, no mechanical MLO with a reciprocating mechanism has been developed yet for such patients.
This new medial hip joint mechanism was designed and developed incorporating reciprocating motion and was analysed for efficacy on four healthy subjects using a lower limb paralysis simulator (LLPS).
A joint with a remote centre of motion was designed to be used as the medial hip joint of the MLO. A prototype of the joint was fabricated and then implemented into a knee ankle foot orthosis, and equipped with a saddle to make the reciprocating motion possible. The efficacy of the orthosis was evaluated on four subjects who were trained to walk with the MLO attached to a LLPS. Spatio-temporal and kinematic parameters of walking and saddle movement were analyzed.
The results showed that with posterior pelvic tilt on the saddle plate, the leg would propel forward. The mean of speed of walking was 0.09±0.007 m/s during ambulation with LLPS. The mean of stride length and time were 0.42±0.01 meters and 4.89±0.45 sec, respectively. The mean of cadence was 29.54±4.32 steps/min when healthy subjects walked with LLPS in this study.
This figure shows the means of the hip joint angle and the trunk angle in walking with LLPS. In comparison with normal gait, both angles (hip and trunk) showed reduction in flexion and extension rates.

The new medial hip joint developed in this study, has the ability to propel the patient’s leg forward. This new orthosis is potentially suitable for SCI patients and improves gait parameters and cosmesis.
1- Motlock W. principles of orthotic management for child and adult paraplegia and clinical experience with the isocentric RGO. proceeding of 7th world congress of the international society in prosthetic and orthotics1992:28.
2- Ahmadi Bani M, Arazpour M, Farahmand F, Mousavi ME, Hutchins SW. The efficiency of mechanical orthoses in affecting parameters associated with daily living in spinal cord injury patients: a literature review. Disabil Rehabil Assist Technol 2014;2014:2. PMID:24383891
3- Harvey LA, Newton-John T, Davis GM, Smith MB, Engel S. A comparison of the attitude of paraplegic individuals to the walkabout orthosis and the isocentric reciprocal gait orthosis. Spinal cord1997;35(9):580-4.
Johnson W, Fatone S, Gard S, editors. Modeling the walking patterns of Reciprocating Gait Orthosis users with a novel Lower Limb Paralysis Simulator. Engineering in Medicine and Biology Society, EMBC, 2011 Annual International Conference of the IEEE; 2011: IEEE
0063
Mokhtar Arazpour (1) presenting Monireh Ahmadi Bani (1) Stephen W Hutchins (2) Sarah Curran (3) Mohammad-Ali Javanshir (4) Mohammad-Ebrahim Mousavi (1)
Orthotics and Prosthetics Department, University of Social Welfare and Rehabilitation Science, Tehran, Iran (1) HSCR, Faculty of Health & Social Care, University of Salford, Salford, UK (2) Cardiff School of Health Sciences, Llandaff Campus, Cardiff Metropolitan University, Wales CF5 2YB, UK (3) Department of Orthotics and Prosthetics, Iran University of Medical Science, Tehran, Iran (4)
Influence of orthotic gait training with powered hip orthosis on walking in paraplegic patients
Gait training with powered gait orthoses (PGOs) is a new and emerging intervention which can help in the rehabilitation of SCI subjects by providing walking and standing activities. PGOs can facilitate ambulation in both the clinical situation and in the home for paraplegic patients. But gait training has been shown to improve the walking performance of spinal cord injured (SCI) patients. The use of powered hip orthoses (PHO) during gait training is one approach which could potentially improve rehabilitative outcomes for such subjects
The aim of this study was therefore to evaluate the influence of a PHO on the kinematics and temporal–spatial parameters of walking by SCI patients.
Four SCI patients participated in this study. Gait evaluation was performed at baseline and at 10 weeks following intervention with the use of a PHO and gait re-training. Walking speed, step length, vertical and horizontal compensatory motions and hip joint kinematics were analysed prior to and following the training regime.
Significant increases in walking speed and step length were demonstrated by the SCI patients when walking with the PHO following orthotic gait training. Sagittal plane hip range of motion also increased, but not significantly. However, vertical and horizontal compensatory motions decreased significantly.
Positive effects on the kinematics and temporal–spatial parameters of gait by SCI subjects were demonstrated following a period of gait training with a PHO. Further studies are therefore warranted to confirm their long term effects on the rehabilitation of SCI subjects.
0064
Mark McAloon (1,2) presenting Stephen Hutchins (1,2) Martin Twiste (1,2) Richard Jones (1,3) Simone Forchtner (1)
The University of Salford, Greater Manchester, UK (1) UNIPOD - United National Institute for Prosthetics & Orthotics Development, Salford, UK (2) Centre for Health Sciences Research, University of Salford, Salford, UK (3)
Validation of the activPAL activity monitor in children with hemiplegic gait patterns resultant from cerebral palsy
(Podium or Poster Presentation).
The absolute agreement between the raters (0.9111) examined with intraclass correlation was very good (confidence interval 95% 0.9814 to 0.9958). The monitor was found to be reliable.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet i. 1986;307-10.
Mark T McAloon, Stephen Hutchins, Martin Twiste, Richard Jones, Simone Forchtner Prosthetics & Orthotics International 2014 Oct;38(5):393-9.
Winters TF, Gage JR, Hicks R. Gait patterns in spastic hemiplegia in children and young adults. Journal of Bone and Joint Surgery 1987; 69A:437-41.
0065
Sarah Deans (1) Kirsty Watters (2) presenting
University of Strathclyde, Glasgow, UK (1) RSL Steeper, Manchester, UK (2)
Physical activity perceptions of prosthesis users: An interpretative phenomenological analysis
Physical activity is good for you and any activity is better than none. A quarter of people with life-long limiting conditions, including lower limb absence, meet physical activity recommendations. We wished to understand why participation is low through an exploration of prosthesis users’ experiences.
To uncover the motivations and barriers people with lower limb absence encounter when contemplating or participating in physical activity. Could positive health interventions be developed to support an increase in physical activity levels? We aim to inform those caring for people with limb absence about patients’ lived experiences of contemplating or participating in physical activity for health.
The study design was a qualitative, small scale social survey one featuring a focus group conducted in early 2014. Eight men living with unilateral trans-tibial amputation participated in a focus group with semi-structured questions posed to them. Data were analysed using interpretative phenomenological analysis.
Three master themes presented; personal; social; and technical. Key motivations were health and well-being maintenance; feelings of normality; and mood improvement. Key barriers included isolation; psychological such as fear; and environmental factors such as weather and uneven terrain.
More barriers to physical activity participation exist than motivations suggesting a role for physical activity promotion. Delivery of physical activity promotion by prosthetists over the lifelong course of prosthetic rehabilitation could facilitate and reinforce long-term positive behaviour change and health benefits. Positive lifestyle interventions could be designed and implemented as part of routine prosthetic rehabilitation, thereby contributing to general health and well-being improvements in those with limb absence.
Bragaru M, van Wilgen CP, Geertzen JHB, Ruijs SGJB, Dijkstra PU, Dekker R. Barriers and facilitators of participation in sports: a qualitative study on Dutch individuals with lower limb amputation. PLOS One 2013;8(3):1.
Deans S, Burns D, McGarry A, Murray K, Mutrie N. Motivations and barriers to prosthesis users participation in physical activity, exercise and sport: a review of the literature. Prosthet Orthot Int 2012;15;36(3):260-9.
Kirk A, MacMillan F, Webster N. Application of the transtheoretical model to physical activity in older adults with Type 2 diabetes and/or cardiovascular disease. Psych Sports Exer 2010;11(4):320-324.
0066
Bryce Dyer (1) Sarah Deans (2) presenting
Bournemouth University, England, UK (1) University of Strathclyde, Scotland, UK (2)
Swimming with upper and lower limb absence: a systematic review
Swimming with limb absence is currently undertaken as a source of leisure or rehabilitation activity and is also part of the current Paralympic Games competition programme. Whilst it is often proposed that research into sport with limb absence can be extremely limited, this study intended to identify the volume, type and historical strategy in this area.
To understand the evolution in the use of prostheses for swimming and developments in their design and function. This review establishes the historical strategy of swimming with limb absence and identifies existing research themes. It summarises the current knowledge base helping to signpost and progress future work for the benefit of those living with limb absence.
This is a documented systematic review of swimming with lower or upper limb absence. A four step search protocol was adopted. Stage one involved a search of bibliographic databases. These comprised the Sportdiscus, CINAHL, Scopus, PsycINFO and Medline bibliographic databases. Stage two involved the removal of any duplicate results. Stage three involved checking the successful papers references for any not already identified in stage one. Finally, stage four used Google Scholar to source any results not identified previously.
The review identified 22 papers which met pre-defined inclusion criteria. The identified peer reviewed publications dating from 1983 until 2014.
Clear themes emerged from the historical research interest in this area. There was a paucity of peer-reviewed literature with respect to swimming with limb absence and the design of adaptive or assistive technology to help facilitate it. The initial trend of publication indicates an interest in the design of prosthetic technology, with the emphasis then shifting to an interest in swimming biomechanics from 2006.
Gailey R, Harsch P. Introduction to triathlon for the lower limb amputee triathlete. Prosthetics and Orthotics International 2009: 33;242-255.
Hanspal R, Nieveen R. Water activity limbs. Prosthetics and Orthotics International 2002: 26; 218-225.
Osborough C, Payton C, Daly D. Influence of swimming speed on inter-arm coordination in competitive unilateral arm amputee front crawl swimmers. Human Movement Science 2010: 29; 921-931.
0067
Gyoosuk Kim (1) presenting Hyeonseok Cho (1) Shinki Kim (1) Museoung Mun (1)
Korea Orthopedics & Rehabilitation Engineering Center, Inchon, Korea, Republic of Korea (1)
Development of indoor mobile device for elderly and disabled
This study was conducted to develop a standing mobilization device which enables elderly and disabled to function for their daily life at standing position. The miniaturization of standing actuator has been proved through the simulation on the amount of torque upon the mechanism installation. The amount of torque and pressure needed to drive the wheel at 5mm curve was simulated to assess the safety of indoor curb-climbing when moving at the standing position
In this study, the 4-bar linkage mechanism was used to enable the independent standing operated by a motor and the safe movement in a narrow indoor at the standing state.
1. Mobile Device Design
4-bar linkage mechanism was used to implement the standing position of indoor mobile device. A small actuator installed at the mechanism allows standing from the sedentary position by a motor. A sling is installed at buttocks and this standing position is to be maintained by 3-point pressure at knee support, upper body support and buttock sling after standing.
2. Modeling and Simulation
The weight of mobile device is 64kgf and 4-bar linkage was used. Dummy’s weight was 80kgf with 170cm in its height. Multi-body dynamics analysis package (RecurDyn™) was used to analyze the loads upon the location of actuator installed for standing.
The lowest actuating power (2,500N) was required to install the actuator at position B (Mid) during the simulation for dummy standing. The initial actuating power (2,700N) has been increased at the highest height of actuator, a position C (Top) in the linkage. The lower location, position A (Low) required about 4,700N of the initial actuating power; however, the angle of standing was shown at around 63 degree when actuator was moved for 90mm. About 24Nm of torque was applied to the front driving wheel when traversing 5mm curb indoor, whereas about 20Nm of pressure torque was generated on wheel when falling at the curb. About 40Nm of torque was generated when back wheel traversed the curb, which to be drawn down in absence of actuating power, requiring the higher torque than front wheel.

In this study, the design and modeling of indoor mobile deice were performed for elderly and disabled individuals. The mechanism design for standing by the minimum load has been confirmed through its simulation. The traverse and basic safety of indoor curb have been confirmed when moving at the standing position. In the future study, the structure of mobile device is to produced to prove the results of simulation and assess its effectiveness on users.
0069
Norman Jacobs (1) Rogers Temu (1) Eunice Kombe (1) Presenting
Kcmu-college, Kilimanjaro, Tanzania (1) Tatcot, Kilimanjaro, Tanzania (2)
A survey on inclusion of employees with disabilities in major companies in Arusha Municipality, Tanzania: January-July 2013
Unemployment among of working age persons with disabilities (PWDs) is far higher than other individuals, with rates up to 80% reported in developing countries In Tanzania, paid employment is a source of income for 10% households headed by persons without disabilities compared to 3.1% of those households headed by PWDs. PWDs tend to experience higher unemployment and have lower earnings than people without disabilities.
This study assesses the inclusion of PWDs in major companies in Arusha Municipality in Tanzania. It examines issues on disability and employment in these companies and provides information regarding them for the broader employment sector in Tanzania.
This was a prospective qualitative study carried out in randomly selected major companies that have 50 or more employees in Arusha Municipality. A total of 45 participants were involved; 13 of the participants were PWDs and 32 were human resource managers in those companies. Different thematic questionnaires were administered to the two classes of participants. The data was analyzed using STATA program and triangulation method.
Majority of the PWDs were male (61.54% n=8) and some had attained university level of education (30.77% n=4). The company with the highest number of employees (n=2150) had the highest representation of PWDs (n=8). The majority of the human resource managers 81% (n=26) were unaware of government policies on disability. Many employers 84% (n=27) stipulate that the perspective on disability issues in the company is a ‘no discrimination attitude’ and also majority of PWDs did not feel as though they were being discriminated against. Majority of the employers (69.2%) indicated that the PWDs performed well and had no detrimental impact on overall production of the company. Majority of the companies (62%) also did not provide any assistive devices to PWDs.
The prevalence of disability in Tanzania is 8.5% among men and 8.2% for women and urban residents in Tanzania were more likely to have attained higher levels of education compared to rural counterparts.
The employment rate of PWDs was 0.34% (n=18) compared to the total number of employees (n=5240) in the companies surveyed. Also large companies are more likely to employ PWDs.
The majority of the companies did not provide any assistive devices agreeing with the findings of WHO who found only 5-15% of PWDs can access assistive devices in developing countries
Regardless that some PWDs had acquired their disability in the workplace, they felt that company administrators did not care to alter the work environment to allow easy access for PWDs.
Most companies revealed that PWDs tend to perform well and add to the company’s profits.
[NBS];2008 National disability survey, 2010. [Domzal];2008, Survey of Employer Perspectives on the Employment of People with Disabilities. [WHO];n.d http://www.who.int/disabilities accessed 10 Jan 2013.
0070
Corry K. van der Sluis (1,2) presenting Marieke Deijs (1,2) Natascha D.M. Ringeling-van Leusen (4) Raoul M. Bongers (1,3)
University of Groningen, Groningen, The Netherlands (1) University Medical Center Groningen, Department of Rehabilitation Medicine, Groningen, The Netherlands (2) University Medical Center Groningen, Center for Human Movement Sciences, Groningen, The Netherlands (3) Revant Rehabilitation Center, Breda, The Netherlands (4)
Flexible and Static Wrist Units in Upper Limb Prosthesis Users
Wrist movements might be important for upper limb prosthesis users to facilitate activities of daily life (ADL) or to prevent overuse complaints. Prosthesis hands with passive wrist motion capabilities, such as flexion/extension, are on the market, but research on the user’s experiences with flexible wrists is limited.
To compare flexible and static prosthetic wrists on functionality, user-satisfaction and compensatory movements in the shoulder joint.
Eight transradial amputees using a myo-electric prosthesis tested two passive prosthetic wrists in a cross over design. The Flex-wrist (Otto Bock) and Multi-flex wrist (Motion Control) were used for two weeks in their flexible and static condition, respectively. Measurements were performed 5 times: at baseline and after each two week period. Activity performance was measured using SHAP and Box & Block tests. OPUS informed after functioning with the prosthesis. Satisfaction was assessed using D-QUEST, TAPES and open-ended questions. Shoulder joint angles were measured using Xsens, when executing six ADL tasks. After finishing all measurements a semi-structured interview inquired after advantages and disadvantages of all wrist conditions.
No significant differences were found for SHAP, Box &Blocks or OPUS over the different wrist conditions. D-Quest results revealed better ‘ease in adjusting’ and ‘ease of use’ for flexible wrists. Participants’ satisfaction tended to be in favor of flexible wrists: these allowed a less restricted way of moving, made handling easier, and required less awkward movements. All participants but one indicated that they would choose a prosthesis hand with wrist flexion/extension capabilities if they could purchase a new prosthesis. Clear structure was lacking in the changes in shoulder joint angles between wrist conditions as a measure of compensatory movements. In the ADL tasks ‘lifting object’ and ‘handling cutlery’, the use of a flexible wrist seemed to indicate a smaller range of shoulder angles.
Patient satisfaction was greater for flexible wrists, which was not reflected in results of objective measurement instruments. These instruments showed comparable functionality for static and flexible wrists. Flexible wrists suggest a decrease of compensatory shoulder movements, which might be important for patients with overuse complaints.
0071
Maryam Maleki (1) presenting Mokhtar Arazpour (1) Stephen W Hutchins (2) Atefeh aboutorabi (1)
University of social welfare and rehabilitation sciences, Tehran, Iran (1) University of Salford, Salford, UK (2)
The effect of knee orthoses on gait parameters in medial knee compartment osteoarthritis: A literature review
Knee osteoarthritis is a musculoskeletal condition which is most prevalent in the medial compartment. This injury causes considerable pain, disability, and negative changes in kinetic and kinematic parameters. The efficiency of unloader valgus brace as a conservative treatment for medial knee osteoarthritis is not well documented.
The aim of this study was to review the previous research regarding the biomechanical effects of knee valgus braces on walking in medial compartment knee osteoarthritis patients.
According to the population intervention comparison outcome measure methods and based on selected keywords, 12 studies were chosen according to (met) the inclusion criteria.
The results indicated that treatment with knee braces was effective in decreasing pain, improving function, ameliorating improvement in range of motion, and increasing speed of walking and step length in conjunction with a reduction in the adduction moment applied to the knee.
Most of the literature demonstrated that wearing a valgus unloaded brace, results in modification of compressive force in medial knee compartment, reducing the knee adduction moment and alleviating symptomatic pain. Following this mechanism, improved gait symmetry, and increased activity of patients with medial osteoarthritis have been demonstrated. In summary, osteoarthritis knee braces may be considered for improvement of walking and treatment of medial compartment knee osteoarthritis.
1. Gaasbeek, R.D., et al., Valgus bracing in patients with medial compartment osteoarthritis of the knee: A gait analysis study of a new brace. Gait & posture, 2007.
2. Pollo, Fabian E., et al. “Reduction of medial compartment loads with valgus bracing of the osteoarthritic knee.” The American Journal of Sports Medicine 30.3 (2002): 414-421.
3. Self, Brian P., Richard M. Greenwald, and Daniel S. Pflaste. “A biomechanical analysis of a medial unloading brace for osteoarthritis in the knee.” Arthritis Care & Research 13.4 (2000): 191-197.
4. Fantini Pagani, C.H., et al., Short-term effects of a dedicated knee orthosis on knee adduction moment, pain, and function in patients with osteoarthritis. Archives of physical medicine and rehabilitation, 2010.
5. Richards, J. D., et al. “A comparison of knee braces during walking for the treatment of osteoarthritis of the medial compartment of the knee.” Journal of Bone & Joint Surgery, British Volume 87.7 (2005): 937-939.
6. 13.Lindenfeld, Thomas N., Timothy E. Hewett, and Thomas P. Andriacchi. “Joint loading with valgus bracing in patients with varus gonarthrosis.” Clinical orthopaedics and related research 344 (1997): 290-297.
7. 14. Jones, Richard K., et al. “A comparison of the biomechanical effects of valgus knee braces and lateral wedged insoles in patients with knee osteoarthritis.” Gait & Posture (2013).
8. 15. Fantini Pagani, C.H., M. Hinrichs, and G.P. Brüggemann, Kinetic and kinematic changes with the use of valgus knee brace and lateral wedge insoles in patients with medial knee osteoarthritis. Journal of Orthopaedic Research, 2011.
0072
Ahmad Aziz (1) presenting
PIPOS, Peshawar, Pakistan (1)
Quality Procedure of Students Recruitment to an ISPO Category II Recognized Program
To have a successful completion of the degree level course in prosthetics and orthotics, quality selection process of the candidates to the course play an important role. Candidate’s aptitude for P&O, brilliance and technical approach is to be judged regardless of cost, creed and religion status
The aim of this work is to ensure that the selection of the students to the ISPO degree level course is based on merit and that the quality students are selected.
The following method is adopted to select the candidates to the P&O course accredited by ISPO as Cat II.

The ISPO accredited school shall show good academic outcome. These outcome results can only be possible with the good input by standardized selection procedure of the students. The results here indicate lower and no dropouts due to multiple reasons including the proper and merit wise selection/ entry to the course.
0073
Maryam Maleki (1) presenting Atefeh Aboutorabi (1) Monireh Ahmadi Bani (1) Navid Monzavizadeh (1)
University of social welfare and rehabilitation sceiences, Tehran, Iran (1)
The effectiveness of Armeo therapy on functional capacity after neurological disorders: A literature review
Effective rehabilitative therapies are needed for patients who suffer from strokes, traumatic brain injuries or other neurological disorders that results in hand and arm impairment. Recent research suggests that the neural plasticity of the brain is retained and new connections can made through intensive, repetitive and task-oriented movements. Therefore, the Armeo therapy concept has been developed to address the improvement of function and quality of life of patients with upper limb deficits.
This Study aims to review of the previous research about the effect of Armeo therapy on functional capacity in neurological dysfunction.
The PICO method was used by an experience researcher based on selected keywords and their composition in well-known databases and an electronic search performed. Finally, 10 articles were selected for final evaluation.
12 articles were selected for final evaluation. Many were case studies, and also had limited and heterogeneous sample sizes. The results of the analysis demonstrated that independence and quality of life were improved when using Armeo therapy. Also significant improvements were found in functional capacity parameters, upper limb and handgrip muscle strength and motor function in a chronically impaired paretic arm after neurological disorders
The Armeo therapy improves the efficiency of therapy treatments because the exercises are self-initiated, self-directed, functionl and intense. Even severely impaired patients can practice independenty, without the constant presence of a therapist, permitting patients to exploit their full potential for recovery. Finally, the Armeo therapy is specifically suited for patients who are beginning to regain active movement of arm and hand.
1.Gijbels, Domien, et al. “The Armeo Spring as training tool to improve upper limb functionality in multiple sclerosis: a pilot study.” Journal of neuroengineering and rehabilitation 8.5 (2011): 5.
2. Zariffa, J., et al. “Feasibility and efficacy of upper limb robotic rehabilitation in a subacute cervical spinal cord injury population.” Spinal cord 50.3 (2012): 220-226.
3. Rudhe, Claudia, et al. “Reliability of movement workspace measurements in a passive arm orthosis used in spinal cord injury rehabilitation.” Journal of neuroengineering and rehabilitation 9.37 (2012).
0074
Tim Eikelboom (1) presenting Axel Schulz (2) Ruethning Holger (3)
Sanitaetshaus Mitschke, Guetersloh, Germany (1) Össur, Frechen, Germany (2) Sanitätshaus Drescher, Haan, Germany (3)
Unloader-Braces and Patient’s Compliance – what’s important for knee-OA patients?
Unloader-Braces are a guideline recommended option within management of symptomatic knee OA- if unicompartmental knee OA with varus-/ valgus deformity is existing. While 1st generation Unloader braces did show a drop-out rate of about 40%, due to insufficient pain relief and poor comfort, 2nd Generation Unloader-braces show a much better drop-out rate of about 15%, by providing more comfort and improved pain relief. If thos Unloader braces are prescribed it is mandatory to select abrace for the patients which fits their needs and expectations regarding the brace.
This observational trial was conducted in order to identify the factors which drive patients decision to choose an unloader brace.
Prospective, multi-Center trial in 14 German medical supply stores evaluating the most important factors influencing knee OA patients, who got an unloader brace prescribed by their treating orthopedic specialist, to choose an unloader brace. Patients were introduced to two different unloader braces from different manufacturers and had to try both braces while walking on plain ground and stairs. Standardized questionnaires were used to document the identified factors which were told by the patients and to document walking pain [VAS scale 0-10] at baseline and after test fitting and walking with the unloader brace.
93 Patients have been evaluated (age: 63,2 years (mean), 79,57% medial, 20,43% lateral knee-OA Walking pain at baseline was 6,85 (mean) and 2,22 (mean) five minutes after fitting. The named reasons to choose an unloader brace were: Low weight (61,29%), easy to use (51,32) Comfort while walking (49,46%) and most importantly an immediate onset of pain relief (86,02%). Patient’s assessment of the braces were diverse, the lightweight three point leverage brace with dynamic force straps was preferred by most of the patients vs. the other hard frame (double-upright) braces -which have been introduced to the patients.
The immediate onset of pain relief, comfort while walking and easy handling are the most relevant factors to select an unloader brace. Those factors can be seen as most relevant in order to ensure good patient compliance and regular usage of the prescribed unloader brace within an ongoing knee-OA management.
0076
Markanda Chandra Dash (1) presenting Aratatran Patra (2)
Northern Railway Central Hospital, New Delhi, India (1) Secretary,Society of Prosthetics & Orthotics(NMS of ISPO in India), Kolkata, India (2)
Prosthetic Rehabilitation of Trilateral amputee with Kinetic Consideration- A case Study
Medical Rehabilitation of vital multiple amputations are a major challenge for prosthetist and the entire clinical team to back to the patient to the main stream of society. Particularly, in case of young unmarried adults in India. In case of trilateral amputee i.e. both lower limbs and one upper limb with traumatic accident is very difficult to design his prosthesis for three extremities with optimal energy expenditure.
To study the energy expenditure of the amputee during his daily activities and to way out to return back to his working area for livelihood.
A 32 year old male train accident patient with
Lt. trans femoral,
Lt. trans humeral and
Rt. Trans tibial amputation reported at Northern Railway Central Hospital, New Delhi Prosthetic & orthotic department for management with prosthesis.
Lt. trans humeral and Lt. trans femoral stumps are having standard length but flabby musculature. Rt. Trans tibial is an ideal stump.
As he had undergone higher end amputations of both lower and upper limbs, so to achieve standing balance and further progression was a difficult task. Trans femoral components were dynamic foot, pneumatic stance control knee joint & laminated ischial containment socket. Lt. trans humeral was a double diode myo- electric prosthesis with manual elbow joint and Rt. trans tibial was having dynamic foot with laminated PTB socket.
At the beginning of prosthetic fitment, energy consumption even in getting standing balance was very high to control all the three limbs. More over psycho- social status of this patient was not so sound, so the rate of fatigue due to the above reasons was more and frequent.
With prolong training and various major alignment considerations; finally this patient was able to walk with minimum expenditure of energy. At an average, the earlier energy expenditure reduces to approximately 46% and was able to return back to his parent job in Railway.
0077
Aston Ndosi (1,2) presenting Helen Buchanan (2) Seyi Amosun (2)
Kilimanjaro Christian Medical University College, Moshi, Tanzania (1) University of Cape Town, Cape Town, South Africa (2)
Locally manufactured wheelchairs in Tanzania – Do they meet the needs of Tanzanian wheelchair users?
Tanzania is estimated to have a population of over 49 million people in 2013. About 8% of the population experience some type of activity limitations. WHO estimates that between 20 to 25 million people worldwide who need a wheelchair are unable to access one. About 3.5 million disabled persons in Tanzania require or use a wheelchair. Wheelchair users in Tanzania experience various challenges relating to mobility and community participation
To determine the extent to which the needs of users of wheelchairs manufactured locally in Tanzanian are met in respect to activity and participation, features and service provision of the wheelchairs.
A quantitative descriptive cross-sectional analytical design was used. The study was done in Tanzania whereby structured questionnaires mostly closed were administered. Convenient sampling was used to obtain 75 users. Inclusion criteria were adults aged 18 – 65 years who were active wheelchair users, should have possessed the wheelchair for at least three months at the time of the study, should have lived in the same area for at least six months at the time of recruitment. The exclusion criterion was people with cognitive impairment. Data were analyzed with the Statistical Package for the Social Sciences (SPSS®) software program version 20.0 (SPSS Inc. 2006).
The median age of participants was 34 years, and the median period of using wheelchairs was 8.0 years (min: 1.0, max:30.0 years). Most participants (61%) had sustained spinal cord injuries, and used three-wheeler chairs (76%). More than 90% reported that their wheelchairs had positively influenced their activity and participation needs, and 85% were satisfied with their ability to carry out their daily activities. Relationship between the type of wheelchair and place of residence indicated that three-wheeler wheelchairs appeared to be mostly used in rural settings (33, 44.0%) compared to four-wheeler wheelchairs (10, 13.3%). Participants expressed satisfaction with the durability of the wheelchair (89%), and the professional services received (71%), but not with follow-up services (77%). There was no significant difference in participant’s satisfaction with functional needs and gender (p= 0.808).
The median age of starting using wheelchair, i.e. median (range) for 73 participants, was 25.0 (2.0-56.0) years. The majority of participants were more satisfied with wheelchair features than the services provided. The majority of participants (n=58, 77.4%) were dissatisfied with follow-up services. The wheelchairs had a positive impact on participants’ activity and participation needs. People with disabilities expressed general satisfaction with the use of locally made wheelchairs but follow-up services need attention.
0079
Caroline E Roffman (1,2) presenting John Buchanan (1,2) Garry T Allison (1,2)
School of Physiotherapy & Exercise Science, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia (1) Royal Perth Hospital, Perth, Western Australia, Australia (2)
Locomotor performance characteristics following lower limb amputation
Locomotor skills have been demonstrated as predictors of prosthetic non-use1. However, there is a lack of consensus on which performance measures should be used to evaluate people with lower limb amputation during rehabilitation2 and limited knowledge on how performance in the functional domains of velocity, distanced walked and balance during rehabilitation relates to future ability to use a prosthesis3.
The study objectives were to determine: 1. If performance measures assessed during rehabilitation could identify individuals at high risk of prosthetic non-use 12 months post-discharge. 2. If diagnostic groups at risk of prosthetic non-use including people with Aboriginal ethnicity, older age, amputation above transtibial level, bilateral lower limb amputation, atraumatic cause, diabetes and high comorbidities had poorer performance measure results.
Medical records of 201 consecutive participants with lower limb amputation from Royal Perth Hospital, the state amputee rehabilitation centre, were retrospectively audited for 10m walk (10MWT), timed up and go (TUGT), 6 minute walk (6MWT) and four square step (FSST) tests and descriptive variables. Participants were interviewed at median 1.5 (interquartile range, 1.2 to 2.2) years post-discharge to identify prosthetic users, non-users and time prosthetic use ceased. Receiver operator characteristic curves were generated to determine performance measure thresholds and relative risk (RR) for prosthetic non-use. Mann Whitney U Tests were used to determine if locomotor performance of diagnostic groups at risk of non-use were significantly different from the remaining cohort.
At 12 months post-discharge 18% (36) of participants were prosthetic non-users. Performance measure thresholds and RR of prosthetic non-use (95% CI) were:
Locomotor performance during rehabilitation may identify future risk of prosthetic non-use. Similar to past studies locomotor performance was poorer in those with amputation above transtibial level, high comorbidities, bilateral lower limb amputation and older age3. Clinical utility was greatest for the 10MWT. Validation is warranted.
1. Roffman CE, Buchanan J, Allison GT. Predictors of non-use of prostheses by people with lower limb amputation after discharge from rehabilitation: the development and validation of clinical prediction rules. Journal of Physio. 2014;In press.
2. Heinemann AW, et al. Outcome Instruments for Prosthetics: Clinical Applications. Phys Med Rehab C N Am. 2014;25(1):179-198.
3. Gailey RS, et al. The amputee mobility predictor: an instrument to assess determinants of the lower-limb amputee’s ability to ambulate. Arch Phys Med Rehab.2002;83(5):613-627.
0081
Caroline E Roffman (1,2) presenting John Buchanan (1,2) Garry T Allison (1,2)
School of Physiotherapy & Exercise Science, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia (1) Royal Perth Hospital, Perth, Western Australia, Australia (2)
Long term locomotor function in individuals with lower limb amputation following discharge from rehabilitation
In Australia there is limited information on long term locomotor outcomes of people with lower limb amputation after rehabilitation discharge1,2. Roffman et al1 demonstrated that indigenous status was not predictive of prosthetic non-use however locomotor function of Aboriginal people has not been reported despite high rates of diabetes related amputation and poor health outcomes. The Locomotor Capabilities Index 5 (LCI5) is a reliable and valid measure of self reported locomotor function for people with lower limb amputation3.
The study aims were to: 1. Quantify prosthetic use for locomotor activities in people with lower limb amputation who have been discharged from rehabilitation in Western Australia. 2. Determine if self reported locomotor function after rehabilitation discharge was different between prosthetic users and non-users; and diagnostic user groups including those with Aboriginal ethnicity, age
201 consecutive participants with lower limb amputation from Royal Perth Hospital, the state amputee rehabilitation centre were recruited. Medical records were audited for descriptive characteristics. Participants were prospectively interviewed at median, 1.5 (IQR, 1.2 to 2.2) years after discharge using the LCI5 and a previously piloted questionnaire regarding their prosthetic use, falls history, functional ability, amputation, general health and demographic details. Time prosthetic use ceased relative to physiotherapy discharge and reasons for prosthetic non-use were recorded for non-users. Descriptive statistics and Mann Whitney U Tests were used to determine if locomotor capabilities were significantly different between prosthetic users and non-users and the diagnostic user groups.
A total of 26% (52) of participants were prosthetic non-users and 74% (149) users. Prosthetic non-users (median, 4 IQR, 1 to 11) reported significantly lower Basic, Advanced and Total locomotor capabilities (z = 8.13, p < .001) than users (median, 24 IQR, 18 to 28). LCI5 scores were significantly different (z
This was the first study in an Australian cohort with lower limb amputation to report long term locomotor function after rehabilitation discharge and demonstrate that locomotor function was not significantly different for Aboriginal people. Ceiling effect in younger participants with traumatic amputation and significantly poorer LCI5 scores for prosthetic non-users and the diagnostic user groups were consistent with past findings. Self reported locomotor performance after rehabilitation discharge using the LCI5 may inform clinical decision making and service model planning.
1. Roffman CE, Buchanan J, Allison GT. Predictors of non-use of prostheses by people with lower limb amputation after discharge from rehabilitation: the development and validation of clinical prediction rules. Journal of Physio. 2014; In press.
2. Hordacre BG, et al. Lower-limb amputee rehabilitation in Australia: analysis of a national data set 2004-10. Aust health review 2013;37(1):41-47.
3. Franchignoni F, et al. Reliability, validity, and responsiveness of the locomotor capabilities index in adults with lower-limb amputation undergoing prosthetic training. Arch Phys Med Rehab. 2004;85(5):743-748.
0082
Noriaki Maeda (1) presenting Yukio Urabe (1) Syou Iwata (1) Junpei Sasadai (1)
Hiroshima university, Hiroshima, Japan (1)
The effect of different ankle braces intervention on static and dynamic postural stability after single-leg landing
Ankle sprains are one of the most common injuries in competitive and recreational sports. In sports, injuries to an ankle ligament account for 15% to 45% of all injuries, and the athletes most commonly affected are participants in jumping and landing activities such as volleyball and basketball. Despite their widespread use, there are a limited number of studies examining the effect of ankle supports brace on postural control.
The aim of the present study was to determine the effect of soft (SB) and semi-rigid (SRB) ankle brace on static and dynamic postural stability in healthy men.
Ten healthy men ( mean ± SD age, height and weight: 25 ± 5 years, 173 ± 6 cm, 67 ± 8 kg) participated in the study. Subjects were assigned to 3 randomly ordered experimental conditions, in which all subjects performed by non-brace (NB), SB and SRB. Static balance (standing with eyes opened and eyes closed) was measured locus length/second (mm/s) and enveloped area (mm/s2 ) on the non-dominant limb for unilateral by using a stabilometer. Dynamic postural stability was assessed Dynamic Postural Stability Index (DPSI, Wikstrom 2005) by using a force platform. DPSI were calculated for each condition [1]. This study also used raw data signals to calculate the GRFmax, which was expressed as the magnitude of the peak force (N).
The difference in the locus length/second (mm/s) and enveloped area (mm/s2 ) were not significant among 3 conditions. The results of this study indicated a significant effect of SRB compared with SB and control for VSI and DPSI (p < 0.05). The difference in the GRFmax was not significant among 3 conditions (Table 1).
Values for the Dynamic Postural Stability Index and Directional Components, GRFmax by three conditions

NB: Non-Brace, SB: Soft Brace, SRB : Semi-Rigid Brace, GRF max : Grand Reaction Force maximum.
Indicates a significant difference among NB, SB and SRB conditions (P < 0.05).
This study suggests that SRB adversely affect dynamic balance of landing single-legged compared with NB and SB. Furthermore, SRB intervention may improve balance performance by increasing dynamic postural stability.
[1] Wikstrom EA, Tillman MD, Smith AN, Borsa PA. New force-plate technology measure of dynamic postural stability: the Dynamic Postural Stability Index. J Athl Train 40: 305-309, 2005.
0083
Sedegheh Malek Mohammadi (1) presenting
Iran University of Medical Sciences, Tehran, Iran (1)
How much load is applied in identified locations of the plantar fascia in static and locomotion
It has been accepted that plantar fascia thickness is a biomechanical variable to understand the concentration of the amount of the applied load in identified locations of the plantar fascia.
The aim of this research is quantifying the amount of the load / body weight applied in identified /equivalent locations of the plantar fascia in both feet.
This research was done through a four- step method. Step 1, literatures were reviewed to search the results, gaps and problems within previous studies about plantar fascia evaluation with ultrasound. Step 2, plan of investigation was designed to recognize each location of the plantar fascia along its length and to identify equivalent locations of the plantar fascia in both feet with ultrasound 2D measuring. Step 3, pressure markers were put on identified locations of the plantar fascia. The amount of the applied pressure was assessed with E-med, through the ground reaction force, in static and locomotion. Step 4, the percentage of the body weight was calculated in identified locations.
It was found that quantifying the amount of the applied load in identified location of the plantar fascia is achievable, individually. The outcome of quantitative information of an individual with 70 Kg weight was; plantar fascia thickness [(1.2 ± 0.7mm) < longitudinally > (1.3 ± 0.3mm) and (1.1 ± 0.6mm) < transversely > (1.4 ± 0.2mm)], [(74 ± 1.6 mm) < the length > (166.4 ± 4.7mm) and (22.2 ± 4.7mm) < the width > (48.3 ± 3.6mm) of the plantar fascia location under pressure], [ (43.3 ± 4.7) < applied pressure on the plantar fascia > (78.3 ± 19.5)], [(0.6% ± 0.18%) <the percentage of the body weight in identified location of the plantar fascia (1.1% ± 0.27%)]
Relying on quantitative information of this research; insole, shoes and foot orthosis can be designed more accurate to relief pain, to prevent / to stop the progression of foot and ankle deformity and to prevent plantar fascia injuries.
[3] Wearing, S.C. 2006. Sports Medicine
[6] Caravaggi, P., 2010. Journal of Anatomy
[15] Rao, S., 2011. Gait & posture
0084
Laure Moisson (1) presenting Corinne Bronfen (2) Briac Colobert (3) Jean-François Mallet (2) Thierry Haumont (2)
Proteor, Caen, France (1) Centre Hospitalier Universitaire de Caen, Caen, France (2) Proteor R&D, Dijon, France (3)
Objective wear time measurement of night brace (Caen brace) in Adolescent Idiopathic Scoliosis
Scoliosis can be treated with brace worn only at night (CAEN, Providence and Charleston). The main problem that may be encountered during brace treatment of idiopathic scoliosis is patient’s compliance. It is still poorly reported wearing time and its evolution during the first year of treatment for night-only type of brace.
To assess CAEN brace adaptation time (the amount of time needed for the brace to be worn at least 7 hours 2 nights in a row), the complete acceptance time (the amount of time needed for the brace to be worn at least 7 hours 6 nights out of 7) and the possible “seasonal” effects.
The Committee for the Protection of Persons Nord Ouest 3 (France) gave a favourable opinion on this study. This is a prospective non-interventional study with the aim to observe the wear time during the first year of prescription of CAEN brace. 20 idiopathic scoliosis patients are followed during 12 months. An initial visit (Week0) includes or excludes patients in the cohort. 3D digital capture and measurements needed to make the brace made within three weeks after the prescription of the brace (Week3) and the brace is delivered at Week6. Duration of use is recorded by a temperature sensor (reference exact). The data are collected during the classical follow-up of the patients (Week10, Week22, Week34 and Week46). The end of the study takes place 12 months (Week58) after the delivery of the corset, then the data are no longer collected but patients continue to be monitored normally. We computed the statistic descriptive and the relationship (r²) of the following parameters: adaptation time, acceptance time, strength of the hypercorrection, age, Risser, total wear time.
As preliminary results, we have collected wear-time data for 11 patients during 52 weeks. All patients completed the first period of 4 weeks. The mean adaptation time was 13 days for 17 patients, and 3 patients failed to achieve 7 hours 2 nights in a row within the first month of treatment.
Figure 1 shows the wear time (in hours) during the first 41 days for patient 10. Two patients discontinue the treatment in the first year.

The results suggest that the first two weeks of treatment are crucial for the compliance of the treatment; the shorter the adhesion the better the brace will be worn.
0085
Jean-Charles Gesbert (1) presenting Philippe Violas (2) Briac Colobert (4) Jean-Jacques Dufournet (3) Didier Vervaeke (3) Delphine Loiseau (3) Lalaonirina R. Rakotomanana (1)
IRMAR Université de Rennes 1, Rennes, France (1) Service de Chirurgie Pédiatrique, CHU Hôpital Sud, Rennes, France (2) Proteor, Rennes, France (3) Proteor R&D, Dijon, France (4)
Geometrical and biomechanical data for scoliosis treatment
Scoliosis is a three-dimensional deformity of the spine and of the rib cage. Understanding the link between the stress-strain behavior of human trunk tissues and the pressure map distributions at the trunk-brace interface is of major interest for scoliosis treatment. The current technology is not able to provide accurate pressure measurement nor direct evaluation of biomechanical tissues properties. In this way, the present work focuses on the quality of the biomechanical data and the multi-sensors data fusion.
The goal of this study is to provide an accurate fusion of multi-sensors data in the perspective of customized brace design.
Brace-trunk pressure fields are measured with a new prototype of vest made of pressure sensitive textile fibers (Figure 1) connected to a small electronic data logger. The high elasticity of the vest allows accurate localization of the pressure. The device can measure over long periods of time. Two orthogonal X-rays images and a 3D digitization of the patient’s trunk are used to create a geometrical spine and ribs model. The geometrical model and the pressure mapping are fused in specifically developed software.

Prototype of sensitive vest
Pressure measurements and 3D reconstruction of the trunk have been realized for ten patients. Projection of pressure maps onto the torso shape shows a coherent localisation of pressure zones with respect to the brace supports. Results show a good agreement between the localisation of the brace (expansion chambers and corrective areas) and positions of low / high pressure. Temporal evolution of pressure for a point of thoracic support shows the influence of breathing on measurement. Temporal evolution of pressure also seems to be well correlated with the position. Different positions can lead to a factor of two between pressure values.
The method presented here is a simple, fast and reliable way to obtain 3D topographical maps of pressure exerted by the brace against the torso. Pressure is position-dependent suggesting that it should be taken into account for brace design. Knowledge of pressure and 3D shape of internal and external components of trunk provides a complete data set for biomechanical studies. The numerical values of the pressure measured should be validated in the future. We are also investigating the way (domain equations, boundary conditions and solver settings) the geometrical reconstruction of the patient’s trunks could be modelled in Comsol Multiphysics® in order to estimate patient’s biomechanical parameters.
0086
Neha Mathur (1) presenting Ivan Glesk (1) Arjan Buis (1)
University of Strathclyde, Glasgow, UK (1)
Thermal Time Constant: Improving the accuracy of skin temperature predictive modelling in Lower Limb Prostheses
Elevated skin temperature at the body/device interface of lower-limb prostheses is one of the major factors that affect tissue health [1]. The heat dissipation in prosthetic sockets is greatly influenced by the thermal conductive properties of the hard socket and liner material employed. This leads to a hypothesis that if the thermal properties of the socket & liner materials are known then the in-socket skin temperature could be accurately predicted by measuring between the socket and interface liner, rather than at the more technically challenging skin interface.
To predict the residual limb temperature by employing a machine learning algorithm -Gaussian processes, which utilizes the thermal time constant values of commonly used socket and liner materials.
In order to measure the level of thermal responsiveness of the prosthetic material, the thermal time constant is evaluated. The thermal time constant is the time it takes for a material to change to 63.2% of the total difference between its initial and final temperatures. The experimental setup included a heat source whose temperature could be controlled through a proportional-integral-derivative (PID) controller. The liner and socket materials were placed both individually as well as in combination on the heat source and the temperature at each interface was measured by K-type thermocouples attached to a data logger. The time constant of the prosthetic materials was determined using the logarithmic method and was then used in the mathematical model to time shift the data for better predictive accuracy. The materials of interest in our study are the Polyurethane liner and the Thermosetting lay-up socket material.

For Polyurethane liner with a 5mm thickness, the thermal time constant was 3.1minutes. But when it was used in combination with a thermosetting socket material of 4mm thickness, the thermal time constant increased to 5.4 minutes. This implies that the choice of materials in prosthesis influences the body’s inability to thermoregulate effectively. The developed Gaussian model [2] does not take into account the effect of thermal time constant of the prosthetic materials. A thermal time delay of 5.4 minutes is in built in the existing model now and as a result the accuracy of the model is improved from ±0.8ºC to ±0.5ºC.
This study highlights the relevance of thermal time constant of prosthetic materials in Gaussian Processes technique which would be useful in addressing the challenge of non-invasively monitoring the residual limb skin temperature. With the introduction of thermal time constant in the model, the accuracy increases, thereby making prediction more reliable. For other liner-socket combinations, the thermal time constant may vary and hence model would need to time shift the data accordingly.
[2] N. Mathur, “Skin Temperature Prediction in Lower Limb Prostheses,” IEEE JBHI, Nov.2014, in press.
0087
Evgueni Dukendjiev (1) Tatiana Dukendjieva (1) presenting
Atypical Prosthetics Laboratory, Riga, Latvia (1)
Sleep rehabilitation by “Bionika II” robotized system
The author’s method is discussed for the rehabilitation of children with cerebral palsies (CP) and cerebrospinal injuries (CSI) in special conditions of brain and body. In informational and energetic aspect, humane brain and body have five conditions in reverse descending order: death, apparent death, apallic state, sleep, wakefulness. Children’s rehabilitation time is limited by diurnal rhythms of body and working hours of clinic and specialists, therefore the out-of-wake treatment time range should be extended.
Developed a method and robot for using the daytime sleep of a child with cerebrospinal and similar injuries who a long time are in immovable state for treatment
Taking into consideration the cataplexy, a child with CP or CSI is brought into a daytime sleep regime by means of monotonous body-rocking in frontal plane accompanied by noninvasive effect upon the frontal semicircular channel of vestibular system. The robot provides the patient’s imperative walking during sleep. The method [2] is implemented by the use of BIONIKA II locomotor robot with a special suspension of orthotic system (ROS) [1]. Common center of mass (CCM) is moved in frontal plane (20-45mm) as a result of ROS suspension on the spherical joint in parafrontal plane at (H) height:
H [CCM+ 12% body height +/- 0.48 %]
CCM traces out a ∞-like trajectory (in the form of two interconnected symmetrical loops). The process of frontal rocking, as a result of movement of the electric treadmill at coordinated speed and rocking of the horizontal reciprocal mechanism is synchronized with the processes of occurrence of fast sleep phase followed by slow sleep phase when active inhibition takes place coming from the brain stem. Presynaptic and postsynaptic inhibition of activity of gamma- and alpha-motoneurons leads to reduction in muscular tone when sleeping thus increasing by an order of magnitude the availability of correction of locomotor centers. Forced mechanical movement, which is realized on macrolevel, changes the intensity of reflectory impact by the spindles and Golgi tendinous receptors thus obtaining any activity ratios of flexors and extensors with the observance of mechanism of reciprocal inhibition of antagonists.
A new method is implemented, which uses the time of artificially induced sleep for the rehabilitation of children with CP and CSI. The sleep is induced by noninvasive method, using the peculiar features of body and cataplexy. External energy of BIONIKA II robot is used for the imperative locomotion. Movement is treatment, but now also during the locomotory sleep.
[1] Дюкенджиев Е. Бионика в реабилитации ЦП и СМЗ Реципрокные ортезные системы и комплексы. Рижский Технический Университет. Том |. Рига, 2011.
[2] Дюкенджиев Е. Бионика в реабилитации ДЦП и СМЗ Роботизированные реципрокные комплексы. Рижский Технический Университет. Том ||. Рига, 2013.
0090
Lina Magnusson (1) presenting Harold G Shangali (2) Gerd Ahlström (1)
Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden (1) Department of Prosthetics and Orthotics, Faculty of Rehabilitation Medicine, Kilimanjaro Christian Medical University College, Tumaini University Makumira, Moshi, Tanzania (2)
Graduates’ perceptions of education at the Tanzania Training Centre for Orthopaedic Technologists and their profession
The Tanzania Training Centre for Orthopaedic Technologists is one of very few schools in Africa providing training for prosthetic and orthotic staff, and it is therefore important that the education offered is of high quality. It is necessary to determine if the education currently provided meets the needs of people with disabilities requiring prosthetic and orthotic services.
To describe how Tanzanian and Malawian graduates of the Diploma in Orthopaedic Technology offered at the Tanzania Training Centre for Orthopaedic Technologists perceived their education in relation to their profession.
Nineteen graduates from the diploma course in orthopaedic technology working in Tanzania or Malawi were interviewed. Phenomenographic analysis was applied on statements of the participants’ perceptions and conceptualized into conceptions. Similarities and differences in conceptions were analysed and grouped into descriptive categories.
Seven descriptive categories emerged namely; Varied awareness of the profession before starting education, Well-equipped teaching facilities, Aspects lacking in the learning context, Need for changes in the curriculum, Enable people to walk is motivating, Obstacles in working conditions and the Need for professional development. All participants perceived possible improvements to the content and learning environment.
The study can contribute to the evidence base for review of the international guidelines for training personnel in developing countries for prosthetics and orthotics services. The major changes to the curriculum suggested were to reduce the time spent on learning to work with metal and wood and to focus more on advanced prosthetic and orthotic technology. The technology used in low-income countries has changed in Malawi and Tanzania, where polypropylene technology is commonly used. However, this development is dependent on the provision of components by the International Committee of the Red Cross or similar provisions to Africa. Sustainability needs to be carefully considered while recommending changes to the curriculum.
Prosthetic and orthotic services can be better provided by modifying the education program content by dedicating more time to the clinical management of different patient groups and applied biomechanics and reducing the program contents focus on technical aspects of prosthetic and orthotic practice. Working in rural conditions has demands that graduates were not prepared for and the graduates desired continued training.
0091
Lina Magnusson (1) presenting
Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden (1)
Variables associated with patients satisfaction with low cost technology prosthetic and orthotic devices and service delivery in Malawi and Sierra Leone
Few studies have investigated overall satisfaction with prostheses fabricated using low-cost technology. Evidence-based recommendations for prosthetic and orthotic services in low-income countries were needed in order to more effectively provide services. Detailed analysis of factors which influence patient satisfaction with assistive devices are therefore of interest to investigate.
Identify variables associated with patients’ satisfaction with their lower-limb prosthetic or orthotic device and associated services in combined data from Malawi and Sierra Leone.
Questionnaires, including QUEST were used to collect self-reported data from 222 patients in Malawi and in Sierra Leone. Simple linear regression analyses of 23 variables was initially conducted separately for the two outcomes of sub-scale scores for satisfaction of assistive device and service. Variables with p-values of less than 0.1 were included in a multiple regression analysis with backward elimination (p<0.1). Final multiple regression analysis included variables with p-values of less than 0.1.
The variables which were significantly associated (p<0.1) to satisfaction of assistive device were; pain, general condition of the device, ability to walk on uneven ground/roads, ability to walk on stairs, and ability to get in and out of a car. The variables which were significantly associated (p<0.1) with satisfaction of service were; country, general condition of the device, ability to walk on uneven ground, ability to pay for costs associated with receiving the service appliances, accommodation, travel, and ability to walk on stairs.
The variables associated with higher satisfaction with assistive devices were absence of pain, condition of the device, and the ability to walk on uneven ground, on stairs, and to get in and out of a car. Higher satisfaction with services was associated with country, condition of the device, ability to walk on uneven ground and on stairs, and the capacity to pay for costs associated with receiving services.
Magnusson L. Prosthetic and Orthotic Services in Developing Countries. Doctoral Thesis. School of Health Sciences Dissertation Series No 56. 2014. ISBN 978-91 Available from: http://urn.kb.se/resolve?urn=urn:nbn:se:hj:diva-24973
0092
Lina Magnusson (1) presenting
Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden (1)
A Comparison of Patients Use and Mobility with Prosthetic and Orthotic Assistive Devices in Malawi and Sierra Leone
ICRC low-cost polypropylene technology for producing prosthetic and orthotic devices and traditional metal orthoses was commonly used in Malawi and Sierra Leone. The proportion of staff with a three year degree were lager in Malawi than in Sierra Leone where most of the staff were trained on the job or had a one year education. Sierra Leone has a history of conflict, while Malawi has a more stable situation.
Compare results from Malawi and Sierra Leone concerning patients’ use and mobility with their lower-limb prosthetic or orthotic device.
Magnusson L. Prosthetic and Orthotic Services in Developing Countries. Doctoral Thesis. School of Health Sciences Dissertation Series No 56. 2014. ISBN 978-91 Avalible from: http://urn.kb.se/resolve?urn=urn:nbn:se:hj:diva-24973
0093
Lina Magnusson (1) presenting
Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden (1)
Human rights for persons with disability using prosthetic and orthotic devices in Sierra Leone
Sierra Leone is a low income countries in west Africa that has a history of conflict. Sierra Leone have signed and ratified the Convention of Rights of Persons with Disabilities.
To evaluate persons with disability that use prosthetic and orthotic assistive devices access to human rights. The addressed areas were; right to health, right to a standard of living adequate for health, right to vote, right to marry and found a family, right to education, right to work and. A further aim was to compare groups of participants regarding gender, area of residence, income and type and level of device.
Questionnaires were used to collect self-reported data from 139 prosthetic and orthotic users in Sierra Leone.
About half of the patient considered their overall physical health as good or very good. Thirty-seven percent of the participants said their mental health is bad or very bad. The majority said they did not have access to medical care and the most common reason given was that they could not afford doctors fee. The orthotic users reported they required medical care outside home more often than the prosthetic users. About half of the participants could not acess afford medication when they needed it. About half of the participants had regularly access to safe drinking water and only 10% had the possibility to eat three times a day. The majority had a reasonably or adequate house to live. Half of the participants were married and 70% had children. Almost all reported that they could vote if they wanted. About half were working but often self-employed with small business. Sixty percent could read and write.
There was still a need for significant progress in increased acess to medical care and medication when needed for persons with lower limb physical disability in Sierra Leone. Increased acess to food and clean water to facilitate an acceptable standard of living adequate for health were also necessary in order to strive towards implementing the rights to health for persons with disability.
0094
AMIT SARAF (1) presenting
Saraswati institute of medical sciences, ghaziabad U.P., India (1)
Role of mirror image therapy for phantom limb pain in below knee amputees
The pain caused by surgery is usually of a transient nature, however the perception of pain in an amputated limb often persists. This prolonged pain, which is often refractory to pain-killing medication, nerve block and surgical treatment may severely affect the patient’s quality of life. The phenomenon of phantom limb pain has been investigated using neurological, neurophysiological and psychopathological approaches. However exact cause of phantom limb pain is still a mystery. In this study we analysed the role of mirror therapy for treatment of phantom limb pain in below knee amputation.
To evaluate the role of mirror therapy in treating phantom limb pain in below knee amputees.
96 patients who had phantom limb pain after below knee amputation were included in this study. They had to visit the hospital four times a week for a 15-minute treatment period. In this technique they performed movement of unaffected limb while watching its mirror reflection and thus creating a visual illusion of movement of affected limb. The degree of pain relief was measured on visual analog scale (VAS).
70 patients out of 96 reported an improvement of 4 or more degrees of VAS score after 6 months of the treatment. The result was statistically significant.

Mirror therapy improves pain sensation of the amputated part when other treatment modalities fail. This therapy works on the principle of mirror neuron system. A mirror neuron fires either when a person acts or when a person observes same action performed by another. The mirror image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the removed body. This reorganization decreases the sense or emotion of phantom limb pain in the amputated part.
Kim SY, Kim YY. Mirror therapy for phantom limb pain. Korean J Pain. 2012 Oct; 25(4):272-4
0095
Silvia Raschke (1) presenting Johanne Mattie (1) Yvette Jones (1) David Kenyon (1) David Moe (2) David Sanderson (3) Angie Wong (1) Lorne Winder (2) Ana Moreno Hernandez (3) Michael Orendurff (4) Toshiki Kobayashi (4)
BCIT, Burnaby, Canada (1) Barber Prosthetics Clinic, Vancouver, Canada (2) UBC School of Kinesiology, Vancouver, Canada (3) Orthocare Innovations, Mountlake Terrace, USA (4)
Can YOU Tell Which Foot is Which?
The need for effective Functional Outcome Measures (FEMs) for prosthetic practice has become pressing, as fee payers are increasingly requiring evidence that prosthetic components actually provide a measurable impact on amputee quality of life1. In this context, both optimizing prosthetic foot choice for individual amputees and justifying the resulting prescription choices have become challenging due to the lack of objective performance data on prosthetic feet for the large number of feet available.
The aim was to use laboratory, community and preference measures to evaluate a range of prosthetic feet in different energy storage categories to determine if it was possible to differentiate between feet using a double blind design.
A pilot project identified functional measures with potential for prosthetic component evaluation and evaluated them in a single subject trial. From this a unique double-blind randomized controlled study design emerged which was tested on 12 amputees and compared 2 foot designs, grouped into 3 ‘stiffness/energy return’ categories, in addition to an amputee’s prescribed foot. Each amputee was evaluated on 4 to 6 blinded study feet using five measures: activity level, moment data, a modified PEQ questionnaire and self-report measures. 2 were chosen for each amputee for one week of community ambulation and activity level, modified PEQ and moment and force data were evaluated at the end of each week.
Results indicated that sagittal moments (P<0.011) and modified PEQ (P<0.025), were able to detect differences in foot design (Fig 1)

Comparing “Heel” moments between energy return categories (A, B & C).
The user preference results were consistent with the mechanical characteristics of the feet, with energy storing foot designs outperforming non-energy storing feet. Energy-storing feet that were more compliant were preferred to energy-storing feet that were stiffer. Furthermore, the moment data collected supported participant’s preferred foot choices, despite both amputees and researchers being blinded to foot design (Fig. 2)
This study offers evidence that prosthetic foot design has a quantifiable effect on amputee gait kinetics and preference during community ambulation. For the trans-tibial amputees measured, flexible energy storage return (ESR) feet produced lower peak moments during walking than non-energy storing feet did and were preferred by amputees. The clinical and economic importance of this double blinded study indicates it is possible to measure prosthetic component designs’ impact on amputee function and wellbeing.
0096
Hugh Watts (2) Sharon DeMuth (3) John Fisk (1) presenting
Retired, Saint Helena Island, SC, USA (1) Retired, Glendale, CA, USA (2) Retired, Glendale, CA, USA (3)
In 2010, Tajikistan experienced a large outbreak of Polio with 457 confirmed cases. This left a large number of people who have paralysis and will need a lifetime of care. The epidemic raises a number of issues about the larger question, can Polio be eradicated.
To survey the need for Polio care in Tajikistan, the level of clinical experience available and who could best benefit from Polio education?
In early 2014, WHO asked ISPO if an educational effort on the management of Poliomyelitis would help to further the WHO goal of capacity building in rehabilitation in Tajikistan? ISPO asked three former short course educators and the authors of this paper, all with extensive experience in caring for children with Polio, about providing a course. The team sought to identify the issues involved in the care of Polio in Tajikistan.
In March 2014, a team, funded by ISPO and WHO, traveled to Tajikistan. It was learned that there are no physical therapists, no certified orthotists and only 15 orthopaedic surgeons for a country of 7 million people. 360 children who had a confirmed diagnosis of Poliomyelitis in 2010 were evaluated. Of these, 193 children were noted to need lower extremity orthoses. Over the succeeding 5 months, 61 children were fitted with orthoses fabricated by non-certified orthotists in Dushanbe.
During a return visit in September some of the orthoses were evaluated and surgical mentoring was undertaken. Of the 24 children seen with orthoses, all were assessed as “inadequate”. It was learned that two physical therapists and two occupational therapists are being trained in India. Three orthotists are being trained in Viet Nam. The orthopaedic surgeons were inexperienced in polio care due to a Russian tradition of not operating on pediatric patients.
ISPO sponsored Short Courses are traditionally targeted to comprehensive health care teams and emphasize that approach to patient care. Where clinical resources are lacking courses can and should be modified. The need in Tajikistan is for education focused on teaching awareness of the role for rehabilitation in persons with Polio. Issues of Polio eradication remain. The numbers of health care professionals skilled in Polio care is on the decline at a time when Polio out breaks are occurring in many regions of the world. Eradicating Polio remains problematic.
0098
Jaap J. van Netten (1) presenting Jeff G. van Baal (1) Anke Kottink (1) Erik Manning (1) Arend Jan Woittiez (1) Max Spraul (2) Sicco A. Bus (1,3)
Ziekenhuisgroep Twente, Almelo, The Netherlands (1) Matias Spital, Rheine, Germany (2) Academic Medical Center, Amsterdam, The Netherlands (3)
The efficacy of removable devices to offload and heal neuropathic plantar forefoot ulcers in diabetes: a multicenter randomized controlled trial
Offloading is required to heal neuropathic plantar foot ulcers in diabetes. While guidelines recommend non-removable offloading, removable offloading is more commonly used, but little is known about its efficacy to offload the foot in combination with healing plantar foot ulcers.
To investigate the efficacy of three removable offloading devices (bivalved total contact cast, cast shoe, and a forefoot offloading shoe) on healing of neuropathic plantar forefoot ulcer in patients with diabetes.
We randomly assigned 60 diabetic patients with non-infected, non-ischemic neuropathic plantar forefoot ulcers to a bivalved total contact cast (BTCC), cast shoe (MABAL), or a forefoot offloading shoe (FOS). Patients were followed until healing or until 12 weeks (primary) and 20 weeks (secondary). Dynamic peak pressure at the ulcer site in the device and daily stride count were measured. Treatment adherence was assessed from patient reports.
According to intention-to-treat, 12-week healing percentages were 58% for BTCC, 60% for MABAL, and 70% for FOS (p = 0.70); 20-week healing percentages were 63%, 83%, and 80%, respectively (p = 0.31). Mean ± SD peak pressure in kPa at the ulcer site was 81 ± 55 for BTCC, 176 ± 80 for MABAL, and 107 ± 52 for FOS (p = 0.005); mean ± SD daily stride count was 4150 ± 1626, 3514 ± 1380, and 4447 ± 3190, respectively (p = 0.71). Percentage of two-week intervals that patients wore the device <50% of time was 17.3% for BTCC, 5.2% for MABAL, and 4.9% for FOS.
Clinical efficacy was not significantly different between removable devices and was lower than previously found for non-removable offloading. Exposure to repetitive stress by lack of forced adherence and high daily stride count, stresses the importance of continuous pressure relief in healing neuropathic plantar foot ulcers in diabetes.
101
Koh Inoue (1) presenting Ryuichi Harada (1) Takahiro Wada (2) Keisuke Suzuki (1) Shin’ichi Tachiwana (1)
Kagawa University, Takamatsu, Japan (1) Ritsumeikan University, Shiga, Japan (2)
A Novel Transfemoral Prosthesis Knee Joint Unit with a Completely Passive Mechanism Allows Amputees to Ascend Stairs
Stair ascent remains a demanding task for transfemoral prosthesis users [1], although many transfemoral prosthesis knee joint units have been developed to expand their gait capacity. Recently, several computerized and motorized knee joint units have allowed amputees to ascend stairs, although cost, maintenance, and the usage environment remain significant concerns. Therefore, a passive mechanism could effectively solve these issues. The existing passive knee can prevent unintended knee flexion, although they cannot support knee extension during the prosthetic stance phase, which is an essential motion for stair ascent.
1) To develop a passive mechanism for the knee joint unit of a transfemoral prosthesis to facilitate stair ascent and 2) to evaluate the stair ascent motion using the proposed passive mechanism.
The new passive mechanism was designed to extend the prosthetic knee using the ground reaction forces or the load on the prosthesis during the stance phase. A unilateral transfemoral amputee who had received the proposed knee joint unit participated in a stair ascent experiment, and was asked to ascend the stairs in a step-by-step manner at a rate of 50 steps/min. The motion during the stair ascent and the ground reaction forces were recorded using a motion capture system and force plates. Data for 3 repetitions were collected, and a rigid body link-segment model and inverse dynamics were used to calculate the joint moments.
The participant succeeded in ascending the stairs in a step-by-step manner. The stance time was 1.62 ± 0.05 s for the intact leg and 1.45 ± 0.10 s for the prosthetic. During the prosthetic stance phase, the peak ground reaction force on the prosthetic side was 102.4 ± 4.8 %BW (body weight), and the prosthetic knee was extended by 48.0 ± 3.9 degrees. The peak values of the hip extension moment and positive power for the prosthetic side were 1.47 ± 0.19 Nm/kg and 2.80 ± 1.08 W/kg, respectively. The net work for the hip moment was 0.66 ± 0.25 J/kg.
The prosthetic knee extension and ground reaction force results suggest that the proposed mechanism functioned appropriately. The positive work at the prosthetic-side hip joint (greater than able-bodied subjects) could compensate for the lack of energy generation by the passive mechanism. Furthermore, the hip extension moment and power generation at the prosthetic side would induce the relatively symmetric leg motion between the prosthetic and intact sides indicated by the stance time. In conclusion, the proposed passive knee joint unit allowed a transfemoral amputee to ascend stairs in a step-by-step manner, and an example of the prosthetic-side hip joint kinetics to use the proposed mechanism for stair ascent was shown.
[1] B.J. Hafner, et al. 2007. Arch Phys Med Rehabil.
102
Igor Shvedovchenko (1) Andrei Koltsov (1) Veronika Yakovleva (1) presenting
Federal State Institution St.Petersburg Scientific and Practical Centre of Medical and Social Expertise, Prosthetics and Rehabilitation named after G.A.Albrecht of the Ministry of Labour and Social Pr, St-Petersburg, Russia (1)
Habilitation of patients with proximal Femoral Focal Deficiency
Congenital aplasia and hypoplasia of the proximal femur occur approximately 1 in 500000 cases of birth and is a major problem for the orthopedic world due to the severity of disease, its relative scarcity and the need for a comprehensive habilitation.
The purpose of this work is the analysis of the characteristics and results of the prosthetics and surgical treatment in the habilitation of patient with PFFD.
124 patients at the age from 8 months to 45 years were analyzed for the period since 1970 to 2014 years. According to the classification of G.T. Aitken(1969) the type A was observed in 34%, B-20%, C -19%, D -27% of cases. When used classification of A.M. Pappas (1983) the most frequent classes of lesions were P4, P2(34%, 27%), P1,P3 and P5 occurred not so often. The atypical prosthetics of femur was conducted in 100% cases, primarily in the earliest possible age. The surgical treatment in most of cases was preparatory stage for the prosthetics and was aimed at stabilization of the lower extremity and the improvement of it’s support; the correction of the deformation of the extremity in order to provide the opportunity of more functional prosthetics.
The efficiency of prosthesises usage and the speed of prosthesis mastering directly depended on the age of primary prosthetics and the regularty of following stages. The stabilization of lower extremity at the junction with the pelvis carried out by method of iliofemoral synostosis. The correction of the external rotation implemented by methods of derotation osteotomy of femur. These operations were indicated with C and D classes of lesion according to Aitken(P2, P3 and P4). The reconstaction of the extremity in order to provide the opportunity of more functional prosthetics consisted of rotary plastic by Van Nes and was carried out in patients with monolateral lesion, the C and D classes of hypoplasia of femur according to Aitken provided the preservation of both legs bones and 4 or 5-dactyl foot (P4).
Proximal ectromelia is a rare and severe form of hypoplasia of lower limbs, which requires an individual approach and a comprehensive habilitation starting in the first year of life;
Atypical prosthesis is the main method of habilitation of patients with severe reduction;
Surgical treatment is an important aspect of the treatment of the patients and in most cases is a preparatory stage for prosthesis.
103
Steven Gard (1,2) presenting Antonia Nepomuceno (3) Matthew Major (1,2)
Northwestern University, Chicago, IL, USA (1) Jesse Brown VA Medical Center, Chicago, IL, USA (2) University of Illinois, Urbana-Champaign, IL, USA (3)
Effect of Ankle Immobilization on Able-Bodied Gait as a Model for Understanding Bilateral Amputee Gait
A critical function of the foot-ankle complex during walking is to facilitate advancement of the stance limb through heel, ankle, and forefoot rockers and generation of power during pre-swing [1]. These features are diminished for bilateral transtibial amputees (BTAs) when using passive foot-ankle components and they must rely on compensatory mechanisms to advance the lower limbs and maintain forward ambulation [2, 3].
The purpose of this study was to determine the effects of ankle immobilization on able-bodied (AB) gait to serve as a model for understanding BTA gait and associated compensatory mechanisms.
Subjects: Nine AB (27.1±2.9 yrs, 1.75 m, 75.5 kg) were included in this study. Additionally, data from ten BTA prosthesis users (50±18 yrs, 1.73±0.08 m, 82±16 kg) in a previous study [2], were included for comparison.
Apparatus: Gait kinematics were measured with an eight-camera digital motion analysis system and ground reaction force data were collected with six force plates embedded in the walkway.
Procedure: Each subject was recorded walking at freely-selected walking speeds, without (control) and with casts, respectively. The bilateral casts were fitted below the knee joint to the toes with the ankle joints in a neutral position to prevent ankle joint motion.
No difference in walking speed was observed between the cast (1.4±0.3 m/s) and no cast (1.34±0.1 m/s) conditions. Ankle range of motion (ROM) was greatly reduced in the cast condition, from 31.1±3.3 degrees to 8.4±3.0 degrees. A four-fold decrease in ankle power generation occurred at pre-swing in the cast condition compared to control. Trunk lateral flexion ROM, trunk transverse rotation ROM and peak hip power generation during pre-swing increased in the cast condition compared to control.
Ankle joint immobilization resulted in a substantial decrease in ankle power generation during pre-swing, which may have been compensated for by increased hip power to achieve limb advancement. The modifications in trunk movement may also act as compensatory mechanisms to maintain forward ambulation. The hip and trunk compensations observed in the cast condition appear to resemble gait patterns of BTAs.
[1] Perry J. Gait Analysis: Normal and Pathological Function, 1992.
[2] Major M. et al. J. Gait Posture 38, 858-863, 2013.
[3] Su P.F. et al. J Rehab Res Dev, 44, 491-501, 2007.
104
Erin Boutwell (1,2) presenting Rebecca Stine (1,2) Steven Gard (1,2)
Northwestern University Prosthetics-Orthotics Center, Chicago, IL, USA (1) Jesse Brown VA Medical Center, Chicago, IL, USA (2)
Effect of Longitudinal Prosthesis Stiffness on Force Transmission during Transtibial Amputee Gait
Shock-absorbing prosthetic components are typically characterized by reduced longitudinal stiffness and are designed to protect users from impact forces that arise during walking. However, their ability to provide appropriate shock attenuation has not been discerned in previous gait analyses [1-3]. These studies have often compared a shock-absorbing component (in its default configuration) to a more traditional/rigid component, with little reported difference in force transmission. Yet, it is unknown whether introducing lower prosthetic stiffness may yield the anticipated benefits in shock absorption
To perform a systematic variation of prosthesis stiffness over a wider range of stiffness values than previously tested, and to investigate the effect on force transmission during transtibial amputee gait.
12 subjects with unilateral transtibial amputations participated in this study. Gait data were acquired using a motion capture system (MAC, Santa Rosa, CA) and force platforms (AMTI, Watertown, MA). Subjects wore their current socket and suspension system, and were provided with an experimental prosthesis consisting of a shock-absorbing pylon (SAP) (Endolite TT Pro, Miamisburg, OH) and a standardized prosthetic foot and shoe. Longitudinal stiffness was varied by substituting the spring within the SAP. A NORMAL (manufacturer-recommended), a SOFT (50% NORMAL) and a MEDIUM (75% NORMAL) stiffness as well as a RIGID pylon were tested for each subject. Gait analyses were performed at freely-selected and fast self-selected walking speeds.
Ground reaction force (GRF) loading peaks and timings were not substantially different across stiffness conditions for the freely selected walking speed (Figure 1). During fast walking, a small increase in GRF loading peak was found in the SOFT vs. NORMAL condition (p = 0.021), as well as a slight decrease in time to peak in the RIGID vs. SOFT & MEDIUM conditions (p ≤ 0.004).

Representative GRF profile for a single subject (freely-selected walking) for all stiffness conditions. No difference
For fast walking, the two significant findings were contradictory: decreased stiffness yielded a longer time to peak force, but a higher peak force. When combined with the lack of meaningful differences from freely-selected walking, we conclude that longitudinal stiffness does not produce altered force transmission during gait. These results may be explained by active compensation of the user, or an insuffient understanding of how to influence the stiffness and loading properties of the prosthetic-side limb system.
[1] Berge, J. 2005. J Rehabil Res Dev.
[2] Gard, S. 2003. J Rehabil Res Dev.
[3] Miller, L. 1997. J Rehabil Res Dev.
105
Shuhei Iida (1) presenting Chikara Aoki (1)
Teikyo Heisei University, Tokyo, Japan (1)
Comparing the surface cerebral-blood-flow changes of the use and disuse of the Ankle foot orthosis(AFO)
There are a lot of reports of kinematics, engineering, gait analysis and so on about ankle foot orthosis(AFO). However, there are few reports of the neurological side such as connection with the abnormal muscle tonus.
The aim is to compare the surface cerebral-blood-flow changes of the use and disuse of the AFO in stroke patients with hemiplegia.
The measure of the surface cerebral-blood-flow were performed by functional Near infrared spectroscopy (fNIRS) machine. Area of analysis was motor area of frontal lobe(channel 14-39,42,43). Subjects were 8 outpatients of putaminal hemorrhage with hemiplegia,and selected similar case of the bleeding part, hemiplegia, sensory disfunction and walking ability. Task1 is walking with the AFO and Task2 is walking without the AFO, each task was performed on the treadmill for 30 seconds for 3 sets. Wilcoxon signed-rank test was used to compare the relative amount of change of oxygenicity hemoglobin in blood between Task1 and Task2.
Each surface cerebral activity of task1 and task2 was shown in Figure 1. And when the two were compared, walking without the AFO significantly increased oxygenated hemoglobin in the next area; the inside primary motor area,the outside primary motor area of the lesion side, the premotor area of the non-lesion side, the premotor area of the lesion side, and the supplementary motor area of both sides.

It was confirmed that the activity of the motor area of frontal lobe was limited by using the AFO. the premotor area and the supplementary motor area work in the adjustment of movement. It was considered that the difference of gait, sensory-input, fear and so on without AFO influenced the adjustment of movement.
Miyai I.,et al. : Longitudinal optical imaging study for locomotor recovery after stroke. Stroke., 34 : 2866-2870, 2003
106
Veronika Noll (1) presenting Janis Wojtusch (2) Jochen Schuy (1) Martin Grimmer (3) Stephan Rinderknecht (1)
Institute for Mechatronic Systems in Mechanical Engineering, TU Darmstadt, Darmstadt, Germany (1) Simulation, Systems Optimization and Robotics Group, TU Darmstadt, Darmstadt, Germany (2) Locomotion Laboratory, TU Darmstadt, Darmstadt, Germany (3)
Measuring Interaction at the Stump-Socket Interface of a Transtibial Amputee during Straight Level Walking
The amputee’s well-being and mobility are determined by the socket fit and consequent stump-socket interaction. Since the rectification process is mainly based on examining the stump in a seated position, the successful fitting mostly depends on the ability and experience of the orthopedic technician. There is little quantitative knowledge about the interaction of the stump-socket interface during gait. Its behavior can be characterized by the applied load as well as the movement of the stump within the socket.
The aim of the presented study is to show the feasibility of measuring the relative movement between stump and socket during gait and allocating it to the coinciding loads.
With consent of the TU Darmstadt ethics commission, experimental trials of a transtibial amputee (50 yrs, 95 kg, PTB socket) walking on a treadmill with constant self-selected walking speed are conducted. Depending on the walking speed, approximately 50 strides are recorded. To measure the loads at the distal end of the socket, a measurement adapter [1] which can be integrated into the prosthetic structure is used. Subject movement and relative motions at the stump-socket interface is recorded using motion capturing technique. The latter one is defined by the relative movement between markers placed on the stump and on the test socket itself.
To the best of the authors’ knowledge this is the first time that measurements of relative movement between stump and socket during gait is presented with the coinciding loads. The displayed figure shows mean and standard deviation of the measured load in the proximal-distal axis (top) with the corresponding relative movement between stump and socket (bottom) during stance phase at a walking speed of 0.85 m/s. As indicated by the similarity of the two graphs, the normalized zero lag cross correlation of the signals is given by -0.96. The noted deviation is mainly caused by the end of stance phase (cf. figure). Without applied load, the calculated relative movement does not return to zero.

While this is the first attempt to measure the biomechanical interaction during gait, the gained insights show that usage and interpretation of motion tracking for the determination of relative movement between stump and socket entail sources of nonconformance. Tensing muscles alter the stump’s structure, consequently influencing the marker’s position on the skin. Thus complementing the measurements with the detection of EMG signals might be an option for further studies.
[1] Schuy, J. and Rinderknecht, S.: Integrated Measurement System for Amputee Gait Analysis: A Pilot Study. In: IEEE EMBC- Healthcare Innovations & Point-of-Care Technologies, 8 – 10 October 2014, Seattle, USA.
107
Nicole Bennett (2,1) presenting Hannah Jarvis (3,1) Lt Col Rhodri Phillip (1)
Defence Medical Rehabilitation Centre Headley Court, Surrey, UK (1) Blatchford Clinical Services, Sheffield, UK (2) The University of Salford, Manchester, UK (3)
Can an Ankle Foot Orthoses be designed to reduce pain and significantly improve function in the UK military limb salvage population?
Recent UK Military operations have resulted in many personnel suffering severe injury from improvised explosive devices (IED). Advances in medical care and body armour design have allowed limbs to be salvaged that would have once faced immediate amputation. Personnel who have their limbs salvaged following blast injuries are associated with poor clinical outcomes. Many seek amputation on average 18 months post injury to improve pain and increase functional ability. In October 2013 DMRC Headley Court began provision of the British Off- loading Brace (B.O.B), a custom composite material ankle foot orthoses which strives through its design to reduce pain, and improve gait and functional ability. This design of ankle foot orthoses was first reported by the US military in 2011.
To compare the biomechanical function and functional outcomes of limb salvage patient’s pre and post-provision of the BOB.
Six military personnel who have undergone limb salvage resulting from unilateral foot and ankle blast injuries participated. All participants completed functional outcome measures and gait analysis pre and post-provision of the BOB. Participants were instructed to walk at a self-selected speed, with temporal and spatial parameters and three dimensional gait measurements were obtained with joint kinematics, moments and power calculated.
All six participants demonstrated an increased walking speed and stride length when using the B.O.B. On walking speed increased by 22% and stride length increased by 12.5%. Participants were able to generate greater power through their lower limb joints when wearing the BOB (Figure 1). Whilst wearing the B.O.B on the injured limb the ankle joint power reduced due to the solid ankle design.

When using the BOB, pain reduced by 18%, symptoms improved by 15%. Functional daily living and quality of life indicators improved by 12 % and 31% respectfully. The ability to participate in sport improved by 44%.
Our pilot study indicates that the B.O.B reduced pain, improved symptoms and increased functional ability in this limb salvage population. The reduction in pain, improved stability and energy return late stance allowed for servicemen to walk faster and generate greater power through both limbs. Most notably all can run without pain when using the B.O.B and cannot without it. Further data collection and analysis is ongoing.
108
Hirotaka Tanaka (1) presenting Keiichi Nakamura (1) Kyohei Kawamura (1) Mina Tomonaga (1) Kanan Yatsuya (1) Masayuki Mizote (2) Mituru Hayashi (2) Yoshiki Matsumoto (2)
Chubu Rosai Hospital, Nagoya, Japan (1) Matsumoto Prosthetics & Orthotics Manufacturing CO., LTD, nagoya, Japan (2)
Relationship between myoelectric hand mounting and QOL in adult upper limb amputees
Workers’ compensation insurance has classified myoelectric hands as formal prosthetics since 2013 in Japan. The costs associated with myoelectric hands are substantial. After a patient receives a myoelectric hand, it is economical to determine which patients use the myoelectric hand continuously. In recent years, health-related Quality Of Life (QOL) metrics have been used to evaluate numerous pathologies. SF-36 is the most famous health-related QOL survey and has been used for amputee patients in Japan.
We assessed the SF36 survey results for patients with myoelectric hands, and examined the relationship scores for each item of the survey as it related to use of the myoelectric hand.
We included 22 upper limb amputees who had been prescribed myoelectric hands in this study. The status of use (or non-use) of the hand was determined by telephone or face-to-face interview. We examined health-related QOL metrics, using the SF-36v2 before, and at the end of myoelectric hand training, and again after 6 months, 2 years, and 3 years. The results were calculated based on national standard values and each subscale was converted to a Z-value. Subscales were compared at each survey instance and over the entire study period by two-way analysis of variance. Each subscale was compared by T-test in the use group and the non-use group.
Analysis of variance of the eight subscales showed that before training, Role physical (RP) 40.6 < General health (GH) 54.0 (P <0.001), Social functioning (SF) 44.3 <GH 54.0 (P = 0.028), RP 40.6 < Vitality (VT) 51.5 (P = 0.04). Immediately following training, RP 43.9 <VT 53.8 (P = 0.02), RP 43.9 <GH 57.5 (P <0.001), RP43.9 < Mental health (MH) 54.4 (P = 0.007). Comparing the use group and non-use group before myoelectric hand training, VT value was 54 (use group) vs 46.6 (non-use group) (P = 0.092). Immediately following training, Bodily pain (BP) value was 51.8 (use group) vs 44.1 (non-use group) (P = 0.098), VT value (use group) was 56.0 vs 50.2 (non-use group) (P = 0.149), MH value was 56.6 (use group) vs 49.1 (non-use group) (P = 0.178), and after 6 months the BP value was 50.0 (use group) vs 40.7 (non-use group) (P = 0.057), VT value was 54.8 (use group) vs 44.1 (non-use group) (P = 0.01), MH value was 54.1 (use group) vs 46.5 (non-use group) (P = 0.086).
Reviewing the survey results showed that the value of physical and social items tended to be lower before patients had completed myoelectric hand training, but improvement was seen over time. For patients who could not continue use of the myoelectric hand, the value of some of the SF36 items is low.
109
Yoshie Nakanishi (1) presenting Hideo Nagata (1)
Yaskawa Electric Corporation, Kitakyushu, Japan (1)
Development of a robotic ankle-assist walking device for use in gait exercises
Stroke-related gait disturbances are devastating disabilities. Their alleviation is therefore a major component of post-stroke rehabilitation. However, even after rehabilitative intervention, many patients continue to suffer from ankle joint disorders. Additionally, during gait exercise, the direct manual approach for the ankle joint is technically difficult. Ankle foot orthoses (AFOs) are often prescribed to fix the constant angle of the joint, but may induce asymmetry, followed by gait compensation, resulting in secondary damage such as lower back or knee pain.
We developed an ankle-assist walking device that enables a direct approach for ankle movement during rehabilitative gait exercises. The study investigated the function, durability, and subjective/objective usability of the device.
We developed a device comprising a controller unit, an AFO with motor, pressure sensors on the insole, and a shoe for the unaffected side. A tablet was used to set the ankle joint angle and the gait speed. The controller recognizes the beginning of the stance or swing phase based on information from the pressure sensors in the heel and forefoot. According to this information, the controller drives a motor to move the pre-set angle. This feasibility study involved 3 healthy subjects (2 male and 1female).
The battery remained functional for more than 1.5 h. Several minutes were required to wear and remove the AFO, controller unit, as well as to adjust the parameters for each subject. The 3 subjects were satisfied with the functionality and usability of the device. Each subject experienced that his/ her weight shifted forward smoothly by dorsiflexion during the stance phase, and his/ her toe lifted appropriately during the swing phase.

The advantages of the device are its simple components. It is easy to wear and remove and is simple to use, with sufficient battery life to be used for gait training for a few consecutive patients. The device has characteristics appropriate for clinical use, and has potential for enhancing gait learning during the early phase of rehabilitation for post-stroke patients; clinical research is planned to begin soon.
111
Navid Monzavizadeh (1) Maryam Maleki (1) presenting Atefeh Aboutorabi (1) Reza Vahab Kashani (1)
University of social welfare and rehabilitation sciences, Tehran, Iran (1)
The influence of Erigo therapy on secondary complications after neurological disorders: A literature review
Patient with severe neurological disorders like spinal cord injury, stroke and Traumatic brain injury are often bedridden for a long time and this may cause many complications, such as the instability of the cardio-pulmonary system, bed sores and other negative physiological and biochemical changes in all organs and systems of the body. Therefore, to overcome some of these secondary complications a safe mobilization and intensive sensorimotor stimulation should performed right after the injury. To offer patients a locomotion therapy a novel, robotic tilt-table (“Erigo”) developed in 1998 that allows passive stepping movements and simultaneous verticalization of the patients.
The aim of this review was to investigate the effect of Erigo on secondary therapy disorders in neurological dysfunction.
According to the PICO methods and based on selected key words, 13 studies chosen and met the inclusion criteria
The results of the analysis demonstrated that an early activation and stimulation of the patient with neurological disorders by means of Erigo therapy improves the secondary complications after these types of injuries such as loss of muscle mass and strength, negative changes in blood conditions, urinary complications, nutritional problems and other side effects like sensory deprivation, isolation and confinement. Also patient that trained with Erigo tolerates the upright position better than patients treated on conventional tilt tables without a stepping function and cyclic leg loading.
Most of the literatures are demonstrated that Erigo therapy in the patient with neurological dysfunction ensures the optimum utilization of the neuroplasticity and recovery potential. Furthermore, it improves the patient’s communication skills and counteracts secondary damage from immobilization. And generally the advantages of early rehabilitation with the Erigo therapy are early and safe mobilization, enhanced cardiovascular output by cyclic leg loading, increased patient’s awareness and, reduced time in acute care. In summary Erigo therapy is safe and suitable to decrease the secondary complications following neurological disorders.
1. Kuznetsov, Alexey N., et al. “Early Poststroke Rehabilitation Using a Robotic Tilt-Table Stepper and Functional Electrical Stimulation.” Stroke research and treatment 2013 (2013).
112
AMIT SARAF (1) presenting
Saraswati institute of medical sciences, ghaziabad U.P., India (1)
Lipid profile in Rheumatoid Arthritis patients and its relation to disease activity
Cardiovascular morbidity and mortality are enhanced in Rheumatoid Arthritis (RA), which may be attributable to dyslipidemia. The dyslipidemia observed in RA appears to be dependent on disease activity, but only a few studies in the world literature are there, providing definite correlation and mechanisms. In this study we prospectively assessed the correlation of lipid profile with the disease activity.
A total of 60 patients who fulfilled the “Revised Criteria for the Classification of Rheumatoid Arthritis 1987” were included in this study. The patients who satisfied at least 4 out of 7 criteria were included in the study. The serum was collected from rheumatoid arthritis patients for the determination of lipid values which are triglycerides (TG), total cholesterol (TC), high density lipoprotein (HDL), low density lipoprotein (LDL). Disease activity was assessed by using DAS 28 ESR score. Disease activity was then correlated to the lipid profile of the patients using co-efficient of correlation.
Out of 60 patients, 42 (70%) patients had very active disease activity at the time of presentation. 16 (26.7%) patients had moderately active and 2 (3.3%) had inactive disease. Patients with very active disease were found to have low levels of LDL, HDL and TC as compared to patients with inactive disease. However the reduction in HDL levels was significantly higher than TC levels. Levels of TG were found to be higher in patients with very active disease.

By causing greater reductions in HDL, RA does increases cardiovascular mortality and morbidity. In patients with RA it is more important to measure both total cholesterol and HDL and to use their ratio for the calculation of absolute cardiovascular disease risk. HDL, LDL, TC can be used as corroborating markers of disease activity in RA.
Wells G et al. Validation of the 28-joint Disease activity score (DAS28) and European League Against Rheumatism response criteria based on C-reactive protein against disease progression in patients with rheumatoid arthritis, and comparison with the DAS28 based on erythrocyte sedimentation rate . Ann Rheum Dis : 2009 ; 68 : 954–960.
113
AMIT SARAF (1) presenting
Saraswati institute of medical sciences, ghaziabad U.P., India (1)
Importance of tying the sciatic nerve in above knee amputation to prevent neuroma formation
Sciatic nerve is the thickest nerve in human body. Neural sheath of sciatic nerve is rich in microvasculature. In this study we compared neuroma formation after tying the sciatic nerve with leaving its cut end open in patients who undergo above knee amputation.
In this study we followed a total of 90 patients who underwent above knee amputation. In half of these patients, cut end of sciatic nerve was left open and in other half, the nerve was tied. Patients in both the groups were age, sex and BMI matched. Neuroma formation in the stump was assessed one year after surgery. This assessment was done by measuring the diameter of sciatic nerve ending using sonogram. Sciatic nerve diameter was measured bilaterally at the same level, and the value of the normal limb was taken as control.
Out of 45 patients who underwent tying of sciatic nerve, only 10 patients developed thickening of the cut end of sciatic nerve in comparison to opposite limb. On the other hand, 45 patients in whom the cut end was left open, 33 patients developed neuroma formation. This result was statistically significant.

Rich microvascularity of sciatic nerve results in the formation of haematoma beneath the cut end, if it is left open. This haematoma eventually results in growth of neural fibres. As a result of this, neuroma formation occurs at cut end of sciatic nerve in above knee amputation. We thus conclude, it is always wise to tie the cut end of sciatic nerve in above knee amputation to prevent neuroma formation.
Göktepe AS, Ozçakar L, Kömürcü E, Safaz I, Yazicioğlu K. Sonographic evaluation of the sciatic nerve in patients with lower-limb amputations. Muscle Nerve. 2010 Jun;41(6):763-6.
114
Fatma Mohsin (1) presenting Anthony McGarry (1) Roy Bowers (1)
University of Strathclyde, Glasgow, UK (1)
The reliability of a video analysis system (SiliconcoachTM) and the universal goniometer in the measurement of hip, knee and ankle motion
Throughout the patient assessment process, adequate recording of joint range of motion (ROM) is essential to facilitate and evaluate the most appropriate treatment. The universal goniometer (UG) is the most common and inexpensive tool used in clinical settings to record ROM. However, a review of the literature examining the reliability of the UG demonstrated considerable variation in results hence, the necessity of introducing a more reliable measuring tool.
To investigate the intratester reliability and intertester reliability of the SiliconcoachTM video analysis system compared to the UG in measuring passive ROM of the lower limb joints amongst supine healthy candidates.
Three testers and eight healthy candidates were included in this study. Sagittal plane motion of the hip joint, knee joint and ankle joint of the dominant leg was measured with and without markers. Each tester repeated each measurement three times using each tool to calculate intratester reliability. Intraclass correlation coefficient (ICC) and Bland-Altman plot (difference plot) were used to calculate the reliability. ICC values above 0.60 were considered to be satisfactory for research purposes. Intertester ICC values were only able to be calculated if intratester ICC values across all the testers were above the satisfactory level (ICC>0.6).
ICC values across all the testers for all motions

Most of the intratester ICC values for SiliconcoachTM were found to be above the satisfactory limit. Intratester ICC values for UG ranged considerably, with some values below the satisfactory limits. Intertester ICC values could only be calculated across all joints for SiliconcoachTM with markers and were found to be above the satisfactory limits. In conclusion, SiliconcoachTM was found to be more reliable than UG. Additionally, use of makers was found to increase the reliability of SiliconcoachTM.
118
Rodrick Shangali (1) presenting Harold Shangali (1) Wilfred Raab (1) Elias Elias (1) Bashiri Majaja (1)
TATCOT, Moshi, Kilimanjaro, Tanzania (1)
Design and Manufacture of a Wheelchair Tricyle Attachment for Peoples in Developing Countries
Most of the wheelchairs being used in Tanzania are imported and do not satisfy the fitting to pathological and environmental (i.e. indoor and outdoor) conditions. The present designs available in the market do not provide optimal qualities required for internal and external wheelchair use. Developing a wheelchair tricycle attachment will provide an effective means of a common wheelchair which is appropriate to the given environmental conditions for a person with lower limb problems.
The main objective of this project was to develop a wheelchair tricycle attachment to provide or enable the easier accessibility and improves performance (Dar-es-Salaam and Kilimanjaro regions (Tanzania)).
A literature review, survey, information analysis, observations, manufacturing, design testing, evaluation and interviews were carried out. Different concepts were generated (conceptual design) and the best was selected followed by embodiment design and detail design to meet the objective of study. The evaluation and ranking of the concepts using Rating and Weighting Matrix Method was through the following criteria; i.e. Easy to manufacture, low production cost, reasonable product price, easy to operate, simple design, efficiency, ergonomics, aesthetics and weight. Detail and assembly drawings of various components and manufacturing were carried out at Tanzania Training Centre for Orthopaedic Technologist (TATCOT).
The results of the majority wheelchair and tricycle users became disabled early in life due to a birth defect, polio or car accidents and most (66%) had to resort to crawling as a means of mobility. As a result, tricycles were observed to be more popular than wheelchairs among the users. Finally we were able to manufacture five units. From these units we were able to test on 5 wheelchair users tested as shown on Figure.1 with the consideration of Operating efficiency, Conformance to standards, Torque transmitted, Power transmitted and Conformance to ergonomics requirements.

Final wheelchair tricycle attachment and testing by the user
The wheelchair tricycle attachment was designed, manufactured and tested. The physical capability of the user to use the wheelchair tricycle attachment is important in allowing him/her to attach/detach the device as well as how to propel it.
1. Pugh, S. 1991. Integrated Methods for Successful Product Engineering, Addison-Wesley Publishing Company. pg 32-50.
2. Winter, G. 2005. Assessment of Wheelchair Technology in Tanzania, Cambridge.pg 10-30
3. Cornick, P. 2002.Wheelchair Technology Manual, UK, Motivation. pg 10-15
119
SIRIRAT SENG-IAD (1) presenting SASITHON SUKTHOMYA (1) PORNCHANOK POBUNDIT (1) ITTIPOL PONGPHANRUAM (1) NISARAT OPARTKIATTIKUL (1)
Sirindhorn School of Prosthetics and Orthotics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand (1)
Students’ expectation in prosthetics and orthotics education program: Sirindhorn School of Prosthetics and Orthotics, Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand
To understand students’ expectations of prosthetics and orthotics (P&O) education program is one of the priorities for Sirindhorn School of Prosthetics and Orthotics (SSPO), Mahidol University Thailand. Students’ expectations are a valuable and constructive source of information. The knowledge of student expectations can help the lecturers to design of teaching programs and the education organization to sustain the quality of the educational and supportive service.
The purpose of this study was to explore the educational and professional expectation of the P&O undergraduate students of Sirindhorn School of Prosthetics and Orthotics, Thailand.
During the first month of academic year 2013-2014 and 2014-2015, the P&O undergraduate students of Sirindhorn School of Prosthetics and Orthotics, Mahidol University, were requested to indicate, on a self-complete questionnaire, how important they consider each of the factors to be in determining their expectation of the P&O education service they are receiving at the university. The questionnaire composed of 21-item questions on a Likert type scale and one opened-end question. Items were based on expectations of lecturer and teaching methods, instructional media, service and supporting system, and after-graduation concerns. Perceived importance was used as a vital indicator of expectations.
Data collection was done in two consecutive academic years. A convenient sample of 85 (77%) and 93 (85%) freshman, sophomore, junior, and senior P&O undergraduate students in academic year 2013-2014 and 2014-2015, respectively, enrolled in this study. The findings indicate that students want lecturers to be knowledgeable, attentive, enthusiastic, and approachable. Students expect for the instruction media and library service to support the learning needs. Students predominately want to gain P&O knowledge and experiences to be able to pass examinations and to be prepared for their profession. This study also shows that students’ expectation to be able to participate and be acknowledged in the multidisciplinary rehabilitation team. The comparison of expectation among those four groups of students was analyzed. Some educational and professional concerns were raised from students.
The findings suggest that student expectations in general P&O education and supportive services are relatively similar in all level of student and stable over time. The study also indicates that lecturers should acquire the desired attributes for knowledge and experience transfer. The approach of teaching for each level of student should be taken into consideration by reflecting the expectations, needs and values of students. Other aspects were also discussed.
120
Mitsunori Toda (1) presenting Takaaki Chin (1) Hideshi Kohno (1) Yaeko Shibata (1) Futoshi Mizobe (1) Yuji Hamamoto (2) Akito Masuda (2)
Hyogo Rehabilitation Center, Kobe, Japan (1) KINKI P&O Cooperation, Kobe, Japan (2)
Use of Powered Prosthesis for Children with Upper Limb Deficiency at the Hyogo Rehabilitation Center
In the 1980’s research papers were issued reporting on the effectiveness of the application of powered prosthesis for young children in Canada and Sweden. Progress in prosthetic limb technology has enabled the miniaturization of powered prostheses, leading to wider use by children with upper limb deficiency in the U.S., Europe, and other regions. However, there has been no research investigating the use of powered prosthesis for children in Japan.
To gain better insight into the state of powered prosthesis usage and identify a ratio of rejection among children.
Subjects were 37 unilateral amputees between the ages of 0 and 16 at the time of their first experienced fitting with a powered prosthesis at our Center. 15 children had transradial amputations, seven had wrist disarticulations, 13 had transcarpal amputations and two had ulnar deficiencies. Information was collected regarding ages and when children started to use their powered prosthesis, the state of continued powered prosthesis usage, reasons for discontinuing the use of their powered prosthesis and the rate of discontinuation.
Table 1 shows the levels of amputation, ages when initially fitted with a powered prosthesis and ages for both groups (users and non-users), and when non-users discontinued to use it. There were 29 children in the users group, and were eight in the non-users group. The rate of discontinuation was 21.6%. Seven of eight children discontinued usage because they found it unnecessary. The age of non-users were significantly older compared with users at the time of their first fitting. The level of amputation had no influence on the use of a powered prosthesis.
Level of deficiency in subjects, ages at initial prosthesis fitting and ages when discontinuing the prosthesis

Children with upper limb deficiency could skillfully use a powered prosthesis even if they started to use it when they were two years old or older. We should sternly abstain from judging the issue of powered prosthesis adaptation by children solely based on their age at the time of the initial fitting, because such an approach might cause them to unfortunately lose an opportunity to use prosthesis.
122
Philip Davenport (1) presenting Siamak Noroozi (1) Philip Sewell (1) Saeed Zahedi (2)
Bournemouth University, Poole, Dorset, UK (1) Chas A Blatchford and Sons Ltd., Basingstoke, Hampshire, UK (2)
A proposed system for automatic categorisation of lower-limb prosthesis alignment using Learning Vector Quantisation and an inverse problem pressure measurement approach
Current methods for evaluating the set-up of lower-limb prostheses are limited by their inability to provide information on optimal socket fit and device alignment to the prosthetist and user as they rely substantially on clinical experience [1]. A non-invasive method for evaluating pressure distribution based on artificial neural networks has been reported [2]. An extension of this system to enable alignment classification is described.
To develop a system capable of mapping socket pressure distribution using external sensors and characterising these results in terms of changes in socket/pylon alignment.
Strain gauges on the external surface of the socket are used as inputs to a neural network. After training with known loads, an estimate of the unknown distribution in the clinical case is made. It is hypothesised that changes in pressure distribution with different alignments will be separable. Literature on automatic classification of gait data was reviewed for techniques suitable for this application. In particular, time series data must be reduced to represent the gait cycles concisely. As data can be collected at different known alignments, supervised learning techniques may be used. Improvements to hardware are described.
The physical elements are a network of strain sensors sampled at 128Hz through nodes transmitting wirelessly to a hub. These voltages are used as inputs to a feed forward back propagation network - this is trained to estimate internal socket loads as in [2] to produce a set of pressure-time series. This data is then reduced using fast Fourier transforms and using these coefficients as the inputs to a Learning Vector Quantisation network (as in e.g. [3]) - with results categorised using collected data in altered alignment conditions. When new data is introduced to the system, it can produce an estimate of the internal load distribution, a comparison to previous loads and an indication of any system misalignment.

123
Michael O’Dell (1) Kari Dunning (1) Patricia Kluding (1) Keith McBride (1) presenting
University of Maryland School of Medicine Department of Physical Therapy and Rehabilitation Science, Baltimore, Maryland, USA (1) Bioness, Inc., Valencia, CA, USA (2)
Efficacy and Prediction of Improvement from 42 weeks of Functional Electrical Stimulation in Post-Stroke Drop Foot: Data from the FASTEST Trial
Functional Electrical Stimulation (FES) is frequently used to address foot drop in persons with stroke. Smaller clinical trials on foot drop stimulation (FDS) have shown effectiveness, but there has been little data published regarding the magnitude, timing, characteristics or prediction of a clinical response. Using the data from the Functional Ambulation: Standard Treatment v. Electrical Stimulation Therapy (FASTEST) trial, we report the efficacy, satisfaction, trajectory and predictors of gait speed (GS) improvement.
The goal of this study was to report the effects of FDS over 42 weeks and investigate the predictors of improvement in persons with post-stroke foot drop.
Subjects were >3 months post-stroke with foot drop randomized into FDS or AFO group. FDS (Bioness L300™) group was used for this analysis. GS was measured at baseline with and without and 6, 12, 30, 36 & 42w with FDS. Response was examined over time as compared to baseline and by change relative to the minimal clinically important difference (MCID)] or advancing by one Perry Ambulation Category (PAC) by 42 weeks. Other variables examined included demographic information, age, Berg Balance Score (BBS), 6 minute walk test (6MWT), lower extremity Fugl-Meyer Assessment (FMA), Timed Up and Go (TUG), and baseline GS. Logistic regression was performed to examine relationships to GS performance.
The 99 subjects in the FDS arm had a mean age of 60.7 years and mean time post-stroke of 4.8 years. Baseline GS was .42 without and .49 with FDS.
GS increased to .54, .55, .58, .60 and .61 at 6, 12, 30, 36 & 42w, respectively. Even baseline (without FDS) to 6w improvements were significant (p<0.003). 67% were MCID and 55% PAC “responders.” Correlations between age, comfortable and fast GS, 6MWT, TUG and BBS and both MCID and PAC were significant (p<0.002.) Regression showed independent contributions for age and comfortable GS for PAC “responders” (p<0.003) and age and BBS for MCID “responders” (p<0.006).

FDS treatment improved GS even after 6w. The majority achieved clinically important endpoints by 42w. Baseline age, balance and GS predicted response, but not motor status (FMA.) Further research should examine the therapeutic effect of FDS.
125
Bastien Moineau (1,3) presenting Bruno Saurel (1) Vanessa Seetha (1) Marie-Pierre De Angelis (1) Cécile Meynard (2) Pierre Chabloz (2) Vincent Nougier (3) Dominic Pérennou (1)
Grenoble University Hospital, Grenoble, France (1) Chabloz Orthopédie, Grenoble, France (2) TIMC-IMAG Laboratory, Grenoble, France (3)
Is there a typical pressures pattern at the stump-socket interface for good above-knee amputee prostheses?
Above-knee amputees’ rehabilitation aims at providing a comfortable prosthesis to recover autonomy in daily life activities. However, pain and dissatisfaction are frequently reported. While there were various attempts to describe pressures pattern at the stump-socket interface there is not yet a clear explanation regarding the clinical meaning of these pressures.
The aim of our study was to provide relevant parameters to evaluate the quality of the stump-socket interface and to define an optimal pressures pattern for above-knee amputee socket.
40 above-knee amputee patients (mean age 49 years) using ischial integrated prosthesis and able to walk without aids were recruited. Clinical scales (SatPro and PPA-LCI) and examinations (stump pains and wounds) were used to separate patients in “good prosthesis” and “bad prosthesis” groups. Pressures exerted by the socket on the stump during gait were assessed with 14 force sensing resistors. Pressures were described regarding their peak values and their cross-correlation with respect to the other pressures (covariation and synchronization).
Significant differences (Wilcoxon test) between the 2 groups of above-knee amputee patients are summarized in the table (median and [1st;3rd] quartiles, covariations are coefficients and synchronizations are time lag in % of gait cycle).
Pressures pattern evidenced higher covariations and better synchronizations in the good prosthesis as compared to the bad prosthesis group (p<.001). Furthermore, pressure peaks were higher in the good prosthesis group on areas with soft-tissues (anterior aspect of the tight and below the buttock, p<.01) and relatively lower in bony areas (ischiopubic ramus, p<.01). Pressures pattern covariated more if patients had a higher body weight index (e.g. bigger stump).

These results are consistent with previous knowledge on stump tissues behavior: soft tissues allow a better repartition of pressures and were thus more tolerant to high pressure intensity (hydrostatic theory). To be comfortable, the socket should tight the stump at mid-eight and at the upper part of the thigh, so that bony areas (distal extremity and pelvis) could be relatively less loaded. The good fitting of the prosthesis is associated to pressures exerted simultaneously on the entire stump during gait. It is unclear whether the present results are generalizable to patients whose amputation was of vascular etiology, because of the poorer vascularization of their stumps. Assessing pressures at the stump-socket interface in above-knee amputee patients might help in dealing with problematic prostheses, particularly when patients are unable to provide relevant feedback.
126
Erin Boutwell (1,2) presenting Rebecca Stine (1,2) Steven Gard (1,2)
Northwestern University Prosthetics-Orthotics Center, Chicago, IL, USA (1) Jesse Brown VA Medical Center, Chicago, IL, USA (2)
Effect of Longitudinal Prosthesis Stiffness on Force Transmission during In Vivo Impact Loading
Shock-absorbing pylons (SAPs) have not been shown to alter force transmission within lower-limb prostheses in studies involving quantitative gait analyses [1-3]. The function of SAPs has been mechanically evaluated [4], but a discrepancy exists between the laboratory testing environment and the actively controlled task of walking. The current study proposes an investigation of SAPs within an intermediate testing environment: one that combines a controlled lab environment with the in vivo factors associated with the prosthetic-side limb.
To perform a systematic variation of longitudinal prosthesis stiffness, and to investigate the effect on force transmission during a controlled, in vivo step loading event.
14 subjects with transtibial amputations participated in this study. A novel testing apparatus was designed to deliver a consistent impact to the prosthesis. Subjects wore an experimental prosthesis consisting of a SAP (Endolite TT Pro, Miamisburg, OH) and a standardized prosthetic foot and shoe. Longitudinal stiffness was varied by substituing the spring within the SAP. A NORMAL (manufacturer-recommended), a SOFT (50% NORMAL) and a MEDIUM (75% NORMAL) stiffness as well as a RIGID pylon were tested. Data were acquired using a motion capture system (MAC, Santa Rosa, CA) and force platform (AMTI, Watertown, MA).
Peak impact forces ranging from 95.5-100.3 % body weight were measured, and total limb stiffness values of 15.0-17.9 kN/m were calculated. However, no statistically significant differences were observed between SAP stiffness conditions for peak force, peak timing, or total limb stiffness.

Representative impact force profile for a single subject for all stiffness conditions. No difference is apparent in peak loading magnitude and timing.
The study hypothesis was decreased prosthetic stiffness would lead to (a) decreased peak impact force, (b) increased time to peak, and (c) decreased total limb stiffness. However, SAP stiffness did not influence any variable related to force transmission. This result indicates that the lack of change in peak forces during previous gait analyses may not be the result of active adaptation by the prosthesis user, as previously hypothesized [1]. Rather, the passive characteristics of the prosthetic-side limb – most notably the residual limb soft tissue – may be dominating system response.
[1] Berge, J. 2005. J Rehabil Res Dev.
[2] Gard, S. 2003. J Rehabil Res Dev.
[3] Miller, L. 1997. J Rehabil Res Dev.
[4] Major, M. 2012. J Rehabil Res Dev.
128
Paul Prusakowski, CPO, FAAOP (1) presenting Cara Negri, BSME, CP (2)
OPIE Software, Gainesville, Florida, USA (1) PnO Data Soultions, Los Angeles, California, USA (2)
Combining Electronic Medical Records (EMR), Outcome Measures and Video Gait Analysis for the documentation of measurable patient centered care
Over 1000 combined clinical care locations in the US, Canada and Australia are utilizing a standardized Electronic Medical Records system (OPIE) for documentation and workflow management. Best Practices are emerging among the users of the software that include comprehensive clinical evaluation tools and processes, incorporating trackable and measurable goals, a matrix of outcome measures and gait analysis video. The data has potential to be the foundation of new ‘Practice Based Evidence’ for the profession.
Demonstrate an emerging Best Practice model for the documentation of O&P care and clinical outcomes in a manner that allows for comprehensive data mining and quantification of clinical outcomes over time.
For the past 10 years, the clinical documentation tools within the OPIE Software platform have continuously evolved to meet the changing needs of the profession, specifically with regards to the quantification of care in a standardized model. Educational workshops have been provided regularly to educate clinicians on advancing professionalism and how to communicate the clinical relevance of O&P intervention through improved documentation standards. These standards are grounded in an improvement of the traditional SOAP note format. This improved model is SOOGAP. Subjective Objective Outcomes Goals Assessment Plan. Through use of a progressive and standardized clinical documentation workflow and a recommended Outcomes Matrix, practices can use reporting tools to measure their successes in elevating their standards.
Practices that have adopted advanced documentation standards have been able to effectively communicate treatment plans and data about care and outcomes of individual patients and patient populations to other medical professionals, payers, and government agencies in ways previously unattainable. An increasing number of practices recognize the growing need and demand for data to prove efficacy of the care we provide above and beyond the prosthetic or orthotic device alone and throughout the duration of the entire episode of care. Standardized processes, databases, and reporting tools allow professionals to collaboratively mine data and begin to establish benchmarks for Best Practices. Integration of Outcome Measures, Measurable Goals, and clinician friendly Video Gait Analysis reporting have improved the capabilities of practices to document and measure care comprehensively and objectively.
The O&P profession must strive to quantify our clinical outcomes and prove efficacy to remain relevant in new healthcare models. The establishment of standards and processes through an electronic medical records platform has allowed for an idealized workflow with more consistent use of outcome measures in the clinical pathway as well as the inclusion of supportive video documentation to support our assemments and treatment plans. Best Practice models that incorporate these data tools into their documentation will set themselves apart from outdated practice models of the past.
129
mehdi moradkhani (1) presenting mahshid akhavan safaei (1)
saba, ouroumieh, Iran (1)
The effectiveness of neoprene ankle support and taping on semi-dynamic balance control of athletes
Ankle sprains are the commonest injuries of lower extremities, especially in athletes involved in high contact sports. It is hypothesized that one of the major causes of ankle instability is balance control deficit. In recent years, postural control as a foundation for athletes has been the focus of attention for investigators to evaluate the efficacy of taping and ankle orthoses on balance control for prevention of injury.
The aim of the present study was to determine whether two different mechanisms
1: ankle joint taping and
2: ankle support fitting
Can enhance semi-dynamic balance control on athletes?
The study subjects were 45 healthy athletes (mean [SD] age 24.4[2.20]) voluntarily participated in this study. This participants completed semi-dynamic balance test with Stabilometer in 3 separated groups. In all groups, 3 trials were recorded before and after taping and bracing. The mean of all trials was used for statistical analysis. Deviation exceeded 5° to right or left plus the length of time the subject was able to balance duration 30 seconds it was recorded. Paired sample T-Test and ANOVA were used to analyze overall semi-dynamic stability in and between groups at an alpha level of P<0.05.
The result of related paired sample T-Test indicated significant changes in semi-dynamic control capability of the subjects with the application of the tape and ankle support but no significant differences were found in control group ( p<0.05). The one-way analysis of variance revealed that there was significant differences in the performance of a balance task between ankle support, taping and control groups (p<0.05).
Mean difference and significant of performance in all experimental groups after intervention

The current study demonstrated that taping and ankle support significantly improved semi-dynamic balance task on athletes .We found that ankle support improved balance capability more than taping. In conclusion, this study suggests that using of ankle support can affect differently the performance of balance task compare with taping.
130
SEHOON PARK (1) presenting BUMKI HONG (1) JINHO SON (1) MUSUNG MUN (1)
KOREC, INCHEON, Republic of Korea (1)
Wireless EMG detector to minimize a Malfunction of the Myoelectric hand prosthesis
The upper-limb amputee has mainly used three types of the prosthesis, such as cosmetic, body-powered, myoelectric hand prosthesis. Myoelectric hand prosthesis is particularly useful because of grasping an object easily and with high torque just as controlling the residual muscles. But, many upper-limb amputees firstly using myoelectric hand prosthesis have trouble in unexpected malfunction, which embarrasses them frequently in daily living. Then, it will hardly be used and the upper-limb amputee will be still uncomfortable in daily living with no-functional cosmetic hand or big-sized body-powered type.
To improve the quality of life of the upper-limb amputee as using myoelectric hand prosthesis, malfunction minimization of the myoelectric hand prosthesis in grasping is absolutely necessary. Therefore, we will solve this problem as finding main cause of the improper EMG (electromyogram) signal states on the activation of daily living.
Many malfunctions mainly arise from the improper EMG signal which is caused by inner socket loosely coupled with the residual part of the amputee. It also arise from the interference of the muscle activation. To prevent these malfunction as finding ahead these situation, we developed the wireless EMG detecting system that monitering the EMG states(2 channels) while the amputee activating the muscle on the inner socket. We also suggest 4 meaningful main acivities of daily living, walking, folding hand, stretching upward and downward that are likely to be generating the malfunction. In addition, we classified the main cause of the malfunction and suggest the solution according to the EMG status .
Using the developed wireless EMG detecting system, we monitored the EMG signal of the 8 subjects who are trouble in malfunction on activities of daily living as follows.

The improper EMG signal from loosely coupled socket has found on 4 amputees while stretching downward, walking, stretch upward. We take a step as fitting the socket with the residual part. 2 amputees are caused from interference while folding arm. In this case, we found more optimized sensor position which has little interference on activation of the other musle. The rest are solved with proper EMG sensor gain variation while monitoring EMG signal on the 4 main activities. All of them haven’t generated any malfunction in fixed position using the current EMG detecting system that are based wired type because of restricting the boundry of the activity
On the states of activating of daily living, we can easily found the imporper EMG signal using developed wireless EMG detecting system from the loosely coupled socket and interference of the residual muscle activation. About 75% of malfunction is cause of the suggested 4 activities, walking or jogging, stretching downward and upward, folding. If we consider these facts on the processing the manufacture of the myoelectric hand prosthesis, we absolutely reduce malfunction cases and it will improve the quality of life of the upper-limb amputee.
133
Pushpa Ratna Bajracharya (1) presenting
POS-Nepal, Kathmandu, Nepal (1)
Development of Prosthetics and Orthotics in Nepal
The study is prepared to share the actual situation of P&O field of Nepal and increase awareness to develop P&O field of Nepal. Teaching and learning activities in P&O field are almost none. P&O profession is still new to government and policy makers; therefore this profession is in very pity condition in Nepal. Because of these reasons people of Nepal are not getting quality and standard P&O service comparable to its neighboring countries.
The aim of the study is to increase information on present situation, problem and possible solution of P&O field of Nepal. The physically disabled people from remote area and with poor socio-economic status are not getting satisfactory P&O service in Nepal.
The topic of study is a general and related with basic development. As development of P&O field of Nepal is in initial phase, the study topic is relevant. Data are taken direct contact and email from different organizations. Many fats and statistic are collected through different meetings related P&O sector, information from prosthetic Orthotic Society of Nepal and booklet published by NGO/INGO. The information and conclusion received from different interaction program among government, non-government and professional level also helped to prepare the study.
The study describes total number of professional, Prosthetic orthotic service centre of country. It describes challenges and possible solutions of P&O field in Nepal.

The discussion and conclusion of the study is that govt., non govt. and international community should support to prosthetic and orthotic field of Nepal in resource. Unity and continuous effort of stake holders will play a vital role to up-lift quality and standard of P&O service in Nepal. At the end all the positive result will contribute comprehensive development of Nepal.
• Documents from POS Nepal
• Booklet ‘Orthopaedic appliances’ published by Handicap International
134
Wieland Kaphingst (1) presenting
Tamarack Habilitation, Minneapolis, MN, USA (1)
Friction & Shear Mitigation in Orthotics, Prosthetics and Rehab – Option or Requirement?
Friction is a material-dependent property in the interface where two materials meet. In O&P fiction is a necessary component of device suspension but it is also a component causing soft tissue shear stress and strain in the socket/skin interface.
To understand both the desired effects of friction and the long-term undesired effect on human soft tissue in either repetitive or constant loading as well as how to avoid harmful friction in a strategically targeted approach.
Friction-related shear in human soft tissue may be mitigated by reducing not only the existing contact pressure in the affected area, but also by controlling force transfer mechanisms for tangential force (shear force by definition), transferred via surface friction. Such shear forces result finally in harmful shear strain (tissue deformation) in the underlying soft tissue layers.
Reducing surface friction in the contact area of device and skin, however, might also reduce friction, which is necessary in part for device suspension. Therefore friction should be reduced in a strategic manner only. Strategic friction management means spot-wise friction reduction as and where needed, but it avoids overall friction release.
Self-adhesive PTFE patches to be placed in the medical device at spots of high friction have been used in O&P for more than 8 years with good success. PTFE is a man-made material with one of the lowest coefficients of friction (cof) when paired with other materials including human skin.
In a second embodiment of friction management technology two-ply and low-cof textile patches, placed between silicone liner and the residual limb, have been used in prosthetic applications and as an insert in wheelchair seat covers for two years.
Both, the PTFE patch and the specific two-ply textile interface, deliver a cof of 0.2 and each of them has specific advantages (permeability, washability, release mechanism etc.).
Limited tissue volume and shape fluctuations, not under the patient’s nor under the care provider’s control, may lead to discomfort, irritation, redness and/or tissue trauma, which could have been avoided. Applying friction management to otherwise well-fitting devices is a low effort, low cost/high reward approach, when compared to an outcome that left the user with painful avoidance of their mobility device. However, it is still an approach not widely understood or applied.
135
Wieland Kaphingst (1) presenting
Tamarack Habilitation, Minneapolis, MN, USA (1)
A new Paraplegic Wheelchair Custom Seating System – Preliminary Experience Report
The paraplegic wheelchair user presents frequently as a highly active individual, who does not easily accept limitations often associated with being wheelchair-bound. Pressure sores of various degrees may be the result not only of being active but also of being dependent on the chair as the only means of body support surface and mobility provision for many hours every day and for the rest of their lives.
Aim is to educate about a new rapid custom seating technology, designed to take care of sitting surface pressure redistribution, avoidance of friction and shear, and improvement of micro-climate at the seating interface.
The new custom seating system consists of a pre-contoured seat perimeter having inter-woven, independently movable seat surface straps. They are pulled into a ratcheted molding system by springs and allowed to be fed out - against spring tension - in mm steps. Rapid customization of the new custom seating system is achieved through a molding process, which allows each strap to automatically conform to the users’ anatomy. Finally each strap is secured with proprietary strap clamps and the rapid molding system is removed. Reattachment is possible for future reconfiguration if required. The system is delivered to the user immediately after the set- up (including wheelchair set-up) is finalized and clinically confirmed.
To date, a total of 6 users – partially with an involvemet of the Minneapolis VA Medical Center - has participtaed in trials and studies of different duration and focus. Most of these trials are still under way and are being continued for further information gathering. Fitting success definition is based on objective measurements (pressure mapping), time of fitting measurements, comparison to conventional systems, as well as on clinician and user feedback. The seat surface molding and contouring results, comparable to results of conventional custom-fitted seats, have been achieved within an hour on the average. Results, as experienced by the time of presentation, will be disclosed in detail.
Paraplegic seating problems are caused by a variety of factors, some of them anchored in the specific pathology, others in personal habits such as the user’s level of activity and also in the individuals’s specific environment. The review provided initial clinical insight on the benefits of a rapid, custom-shaped seating system. However, the small volume of participants to date could not provide sufficient data for scientific result analysis. Further research is required.
138
Shaari Ida Hasni (1) presenting Abu Osman Noor Azuan (1) Shasmin Hanie Nadia (1)
University of Malaya, Kuala Lumpur, Malaysia (1)
The Immediate Effects of Lycra Fabric Soft Orthosis (LFSO) Garment on Trunk and Pelvis Kinematic during Sit-To-Stand (STS) on a Healthy Child
The application of soft orthosis made from Lycra® fabric produces positive outcomes on movement pattern and level of function, in patient with neurological deficits [1, 2, 4, 6]. However, focused was given more on improving gait and reaching parameter. None of the previous studies has explored the immediate effects of the LFSO garment on spine and pelvis movement during sit-to-stand (STS) motion [5].
To identify the immediate effects of the Lycra® Fabric Soft Orthosis (LFSO) garment, on the trunk and pelvis range of motion (ROM) during STS, in a healthy child.
The STS motion was captured using 3D Vicon cameras system. The full body Plug-in-Gait (PiG) was placed accordingly. First, subject performed 10 STS trials without the LFSO garment. Subject then performed another 10 trials of STS with wearing the LFSO garment. The movement pattern were presented in graph, and, the Wilcoxon signed rank test was used to determine the mean differences of the movement pattern and ROM for trunk and pelvis in all movement plane.
Plotted graph shows differences on STS movement pattern with and without LFSO (Figure 1 and Figure 2). There are significant different for the trunk ROM in frontal plane (Z = -8.76; p= 0.000), but not in sagittal and transverse plane. For pelvis, there are significant differences on the pelvis ROM in all movement plane (p = 0.000).


There is immediate changes observed on the trunk and pelvis movement pattern and ROM the when wearing the LFSO garment. However, there are different movement pattern was reported in previous studies [1, 6]. Such differences could be due to different subject with physical impairment is recruited. Overall, results shows that, the LFSO garment did provide immediate changes on the spine and pelvis movement pattern and ROM, during STS motion in a healthy child.
[1] Elliott CM et al. 2011. NeuroRehabilitation.
[2] Matthews JM et al. 2009. Prosthetic Orthotics International.
[3] Matthews M et al. 2006. Prosthetic Orthotics International.
[4] Nicholson JH et al. 2001. Developmental Medicine & Child Neurology.
[5] Gudjonsdottir, B. 1997. Journal of Pediatric Physical Therapy.
[6] Abdul El-Kafy EM. 2014. Clinical Rehabilitation.
140
Sumiko Yamamoto (1) presenting Tadashi Yasui (2) Toshikazu Kawaguchi (2)
International university of health & welfare, Tokyo, Japan (1) Kawamura-gishi, Osaka, Japan (2)
Development of a device to feedback assistive moment by an oil damper ankle-foot-orthosis during gait and its effect
It is well known that feedback is important for gait training in rehabilitation but an effective way for feedback has not been clarified. An Ankle Foot Orthosis to assist the heel rocker during gait using an oil damper (AFO-OD) was previously developed. Results of gait analysis showed the improvement of the gait of stroke patients who took the gait training using the AFO-OD. A device to detect the assistive moment of the AFO-OD and show it as a feedback signal during gait training has recently been developed.
The aim of this study is to show the effect of gait training using the device on the gait of patients.
A device to detect the assistive moment by the AFO-OD and the 2ch EMG (Tibialis anterior and Gastrocnemious) has been developed. Obtained data are shown on the graphic display of an iPad in real time. During the gait training, patients are told to make the heel contact with the knee joint extended as much as possible. The assistive moment by the oil damper is generated during the plantar flexion movement in loading response. The magnitude of the assistive moment becomes larger if the plantar flexion of the ankle joint occurs quickly. Therefore the visual feedback of the assistive moment facilitates the effective heel rocker function. Gait training using this device has already been performed in two patients: a stroke patient in acute phase and a patient with paralyzed tibial nerve.
The average peak of assistive moment was 1.4Nm before gait training and it became 2.0Nm after a 15-minute training for the stroke patient. It meant that the definite heel contact became possible after gait training. Regarding EMG data, co-contraction of both muscles was shown throughout the gait cycle before training, but separated activities of the muscles were found after training. As for the patient with paralyzed tibial nerve, the peak assistive moment was 1.6Nm before training, and 7.4Nm after training. The activity of the Gastrocnemious, which was not found before training, was observed after training. The figure shows the graphic display of the stroke patient after training.

The gait training using the device to feedback assistive moment by the AFO-OD improved the muscle activities of a stroke patient and a patient with paralyzed tibial nerve.
Yamamoto S; 2011, Prosthetics and Orhtotics International.
141
Lee Brentnall (1) presenting Kylie Mines (1)
Motivation Australia, Willunga, South Australia, Australia (1)
Keep Moving: Training tools for the prevention and management of amputation in Pacific Island Nations
Seven of the top ten countries in the world for diabetes prevalence are Pacific Islands Nations (IDF 2013); countries that are arguably least equipped to meet the challenges associated with effectively managing diabetic foot problems and high rates of amputations. There is a limited health workforce to provide amputation prevention services and specialists are not existent in many countries. Further, access to rehabilitation services after an amputation is extremely limited.
To identify and develop resources that could assist in the prevention of diabetic related lower limb amputation
The project began with an analysis of the prevention and management of lower limb amputation; including identification of six phases and a range of interventions possible during each phase. A literature search was undertaken to identify related training tools and resources freely available for the health workforce in the Pacific region. Priority areas were then identified by a working group of stakeholders from Pacific Island Nations and resources developed addressing these priority areas. The resources were peer reviewed; piloted in one country (Kiribati); and tested by stakeholders in three countries by means of tablet technology.
Training resources were developed for three priority areas; offloading foot ulcers, shoes for healthy feet and mobility without a prosthesis. Each topic is structured into three areas: 1) “Learn,” resources targeted at health and rehabilitation personnel to learn new skills and knowledge, 2) “Teach,” tools for personnel, to facilitate their education of clients and 3) “Advocate and share,” resources that personnel could use with local adaptation to raise awareness amongst managers of the rationale for services, and human and physical resource requirements to implement specific interventions (for example off-loading). Feedback has been positive, with stakeholders noting content developed is appropriate and resources are easy to understand and follow. The three organisations trialling the tablets noted the use of tablets reinforced and strengthened the practise of providing client education, made client education easier; and were useful to share with and educate fellow health professionals.
Stakeholders identified many gaps regarding training resources for the prevention and management of amputation in their region. The tools developed through the Keep Moving project have begun to fill this gap. However further development of the remaining topics, development of video tools and increased support to use the resources would be beneficial to increase the impact and improve amputation prevention and management efforts in the region.
International Diabetes Federation (2013) IDF Diabetes Atlas 6th edition. Brussels, Belgium. http://www.idf.org/diabetesatlas
144
Helen Naylor (1) Pip Russell (1) presenting
Blatchford Clinical Services, Leicester, UK (1)
A Scoring Tool to Predict Functional Outcome in Lower Limb Amputees (BLARt) – A Pilot Study
Current pre-operative patient advice on the likely success of post-operative prosthetic ambulation is based on subjective clinician opinion. Lack of objective assessment often results in the referring clinician and patient expectations being unrealistic. In response to this lack of objective assessment we have developed a pre-operative predictive assessment tool for amputee outcomes, the
The aim of this study was to pilot the efficacy of a preoperative assessment tool which would calculate the likelihood of successful prosthetic mobility outcomes following lower limb amputation.
The study population consisted of patients referred following lower limb amputation to the rehabilitation service in Leicester during 2010-2013 and the Northern General Hospital, Sheffield during the years 2012-2013. Scores were subsequently derived from this information and compared to patients’ functional outcome at discharge from primary prosthetic rehabilitation. Continuous data were reported as means and 95% confidence intervals, with comparison by the student’s t-test. Comparison of proportions was by the X2 test. For both, significance was assumed at the 5% level.
Twenty patients (10%) died during the first 12 months. Patients 65 years or older were less likely to realise any form of functional rehabilitation compared to patients younger than 65 years (52/110, 47% vs. 53/69, 77%, p=0.0002). Levels of preoperative mobility were closely linked to functional rehabilitation, 21% who were wheelchair bound preoperatively and 85% who were mobile preoperatively, p<0.00001. The presence of any associated comorbidity significantly impacted on rehabilitation (p<0.00001) although when individual comorbidities were considered in isolation, the association was not significant (p=0.10). Likewise, the chances of any functional rehabilitation were significantly better for patients with normal cognitive function (68%) or severe cognitive impairment (9%), p<0.00001.
A score of 12 or below was associated with a 95% success rate of rehabilitation, while a score of 24 or more was associated with a 3% success rate. Scores in the range 13-23 were associated with an intermediate chance of success (47%). There was no obvious inflection point to the curve, rather a strong linear relationship.
The BLARt tool offers a consistent pre-operative assessment based on objective evaluation of underlying clinical parameters and their influence on the rehabilitation process following lower limb amputation.
It provides patients with more realistic probability of rehabilitation success and can assist in setting realistic objectives. It is essential that patients should still be given the choice of attempting prosthetic rehabilitation but by having a BLARt assessment completed it is hoped that they will have a more realistic assessment and expectation of their probability of success in becoming ambulant once again.
145
Anka Michielsen (1) presenting Iris van Wijk (1)
Centre of Excellence for Rehabilitation Medicine Utrecht (De Hoogstraat Rehabilitation, Utrecht and UMC Utrecht), Utrecht, The Netherlands (1)
Participation in Sports of Dutch Children with Lower Limb Deficiencies
Sports can and do, make a profound and positive impact on individuals. Physical activity, including sports, is linked to reduced risk of illnesses including obesity, cardiovascular diseases and some cancers. Studies have found that sport programmes can enhance self-esteem and confidence . Children playing sports have a more positive body image and experience higher states of psychological wellbeing compared to children who do not play sports.
to describe sports participation of Dutch children with congenital lower limb deficiencies (LLD) in comparison with typically developing children.
Cross-sectional study. A questionnaire was sent by mail to 94 children and adolescents with LLD, aged 8-18 years.
Participation in sports of Dutch children and adolescents with LLD (age range 8-18 years) does not differ from sports participation in healthy peers. A small percentage of the children that do participate in sports, do not play the sports of their choice. Although being able to participate in sports some of the children think they are not able to participate in every sport. Running, jumping and endurance were mentioned as the most limiting factors in participating in sports of preference
Dutch children and adolescents with LLD participate in sports similar to those among typically developing children. Not all children participate in the sports of their preference because of experienced limiting function of the lower limb prosthesis.
146
Heiko Glindemann (1) presenting Norman Pfeiffer (1) Bernhard Graimann (1)
Otto Bock HealthCare GmbH, Duderstadt, Germany (1)
Multivariate myoelectric signal acquisition based on conductive silicone
Advanced myoelectric man-machine interfaces require improved signal acquisition. The few electrodes usually used in conventional upper limb prostheses provide only sufficient information for direct and sequential control. For intuitive, simultaneous and proportional control of multifunctional prostheses, multivariate signals are necessary, which capture more information about the muscle activity in the residual limb. Moreover, such a signal acquisition system should be cost effective. This latter requirement is difficult to attain with conventional EMG electrodes used in prosthetics.
In this work, we propose a new, cost effective signal acquisition system for multivariate myoelectric signals based on silicone electrodes. We demonstrate the design of the system and show first evaluation results on able-bodied subjects and amputees.
To reduce the influence of external artifacts the amplifier is usually integrated into the electrode. Alternatively, guarded shielding can achieve similar results. Shielding has the advantage to separate electrodes and amplification which leads to more cost effective solutions. Therefore, we used a guarded shielding approach in combination with electrodes made of conductive silicone. These electrodes were embedded in non-conductive silicone in a special design to reduce triboelectric effects and movement artifacts. To evaluate this new signal acquisition system, we conducted a study with four abled body subjects to evaluate EMG signal quality as well as online and offline control performance. We compared our system to conventional EMG electrodes used in prosthetics as well as a system based on gel electrodes. Additionally a clothespin test was performed with an amputee.
A cuff was made integrating 16 conductive silicone electrodes for able bodied subjects made out of standard socket material. First tests with four able-bodied subjects showed a comparable signal quality to conventional, active EMG electrodes. Offline classification using linear discriminant analysis with 5 classes leads to similar accuracies (silicone electrodes: 99,49 ± 2,0 %, active EMG electrodes: 99,27 ± 1,9 %). Online control performance was rated by measure speed and throughput during the fulfillment of tasks in a certain virtual reality. Executed tests showed no relevant differences between silicone and gel electrodes. However, it turned out that silicone electrodes are more prone to electrostatic and movement artifacts than conventional electrodes. This was confirmed during a clothespin relocation test with one amputee to control a multi DOF hand prostheses. The completion time was 20% higher than with conventional electrodes.
The results confirmed the potential of conductive silicone to build cost effective systems for multivariate, myoelectric signal acquisition. Using guarded shielding the electrodes and signal amplification can be separated while the signal quality is not influenced. However, the work also showed that the silicone is more prone to electrostatic noise and movement artefacts. Although measures were introduced to reduce those artefacts further improvements are necessary.
147
Joanne Allan (1) presenting William Munro (2) Elaine Figgins (1)
University of Strathclyde, Glasgow, UK (1) Anatomical Concepts (UK) Ltd., Clydebank, UK (2)
Foot deformities within the diabetic foot and their influence on biomechanics: A review of the literature
Diabetes Mellitus (DM) can cause a multitude of complications. Foot ulceration is one complication that has the potential for further serious consequences, such as amputation. Foot deformities have been identified as one of the contributing factors in the development of ulcers within the diabetic foot. It would be advantageous to ascertain if foot deformities within DM are a preventable complication because, if the risk of ulceration could be reduced, then so too could the risk of amputations.
The aims of the literature review were to understand the development of the common foot deformities in DM and explore their biomechanical effects within DM.
In February 2014 CINAHL, Embase, Ovid, Medline and Ovid were searched for studies that reported on the development of foot deformities within DM or the biomechanical impact of these deformities. The quality of articles was considered to be high overall, assessed using SIGN and CARS assessment tools.
17 studies were included for review. The main themes identified were Nerve Function, Intrinsic Foot Muscles, Muscle Weakness, Limited Joint Mobility, Gait Abnormalities and Foot Deformities. The common foot deformities that resulted were not identifiable. Aetiology was unclear.
There is a lack of understanding about the common foot deformities in DM and their development. The common belief that motor neuropathy causes atrophy and muscle imbalance that results in foot deformities was not supported by the literature. IFM atrophy, muscle imbalance and a reduction in nerve function did not display definitive associations with foot deformities. However, muscle weakness and LJM were associated with foot deformities.
The articles that discussed muscle weakness displayed conflicting results. The first identified a causal relationship between muscle weakness and foot deformities within DM. Conflictingly, the second article found that muscle weakness increased the frequency of foot deformities, in particular the presence of a high arch, which was found to be present in 80% of participants with muscle weakness. This clear association between muscle weakness and foot deformities may be a useful clinical tool in detecting the risk of developing foot deformities.
Those patients who had pronation of the foot also had an increase in LJM of the 1st MTPJ. Therefore, assessing joint mobility would be beneficial as it is not costly, is a relatively quick assessment and is easily done within a clinical environment.
Foot deformities within diabetes need to be studied further to establish if the assessment of muscle weakness, LJM or another clinical sign could be utilised to predict the development of foot deformities. Once the common foot deformities have been identified, it will be possible to evaluate the impact they have on biomechanics.
148
Rachel Hogg (1) presenting Alan De Asha (1) John Buckley (1)
University of Bradford, Bradford, UK (1)
The effects of using passive hydraulic ankle-foot device in unilateral trans-femoral amputees when crossing obstacles leading with the intact limb
Lower-limb amputees have a higher incidence of trips and falls than the able-bodied, and the incidence of falls increases with higher amputation levels. When stepping over obstacles lower-limb amputees are ten times more likely than the able-bodied to contact the obstacle with their foot [1]. It has recently been demonstrated that use of a passive, hydraulically articulating, prosthetic ankle-foot device (Echelon, Chas. A. Blatchford and Sons, Basingstoke, UK; hyA-F) resulted in bilaterally increased minimum toe clearance and a smoother centre of mass progression over the prosthetic foot [2] during overground gait.
To investigate whether use of a hyA-F in unilateral trans-femoral amputees would alter clearance metrics during obstacle crossing compared to using a conventional prosthetic-foot.
Segmental kinematic data were recorded using eight infrared cameras and passive markers while seven unilateral trans-femoral amputees crossed obstacles of height 3, 7 and 10 cm (low, medium, high) while using their habitual, conventional prosthetic-foot and a hyA-F. Foot-type order was counter balanced across participants and obstacle height was randomized between trials. Participants completed three trials at each height using each device, crossing the obstacle leading with their intact limb. Whole-body centre of mass (CoM) forwards velocity, foot placements, lead and trail foot clearances and the number of failures (foot–obstacle contacts) were compared between prosthetic devices.
Lead-foot toe clearance was unchanged across foot conditions but trail-foot toe clearance significantly increased when using the hyA-F. There were nine failures (all by the trailing, prosthetic-limb) while using participants’ habitual foot devices and only two while using the hyA-F. Average crossing CoM velocity was (non-significantly) lower, and trail foot placement prior to the obstacle was (non-significantly) further from the obstacle when using the hyA-F (Table 1). Crossing step length was unchanged between devices.
Group mean (SD) trail foot clearance, crossing vel and foot placement and number of failures at each obstacle height in each foot condition.

As failures only occured on the trailing, prosthetic-limb, this likely reflectives the mechanical constraints of an above-knee prosthesis. The decrease in failures when using the hyA-F appears to have been driven by a combination of increased foot placement distance prior to the obstacle, possibly reflective of improved step length symmetry [2], and a reduced crossing CoM velocity, which, together, would have provided more time and space in which to elevate the trailing, prosthetic-limb, over the obstacle.
Hofstadt et al. (2006) Arch. Phys. Med. and Rehab. 87, 1115-22.
De Asha et al. (2014) Clin Biomech, doi: 10.1016/j.clinbiomech.2014.06.009
152
Kenji Kawamura (1) presenting Yoshio Kano (1)
Kibi International University, Takahashi-city, Okayama, Japan (1)
Surface electromyographic evaluation of quadriceps setting and seating-belt press exercise
A quadriceps femoris muscle setting is isometric quadriceps femoris exercise which can be widely used in early knee rehabilitation. However this exercise cannot obtain enough co-contraction of the hamstrings. Isolated quadriceps femoris contraction in knee extension imposes severe strain to knee joint. We succeeded in developing a simple training maneuver that is effective in obtaining coactivation of quadriceps and hamstrings using a simple portable sitting aid : seating-belt [1].
The objective of this study was to compare the electromyographic activities of lower extremity muscles under the condition of quadriceps setting and seating-belt press exercise.
Ten healthy young males (average age, 21.8 ± 0.4 years) were tested. The EMG activity from eight muscles was monitored simultaneously for each exercise using surface electromyography. The Noraxon TeleMyo 2400T G2 (Noraxon Inc., USA) at sampling cycles of 1500Hz, was used. Each exercise was performed for 5 s, and the derived electromyographic activity from each muscle was rectified, smoothed, and integrated for 3 s (IEMG : Integrated EMG). The MyoResearch XP Master Edition Version 1.07.05 program was used for this process.

When the subjects performed quadriceps setting exercise without seating-belt, quadriceps groups were mainly active. When the subjects performed press exercise with seating-belt, the activity of the quadriceps femoris was observed in parallel with the activities of the hamstrings and gluteus maximus. The %MVC of the vastus medialis and the hamstrings varied significantly in the seating-belt press exercise.
The straps of this device act in place of the bi-articular muscle: rectus femoris. The hamsrings co-contraction obtained in seating-belt press exercise achieved by a pelvic anteversion generated by seating-belt. To counter this pelvic anteversion, the subject produces opposing moment in the anti-rotatory direction on the pelvis by contracting gluteus maximus and hamstrings. This study suggests that effective co-contraction of the quadriceps and the hamstrings can be obtained by seating-belt press exercise.
[1] K Kawamura ; Development of a Portable Sitting and Transfer Aid for Bed Recumbent Patients. Proceedings of ISPO 2004.
153
Zala Kuret (1) presenting Helena Burger (1) Tomaz Maver (1) Gaj Vidmar (1)
University Rehabilitation Institute, Republic of Slovenia, Ljubljana, Slovenia (1)
Influence of silicone prosthesis for finger amputation on body functions, activities and quality of life
Finger amputations are the most frequent amputations of upper limb and they affect many people. Amputations cause participation restriction and affect all functioning levels according to International Classification of Functioning, Disability and Health (ICF). There are several rehabilitation methods: activity modification, use of adaptive equipment or use of prosthesis.
The aim of our study was to evaluate the influence of silicone finger prosthesis on hand function, activities and quality of life.
We included 44 patients with partial or complete single or multiple digit amputation of one hand and a healthy and uninjured other hand. We evaluated hand function with SHAP test and measured grip strength of the healthy hand, of the injured without and with the prosthesis. We used OPUS-UEFS II questionnaire and TAPES.
The average values of all SHAP grip indexes were statistically significantly higher for the healthy hand compared to the injured one. Indexes slightly improved with the use of prosthesis, except for the lateral grip. Grip power of the healthy hand was better compared to the injured hand, but it was not significantly affected with the use of prosthesis. Results of OPUS-UEFS II questionnaire did not show significantly better achievements in different activities with the prosthesis. According to TAPES prosthesis seems to be an obstacle to patients when engaging in more strenuous activities and sports.
Patients achieved statistically significantly better results on the SHAP test and better strength with the healthy hand compared to the injured. Our study partially confirmed the results of previous publications (1,2,3) that use of prosthesis improves different grips (exception of lateral grip). In contrast to our findings previous study (4) describes improvement of grip strength. Most patients wear the prosthesis daily and it improves their quality of life.
1. O’Farrell DA; 1996, J Hand Surg.
2. Alison A; 1992, J Hand Surg.
3. Pillet J; 1992, St. Louis: CV Mosby.
4. Lifchez SD; 2005, J Hand Surg Am.
154
Subhash Sinha (1) presenting Prem Saggurthi (1) Barbara Rau (1)
International Committee of the Red Cross, Gaza, Palestine, Occupied Palestinian Territory (1)
Experience of prosthetic and orthotic services for people with disabilities in an interdisciplinary physical rehabilitation team setting; post armed conflict context, Gaza
Recurrent protracted armed conflicts in Gaza have resulted in a large number of people with disabilities (PwDs). According to World Health Organization, 11’066 people* were injured in the 2014 conflict, adding to an existing high number of PwDs. The Artificial Limb and Polio Centre (ALPC) and the ICRC** have been working together since 2007 to establish an interdisciplinary team approach to provide full physical rehabilitation services. ALPC also coordinated activities with national/international organizations.
This presentation aims to share experiences and challenges working in armed conflict situations and on how an interdisciplinary approach and coordination among organizations helped PwDs benefit from comprehensive physical rehabilitation services.
An interdisciplinary coordinated approach was applied to help ALPC respond to the emergencies. Accessibility, quality and long term sustainability of services at the ALPC were the main objectives of the project. Existing tools to ensure accessibility and quality were adapted while service protocols were implemented to achieve the best services in the short and long term. Capacity building to integrate the use of affordable ICRC Polypropylene technology and pyramid adapter technology was used for manufacturing Prosthetic and Orthotic (P&O) devices. Additionally, Mental Health and Psycho-Social support (MHPSS) approach was applied to complement the physical rehabilitation of service users.
The interdisciplinary team was formed by five P&O technologists trained in Category II, eight bench-workers trained on the job, five physiotherapists trained in amputee rehabilitation, an orthopedic surgeon, PwDs and their care givers. Holistic assessments and treatment plans for the PwDs to achieve maximum functional outcomes were further developed. 45 community workers (physiotherapists, occupational therapists and nurses) were trained on PwDs home based care and referrals to ALPC. MHPSS sessions helped the affected ALPC staff to recover from post conflict distress and strengthened the capacity of rehabilitation staff to provide psychological first aid for affected PwDs. A referral network for rehabilitation was established with effective coordination among organizations. Today ALPC ensures the availability of quality services and follow up within Gaza avoiding the need for PwDs to travel abroad.
Adapted P&O technology and integrated interdisciplinary team approach are essential for quality service provision in post armed conflict situations. Indeed, physical rehabilitation in such a context is a complex and challenging task and it is definitely more than the sole provision of P&O devices. Last but not least, the interdisciplinary approach using MHPSS as a tool and effective coordination could help to address the complexities of rehabilitation in conflict contexts.
References (optional):
*http://www.moh.ps/?lang=1&page=4&id=963 (last accessed on 18-11-2014)
**https://www.icrc.org/en/what-we-do/health/physical-rehabilitation
156
Todd Kuiken (1,2) presenting Laura Miller (1,2) Kristi Turner (1)
Rehabilitation Institute of Chicago, Chicago, IL, USA (1) Northwestern University, Chicago, IL, USA (2)
A Comparison of Direct Control and Pattern Recognition Control in Transhumeral TMR Subjects
Individuals who have had Targeted Muscle Reinnervation (TMR) surgery are able to control a prosthetic elbow and hand simultaneously, without mode-switching. However, for direct control, it can be difficult to isolate four different control signals using thresholds and gains. In pattern recognition control, a controller is trained to recognize the different movements, precluding the need to set gains and thresholds and allowing the possibility of controlling additional degrees of freedom, such as the wrist.
The goal of this study is to compare function in individuals with transhumeral TMR amputations using a commercially available arm system with either direct control or pattern recognition control.
To date, five subjects with transhumeral amputations and who have had TMR surgery were fit with a commercial elbow system (Boston digital arm), a powered wrist rotator, and a powered terminal device (hook or hand). Subjects controlled this device during separate home trials using direct control or pattern recognition control. Subjects were randomized as to which control method was implemented first and used the device for a minimum of six weeks at home with each control paradigm. Pre- and post-home trial outcome measures included the Box and Blocks, the clothespin relocation task, Jebsen, SHAP, and ACMC (post-trial only). Subjects also completed a survey to provide subjective evaluations of control in each configuration.
Using pattern recognition control, subjects had improved scores on the SHAP with an index of function score average of 30.80 (
During activities where there was an advantage to accessing all degrees of freedom quickly (e.g., SHAP and clothespin relocation test) scores improved when subjects used pattern recognition control. Subjects also preferred this configuration over direct control, when they were required to switch between the wrist and hand (or wrist and elbow). However, when only hand and elbow movement was desired (e.g., Box and Blocks), subjects had better scores when using direct control, since inadvertent movements did not elicit unwanted prosthesis movements that compromised function. Five additional subjects will complete this study.
157
Urban Daub (1) presenting Urs Schneider (1)
Fraunhofer IPA, Stuttgart, Germany (1) Donau Universität Krems, Krems, Austria (2)
A review of validity, reliability and practicability of internationally used assessments scores for lower limb amputees as basis for daily clinical use recommendations
To minimize secondary diseases and losses of quality of life and mobility, therapy and prosthetic provision of lower limb amputees (LLA) must be optimized continually. At present day, a vast variety of different questionnaires, documentation and assessment forms are being used in daily practice by physicians, technicians, prosthesis suppliers, and the industry. There is no national or international gold standard and the outcomes are often barely comparable. To raise quality in therapy and prosthetic provision of LLA, coherent active examination would be strongly reasonable.
With the aim of providing a well-founded recommendation for the broad active use, this review was conducted to examine the validity, reliability and practicability of assessments being used internationally for patients with LLAs.
Studies of this review were searched according to the PICO-scheme in Pubmed, limited on publications of the last five years. Further studies were searched in Cochrane and Pedro databases. All articles were screened for matching references regardless of the references’ publication dates. The assessments were categorized into questionnaires or active assessments. Further they were subdivided into generic, amputee specific and other relevant assessments analogous to the systematic review by Condie et al. (2006). The studies were examined for parameters describing internal consistency or intra- or interrater reliability to quantify reliability. Validity was evaluated based on effect size and correlations with other assessments. To evaluate the practicability references describing time effort, costs or exceptional qualifications were registered. Assessment recommendations of authors were also ascertained.
In total 158 studies were examined to analyze 52 assessment scores. Eleven of them were active assessments and 41 were questionnaires. Nineteen of the questionnaires were categorized into “quality of life” and another 19 into “mobility”. The last three were categorized into “satisfaction with the prosthesis”. Twelve of the internationally used assessments have been applied in studies, although neither their reliability, validity nor their practicability was examined for LLAs. Only eight of the 41 questionnaires could proof reliability, validity and practicability on LLAs, such as five active assessments. Six of these left 13 assessments were criticized for their ceiling effects or were not recommended for their use with LLAs for other reasons.
Only one of the remaining questionnaires was also applicable in a German validated version. Of the active assessments remained three as possibly recommendable for daily clinical use in Germany.
Included studies were very miscellaneous in regard to setup and quality. Participants were very dissimilar between the studies, especially in regard to age, reason for amputation or amputation level. Conducted to this review, Trinity Amputation and Prosthesis Experience Scales (TAPES) plus L-Test or Two-Minute-Walk-Test can be recommended in Germany.
[1] Condie; 2006 JPO
158
Sirintip Kaewtip (1) presenting Anna O’Neill (1) Elaine Figgins (2)
University of Glasgow, Glasgow, UK (1) University of Strathclyde, Glasgow, UK (2)
Title: How do formative assessments influence teaching and learning in P&O education?
Formative assessment refers to assessment that is specifically intended to generate feedback on students’ performance to improve and accelerate learning. Recently, considerable research evidence concluded that effective feedback leads to a number of learning gains. Formative assessment, therefore, is becoming a popular topic among academic staff.
In health professions education, there are some schools where formative assessments are institutionalized and carried out systematically. Unfortunately this mode of assessment, from the researcher’s observation, is not very frequent in Prosthetics and Orthotics (P&O) education. This may be due to a lack of empirical evidence on its advantages particularly regarding P&O education. Therefore, this research will focus on the application of formative assessment in P&O education.
To explore the application of formative assessment in P&O education. The specific objectives included: to investigate how formative assessment was provided, what factors were involved in successful and unsuccessful formative assessment practice and what could be done to make improvement.
The study was a qualitative, descriptive study based on semi-structured interviews with seven experienced P&O educators who are working in ISPO certified category I school.
The qualitative descriptive research design was employed. The purposive sampling technique was used to obtain only the eligible participants. The data was collected from experienced P&O educators using semi-structured interviews method to determine how they personally experienced formative assessment practice.
Four main categories regarding formative assessment activities in P&O education were identified: 1) purpose of formative assessment, 2) benefits of formative assessment 3) Formative assessment practice and 4) Strategies to engaged student in formative assessment.
Whilst the topic of formative assessment is not new, for the first time research in this area has been explored in P&O education, the findings of this study present the situation and suggest the opportunity of maximizing quality of P&O education by addressing the role of formative assessment. Further researches on formative assessment in P&O education were recommended for example, exploration on P&O student experience and perspectives of formative assessment, investigation into the quality of feedback used in P&O practical subject, and exploration into the use of formative assessment in P&O curriculum
160
Todd Kuiken (1,2) presenting Kristi Turner (1) Nicole Soltys (1) Gregory Dumanian (2)
Rehabilitation Institute of Chicago, Chicago, IL, USA (1) Northwestern University, Chicago, IL, USA (2)
First Clinical Fitting of an Individual After Bilateral TMR With Pattern Recognition Control
Targeted Muscle Reinnervation (TMR) surgery has been performed in more than 100 individuals and has been available since 2002. Additionally, after decades of research on pattern recognition based myoelectric control, a clinical pattern recognition system is now commercially available. When used together, TMR and pattern recognition algorithms can provide intuitive control of many degrees of freedom in upper-limb prostheses.
To describe the clinical fitting and functional outcomes of the first patient to have bilateral upper limb TMR surgery who also received the first commercially available pattern recognition controlled prostheses.
TMR was performed on the patient’s left shoulder disarticulation side in January 2012. In May 2012, TMR was performed on his right transhumeral side, in which the gracilis muscle was transferred from his right leg due to lack of biceps muscle. The patient received a direct controlled prosthesis (conventional EMG amplitude based control) for his left side and began occupational therapy (OT) in August 2012 with three, one-week visits for 90 minutes a day. In October 2012, he was fit with a research pattern recognition controlled prosthesis on his right side, and then with commercially available pattern recognition systems from Coapt LLC on both sides in November 2013. The patient received OT with the Coapt system for a total of four days, which emphasized identifying unique and repeatable muscle movements.
Using the pattern recognition system, the patient could control elbow function better than with his direct control system. He could seamlessly switch between his elbows, wrists, and terminal devices with pattern recognition control, not needing to switch for wrist function. He also performed tasks he could not achieve using direct control, such as feeding himself, and grasping items at various levels, including objects from the floor. When performing various outcome measures (Box and Blocks, Clothespin Relocation tests), the patient performed similarly on both sides, despite the different amputation levels. He demonstrated such skill with his prostheses that he was able to perform the same movements at the same time on both sides (e.g., wrist supination with the right and left devices at the same time) as well as opposing movements (e.g., wrist supination on the right at the same time as wrist pronation on the left).
Performing bilateral functional tasks is extremely challenging for patients with high level bilateral amputations, including a shoulder disarticulation. However, with the addition of pattern recognition control, the patient demonstrated marked improvement. Using bilateral pattern recognition systems, the patient could control his prostheses with physiologically correct movements; thus, he could perform tasks on both sides with similar function, as well as operate both devices simultaneously for all degrees of freedom.
161
Timothy Reissman (1,2) Elizabeth Halsne (1) Todd Kuiken (1,2) presenting
Rehabilitation Institute of Chicago, Chicago, IL, USA (1) Northwestern University, Chicago, IL, USA (2)
Clinical Evaluation of a Novel Gel Liner System Developed to Improve Use and Function of Transhumeral Myoelectric Prostheses
The uses of EMG electrodes in liners has been studied and frequently attempted, but many challenges remain—especially wire management and robustness [1-2]. Recognizing this technological gap, we have developed a gel liner with embedded electrodes and flexible fabric leads, and a distal magnetic electrical connector (Figure 1), to provide an integrated socket interface for myoelectric prostheses [3-5].

Gel liner system. (a) Interior with embedded electrodes and flexible fabric leads (b) Exterior with distal magnetic electrical connector.
To evaluate the gel liner system and magnetic electrical socket connector for durability and clinical efficacy—specifically for ease of use, comfort, suspension, and prosthetic function.
Six individuals with transhumeral amputations participated in the study. Subjects were instructed to use the gel liner system with their myoelectric prosthesis over a period of 2 months at home. To evaluate durability of the liner system, the electrical resistance of the embedded electrodes was measured before and after the home trial. To evaluate clinical efficacy, a questionnaire was used to obtain user perceptions of the liner system, within the clinical areas listed in the Aim, after the home trial. Subjects recorded their perceptions for each survey item using a Likert scale. A nonparametric Wilcoxon signed rank test was performed to determine the statistical significance of the data.
Before use, the embedded electrodes had electrical resistances of 12.7 ±6.4 Ω, (measured from the electrode to the magnetic electrical socket connector). After use, electrical resistances increased to 19.8 ±13.4 Ω. A paired sample t-test analysis showed this increase to be statistically significant (p<0.001). Upon visual inspection, no differences were observed in the structural integrity of the gel liners. In questions ranking difficulty with donning/doffing the liner and with connecting the liner to the myoelectric prosthesis, users strongly indicated that the liner system was easy to use (p<0.05). In comparing the liner system with their usual myoelectric socket interfaces, users consistently agreed that the liner system was easier to use, more comfortable, and offered better suspension and prosthetic function (p<0.05).
The results support the clinical viability of our gel liner as an EMG recording system. Although electrical resistance of embedded electrodes increased with use, this remained well within the range required for consistent myoelectric prosthesis performance. The questionnaire provides strong evidence that our gel liner system is a practical alternative to, and offers advantages over currently available socket interfaces for upper limb myoelectric prostheses.
[1] Salam; 1994 JPO
[2] Daly; 2000 JPO
[3] Lipschutz; 2012 U.S. Patent Application
[4] Lipschutz; 2014 Proc. AAOP
[5] Reissman; 2014 Proc. MEC Symposium
162
Louis Desrosiers (1) Danielle Boucher (1) presenting
Laboratoire Victhom, Quebec, Canada (1)
Clinical and biomechanical efficiency evaluation of a new distraction/rotation knee brace in the treatment of medial knee osteoarthritis
Valgus knee braces are recommended for the management of medial knee osteoarthritis (KOA). Recent studies have shown that valgus knee braces with a three point bending system allow reduced knee loading but have low daily use and poor compliance. A new unloader brace with distraction and external rotation functions has recently been introduced in clinical practice. The brace efficiency was validated through patient’s satisfaction survey and biomechanical analysis.
The study aimed at simultaneously evaluating efficiency of the new brace through patient satisfaction survey and motion capture system data acquisition.
Over 2000 braces were fitted on KOA suffering patients. 75 patients wearing the brace for more than a year period were surveyed by clinicians and referring doctors for evaluating their satisfaction level. In parallel, the brace efficiency was evaluated by measuring its effects on pain and medial knee loading. Twenty-four patients with medial knee osteoarthritis (grade II or III) were included. Pain relief, comfort, kinematics and kinetics of the lower limbs during walking were compared with and without knee brace. Data were acquired by an optoelectronic motion analysis system composed of cameras, capture software and markers attached to anatomical landmarks.
The new brace is designed to work by creating a valgus (i.e., distraction between femur and tibia) and apply a slight external rotation to the leg during knee extension. Our clinical experience showed that immediate pain relief was observed with the new brace system. A specific follow-up procedure (1-week, 1-month and 3-month clinical intervention) was adopted and a precise brace adjustment methodology was implemented. Critical success factors were identified. Biomechanical analysis results showed a second peak KAM reduction of - 14% and KAM impulse -8.8%. A 43 % pain relief was observed. These results suggest that compliance, major problem observed in 3-point leverage knee brace use (40 % of patients withdraw brace in the first 3 months) could be favored with the distraction/rotation brace on long-term wear period.
The quite large number of braces delivered, the optimized attribution procedure and adjustment method and biomechanical analysis demonstrated that the new brace has great benefits for pain, symptoms, and daily use among the medial KOA population. The new distraction brace offers advantages in terms of comfort and knee loading during terminal stance and could improve poor compliance with knee brace treatment.
163
Alexander Joseph (1) Louise Tisdale (1) presenting
Maltings Mobility Centre Royal Wolverhampton Trust, Wolverhampton, UK (1)
Development of the Role of the Specialist Physiotherapist in Amputee Rehabilitation to Improve the Quality of Care through the Implementation of Physiotherapist Independent Prescribing
UK Physiotherapists have now been granted with the opportunity to gain independent prescribing rights. Upon qualification they are able to prescribe any licensed medicine from the British National Formulary for any condition within the practitioner’s area of expertise and competence to improve movement, performance and function of individuals on their caseload. (CSP 2013)
To improve the quality of care provided to individuals referred to a regional amputee rehabilitation service through streamlining access to pharmacological treatment of neuropathic pain, musculoskeletal pain and dermatological conditions.
The team developed a Physiotherapist’s Formulary for implementation of independent prescribing upon qualification and subsequent registration with the HCPC as an Independent Prescriber.
Items in the Formulary

The regional amputee rehabilitation service has taken on the development of a highly experienced Physiotherapist as an independent prescriber at the earliest opportunity. Independent Prescribing rights were given to Physiotherapists in England in 2013, with appropriate training made available at the beginning of 2014. Reducing waiting time for review and commencement of appropriate medication will avoid the development of chronic pain and dermataological conditions.
HCPC (2014) http://www.hcpc-uk.org/aboutregistration/standards/standardsforprescribing/
NICE (2013) Neuropathic pain – pharmacological management: The pharmacological management of neuropathic pain in adults in non-specialist settings http://www.nice.org.uk/guidance/CG173
NICE (2013) Clinical Knowledge Summaries-Hyperhidrosis http://cks.nice.org.uk/hyperhidrosis
NICE (2010) Clinical Knowledge Summaries- Analgesia-mild- moderate pain
http://cks.nice.org.uk/analgesia-mild-to-moderate-pain
CSP (2013) Medicines, prescribing and Physiotherapy, 3rd edition. http://www.csp.org.uk/documents/pd019-medicines-prescribing-physiotherapy-3rd-edn?networkid=226227
164
Edwin Iversen (1) presenting Harold Sears (1) Scott Hosie (1) Jeff Christenson (1) Tony Jacobs (1)
Motion Control Inc., Salt Lake City, Utah, USA (1)
Analysis and Gait Lab Testing to investigate the reduction of Loading on Residual Limb and Proximal Joints with Hydraulic Ankle
Individuals with lower limb loss can be subject to higher than normal loading on both sound and affected limbs. Uncorrected, this can lead to premature degeneration of joints and soft tissues. [1,2,3] Although higher loadings can be a result of improper fit or alignment, or lack of proper gait training, the design of prosthetic components can also improve proximal joint loads. This research investigates how the use a hydraulic ankle effects limb loads.
The aim of this research is to investigate the clinical benefits of an advanced prosthetic foot with a hydraulic ankle with near anthropomorphic range of motion. The effects on limb loading and gait patterns for individuals with lower-limb loss will be explored.
A simple mathematical model of the prosthetic limb was developed to predict the theoretical maximum loading at heel strike in the proximal joint due to a hydraulic ankle. For comparison, a gait lab study using an instrumented treadmill measured actual limb loading on an individual with a transtibial amputation, during incline as well as level walking, at self-selected walking speed. Three different feet were compared: a dynamic carbon fiber foot (without hydraulic ankle), a low-range hydraulic ankle (with 9 deg. ankle ROM), and a high-range hydraulic ankle (with 50 deg. ankle ROM).
The mathematical model has shown that forces can theoretically be reduced significantly by use of a dynamic prosthetic foot and a hydraulic ankle with 20 deg. ROM for level walking, and up to 50 deg., especially for walking down inclines. The gait lab study generally validated the theoretical model. (see Fig. 1). Furthermore, the model predicted and the gait lab study validated a decrease in the energy needed to walk up and down inclines and level ground when using a prosthesis with high ROM hydraulic ankle.

This figure shows a 10% lower peak load on the hip joint with a dynamic prosthetic foot with hydraulic ankle compared to a fixed ankle. (Black without hydraulic ankle, Gray with hydraulic ankle)
The theoretical analysis and gait study show that residual and proximal limb loading can be reduced with a hydraulic ankle while walking up and down inclines and on level ground. The research suggests that the range of motion of the hydraulic ankle is important and that having near anthropomorphic ROM of 50 degrees is especially important for reduced shock loading, and stability when walking down inclines.
1. Gailey, Robert, 2008, Department of Veterans Affairs,
165
Harold Sears (1) presenting Edwin Iversen (1) Michael Myers (1) Klaus Biggers (1)
Motion Control, Inc., Salt Lake City, Utah, USA (1)
Force Limiting Auto Grasp (FLAG): A User–Initiated Method for Grip Security of Electric Hands and TDs
High pinch force electric hands and terminal devices (TDs) are difficult to control by the novice wearer, and with 20-25 lb (88-110 N.) pinch force, can exceed even natural hand pinch forces.
New myoelectric TD wearers usually do not have well-developed proportional control, and are very cautious gripping fragile objects using their TD around others, especially children. The goal of this project was to develop a simple, easily enabled force limit technique, so the prosthesis wearer can feel comfortable using their high-force TD, resulting in using their prosthesis more.
Specifications were:
The wearer must be able to turn the feature on/off at will.
Pinch force must be easily limited, and maintained.
Auto Grasp, i.e., automatic response to electrode slip or loss of contact with skin, should occur when needed, but not occur accidentally.
The combination of these features is termed Force Limiting Auto Grasp (FLAG).
FLAG is implemented by integrating additional controls within existing electronic circuits (the ProPlus Controller), supplemented with sensors within the driven fingers in the Hand prosthesis, and the Electric Terminal Device (ETD).
The wearer completes the following sequence to utilize the FLAG feature:
FLAG is enabled with a Hold-Open command for three continuous seconds. An audible and palpable buzz signals the wearer that the FLAG feature is enabled.
The wearer intentionally grips an object – the TD will stop gripping at ~2 lb grip force (9 N). A buzz signals the wearer that the grip force has limited, and the motor turned off.
The wearer may pulse the grip force (by a contraction of the “close” muscle) to increase the pinch force by ~2 lb (9 N). Each pulse provides a buzz, for feedback to the wearer.
To disable FLAG, the wearer performs a Hold-Open command again, for three sec. A double buzz indicates the feature is turned off.
While FLAG is enabled, Auto Grasp will trigger a single additional closing pulse, whenever a very sudden opening signal is created, either by a panic or an electrode slip.
A small scale field trial is providing feedback from actual wearers. A sampling of the total data is shown in Table 1. The data is verifying the kinds of tasks for which the feature is useful to the wearers, how frequently the FLAG is utilized, the ease with which the wearers learn its function, and the problems which may require revision to the design or implementation.

High pinch force can have its downside. Damage to fragile objects, and potential harm to children discourages prosthesis use especially by new wearers. Force Limiting Auto Grasp (FLAG) is shown to increase confidence and usage.
166
Sara Morgan (1) presenting Valerie Kelly (1) Rana Salem (1) Brian Hafner (1)
University of Washington, Seattle, WA, USA (1)
Self-report of cognitive concerns in people with lower limb loss
Loss of a limb has traditionally been viewed as a musculoskeletal condition. However, lower limb loss (LLL) has also been associated with presence of cognitive impairment.1 One limitation to prior studies is that studied participants were primarily persons with comorbid dysvascular conditions (e.g., diabetes) and rarely included persons with amputation from traumatic etiology. As such, differences in CI among people with different etiologies of amputation are unknown. Further, prior research most often assessed cognitive difficulties from the perspective of health care providers, rather than people with LLL themselves.1
To estimate the prevalence and severity of cognitive concerns in persons with LLL by comparing self-reported cognitive difficulties to normative scores. Presence of cognitive concerns by etiology was also examined to assess the relationship between etiology and cognition.
Adult prosthetic limb users with unilateral LLL from dysvascular or traumatic causes were recruited to participate in a cross-sectional study. Each participant completed a one-time paper or electronic survey that included the NeuroQoL Applied Cognition General Concerns (NeuroQoL AC-GC) instrument.2 NeuroQoL AC-GC is an 8-item survey that measures perceived difficulties with cognitive processes (e.g., memory). NeuroQoL scores were compared to normative sample scores (i.e., a T-Score of 50) using one-sample t-tests. Data were then compared by etiology using t-tests to assess differences between groups. The threshold for significance was set at 0.05.

Participants (n=1086) were an average of 55 (SD=13) years old. The majority were male (71%) and had at least a high school education (70%). Over half of the sample had amputation from traumatic causes (55%) and most had an amputation at the transtibial level (65%). On average, participants’ most recent amputation occurred 12 (SD=14) years prior.
People with LLL reported significantly more difficulties with cognition than the normative sample (p<0.001). Subgroups defined by age and etiology had significantly different NeuroQoL AC-GC scores from the normative sample (both p<0.001), but not significantly different from each other (p>0.05).
Overall, people with LLL report concerns with cognitive function. NeuroQoL AC-GC scores are approximately 0.4 SD lower in people with LLL compared to a normative sample based on the U.S. general population. One-half SD has been demonstrated as an acceptable estimate for meaningful difference across outcome measures.3 Additionally, people with LLL from dysvascular causes report similar difficulties with cognition than do those with amputation from traumatic etiology. This result may indicate that concerns with cognitive function are not solely associated with dysvascular comorbidities, but are common to many people with LLL.
1. Coffey, L. Disabil & Rehab. 34(23), 1950-64, 2012.
2. Cella, D. Neurology. 78, 1860-67, 2012.
3. Norman, G.R. Medical Care. 41(5), 582-92, 2003.
167
Sara Morgan (1) presenting Robert Askew (2) Brian Hafner (1)
University of Washington, Seattle, WA, USA (1) Northwestern University, Chicago, IL, USA (2)
Equivalence of electronic and paper administration for four self-report instruments used in prosthetic clinical care
Evidence of mode-of-administration equivalence is needed to demonstrate that scores obtained from different methods of administration (e.g., paper or electronic) are directly comparable.1 Electronic survey administration offers numerous benefits compared to paper surveys, including automated and accurate scoring and direct import into a medical or research record. Evidence of paper-electronic equivalence would also allow administrators to choose the format most appropriate for the respondent (e.g., patient).
The purpose of this study was to evaluate equivalence between paper and electronic modes of administration for four self-report outcome instruments: Activities-Specific Balance Confidence Scale (ABC), Prosthetic Evaluation Questionnaire- Mobility Subscale (PEQ-MS), Prosthetic Limb Users Survey of Mobility (PLUS-M), and Socket Comfort Score (SCS).
Mode of administration equivalence was evaluated by administering two surveys to participants via one or both methods (i.e., paper and electronic) over a 48-72 hour period. Participants were randomly assigned to one of three study arms based on modes of administration (i.e., paper, electronic, and mixed). Eligibility criteria included being over 18 years old, having unilateral lower limb loss, access to the internet, and the ability to read, write, and understand English. Intraclass correlation coefficients (ICCs) and 95% confidence intervals (CIs) were estimated and compared across groups differing by mode of administration to evaluate equivalence.1
Participants (n=201) were predominantly male (67%), white (91%), and had a mean age of 60 years. Etiology of amputation varied across participants, with most reporting either traumatic causes (60%) or dysvascular (23%) complications. The majority of the sample had an amputation at the transtibial level (65%). ICCs and the 95% Cis by mode for the four measures are reported in Table 1. With the exception of the SCS, ICCs were similar across modes of administration.
Mean scores, ICCs, and 95% CIs for the ABC, PEQ-MS, PLUS-M, and SCS

Differences in mean scores between modes of administration were small for the ABC, PEQ-MS, PLUS-M, and SCS (less than 2% of the scale range). Comparisons of ICCs and 95% CIs indicate measurement equivalence across paper, electronic, and mixed models of administration for all measures. While all modes appeared to be statistically equivalent for the SCS, clinicians and researchers should use caution when employing mixed modes of administration for this measure due to the lower overall reliability observed in the mixed-mode study group.
1. Coons, S. Value in Health. 12(4), 419-429, 2009.
168
Junji Katsuhira (1,2) presenting Nodoka Miura (1) Yuji Ohmura (1) Tadashi Yasui (3) Masahiro Tosha (3) Sumiko Yamamoto (2)
International University of Health and Welfare, Odawara, Japan (1) Graduate school of International University of Health and Welfare, Tokyo, Japan (2) Kawamura-Gishi Company, Ltd, Osaka, Japan (3)
Synergetic effects of a newly designed trunk orthosis with joints providing resistive force and an ankle-foot orthosis with an oil damper in adults with post-stroke hemiparesis
We developed a newly-designed trunk orthosis (NDO) that provides resistive force through spring joints and the trunk orthosis contributed to improve gait performance in pre-swing of hemiparetic patients1). Also, an ankle-foot orthosis with an oil damper (AFOD) is widely used in Japan to mainly improve gait performance in initial contact and loading response. However, synergetic effects of the NDO and the AFOD are still unclear.
The purpose of this study is to examine the biomechanical synergetic effects of a NDO and an AFOD in adults with post-stroke hemiparesis.
Participants were 13 stroke patients in the chronic phase. We randomly allocated patients into two groups: six patients wearing a corset and an AFOD and 7 patients wearing a NDO and an AFOD. We recorded gait data using a three-dimensional motion capture system consisting of nine infrared cameras and four force plates. First, we measured gait wearing an AFOD without any trunk orthosis at the patient’s selected speed. Next, after the patient put on any of the trunk orthosis which were a corset or a NDO and practiced wearing it for 10 min, we measured gait with any of the trunk orthosis. After this measurement, the patient removed the trunk orthosis and we recorded gait immediately using the same protocol.
Gait speed in condition of wearing a NDO and after removal of it were significantly faster than that before wearing it (p<0.05). Also, step length of a paretic limb in condition of after removal of a NDO was significantly larger than that before wearing it. In addition, some of the patients increased paretic ankle plantar flexion moment in pre-swing and others increased paretic hip flexion moment in the same period in condition of wearing a NDO and after removal of it. In contrast, no significant difference was observed between conditions in a corset wearing group.
In our previous study1), paretic step length and hip flexion moment in pre-swing significantly increased in only condition of after the NDO removal without any ankle foot orthosis but not in gait speed. In the present study, wearing both the NDO and the AFOD led to increase of gait speed and the increase was maintained in condition after the NDO removal. Synergic effect of the NDO and the AFOD might have contributed to increases of paretic hip flexors and plantar flexors and this effect could have increased gait speed of hemiparetic patients.
169
M. Jason Highsmith (1) presenting Jason T. Kahle (1)
University of South Florida, Tampa, FL, USA (1)
Functional Effects of the Genium Knee in Transfemoral Amputees Measured with the Continuous Scale Physical Functional Performance-10 (CS-PFP10) Assessment
Home and community simulation obstacle courses are the extent to which functional benefits of microprocessor knees (MPKs) have been evaluated. In these simulations, C-Leg use generally improved function compared with non-MPKs. These studies had numerous methodologic issues. Improved methodologic quality and selection of outcome measures are clearly indicated. Preliminary data with the Genium knee shows gait improvements, however there is no data on potential integrated functional benefits.
This aim of this study was to improve methodologic quality over prior MPK functional studies and to determine if Genium provides advantages in functional abilities compared to C-Leg.
The IRB approved study used a randomized cross-over design (C-Leg and Genium) and a sample of non-amputee controls. Unilateral TFAs who used C-Leg (≥1y) were recruited. All subjects were 18-85y and free of medical comorbidities. TFAs’ preferred sockets were retained and prostheses were fitted with a study foot. Component alignment was set to specification. Subjects were trained and accommodated with each component. After data collection, knees were crossed-over and the process repeated. CS-PFP10 was administered via standardized procedure. CS-PFP10 scores 10 ADLs in time, distance, and mass and reflects physiologic functional domains. Raw data convert to summary scores with a validated algorithm (licensed software). Scaled from 0-100, summary scores include CS-PFP total score (CS-PFP TOT) and 5 physiologic domain scores: upper/lower body strength (UBS/LBS) & flexibility (UBF), balance & coordination (BAL), & endurance (END).
Paired t-tests were used to compare between-knees and independent samples t-tests to compare with controls (normally distributed data; otherwise Wilcoxon’s Signed-Rank test used). Effect size(ES) was also (Cohen’s d). The a priori significance level was p≤0.05.
20 traumatic TFAs (age: 46.5y±14.2) and 5 controls (age: 57.2y±15.7) completed the study. Alignment was consistent between knees. UBF score improved (7.0%, p=0.01, ES=0.45) when subjects used Genium compared with C-Leg. BAL and END scores also improved with Genium use [(7.6%; p=0.03, ES=0.28) & (8.4%; p=0.02, ES=0.32) respectively]. CS-PFP total score improved 7.4% (p=0.03, ES=0.28) with Genium use.
Controls scored higher than TFAs in all domains. No statistically significant difference was found between controls and TFAs when using Genium except in END (22.4%; p=0.05). Controls scored higher in 4/5 domains (except UBS), compared to TFAs when using C-Leg. The smallest difference in this comparison was UBF (13.4%; p=0.01) whereas the largest was END (28.9%; p=0.01).
There were no significant differences in UBS between controls and TFAs. Genium use improved total CS-PFP scores likely due to improved confidence, willingness to lift and carry greater mass and move faster in activities from UBF, BAL and END domains. In LBS, UBF, and BAL domains, C-Leg use resulted in scores lower than controls. END was the only domain where Genium use significantly improved function compared to C-Leg, while both conditions were still lower than controls. In total CS-PFP, controls had significantly higher scores than TFAs using C-Leg. Regardless of knee condition, TFAs did not equal or surpass controls in any functional domain, suggesting room for improved TFA functional performance.
Seymour R DJ et al. POI; 31; 2007.
Theeven P et al. J Rehabil Med. 43; 2011.
Meier MR et al. JRRD; 49; 2012.
Cress ME et al. PTJ; 85; 2005.
170
John Cagle (1) presenting Brian Hafner (1) Joan Sanders (1)
University of Washington, Seattle, WA, USA (1)
Prosthetic Liner Assistant (PLA): An online database to facilitate individualized liner selection
At present, there are more than 60 commercially-available prosthetic liners on the market. Given the large number of products to choose from, liner selection can be a challenging task for prosthetists. In absence of objective and comparable technical data, liner selection often becomes an uncertain process that depends largely on clinical experience with each product.1 Evidence-based tools are therefore needed to assist practitioners in comparing and selecting liners for each individual patient.
The purpose of this research is to develop an intuitive and accessible database of liner properties that clinical prosthetists can use to evaluate a patient’s existing liner and identify potential alternatives.
Each of 20 liners from 7 different manufacturers was evaluated across 7 properties inherent to prosthetic liners, including compressive resistance, shear resistance, stretch resistance, adherence, volume accommodation, thermal conductivity, and cost. Relative results are displayed in a flexible graphical user interface (GUI) that allows practitioners to select a patient’s current liner and compare it to others liners, sorting by desired property. The selected properties were derived from test protocols established by the American Society for Testing and Materials (ASTM). Details of the test methods and clinical relevance of each material property were developed and incorporated into the GUI to facilitate selection.
Liners currently included in the PLA (www.linerassit.org) are categorized by their material types (e.g., thermoplastic elastomer (TPE), silicone elastomer, copolymer, and polyurethane). In general, silicone and urethane liners have the highest compressive resistance, while TPE and copolymer have the lowest. Fabric backings have a moderate impact on compressive resistance and a significant impact on stretch resistance. Adherence (coefficient of friction) is strongly dependent on the material surface finish and does not correlate directly with base material. However, TPE consistently has the highest adherence and polyurethane the lowest.

Differences between liners are often ambiguous. The PLA is a freely and easily accessible tool that can be used in practitioner-patient interactions to help determine if existing limb discomfort might be a result of the liner, and presents the practitioner with an interactive list of liner alternatives. The PLA synthesizes objective data with a practitioner’s clinical experience to enhance the fitting process.
1. Klute et al. Prosthet Orthot Int. 2010; 34(2):146-53.
172
Joan Sanders (1) presenting John Cagle (1) Brian Hafner (1)
University of Washington, Seattle, WA, USA (1)
Day to day variability in residual limb fluid volume change
Many prosthesis users have difficulty managing daily volume changes in their residual limb. Part of the difficulty may be that they experience different volume changes from one day to the next, even when their activity patterns are consistent. Because clinical socket fit is detrimentally affected by small fluid volume changes as low as 1%1, even slight differences in volume fluctuation from day to day may affect a person’s comfort and ability to ambulate. People with peripheral arterial disease (PAD) would be expected especially affected because of their compromised physiological condition.
The purpose of this research was to evaluate limb fluid changes experienced by participants with transtibial amputation across different days. We sought to determine if participants experienced consistent changes in their limb fluid volume. In other words, we wanted to see if a participant lost volume across test days or if the person lost volume some days and gained volume on other days. We also assessed if people who experienced day to day differences in the direction of their limb fluid volume changes had PAD.
Limb fluid volume was monitoring on a group of transtibial amputee participants using a custom instrument described previously2. On three separate test days, subjects were asked to conduct three cycles of: resting (sitting) for 90 seconds, standing for 90 seconds, and walking for 5 minutes. Tests were all conducted in the late morning or early afternoon and participants were instructed to maintain a similar routine prior to testing (e.g., eat a similar breakfast). The overall direction of residual limb fluid volume change from the beginning to the end of the test session and the fluid volume changes during each of the three activities (resting, standing, and walking) were compared across test days.
A total of 15 subjects participated in the study, 12 male and 3 female. Four subjects were diagnosed with PAD. Test results are summarized in the table below.

The result that 20% of participants (3 of 15) demonstrated day to day variations in the direction of their session fluid volume changes points to the importance of understanding individual characteristics that may affect socket fit. Surprisingly, none of those 3 participants had PAD. Walk results that all 3 subjects with day to day variations had PAD, however, are consistent with expectation; PAD is associated with compromised and inconsistent vascular drive during activity.
1 Sanders et al. J Rehabil Res Dev. 2012; 49(4):567-582.
2 Sanders et al. Prosthet Orthot Int. 2014 (submitted).
173
John Cagle (1) presenting Krittika D’Silva (1) Brian Hafner (1) Daniel Harrison (1) Joan Sanders (1)
University of Washington, Seattle WA, USA (1)
Is the thickness of used prosthetic socks related to their age?
Prosthetic socks allow patients who use a prosthesis to manage short- and long-term changes in residual limb volume. Prior research has shown that ply is not a direct indication of new sock thickness across different materials.1 Further, stacked new socks differ in thickness from single new socks of equivalent ply.2 It is expected that sock thickness also changes over time (and use), but the effect has yet to be quantified.
This study was conducted to examine the effect of normal use on sock thickness and elasticity.
Subjects: 20 amputee volunteers donated 42 used socks over a 9 month period. Sock age ranged from 0.5 to 60 months (Mean 8, SD 14) and ply ranged from 1 to 6 (Mean 3, SD 2).
Procedures: The axial and circumferential stretch of each sock was measured while it was donned by the donor. Socks were then doffed and placed into a knitting hoop, replicating the donned stretch. Thickness was measured at pressures ranging from 4 to 100 kPa using a custom testing apparatus and method described in a previous publication.1 Thicknesses of used socks were compared to equivalent new socks (i.e., same manufacturer, product, and ply and comparably stretched to simulate a donned condition).
The mean total in-plane biaxial donned stretch was 20 ± 14 percent for used 1-ply socks, 15 ± 9 percent for used 3-ply socks, and 15 ± 15 percent for used 5-ply socks. Across all used socks, the mean axial stretch was 15 ± 15 percent while the mean radial stretch was 19 ± 9 percent.
Age was not a strong predictor of sock thickness. On average, socks were 75 ± 17 percent of their initial thickness after one month while socks older than one month were 72 ± 18 percent of their initial thickness. Across all used socks, mean thickness at 100 kPa was 0.5 ± 0.2 mm for 1-ply socks, 0.9 ± 0.3 mm for 3-ply socks, and 1.2 ± 0.3 mm for 5-ply socks.
Results from this and prior research show that it may be difficult for prosthetists to accurately assess socket fit based on sock ply alone. There was large variability and overlap in measured thickness between 5-ply and 3-ply used socks. An instrument that could quickly and easily take a single thickness measurement of a prosthetic sock (new or used) would offer clinicians meaningful insight into their patients’ volume accommodation needs. Such an instrument would provide clinicians a quantitative method for evaluating patients’ current socket fits.
1. Sanders et al. Prosthet Orthot Int. 2012; 36(1):77-86.
2. Cagle et al. Prosthet Orthot Int. 2014; 38(5):405-12.
174
Christian Redd (1) David Gardner (1) John Cagle (1) Joan Sanders (1) presenting
University of Washiington, Seattle WA, USA (1)
Monitoring donning and doffing with subject activity in transtibial amputee prosthesis users
Monitoring activity patterns on patients with limb loss has been suggested to provide useful insight to practitioners in their clinic care1. Adding detection of donning and doffing events may extend the utility of activity monitoring, particularly as related to limb volume management. Practitioners prescribing temporary doffing of the prosthesis during the day, a technique shown to facilitate limb fluid volume recovery in transtibial amputee prosthesis users2, may use donning and doffing event information to help their patients optimize accommodation practices and enhance comfort and satisfaction with the prosthesis.
The purpose of this research was to develop a small portable means to accurately monitor sitting, standing, ambulation, and donning and doffing events on people with transtibial limb loss.
Residual limb presence within the socket (donned prosthesis) was detected using two small infrared proximity sensors (QRE1113, Fairchild Semiconductor) housed in small custom made jigs that affixed to the lateral and medial socket brim. Durations of sitting, standing, and walking were monitored using two Actigraph GT3X+ sensors (ActiLife), one affixed to the pylon between the socket and foot and one wrapped to the thigh with a Velcro strap. Data from the two proximity sensors and 3-axis accelerometers were used in a processing algorithm to distinguish donning, doffing, sitting, standing, and ambulation. Initial verification testing was conducted on 11 transtibial amputee participants performing a 40 minute test session with numerous changes of posture and activity as well as at least 2 donning and doffing events. A timer, hand-written notes, and a video camera were used for ground truth comparison. A second evaluation was conducted by monitoring 28 participants while they left the laboratory for approximately 3 hours. The algorithm was enhanced to distinguish bouts of riding in a vehicle with bouts of ambulatory activity. Subjects were queried upon return about their activities and approximate durations. Comparisons were made between with sensor data classified with the algorithm and subject reported activities.
In both the controlled study and field test, the system accurately identified all donning and doffing events, and categorized ordering of all activities (sitting, standing, walking) correctly. In the controlled study the average difference across the 11 sessions between timer/notes results and sensor data classified with the algorithm was 0.35 min (SD 0.17 min) for sitting, 0.33 min (SD 0.30 min) for standing, and 0.23 min (SD 0.17 min) for walking.
Differences in results for the initial verification test are likely due to the weak resolution of the ground truth data collected with the timer, notes, and camera. The ease with which the algorithm classified sensor data during field testing demonstrate its effectiveness for prosthetic application. Reducing the size of the system is a next step towards regular use in clinical prosthetics care.
1 Dudek et al. J. Rehabil. Res. Dev. 2008; 45(4):577-585.
2 Sanders et al. Prosthet. Orthot. Int. 2014 (submitted)
175
Sol-Bi Kim (1) Jeicheong Ryu (1) Jin Ho Son (1) Sungjae Kang (1) Museong Mun (1) Chang-Yong Ko (1) presenting
Korea Orthopedics & Rehabilitation Engineering Center, Incheon, Republic of Korea (1)
Enhancement of knee range of motion and gait features in a trans-tibial amputee with knee flexion contractures via an adaptive training for an assistive device program
An electric shock causes knee flexion contractures (KFC) as well as tissue damages, leading to amputation of lower extremities. The amputees with KFC are difficult to walk with wearing prosthesis. An adaptive training for an assistive device (ATAD) program is administered to rapidly adapt prosthesis and improve gait features. However, there is little study on ATAD’s effects on trans-tibial amputees with KFC.
This study aimed to verify whether ATAD program can release in a trans-tibial amputee with KFC by an electric shock and enhance gait features.
A trans-tibial amputee with KFC caused by an electric shock was involved. The amputee was administrated ATAD program by an interdisciplinary team consists of several experts like biomedical/biomechanical engineers, CPOs, physiotherapists, medical doctors, etc. During ATAD program, the amputee conducted neither surgery nor drug treatments to release his KFC. Detailed contents of ATAD program were planned according to the amputee’s accomplishments. Before and during ATAD program, gait analysis, functional gait abilities, and range of motion (ROM) of the knee joint were evaluated every 4 weeks. Additionally, the quality of life (QoL) was evaluated by using SF-36.
ROM of the knee joint was increased. Temporal-spatial parameters of gait were continuously improved over time; increase in cadence, speed, stride length, step width, and swing time and decrease in stance time. Effective limb length was increased over time. Center of mass in medial-leteral direction was biased toward sound leg at baseline and was shifted into between sound and amputed leg. Furthermore, QoL was improved for both the amputee and his wife.

Photographs at mid-stance, left: before ATAD program, right : after ATAT program for 14 weeks
As a result, the gait traning of ATAD program can attribute release of KFC and enhancement of gait features without any surgery and drug treatments for a transtibial amputee with KFC, leading to improvement of QoL for his family as well as the amputee. Therefore, ATAD program is likely to be effective method for a transtibial amputee with KFC.
176
Inger-Marie Starholm (1) presenting Terje Gjøvaag (1)
Oslo and Akershus University College of Applied Sciences, Oslo, Norway (1)
The oxygen cost of walking is not a good measure for quantifying the physical effort of prosthetic ambulation
The oxygen uptake (VO2) during walking is widely recognized as a measure of the whole body energy expenditure, while the oxygen cost of walking (Cw; ml kg-1meter-1) is regarded as a measure for quantifying the actual effort exerted (1). Transfemoral amputees (TFA) have slower preferred walking speeds (PWS) than healthy subjects (CON) (2), but when walking with their respective PWS, the VO2 of the TFA and CON are similar (2). Thus, the importance of using Cw as a measure of physical effort is questioned.
Investigate if the effort of prosthetic ambulation is better described by relating the oxygen uptake during floor walking to the maximal aerobic capacity (% VO2max) of the TFA.
A group of unilateral TFA (n=8) and a group of healthy age matched subjects (n=8) were recruited to the present study. Oxygen uptake (VO2) was measured during steady state conditions by a portable oxygen analyzer (Cortex Metamax 3B, Germany) when the subjects were walking along a 40 meter indoor track and on a treadmill (Woodway, ELG70, Germany). Walking speed was controlled by an optical gait analysis system (OptoGait, Italy). VO2max was measured by an incremental treadmill test to voluntary exhaustion. The Cw was calculated as relative oxygen uptake divided on the subjects walking speed. % VO2max is the percent oxygen utilization of the maximal aerobic capacity (VO2max) at the PWS.
Energy expenditure of transfemoral amputees (TFA) and healthy controls (CON) during floor walking at their preferred walking speed (PWS).

TFA vs. CON; †† p < 0.01, †††p < 0.001.
The mean ± SD VO2max of the CON group was 49.0 ± 14.4 mL kg-1 min-1, and significantly higher (p < 0.05) compared to the TFA (30.6 ± 8.7 mL kg-1 min-1). Compared to the CON, walking speed was lower (p < 0.01), while the Cw was higher (p <0.001) for the TFA. VO2 was similar for the TFA and CON. The percent utilization of VO2max was substantially higher for the TFA compared to the CON (p < 0.001).
There was no significant difference in VO2 between the TFA and CON walking on floor and treadmill, but due to a lower PWS of the TFA, their oxygen cost of walking (Cw) was higher compared to the CON. Thus, the Cw is too influenced by the walking speed to accurately reflect the physical effort of prosthetic ambulation. The %VO2 max reflects the relative utilization of the individuals’ maximal aerobic capacity and thus is a good indicator of the actual effort exerted during activity.
% of VO₂ max is a more adequate measurement for physical effort than the Cw
1. Traballesi et al. Gait and Posture 27: 70-75, 2008
2. Gjovaag and Starholm. Prosthetic Ort. Int 38(2): 140-147, 2014
177
Evgueni Dukendjiev (1) Vera Lavretskaya (1) Tatiana Dukendjieva (1) presenting
Atypical Prosthetics Laboratory, Riga, Latvia (1)
Robotized complexes for home abilitation and rehabilitation of children with cerebral and spinal diseases
The present report considers the world’s only robotized complexes BIONIKA-I (crawling and walking on all fours) and BIONIKA-II (two-leg walking), which are used in domestic conditions and controlled by parents. BIONIKA-I and BIONIKA-II creates for the child an image of symmetrical quasi-walking accompanied by a forced bending of the axial skeleton in all three planes by forced movements of body and extremities.
By Imperative locomotion by means of numerous repetitions and muscle strengthening to gradually involve the child into the training process, creating the conditionally reflex movement synergies.
A method is used of compensating the deficiency of muscular and controlling activity by external energy. BIONIKA-I creates for the child in the horizontal plane – swimming and crawling, and then in both horizontal and vertical plane - walking on all four by forced movements of head and extremities. BIONIKA-II by means of a whole-body reciprocal system generated for the patient, who has stepped on the treadmill, an image of asymmetrical two-leg walking.
Forced movements through the use of external energy in the absence of supraspinal influence, due to the plasticity of cerebral structures and the ability of autogeneration, lead to the adaption for motoric activity. Locomotions with the body weight support to a significant extent train children with cerebral paralysis and cerebrospinal diseases in purposeful movements. Central nervous system gradually makes new paths by which the brain commands reach the extremities. Trying the method and BIONIKA robots with 12 patients, the authors have found out a considerable reduction in the time of motive abilitation and rehabilitation compare to traditional remedial gymnastics.
the imperative locomotion has accelerated the process of restoring or learning the skills of standing, crawling and walking; metabolism of the child has been improved and a powerful psychoemotional occurred, increasing the independent motion in space. It should be particularly noted that all these processes were carried out in domestic conditions.
For the first time a robotized complex has been created for swimming, crawling and walking on all four movements imitation . The tests have demonstrated the promising outlook of this direction in abilitation and rehabilitation. BIONIKA-II complex ensures the two-leg walking, completing the evolutional stages in development of locomotion.
[1] Dukendjiev E. Rehabilitacijas lokomotora robots . Patienta pieteikums Nr.P-12-15, 31.01.2012.
[2] Dukendjiev E. Rehabilitacijas lokomotora robots . Patienta pieteikums Nr.P-12-59, 16.04.2012
178
Kerstin Caine-Winterberger (1) presenting Rickard Brånemark (1)
Sahlgrenska University Hospital, Gothenburg, Sweden (1)
Long term follow up of Osseo-integrated prosthesis for transmetacarpal I amputation
One of the most common traumatic amputations is at the fingers level. According to an epidemiologic study in Maryland, USA fingers amputations accounted for 52.7% of all amputations. A similar study from the Swedish Hospital Discharge Register found that 77% relate to wrist and hand amputation. Thumb amputation can be treated surgically by transplantation, pollicization, toe-to-thumb transplantation, lengthening procedures, using osteocuteneous flaps or an osseointegrated implant.
To analyse and describe hand-function and prosthetic use in patients treated with bone anchored thumb prosthesis.
This was a retrospective study, from 1990 to 2013, consisting of 12 patients with thumb amputation at metacarpal level. The procedure consists of two surgeries. A threaded titanium implant is inserted into the residual bone. At the second operation, 4 months later, the abutment is inserted into the fixture and secured with a screw. Range of motion was exercised postoperatively, when oedema was diminished (Jönsson, Caine-Winterberger, & Brånemark, 2011). Three months later the patients starts strengthening exercises, full active motion is allowed and light ADL-activities can be commenced. To measure hand-function Jamar, pinch-dynamometer, monofilaments, goniometer and Sollermans’s grip-function-test were used.

Seven out of 12 transmetacarpal amputees with osseointegrated thumb prostheses were tested. One patient was deceased, 3 had lost their implants and one patient lives abroad and is lost to follow-up. Only one patient has chosen not to use his prosthesis. All patients were able to feel sensation in their OI prosthesis from 2,83 to 6,65 measured with monofilament. Hand-function was 95% of normal function measured with Sollerman’s grip-function test.
Functionality was graded from very low to excellent (1-5) with the mean value 4,1 and quality of life 4,3.
Three of the patients who lost their implants were operated before 2005, before the standardised protocol was used. Seven out of 8 are prosthetic users and use their prosthesis 8 and 24 hours per day. They have 66, 6 % of grip-strength compared with unaffected hand, 95% of hand-function and measurable sensation via the osseointegrated prosthesis. Patient rated functionality and quality of life with osseointegrated prosthesis between good and excellent.
179
Pascal POMMIER (1) Kévin DANIGO (1) presenting
Pommier Orthopédie, villebon sur yvette, France (1)
Dynamic silicone socket technology for above knee amputees
Comfort, autonomy, improvement of the capacities of a patient are the desired goals when fitting a prosthesis. The socket, interface between the patient and his prosthesis, becomes the key element to reach these goals. But constraints associated with wearing conventional sockets (difficulties with donning, volume variations of the stump poorly tolerated by the socket, discomfort including sitting position…) drive us to make the technology evolve.
The aim was to create a concept and an auto-adaptive socket technology able to solve the various problems commonly encountered when fitting above knee prosthesis, into improve patient’s quality of life.
We therefore designed a socket capable of self-shaping in all planes of motion to allow free globulization of stump muscles. It is entirely made of silicone and includes a dynamic structure that allows energy restitution. To date, about 40 patients of different ages, various pathologies and stump forms (tonic or flaccid) are equipped with this new technology on which we are leading tests since 3 years. We have developed an associated specific cast technique that brings us more physiognomic socket forms.

The flexibility of the socket allows the patient to don it without technical assistance such as a liner or a donning sheath. Comfort is improved due to the reduction of support constraints and pressure, notably in sitting position : deformation of the socket brings a better equilibrium of the pelvis, avoiding inconvenience and dorsolumbar pain. Muscular work isn’t constrained during the walk, so have we noticed an increase of muscles tone, that gives the patient a better control of his walk. Daily stump volume variations are well tolerated by the socket. Energy restitution due to the internal structure of the socket brings an absorption of musculoskeletal shocks and a more fluid and dynamic walk. Autonomy is therefore increased. Proprioception and sensations through the socket are better felt by the patient.
A clinical and scientific walk study is currently conducted into bring out the service provided to patients. As the dynamic silicone socket brings a real profit to above knee patients, we can wonder if this concept is relevant for below knee amputees. Are the inherent constraints of these kinds of amputation an obstacle ? In this way, a feasability study is being carried.
181
James Gardiner (1) presenting Laurence Kenney (1) David Howard (1)
University of Salford, Salford, UK (1)
Meta-analysis of metabolic cost of amputee walking shows only a marginal improvement in cost when using ESR feet compared to conventional SACH feet
Energy storage and return (ESR) prosthetic feet are designed to store strain energy during stance and release that energy during push-off and, hence, promote a more energy efficient gait. However, despite ESR feet being prescribed for approximately thirty years, most previous studies have not provided statistically significant evidence that they reduce the metabolic cost of amputee walking.
We report a meta-analysis of previously published data with the aim of providing a definitive answer to whether ESR feet result in more energy efficient amputee walking than conventional solid ankle cushioned heel (SACH) feet.
We normalised data from previously published studies so that these data could be combined to provide a larger sample and, hence, achieve statistically significant results. Since the majority of amputee metabolic cost studies don’t include a non-amputee control group, we normalised the data by dividing the cost of amputee walking with ESR feet by the cost with SACH feet, using data from the same study. This removed protocol bias and thus allowed statistical tests using the combined data from the previous studies. Additionally the normalised data was tested for a relationship with speed; since we hypothesised that ESR feet might perform better at higher speeds.
The raw data from previous studies for any given foot type is difficult to interpret due to variations in protocol causing considerable variability amongst the results from different studies (figure A). This highlights the importance of normalising the cost of walking when combining results from different studies (figure B). After doing this, we found a statistically significant difference between ESR and SACH feet. However the magnitude of this difference was relatively minor, with the cost of walking with ESR feet (figure B: dashed line) being 96.8% (p < 0.001) of that with SACH feet (figure B: solid line). No relationship between normalised cost of walking and speed was found.

These results suggest that, in general, ESR feet are not effective at improving the metabolic cost of amputee walking to a clinically relevant degree. The failure of passive ESR feet to improve the cost of walking is likely related to their inability to plantarflex beyond their neutral ankle angle; so that they are unable to provide significant push-off at the end of stance. Future designs of prosthetic feet should focus on providing push-off in a manner similar to a healthy intact ankle and foot.
182
Ayaka Nakasho (1) presenting Yaeko Shibata (1) Jumpei OBA (2) Futoshi Mizobe (1) Takaaki Chin (1) Makiko Okamoto (1) Nobuyuki Honda (1) Yu Ando (1) Yuka Mouri (1)
Hyogo Rehabilitation Center, Kobe,Hyogo, Japan (1) Kobe Gakuin University, Kobe,Hyogo, Japan (2)
Study of the support system for children using myoelectric arm prosthesis for daily activities-exchange between children and parents
We have been engaged in the myoelectric arm prosthesis approach for children at the Hyogo Prefecture Rehabilitation Center in Japan since 2002. We have provided support centered on individual training according to the stage of development and life task. Thus, we felt the importance of a platform to interchange findings on how others are engaged with this approach, what methods of use will become possible in the future and so on, for children and their guardians to more actively consider the option of “daily living using a myoelectric arm prosthesis”.
For children that are undergoing training to operate a myoelectric arm prosthesis experience using the prosthesis to play while interacting with other friends. This is to expand the range of use of the prosthesis, improve operating skill and so on. Moreover, as their friends also know that they use a prosthesis, they can proactively seize the opportunity to use the prosthesis. When the guardians know the correct information, they can exchange opinions amongst each other which is linked to resolution of distress and anxiety. This provides an opportunity to examine their reactions towards their children.
A parent exchange event on a holiday for families of children undergoing training of the myoelectric arm prosthesis at this center was announced. Families that desired to participate in the event where the subjects and the site was this center where the event was held for about 6 hours from morning until the afternoon. The program, which consisted of a short training course, was provided for the children to play using a prosthetic arm and for the guardians to exchange opinions and enrich their knowledge. This event was held in 2013 and 2014.
Participants comprised 24 families in 2013, 20 families in 2014. Children were seen to play actively using a prosthetic arm, wore the prosthetic arm longer than usual (without disliking it), and made friends. Though the guardians could exchange information based on experiences, they gave affirmative opinions regarding daily distress and use of prosthesis in the future.
Exchange events are platforms where children can enjoy using prosthetic arms and guardians can deepen their understanding regarding the use of myoelectric arm prosthesis. In addition to individual training, providing such opportunities will either promote the use of myoelectric arm prosthesis or create opportunities to select such usage. Thus, it is preferable for these participants to form a self-help group where they can be exchanging information while investigating ways of making life easier.
183
Jumpei OBA (1) presenting Yaeko Shibata (2) Futoshi Mizobe (2) Ayaka Nakasho (2) Takaaki Chin (2) Akio Nakagawa (1) Akito Masuda (3) Yuka Mouri (2) Yu Ando (2) Makiko Okamoto (2) Nobuyuki Honda (2)
Kobe Gakuin university, Kobe,Hyogo, Japan (1) Hyogo Rehabilitaion Center, Kobe,Hyogo, Japan (2) Kinki-Gishi, Kobe,Hyogo, Japan (3)
Necessity of parents of children that use myoelectric hand to experience using myoelectric hand
We are engaged in the myoelectric hand approach for children. To date, approximately 50 children.The approach towards children requires the cooperation and understanding of the parents. We are involved not only in children’s use of a myoelectric hand but also actively engaging parents also. Though parents are involved cooperatively in children’s training with myoelectric hand, to date, parents have hardly experienced using myoelectric hand personally.
The aim was to investigate the need for parents whose children are being trained with myoelectric hand to experience operating a myoelectric hand.
The subjects were parents of children undergoing training with myoelectric hand. Subjects completed in advance a questionnaire on status of experiencing operating a myoelectric hand by gender and age, feeling towards experience the operation of a myoelectric hand, and attitude towards their child using a myoelectric hand. Next, subjects wore and operated a simulated myoelectric hand. Then, they completed a questionnaire on the ease of operating a myoelectric hand and changes in their attitude from then on towards their child who is using a myoelectric hand.
Twenty seven subjects gave their consent and cooperated in this investigation. Subjects comprised 20 females and 7 males. Mean age was 36±6.97 years. No subject had experienced operating a myoelectric hand and 80% expressed interest in having such experience. After experiencing operating a myoelectric hand, 81% felt it difficult to operate the prosthesis. Feelings of the subjects were ‘I now respect my child’, ‘I will support my child more from now’ and so on. Moreover, 81% responded that attitudes towards children when using a myoelectric hand will change. Details of the attitudes were ‘praise’, ‘I will wait until you can operate it, ‘happily connect the prosthesis to the child’ and so on.
The parents were interested in experiencing operating a myoelectric hand and from such experience, they could obtain an understanding of the use of a myoelectric hand by their children. In addition, obtaining such understanding towards the use of myoelectric hand will produce good changes in the attitude and feelings of parents towards their children. We think that important is parents have to personally experience operating a myoelectric hand.
184
Liezel Wegner (1) presenting Anthea Rhoda (1)
University of the Western Cape, Cape Town, South Africa (1)
The use of the modular socket system in a rural community in South Africa: A longitudinal case series description
Providing prosthetic services in rural areas in South Africa pose many challenges. Poor accessibility to health services, lack of rehabilitation and a shortage of staff and other resources negatively affect the functional outcome of transtibial amputees in this setting. Providing a transtibial amputee with a prosthesis removes some of the participation restrictions that “disables” this group of patients, and enable them to actively participate in their communities. The MSS can be manufactured and fitted in rural clinics in approximately one hour and could potentially alleviate some of the challenges experienced by rural amputees and prosthetists.
To field-test the use of the modular socket system (MSS) in a rural community in South Africa.
A mixed methods, longitudinal case series design was used to field-test the use of the MSS in this rural community. Participants were purposively selected unilateral primary transtibial amputees. The total sample consisted of 19 amputees who were fitted with the MSS, and followed up at 1-, 3- and 6-months post fitting. Data from the Orthotic and Prosthetic User’s Survey (OPUS), the 6 min walk test, and Focus Group Discussions (FGD) were triangulated to determine functional status, quality of life and satisfaction with the prosthesis. The OPUS is a valid and reliable tool, but was translated into isiZulu, and back-translated to improve validity. The 6 min walk test is a reliable measure of functional status in amputees, and trustworthiness of the qualitative data from the FGD were established. Triangulation of quantitative and qualitative data improves the reliability of findings in a smaller sample size.
Of the 19 participants fitted with the MSS, nine (47%) completed the 6 months follow up. The functional status, quality of life and satisfaction with prosthesis compares well with the OPUS standard. The results from the 6 min walk tests are slightly below average due to normal complications encountered after the socket fitting in a primary amputee, and prosthetist inexperience with the MSS. The qualitative data provided good supporting data to the quantitative results from the OPUS and the 6 min walk test. Overall, patients reported a good functional status, increased participation in society and improved quality of life. Participants did however make some recommendations for improvement to the aesthetics of the prosthesis.
The MSS could potentially be used as an alternative to the traditional method of plaster casting in this rural setting in order to address the long waiting periods for transtibial prostheses. The high drop-out rate in this study is a definite limitation, and affects the reliability of the findings to some extent, but also re-inforces the need for an alternative solution in this setting.
185
Yaeko Shibata (1) presenting Ayaka Nakasho (1) Futoshi Mizobe (1) Makiko Okamoto (1) Yu Ando (1) Yuka Mouri (1) Nobuyuki Honda (1) Takaaki Chin (1) Yuichiro Honda (1) Jumpei Oba (2) Akio Nakagawa (2) Haruki Nakamura (1)
Hyogo Rehabilitation Center, kobe,Hyogo, Japan (1) Kobe Gakuin University, Kobe,Hyogo, Japan (2)
Myoelectric arm prosthesis approach in children at the Japan Hyogo Rehabilitation Center
In the West, early aggressive training with myoelectric arm prosthesis has been reported to be effective for children that lost an arm due to accident and children with birth defects. This is to enable the children to personally decide whether they want to live using a prosthetic arm in the future.
Although the approach in Japan has been inadequate, trials with myoelectric arm prosthesis from infancy were started from 2002 at the Hyogo Prefecture Rehabilitation Center and that approach is still in place.
To clarify the trend in 50 children who underwent training using myoelectric arm prosthesis at this institution in 2002-2014.To introduce the approach and progress of myoelectric arm prosthesis for children and report the usage features and effectiveness of using myoelectric arm prosthesis in real-life setting by age.
Fifty children who had lost (amputation) an arm that were examined at the Hyogo Prefecture Central Rehabilitation Hospital and had started training with a myoelectric arm prosthesis in 2002-2014 were the subjects.
There were 26 males and 24 females. Eighteen had lost the right arm and 32 the left arm. Cause of the loss was congenital loss of an arm in 49 children and amputation due to trauma in one child.
All training was out-patient based and one session was approximately 60 min.
Forty five children continued using myolectric arm prosthesis and 5 discontinued the use. Infants were started from the use of decorative prosthetic arms, then introduced to one-electrode controlled and 3-electrode controlled myoelectric arm prosthesis from 1 year of age and 3 years of age onwards, respectively. Methods of play according to age were introduced focusing on grip training such as opening and closing of the hand, and playing with the use of both hands. Moreover, not only use of the prosthesis at home, but motions of using it in social life such as in the nursery and kindergarten were actively conducted.
By wearing a prosthetic arm and using it in daily life from early stages, children will want to use both hands to accomplish tasks, and will have many opportunities where they can experience enjoyment in playing.
Increased desire to opt for a prosthetic arm leads to improvement in the quality of life of the person affected.
As the role and methods of use of a prosthetic arm changes as a child grows, continued periodical follow up and approaches are indispensible with myoelectric arm prosthesis for children.
187
Leigh Wallace (1) presenting
Peacocks Medical Group, Newcastle upon Tyne, UK (1)
A comparison of handheld 3D scanners for use in a clinical environment
When designing and manufacturing bespoke orthotic devices, it is important for the anthropometric data to be accurate. Also, it is essential for this data to get from the clinic to the manufacturers as quickly as possible. It is believed that using handheld 3D scanners could improve on the current data collection process. This investigation assesses the accuracy of handheld 3D scanners and their compatibility for use in a clinical environment.
The study compares the accuracy of different handheld 3D scanners for use in orthotics in order to determine which, if any, could be used in a clinical environment
Three geometrical test pieces were measured at six different points using a digital calliper and then scanned five times with each handheld scanner. These same measurements were then taken from all of the scans in a design software. From this data, the average errors were calculated and compared. In addition to this, patient foam impression boxes were scanned and the measurements (heel width, foot length and joint width) compared with those from scans taken using an expensive foot bed scanner (currently used for commercial production). The capabilities of the scanners were also tested by scanning lasts and positive casts.
The maximum error calculated from the Sense scans was 1.26mm and the maximum average error was -0.67mm. In comparison, the EVA was slightly less accurate with a maximum error of 1.52mm and a maximum average error of 0.72mm. The error from the Sense scans varies between negative and positive whereas the EVA scans have consistently positive error. Measurements from the Sense foam box scans showed a maximum difference of 5mm to the ParoContour scans; however, out of sixty measurements, only five had a difference above 3mm. The maximum acceptable error would be ±3mm. Casts and lasts need to scanned at least twice to capture every surface; as the EVA software allows multiple scans to be aligned and stitched together, this scanner is the only one suitable for scanning such parts.

On the whole, the Sense scanner would be recommended for simple scanning, such as foam impression boxes, in a clinical environment; this is because it is more accurate than the EVA and has an acceptable error percentage. Also, it is relatively low-cost, lightweight and does not require mains power. However, this may change as the investigation is on-going and at least one other scanner will be trialled within the coming months.
188
Terje Gjøvaag (1) presenting Peyman Mirtaheri (1) Nihad Kapetanovic (1) Inger Marie Starholm (1)
Oslo University College, Oslo, Norway (1)
The preferred walking speed of unilateral transfemoral amputees is not similar to their most economical walking speed
The quantitative relationship between the walking economy (Cw) and speed of walking during floor and treadmill walking is little investigated in unilateral transfemoral amputees (TFA). In addition, it is still debated whether the preferred walking speed (PWS) of TFA and healthy subjects (CON) is similar to their most economical walking speed (ECOws).
Investigate the energy-speed relationship and ECOws of a group of TFA and CON during level walking on the treadmill and on the floor.
A group of TFA (n=8) and a group of CON (n=8) were recruited to the study. Oxygen uptake (VO2) was measured at steady state conditions by a portable oxygen analyzer (Cortex Metamax 3B, Germany) when walking along a 40 meter indoor track and on a treadmill. Both the TFA and CON walked on the two surfaces with five different speeds in random order. Walking speeds were: Preferred Walking Speed (PWS), PWS pluss/minus 12.5 % and PWS pluss/minus 25%. The walking speeds were controlled by an optical gait analysis system (OptoGait, Italy). The Cw was calculated as relative oxygen uptake (ml kg-1 min-1) divided by walking speed.
Mean±SD treadmill PWS were 0.89±0.2 and 1.33±0.3 m sec-1 for the TFA and CON (p < 0.01), while the floor PWS were 1.22±0.2 and 1.52±0.1 m sec-1 (p<0.01), respectively. The average ECOws (both on treadmill and floor) derived from Figure 1 was 1.07 m sec-1 for the TFA (dotted vertical line) and 1.26 m sec-1 (dashed vertical line) for the CON. On the treadmill, the ECOws was faster than the PWS (filled star) for the TFA, but slower than the PWS for the CON (open star). On floor, the ECOws is slower than both the TFA PWS (filled star) and the CON PWS (open star).

Lower limb amputees walk slower than healthy subjects, thus the higher Cw observed in lower limb amputees could in part, be due to the fact that they cannot reach their most economical walking speed (Genin et al. 2008). The present study show that the ECOws, in general, is slower than the PWS of both TFA and CON. Consequenty, the PWS is perhaps governed by other factors than the energy expenditure during walking.
Genin et al. Eur J Appl Physiol 103:655-663, 2008
189
Samuel Bonnet (1) presenting
The International Committee of the Red Cross, Geneva, Switzerland (1)
Physical Rehabilitation Centres - Architectural Programming Handbook
The physical rehabilitation activities of the International Committee of the Red Cross (ICRC) can be traced back to the Second World War. However, the beginning of the ICRC’s major commitment in this field came with the creation of the Physical Rehabilitation Programme in 1979. This resulted in the construction and refurbishment of many Physical Rehabilitation Centers (PRCs) in situations of armed conflicts and violence. Since then, the ICRC has documented over 35 years of work on PRCs.
The handbook provides a decision-making process for the creation of a PRC operated by, or with the support of, the ICRC. It gives other humanitarian actors a model for their programmes.
The proposed framework that can be used by all parties involved in the setup of a PRC is to systematize the architectural programming. Architectural programming is the decision-making process with regard to the purpose and function of a PRC. It is a key process in any construction project. It takes place at project inception and is finalized at the beginning of the design process. Because its development involves a large number of different factors, the proposed framework presents various approaches to facilitate the interaction of the different specialists involved.
An architectural study of ten existing PRCs built in different countries over the past 30 years provides the understanding necessary for the development of a PRC: floor area, plot ratio, area by service vs service users / devices produced.
A set of tools (bubble diagrams, space cards and component cards). These tools track three different levels of abstraction of an architectural programme: the first for the services, the second for the rooms and outdoor spaces, and the third for the equipment and furniture. They facilitate the transition to the design process.
A general approach to accessibility in a PRC based on the standards derived from the United Nations Convention on the Rights of Persons with Disabilities (CRPD).

Can this handbook be used in any given context? And can it serve any organization or is it specific to the ICRC?
This handbook facilitates clear communication between all specialists involved and reduces the time spent on planning and design. Moreover, the integration of international standards removes or reduces restrictions on the activities of people with disabilities, whether they are service users or staff members at the PRC.
Building construction – Accessibility and usability of the built environment, ISO 21542:2011, International Organization for Standardization, Geneva, 2011.
John Mejia Rios, Programming guide for the setting up of a rehabilitation centre, Handicap International, Lyons, 2001.
Otto Bock (ed.), Consulting, Planning and Equipping, Otto Bock GmbH, Duderstadt, 2010.
190
Coralie Villa (1,2) presenting Karine Langlois (2) Xavier Bonnet (3) Isabelle Loiret (4) Pascale Fodé (1) Francois Lavaste (2,1) Helene Pillet (2)
INI/CERAH, Créteil, France (1) Arts et Métiers ParisTech, Institut de Biomécanique Humaine Georges Charpak, Paris, France (2) Proteor, Seurre, France (3) IRR, UGECAM Nord EST, Nancy, France (4)
Physiological and prosthetic ankle behaviour on cross-slopes
Cross-slopes walking is a common situation of daily living in which one has to adapt to the transverse inclination of the ground relative to his progression direction. This situation described as limiting for lower limb amputees has yet barely been studied in the literature [1][2][3]. Dixon et al. [1] highlighted that non amputee subjects gait is mainly adjusted on cross-slopes with changes in ankle behavior in the frontal plane.
Seventeen non amputee subjects, thirteen transfemoral amputees and fifteen transitibial amputees were asked to walk at a comfortable speed on a flat pathway and on a cross-slopes device inclined of 6° both instrumented with force platforms (AMTI, 100Hz) in a motion analysis lab (Vicon V8i, UK) [4]. Ankle angle and moment in the frontal plane were studied during stance when the lower limb was loaded: from heel strike to the end of the single limb support. The analyses were conducted for the residual limb (amputee groups) or the left lower limb (control group) during level walking (LW), cross-slopes walking with the limb uphill (CSU) and with the limb downhill (CSD).
Figure 1 summarizes the ankle frontal plane behaviour in all situations. In the control group, a shift of the ankle angle was observed at heel strike. This adjustment resulted in an internal varus moment at the ankle in all situations. In the two amputee groups prosthetic ankles were adjusted on cross-slopes according to the inclination: ankle internal moment and angle changed sign between CSU and CSD. Prosthetic ankles were passively adjusted to cross-slopes with the changes in mediolateral direction of the ground reaction force among conditions.

Ankle moment vs ankle angle in the frontal plane between heel strike (0%) and the end of single limb support during stance phase (end) for LW, CSU and CSD in the two amputee patients groups and the control group.
Physiological ankles were in a pre-adapted position at heel strike resulting in a similar evolution of the moment during cross-slopes walking uphill or downhill and level walking. Prosthetic ankles only provided passive adjustments on cross-slopes. To facilitate amputee people locomotion on cross-slopes, prosthetic design should better reproduce physiological ankle behaviour on cross-slopes including the shift of the initial valgus angle position at heel strike according to the slope inclination.
[1] Dixon et al., J Appl Biomech, 26(1):17-25, 2010.
[2] Damavandi et al., Hum Mov Sci, 31(1):182-189, 2012.
[3] Starholm et al., Prosthet Orthot Int, 34(2):184-194, 2010.
[4] Pillet et al., Innov Res Biomed Eng, 35(2) : 60-65, 2014.
191
Ko Asayama (1) presenting Yohei Konishi (1) Atsushi Tagawa (1) Fumitada Hattori (1) Haruo Kodama (2)
Nagao Hospital, Fukuoka City, Japan (1) Advanfit Inc, Yatsushiro City, Japan (2)
Much lighter AFO becomes applicable for severe foot deformities of stroke patients through simple invasive procedure, including the follow-up survey of patient’s contentment
For the spastic foot deformities of hemiplegics, various orthotics have been applied which tend to become sturdy for severe cases. But, simple and lighter orthoses are preferable. We have reported one day hospitalization regime for the minimum invasive procedure to solve this problem. The degree of our patient’s contentment will also be followed.
One of the permanent methods to decrease severe spastic foot deformity is the combination tenotomies of target tendons for creating the balance. One day hospitalization procedure and the results will be presented.
Sixty-six stroke patients in these five years were targeted(age:61Y/O±SD). All were old stroke cases, wearing various heavy duty orthotics (mainly shoe horn type AFO), ambulating independently or assisted. Their involved foot hadn’t met their orthosis. With cautious gait analysis, the target tendons were selected for combination tenotomies to create muscle balance. Achilles tendon aponeurosis, FDL, TP, FHL, intramuscular TA tendon and FDBs were among them. NLA and local anesthesia were used. With no medication disruption, no tourniquate during the procedure, patients were encouraged to walk with full weight bearing soon after the procedure or on the next morning. Follow-up results were surveyed.
The combination of Vulpius procedure, tenotomies of TP,FDL,FHL and TA release was the highest number, 37 out of 66 cases. For equinus, one or two cut line to gastrocunemius aponeurosis was selected. About knee recurvatum, the highest incident rate was with shoe horn brace, followed by non-brace wearing. Patient’s old orthotics were replaced with simple one such as anterior leaf type plastic AFO. Follow up study revealed 74.5% of patients had functionally improved or remained the same, 9.8% had expired or suffering from other illness. 85.4% was the all the time user of orthosis or using only at outdoor activity, 10.4% was barefoot walking with no more orthosis. 81.3% of the subjects were satisfied, 14.6% not satisfied.
Ambulation wearing sturdy leg orthosis on Tatami mat tends to be unacceptable in Japanese life style. The minimum invasive operation without requiring postoperative bed rest is one choice for reducing severe hemiplegic foot deformity. Thereafter, simple, lighter and cosmetic orthosis can be applied. Some patients become barefoot walkers. However, loss of the foot power seems to become the cause of complaining in a small number of less spastic feet.
194
Biden Ed (1) Hill Wendy (1) presenting LeBlanc Shannon (1) Bush Greg (1) Kyberd Peter (1)
University of New Brunswick, Fredericton, NB, Canada (1)
Repetitive Strain Injury Risk Factors in Upper Limb Amputees
Surprisingly little research has been done regarding repetitive strain injury or its risk factors in upper limb amputees. Jones and Davidson in 1999 report on a survey and case studies targeted at amputees in their hospital in Australia. Up to half of their amputee population had overuse symptoms. Ostlie et al 2011 reported a relatively large study of amputees in Norway and found similar results. The incidence of pain was higher in the amputees than in their normal controls and they speculate that this may lead to overuse syndromes.
This study examined self reported pain in working age adults within our clinic population and compared those results to an age matched group of normally limbed controls.
Our clinic includes about 140 upper limb amputees. This study included a survey designed to identify activities and characteristics which might be risk factors for Repetitive Strain Injury. We received responses from 33 of 65 working age adults in our clinic and from 40 age matched normally limbed adults. The survey included basic information on gender, height, weight, etc. as well as asking about participation in activities with or without a prosthesis and questions on pain. Results were analysed using MiniTab V17 ™ statistical software. Comparisons were made between the amputee and normally limbed groups to ensure comparability. Amputees were compared with normally limbed for activity and pain, and comparisons were made between pain levels associated with the sound limb of the amputees and the dominant arm of the normally limbed.
The amputee and normally limbed controls were compared as a group and sub grouped by sex. Comparisons of age, height weight, BMI etc. showed the groups to be similar. A high proportion of both groups reported back pain. Normally limbed individuals reported minimal levels of pain in a combined neck/shoulder/ upper arm measure. By comparison 25% of the amputee population reported more than minimal pain levels. A significant finding is that about 12% of normally limbed reported wrist and hand pain vs 36% for the sound side of the amputees. These are broadly comparable to the results of the study by Osterlie et al. An interesting finding was that 77% of amputees reporting hand and wrist pain were regular texters whereas all of the normally limbed texters had hand and wrist pain.
Upper limb amputees exhibit patterns of pain which are different from those of normally limbed individuals and suggest that they may be at risk of developing Repetitive Strain Injuries in their sound hands. Current activities such as texting may contribute to these risks.
- Jones, L.E., Davidson, J.H., “Save that arm: A study of problems in the remaining arm of unilateral upper limb amputees”, Prosthetics and Orthotics International, 1999, Vol. 23, No. 1, Pages 55-58
- Østlie, K, Franklin, R, Skjeldal, O., Skrondal, A., Magnus, P., “Musculoskeletal Pain and Overuse Syndromes in Adult Acquired Major Upper-Limb Amputees”, Archives of Physical Medicine and Rehabilitation, Volume 92, Issue 12, December 2011, Pages 1967–1973.e1
195
Jon Sensinger (1) presenting Adrian Aleman (1,2) Kevin Englehart (1)
University of New Brunswick, Fredericton, New Brunswick, Canada (1) University of Guadalajara, Guadalajara, Jalisco, Mexico (2)
Assessing the cost of small vs. large errors in myoelectric movement control
The cost of a mistake influences control. For example, holding a rigid cup slightly too tightly with a terminal device has little cost, whereas holding a rigid cup slightly too loosely results in it falling and breaking [1]. Similarly, most people don’t mind small errors in movement, but as the error gets larger, they quickly care more. Knowing this behavior of how much they care as a function of the size of the error is important knowledge that can help us design better prosthesis controllers that minimize the total cost of a given motion.
Twenty-four able-bodied subjects controlled a 1-D cursor on a computer display using two myoelectric sensors placed on their forearm flexors and extensors. They were instructed to follow a random path presented on the screen. The position of their cursor was presented in 50 ms bursts, and unbeknownst to the subjects, we altered the distribution of the cursor position relative to their actual myoelectric-controlled position. But measuring their compensation to changes in the distribution, we were able to assess the cost-function (e.g., how much they cared about little errors vs. big errors) using a previously published technique [2].
We found that subjects had the same cost function for myoelectric control that has previously been reported for joystick control [2], even though myoelectric control has substantially more noise in it. We also found that the cost function is best represented by an upside down bell-curve. This means that subjects care proportionally more about medium errors than small errors, but that for large errors cost begins to level out and they behave the same no matter how large the error is.
We have been able to accurately quantify the cost-function of myoelectric control for movement-tracking. Knowledge of this cost-function will improve our intuitive understanding of designing controllers. It will also be combined with other recently acquired parameters [3] to form a model of human control of prostheses, which can be used to generate an optimal controller.
[1] K. Körding, “Decision theory: what ‘should’ the nervous system do?,” Science, vol. 318, no. 5850, pp. 606–10, Oct. 2007.
[2] K. P. Körding and D. M. Wolpert, “The loss function of sensorimotor learning.,” Proc. Natl. Acad. Sci. U. S. A., vol. 101, no. 26, pp. 9839–42, Jun. 2004.
[3] R. E. Johnson, K. P. Kording, L. J. Hargrove, and J. W. Sensinger, “Does EMG control lead to distinct motor adaptation?,” Front. Neurosci., vol. 8, no. September, p. 302, Jan. 2014.
196
Sophie Daigle (1) Reva Johnson (2,3) Jon Sensinger (1,2) presenting
University of New Brunswick, Fredericton, New Brunswick, Canada (1) Northwestern University, Evanston, Illinois, USA (2) Rehabilitation Institute of Chicago, Chicago, Illinois, USA (3)
Making EMG control more predictable improves performance
Many amputees want to rely less on visual feedback [1]. However, attempts to provide alternative feedback sources have not been largely successful [2]. There is another way to think of this problem, however – if control was more predictable, amputees would not have to rely on any feedback. Indeed, studies have shown that feedback is not useful in itself for real-time control due to sensory delays, but that it is useful in forming internal models that make control more predictable[3]. We have recently demonstrated that although EMG is a relatively noisy control signal, both able-bodied subjects and amputees do indeed develop internal models that make their control more predictable [4], [5]. It remains unclear, however, if these models actually improve performance.
The aim of this study was to assess whether the formation of internal models improves the accuracy of EMG-controlled movement. The secondary aim was to see whether the formation of internal models reduces the amount of effort required to accurately control prostheses.
20 able-bodied subjects controlled a 1 degree-of-freedom computer display using EMG sensors placed on the forearm extensor and flexors. They were asked to track a moving target, and were provided with one of three different visual displays that have been shown to provide varying levels of internal model formation [6].
We found a statistically significant reduction in tracking error when subjects were provided with a visual interface that allowed for the formation of internal models (p<0.01). We also found a significant reduction in muscle effort to achieve this level of accuracy (p<0.01).
Our work in this area has shown that 1) people using EMG control do develop internal models, and that 2) these models improve performance. This work provides a framework from which we can move forward in our quest to reduce reliance on visual feedback. Rather than looking at feedback for the sake of feedback, we will now begin to ask the question – which feedback sources most strengthen internal models? Importantly, any feedback source that provides lower-quality redundant information will not strengthen these models [7], so we need to look for feedback that provides additional information that vision is unable to adequately capture.
[1] D. J. Atkins, D. C. Y. Heard, and W. H. Donovan, “Upper- Epidemiologic Overview of lndividuals with Upper - Limb Loss and Their Reported Research Priorities.”
[2] C. Antfolk, M. D’Alonzo, B. Rosén, G. Lundborg, F. Sebelius, and C. Cipriani, “Sensory feedback in upper limb prosthetics.,” Expert Rev. Med. Devices, vol. 10, no. 1, pp. 45–54, Jan. 2013.
[3] P. Cisek, “Internal Models,” Encyclopedia of Neuroscience. 2009.
[4] R. E. Johnson, K. P. Kording, L. J. Hargrove, and J. W. Sensinger, “Does EMG control lead to distinct motor adaptation?,” Front. Neurosci., vol. 8, no. September, p. 302, Jan. 2014.
[5] R. E. Johnson, K. P. Kording, L. J. Hargrove, and J. W. Sensinger, “Similar trial-by-trial error correction behavior across transhumeral amputees and able-bodied subjects,” in IEEE/EMBS Conference on Neural Engineering, 2015, p. submitted.
[6] J. Lobo-Prat, A. Q. L. Keemink, A. H. a Stienen, A. C. Schouten, P. H. Veltink, and B. F. J. M. Koopman, “Evaluation of EMG, force and joystick as control interfaces for active arm supports.,” J. Neuroeng. Rehabil., vol. 11, p. 68, Jan. 2014.
[7] M. O. Ernst and M. S. Banks, “Humans integrate visual and haptic information in a statistically optimal fashion.,” Nature, vol. 415, no. 6870, pp. 429–33, Jan. 2002.
197
Jon Sensinger (1) presenting James Lipsey (2) Ashley Thomas (2)
University of New Brunswick, Fredericton, New Brunswick, Canada (1) Rehabilitation Institute of Chicago, Chicago, Illinois, USA (2)
VOVC Body-powered hand with multiple grasp patterns
Body-powered terminal devices are commonly used due to low weight and cost, ruggedness, and accurate control [1], [2]. In contrast, body-powered hands are rarely used – their benefits are similar to terminal devices, in that they both perform a single grasp, but they have a number of relative weaknesses, including added cosmesis inefficiency and visual obstruction of the object being grasped [3]. We have recently designed a body-powered terminal device that can switch between voluntary-opening (VO) and voluntary-closing (VC) mode. This VOVC device has shown improved performance relative to conventional devices when tested using the SHAP test [4], and the concept has promise to improve the performance of body-powered hands.
The goal of this project was to develop a VOVC body-powered hand that offered a substantial increase in performance compared with split-hook terminal devices.
We redesigned the VOVC mechanism to fit within the palm of the hand, allowing the user to either use voluntary-opening mode or voluntary-closing mode.
We also designed a thumb that could be manually positioned in different postures such as chuck-grip, fine-tip, and palm-flat. Perhaps most importantly, we designed the fingers such that they could be individually locked in a fully-flexed state without inhibiting the motion of the other fingers. This function was achieved by using springs to individually bias each finger in extension; pulling fingers closed using a series of links connected to each finger; and including a push-lock in each knuckle. This design results in a large number of possible grip patterns.

We were able to combine all of these features into a small #7 hand design that weighs approximately 470g. This hand can achieve a variety of grasp patterns needed to perform activities of daily living.
The added functional benefits of this hand compared with a split-hook design may allow it to be adopted by more users than previous hands. The design is rugged and comparable in size and weight to existing hands. In future work we will evaluate the performance of this hand using outcome measures such as SHAP and take-home trials.
[1] K. Berning, S. Cohick, R. Johnson, L. Miler, and J. W. Sensinger, “Comparison of body-powered voluntary opening and voluntary closing prehensor for activities of daily living,” J. Rehabil. Res. Dev., vol. 51, no. 2, pp. 253–262, 2014.
[2] R. F. ff. Weir and J. W. Sensinger, “Design of Artificial Arms and Hands for Prosthetic Applications,” in Biomedical Engineering and Design Handbook, 2nd ed., vol. 2, M. Kutz, Ed. New York: McGraw-Hill, 2009, pp. 537–598.
[3] C. M. Fryer, G. E. Stark, and J. W. Michael, “Body-Powered Components,” in Atlas of Amputations and Limb Deficiencies, 3rd ed., D. G. Smith, J. W. Michael, and J. H. Bowker, Eds. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2004, pp. 131–143.
[4] J. W. Sensinger, J. H. Lipsey, A. Thomas, and K. Turner, “Design and evaluation of a voluntary-opening/voluntary-closing prosthetic terminal device,” J. Rehabil. Res. Dev., vol. In press, 2015.
198
Ali Hussaini (1) presenting Peter Kyberd (1)
Institute of Biomedical Engineering - University of New Brunswick, Fredericton, New Brunswick, Canada (1)
Independent Prosthetic Wrist Rotation for Transradial Myoelectric Prosthesis Users and Assessment of Compensatory Motions
Transradial myoelectric prosthesis users face difficulty positioning the electric hand. Many of these users lose their wrist during an amputation. As a result, they are forced to over rotate their shoulder and perform other body compensation to properly orient the hand for a given task. This puts them at risk for developing repetitive strain injuries. Prosthetic wrist units exist but their utility is limited by the lack of independent control from the user to make functional improvements.
The goal was to investigate new methods of control to augment the available inputs in a standard 2-site myoelectric device. The design of an objective assessment for detecting functional improvement, if any, was also a necessary for evaluation.
The prosthetic socket was redesigned and the user’s residual forearm rotation was used as a new input source to control a wrist rotator. The design is only viable if the user has a certain level of forearm rotation remaining post-amputation. The new input was used along side surface level EMG which is used to drive hand function. This resulted in a solution where the user could control a prosthetic wrist independently of a one degree of freedom prosthetic hand.
A timed assessment test involving the grasping and relocation of 3 clothespins was used to measure the effect of the new prosthesis on the user’s compensatory motions. Motion capture was used to calculate joint angles.
The user performed the test with their current prosthesis and with the new prosthesis with wrist rotation. The motions of the trunk, head, and shoulders were analyzed to see if the new design had an effect on body motion.
A reduction in several body motions including a reduction in shoulder angles was seen. Overall a more neutral stance resulted during the assessment, as a result of introducing the new degree of freedom of wrist rotation.
The wrist rotator did cause the user to take a longer time to complete the assessment, but there was a willingness to use the new wrist output. The user also reported a reduction in pain at the neck and shoulders.
The study identified the limitations of current prosthetic interventions and presents a potential solution to improving functional outcomes for the prosthesis user. A reduction in compensatory motions is possible if additional independent control inputs can be obtained from the user. A new assessment procedure is presented as well that can aid in clinical assessment of any new prosthetic intervention.
199
Ecaterina Vasluian (1) Iris Van Wijk (2) presenting Pieter Dijkstra (1) Heleen Reinders-Messelink (3) Corry Van der Sluis (1)
University of Groningen, University Medical Center Groningen, Department of Rehabilitation, Groningen, The Netherlands (1) Centre of Excellence for Rehabilitation Medicine Utrecht (De Hoogstraat Rehabilitation and UMC Utrecht), Utrecht, The Netherlands (2) Rehabilitation Friesland, Beetsterzwaag, The Netherlands (3)
Use and satisfaction with adaptive devices in youngsters with upper limb reduction deficiencies
Youngsters with upper limb reduction deficiency (ULRD) may encounter limitations in daily life activities. Prostheses are prescribed to overcome activity limitations, but many are rejected due to discomfort or lack of functionality. Alternative solutions, such as adaptive devices (ADs), may be considered.
To evaluate the use, satisfaction and social adjustment with ADs compared to prostheses in youngsters with ULRD.
A cross-sectional study using questionnaires was performed. Youngsters with ULRD between 2-20 years old responded to questions about usage of ADs versus prostheses. D-Quest and TAPES were used to evaluate satisfaction and social adjustment, respectively.
360 ADs were used by 76% of 218 participants (n=166). Eighty youngsters used or had used prostheses (37%). Participants were mainly boys (58%) with transversal ULRD (87%). ADs were used in 43% for self-care (using cutlery), mobility (cycling, 28%) or leisure activities (sports, playing musical instruments, 5%). Prostheses were used for mobility (9%), recreation/leisure (6%), work (4%), self-care (4%). The most preferred solution to overcome activity limitations was using own body-parts (>60%), help from others (>50%), using ADs (48%) or prostheses (< 9%). Satisfaction with ADs was higher than with prostheses (P<0.001). Social adjustment with ADs compared to prostheses did not differ.
Youngsters with ULRD used ADs much more than prostheses and were more satisfied with ADs. ADs were mainly used for eating, cycling, sports or playing musical instruments. Social adjustment with ADs or prostheses was comparable.
ADs should be included in standard rehabilitation treatment of youngsters with ULRD.
Adaptive devices in youngsters with upper limb reduction deficiencies : use and satisfaction. Ecaterina Vasluian, MSc, PhD, Iris van Wijk, MD, PhD, Pieter U Dijkstra, Prof, PhD, Heleen A. Reinders-Messelink, MSc, PhD, Corry K. van der Sluis, Prof, PhD. Journal of Rehabilitation Medicine 2014 ; in press.
0200
Solange ehrler (1) presenting chloe blum-demans (1) serge coulon (1) marie eve isner-horobeti (1) IURClémenceau, Strasbourg, France (1)
Assessment of therapeutic education in lower-limb amputees
S.Ehrler; C.Blum-Demans ; S.Coulon; ME Isner-Horobeti
Institut Universitaire Réadaptation Clémenceau, Strasbourg, France
Therapeutic patient education (TPE) is a continuous process. Through TPE, such patients should acquire and maintain the resources and skills required for optimal self-management of their illness and thus of their life.
A French national TPE group for lower-limb amputees was constituted with the backing of French scientific societies, such as SOFMER, AFA, AMPAN and ISPO France. TPE approach starts about self-care and self-management, particularly in view of the autonomy offered by the prosthesis.
We wanted to determine the place of self-care in patients following lower limb amputation by evaluating prosthetic and limb management and prosthesis use.
To this aim, we followed 95/135 trans-tibial amputees between May 2011 and December 2013 who were fitted with contact silicone socket prosthesis with distal lock. Within this cohort of patients (n=135), 13 could not be followed due to death; 14 were lost to follow-up and three lived too far away to allow a follow-up evaluation; and ten patients stopped using the prosthesis because of medical complications (n=5) or following a double amputation (n=5). All trans-tibial amputees who were fitted with prosthesis received TPE. or their relatives/carers, if they had cognitive or functional problems.
We found that the prosthesis was donned daily by the 95 patients under study. The self-management of complications was well acquired, as indicated by the absence of skin abrasions, thanks to their own knowledge on how to assess proper fitting and on the proper use of prosthetic socks while wearing the prosthesis . The autonomy concerning prosthesis donning was complete in 78/95 patients. Walking inside the house or in the area around the house was acquired, for a limited distance (<500m) But walking from 1km to unlimited for fast half of all the patients is possible and all-terrain walking for few patients. Physical and sports activities were also practiced by 13 patients and included hunting, mountain bike, swimming, hiking and electric bike.
Our patients were mainly amputated as a results of vascular disease, or diabetic complications. The other causes are traumatic, sepsis or skin cancer. The finding that the prosthesis was donned for more than 12 hours by 54% of patients indicates the high degree of autonomy and self-management in the daily life obtained thanks to the personalized care pathway of our patients. Certainly, TPE contributed to the ability of our patients to make informed choices and to take control of their situation.
TPE allowed us to better understand the patients’ personality through the diagnosis of their educational needs, the identification of their specific requirements and the assessment of their potentials. We could thus take into account their questions/specific needs through personalized care pathways.
140 caractères pour promouvoir l’étude
What brings Therapeutic Patient Education in self- management after lower limb amputation? A study about 135 patients by evaluating prosthetic and limb management.
0201
Jan Andrysek (1,2) presenting Debra Cameron (2) Janet Njelesani (2) Season Kam (2) Mallory Kent (2) Alin Khodaverdian (2) Liane Daiter (2)
Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario, Canada (1) University of Toronto, Toronto, Ontario, Canada (2)
The influence of environmental and personal factors on the rehabilitation and participation of lower-limb prosthetic users in low-income countries
Thirty million individuals in low-income countries (LICs) currently require prosthetic and orthotic services; approximately 10 million of these are individuals with lower-limb amputations (LLA) who require the use of a prosthetic device [1,2]. Despite this high need, there is a limited understanding of prosthetic rehabilitation services in LICs as most research has focused on prosthetic use in high-income countries (HIC) [2-6]. No studies have looked at the perspective of prosthetists in LICs.
To examine the environmental and personal factors in LICs that influence prosthetic rehabilitation of adults with LLA and their ability to participate in daily activities from the perspective of prosthetists.
In this qualitative descriptive study, 11 prosthetists participated in semi-structured interviews by telephone or Skype. The interview guide and qualitative thematic analysis was guided by the International Classification of Function. The target participants for this study were trained prosthetists or prosthetic technicians working directly with clients to provide them with prostheses (i.e. doing both functions of fabricating prosthesis and fitting them to patients) in a LIC as defined by the World Bank for a cumulative period of at least 1 year over the past 5 years. Individuals were excluded if they were not fluent in English or were deemed unable to provide informed consent.
Thematic results revealed that unique environmental and personal components can influence activity and participation of lower-limb prosthetic users in low-income countries (LICs) which are often overlooked in the design of prosthetic devices and provision of prosthetic services. These components include facilitating continuity of care, condition of the post-surgical residuum, outdoor environments of common occupations, aesthetics and durability of prostheses, and user comfort. These components are captured in the four main themes derived from the data: “They don’t get the care they need’’ lack of continuity of care during the prosthetic rehabilitation process: ‘‘Up and down the hill’’: common occupations in LICs occur in outdoor terrains; ‘‘Staring at the stump’’: cultural stigma relating to limb amputations; and ‘‘Satisfying the patient’’: comfort and utility of a prosthesis as a foundation.
Environmental and personal factors must be considered when providing prosthetic rehabilitation for adults with LLAs in LICs in order to optimize participation in activities. This study provides new insights about some of the factors that influence the ability of individuals with lower-limb amputations to participate in meaningful activities within their communities. Results can also inform the practice of prosthetists in LICs as it highlights their contributions in enabling participation for lower-limb prosthetic users.
[1] World Health Organization; 2005 http://whqlibdoc.who.int/publications/2005/9241592672.pdf
[2] Pearlman J, Cooper RA, Krizack M, et al.; 2008 IEEE Eng Med Biol Magaz
[3] Hussain S.; 2011 Qualitat Health Res
[4] Matsen SL.; 1999 Prosthet Orthot Int
[5] Mulholland SJ, Packer TL, Laschinger SJ, et al.; 1998 Disabil Rehabil
[6] Van Brakel WH, Poetsma PA, Tam PT, Verhoeff T.; 2010 Disabil, CBR Inclusive Dev
0202
Hossein gholizadeh (1,2) Elham sadat Yahyavi (2) Arezoo Eshraghi (1,2) presenting Hassan Saeedi (2) Vahid Abdollah (2) Noor Azuan Abu Osman (1)
university of malaya, kuala lumpur, Malaysia (1) Iran University of Medical Sciences, Tehran, Iran (2)
Adverse Effect of Improper Interface Pressure Distribution within Transtibial Prosthetic Socket
Successful rehabilitation of an amputee is pertinent to the design and fit of the socket because the weight-bearing capabilities of the residual limb and the foot are not identical. Distribution of interface pressure between the socket and the tissues of residual limb may alter the user’s comfort, and thus is important for the socket design.
This paper describes a total surface bearing prosthetic socket with Velcro suspension system for a patient (25-yr-old female) with a bulbous stump.
The subject had unstable excessive soft tissue at the distal end of the residuum (figure 1). After two years of prosthetic use, she experienced several problems, including pain in the residual limb and knee joint. Pressure distribution was evaluated during ambulation. We also designed a total surface bearing socket (TSB) with Velcro as suspension system to distribute the load evenly on the residual limb, and to facilitate donning procedure.

The main site of weight bearing in the old prosthesis (PTB) was anterior proximal region of the residual limb, especially the patellar tendon. The pressure was almost 10 times higher than the distal region during level walking. Pressures were distributed more evenly with the TSB socket design, and the donning was much easier.
Pressure distribution within the socket could be affected by socket design and suspension system. Using the TSB socket and Velcro as suspension system might facilitate donning of prosthesis and reduce traction at the end of residual limb during the swing phase of gait.
Gholizadeh H, Abu Osman NA, Eshraghi A, Afirin NA, Yang CT. A comparison of pressure distributions between two types of sockets in a bulbous stump. Prosthetics and Orthotics international. (2014), (Accepted)
0203
Daiki Shimotori (1) presenting Yoshihiro Ehara (1) Takahiro Gou (2) Mayuko Ikeda (1) Motohiko Takahashi (1) Yu Maeda (1)
Niigata University of Health and Welfare, Niigata, Japan (1) Katou Gishi, Niigata, Japan (2)
Measurement of the rotation axis of the ankle in vivo
Mechanical joint axis of an Ankle-Foot-Orthosis should be placed on the patient’s anatomical foot joint axis of rotation. The misalignment of anatomical joint axis and orthotics joint axis generates undesirable piston-like motion between his or her shank and the orthosis. Previous studies have defined the anatomical joint axis based on cadaver of lower limb skeleton [1]. However, the joint axis of a cadaver foot might be different from a living foot.
This study aimed to calculate the rotation axis between the shank and the foot in vivo with 3D motion analysis system, VICON.
Six healthy subjects, aged between 20 and 23, voluntary participated in this study. Subjects stood on a 15 degree slope with their soles touching to the surface of it, and took hold of a handrail to keep their balance. The subjects performed flexion and extension of the knee joint during about 2sec trial, so that the shank could move from 15 degree planter flexion to 30 degree dorsiflexion around the foot. The trajectory of reflective markers on the shank segment and the foot segment were measured by VICON motion analysis system with sampling rate of 100Hz. Each subject performed 10 trials.
3D direction of the rotation axis was calculated as the vector perpendicular to the plane that contained the trajectory of the shank markers. The instantaneous centre of rotation was determined as the point of the intersection of two lines which were the perpendicular bisectors of the arc on the trajectory.
The rotation centre of the lateral side was located 2.3±3.4mm posterior and 0.3±0.4mm superior from the lateral malleolus centre. The rotation centre of the medial side was located 13.9±6.0mm posterior and 1.0±1.2mm superior from the medial malleolus centre.
The cadaver study showed that the rotation centre of the lateral side was located 11mm anterior and 12mm inferior from the lateral malleolus centre, and that the rotation centre of the medial side was located 1mm posterior and 16mm inferior from the medial malleolus centre. In our study, the rotation centre of the lateral side was almost coincident with the location of the lateral malleolus. For the medial side, it was located 14mm posterior from the medial malleolus. This discrepancy between the cadaver study and our study might be due to the ligament and the muscle force.
The rotation axis of individual living feet were obtained.
[1] Isman RE, et al ; Bull Prosthet Res,1969
0204
Akouetevi Aduayom-Ahego (1) presenting Yoshihiro Ehara (1)
Niigata University of Health and Welfare, Niigata, Japan (1)
Estimation of the location of the hip joint center based on potential energy and mechanical work
Accurate position of the joint center when collecting three-dimensional motion analysis data is important. The combination of ground reaction force, kinematic, and anthropometric data leaves many possible sources of error in the calculation of joint forces and moments. The accuracy of the kinetic data such as the hip joint moment is highly dependent on the location of the hip joint.
The aim of this study is to estimate the location of the hip joint center by comparing the potential energy and the mechanical work, and to establish the new method to define the location of the hip joint center.
A group of five healthy students between the ages of 20 and 28 with the ability to flex and extend joints without assistance participated in the study. Participants were instructed to stand and bow with his or her trunk about 40 degree forward bending. From this posture participants were instructed to extend slowly the hip joint from approximately 40 degree flexion to full extension motion so that they could stand back to their posture of the verticality. Kinematic data was collected with an eleven camera VICON system. Two AMTI force plates collected data simultaneously for the calculation of joint kinetics. All data were processed using Nexus, and the location of the hip joint centers were calculated by using a conventional method. Then the hip joints were relocated 5mm to 55mm posterior from the original position. For each hip joint location, potential energy and mechanical work of the joints were calculated and compared with each other.
For the original location of the hip joint center, positive power was generated at hip joint and potential energy of the body. However the knee joint and ankle joint generated very small power. As the movement started, the total work of the joints and the potential energy increased respectively up to 20J and 25J, and then attained the peak when the motion ended. About 20% of the difference between the work and the potential energy was observed. The hip joint displacements (from 5mm to 55mm) in posterior direction affected the hip power and the work. When the hip joint centers were moved 27mm posterior from the original position, the total work became closest to the value of the potential energy.
The inaccuracy of the estimation of the joint center location might be the main error of the joint moment calculation. When the joint moments are accurate, the total work of the joints should be identical with increase of the potential energy. Using this concept we estimated the best location of the hip joint center, which is 27mm posterior from the original position.
0205
Woo Sob Sim (1) presenting Woo Sung Seong (1) Hee Seung Yang (2) Dong Young Ahn (1) Hea Eun Yang (2)
Veteran Health Service Medical Center Department of P&O Center, Seoul, Gangdong-gu/Dunchon-dong, Republic of Korea (1) Veteran Health Service Medical Center Department of Physical Medicine and Rehanilitation, Seoul, Gangdong-gu/Dunchon-dong, Republic of Korea (2)
The Effect of Postural Support Device on Wheelchair Usersip joint center, which is 27mm posterior from the original position.nd
Postural support device (PSD) is to support posture by applying a seat-shaped device to a wheelchair or chair for the disabled with cerebral palsy (CP), spinal cord injury (SCI) who needs postural support. Previous studies include a survey on the satisfaction of the effect of customized seating system and PSD conducted targeting disabled children with CP, but studies on the effect of application of PSD targeting the disabled with SCI still remain insufficient.
The aim of this study is to enable the disabled to maintain the optimum sitting posture by analyzing maintenance of sitting posture and distribution of buttock pressure in accordance with the PSD targeting the disabled with SCI.
Total five patients were enrolled who have been diagnosed as quadriplegia or paraplegia with experience of pressure ulcer and treatment has been completed. They have used wheelchair more than five hours a day. Patients with hip flexion contracture or heterotopic ossification were excluded. This study measured buttock pressure using Body Pressure Mapping System (BPMS) and analyzed their sitting posture by using 2 digital cameras and Dartfish Teampro 6.0 program. To evaluate the effect of fitting PSD, all data were analyzed by paired t-test with SPSS ver. 12.0 and the results were found to be statistically significant at p<0.05.
All subjects were male and their mean age was 51.6cts 36 years, mean weight was 67.2±9.18㎏, mean wheelchair using time was 25.42±9.18n image or insert a table ) wheelchair for a day was 7.6was 25.42±9.18n image or insert a table ) subjects belong to level C, 2 were in level T, and in ASIA classification, 3 were in A, 1 in B and 1 in C. When the subjects sat in the wheelchair without a PSD, contact area between seat of wheelchair and buttock was 160.4assifi㎠ but increased significantly to 236.2air an㎠ when they used a PSD. While hip joint flexion angle was 106.92ssification, 3 were in A, 1 inased to 98.82±4.59° when using a PSD. Tilt angle of head was −7.54 they used a PSD. While hip joint flexion angle was 106.92ss–2.97 they used a PSD. While hi
When a PSD was applied according to the result of this study, contact area increased and it decreased maximum pressure on a specific area of body by dispersing buttock pressure properly, tilt angle of head came close to a correct sitting posture. Application of a PSD has a positive effect on wheelchair sitting posture and prevention of pressure ulcer for the disabled with spinal cord injury.
0206
Atsushi Tagawa (1) presenting Youhei Konishi (1) Ko Asayama (1) Kenji Kai (1) Katsuyoshi Setsu (1) Kei Hori (1) Fumitada Hattori (0)
nagao hospital, fukuoka, Japan (1)
Evaluation of the efficacy of simple plastic surgery to hemiplegic foot deformity; its effect regarding the changing of physical performance and of orthotic type
Spastic gait in stroke hemiplegia causes obstructive factors, especially among Japanese barefoot living-in feel. Through the simple plastic surgery on involved foot deformity, the effect of following accompanying factors was compared before and after the procedure; change in spastic foot correction, alleviating the pain complaints, obtaining barefoot walk, improving the gait ability along with changing in the orthotic type.
With simple corrective surgery to spastic deformed foot, many patients become to adjust their Japanese life style, to improve physical activity and to change their mal adjusted orthotics to cosmetic, lighter one and, or to gain barefoot walking. These changes were investigated for the presentation.
Five years duration, from Sep.2009 to august 2014, 61 hemiplegic subjects (64 legs) received simple foot plastic surgery. Age: mean 61.5 ±11.1SD years. Suffering duration: minimum 4.5 to max 405 months, 30male, 31 female. Palsy side: 30 : right, 27 left, 4 bilateral. Brunnstrom recovery stage: Ⅱ;2, Ⅲ;18, Ⅳ;20, Ⅴ;17 others;4 case.
Before and after the surgery, the following evaluation was measured: Walk of functional independence measure (wFIM), orthotics style, 10m walking test (10MWT: time and step), indoor bare foot walk ability. The subjects of more than 5 point by wFIM (above supervision level) were selected. Paired t test was used for statistical analysis. Orthotic style was classified into 5 grades up to its control force.
More than 5 score by wFIM scale (45 cases) and 11 cases by 10MWT scale were selected for the evaluation. The number of wFIM improvement was 13, decreased one was 1, and no change was 31. Regarding the orthotic change, 8 cases became less control degree, 4 cases became more, and 33 cases didn’t change. Number of indoor bare foot walker increased up to 31 (26.67%) post operatively. About 10MWT, time was 18.62±5.90 sec vs. 16.97±4.40sec: p=0.088. Step was 27.91±5.00 steps vs. 26.54±6.30 steps; p=0.176.
Simple plastic surgery can bring certain amount of expected effects on hemiplegic foot deformity. Present foot surgery to stroke foot enhanced ADL freedom rather than gait ability, by changing the orthotics to more comfortable one, and improving patient’s satisfaction more toward the newly provided orthotics. Gaining bare foot ambulation through the procedure enables patients living in Japanese life style to walk with bare foot or with simple AFO on Tatami floor.
0208
Yukio Mikami (1) presenting Kouki Fukuhara (1) Toshihiro Kawae (1) Hiroaki Kimura (1)
Hiroshima University Hospital, Hiroshima, Japan (1)
The effect of anti-gravity treadmill training for prosthetic rehabilitation of two cases with lower limb amputation
The anti-gravity treadmill applies air pressure to a patient’s lower body to alter body weight support and can decrease the load on lower extremities and cardiovascular function. Therefore, the anti-gravity treadmill could be a useful instrument for prosthetic rehabilitation of lower limb amputees, especially for those patients with reduced physical strength and vitality. However, so far there have been no reported investigations of the efficacy of anti-gravity treadmills for prosthetic rehabilitation.
The aim of this case study was to verify the efficacy and safety of anti-gravity treadmill training for prosthetic rehabilitation for lower limb amputees.
Case 1 underwent left below-knee amputation as a result of diabetic foot gangrene and Case 2 underwent bilateral above-knee amputations as a result of a traffic accident. Outpatient rehabilitation was conducted for 20-40 minutes three times a week for six weeks (Case 1) and for six months (Case 2), using the anti-gravity treadmill. At the initial and final examinations, performance of walking on the floor including a six-minute walking distance was evaluated. During anti-gravity treadmill training, pulmonary gas exchange was measured breath-by-breath with a mobile aero monitor. Oxygen consumption rate was recorded throughout the tests.
Stable prosthetic gait exercise was possible, resulting in improved gait. Before the introduction of anti-gravity treadmill training, Case 1 required crutches and assistance when walking. However, at the final evaluation, the patient had fully acquired prosthetic gait ability with the aid of a T-cane and no longer required assistance. At the initial examination of the study, the six minutes walking distances were 230m in Case 1 and 30m in Case 2. However, at the final evaluation of the study, the walking distances were 331m in Case 1 and 198m in Case 2. Oxygen consumption rate at the final evaluation was lower than that at the initial examination for the same treadmill conditions, demonstrating improvement in motion efficiency following anti-gravity treadmill training.
Two cases of lower limb amputation (caused by diabetic gangrene and a traffic accident) were reported where prosthetic rehabilitation using an antigravity treadmill was shown to be successful and efficient. Stable walking exercises could be performed with little risk of falling. After training, exercise tolerance was elevated and the patients progressed efficiently to improve their prosthetic gait performance. The antigravity treadmill is therefore recommended as a useful instrument for prosthetic rehabilitation for lower limb amputees.
0209
Kajsa Lindberg (1) presenting Morten Tange Kristensen (2)
Rehabilitation Centre Vanløse, Copenhagen Municipality, Denmark (1) Physical Medicine and Rehabilitation Research – Copenhagen (PMR-C), Departments of Physiotherapy and Orthopaedic Surgery, Copenhagen University Hospital Hvidovre, Denmark (2)
Construct validity and responsiveness of functional measures used in lower limb amputees following an outpatient prosthetic rehabilitation program
Patients surviving a major lower limb amputation (LLA) are quite often provided with prosthesis for optimised function in daily life. Still, there is a lack of knowledge about the effect of early rehabilitation programs, as to which tests to be used to show progress.
To examine construct validity and internal responsiveness of performance-based measures of functional mobility and endurance after LLA. Secondary, to evaluate if performances differed between amputee levels and gender.
Eleven women and 31 men with a mean age of 63.9 (SD 11.5) with a recent below knee (BKA, n=24) and above knee (AKA, n=18) amputation. All amputees followed a rehabilitation program (twice weekly); focused at improving balance, muscle strength, and prosthetic function. The Timed Up and Go (TUG), the 10 meter fast speed walking test (10MWT) and 2-minute walking test (2MWT) were performed at baseline and end of the program. Pearson’s r was used to assess construct validity. Responsiveness was assessed by calculating the effect size (ES) as the mean change in performance scores divided by the baseline SD, and the standardized response mean (SRM) as the mean change in scores divided by the SD of changes.
Performances of the three tests improved (P<0.001) from 34-85% ; the TUG from a mean (SD) of 34.5 (23.4) seconds to 18.9 (11.3) seconds, the 10MWT from 0.47(0.33) meter per second (m/s) to 0.80 (0.47) m/s and the 2MWT from 58.5 (31.5) meters to 90.4 (44.0) meters.Amputees with a BKA performed the three tests faster (P≤0.003), than those with an AKA at both assessments, but with larger improvements seen for the AKA group compared to the BKA group. On the contrary, no significant difference in performance was observed between men and women. The three outcome measures were highly correlated at baseline (r>0.63, P<0.001) and at end of the program (r >0.80, P<0.001). Responsiveness was high for all tests: TUG (ES 0.67, SRM 1.00), 10MWT (ES 1.00, SRM 1.10) and 2MWT (ES 1.01, SRM 1.15).

Construct validity and internal responsiveness of the three measures were high, and they all seem able to distinguish between amputee levels. We recommend other centres use the three tests. Only one-fourth walked faster than 1m/s, supporting the need for studies examining the effect of e.g. progressive strength training for further improvements.
0210
Amir Shahzad (1) presenting
PIPOS, Peshawar, Pakistan (1)
Causes of club foot at PRSP, KPK, Pakistan
Club foot or CTEV is one of the deformities of the lower limb that is most commonly perceived. Many epidemiological studies are being held to know the cause, even though it is concluded that genetic and environmental factors play central role to cause the disorder but exact cause is still remains unknown. Outcomes of epidemiological studies were remained to apply in Pakistan.
To explore the cause of CTEV and evaluate the cause of club foot from the known cause, which is, published previous literature.
The Study design was a Questionnaire survey (descriptive) and conducted at PRSP, Peshawar from April 11 to May 30, 2014. PIPOS Rehabilitation Services Program (PRSP) is the leading Institute in Pakistan consisted of many centers across the country. The inclusion criteria was club feet and exclusion criteria was more than the age of 12 months. All the information were collected by the subject parents. The data were analyzed using SPSS 20
Sample size was 107 consisting of 84% male and 16 % female. Minimum age of participants was 1 and maximum age was 24 with mean of 8.22± 6.10. Mostly mother of affected child was illiterate and belonged to rural area of KPK. 78% of respondent married within the family while 22% of respondents married outside the family. Study contained 65 % participants were bilateral and 35% were unilateral. There was no effect of age of parent on the occurrence of club foot. The study included 18 participants were having effected siblings in which at least 1 and utmost 2 siblings were present. There were no participant whose mother did smoking during pregnancy but there was 47 participants whose father did smoking. Only five child who had neuromuscular disorder.
My study showed the positive family history likewise previous studies. In contrast to epidemiological study, my study showed that there was no mother who did smoking during pregnancy but similar to father smoking.
A huge of participant’s mother were illiterate. Respondents were affected more bilaterally as compared to unilaterally. Ratio of male was higher than the female similar to previous studies. The data also showed that participants having affected siblings. It has clearly showed that parental smoking can also cause the defect but my study didn’t take any case whose mother did smoking during the pregnancy.
0215
Ludger van Dijk (1,2) presenting Hylke van Dijk (3) Corry van der Sluis (1,2) Raoul Bongers (1,2)
University of Groningen, Groningen, The Netherlands (1) University Medical Center Groningen, Groningen, The Netherlands (2) NHL University of Applied Sciences, Leeuwarden, The Netherlands (3)
Does EMG control transfer from a serious game to prosthesis use?
State-of-the-art myo-electric prosthetic hands require generating complex EMG signals for appropriate control. However, current prosthetic rehabilitation training does not train prosthesis users to reach such an advanced level of skill. Employing serious games in rehabilitation may offer a way of doing that - allowing for feedback about EMG signal quality tailored to an individual user while also creating an enjoyable and stimulating learning context. However, serious games often also change the task the generated EMG signals are involved in. As research suggests skill learning may be fundamentally based on the task the actions aim to accomplish, the question that needs to be addressed is whether learning to control the EMG signal in a serious game will transfer to prosthesis use in daily life.
To establish (1) whether the control of EMG signals can be trained through serious gaming, and (2) whether this control transfers to a prosthesis-simulator task.
In an experimental pre-test post-test design we trained 15 able-bodied participants to control a video game (Breakout). The goal of the game was to hit bricks by bouncing a ball using a paddle. Participants controlled the movements of the paddle through the EMG signals of the flexors and extensors of the wrist. Another 15 participants, making up the control group, played a regular Mario computer game. Two tests were conducted: (1) one level of the Breakout game was performed and the accuracy of intercepting the ball and EMG signals were measured, (2) participants grasped objects that varied in size with a prosthesis-simulator. Movement time and hand aperture profile were measured.
Analyses showed strong learning effects within the gaming task – on accuracy as well as on the effectiveness of the generated EMG signals. There was no transfer to the task with the prosthesis-simulator.
To employ serious gaming in prosthetic rehabilitation it is required that actions used in prosthetic tasks improve by playing the game. The current research suggests that this is not always the case. The results will be used to provide guidelines for a serious game to train prosthesis use.
Training sophistication of EMG signals through serious gaming leads to improvement of in-game performance but transfer to prosthetic control is limited.
0216
Dayna Pool (1,2) presenting Catherine Elliott (1) Natasha Bear (1) Jennifer Colegate (1) Cyril Jon Donnelly (2) Katherine Stannage (1) Jane Valentine (1)
Princess Margaret Hospital For Children, Perth, Western Australia, Australia (1) School of Sport Science Exercise and Health, The University of Western Australia, Perth, Western Australia, Australia (2)
The orthotic and therapeutic effect following daily community applied functional electrical stimulation in children with unilateral spastic cerebral palsy: a randomised controlled trial
Children with unilateral spastic cerebral palsy (USCP) are functionally ambulant, but equinus and drop foot during gait are common, alongside functional issues with balance and community mobility. Whilst there have been some reports that Functional Electrical Stimulation (FES) may address these problems in gait (providing an orthotic effect) that may even be sustained without FES (therapeutic effect), the evidence supporting this in children with USCP has so far been inconclusive1.
The aim of this study was to determine the orthotic and therapeutic effect of daily community applied FES to the ankle dorsiflexors in a randomized controlled trial. The primary outcome measures included ankle kinematics, temporal-spatial gait measures and community mobility.
This randomized controlled trial involved 32 children (15 females, 17 males; age range 5y 5mo to 18y 1mo; median age 10y 3 mo) with USCP and a Gross Motor Function Classification System of I or II. Children were randomly allocated to a FES treatment group (n=16) or control group (n=16). The treatment group received eight weeks of daily FES that was worn at home and community (four hours/day, six days/week) whilst the control group received usual orthotic and physiotherapy treatment. Children were assessed at baseline, post FES treatment (eight weeks) and at follow-up (six weeks later). Ankle kinematic and temporal-spatial measures with and without FES were analysed using video software with force platform data to signal gait events. Community mobility was assessed using the Community Mobility Balance Scale and participant performance and satisfaction on the Canadian Occupational Performance Measure.
All 32 children who entered the study finished the study in their original group allocation. FES was well tolerated with usage logs indicating mean daily use of 6.2 hours (SD 3.2 hours). Mixed ANOVA for repeated measures revealed that with FES, the treatment group demonstrated a significant improvement in initial contact ankle angle (p <0.001), maximum dorsiflexion ankle angle in swing (p=0.007), time in stance (p =0.011) and step length (p= 0.035) post treatment when compared to the control group. The treatment group had significantly better community mobility post treatment (p <0.001) and at follow-up (p <0.001). Participants in the treatment group reported significantly higher performance (p =0.034) and satisfaction (p =0.004) post treatment and in satisfaction only (p =0.030) at follow-up.
This study provides Grade II level evidence supporting daily community FES in children with USCP. The direct orthotic effects in gait are use-dependent. However therapeutic effects in community mobility were not only noted in the treatment group post treatment but also at follow-up suggesting the role of motor learning. Therefore, FES can be considered to be an appropriate treatment option to address gait and community mobility problems in children with USCP.
1 Cauraugh J.H., et al 2010, Clin Rehabil
0218
Lara Grobler (1) presenting Suzanne Ferreira (1) Elmarie Terblanche (1)
Stellenbosch University, Stellenbosch, South Africa (1)
Responsiveness of different running specific prostheses
The competitiveness of sprint races for athletes with lower limb amputations has increased significantly. Similarly, running specific prosthesis (RSP) has also undergone much change. However in a review by Bragaru et al. (2012) it was stated that there was a scarcity in literature regarding sport prostheses and that more effort should be made to publish data on the characteristics of the prostheses.
The aim of this study was to determine the difference in the reactive strength characteristics of two different types of RSPs.
Two different types (E and X) of RSPs were tested in seven different alignment settings. RSP type X is prescribed for short distance sprints (100 and 200m) and E for longer distances (> 400m). Three categories (3, 4, 5) based on athlete weight class were used for both RSP types. The prosthesis was attached to a socket specifically designed for this testing. The socket in turn was attached to a smith machine loaded with 28, 38 and 48 kg. The weight was dropped from a 30cm height, while the Optogait measurement equipment (Microgait, Italy) was used to measure contact and flight time of the first hop of the RSP. Changes were made to both the RSP length and attachment angle. Each setup was dropped three times per weight category and the mean of the three drops was used for analysis.
The contact time and flight height obtained from the Optogait was used to calculate the reactive strength index (RSI) of the different blades. Between blade types E and X there were statistically significant differences in category 3 (E = 141.83 ± 12.34 cm.s-1 vs. X = 114.85 ± 9.66 cm.s-1), category 4 (E = 145.86 ± 10.80 cm.s-1 vs. X = 118.21 ± 10.51 cm.s-1) and category 5 (E = 152.51 ± 10.90 cm.s-1 vs. X = 129.16 ± 10.81 cm.s-1). Statistically significant differences were observed between category 3 and 5 as well as category 4 and 5 (p < 0.05).
From the results it was evident that there is a difference in the reactive strength of the two different types of RSPs, with type E having a greater reactive strength than type X. This is contrary to what was expected as type X is said to be designed for shorter distance sprints. These differences may be attributed to the shape of the RSP and its recoil action.
Bragaru, M. ; Dekker, R. & Geertzen, J.H.B. (2012). Sport prostheses and prosthetic adaptations for the upper and lower limb amputees : an overview of peer reviewed literature. Prosthetics and Orthotics International. 36(3):290-296
0220
Mary Jane Cole (1) presenting
Kingston and St George’s, University of London, London, UK (1)
Equipping therapists to rehabilitate amputees post natural disaster – BACPAR’s (British Association of Chartered Society of Physiotherapists in Amputee Rehabilitation) collaboration with Handicap International (HI) and the UK International Trauma Register (UKIETR)
The UK International Emergency Trauma Register (UKIETR) was established to facilitate the deployment of surgical teams from the UK to sudden onset disasters overseas. Traditionally therapists have not been included in medical humanitarian response teams however recent research and best practice guidance has placed rehabilitation professionals at the forefront of the emergency response. Handicap International (HI) were awarded funding for 2 years to integrate rehabilitation professionals into the UKIETR. HI is working with several UK physiotherapy professional networks – including BACPAR – to train and deliver training appropriate for the humanitarian context to therapists on the register.
The development and delivery of theoretical, practical and e-learning modules aim to equip therapists on the UKIETR with relevant specialist knowledge and skills to manage people acquiring amputation following natural disaster.
Under the guidance of HI, BACPAR was tasked with developing and delivering 3 amputee specific modules to therapists on the Register. The core amputee rehabilitation training module focuses on acute management including pre-amputation, perioperative and pre-prosthetic phases. Participants complete a post core training self-assessment and attend a top-up workshop (practical training module) to develop competence and confidence with practical skills as required. An e-learning module is in development to support and complement prior learning, advancing theory in key areas in an emergency context.
Overall there has been a positive response by UK therapists to supporting an emergency response with 63 joining the register by October 2014. BACPAR’s collaboration with HI is also prompting therapists specialised in amputee rehabilitation to join the UKIETR. Core training and workshop modules in amputee rehabilitation are being delivered across the UK. To date 2 core training modules have been delivered to 40 therapists in London. Self-assessment post core training has prompted 1 practical workshop to date with 10 participants and further trainings planned. Feedback has been positive to module content and delivery. At the time of writing the e-learning module remains in development.
“Early rehabilitation can greatly increase survival and enhance the quality of life for injured survivors.1. The collaboration between HI and BACPAR is preparing therapists for deployment in the situation of a sudden disaster and reflects the movement towards increasing professionalism
standards in humanitarian response. The uptake of therapists on the UKIETR is encouraging and feedback on training is positive, however the effectiveness of the deployment of appropriately trained therapists in a post disaster will need to be evaluated following future sudden onset disaster.
1. Humanitarian Charter and Minimum Standards in Humanitarian Response Third Edition 2011. The Sphere Project. www.sphereproject.org
0221
Abdullah Fatlawi (1) presenting
Uiversity of Strathclyde, Glasgow, UK (1)
Appropriate liner technology for low income and post war countries
The World Health Organization (WHO) estimate that one billion people worldwide experience some form of disability and that the majority are from low to middle income countries
The demands for prosthetic needs are increasing particularly in war zones. A variety of prosthetics liners are available in the developed world and may offers benefits for the use with prostheses. Such liners are generally expensive and therefore unobtainable in the developing countries.
The aim of the study is to investigate the need for a custom made silicone liner for prosthetic use in low Income (LICs) or Post War Countries (PWCs), and explore the possibility of fabrication for trans-humeral (TH) level.
A literature review was conducted and the advantages and disadvantages of silicone liners discussed. Design criteria using low cost materials for silicone liner production in LIC/PWCs were presented.
The search strategy was intentionally liberal to select as many potential articles as possible. Terms were individually entered, occasionally excluding previous terms, avoiding duplication. Titles, and where appropriate abstracts, were read to ascertain individual paper contents. A traffic light system was used. Red – ignore. Yellow – considered. Green – include. Mainly studies which included upper limb (UL) prosthetics level of amputation were included in the search.
Several databases were searched including: Medline: Embase, Cochrane library, SUPrimo, google news search, compendex, sciencedirect and google scholar.
Results were organised into 2 tables for clarity; ‘previous attempt to produce liners’ and ‘types of silicone’. Table 1 lists previous attempts of liner production. 3 papers were found from literature, two of which considered custom made liners and one technical note on the production of hand prosthesis for partial hand amputation. No of the study concerned manufacture of silicon liners for use for LICs only. Tables are too much to be uploaded on this document
Design criteria were developed to facilitate production of silicone liners in LICs/PWCs and included: affordability; durability; easy of manufacture; easily obtainable materials / equipment; and biocompatibility. A production method was determined. Such liners would minimise material usage while maximising value. Costs will be as low as £4.
0222
Mary Jane Cole (1) presenting Rosalie Barrett (2) Penny Broomhead (3)
Kingston and St George’s, University of London, London, UK (1) University of Brighton, Sussex, UK (2) Independent practictioner, England, UK (3)
The UK International Emergency Trauma Register (UKIETR) provides specialist amputee rehabilitation training to local staff in Gaza following the 2014 conflict
In July and August 2014, 2,150 Palestinians and 73 Israelis were killed in the conflict between Gaza and Israel. Approximately 11,000 Palestinians were injured. The UK International Emergency Trauma Register (UKIETR) undertook a remote needs assessment and a critical need for specialist training of multidisciplinary rehabilitation staff in Gaza was identified in order to treat and improve management of complex trauma cases including people with limb loss.
This case example illustrates how a rehabilitation team from one country (i.e. the UK) provided support to local community teams (supported by Handicap International (HI)) via ‘on-the-job’ work-based learning and workshops – including amputee rehabilitation – to local and international rehabilitation providers.
3 small teams of clinicians (physiotherapy, nursing and occupational therapy) with a range of specialist knowledge and skills were deployed to Gaza over 2 months. Capacity and topics for workshops were identified in consultation with local HI in-country staff through working with outreach teams and collaboration and visits to rehabilitation providers including the International Committee of the Red Cross (ICRC) and Gaza’s Artificial Limb and Polio Centre (ALPC). Participants completed a pre and post-training self-assessment to reflect change in confidence with competencies. Clinical work-based learning happened throughout the deployment and after each workshop to facilitate teams apply newly learned theory.
Areas where specialist knowledge in managing trauma cases is required were identified. In addition, the rapidly evolving crisis situation led to gaps in awareness of the best referral pathways among local providers e.g. to the prosthetic service in Gaza. UKIETR team members provided 32 clinical days of work-based learning. 141 trauma patients were treated; 16% amputees. 15 specialist workshops were delivered to 364 staff. The 3 amputee rehabilitation workshops were delivered in partnership with ICRC and the ALPC to enable local staff to deliver enhanced amputee rehabilitation in the community in preparation for prosthetic referral. Feedback and self-assessment indicated that the workshops enhanced clinical knowledge and skills and work-based learning in the community setting was valued.
Rehabilitation following a humanitarian crisis (conflict or natural) is necessary 1. This case example illustrates the need for timely rehabilitation support, increased capacity amongst local staff and specialist knowledge (and skills) in less resourced settings following conflict. Deployed teams enabled local staff to enhance their clinical skills and knowledge to improve the management of complex trauma cases – including amputees – in the community setting. Further research is recommended to identify the impact of this support on local staff, practice and patient outcomes and to explore the experience of those deployed.
1. Knowlton et al. 2011. Prehospital and Disaster Medicine.
0223
Kevin Murray (1) presenting Jonathon Corney (1) Karena Moore-Millar (1) Nicola Cairns (1)
University of Strathclyde, Glasgow, UK (1)
Extending the life and improving the appearance of cosmetic foam covers for people with trans-femoral amputations
Flexible polyurethane (PU) foam cosmeses are a widely used component of lower limb prostheses. Current practise is that they are shaped to match patient’s requirements (size and shape) and then covered in a nylon stocking to enhance the cosmetic appearance of the prosthesis.
This investigation into improving the material used in the covering of prosthetic limbs has resulted in a modification to the established design that significantly improves the lifespan, appearance and functionality of cosmetic foam covers.
To improve the durability and lifespan of standard cosmetic foam covers on lower limb prostheses and improve physical access to prosthetic components, for routine alignment changes and/or mechanical maintenance.
Ease of removal was enhanced by the introduction of a medially positioned internal zip. The life and appearance of the cosmesis was improved by the addition of a plastazote foam patella insert into a hole cut in the foam over the knee area.
Six prototype foams were manufactured and fitted during clinical trials. 3 technicians and 7 patients completed a questionnaire following manufacture and at 4 and 8 week review periods. Two standard and four modified foam covers were tested for durability using a bespoke electromechanical test rig. The rig fully flexed and extended the prosthetic knee during rotation, simulating both walking and sitting activities.
The questionnaire suggested that the manufacturing time of 3-4 hours was the same for both traditional and removable foam covers. During review appointments the insertion of the medial zip made it easier to don/doff the cosmesis without damaging it and reduced the time required to adjust knee mechanisms or complete maintenance checks. The medial zip was well concealed and had no detrimental effect on cosmesis when stockings were applied. The patellar insert improved the realistic shape of the cosmesis and the hole cut out increased the flexibility of the foam. Patient responses were generally positive as the knee insert made kneeling more comfortable and improved cosmesis through clothing while sitting.
The results of fatigue tests on 4 modified and 2 standard foams suggested that cosmeses with knee hole cut outs last over 300% longer (i.e. 1.12M compared to 0.35M cycles).
By comparison to traditional foam covers the new removable foam cover with knee hole cut out improved the durability of the foam over the knee by a factor of 3. The patellar insert improved cosmesis appearance through clothing while sitting and comfort while kneeling. Anecdotally patients commented on increased knee flexibility when first fitted. Maintenance and adjustment time was reduced at review appointments and the overall time to manufacture remained the same.
Satisfaction with cosmesis and priorities for cosmesis design reported by lower limb amputees in the United Kingdom: instrument development and results. Cairns N. et al, 2014 POI.
0224
Ronald Bos (1) presenting Claudia Haarman (2) Teun Stortelder (2) Kostas Nizamis (2) Just Herder (3) Dick Plettenburg (1) Arno Stienen (2,4)
Department of Biomechanical Engineering, Delft University of Technology, Delft, The Netherlands (1) Department of Biomechanical Engineering, University of Twente, Enschede, The Netherlands (2) Department of Precision and Microsystems Engineering, Delft University of Technology, Delft, The Netherlands (3) Department of Physical Therapy and Human Movement Sciences, Northwestern University, Chicago, IL, USA (4)
Exploring the solution space of hand assistive devices using an overall framework
Many stroke survivors or people with Duchenne Muscular Dystrophy (DMD) are limited in hand dexterity, often negatively affecting independency and social interaction. Assistive devices for the hand aim to recover or enhance hand functionality, ultimately improving the quality of life for such individuals. Many devices have already emerged and cover a large solution space, but they can also be linked through their fundamental design choices in function, energy and mechanism.
This study aims to provide for an overview of the complete solution space of hand assistive devices using an overall framework, by connecting the state-of-the-art on these devices through their fundamental design choices.
During the literature search, only design and review papers of hand assistive devices were included in the analysis. The proposed framework consists of a structure of tree diagrams, allowing for backwards reasoning towards the fundamental design choices and forwards reasoning towards a multidisciplinary solution space. The basis is formed with three core aspects through which the device interacts with the human, introduced as ‘function’, ‘energy’ and ‘mechanism’. On one side of these core aspects, preliminary design strategies were defined which are independent of physical components and formed the roots of the tree diagram. On the other side, branches reach out towards unique component implementations.

A total 77 different hand assistive devices were found. The majority focuses on the development of devices for a domestic setting, allowing physical therapy at home or assisting activities of daily living. The established framework reveals 97 unique component implementations, of which 44 were used only twice or less (e.g. task-monitoring control, hydraulic transmission). The most popular method for actuation is by far electric, mostly DC motors. The use of force control, transmission by (Bowden) cables and underactuated finger mechanisms are the most reoccurring component implementations.
Results show that the development of a hand assistive device is becoming increasingly popular and the established framework illustrates the high complexity and diversity. The number of rarely-used compared to favoured component implementations indicates that the complete solution space is not yet fully explored. Here, the presented framework may help in the search for such novel solutions.
This research is supported by STW (NL, #12479, #13524 and #13525), Hankamp Rehabilitation (Enschede, NL), Hocoma (Volketswil, CH), TMSi (Oldenzaal, NL), Moog (Nieuw Vennep, NL), FESTO (Delft, NL), and multiple Duchenne foundations (NL & USA).
0225
Anja Udovcic Pertot (1) presenting Helena Jamnik (1)
University Rehabilitation Institute Republic of Slovenia, Ljubljana, Slovenia (1
Three-dimensional analysis of spinal motion and cervical joint position sense in healthy subjects: normal values and inter –examiner reliability study
Describing and measuring active range of motion in especially cervical and lumbar segments of spine are very important parts of procedure in patients with different spine diseases or trauma. Physical examination, observation and description of active range of motion are subjective methods and as such less reliable. Instrumental methods (goniometers,non-invasive three dimensional measuring devices) are more precise, but for clinical practise of comperable features.
In our study healthy volunteers’ active range of motion in cervical and lumbar segments of spine in all standard planes of motion were measured by Zebris CMS20 and inter-examiner reliability of these measurements were assessed. We also evaluated the inter-examiner reliability of cervical joint position sense measurements using test of head turning into neutral position.
A total of 28 healthy participants. Two examiners performed the measurements of three dimensional spinal motions and the test for cervical joint position sense. Descriptive statistics for active cervical and lumbar range of motion, relocation position error for cervical joint position sense were calculated and mean value of variation coefficient for all movements of cervical and lumbar range of motion were calculated. Correlation between all measurements and age and test retest reliability by intra class coefficient (ICC) were assessed.
The results for active cervical range of motion were comparable with data published in literature. Active cervical and lumbar ROM decreases with increasing age. Inter-examiner reliability of measurement of active cervical and lumbar range of motion was very high. Test- retest reliability of measurement of cervical joint position sense using test of head turning in neutral position was poor.
This study defined normative values and confirmed inter-examiner reliability for measuring active cervical and lumbar range of motion using a system for three dimensional analyses of spinal motion. The reliability of cervical joint position sense assessment using protocol of head turning in neutral position was not proven.
0227
Alessandro Zati (1) Elisabetta Mariani (1) Lorenzo Cavazzuti (1) Maria Grazia Benedetti (1) presenting
Physical Medicine and Rehabilitation Unit, Istituto Ortopedico Rizzoli, Bologna, Italy (1)
Use of an innovative temporary prosthesis for verticalization and early ambulation in patients with lower limb amputationsdue to oncological pathologies of the musculoskeletal system
Pneumatic prosthesis has long been used for amputations of vascular and metabolic origin, with the aim to reduce the edema of the stump, promote the verticalization and ambulation of the patient within short time, in order to preserve the body schema and reduce phantom limb sensation. This is the first feasibility study carried out in Italy on the early use of pneumatic prosthesis with innovative features in oncologic patients, developed through collaboration between RTM and Istituto Ortopedico Rizzoli.
The purpose of this study is to evaluate the feasibility of the postoperative use of a pneumatic prosthesis in early ambulation for patients who underwent lower limb amputation due to bone cancer.
Fourteen patients who underwent lower limb amputation were recruited: 7 trans-femoral amputation (group I), 5 trans-tibial amputation (group II). From the 4th post-operative day, with the removal of the drainage, the standard rehabilitation program was associated with gait training with a temporary pneumatic prosthesis (TPP), proprioceptive and balance exercises, and mirror therapy. In addition, local stump analgesia was achieved by continuous peripheral nerve block. Serial dressings, conical bandages and photographic monitoring of the surgical wound were performed every 3 days.
The evaluations were performed in 3 different times: T0 (ROM of the hip or knee); T1 (ROM, VAS-score, The 10 Meters Walking Test (10MWT), Musculoskeletal Tumor Society Test (MSTSt), Prosthesis Evaluation Questionnaire mobility stairs (PEQms)); T2 (ROM, VAS, 10MWT, MSTS, PEQms, Short-Form 36 (SF36)).
All patients showed a regular healing of the surgical wound . Two patients who had a local allergic reaction at he stump wound healed completely during the training with the pneumatic prosthesis.
ROM: all patients had a good recovery of joint ROM in flexion-extension of the hip (gr. I) and knee (gr.II) that remained constant or improved in T2.
VAS: pain was well controlled switching from a mean value of 2.4 in T1 to 0.8 in T2 in patients with trans-femoral amputation. Patients with trans-tibial amputation showed a variation between T1 and T2 from 2 to 1.2.
10 MWT: both groups examined at T1 and T2 showed a reduction in the execution of the tests, respectively, from 39" to 16" for group I and from 32" to 20" for group II.
MSTS: The results showed an improvement in functional performance between T1 and T2 in both groups: in group I 45 vrs 60 and in group II 60 vrs 69.
PEQ-Ms The scale showed a positive trend for both groups. All patients were satisfied about the trial with the pneumatic device (3.5 to 5.9 at T1 and T2 for group I, 4.6 to 6.9 at T1 and T2 for group II).
-SF 36: the values of the mental component (MC) has approached more to the average of the healthy population (MC=PC=50) compared to the values of the physical component (PC) for both group I (MC=50 and PC= 36)and II (MC=54 and PM=40)
This research showed the feasibility of early rehabilitation with innovative pneumatic prosthesis; in particular, patient compliance was high in the absence of adverse events. The good results in terms of pain control, ROM, walking performance and balance are accompanied by a normal healing of the surgical wound and an easier definitive prosthesization.
0231
Trivikram Annamalai (1) presenting Soikat Ghosh (1) Raju S (1)
Indian Institute of Technology Bombay, Mumbai,Maharashtra, India (1)
A low cost Special chair cum standing frame for children with cerebral palsy
The development aids made for children with cerebral palsy are usually one for seating and other for standing, which adds to the economic burden of people living below poverty line, also two products could mean additional space occupied in the already cramped small houses. Due to the lack of empathetic design the existing products are extremely repulsive to the children. This lead to the need for making an aid to overcome the above mentioned snags.
To make a low cost, pre-fabricated developmental aid, which meritoriously caters to the needs of children suffering from cerebral palsy, and is also space and material saving.
A clear design brief was made which lead to the directions of having a single product which could be used as both seating and standing frame, without compromising on the core functionalities that needed to be addressed for children with cerebral palsy. A parallel product study was done in that regard which further opened avenues on making a space saving design. Ergonomic data of Indian children were then incorporated in making the device along with considerations to stability of the product. Once a prototype was made, the product was tested on a child which lead to refinements and perfecting the device, lastly an asthetic upliftment was given to increase the visual appeal of the product.
The device was tested successfully with the service users who were happy with the salient features of the product like customizability the device provided for a growing child with adjustable features of foot-rest, hip width and thigh length / seat depth.

The device was found to cater well with the needs of the service user suffering from cerebral palsy, it can be safely concluded that the device will be helpful to the needy society.
1: Chung J, Evans J, Lee C, Lee J, Rabbani Y, Roxborough L, Harris SR. Effectiveness of adaptive seating on sitting posture and postural control in children with cerebral palsy. Pediatr Phys Ther. 2008 Winter;20(4):303-17. doi: 10.1097/PEP.0b013e31818b7bdd. Review. PubMed PMID: 19011521.
2. Ryan SE. An overview of systematic reviews of adaptive seating interventions for children with cerebral palsy: where do we go from here? Disabil Rehabil Assist Technol. 2012 Mar;7(2):104-11. doi: 10.3109/17483107.2011.595044. Epub 2011 Aug 30. Review. PubMed PMID: 21877900.
3. Puliti, B (2010) Today’s standing and seating options improve pediatric patients’ quality of life. ADVANCE for Physical Therapy and Rehab Medicine [serial online] 21(22) p37.
4. Wright C, Casey J, Porter-Armstrong A (2010) Establishing best practice in seating assessment for children with physical disabilities using qualitative methodologies. Disability and Rehabilitation: Assistive Technology, 5(1), 34-47.
0233
Hiroaki Kimura (1) presenting Akiyoshi Nagatomi (1) Yukio Mikami (1)
Department of Rehabilitation Medicine, Hiroshima University Hospital, Hiroshima city, Japan (1)
The brace therapy for hemophilic arthropathy
Hemophilia is a sex-linked recessive inheritance of disease that results in bleeding tendency due to the decrease of blood coagulation factors, develops a joint deformation (hemophilic arthropathy) by joint hemorrhage especially in severe cases. Although prophylaxis of blood coagulation factor for joint hemorrhage is useful, it is not possible due to medical cost and a self-injection problem. Since the hemophilic arthropathy affecting the QOL of hemophilia patients, simple and inexpensive treatment is required.
The aim of this study is to confirm the effect of the brace therapy for hemophilic arthropathy.
40 patients (40 males only with 37 hemophilia A and 3 hemophilia B) aged between 1 to 27 years (an average of 10.6) were recruited for the study. We followed for a mean duration of 24 months (range, 12-60 months). Radiographic evaluation of hemophilic arthropathy was performed using Pettersson score (13-point scale). We prescribed a rigid knee brace for one hemophilic knee arthropathy patient, the AFO with strut for one hemophilic ankle arthropathy patient and the soft brace (SHILAC Inc.,USA) for ten hemophilic ankle arthropathy patients.
We found hemophilic arthropathy in 23 cases of 58% (five cases with one joint, 18 cases with more than two joints), 12 cases of hemophilic knee arthropathy (seven cases with one side, five cases with both sides) and 17 cases of hemophilic ankle arthropathy (seven cases with one side, ten cases of both sides). Pettersson Score was from 1 to 13 points (an average of 9.5 points: hemophilic knee arthropathy 5.5 points, hemophilic ankle arthropathy 12.4 points). The brace therapy reduced the joint pain and subjective bleeding frequency. The exacerbation of Pettersson Score was 0.18 points / year.
Although prophylaxis treatment is useful for hemophilic arthropathy, it has been used only 20% of the world. The brace treatment can inhibit not only joint bleeds but also exacerbation change of arthropathy. Because the brace treatment is cheap and anywhere, it can be recommended widely for hemophilia patients and then reduce the medical cost.
We conclude that the brace therapy is useful for the treatment of hemophilic arthropathy.
0234
Krista L Best (1,2) presenting William C Miller (1,2) Grant Huston (2) Francois Routhier (3,4) Janice J Eng (1,2)
University of British Columbia, Vancouver, BC, Canada (1) GF Strong Rehabilitation Centre, Vancouver, BC, Canada (2) Centre interdisciplinaire de recherche en réadaptation et intégration sociale, Quebec City, QC, Canada (3) Université Laval, Quebec City, QC, Canada (4)
Self-efficacy enhanced wheelchair training for manual wheelchair users: A pilot randomized controlled trial of a peer-led approach
Training is an important component of wheelchair provision. Existing wheelchair training programs focus mainly on wheelchair skill acquisition and rely heavily on expert health professionals. Novel approaches to wheelchair training are needed to enhance wheelchair use self-efficacy1 and to reduce clinician burden2. Peer-led approaches have been effective at improving self-efficacy and changing behaviour in other clinical areas3. A community-based, peer-led
The primary aim of this study was to estimate the effect of WheelSee on wheelchair use self-efficacy. Secondary aims were to explore effect size estimates for wheelchair skills capacity and performance, wheelchair mobility, and satisfaction with participation.
Twenty-eight community-living, manual wheelchair users with various diagnoses who had mobility goals participated in a randomized controlled trial. Participants in the intervention group (n=16) received 6 x 1.5 hour sessions of individualized, peer-led wheelchair training in pairs. Participants in the control group (n=12) received no intervention. Analysis of co-variance was used to estimate the effect size of the intervention on wheelchair self-efficacy (Wheelchair Use Confidence Scale), wheelchair skills capacity and performance (Wheelchair Skills Test- Questionnaire), and wheelchair mobility (Life-space assessment). Analysis of variance was used to estimate the effect of WheelSee on satisfaction with participation (Wheelchair Outcome Measure). Intention-to-treat analyses were performed.
Participants were 48.8 ± 17.0 years of age, mostly unmarried (19/28) male (22/28) and had 13.1 ± 12.6 years of previous wheelchair experience. All but one participant in the intervention group completed the study. Self-efficacy enhanced peer-led wheelchair training had a large statistically significant effect on wheelchair use self-efficacy (Cohen’s d = 1.4, p = 0.002). WheelSee also had a large statistically significant effect on wheelchair skills capacity (Cohen’s d = 1.2, p = 0.005) and wheelchair skills performance (Cohen’s d = 1.0, p = 0.02). Based on participant identified goals, WheelSee had a moderate effect on satisfaction with performance (Cohen’s d = 0.7), but the between-group differences did not reach statistical significance (p = 0.1). WheelSee did not have an effect on life-space mobility (Cohen’s d = 0.1, p = 0.75).
A self-efficacy enhanced peer-led wheelchair training program offers a promising intervention strategy to accommodate the training needs of community-living manual wheelchair users. Literature suggests that wheelchair use self-efficacy and wheelchair skills may influence social participation, but more research is needed. Future research is also needed to determine how peer-led programs may augment existing clinical practice, cost-effectiveness, and to understand when optimal timing to initiate wheelchair training programs.
[1] Sakikibara 2014 Phys Ther ; [2] Best 2014 Dis Rehabil ; [3] Webel 2010 Am J Pub Health.
0235
Ryuji Tao (1) presenting
Kagawa University, Takamatsu, Japan (1)
Ryuji Tao (1) presenting
Kagawa University, Takamatsu, Japan (1)
What should above knee prosthetics be like which are useful and practical in developing countries for farm work on rough terrain or in mud?
80 to 85 percent of amputees are land mine survivors in war-torn countries of the world such as Cambodia, Iran, and Afghanistan. These mines are responsible for 26,000 amputations per year and have produced 300,000 amputees worldwide [1]. Although these numbers include both those of upper extremity amputees and those of lower extremity above knee and below knee amputees, it should not be too much overestimated if one estimates as many as 10,000 amputees are produced every year who need above knee prosthetics in developing countries where many of them cannot help but keep farming to gain their livelihood even wearing above knee prosthetics.
The aim of this study is to understand what the above knee prosthetics should be like which are useful and practical in developing countries for farm work on rough terrain or in mud and investigate how the existing or planned above knee prosthetics can be enhanced so that they can be well suitable for farm work.
First, a previous study [2] on the current situations in Thailand about the above knee prosthetics supplied to farmers for farm work was referred to. Then, it was concluded what features should be implemented in above knee prosthetics for farm work in developing countries and what additional features should be realized to the above knee prosthetics which have already been commercialized or prototyped so that they can be well suitable for farm work.
This study has resulted in a conclusion that at least the following features should be most likely indispensable for farm work and how some of the existing or planned above knee prosthetics can be enhanced like the LKJ Knee [3] so that they can be well suitable for farm work.
1) Highly cost sensitive and affordable to those who are farming in developing countries
2) Robust, water proof, and repairable in developing countries
3) Capable of stepping the stairs up and down for walking on rough terrain or in mud
4) Capable of holding half-sitting postures with knees bent for performing farm work
A field study in developing countries with some enhanced above knee prosthetics should follow to confirm the conclusion of this study that some of the existing or planned above knee prosthetics can become well suitable for farm work once some features are added.
1) Erin Strait. American Academy of Orthotists and Prosthetists. 2006, 2) Michiyo Yamakawa et al. J. of International Health. 2008, 3) Koh Inoue et al. Proceedings of the 2013 IEEE International Conference on Rehabilitation Robotics. 2013
0238
Toyoko Asami (1) presenting
Saga University Hospital, Saga, Japan (1)
The effect of combined botulinum therapy and robot rehabilitation on outpatients
In 2001 we began using myoelectric upper arm prostheses in the rehabilitation programs for upper arm amputees. In 2011 we introduced a variety of robot devices for use in outpatient rehabilitation, including the HAL robot suit, the Honda Walking Assist device, the NESS200 and the WalkAide. We also use botulinum therapy in combination with robot rehabilitation in order to achieve improvement in previously difficult to treat functional disabilities.
On October 1, 2014 our hospital launched a rehabilitation program advocating “robot rehabilitation outpatient care” in order to provide robot-based rehabilitation to as many patients as possible.
The outpatient robot rehabilitation system at our hospital includes a scheduled examination and, when deemed appropriate as a result of the initial examination, outpatient robot rehabilitation is performed by an appointed physiotherapist.
Robot rehabilitation is performed on an outpatient basis after botulinum is administered to the
patient’s lower limbs.
Walking assessments are performed using three-dimensional gait assessment (14-camera VICON camera system and 25-piece Kistler force platform with 25 plates), the 10-meter walking time, Timed Up & Go Test (TUG), and the 6-min walking distance.
The 10-meter walking time, TUG, and 6-min walking distance all showed improvement over pre-therapy results, and these improvements were maintained even after outpatient robot rehabilitation was completed.

Combined botulinum therapy and robot rehabilitation resulted in improved 10-meter walking time, TUG, and 6-min walking distance. Some patients also reported that decreased lower back pain led to increased opportunities to go out. However, as the degrees to which botulinum therapy and robot rehabilitation were individually effective are not yet known, we would also like to investigate effective uses for botulinum therapy and robot rehabilitation with larger numbers of subjects.
1) Asami T. Orthotic intervention in stroke. Brain and Circulation 19:31-36, 2014
2) Nakashima T. HAL robot suit. Clinical rehabilitation 22:792-797, 2013
3) Perry J. Gait Analysis, Slack; 2010
4)Stein RB et al, Neurorehabil Neural Repair 2006
0240
Kazuhiko Hara (1) presenting Akira Toyota (2) Masafumi Morita (3) Yosuke Suzuki (4) Yasuyo Sunaga (1) Hiroshi Takasaki (1)
Department of Physical Therapy, School of Health and Social services, Saitama Prefectural University, Kosigaya-shi, Saitama, Japan (1) Department of Tokyo Physical Therapy, Faculty of Medical Sciences, Teikyo University of Science, Adachi-ku, Tokyo, Japan (2) Graduate School of Science and Engineering Saitama University, Saitama-shi, Saitama, Japan (3) Shiraoka Orthopedics Clinic, Minamisautama-gun, Saitama, Japan (4)
Socket inner pressure and knee moment during gait in an amputee with transtibial prosthesis – a pilot study
There has been a limited understanding of individual fittingness of the prosthesis from a biomechanical perspective. The control of a prosthesis is conducted by the control of a stump through a socket. However, internal socket pressure during gait has been unclear in amputees with transtibial prosthesis. It is prudent to conduct a pilot study first before conducting a formal study.
The purpose of this single case study was to understand the socket internal pressure during gait.
The participant was a self-reliant man with a right transtibial prosthesis (42 years of age, 13 cm stump length, a total surface bearing socket with a silicone liner). The internal pressure between the socket and silicone liner was measured using F-socket (Nitta Corporation, Japan, 100Hz). The internal pressure producing socket movements in the direction of 1) flexion, 2) extension, 3) abduction and 4) adduction was the mean of the internal pressures at the 1) upper anterior and lower posterior (flexion pressure), 2) lower anterior and upper posterior (extension pressure), 3) upper medial and lower lateral (abduction pressure), 4) upper lateral and lower medial (adduction pressure), parts of the socket, respectively. Gait analysis was undertaken using a Vicon motion system (Vicon, Oxford, UK).
The peak pressure at the lower anterior part was 60kPa in the loading phase. The force controlling the prosthesis over the sagittal plane is produced by the difference between the flexion pressure and extension pressure. The difference between the flexion pressure and extension pressure seemed to be corresponding to the knee sagittal moment. The difference between the abduction pressure and adduction pressure reached to a peak of 20kPa in the terminal phase. The internal pressure at the upper lateral part was apparently lower than the other parts throughout gait (Fig1).

the socket internal pressure and knee moment during gait
The similarity between the knee sagittal moment and the difference between the flexion pressure and extension pressure indicates that internal socket pressure can control the prosthesis over the sagittal plane. It may be also considered that the difference between the abduction pressure and adduction pressure contributes to the dynamic posture control over the coronal plane. This study has become a foundation for future studies.
0243
Amir Shahzad (1) presenting Liaquat Ali Malik (2)
CHEF International, Peshawar, Pakistan (1) PIPOS,ISPO Pakistnan, Peshawar, Pakistan (2)
Current Indication in trauma for cause of amputation in Pakistan
Globally, the rate of amputation has been on rise due to accidents, gun- shot injuries, vascular diseases, infection, diabetes, terrorist attack, bomb blasts and earthquakes. It had been noticed that overwhelming majority of amputees were being brought to center for the prosthetic management since the year dot.
In order to seek out the major causes in trauma of lower and upper limb amputees who were getting rehabilitation with different respective prosthesis in the mentioned period
our study was Cross-sectional Retrospective study. The registered patient record was collected from the PRSP from the January 1st, 2010 to December 31st, 2012. PIPOS Rehabilitation Services Program (PRSP) is the leading Institute in Pakistan consisted of many centers across the country. There was inclusion of only new patient with the exclusion of old patient in the mentioned time period. The Data were analyzed using SPSS 20.0.
The study was consisted of male and female ratio of 4.9:1 respectively counting towards the 3268 amputees and the mean age was 28.5 (4≤28.5≤80). The data were to first analyze the common cause of amputation similarly 17.4% by Disease, 7.7 % by Congenital, and 75% by Trauma, thereafter the result showed the major cause was trauma because of enormous assortments. The objective was to seek out the cause nature in trauma, therefore the trauma was further assorted by nature: Road Accident 20%, Bomb blast 37.2%, Gunshot 22.6%, Electric current 6.1%, Shelling 2.7%, Work related accident 2.6%, mine Accident 1.4%, Diabetes trauma 2.8 %, Burn 1.6% and punishment/Animal bits/fall injury 3%. Amputation caused by the bomb blast was also clear result of current situation across the KPK. Study also observed that there was 50.1% below knee amputation, 22.4 % above knee amputation and 27.4% amputation of either levels of lower or upper limb.
In developed countries, the most common cause of amputation is peripheral vascular disease but in Pakistan common cause is trauma. Our study showed that current indication in trauma for amputation is bomb blast due to situation in Pakistan from last few years.
The study concluded by the samples collected from PRSP to assess the frequent cause was the trauma. In the trauma, the most frequent component was the Bomb blast and mentioned causes transform a person to an amputee of either lower or upper limb particularly the below knee amputee.
0246
Ka Lai Christina LEE (1) presenting
Prosthetic and Orthotic Department, Tuen Mun Hospital, Hong Kong, Hong Kong (1)
The effectiveness of the stoma support belts on the pain, ADL and size control of the parastomal hernia
Parastomal hernia occurs in approximately 20–50% of patients with stomas. Contributing factors to a parastomal hernia differs from study to study, with some reporting factors such as obesity, gender, age, siting of stoma, abdominal distension and chronic cough. Abdominal support belts or girdles were recommended to provide comfort and support to prevent or minimize further enlargement of the parastomal hernia.
To study the pain score and difficulties in functional activities of the Chinese patients with parastomal hernia and to evaluate the effectiveness of the stoma support belt in these parameters.
30 patients with different severities of parastomal hernia (13 females and 17 males) were recruited in the study. The mean age was 65.80 (SD 9.14). Two questionnaires, Surgical Pain Scale [1] and Activities Assessment Scale [2], were used to quantify the VAS of pain at rest, normal activities and vigorous activities and the functional status of sedentary, ambulatory and graded-intensity physical activities respectively. The patients were required to fill in the questionnaires before and one-month after stoma support belt fitting. Patients with poor compliance were excluded in this study. This project is ongoing, and there were 12 patients completed the 1-month follow up evaluation in November 2015. Paired t-test was used to compare the pain score and functional status before and after stoma support belt fitting. The confidence interval is 0.05.
Among all 30 subjects, 21 of them (70%) experienced VAS = 0 for the stoma condition and 24 of them (80%) found no difficulty for attempting sedentary activities. After the stoma support belt fitting (n=12), the mean VAS at rest and normal activities and the difficulties at sedentary and ambulatory were reduced (Table 1). There was no significant difference in these parameters.

Chinese population was found to have similar result with western countries that parastomal hernia was asymptomatic in about 80% of patients. VAS and the functional status might not be sensitive to reflect the effectiveness of the stoma support belt to control the progression of the hernia. To improve this study, the stoma size measured by nursing specialist will be included for monitoring the change of the hernia condition.
1. McCarthy (2005). J Am Coll Surg. 2005 Aug;201(2):245-52.
2. McCarthy (2005). J Am Coll Surg. 2005 Aug;201(2):171-8
0248
sadeeq Ali (1) presenting Azuan Abu Osman (1) Zia ur rehman (2) Sajjad Hussain (1) Nasrul Abdur razak (1)
University of Malaya, Kuala Lumpur, Malaysia (1) PIPOS, Peshawar, Pakistan (2)
A comparison between Pelite, Dermo and Seal-In X5 interface systems in transtibial amputees: assessing interface pressure between the stump and socket
Prosthetists always try to manufacture a good socket for amputees, who offer a firm connection to residual limb without producing any skin pain and disorders. It is a challenge for prosthetists to place a huge amount of pressure on the previously non-weight-bearing tissues of the residual limb. To avoid skin complications and to avert discomfort while using the prosthesis for daily activities, users need a comfortable liner.
Objectives of this research was to compare the interface pressure between socket and residual limb with three different interface systems.
Twenty transtibial amputees participated in this study. Three prostheses were fabricated for each participant with the three different interface systems. After one month of acclimation period participants were requested to come to motion laboratory for experiments. Four F-socket sensors were attached to the residual limb at the anterior, posterior, medial and lateral surfaces. Participants were requested to walk on 9 meter long and 5 meter wide walkway with the self selected speed. Participants completed 4 consecutive trials; at least 12 steps were recorded in each trial.
Statistical test showed significant (p<0. 05) differences between the three liners in terms of pressure magnitude. Overall the Average Peak Pressure (APP) was the lowest with the Dermo liner compared with the Pelite and seal-In X5 liner at the anterior (58.12 kPa vs. 74.22 kPa and 71.91 kPa; P= 0.00, respectively), posterior (58.04 kPa vs. 86.44 kPa and 87.33 kPa; P= 0.00, respectively) and lateral surfaces (41.51 kPa vs. 57.22 kPa and 51.42 kPa; P= 0.01, respectively). No differences were recorded among the three liners at the medial region. The same lowest pressure was observed with the Dermo liner at all the proximal and distal surfaces except medial proximal and medial distal.

Average mean peak pressure at the main regions of the residuum. The asterisks (*) indicate significant differences between the three liners.
The result of the interface pressure analyses showed less pressure within the socket wearing the Dermo liner. Hence, it can be concluded that the Dermo liner provides more comfortable socket-residual limb interface than the Seal-In X5 liner and Pelite liner. Dermo liner might be the best choice for transtibail amputees.
0249
Lollo Frimore (1) presenting Anita Stockselius (2) Marie Wikström (3) Helene Alexanderson (4)
The Swedish school of sport and health sciencies, stockholm, Sweden (1) Bräcke Diakoni, stockholm solna,
Quality of life in Swedish individuals with multiple limb deficiencies
Multiple limb deficiencies or loss of more than one extremity are congenital (idiopathic or caused by medication side effects, such as Thalidomide) or acquired due to amputation. Most of the studies in this area have investigated quality of life in individuals with amputations, but little is known about the impact of acquired multiple limb deficiencies on quality of life and this has never been studied in Sweden. EX-Center is a centre for rehabilitation and information for individuals with multiple limb deficiencies in Stockholm, Sweden.
The purpose of this study was to investigate how individuals with multiple limb deficiencies in Sweden experience their quality of life compared to population-based reference values, to study possible differences in quality of life between genders and type of limb deficiency, as well as to investigate possible correlations between different aspects of quality of life
The quality of life survey Short form 36 (SF-36) and a demographic data survey has been used in this quantitative cross sectional study. 106 individuals were invited to participate and the inclusions criteria were: individuals with multiple limb deficiencies, over the age of 15, understand the Swedish language and previously have been at EX-Center. 62 individuals (59 %) participated (33 women and 29 men, 19 and 43 individuals had acquired and congenital limb deficient, respectively). Mean age in years; women 52.0, men 51.5, congenital limb deficiencies 51.0 and acquired limb deficiencies 56.0.
Non-parametric analysis were used; One-sample Wilcoxon Signed Ranked Test, Mann Whitney U-test and Spearman’s rank correlations.
Individuals with multiple limb deficiencies had reduced quality of life compared to population-based reference values in all SF-36 domains except for the Role-emotional domain (p = 0.000-0.011. Women scored significantly lower quality of life compared to men in domain Physical Function (p=0.03). Individuals with congenital limb deficiency scored lower quality of life in domains Bodily pain compared to individuals with acquired limb deficiency (p=0.03). There were moderate correlations between Bodily pain BP and General health GH, Vitality V, Social function SF and Mental health MH (rs = 0.50-0.63).
This is the first study to investigate quality of life in individuals with multiple deficiencies in Sweden. This group had lower quality of life compared to population-based reference values and our results also indicated that women have lower quality of life than men and that individual with congenital limb deficiencies experience more pain than those with acquired. These results are to some extent in concordance with results from a similar study of individuals affected by Thalidomide in United Kingdom (1). Our results emphasize that there is a need to further study quality of life for individuals with multiple limb deficiencies and to individualize interventions to improve quality of life.
1. Bent, N., Tennant, A., Neumann, V. & Chamberlaine, M.A. (2007). Living with Thalidomide. Health status and quality of life at 40 years. Prosthetics and Orthotics International 31, ss.147-156.
0250
Mona Hichert (1) presenting Peter J. Kyberd (2) David A. Abbink (1) Dick H. Plettenburg (1)
Delft University of Technology, Delft, The Netherlands (1) University of New Brunswick, Fredericton, Canada (2)
High cable operation forces deteriorate pinch force control in voluntary closing body-powered upper-limb prostheses
Operation of upper-limb prostheses requires sufficient feedback to obtain adequate control of digit positioning and pinch forces [1]. Body powered upper-limb prostheses can offer intuitive mechanical feedback about grasping. However, how design choices impact prosthesis operation is largely unknown. An important design factor is the relationship between the operating force at the shoulder and the overall gripping control accuracy.
A recent study has shown that during body-powered prosthesis operation the control accuracy decreases with increasing force [2]. Additionally, psychophysic literature states that feedback force fidelity decreases at higher amplitudes [3]. This suggests that the higher the operating forces at the shoulder, the less accurate the control of the forces at the prehensor. However, this has never been quantified for body-powered prosthesis operation.
The aim of this study is to quantify the influence of high cable forces on the accuracy of pinch force control.
Healthy control subjects (n=12; all male) were fitted with a bypass-prosthesis. The prehensor, a modified TRS hook, had a low and a high cable force setting. Subjects were requested to transfer a ‘mechanical egg’ [4] from and to a predefined position as fast as they could without dropping or breaking it. The ‘mechanical egg’ had two fragility settings: a wide and a narrow allowable grasping force range to grasp the egg without breaking or dropping it. Each of the four conditions (combinations of low and high cable forces and wide and narrow allowable grasping force range), were tested 25 times, resulting in a total of 100 trials per subject. The order of conditions was counterbalanced across subjects to minimize learning and fatigue effects. As outcome measures the amount of failures (breaking or dropping the object), as well as the required execution times, were recorded, and statistically analysed with a repeated measures ANOVA (CI=95%).
Subjects conducted significantly more successful trials and completed the task significantly quicker with the low cable force setting. The wide allowable grasping force range resulted in more successful trials in less time compared to the narrow grasping force range.
The results of this study show that lower operation forces for body-powered upper-limb prostheses enhance the control accuracy and task completion time. Other advantages of low operation forces are that they enable more users to operate a body-powered prosthesis and that they reduce fatigue effects during or after prosthetic operation [5].
In conclusion, low cable operation forces should be maintained as a design requirement for body-powered prostheses to enhance control accuracy, minimize activity completion time, reduce fatigue and pain during or after use and enable more users to operate a body-powered prosthesis.
[1] Wiener N., 1948, John Wiley & Sons, Inc., New York, USA
[2] Plettenburg D.H., 2011, Proceedings of the 2011 Myo Electric Controls/Powered Prosthetics Symposium Fredericton, New Brunswick, Canada: August 14-19
[3] Gescheider G.A., 1976, John Wiley & Sons, Inc., New York, USA
[4] Meek S.G., 1989, Journal of Rehabilitation Research and Development, vol.26, no.3, p.53-62
[5] Hichert M., 2014, Proceedings of the 2014 Myo Electric Controls/Powered Prosthetics Symposium Fredericton, New Brunswick, Canada: August 19-22
0251
Pierre Chabloz (1) presenting Bruno Saurel (2) Bastien Moineau (2,3) Vanessa Seetha (2) Marie-Pierre De Angelis (2) Cécile Meynard (1) Vincent Nougier (3) Dominic Pérennou (2)
Chabloz Orthopédie, Grenoble, France (1) Grenoble University Hospital, Grenoble, France (2) TIMC-IMAG Laboratory, Grenoble, France (3)
Ischial-integrated socket for above-knee amputees: evaluation of pressures exerted on the stump and prospects
Above-knee amputees in our rehabilitation units are fitted with ischial-integrated socket. Conception is based on a plaster casting of the stump with an orientation of lateral soft tissues, followed by an homogeneous reduction of the positive mold (about 2%). The ischial tuberosity is placed on a slop looking above, outside and forward, so that the lateral face of the femur is pushed against the lateral wall of the socket.
Evaluate objectively the effectiveness and the relevance of our method and discuss the results to propose future enhancement for above-knee amputee fitting.
Pressures exerted on the stump during gait were assessed with 14 force sensing resistors. Pressures were described regarding their peak values (spatial repartition) and their cross-correlation with respect to each over (time repartition). Forty above-knee amputee patients were recruited. Quality of the prosthesis was assessed through gait capabilities, clinical scales of satisfactions and clinical exams of pains and wounds.
The group had a mean satisfaction of 78 ±12% (SatPro scale) and performed 165 ±39 m at the 2 minutes walk test. However, 13 patients had pains of intensity above 4/10 (visual analogic scale) and 14 had cutaneous lesions.
Pressures were exerted simultaneously on the whole socket during gait, except if the stump had his volume reduced since last fitting. In these cases, and in case of stump wounds, the pressures were null or with poor synchronization on certain zones, while pressures were too high on over zones. In the more satisfying prosthesis, the higher pressures were on the areas with soft tissues at mid-height and at the upper part of the stump, and particularly on the adductor area. At the same time, pressures were moderate on the ischial area and low at stump extremity in these satisfying prostheses.

On a biomechanical perspectives, our results illustrate the hydrostatic repartition of pressures due to stump tightening (synchronization of loading), and the force moments due to the lever arm between body weight and prosthetic reaction (dominant area of pressures). Facilitating pressure repartition and targeting biomechanically efficient and pressure tolerant area could be a way to enhance prosthetic comfort and patient satisfaction. To date, we experiment in 5 patients a new prosthetic socket design that aim to reproduce current socket performance (high satisfaction and walking abilities) with better sitting comfort.
0252
Hans-Rudolf Weiss, Dr. med. (1) presenting
Spinal Deformities Rehabilitation Services, Gensingen, Germany (1)
CAD / CAM Bracing Scoliosis - Classification based approach vs. Finite element modelling
A RCT published recently has demonstrated that 72% of a population complying to the SRS inclusion criteria on bracing did not progress using the TLSO braces used in the USA and in Canada with moderate corrective effect. It has been shown that in-brace correction and compliance correlate with outcome. The more standardized CAD braces available today should enable to improve in-brace correction and outcome.
Purpose of this paper is to compare the recent CAD brace developments with respect to the in-brace corrections.
In-brace corrections achieved in a sample of patients fulfilling the SRS inclusion criteria for studies on bracing using the classification based approach (CBA) are compared to the recent individual CAD / CAM bracing approach based on finite element modelling (FEMA).
In-brace corrections differed widely when comparing the different approaches. In-brace corrections in the CBA was 66% of the initial value and in-brace correction in the FEMA was 42% of the initial value without the brace on.
Considering the fact that in-brace correction (and compliance) determine the end result of bracing in the treatment of scoliosis we must acknowledge that currently the CBA of bracing scoliosis is superior to the FEMA and the standard plaster based brace applications.
1. Chaves A (2014) A Perfect Fit: 3D Systems Unveils Bespoke 3D Printed Braces for Chronic Scoliosis. 3D PRINTING, 3DP APPLICATIONS, DESIGN, INDUSTRY NEWS, JUNE 12, 2014 (http://3dprintingindustry.com/2014/06/12/perfect-fit-3d-systems-unveils-bespoke-3d-printed-braces-chronic-scoliosis/).
2. Clin J, Aubin CE, Labelle H. (2007) Virtual prototyping of a brace design for the correction of scoliotic deformities. Med Biol Eng Comput. May;45(5):467-73. Epub 2007 Mar 17.
3. Clin J, Aubin CE, Parent S, Sangole A, Labelle H. (2010) Comparison of the biomechanical 3D efficiency of different brace designs for the treatment of scoliosis using a finite element model. Eur Spine J. Jul;19(7):1169-78. doi: 10.1007/s00586-009-1268-2. Epub 2010 Jan 22.
4. Clin J, Aubin CÉ, Sangole A, Labelle H, Parent S. (2010) Correlation between immediate in-brace correction and biomechanical effectiveness of brace treatment in adolescent idiopathic scoliosis. Spine (Phila Pa 1976). Aug 15;35(18):1706-13. doi: 10.1097/BRS.0b013e3181cb46f6.
5. Clin J, Aubin CÉ, Parent S, Labelle H. (2011) Biomechanical modeling of brace treatment of scoliosis: effects of gravitational loads. Med Biol Eng Comput. Jul;49(7):743-53. doi: 10.1007/s11517-011-0737-z. Epub 2011 Feb 2.
6. Clin J, Cobetto N, Desbiens-Blais F, Le May S, Labelle H, Parent S, Aubin CE. (2014) Advanced brace design combining CAD/CAM and biomechanical simulation for the treatment of adolescent idiopathic scoliosis. Paper presented at the OTWorld, Leipzig, Germany, May 13th.
7. De Giorgi S, Piazzolla A, Tafuri S, Borracci C, Martucci A, De Giorgi G. (2013) Chêneau brace for adolescent idiopathic scoliosis: long-term results. Can it prevent surgery? Eur Spine J 2013 Nov;22(Suppl 6):S815-22.
8. Weiss HR, Moramarco M. (2013) Scoliosis - treatment indications according to current evidence. OA Musculoskeletal Medicine. Mar 01;1(1):1.
9. Weiss HR, Seibel S, Moramarco M, Kleban A. (2013) Bracing scoliosis: The evolution to CAD/CAM for improved in-brace corrections. Hard Tissue. Nov 25;2(5):43.
10. Weiss HR, Seibel S, Kleban A. (2014) Deformity-related stress in a sample of patients with adolescent idiopathic scoliosis after brace weaning: a cross-sectional investigation. OA Musculoskeletal Medicine. Mar 12;2(1):5.
11. Weiss HR. (2014) Standardising the treatment with Chêneau braces via CAD: Prospects and risks. OA Musculoskeletal Medicine. May 03;2(1):10.
12. Weiss HR, Seibel S, Moramarco M, Kleban A. (2014) Scoliosis bracing – from cast to CAD / CAM. Paper presented at the OTWorld, Leipzig, Germany, May 13th.
0253
Nikolai Santos (1) presenting Anna Margarita Lugue (1) Catherine McConnell (2) Weerawat Limroongreungrat (4) Sunnee Bovoonsunthonchai (3) Pitchaya Rayothee (1) Kazuhiko Sasaki (1)
Sirindhorn School of Prosthetics and Orthotics, Faculty of Medicine-Siriraj Hospital, Bangkok, Thailand (1) West Park Healthcare Centre, Toronto, Canada (2) Faculty of Physical Therapy, Mahidol University, Nakhon Pathom, Thailand (3) College of Sports Science and Technology, Mahidol University, Nakhon Pathom, Thailand (4)
Effects of socket alignment combinations on minimizing gait deviations of long-term unilateral trans-femoral prosthetic users
Excessive trunk sways and pelvic tilts are common gait compensations seen in trans-femoral (TF) amputees. While alignment paradigms suggest that systematic adjustments to socket tilts and shifts can potentially improve TF gait patterns, the quantification of these effects have received little attention in literature. The non-inclusion of the trunk and pelvis in observations and non-use of shift and tilt combinations in alignment protocols limit the clinical usability of previous studies.
This study aimed to quantify the effects of changes in alignment on TF gait patterns in terms of joint angles and mediolateral (ML) and anteroposterior (AP) ground reaction forces (GRF) during level-surface ambulation.
A Vicon® motion analysis system with AMTI® force plates was utilized to measure spinal, pelvic, hip and knee angles and AP and ML GRF from five unilateral TF amputees in six socket alignment variations tested in random order: FA (6° flexed, shifted anteriorly), EP (6° extended, shifted posteriorly), ABL (6° abducted, shifted laterally), ADM (6° adducted, shifted medially), neutral (socket middle reference lines are perpendicular to the top of the prosthetic foot, both in sagittal and frontal planes) and optimized (socket configuration after dynamic alignment by an experienced certified prothetist). Peak GRF values and joint angles were averaged from five subjects in each alignment condition and statistical differences across all conditions were analyzed using the Friedman test with post-hoc analysis.
Neutral alignment values most closely resembled optimized. No statistically significant changes were detected for most hip and knee values across all alignment combinations. FA produced the least amount of spinal hyperextension (p=0.02) and anterior pelvic tilt (p=0.001) compared with EP. ABL and ADM exhibited significantly contrasting effects on lateral spinal deviation (p=0.009), lateral GRF (p=0.004) and medial GRF (p=0.009). ABL promoted the highest lateral spinal deviation and lateral GRF distortion in early stance while ADL reflected the highest increase in medial spinal deviation and medially directed GRF distortion in late stance.
Systematic changes to linear and angular socket alignment can aid in reducing TF gait deviations. Socket flexion and adduction reduced spinal hyperextension, anterior pelvic tilt and lateral spinal deviation of the participants. The subjects mostly used their trunk in adapting to alignment changes. Close observations of the trunk may be helpful in monitoring mal-adaptations resulting from GRF distortions during clinical alignment procedures. Future studies monitoring long-term effects of alignment on a bigger number of participants including new prosthetic users are recommended to better understand how alignment can be used to maximize patient outcomes.
0254
Anna Margarita Lugue (1) presenting Nikolai Santos (1) Catherine McConnell (2) Weerawat Limroongreungrat (4) Sunnee Bovoonsunthonchai (3) Kazuhiko Sasaki (1) Pitchaya Rayothee (1)
Sirindhorn School of Prosthetics and Orthotics, Faculty of Medicine-Siriraj Hospital, Bangkok, Thailand (1) West Park Healthcare Centre, Toronto, Canada (2) Faculty of Physical Therapy, Mahidol University, Nakhon Pathom, Thailand (3) College of Sports Science and Technology, Mahidol University, Nakhon Pathom, Thailand (4)
Effects of socket alignment combinations on the muscle activity and comfort of unilateral trans-femoral amputees during level surface ambulation
Prosthetists use systematic adjustments to linear and angular alignments of trans-femoral (TF) prostheses to optimize pressure distribution on the residual limb and enhance the leverage of muscles that act to stabilize the pelvis during ambulation. Research that investigates the effects of combining linear and angular changes is limited in the current body of literature. Investigations that help to quantify the effect of changes in alignment may help to improve outcomes for prosthetics users.
This study aimed to quantify the effect of changes in alignment on comfort and muscle activity in unilateral TF amputees during level surface ambulation.
Investigators studied five unilateral TF participants during level surface walking at self-selected speed. Six variations of socket alignment were used to compare the effect on muscle activity and reported comfort between alignment variations; FA (6o flexed, shifted anteriorly), EP (6o extended, shifted posteriorly), ABL (6o abducted, shifted laterally), ADM (6o adducted, shifted medially), neutral (socket middle reference lines are perpendicular to the top of the prosthetic foot, both in sagittal and frontal planes) and optimized (resultant socket position after completion of dynamic alignment by an experienced certified prosthetist). Muscle activity was measured through surface electromyographic (SEMG) activity of gluteus maximus (GMAX), gluteus medius (GMED) and erector spinae (ESPIN). Mean SEMG amplitudes were extracted from each subphase of stance per test condition. Results from each socket alignment condition were compared against optimized alignment using the Wilcoxon signed rank test. The Borg psychophysical scale was used to quantify comfort in each trial and mean comfort ratings were tested using the Friedman test with post-hoc analysis.
Compared with optimized, EP produced statistically significant increase (p=0.043) in ESPIN activity during early midstance while ABL promoted marginally significant increase (p=0.08) in the activity of the same muscle in late midstance. FA did not promote statistically detectable changes to mean SEMG activity of any of the muscles tested. Comfort ratings suggest FA was the most uncomfortable (p=0.002) condition among all alignment combinations. Neutral alignment reflected values that most closely approximated optimized alignment, both in mean SEMG amplitudes and comfort ratings.
The results suggest that systematic combinations of linear and angular socket alignment promote significant changes in the muscular activity and comfort of TF amputees. Subjects mostly used their spinal muscles in adapting to changes in socket alignment. It is thereby suggested that prosthetists pay close attention to the trunk region when monitoring mal-adaptations during alignment procedures. The results of this study are limited to short term effects of alignment perturbations on long-term prosthetic users. Future studies on new prosthetic users may be beneficial in better understanding how alignment can be maximized to prevent development of gait asymmetries which are commonly associated with secondary musculoskeletal disorders.
0256
Ching Yee Tse (1) presenting Chi Ping Chow (1) Hon Bong Leung (1) Wai Hing Wong (1)
Chinese University of Hong Kong, Hong Kong, Hong Kong (1) Hospital Authority, Hong Kong West Cluster, Hong Kong (2)
A prospective cohort study on the subjective outcome of wrist splintage in patients with different severities of carpal tunnel syndrome based on electrodiagnostic studies
Carpal tunnel syndrome(CTS) is the most common nerve entrapment disease while splintage is the commonest conservative treatment for CTS. However, the relationship between the severity of CTS and the outcome of splintage was not well investigated. Understanding the relationship could help the clinicians to predict the splinting outcome in each patient and determine the most suitable treatment.
This study aimed to compare the splintage outcome in different electrophysiological severities of carpal tunnel syndrome (CTS), using a self-administrated questionnaire.
36 subjects with clinical diagnosis of CTS were classified into three severity groups CTS by Nerve Conduction Studies (NCS). They completed the Boston questionnaire covering ratings of the hand symptoms and functions prior to splinting treatment. After 2 months of splinting intervention, they filled the questionnaire again for outcome evaluation. The outcome differences among the three severity groups were compared. Significant confounding factors were also investigated in secondary analysis.
36 subjects (11 mild, 18 moderate, 7 severe) completed the study and included in data analysis. Only the moderate CTS group showed a significant change in hand symptom score(Wilcoxon; p = 0.018) after splintage. No significant change of hand function score was found in all three severity groups. The employment status (Chisquare; p=0.041) and dominant hand involvement (Chisquare; p=0.003 & p=0.005) were significantly associated with hand symptom improvement
This study demonstrated that splinting intervention could offer a significant improvement in hand symptoms for moderate CTS as diagnosed electrophysiologically, but might not result in significant improvement in mild or severe CTS. Unemployed status and dominant hand involvement might also predict insignificant improvement in hand symptom. This study suggested that classification of CTS severity by electrodiagnostic studies can be useful to predict the hand symptom improvement after short term splintage, hence facilitating the treatment decision.
0257
Tawatchai Junsaard (1) Visanurak Dowloy (1) Jutharat Poomulna (1) presenting
Sirindhron National Medical Rehabilitation Centre, Bangkok, Thailand (1)
Analysis of Pressure and Shear in a PTB Sockets: A Pilot Study
A pain at the residual limb is one of the problems that can be caused by the improper socket. This system is developed to analyze the pressure and shear force in a patella-tendon-bearing (PTB) socket which has been designed to bear the weight on four specific areas and to avoid five pressure areas. The system consists of low cost and readily available sensors, integrated or connected to a data collection tool and a display programme that shows the relation of pressure and shear force with the percentage of time in stance phase of gait cycle.
The system aims to measure and analyze the pressure and shear force which have been created in the PTB socket; and the system can be used as a measuring tool in a clinical setting.
Two healthy unilateral transtibial amputee subjects who had been wearing a below-knee prosthesis (PTB socket type) were installed with the newly designed system. Eight force-sensing resistors (FSRs) were used for measuring the pressure in the specific areas; the strain gage and polydimethysiloxane (PDMS) were used to determine shear force; and inertial measurement units (IMUs) were attached to the ankle of the prosthesis to identify the phase of gait while walking. Data from five trials of walking at a self-selected speed were collected. The display of the analyzed data was shown on the computer monitor to compare the maximum pressure and shear force in stance phase of gait cycle.
Two subjects showed the different results of pressure that were created on the patient stump by the socket. Subject A presented the maximum pressure value on the lateral tibial crest and small pressure on three parts – the cut of bone, the patella tendon and the posterior popliteal shaft. Subject B showed the maximum pressure value on the cut end of bone where the pressure had to be avoided, while there was a small pressure on the medial tibial shaft and hamstring tendon. The peak of the pressure presented during the stance phase period, i.e. loading response. The differences in the pressures which occurred in the two patients could result in prosthesis misalignment and improper fit of the socket. The two values of shear force derived from the two sensors were the maximum shear force occurring while walking (loading response period) and the minimum shear force shown while standing.
The developed system showed pressure and shear force which were created in prosthesis sockets and presented on the monitor. The prosthetist and orthotist who attends to the patient could see and adjust their sockets by using these data. However, the system requires a specialist to set accurate sensor points and analyze the data. In the future, we are interested in conducting this kind of study on new prosthetic device users who have never had any experience with the pain from the socket.
Polliack AA, Sieh RC, Criaig DD, Landsberger S, McNeil DR, Ayyappa E; 2000, Scientific validation of two commercial pressure sensor systems for prosthetic socket fit.
Buis AWP, Covery P; 1997, Calibration problems encountered while monitoringstump/socket interface pressures with force sensing resistors: techniques adopted tominimise inaccuracies.
Shem KL, Breahey JW, Werner PC; 1998, Pressures at the residual limb – socket interface in transitibial amputees with thigh lacer-side.
Kishore Sundara-Rajan, Student Member, IEEE, Gabriel I; 2010, Shear sensor for lower limb prosthesis.
Jacquelin Perry, MD; 1989, Gait Analysis Normal and Pathologocal Function.
258
Makoto Ninomiya (1) presenting
Nagasaki KANAE Co.,Ltd., Nagasaki-City, Japan (1)
The Development Of A Carbon Hydraulic Unilateral Brace Knee-Ankle-Foot Orthosis For Use In Early Gait Training After Stroke
Gait training after the onset of stroke must begin at an early stage. The knee-ankle-foot orthosis used for that training must prevent the knee from buckling, and it should have a unilateral brace structure of adjustable length, to make it light and easy to put on. These knee-ankle-foot orthoses must be on hand as standard hospital equipment, to be available for use at any time.
Use thermoplastic carbon sheet to fabricate a light and robust knee-ankle-foot orthosis with a unilateral brace structure. Control the knee joint on one side of the structure to prevent the knee from buckling.
Use a newly-developed hydraulic rotary damper for the knee joint, to fix the knee in the stance phase and leave it free to move in the swing phase. Operate a hydraulic valve by electronic control, to lock the knee in the stance phase. The knee moves freely in the swing phase, so the assistance of a physiotherapist enables a stroke patient to practice from an early stage, walking with close to normal gait.
The developed thermoplastic carbon sheet consists of continuous carbon fibers impregnated with polycarbonate. It softens at 280° and can be remolded any number of times. Strength testing confirmed strength equal to that of high-strength duralumin, at lower weight. The newly-developed rotary damper was able to lock the knee at any desired angle by closing the hydraulic valve. The knee is free to move in the extension direction. The damper is also the shaft of the knee joint, so it was possible to fabricate it with light weight and no major increase in size. We were able to confirm that the assistance of a physiotherapist enables stroke patients to walk with close to normal gait in early gait training.
Early practice in normal walking is necessary to prevent stroke patients from walking abnormally. To that end, this knee-ankle-foot orthosis is effective as hospital equipment to serve a wide range of patients, such as those unable to fully extend the knee.

0259
Christine Joy Dee (1) presenting Rachelle Ann Ligan (1) Joaquin Louis Sangalang (1) Nikko Antonio Taotjo (1)
Philippine School of Prosthetics and Orthotics, College of Allied Rehabilitation Sciences, UERMMMCI-EXCEED, Quezon City, The Philippines (1)
Pilot Study on the Socioeconomic Status: Pre and Post Lower Limb Amputation Among Philippine School of Prosthetics and Orthotics Patients
The Magna Carta for Disabled Persons (Republic Act 7277) aims for the integration of individuals with disability into mainstream society. However, in the Philippines, the International Disability Rights Monitor: Regional Report of Asia 2005 study showed 57.12% of PWDs were employed compared to 82.3% of the general population, showing the need to translate disability related laws into tangible programs. The extent, therefore, of socioeconomic changes brought about by major limb amputation is of significant interest.
The aim of this study was to assess the difference between self-reported socioeconomic status of individuals with major lower limb acquired amputations pre and post disabling event.
A convenience sample of 14 unilateral transtibial or transfemoral amputees without previous history of disabilities or concomitant upper extremity amputation and with no known cognitive dysfunction was identified with the following criteria: 1.) Amputation was done within 1-10 years prior to the survey, 2.) of working age (25-60 years old) at the time of the study, and 3.) from the patient pool of the Philippine School of Prosthetics and Orthotics clinic collected from January 2013–February 2014. The assessment tool is a structured interviewer-administered self-reported questionnaire designed to gather data related to socio-economic status pre and post-amputation. Chi-square test was utilized to determine the difference between the 2 status.
Average number of earners at respondents’ households increased significantly from an average of 1.8± 0.7 pre-amputation to 2± 1.04 post-amputation (p value = 0.014). Average household monthly income decreased from PhP27,564± 32,127.81 before disabling event to PhP17,528.57± 25,423.867 after (p value = 0.010). Among 14 participants, twelve (86%) indicated having additional expenditures related to their disabling event, and two (14%) indicated that they don’t. Eight (57%) respondents reported having insufficient financial resources to meet their needs pre-amputation. Post-amputation, this increased to twelve (86%) participants. Table 1 shows mean household income and mean personal income pre and post-amputation, expense to date and monthly expenses related to disabling event.
Income and expenditure

0260
Kazuhiro Tanaka (1) presenting Takahiko Fukumoto (1) Yohei Okada (1)
Graduate School of Health Sciences, Kio University, Nara, Japan (1)
The effects of insoles on the lateral thrust and lower limb muscle activation of osteoarthritic knees: Comparisons between shoes of matching size and shoes not matched for size
Insoles have been widely used for the relief of symptoms associated with osteoarthritis of the knee (knee OA). The most popular types of insoles are shoe insoles. Because shoes contact the ground, it is necessary to consider the effects of the shoes when prescribing insoles. However, the effects of shoes have not been sufficiently studied, and the effects of insoles on lateral thrust and electromyographic analysis have been seldom reported.
The purpose of this study was to determine insole and shoe effects on the hip muscles and lateral thrust during gait.
Six female patients with a diagnosis of knee OA walked under 7 different insole conditions: barefoot, with a lateral wedge, with a medial wedge, forefoot, hindfoot, with shoes of matching size, and with non-size-matched shoes. Measurements were ankle range of motion, the leg/heel angle, maximum lateral thrust, root-mean-square (RMS) for lateral thrust, and integral EMG value (iEMG) for hip muscles in the stance phase of gait. Paired t-tests were used to compare the maximum value and RMS of lateral thrust and iEMG between the conditions at each time point. This study was approved by the Ethical Review Board of Kio University (H25-45).
Leg/heel angle was within the normal range (9.3 ± 1.6°). Ankle range of motion showed no significant restriction (dorsiflexion, 13.3 ± 7.5°; plantar flexion, 45.8 ± 3.8°). RMS for lateral thrust during gait was significantly reduced in shoes of matching size compared to barefoot. Muscle activity of the hip muscles and the maximum and RMS of lateral thrust were not significantly different among the various insoles and shoes as compared to barefoot.
The RMS results suggest that size-matched shoes reduce a fixed calcaneus’s lateral thrust while allowing sufficient foot flexibility and range of motion. Sufficient flexibility and range of motion were retained for the ankle and reduced for the hip. Our findings suggest that there was no significant difference in the maximum and RMS values for lateral thrust and hip muscle activity. Therefore, the effects of insoles and shoes may be affected by ankle joint functions in addition to knee joint functions.
0261
Ana María Posada (1,2) presenting Luz Helena Lugo (1,2) Jesús Alberto Plata (1,2) Alonso Castaño (1,2) Juan Manuel López (1,2)
Universidad de Antioquia, Medellín, Colombia (1) Grupo de Rehabilitación en Salud, Medellín, Colombia (2)
Patients’ perspectives on lower limb amputation outcomes
Clinical Practice Guidelines (CPG) are recommendations based on scientific evidence to give information for decision making on health care. In the development of a CPG for the rehabilitation and prosthesis’ prescription for major lower limb amputees, it is important to identify patient’s priorities on the outcomes related to prosthetic fitting. These priorities are crucial to develop the guidelines, especially when there is scarce evidence to make the recommendations.
The purpose of the study is to identify patient’s priorities and perspectives on the outcomes related to prosthetic fitting.
A cross-sectional study was conducted on 28 subjects with transtibial or transfemoral amputation, secondary to trauma or vascular disease, between ages 18 and 65 years, that had had a prescription for a prosthesis or a prosthetic component between 2012 and 2014. Patients evaluated the relevance of different outcomes using the GRADE scale (1 to 3 as non-important; 4 to 6 major-non critical and 7 to 9 critical). Possible outcomes were selected from prosthesis adaptation evaluation tools (The Trinity Amputation & Prosthesis Experience Scales Revised and the Prosthesis Evaluation Questionnaire) and the priorities of the guideline development group. Categorical variables were reported as percentages and continuous variables as averages or medians. A subgroup analysis of Chi² tests was performed.
This study showed that the most critical complication reported by the patients is stump infection (8 on the GRADE scale). The most important activity is to walk (8 on the GRADE scale). And the main variable that may affect prosthesis adaptation is a lesion of the skin of the stump (9 on the GRADE scale). Other critical outcomes reported were quality of life, independence for basic and complex activities, and the ease to use the prosthesis and wear shoes. There were no statistically significant differences on the subgroup analysis. Median satisfaction with the prosthesis was 61 mm (On a 1-100 scale).
The identification of the priorities and perspectives of patients on prosthesis adaptation and rehabilitation allows us to make recommendations to improve prosthetic fitting and quality of life related to health in the people with amputation.
0262
Amir Shazad (1) Ayaz Muhammad (1) presenting Sundas Khalid (1)
CHEF International, Islamabad, Pakistan (1)
Quality of Life of People with Disabilities Using Prosthesis and Orthosis in Capital of Pakistan
According to World Bank, 3.08 % - 16.21% of population is living with disability in developing countries around the globe. In Pakistan, disability ratio is 5.99% (1). Disability affects physical health, social relationship of people and family, friends, psychological state, and level of independence (2). WHO has developed community-based rehabilitation program to improve the quality of life (QOL) of people with disabilities (PWD’s) by delivering the prosthetic and Orthotics devices.
The aim of our study was to evaluate quality of life applying different variable i-e demographic, activity level, QOL, social relationships and psychological state of the person who received a Prosthesis and Orthosis (P&O).
The Study design was a Questionnaire survey (descriptive) and conducted across the Islamabad (capital) which is advanced city of Pakistan from June 1, 2014 to November 30, 2014. The method for collection of information was one-on-one interviews of subject belonging to Islamabad; some of them were interviewed twice who didn’t have devices already. Research tools were questionnaire and consent form. The data was analyzed using SPSS 20.
Sample size was 80 consisting of female (38.8%) and male (61.3%). Mean age of respondents was 26.75±15.2. Only 12% PWD’s didn’t have P&O. All the participant were educated having minimum education were primary and maximum qualification was Ph.D. According to disability CP was 25% using AFO, polio was 23.8% using KAFO and TTA was 13.8% using TTP. Occupation wise, 45.0% were student and 30% were job holder, rest were doing business/house wife. Mean time of appliance use was 10 hours. Significant results were analyzed by applying Chi-square test for:
Availability of facilities regarding Prosthetic and Orthotic devices does help in improving the LOQ, as similar to our study in Islamabad which is advanced city with respect to facilities in Pakistan. Higher education levels also improve their status and enable full participation in society.
References:
1. Sophie Mitra, Aleksandra Posarac, and Brandon Vick, Disability and Poverty in Developing Countries: A Snapshot from the World Health Survey, SP Discussion Paper NO. 1109, 2011;April: p 34.
2. Hosain GMM et al. Impact of Disability on Quality of Life of Rural Disabled People in Bangladesh. J Health Popul Nutr 2002 Dec;20(4):297-305
0263
Sietske Romkema (1) presenting Raoul Bongers (2) Corry van der Sluis (1)
University of Groningen, Unitversity Medical Centre Groningen, Department of Rehabilitation, Groningen, The Netherlands (1) University of Groningen, University Medical Center Groningen, Center of Human Movement Sciences, Groningen, The Netherlands (2)
Intermanual Transfer Effects in Upper-Limb Prosthesis Training: the Influence of Inter-Training Intervals
Myo-electric prosthetic training should start within the first month after amputation for the best results. To start training directly after an upper-limb amputation intermanual transfer can be used.1,2 Intermanual transfer implies that motor skills learned at one side of the body, transfer to the other side. This suggests that by practising the unaffected arm, in the period between amputation and prosthetic fitting, the affected arm will also improve. Practising the unaffected arm is possible using a prosthetic simulator, a myo-electric prosthesis that can be attached to a sound arm.
The aim of this study was to determine the influence of inter-training intervals on the magnitude of the intermanual transfer effects.
A mechanistic, randomized, single blinded pretest-posttest design was used. Sixty-four able-bodied, right-handed participants were randomly assigned to two training groups and two control groups. The training groups performed a training program with a prosthesis simulator. The control groups performed a sham training. One of the training groups and one of the control groups trained on five consecutive days, while the other two groups trained twice a week. To determine the improvement in skills, a test was administered before, immediately after, and at two moments after the training. Training was performed with the ‘unaffected’ arm; tests were performed with the ‘affected’ arm. The outcome measures were the movement time (the time from the beginning of the movement until completion of the task), the duration of hand opening, (the opening of the prosthetic hand during grasping an object), and the force control (the error from the required force during a tracking task).
Intermanual transfer was found in movement times, (F3,180=2.847, P=.039), but not in hand opening or force control. The length of the inter-training interval did not affect the magnitude of intermanual transfer effects.
Intermanual transfer effects were present in the movement times after prosthesis training. Different inter-training intervals did not influence these effects. Persons with an upper-limb amputation are advised to use intermanual transfer techniques during the period they are waiting for their prosthesis to be manufactured. Patients can then use a daily training program or a training program with larger inter-training intervals.
1. ROMKEMA, S., BONGERS, R.M. and VAN DER SLUIS, C.K., 2013. Intermanual transfer in training with an upper-limb myoelectric prosthesis simulator: a mechanistic, randomized, pretest-posttest study. Physical Therapy, 93(1), pp. 22-31.
2. ROMKEMA, S., BONGERS, R.M. and VAN DER SLUIS, C.K., In pres. Intermanual transfer effects in young children after training a complex skill: A Mechanistic, Pseudo-Randomized, Pretest-Posttest Study. Physical Therapy
0264
Amélie TOUILLET (1) presenting Laetitia PEULTIER (4) Isabelle LOIRET (1) Noël Martinet (1) Caroline NICOL (2) Nathanaël JARRASSE (3) Jean PAYSANT (1) Jozina DE GRAAF (2)
IRR, Nancy, France (1) ISM, Marseille, France (2) ISIR, Paris, France (3) DevAH, Nancy, France (4)
Voluntary phantom movements in an upper arm amputee population: description and evolution
After limb amputation, patients often experience vivid perceptions of the missing limb. Phantom limbs have mostly been studied with regard to their sensations, whether painful or painless. However, patients can describe many other phantom phenomena, in particular the ability to voluntary move their phantom limb [1].
To evaluate the frequency of mobile phantom limbs in an upper limb amputee population, to describe these movements and to follow their evolution over time.
Since June 2013, all patients seen after an upper arm amputation in our rehabilitation center (first contact or follow up) were interviewed about their phantom limb after giving their consent. They were encouraged to describe all phantom sensations and in particular the capacity to make voluntary phantom movements. For patients who reported having phantom movements, we asked them to describe them or to mimic the different movements with the intact limb if possible.
For patients interviewed early post amputation (within 6 months), a second interview has been carried out several months later to follow the evolution of the phenomenon.
Thirty two amputees were met. Thirty patients (aged 49±15.5 years (mean±sd), 9 women, 21 above and 9 below the elbow) were interviewed. The median time delay since amputation is 5.4 ; 0.4 – 13.8 years (median, 1st - 3rd interquartile).
77% of them described the ability to voluntarily move their phantom limb. The movements seem to appear early after amputation. Some patients still have a mobile phantom limb more than 30 years after amputation. Eight different types of movements were described: they mostly concern the hand; elbow movements are scarce. Phantom movements seem to be more frequent after above elbow amputation.
Nine patients were interviewed less than 6 months after amputation. Among them, 6 described movements. During the second interview, 2 patients (who did not have a mobile phantom before) described the appearance of movements. Many described different movements from the previous interview.
Phantom limb mobility is frequent after amputation and seems to be persistent. Identifying the concerned patients and the characteristics and evolution of their movements can allow better understanding the involved neurophysiological mechanisms: cortical plasticity and/or neuromuscular peripheral reorganization? Electrophysiological evaluations are necessary to clarify this issue.
1 Kooijman CM; 2000; Pain
0265
Lori Pipinich (1) presenting
Ossur Americas, Foothill Ranch, CA, USA (1)
Transfemoral Vacuum: An Innovation in Advancing Amputee Clinical Care
Until recently transfemoral vacuum has not been widely utilized due to perceived conceptions around proper techniques and limitations in products available. The purpose of this presentation is to provide clinicians with a number of case studies demonstrating the techniques and outcomes utilizing innovative transfemoral technologies. The technology and clinical tools are centered on the utilization of XTF and Evolution liners that provide the greatest level of flexibility and options for a broad patient population. Clinicians will leave this session with a greater understanding of the breadth of applications in which vacuum can be beneficial as well as some of the common pitfalls of ineffective vacuum fittings along with the tools to fitting TF vacuum successfully.
Increase the utilization of TF vacuum through the evidence based illustration of improved clinical outcomes through proper patient assessment and clinical techniques.
Because of the wide number of variables that are involved with amputees, a statistical study is not only challenging but very lengthy with the limitation of the size of the patient population. This study is based on clinical significance by demonstrating the impact of a single technique over a wide population of patients with varying level of residual limb anatomy including length, skin integrity, invaginations, tissue definition, and skin grafts. This is successfully demonstrated through the use of the Ossur Unity vacuum system with the flexibility of custom liners and custom seal placement. However, the products are only one component of the equation. The foundation of the technologies success is also coupled with a simple yet underutilized technique of a combination of proper casting techniques, modification, and a flexible inner socket. The fabrication of the socket technique allows for vacuum to be pulled on both sides of the flexible inner socket. This allows the system to be sleeveless and provides for greater adjustability and flexibility for the prosthetist.
Seven case studies will be presented with a patient population ranging in age, level of ambulation, and anatomy. The results of the techniques demonstrated were reduced skin breakdown, increased suspension force resulting in greater patient control over the prosthesis, volume control, and ultimately greater patient satisfaction with reduced office visits.
Patients with bony residual limbs benefitted from the volume control of this process that provides a layer of protection throughout the day that would have otherwise deteriorated over short periods of time. Patients with scar tissue, invaginations, and grafted tissue benefit from the reduction of skin breakdown and volume control that results from traditional prosthetic techniques. This is a result of elimination of pistoning that would historically occurred as volume fluctuates and sheer forces are constantly imposed on the residual limb through normal activities. All patients experience a sense of greater control over their prosethesis which results in a desire for more activity but can only be achieved with the combination of reducing the impact of volume control and skin breakdown that would make higher levels of desired activity uncomfortable and sometimes extremely painful.
In conclusion, Vacuum technology provides a wide variety of clinical benefits for patients that can now be applied to both TT and TF patients with a wide variety of anatomical structures. The limitation of vacuum systems are that they are less intuitive than traditional mechanical systems and should be used with caution with patients with limited cognitive capabilities. With the exception of that population, vacuum is a generalizable technique that can be used for a breadth of patients with sigificant outcomes across all demographics. It is the intent of this paper to show that vacuum technology should be a standard of care rather than an exception and how vastly different patients live scan be as a result of good clinical practices.
0267
Christopher Harper (1) presenting
Christopher Harper Prosthetist, Johannesburg, Gauteng, South Africa (1)
A new concept in bench alignment for lower extremity prostheses
As a prosthetist I struggled with lower extremity alignment, especially higher levels of amputation. I started researching prosthetic alignment and designed an alignment jig to assist me to achieve the correct alignment objectives and to be able to measure and record the alignment of a prosthetic socket. There have been many improvements in the field of prosthetics, but I don’t believe that modular adjustable components have provided much improvement in alignment.
The aim of my project was to develop a device which would assist me to accurately attach the socket adaptor to the socket, to hold the prosthetic socket in the correct alignment.
The alignment process consists of bench alignment, static alignment and dynamic alignment. Much of our current bench alignment techniques rely on visualization of the prosthesis rather than on measurements. I first identified the six alignment parameters of a prosthetic socket (flexion, extension, abduction, adduction, height and rotation). I then developed a device which would be able to independently adjust and set each of these alignment parameters. The jig I have designed uses measurements to achieve the alignment objectives. This alignment jig follows the principle of the ‘six degrees of freedom’ of a prosthetic socket on a Cartesian coordinate system.
With this prototype bench alignment jig I am able to record a patient’s alignment. I am able to change one alignment parameter without affecting any other parameters. I am able to use it to transfer alignment to the definitive socket. With more accurate alignment I am able to use fewer components thereby reducing the weight of a prosthesis.

It can take a prosthetist many years to gain the necessary experience to be able to accurately align a prosthesis. This results in many prostheses not being aligned to their optimum. With the correct tools and alignment principles, I believe that it is possible for all prosthetists to achieve accurate repeatable alignment. The one limitation in my study is difficulty in accurately determining the centre of the hip joint of the patient. However, despite this limitation I have had successful outcomes using this technique and device.
Zahedi MS, Spence WD, Solomonidis SE, Paul JP. Alignment of lower-limb prostheses. J Rehabil Res Dev. 1986;23:2-19.
0269
Bianca Buijck (1) presenting Sytse Zuidema (3) Monica van Eijk (4) Debby Gerritsen (2) Raymond Koopmans (2)
Rotterdam Stroke Service, Rotterdam, The Netherlands (1) Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands (2) University of Groningen, Groningen, The Netherlands (3) Leiden University Medical Centre, Leiden, The Netherlands (4)
The association between neuropsychiatric symptoms and quality of life in geriatric patients with amputation or stroke after rehabilitation in skilled nursing facilities
The most common causes of lower limb amputation (LLA) are peripheral arterial disease (PAD) and diabetes, which frequently occur in the elderly. Thirty percent of LLA patients have had a stroke prior to amputation. LLA and stroke, and associated co-morbidity cause major problems in daily life such as physical disabilities, psychological ill-being and dependency on care. Physical disabilities, less social activities, vascular disease, depression, gender and higher age, are factors affecting Quality of Life (QoL).
The objective of this study was to identify the determinants of quality of life of home dwelling patients with amputation or stroke three months after rehabilitation in a skilled nursing facility.
This study is part of the Geriatric Rehabilitation in AMPutation and Stroke study, which is a prospective, multi- centre, cohort study aimed at identifying determinants of rehabilitation outcomes. Quality of life was the primary outcome (RAND-36). Neuropsychiatric symptoms, depressive complaints, (instrumental) activities of daily living and balance were the possible determinants of quality of life. Additional, for amputation we assessed walking ability and for stroke we assessed arm function. Linear regression analysis was used to identify the possible determinants.
Twenty-seven out of 48 patients with amputation and 123 out of 186 patients with stroke were discharged to their homes or to an assisted living situation. On the eight quality of life domains (range 0-100) the main scores varied between 22 and 87 for patients with amputation and between 48 and 85 for stroke patients, with the lowest scores in both groups for the domain Physical Functioning. For both groups, low quality of life on the domains Role Limitations Emotional, Social Functioning, Mental Health and Vitality were primarily explained by neuropsychiatric symptoms and depressive complaints. Stroke patients also experienced lower quality of life on the domain Role Limitations Physical.
The presence of neuropsychiatric symptoms and depressive complaints negatively affect quality of life of patients with amputation or stroke. The two groups of patients had severe disabilities. These patients may experience a good quality of life. This phenomenon is known as the disability paradox, suggesting that quality of life is about finding a proper balance between several factors, even when important life domains are severely affected.
0270
Jennifer Ernst (1) presenting Thomas Schmalz (2) Veit Rohde (3) David Liebetanz (1)
Department of Clinical Neurophysiology, University Medicine Göttingen, Göttingen, Germany (1) Department of Research, Otto Bock Healthcare, Duderstadt, Germany (2) Department of Neurosurgery, University Medicine Göttingen, Göttingen, Germany (3)
An overview of a seven years experience in restoration of gait with the FES based implantable drop foot stimulator system ActiGait in chronic stroke patients
Drop foot is a major disability, which often remains after stroke.1 The foot drags along the ground during the swing phase.2,3 Finally drop foot leads to decreased speed, limited endurance and increases the risk of falls. These factors can limit mobility, independence and reduce the quality of life (Perry, 1995)
Aim of the study was to demonstrate that functional electrical stimulation represents an alternative treatment of stroke-related drop foot compared to the conventional treatment by an ankle foot orthosis (AFO).
The system consists of an externally worn heel switch which is sensitive to pressure, thus controlling wireless the time point of the stimulation which is applied via a cuff electrode to the common peroneal nerve. Walking speed (10-meter gait test, [m/s]) and walking endurance (6-minute gait test [m/6min]) were tested prior to, 6 and 12 weeks after the implantation (n=5). In addition, ankle joint angles were assessed via an optoelectronic six camera system (Vicon), i.e. initiation angle, initial plantar flexion, dorsiflexion and final plantar flexion [◦] during stance phase at baseline and 12 weeks after implantation.
In 7 years a neurologist examined more than 300 patients suffering drop foot and 60 patients fulfilled criteria for implantation. The most important inclusion criterion for implantation was to elicit balanced dorsiflexion by a surface droop foot stimulator. The results of the safety study (n=5) showed that patients’ gait speed have increased (0.55; 0.77 m/s) as had walking endurance (211; 260 m). In addition, gait analysis after 12 weeks revealed a nearly normal physiological initiation angle (113◦ vs 122◦) and an increase in the initialplantar flexion (7◦ vs. 0◦).
Within a safety study (n=5)4 and up to now in a 7 years experience we evaluated the effects of the system on gait. The system increased gait speed, walking endurance and ankle joint kinematics. This is the result of active ankle dorsiflexion via electrical peroneal stimulation during the swing phase of gait and a stabilized prepositioning of the foot at the beginning of stance phase. Thus ActiGait system represents an active alternative therapeutic option for the treatment drop foot due to a cerebrovascular insult.
1Duncan, P.W. (1994). Stroke disability. Phys Ther. 74(5), 399-407.
2Perry, J. (1992).
3Perry, J., et al.(1995). Classification of walking handicap in the stroke population. Stroke 26(6), 982-9.
4Ernst et al. (2013). Towards physiological ankle movements by using ActiGait implantable drop foot stimulator in chronic stroke. Restor Neurol Neurosci.
0272
Karen Rispin (3) Virginia Wright (1,2) Jan Andrysek (1,2) presenting
Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario, Canada (1) University of Toronto, Toronto, Ontario, Canada (2) LeTourneau University, Toronto, Ontario, Canada (3)
Assessing the test-retest reliability of the Lower Limb Function Questionnaire (LLFQ)
Psychometrically strong outcome measures are essential tools in research and clinical practice that allow evaluation of impact and lead to better clinical care. However, there is lack of outcome measures for lower limb function of orthotic and prosthetic users that are contextually relevant and appropriate for low and middle income countries. In response, our team developed the Lower Limb Function Questionnaire (LLFQ). This youth-report measure is comprised of 20 walking-based items relating to balance/falls, fatigue, pain, walking on uneven terrain, navigating obstacles, running, vehicle use, device appearance and sound, and overall satisfaction with lower limb function.
To evaluate the test-retest reliability of the LLFQ with a population of teens and young adults with gait abnormalities
Participants were a convenience sample of students with gait abnormalities at a boarding school for children/youth with disabilities in a low-resource setting in Africa. Many used lower limb orthoses, prostheses, and/or assistive devices. The LLFQ was administered in a group classroom setting so that all participants heard the same test instructions. It was administered twice with the second session (re-test) six days later. Each LLFQ item was scored using a 100 mm-visual analogue scale (VAS) with item-specific word anchors at either end. A total summary percentage score was calculated. Intra-class correlation coefficients (ICC) and 95% Confidence Intervals (CIs) were used to evaluate test-retest reliability.
Forty-four students completed the LLFQ twice (20 males; mean age 16.7 SD2.4). Other demographics were as follows: Disabilities - 15 cerebral palsy, 9 trauma, 4 spina bifida, 1 club foot, 7 congenital abnormality, 8 other; Assistive devices – 13 no device, 14 raised shoe, 4 ankle foot orthoses, 5 knee ankle foot orthoses, 6 above knee and 2 below knee amputations; and 29 had unilateral and 15 bilateral disabilities. LLFQ mean scores were 60.6 (SD 18.1, range 17 to 94) at session 1 and 62.0 (SD 17.2, range 22 to 94) for session 2. Both data sets were normally distributed (D’Agostino-Pearson test, P >0.40). The test-retest ICC was 0.86 with 95% Confidence Intervals of 0.76 to 0.92. All youth were able to complete the LLFQ on their own following the group instructions, and did so within 20 minutes.
The LLFQ demonstrated mean scores near the middle of its scale and a normal distribution showing that it was able to effectively capture the broad spectrum of functional gait abilities in the study sample. The ICC of 0.86 and lower 95% confidence interval of 0.76 demonstrated that the LLFQ had strong reliability in this sample. Validity testing and comparative evaluations of the LLFQ with a grade level based VAS (F to A+)) are underway.
0273
Jan Andrysek (2,3) presenting Karin Rotter (1) Daniela Garcia (1) Rebeca Valdebenito (1) Virginia Wright (2,3) Ricardo Torres Moreno (2,3) Carlos Alvarez Mitchell (1) Rafael Cubillos (1)
Sociedad Pro Ayuda del Niño Lisiado, Santiago, Chile (1) University of Toronto, Toronto, Ontario, Canada (2) Holland Bloorview Kids Rehab Hospital, Toronto, Ontario, Canada (3)
Clinical field trials of a new type of prosthetic knee joint utilizing the automatic stance-phase lock mechanism
For transfemoral amputees, a functional prosthesis is essential for safe, efficient and effective mobility. To address global need for affordable, durable and functional prostheses, we developed a new type of stance-phase control mechanism for prosthetic knee joints providing a high level of stability without impeding the natural movements of gait. The mechanism is based on a lock that engages to provide stability in response to the loads placed on the limb. The mechanism is simple to repair, maintain and setup.
The aim of this work was to conduct a clinical field trial to evaluate the new knee joint. Our objectives were to measure function, user satisfaction and long term performance.
In this prospective cross over study we compared the new knee to each participant’s regular weight-activated friction knee (3R15, Otto Bock). At baseline, 10 participants (adolescents with transfemoral amputations) were assessed with their regular knee and then provided with the new knee to wear for one month before doing the assessments. In the second part of this work, long term follow-up assessments with the new knee were conducted at 3, 6 and 12 months for 9 of the 10 participants who continued using the new knee. Main outcomes were mobility function using walk tests (20 meter and 6 minute walk tests) as well as energy expenditure based on the physiological cost index (PCI). User satisfaction was evaluated during each session using self-report questionnaires adapted for the study.
Over the short term (one month of using the new knee), no differences were found between knees for the walk tests or PCI. Walking speeds for the 20 meter walk tests were on average 1.1 m/s for both prostheses, PCI was 0.71 beats/meter for the regular knee and 0.6 beats/meter for the new knee and 6 minute walk test distance was ~ 370m for both knees. The PCI for the new knee decreased to 0.52 beats/meter at 3 months and 0.40 beats per/meter at 6 months (p<0.002). Nine out of the 10 participants preferred the new knee for its stability and ease of walking and chose to use the new knee at month one. At 12 months minor technical issues were reported but all participants were still using the new knee (n=9).
Many of the participants were long term users of the weight-activated knees, which may explain the long acclimatization period to the new knee, and significant decreases in energy expenditure (PCI) that were measured only after 3 and 6 months of use of the new knee. These findings are in agreement with the user feedback suggesting greater ease of walking. Based on the long term evaluations the new knee and its locking mechanism appear to be highly durable and reliable.
0275
Eiichi Genda (1) presenting Takuya Miyagawa (2) Mitsuru Hyashi (2)
Minami Seikyo Hosoital, nagoya, Japan (1) Matsumoto PO manifacturing co.ltd, nagoya, Japan (2)
Leg driven wheel chair for hemiplegic people
Not all wheelchair users have completely disabled legs. Wheelchair users include the people who are able to move their legs but do not have enough strength to walk, and also the people who can walk but are easily get tired or who are unstable to walk. Once those people start using wheelchairs, they stop moving their legs, and that makes their movable leg’s muscle to become even weaker, and diminishes the ability to walk again. In order to interrupt this vicious cycle, we recommend to use the leg-driven wheel chair for the people who can still move their legs but not able to walk. When using this leg-driven wheelchair, people are using their legs and it prevents atrophy of leg muscles. Incomplete SCI people, hemiplegics and aged people are good potential users for this wheelchair.
The aim of this study is to provide hemiplegic people with easy moving and easy handling wheel chairs driven by their healthy legs and controlled by their healthy arms.
Driving method for easily exerting muscle force, and easy back-and-forth change without clutch operation were adopted. Single side pedaling with a healthy leg and steering with a healthy arm were adopted. The driving mechanism is consisted of four parts; a pedal, a pulley at the axis of wheel, a steel wire which winds around the pulley, and a spring which connects the end of the wire and frame of wheelchair. When the pedal is not pushed, the wire is loose and the pulley rounds freely. When the pedal is pushed, the wire winds up and rotate the pulley by friction. In other words, driving force is transmitted only when necessary. A steering handle is attached to one of the front wheels.

We measured time required for driving around 30 m track and figure-of-eight slalom course by using this leg-driven wheelchair and the conventional wheelchair.
The subjects were seven healthy people and three hemiplegic people. For 30 m track drive, on conventional wheelchair, it took averaged 25 seconds for healthy people, and 82 seconds for hemiplegic people. When using leg-driven wheel chair, it took only 22 seconds for hemiplegic people.
In case of slalom course, on conventional wheelchair, it took averaged 80 seconds for healthy people, and 180 seconds for hemiplegic people. When using leg-driven wheel chair, it took only 70 seconds for hemiplegic people. When using conventional wheel chair, hemiplegic people take 2 to 3 times longer than healthy people. But when hemiplegic people use leg-driven wheelchair, they can actually drive faster than healthy people on the conventional wheelchair.
Our leg-driven wheelchair was easier to drive for hemiplegic people than conventional wheel chair.
0276
Daranee Suvapan (1) Sarinee Kaewsawang (1) presenting Suleepun Solunda (1) Bootsakorn Loharjun (1)
Sirindhorn National Medical Rehabilitation Centre, Nonthaburi, Thailand (1)
Epidemiology of Lower Limb Amputees and Accessibility Rate to Prosthetic Services in Thailand
Access to health services improvement, rehabilitation and assistive technology development, and support related research are increasing global concern on better health for people with disability. In Thailand, Ministry of Public Health (MOPH) has conducted a 3-years program since October 2013. This implemented program has aim to increase medical services accessibility and develop for barrier eradication of Thai amputees. There were a few reports on causes and level of amputation in Thailand. Moreover, monitoring and evaluation has required for further strategic planning and program improvement.
The study was aims to provide current report on demographical and epidemiological situation including gender distribution, causes and level of amputation in Thailand. Moreover, accessibility rate of prosthetics providing had identified.
The implemented program has involved medical management, rehabilitation design arrangement and assistive technology development. The main operation has consisted of four relating stages: (1) community survey of the old and new case of amputees (2) registration of all amputees (3) medical service management for amputees, and (4) follow up and evaluation. Structured questionnaire was used for collected on baseline data as well as gender, cause and level of amputation, comorbidity, accessibility and prosthetics used. According that, the database has been updated by cooperation with National Health Security Office (NHSO) and local administration. Descriptive statistics were initially analysed. In addition, comparison was made between genders in terms of access to prosthetic service, needs, utilization of prosthetic limb and comorbidity. Moreover, geographical distribution of accessibility rate for the prosthetic services was presented.
In Thailand, we have currently registered 15,684 prevalence cases of lower limb amputee. Three-quarter (75.2%) are male. Major cause of the lower limb amputation are injury (58%), diabetes (17.4%), others included conflict (17.1%), birth defect (4.6%) and cancer (2.9%) respectively. Whereas, level of the lower limb amputated is at below knee (51%), above knee (32.9%), knee joint (7.5%), ankle joint (5.2%) and hip joint (3.4%). According to the policy implementation for the amputees, there has focused on access to medical service and management for prosthetic and assistive devices. Accessibility rate for the services is reported very high (91.9%); however estimated one-quarter (23.2%) of the rate has out of order devices. The rate (median 67.3%, IQR 56.1- 76.6%) has geographical attributed in figure 1.
Characteristic and caused of lower limb amputation in Thailand, 2014.


Accessibility rate of prosthetic service by province
Gaining insight on this information will enable policy planners to regulate accessibility rates and alleviate the barriers for amputee. Epidemiology, disability studies and research need more support. In addition, registry system and lifetime health informatics should be encouraged. Moreover, utilization of assistive device and training need more concern. Above all, it could be beneficial for further strategic planning in eradication of barriers for Thai disabled people.
0277
Ecaterina Vasluian (1) presenting Raoul M. Bongers (2) Heleen A. Reinders-Messelink (1,3) Pieter U. Dijkstra (1,4) Corry K. van der Sluis (1)
Department of Rehabilitation Medicine, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands (1) University of Groningen, University Medical Center Groningen, Center of Human Movement Sciences, Groningen, The Netherlands (2) Rehabilitation Center ‘Revalidatie Friesland’, Beetsterzwaag, The Netherlands (3) Department of Oral and Maxillofacial Surgery, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands (4)
Preliminary study of the Southampton Hand Assessment Procedure for Children and its reliability
The Southampton Hand Assessment Procedure (SHAP) is currently used in the adult population for evaluating the functionality of injured or prosthetic hands (1). The SHAP provides functional scores for six hand grips (spherical, tripod, power, lateral, extension, and tip) and an overall score. The scores are calculated from the performance times of 26 tasks. The SHAP cannot be used for children because of the relatively large size of the objects used to perform SHAP tasks and unknown clinimetric properties.
The aims of this study were to adapt the SHAP for use in children (SHAP-C) and to analyze the reliability of the SHAP-C in unimpaired children.
The SHAP-C was adapted based on the SHAP protocol. Some objects were downsized to allow grasping with a pediatric hand or pediatric prosthesis. The timing of tasks was performed by the rater instead of the participant; in case of original SHAP the participant times his/her own performance. Intra- and inter-rater reliability were assessed in 4-6 years old children between with unimpaired hands. The repeatability coefficients (RCs) were calculated. An RC ≤ 75% of the mean SHAP-C task values was considered adequate reliability.
In total 24 children (13 boys), 5 y/o (sd 0.54) participated. Children were all able to perform SHAP-C tasks. The means of the SHAP-C tasks ranged from 0.8 to 1.2 seconds for abstract objects and from 0.6-19.1 seconds for activities of daily living. The RCs of a single assessor did not exceed 75% in 17/26 SHAP-C tasks, displaying a relatively good intra-rater reliability, whereas the RCs for the inter-rater reliability exceeded 75% in 22/26 SHAP-C tasks, thus displaying poor inter-rater reliability.
In this first study that adjusted the SHAP for pediatric use, we found that all SHAP-C objects and tasks could be performed by children. The intra-rater reliability was better than the inter-rater reliability. Possible factors that may have influenced results are data collection method, variation in children’s motivation and assessors’ reaction time.
Although the SHAP-C appears to be a promising instrument, the protocol requires further modifications to provide reliable measurements in children.
Light CM; 2002 Arch Phys Med Rehabil. Establishing a standardized clinical assessment tool of pathologic and prosthetic hand function: Normative data, reliability, and validity.
0278
SASITHON SUKTHOMYA (1) presenting SIRINTHIP KAEWTIP (1)
SIRINDHORN SCHOOL OF PROSTHETICS AND ORTHOTICS, BANGKOK, Thailand (1)
The effect of fiberglass cast bandage UCBL orthosis by direct casting technique: A case report
This pilot study has developed alternative methods in providing UCBL orthosis by used the fiber glass cast bandage for mobile unit in Thailand. Adoption of the available materials and knowledge can result in an increase of productivity as well as improvement of quality. In order to improve service in Thailand of the patient in speeding provision of the devices and reducing the time visit to P&O facilities. This technique can also increase the productivity of the clinician.
The purpose of this study was to understand the effectiveness of fiberglass cast bandage UCBL orthosis in controlling of the calcaneus alignment as well as compare the strength and cost of this method to the standard method
During this study, a 23 year old with flexible calcaneus valgus was selected. Three times casting of the fiberglass cast UCBLs with non weight bearing technique and controlling subtalar joint in neutral position by the Orthotist was applied to the subject. The casts were fabricated and trim according to the standard trim line. The fiberglass cast UCBLs were fit to the subject and the orientation of calcaneus alignment was checked by standard Goniometer. Then the strength of material was tested by compression and tensile test machine as well as the times and costs assumption used in this study by comparing to the standard method.
The study reported that the fibreglass cast UCBL orthoses are possibly realigned the calcaneus from 10° valgus to 3°, 0° and 3° respectively in three times fitting process wiin difference devices. The time spent in rectification and fabrication of fibreglass cast bandage UCBL was around 60 percent less than polypropylene UCBL. Future, there was a higher force resistance with a fiberglass cast bandage UCBL by 18 kg while no significantly difference in thickness as appear in figure1. This study also shows cost of UCBL associated with fiberglass cast bandage provision include direct and indirect costs, that is the price of staff time (labor cost), materials and participants attendance were about 50 percent less, compared to a conventional.

Directed casting from patient by using fiberglass cast bandage require the skills with highly trained and experience to cast and control subtalar joint in desired position. An advantage of this technique, besides comfortable fitting and realignment is rarely the reduction of fabricating time, often to less than 3 hours as well as costs. The study provides widespread treatment for related foot problems for patient, especially in local area unit within limitation of time, material, tools and financial support.
0279
Claudio Vergari (1) Justin Mazué (1) Kariman Abelin-Genevois (2) Clayton Adam (1) Wafa Skalli (1) presenting
Arts et Metiers ParisTech, Institut de Biomecanique Humaine Georges Charpak, LBM, 151 bd de l’hopital, 75013, Paris, France (1) Department of Paediatric Orthopaedics, Hospices Civils de Lyon, Claude Bernard Lyon 1 University, Lyon, France (2)
Personalization of spine and trunk models for the simulation of brace action in spinal deformity: an inverse approach
Simulation of spine and trunk biomechanics could become a common tool in orthotic and prosthetic design and manufacture for the treatment of spinal deformity. The utility of such tools requires personalization of the underlying biomechanical models on which simulations are based. While improvements have been made in obtaining patient-specific geometries for trunk models [1-2], mechanical properties (MP) for tissues are still based on literature data.
To propose an inverse method to personalize trunk MP in spinal deformity patients, with relevance to the application of brace simulation.
Stereoradiographs of ten patients diagnosed with progressive adolescent idiopathic scoliosis were acquired before bracing and in-brace. Brace action was simulated with a geometrically personalized finite element model [2]. A sensitivity analysis was performed to determine the influence of MP (elastic modulus) for the following eight anatomical structures: ribs, rib joints (costovertebral and costotransverse), sternum, vertebrae, intervertebral discs (IVD), posterior ligaments, intercostal wall and ligaments. The values of the most influential parameters then modified, independently in each patient, in order to reduce the simulation error as compared to each patient’s measured in-brace clinical parameters.
Sensitivity analysis showed that the models were most sensitive to MP for five anatomical structures (IVDs, vertebrae, intercostal wall, ribs and rib joints). Overall, the models were not very sensitive to mechanical property variations; for instance, a variation in IVD elastic modulus between 50% and 200% of the benchmark value induced a mean change of 0.8° in simulated in-brace Cobb angle and 0.7° in rib hump. The procedure of mechanical property personalization, however, improved simulation results (Figure 1, actual in-brace geometry, nominal and mechanically personalized brace simulations of a patient in whom the AVR error was reduced by 2° and kyphosis by 1°).

This work is a preliminary approach to an inverse method for the personalization of tissue MP in computational simulation of bracing. The procedure reduces errors compared to clinically measured indices; the lower limit of these errors is the measurement uncertainty of the 3D reconstruction. The optimization process was manual in this preliminary work, and it was guided by a sensitivity analysis. The next step is to fully automate the optimization procedure, thus allowing personalization of MP not only when simulating brace action in adolescent idiopathic scoliosis, but potentially in other orthotic treatments.
[1] Cobetto et al.; 2014 Spine Deformity
[2] Vergari et al., 2014 Accepted Spine Deformity
0280
Takuya OKAMOTO (1) presenting Makoto ASAEDA (1) Yoshihumi KONO (1) Chiaki TERAI (1) Wataru KUWAHARA (1) Hodaka WATANABE (1) Noboru SHIMADA (2) Naoto FUJITA (3) Masataka DEIE (3)
Health Science Major, Graduate School of Biomedical & Health Sciences, Hiroshima University, Hiroshima City, Japan (1) Hiroshima University Hospital, Department of Rehabilitation, Division of Clinical Support, Hiroshima City, Japan (2) Department of Musculoskeletal Functional Research and Regeneration, Integrated Health Sciences, Hiroshima City, Japan (3)
Soft Knee Brace for Medial Osteoarthritis Knee Reduces the Amount of Lateral Thrust Using Gait Analysis
Knee osteoarthritis (OA) is seen most of the elderly people and the main symptom is pain during gait. In the stance phase of gait, medial knee OA patients have lateral thrust and are increased in the external knee adduction moment (EKAM). These kinematic changing may be the factor of the pain during gait. Soft knee brace is used to reduce the pain for medial knee OA patients. However, the soft brace’s mechanism of pain relief is unknown.
We investigated the effect of the soft knee brace on lateral thrust, EKAM, and pain for medial knee OA patients by using gait analysis system.
Six medial knee OA patients [Age: 64.5 ± 6.6(Mean ± SD), BMI: 26.4 ± 4.9(Mean ± SD), Kellgren-Lawrence grade Ⅲ:Ⅳ= 2 : 4] participated in this study. Gait analysis was used three-dimensional motion capture systems VICON MX (VICON, Oxford, UK) and multiple force plates (AMTI, Watertown, US). The EKAM was time integrated and normalized to body mass (EKAM impulse). Lateral thrust was computed by the change of the amount of maximum to minimum knee varus-valgus angle. The knee varus-valgus angular velocity was defined as taking the time derivative of the varus-valgus angle and calculated peak value. These gait variables were extracted from 0 to 20 % of one gait cycle of each trial and averaged each patient’s three trials. The pain during gait was measured by Visual Analogue Scale (VAS). Significance of differences between with and without brace was determined by paired t-test, and p<0.05 indicated a statistically significant difference.

The pain during gait was significantly reduced in the braced conditions. There were no significant differences between two conditions in EKAM impulse. Lateral thrust and the peak of knee varus-valgus angular velocity was significantly lower in the braced conditions than unbraced conditions.
The results of this study suggested that soft knee brace did’nt affect the EKAM impulse, but it contributed the reduction of lateral thrust and pain during gait for medial knee OA patients. From this study, the effect of the soft knee brace could suppress lateral thrust and knee varus-valgus velocity, and these kinematic changings may be the mechanism of pain relief with using brace for medial knee OA patients.
0281
Masaya Nomura (1) presenting Kiyoshi Nishimoto (2)
REHABITECH Co.,LTD, Kyoto-shi,Kyoto, Japan (1) Hiroshima Institute of Technology, Hiroshima-shi,Hiroshima, Japan (2)
Development of a modular multi-fingered electric prosthetic hand
A modularized multi-fingered electric prosthetic had (MMEPH) is developed. The MMEPH us consisted of three modular parts which were a wrist module, metacarpal module and finger module. The wrist module is constructed of two parts which are a mobile hand wrist joint and the carpal joint that are connected to each metacarpal module. The metacarpal module is consisted of a drive unit that moves the finger modules. The finger module is consisted of a joint unit which generated a rotational movement and skeletons that link the joints.
Our aims of this study are a development of MMEPH and an evaluation of its movement as well as grasping performance.
First of all, the motor performance of a single finger which consists of finger and metacarpal module with 3 joints within is evaluated. A motion speed and placement reproducibility are examined. A time from the maximum extension to the maximum flexion is measured for a motion speed. Also placement reproducibility is measured by angle error occurred by placing a joint at 30 degrees from 0 degrees 10 times. A placement of a fingertip is calculated by from forward kinematics from the values of potentiometer
Secondly in order to verify the gripping stability by multiple fingers, both three fingers with three joints and five fingers with human like configuration. A successful result is set to be grasping more than 10 seconds. The maximum weights exerted are measured when 30mm diameter tube with a power grasp and 80mm diameter sphere with fingertips grasping.
A motion time require from maximum extension to maximum flexion is 2.0 seconds. The placement repeatability is 1.5+/-0.3mm (Ave.+/-SE). 840gf with 3 finger configuration and 1050gf with 5 finger configuration were possible with a power grasping. 700 gf with 3 finger configuration and 760 gf with 5 finger configuration were possible.
MMEPH is developed. Evaluation of finger motion performance of a single finger is evaluated as well as the grasping performance of both three and five finger configurations. The five finger configuration possesses better grasping stability than the three finger configuration regardless of shape of grasping. However the three finger configuration still shows sufficient ability in practical situation. For instance when the weight and cost of five finger configuration is insufficient to fulfil patient needs, three finger configuration may be used. Hence availability of MMEPH may be highly required.
0283
Maja Mlakar (1) presenting Helena Burger (1)
University rehabilitation Institute, Ljubljana, Slovenia (1)
Satisfaction of upper limb amputees with their prostheses
Experiences of rehabilitation team for persons with upper limb amputations shows that satisfaction of the patients with their prostheses varied from the very high level of satisfaction to zero. We didn’t find the validate questionnaire which the patients can fill in quickly and we can use them in our every day practice.
The aim of our study was to find out the opinions of persons who wear upper limb prosthesis about appearance, comfort of socket, durability, function, donning and doffing, ability for daily activities, weight of prosthesis and the feeling of temperature in the socket.
We prepared the questionnaire on the basis of two articles [1,2]. In the study were included all upper limb amputees who visited our outpatient clinic between August 2007 and February 2008 and were active users and willing to participate. The questionnaire had questions about appearance, comfort of socket, durability of prosthesis, function, donning and doffing, ability for daily activities, weight of prosthesis and the feeling of temperature in the socket with four possible answers: bad, satisfying, good and excellent.
In the study were included 19 persons, 5 women and 14 men. They were 50 years old on average (from 20 to 84). Mostly they use cosmetic prosthesis. In the group of persons with cosmetic prosthesis majority of them assess as “good”: appearance, comfort of socket, durability, donning and doffing and the weight of their prostheses. Mark “bad” half of them gave to functionality, ability for daily activities and the feeling of temperature in the socket. Persons with body-powered prosthesis were more satisfied with appearance and donning/doffing of their prostheses while the temperature of the socket was assessed as “bad”. All other factors in this group were assessed mostly as “satisfying”.
There are no many studies about satisfaction of upper limb amputees with their prostheses. Davidson [1] reported that 55% respondents express greatest dissatisfaction with sweating what we can compare with 68% of persons in our study which asses feeling of temperature in the socket as “bad”. Kyberd [3] asked the upper limb amputees about problems with prosthesis. 20% reported about problem with fit, cosmesis and maintenance and 33% reported problem with function. In our study 53% of answer also assesses the function as “bad” or as “satisfying”. Upper limb amputees are partially satisfied with their prosthesis. The questions about topic of satisfaction with upper limb prosthesis have not been fully researched yet.
[1] Davidson J. J Hand Ther, 2002,15:62-70.
[2] Alsancak S. Prosthet Orthot Int, 2003, 23:139-145.
[3] Kyberd et al. J Prosthet Orthot, 1998;10(4): 85-95.
0284
Dominik Erzar (1) presenting Helena Burger (1)
University rehabilitation Institute, Ljubljana, Slovenia (1)
Comparison of two casting methods for trans-tibal socket
Prerequisite for good socket fit is a good cast. Casting can be done in different ways, by Plaster-of-Paris, scanner or by CIR system [1 – 3]. Good system is quick, easy and gives an exact replicate of the stump.
The aim of our study was to compare time need for casting and model rectifications, different measures and patients comfort with socket made after casting by Plaster-of –Paris and by CIR system.
Eight persons after trans-tibial amputation, all already walking with prosthesis at least 500m, with no wounds and no neurological impairments were included into study. The same prosthetist cast them by Plaster-of-Paris and by CIR system in random order. We measured time needed for casting and model rectification by both methods, patients satisfaction with socket fit on VAS. AP and ML measures, circumferences at knee, PTB, fibular head and the distal end and the stump length were taken for stump and both models. Data were statistically analysed. The study was approved by Ethic committee of our Institute.
Casting by CIR system was three times shorter than by Plaster-of-Paris (15.9s vs 49.6s, p<.001). Cast modification was half shorter after casting by CIR system than by Plaster-of-Paris (16.6s vs 31.1s, p=.002). Socket made by CIR system patients scored significantly less comfortable than the one made by Plaster-of-Paris (1.6 vs 8.8, p<.001). The difference between stump measures and model made by CIR system were for AP, ML measures, and all circumferences of CIR greater than between stump and model made by Plaster-of-Paris, whereas CIR model was shorter than model made by Plaster-of-Paris (p<.001).
As all other studies [1-3] we also found out that casting and cast modification by CIR system is much quicker that by Plaster-of-Paris, but unfortunately we were not able to obtain good and comfortable socket fit as described by others [1-3]. There may be several reasons for this. All included persons were used to have a not full contact socket for several years and may find full contact uncomfortable. After casting by CIR system the prosthetist did not do all rectifications as when cast was taken by Plaster-of-Paris. It seems that in spite of workshop on how to use the system, we are doing some mistakes that have to identify and correct.
[1] Wu Y et al. Prosthet Orthot Int 2009;33(1):1 – 9.
[2] Thanh NH et al. Prosthet Orthot Int 2009;33(2):130 – 4.
[3] Jivacate T et al. Prosthet Orthot Int 2011;35(1): 70 – 5.
0285
Bertrand Frossard (1) Lewis Mackay (1) presenting
Touch Bionics, Livingston, UK (1)
Upper limb myoelectric prosthetics: outcomes, reimbursement, and beyond
The lack of evidence showing the efficacy of upper limb prostheses has been highlighted (Biddiss & Chau, 2007; Kyberd & Hill, 2011), as a result, the authors of these studies called for the use of standardised measures to meet this need. The need to provide evidence of efficacy using validated measurement tools is also important due to increasing pressure to justify provision of advanced prostheses (Hill et al, 2009).
This study aimed to determine the efficacy of the i-limb ultra myoelectric multiarticulating hand, as a prosthetic intervention for upper limb absence, to support the French health authority reimbursement application
The Patient Care Pathway (PCP) is an online questionnaire which gathers responses to standardised measures. Data from the Disability of the Arm Shoulder and Hand (DASH) questionnaire were compared via mean comparison and rank tests for 69 i-limb ultra users at pre and post fitting, to demonstrate change in function and symptoms. All patients using an i-limb who had completed a pre and post assessment were included. The population was found to be representative, and consisted of responses from multiple centres. The population size allowed subgroup analyses. As the data collection is ongoing, the current state of the evidence will be shown in addition to the data presented for the reimbursement request.
Table1 shows pre and post fitting mean scores for subgroups and the full cohort:
–15.44 (Statistic Z= -3.727; p<0.05) for 23 patients that previously used a myoelectric hand (all types) prior to the i-limb ultra.
–18.71 (Statistic Z= -3.203; p<0.05) for 14 patients who previously used a myoelectric hand not developed by Touch Bionics.
–8.83 (Statistic Z= -4.523; p<0.05) for full cohort.
Pre and post DASH previous prosthesis users subgroup descriptive statistics

These results show change in excess of the MDC of the DASH for the whole cohort. The change in mean scores for the subgroups were clinically significant as they were approaching the MCID (Kennedy et al, 2011). The post fitting mean (14.94) for the subgroup of 14 was approaching the normative value for the US population (Kennedy et al, 2011). These results were a statistically significant indication that the i-limb ultra improved the functional outcomes of this cohort.

[1]Biddiss ; 2007 ; P&O Int. [2]Kyberd ; 2011 ; P&O Int.[3]Hill ; 2009 ; JPO [4]Kennedy ; 2011 ; Institute for Work&Health, Toronto.
0286
Michael Rexing (1) presenting
Scoliosis treatment center Bad Sobernheim, Bad Sobernheim, Germany (1)
Is a functional brace classification a better approach in the light of the modern three-dimensional understanding of scoliosis?
Modern braces for the treatment of adolescent idiopathic scoliosis (AIS) derived from Cheneau Brace have as a basis the old Schroth body block model and a radiological classification according to curvature pattern. The custom brace type is then selected based on the individual radiological pattern. The radiological classification does partially not match the clinical functional findings; therefore then the experience of the treatment team must often be used to select the individual brace type. 2014 a new functional Schroth classification was published from the Schroth-Institute. The terms 3 and 4 arching has disappeared. This new classification takes into account the necessary intervention in the sagittal profile.
Adapted to the new Schroth-Classification an attempt is made to describe a functional brace classification. This functional classification is to facilitate the work, especially in a functional oriented interdisciplinary team, and support the decision making process which brace is the best for an individual patient.
In a first step the basic models previously used have been allocated to the new Schroth-Basic-Pattern according on the functional three-dimensional aspects. In a second step these basic models have been modified according to the necessary intervention in the sagittal profile and in terms of a more functional correction approach. Finally, a new classification has been determined and is now used for the decision-making process which brace type is the best suited for the individual patient. Primary in-brace results are documented.
In a functional approach there is a clear assignment to 6 different basic-types. An allocation to the most common radiological classification and also to the common Rigo-Classification is given. It will be presented the first n200 initial in-brace correction effects from a group treated according to the new functional brace classification and will be compared with patients matched out of a population n713 treated according to the Rigo-Scheme between 2010-2013 presented at the SOSORT 2014 meeting.
For us the decision work which brace is the best for the individual patient is easier and the communication with the clinical specialist has got much clearer. The first results show no significant differences to our previous outcomes. De Mauroy from Lyon presented this year first results from his new ART-Brace, which show impressively how effective a brace is, if it is designed according to functional criteria. However it is not clear how helpful a functional classification is for teams do not work in a functional approach. Also there should be investigated whether this functional brace scheme is suitable for patients not treated with Scoliosis specific exercises like Schroth.
Rexing, M. AIS and current treatment approaches in orthotics. Presentation held on Antalya Meeting of ISPO/EPO 2014
0289
Brian Hafner (1) presenting John Cagle (1) Joan Sanders (1)
University of Washington, Seattle, WA, USA (1)
Prosthetic liner prescription practices: a survey of prosthetists in North America
The prosthetic liner serves as an interface between the rigid socket and the delicate soft tissues of the residual limb. As such, selection of an appropriate liner is of critical importance to the health of patients with lower limb amputation. It has been suggested that liner selection is primarily based on intuition, product literature, peer recommendations, and experience.1 However, limited evidence exists to accurately characterize prosthetists’ liner selection practices. Specifically, it is unknown how or why practitioners select specific liners for each individual patient.
The goals of this project were to characterize the range of liner products commonly used by prosthetists and to determine how they typically select liner products for individual patients.
A cross-sectional survey was developed by the investigators to evaluate prosthetists’ liner selection practices. Questions were created to assess respondent characteristics (e.g., age, clinical training, and clinical experience), resources they use to learn about liners, frequency with which they use specific liner products, and features of liners they deem important to the liner selection process. Prosthetists in the US and Canada with at least 1 year of experience managing prosthetic patients were recruited via clinical magazine advertisements, professional meeting flyers, and orthotic and prosthetic listserv postings. The survey was administered online using WebQ open-source software.
Respondents (n=107) were mostly male (79%), non-Hispanic white (87%), and resided in the United States (89%). Respondents were generally educated at the certificate (38%), bachelors (52%), or masters (11%) level and practiced as a certified prosthetist (43%) or certified prosthetist-orthotist (54%). The large majority of respondents indicated they received information about new liner products directly from manufacturers (94%). Fewer reported receiving information from clinical magazines (60%) or scientific journals (15%). The top 25 liner products routinely used by practitioners varied by manufacturer (Össur=11, WillowWood=7, ALPS=3, Otto Bock=3, medi=1). Prosthetists reported the most important liner properties included durability (91%), comfort (87%) and suspension features (78%). A small proportion (11%) of respondents acknowledged using a single liner product with all of their transtibial patients. A larger portion of prosthetists (86%) said they most often used only a few different products (mean=2.4, median=2) for their patients.
Results of this study indicate that prosthetists generally use only a few different prosthetic liner products for their patients with transtibial amputation, despite the availability of more than 60 unique liners on the market. Reasons for prosthetists’ selection practices are unclear, but may be due to a scarcity of comparable information about commercially available prosthetic liners. Objective tools or resources that allow practitioners to compare and contrast desirable liner characteristics may help to facilitate greater variety in product selection and improve health outcomes by matching individual patients with the liner product best suited to their needs.
1. Klute et al., Prosthet Orthot Intl, 2010, 34(2):146-53.
0290
Brian Hafner (1) presenting Sara Morgan (1) Robert Askew (2)
University of Washington, Seattle, WA, USA (1) Northwestern University, Chicago, IL, USA (2)
Reliability of self-reported outcome measures in people with lower limb loss: implications to clinical care and research
Evidence of reliability is needed to determine the purposes for which an outcome measure can be used. It is generally accepted that measures should demonstrate reliability of 0.7 or greater to be used for comparisons between groups of people.1,2 For applications that involve decisions about individuals, measures should demonstrate reliability of 0.9 or greater.3 Reliability therefore becomes a key factor in distinguishing measures that can be recommended for individual-level applications and measures that can be recommended for group-level applications.
The goal of this project is to assess the test-retest reliability of self-reported outcome measures designed to assess people with lower limb loss and to make recommendations for those that are best suited to individual- or group-level assessments.
People with unilateral, lower limb loss were recruited to take two self-reported outcome measure surveys 2-3 days apart. Mode of administration (paper or computerized) was randomly assigned. Surveys included several standardized measures, including the Prosthetic Limb Users Survey of Mobility (PLUS-M), the Prosthesis Evaluation Questionnaire Mobility Subscale (PEQ-MS), Activities Specific Balance Confidence Scale (ABC), Socket Comfort Score (SCS), and Patient Reported Outcomes Measurement Information System Brief Profile (PROMIS-29). Surveys also included demographic and health questions that were used to characterize the sample. Reliability of each instrument was quantified using the intraclass correlation coefficient model 3, type 1 (ICC 3,1).
Participants (n=201) were an average of 60 (SD=11) years of age and 18 (SD=17) years post-amputation. They were mostly male (67%), white (91%), and non-Veteran (74%). Participants were of mixed level of amputation (35% above-knee, 65% below-knee) and etiology of amputation (60% trauma, 23% dysvascular, 12% infection, 4% tumor, 1% congenital). Retest surveys were taken, on average, 2 (SD=0.2) days after the test survey. Time to complete the test and re-test surveys was 12 (SD=7) minutes and 10 (SD=6) minutes, respectively. Reliability of the administered measures ranged from 0.74 to 0.96. PLUS-M, ABC, and PEQ-MS showed high reliability (0.96, 0.95, and 0.92, respectively). SCS showed lower reliability (0.74) and reliability of PROMIS instruments ranged from 0.79 (Social Role Satisfaction) to 0.88 (Physical Function and Depression).
Results of this study indicate that the tested self-report health surveys have moderate-to-high (>0.7) test-retest reliability among people with limb loss. This indicates that the measures tested are suitable for group-level applications, such as quality improvement programs. Select measures (PLUS-M, ABC, and PEQ-MS) have high reliability (>0.9) and are suitable for individual-level applications, like monitoring patients over time. Use of these measures is therefore advocated, given their reliability, ease of administration, and potential to inform on individuals’ health outcomes.
1. Reeve BB, et al. Qual Life Res. 2013;22(8):1889-905.
2. Terwee CB, et al. J Clin Epidemiol. 2007;60(1):34-42.
3. Fitzpatrick R, et al. Health Technol Assess. 1998;2(14) :1-74.
0293
PRITPAL SINGH SIDHU (1) presenting
Indian Red Cross Society, District Branch, PATIALA, Punjab, India (1)
The Effects Of Tone Reducing Orthotics Appliances & Positioning Devices In Pain Intensity In Children With Cerebral Palsy
Pain is a concern for many children diagnosed with Cerebral Palsy, which may result from the inherent deficits associated with the condition due to spastic muscles and the stress and strain on parts of the body that are compensating for muscle abnormalities. Constant muscle tightening can affect other body part and may lead to sever pain in later years if the body does not learn to better control the movements.
The aim of this study is to investigate the feasibility of tone reducing orthotics appliances & positioning devices in order to improve joint range of motion, manage pain & to control spasticity.
Twenty children aged between 4-17 years with cerebral palsy were recruited from routine appointments in clinics. The inclusion criteria were diagnosis of Spastic CP, history of pain, and behavior ability to allow full compliance with the assessment procedures and treatment regime. Orthotics appliances & positioning devices were provided to the subjects as per the recommendations of the prescribing authority. Children with epileptic, dystonia & corrective surgeries were not the part of study. Intensity of pain was assessed by using simple descriptive Pain Intensity Scale. The variables were pain & muscle spasm.
After 180 days of fitment of positioning devices & other orthosis, the results of this study shows that in 65% (13) cases there is reduction in pain intensity up to 50%, four cases reported no change in pain & 55% (11 cases) there is reduction of spasticity. In 45% (09 cases) there is no change in muscle spasm as per modified ashworth scale. As per analysis of variance (ANOVA) pain intensity, the compared groups differ significantly, F(2,38)(ie,3.25) = 6.618, p < 0.05 & for spasm, the compared groups also differ significantly, F(2,38)(ie,3.25) = 12.287, p < 0.05. Table shows the various results in both situations from day 01 to day 180 & the null hypothesis was rejected.

Motor, cognitive and communication impairments complicate the task of appropriate pain assessment and should be considered when choosing instruments to evaluate pain. A bio-mechanical approach (to support body part) and /or neuro-physiological (to decrease spasticity) have significant role in controlling pain, improving posture, joint ROM and preventing contractures.
McKearnan, (2004) Pain In Children With Cerebral Palsy: A review. The Journal of Neuroscience Nursing, 26(5):252-259.
0294
Jinghua Tang (1) presenting Liudi Jiang (1) Dan Bader (1) Joe McCarthy (2) Richard Bradbury (2) Saeed Zahedi (2) David Moser (2)
University of Southampton, Southampton, Hampshire, UK (1) Chas A Blatchford & Sons Ltd, Basingstoke, Hampshire, UK (2)
Use of gait lab 3D motion capture for dynamic assessment of amputee socket interface biomechanics – a preliminary study
Conventional gait analysis models used in the study of amputee locomotion are based on intact skeletal structures and rigid linked segment models and analysis. However, in reality for amputee gait analysis, the stump/socket interface effectively represents an additional joint, which may adversely affect the accuracy of the results. Indeed relative movements at this interface in sagittal and coronal planes have been previously experimentally reported during level walking to yield values of up to 7° and 9°, respectively[1].
The aim of this study is to demonstrate a new linked segment model, which can be used to characterise stump/socket interface biomechanics for above-knee amputees, using a gait lab 3D motion capture system.
Gait lab measurements of an above-knee amputee fitted with an ischial containment socket performing different daily activities incorporating sit-to-stand, weight on/off, swing and walking trials (n=6) were recorded. Based on a 6-DoF marker model, a socket axis was defined and constructed from the cluster of markers located on the socket and knee joint. A stump axis was defined by the hip joint and the knee joint by convention. Relative segment axes angles were computed with respect to a standing calibration. Pistoning length was also computed as the distance between hip and knee joint.
Results from this pilot study suggested angular difference between stump and socket axes can be up to approximately 4° in the sagittal plane during the stance phase and 1° in the swing phase during level walking (Figure 1). In the coronal plane, the angle difference of up to 10° was obtained. The magnitude of relative movement at the stump/socket interface we obtained corresponds well with data from an experimental ultrasound observation[1]. Up to 30mm change in pistoning length was estimated in level walking. For other daily activities, mean values of up to 10° in sit-to-stand and 12° in swing trials were estimated.

These pilot results show that specific consideration of the socket joint motion is warranted when analysing amputee gait. Further work is required to quantify these effects in a large cohort of amputees associated with the development of alternative modelling and gait analysis approaches. This could potentially lead to a practical means for quantitative assessment of socket fit and limb control by using gait lab 3D motion capture.

Angular difference between stump/socket axis in sagittal plane (n=6)
[1] Convery; 2000 Prosthet Orthot Int
0295
Hannah Jarvis (1,2) Richard Baker (1) presenting Alex Bennett (2) Martin Twiste (1,3) Rhodri Phillip (2)
University of Salford, Salford, UK (1) Academic Department of Military Rehabilitation, Defence Medical Rehabilitation Centre, Headley Court, Epsom, UK (2) UNIPOD (United National Institute for Prosthetics & Orthotics) Development, University of Salford, Salford, UK (3)
Kinematics, kinetics and Gait Profile Score in highly functioning amputees
Operations in Afghanistan and Iraq have resulted in many UK military personnel suffering traumatic loss of limb, often with associated injuries. Gait analysis can inform rehabilitation and improve prosthesis design. Previous studies have reported large differences in the biomechanical function of amputees during walking compared to the able-bodied. Most studies report data from small cohorts who are generally older and less active than a military population, nor have they undergone an intensive rehabilitation programme such as that at the Defence Medical Rehabilitation Centre (DMRC) Headley Court. Therefore, UK military personnel may walk differently to that reported in the current literature.
The aim of this investigation is to compare the kinematics, kinetics and Gait Profile Score (GPS) during walking of amputees with different levels of amputation to that of an able-bodied cohort.
This investigation received ethical approval from the Ministry of Defence Ethics Committee and the University of Salford ethics panel. Amputees were recruited from those attending DMRC Headley Court. Participants were instructed to walk at a self selected speed for 5 minutes and three dimensional gait measurements were obtained including joint kinematics, moments and powers calculated. GPS was calculated in accordance with Baker et al [1]. All data was checked for normal distribution, and to compare between different groups a one-way ANOVA was used, with post-hoc analysis.
Ten unilateral trans-tibial (UTT), ten unilateral trans-femoral (UTF), nine bilateral trans-femoral (BTF) amputees and nine control participants gave informed consent to participate. On the prosthetic side for UTT and UTF there is reduced knee flexion during the contact phase and reduced ankle joint dorsiflexion and plantarflexion during the gait cycle compared to control. BTF demonstrated reduced hip flexion. Kinetic data was collected simultaneously and will be presented. GPS’s were statistically greater for UTF and BTF compared to control.
Comparison of Mean GPS for Intact/Prosthetic for UTT, UTF and Right/Left for BTF.

Differences statistically significant from control (<0.05)
This is one of the largest studies of amputee kinematics, kinetics and GPS data during walking. The kinematics and kinetics indicate that all amputee groups demonstrated a similar movement pattern to the control throughout the gait cycle. The GPS for amputees in this study is higher than previously reported for able-bodied individuals. However, the difference is very small and suggests in agreement with the energetic data also reported, that this cohort has high levels of function having benefitted from excellent prosthetic and rehabilitation care. We propose that this data might be used as a benchmark to compare with other groups of amputees
1. Baker, R. et al (2009) Gait Posture, 30 (3): 265-269.
0296
Hannah Jarvis (1,2) Richard Baker (1) presenting Alex Bennett (2) Martin Twiste (1,3) Rhodri Phillip (2)
University of Salford, Salford, UK (1) Academic Department of Military Rehabilitation, Defence Medical Rehabilitation Centre, Headley Court, Epsom, UK (2) UNIPOD – United National Institute for Prosthetics & Orthotics Development, Salford, UK (3)
Walking speed, oxygen consumption and cost during walking in military amputees
Operations in Afghanistan and Iraq have resulted in many UK military personnel suffering traumatic loss of limb, often with associated injuries. Amputee gait is less efficient than able-bodied gait, and the more proximal the level of amputation, the greater the effort required to walk. Previous studies suggest that unilateral trans-tibial (UTT) amputees consume 25% more oxygen during walking than the able-bodied, and this increases to 55-60% for unilateral trans-femoral amputees (UTF) [1]. Most studies report data from small cohorts who are generally older and less active than a military population, nor have they undergone an intensive rehabilitation programme such as that at the Defence Medical Rehabilitation Centre, Headley Court. Therefore, UK military personnel may walk differently to cohorts reported in the current literature.
The aim of this investigation is to compare walking speed, oxygen consumption and cost during walking of amputees with different levels of amputation to that of an able-bodied cohort.
This investigation received ethical approval from the Ministry of Defence Ethics Committee and the University of Salford ethics panel. Amputees were recruited from those attending DMRC Headley Court. Participants were instructed to walk at a self selected speed for 5 minutes and walking speed and oxygen utilisation were measured, with the last minute used for analysis. All data was checked for normal distribution, and to compare between different groups a one-way ANOVA was used, with post-hoc analysis.
Ten UTT, ten UTF, nine bilateral trans-femoral (BTF) amputees and nine control participants gave informed consent to participate. UTT, UTF and control participants walked at a similar speed whilst BTF walked significantly slower (Table 1). BTF consumed significantly more oxygen and the cost of walking was also significantly higher than control or UTT and UTF (Table 1).
Comparison of walking speed (m/s), oxygen consumption (ml/kg/min) and cost (ml/kg/m).

All entries in form: mean (standard deviation). * significantly different to control (p<0.05)
This study is one of the largest studies of amputee oxygen consumption and cost during walking to be reported. UTT and UTF amputees walked at a comparable speed, and BTF walked faster than has been reported in the literature. The cost of walking was significantly greater for BTF and UTF amputees compared to the control. The oxygen consumption and cost for all amputees were substantially less than reported previously.
1. Schmalz, T. et al. (2002) Gait Posture, 16 (3): 255-263.
0297
Piotr Laszczak (1) presenting Liudi Jiang (1) Jianliang Gao (1) Michael McGrath (1) Dan Bader (2) Joe McCarthy (3) Richard Bradbury (3) Saeed Zahedi (3) David Moser (3)
Faculty of Engineering and Environment, University of Southampton, Southampton, UK (1) Faculty of Health Sciences, University of Southampton, Southampton, UK (2) Chas A Blatchford & Sons Ltd., Basingstoke, UK (3)
Tri-axial pressure and shear (TRIPS) sensor system for stump/socket interface
The quality of socket fit has been long-recognised as an important factor affecting amputees comfort and outcome of the prosthesis. However, real-time sensory monitoring of pressures (normal to the surface) and shear stresses (tangential to the surface) at the stump/socket interface, which is appropriate for use in clinical settings, has remained a challenge in the prosthetic field.
The aim of the present work is to develop a novel tri-axial pressure and shear (TRIPS) sensor technology, which is capable of measuring dynamic stresses at the stump/socket interface.
A novel, thin and flexible sensor, termed TRIPS, was designed and extensively characterised in lab settings. Furthermore, a pilot test was performed using a trans-femoral amputee walking on a range of terrains. During the study, a single TRIPS sensor was placed at the distal end of the socket while the prosthesis was instrumented with a 6-axis load cell located at the ankle.
The developed sensor system demonstrated high repeatability and high resolution for both pressure (5kPa) and shear (2kPa), when subjected to static and dynamic loading.
The pilot tests suggest that pressure and shear stress patterns at the distal end of the socket resemble ground reaction forces (GRF), as well as forces measured with the load cell (see Fig. 1) in terms of shape and timing of peaks. Furthermore, the stresses measured with TRIPS sensor exhibit a more pronounced first peak when walking up a ramp and more elevated second peak when walking down the ramp, which follows a typical pattern of GRF.

A comparison between three directional stresses sensed with the TRIPS sensor and forces measured with the load cell.
The TRIPS sensing technology provides a method to measure three directional loads at a stump/socket interface and hence offers an enhanced insight into the dynamic nature of socket loading. To-date, results suggest feasibility of use of the TRIPS sensors, and indicate good agreement with theory, as well as supplementary instrumentation using a load cell. Accordingly, the sensors exhibit potential for quantification of socket fit and in the future could provide an objective assistive tool and monitoring system for clinicians as well as amputees.
0298
Michael McGrath (1) presenting Jianliang Gao (1) Jinghua Tang (1) Piotr Laszczak (1) Liudi Jiang (1) Dan Bader (2) David Moser (3) Joe McCarthy (3) Richard Bradbury (3) Ana Gallego (3) Saeed Zahedi (3)
Faculty of Engineering and the Environment, University of Southampton, Southampton, UK (1) Faculty of Health Sciences, University of Southampton, Southampton, UK (2) Chas A. Blatchford & Sons Ltd, Basingstoke, UK (3)
A lower-limb stump/socket interface simulator to aid assessment of clinical interventions
Socket fit is integral to stump health[1], with expert knowledge being required to make necessary adjustments. However, to-date, there is a lack of effective tools to assist prosthetists with their assessments. Interfacial loads between the stump and socket are an important factor which can be potentially affected by many variables e.g. alignment, liner choice etc. The ability to assess these effects in a lab setting would be advantageous.
To design, build and optimise a stump/socket interface simulator, which can be used to assist clinical investigations and enable training in a laboratory setting.
A 6-axis load cell was integrated into a lower-limb prosthesis and reference gait data was collected from a below-knee amputee. A laboratory-based apparatus was constructed, incorporating the 6-axis load cell and an anatomically-shaped, artificial stump, made from rigid bones encased in silicone. The apparatus was constructed and tuned with a view to reproducing the load cell readings recorded in the amputee’s gait session, thus mimicking stump/socket interface performance. Stress sensors, recently detailed in ref [2], were placed at the stump/socket interface and their values were compared to those reported in previous clinical-based studies.
Figure 1 shows the constructed simulator with its key components. The simulator can be set up in two orientations in order to replicate the load-intensive phases of the walking cycle i.e. loading response and heel-rise, respectively. The 6-axis load cell readings obtained from the simulator matched the reference data well, implying a good representation of amputee walking cycles. Interfacial loads at a series of stump locations e.g. patellar tendon, popliteal fossa, fibular head etc. were obtained using the simulator, which correlated well with those previously reported[1, 3].

A photo of the stump/socket simulator in the loading response setup
The results showed that the simulator provided a robust simulation of the stump/socket interface conditions during walking. It is envisaged that the developed simulator could be used to assess the long term effects of clinical interventions in a relatively short time frame as well as providing further insights at the critical stump/socket interface. As a result, it could be potentially used to help clinicians evaluate the quality of a socket fit as well as identify stump locations at risk of tissue breakdown.
[1] Sanders; 1997 J Rehabil Res Dev
[2] Laszczak; 2014 Med Eng Phys
[3] Zahedi; 2001 ATLAS of Prosthetics
0299
Emma Tebbutt (1) presenting Vennila Palanivelu (1) Ritu Ghosh (1)
Mobility India, Bangalore, India (1)
An evaluation of Indian and Nepali graduates from a mid-level therapist program, focusing on: graduate’s skills; professional development; and the impacts on service users
Globally, there is a lack of rehabilitation professionals and graded levels of training are required to increase provision1. Existing training programs do not focus on community based rehabilitation (CBR). To address this need, an Indian training organization developed a one year mid-level therapist (MLT) program in 2002. 136 Students from nine countries in South Asia and Africa have graduated, presenting an opportunity to evaluate the graduates and provide evidence for all stakeholders.
To improve the training of MLT through gaining an understanding of:
1. the MLT work setting and caseload
2. MLT skills and his/her professional development needs
3. changes in the lives of service users (SU) as a result of MLT intervention.
A mixed methods (qualitative and quantitative) approach was used. 26 graduates working in different settings within 16 organizations in India and Nepal were evaluated. Supporting data was gathered from 25 of the MLT supervisors and 23 of their SU. Each evaluation included:
MLT
questionnaire and follow-up interview, focusing on clinical practice and professional development
review of clinical records
case presentation, including demonstration of therapy techniques.
SUPERVISOR
questionnaire relating to MLT competencies.
SERVICE USER
semi-structured interview about his/her rehabilitation experience and life changes in activity/participation resulting from the intervention.
Consent was obtained from all study participants.
Most MLT work for non-governmental organizations in a CBR or mixed CBR/institution-based setting. They treat diverse conditions in children and adults. MLT are working across all areas of the CBR matrix, from awareness programs to National Paralympic competition, although therapy interventions were often impairment focused.
Most MLT overall skill level was at or above the expected standard and three MLT have been promoted to project manager roles. Supervisor/SU feedback was almost all positive, especially in relation to communication with SU. Most MLT records were below expectation, with lack of detail and inadequate goal setting.
All SU were satisfied with MLT intervention, giving examples of changes at the activity and participation levels, although they had poor understanding about their conditions and prognosis.
MLT identified specific training needs across diverse areas. Nepalese MLT raised the issue of professional status, as their qualification is not yet recognized, and this absence of professional status causes perceived lack of respect from other professionals, barriers to career progression and retention problems.
The evaluation produced a clearer picture of graduates’ activities, skill level and development needs, as well as SU experiences. This information will inform curriculum development, priorities being; record keeping and goal setting; more focus on interventions at the activity and participation level; and educating SU about diagnosis and prognosis.
Further evaluation of SU would be interesting; to understand which therapy interventions and CBR activities have most impact.
1. World Report on Disability. World Health Organization 2011
301
Jianliang Gao (1) presenting Michael McGrath (1) Piotr Laszczak (1) Jinghua Tang (1) Liudi Jiang (1) Dan Bader (1) David Moser (2) Joe McCarthy (2) Richard Bradbury (2) Saeed Zahedi (2)
University of Southampton, Southampton, UK (1) Chas A Blatchford & Sons Ltd, Basingstoke, UK (2)
Assessment of alignment effects on stump/socket interface and socket reaction moment using a lower-limb prosthetic simulator
Prosthetic alignment is important to ensure functions and outcomes of lower limb prostheses [1]. However, there are relatively few studies on the effect of alignment changes on both socket moments and the loading at the stump/socket interface. A recent study in clinical settings illustrated the effect of socket alignment changes on socket reaction moments [2]. Nevertheless, a scientific and systematic apparatus is required to assess prosthetic performance in a repeatable and reproducible test. This motivated the design and building of a lower-limb stump/socket simulator.
To assess stump/socket interface stresses and socket reaction moments based on perturbation of socket alignment, using a lower-limb prosthetic simulator in a laboratory setting.
Stress sensors [3] were deployed in load bearing regions at the stump/socket interface using a lower-limb prosthetic simulator. A 6-axis load cell was incorporated beneath the socket to measure sagittal and coronal forces and moments. Tests were performed on the simulator by changing the angular and translational alignment from the nominal alignment of the socket in both sagittal and coronal planes. To replicate clinical events, every change of alignment was tested with 3 separate cycles representing heel-strike, mid-stance and heel-rise to incorporate critical features of the stance phase of gait.
Figure 1 shows example simulator settings for performing the tests on nominally aligned and malaligned sockets about angulations in coronal plane. The alignment effects were studied by implementing multiple angular (up to 6°) and translational (up to 10mm) changes from the nominal alignment, respectively. The results revealed that sagittal malalignment of the socket had more complex effect on stump/socket interface stresses and socket reaction moments than coronal malalignment. Furthermore, the observation suggested that the effect of socket malalignment at the heel-strike event was different from that at the mid stance and heel-rise events in a gait cycle. The results were analysed and compared with published clinical data [2].

Posterior views (coronal plane) of simulator settings at the heel-strike event. (a) malalignmnet toward lateral side. (b) nominal alignment. (c) malalignment towards medial side.
This study illustrated the alignment effects on stump/socket interfacial stress and socket reaction moments in both sagittal and coronal planes. The developed methodology can potentially be used to provide quantitative assessment of malalignment on a lower-limb prosthesis. This study will potentially generate a guide for clinicians to adjust the alignment of prostheses for patients, in particular, the new wearers.
[1] Zahedi; 1986 JRRD.
[2] Kobayashi; 2013 J. of Biomechanics.
[3] Laszczak; 2014 Med Eng Phys.
302
Bob Giesberts (1) presenting Floor Maten (1) Eline Kolk (4) Edsko Hekman (1) Arjen Bergsma (3,1) Bart Verkerke (2,1)
University of Twente, Enschede, The Netherlands (1) University of Groningen, Groningen, The Netherlands (2) Radboud University Nijmegen, Nijmegen, The Netherlands (3) Coventry University, Coventry, UK (4)
Development of a lower leg prosthesis for a mobile workshop in rural Indonesia
Indonesia has a limited number of prosthetic and orthotic workshops, most of them are situated on Java Island. The time involved in obtaining a prosthesis includes travel time (often multiple days) and production time (typically two weeks). Only a few users can afford the costs for travel, food and accommodation while at the same time missing several weeks’ worth of income. A prosthesis which can be fabricated locally will reduce financial burden for the user.
To design a lower leg prosthesis that can be produced in a mobile workshop in the rural areas of Indonesia.
Inspired by the minimal equipment required for production of the Zwolle Isala Prosthesis (ZIP; OIM, The Netherlands) a concept was developed in close cooperation with prosthetic experts from workshops in North-Sumatra, Jakarta and Bali. In the concept a synthetic cast tape (Delta Cast Prints; BSN Medical, Germany) is wrapped around a corrected plaster cast of the stump to create a PTB socket. With EVA-foam a liner is formed around the same cast. Standard components from the International Committee of the Red Cross (ICRC) and locally produced feet are used to complete the prosthesis. Twelve volunteers who already had a proper prosthesis evaluated prototypes at their own discretion
The resident prosthetists were able to produce the prostheses within a day without requiring any heavy or bulky equipment. This makes it reasonable to assume that the production process is suitable for use in a mobile workshop, but according to prosthetists the quality of the prosthesis can still be improved. A follow-up after one year revealed damage to the cosmetic cover (not in the image) without any apparent structural damage and all four interviewed users indicated to use the new prosthesis for longer periods of time than they did with their old one.

303
Dimitrios Sokratis Komaris (1) Stephanos Solomonidis (1) presenting
University of Strathclyde, Glasgow, UK (1)
Investigation of Bench Methods for Determining Stiffness of Solid Ankle-Foot Orthoses
The prescription of ankle-foot orthoses (AFOs) is one of the most common and effective treatments for the compensation of neuromuscular disorders (Bregman et al., 2010). The biomechanical function of plastic AFOs is determined by their thickness, the material selection and their trim-line. Their design, however, is mainly empirical due to a lack of evidence-based research on their geometrical characteristics (Papi, 2012). Therefore, experimental data are critical for the optimization of AFOs’ characteristics.
This project aimed to investigate the different experimental methods currently utilized for determining the stiffness of polypropylene AFOs. The experimental procedure had two aims: to fabricate an artificial leg suitable for the stiffness testing of an AFO, and to measure the stiffness of an AFO with/without the presence of the leg by means of different stiffness-measuring methods.
The strengths and weaknesses of eight bench testing methods were analysed and two different techniques were implemented: the mechanical test by Major et al. (2004) in the Instron E10000 (Fig. a) and the bending test by Ross et al. (1999) in a custom-made rig (Fig. b). Three AFOs were tested in total: a 4.6mm black co-polymer solid AFO (4.6BCP), a 6mm homo-polymer solid AFO (6HP) and a 4.6mm co-polymer solid AFO with carbon fibre shape corrugations (4.6CP).

The table below demonstrates the different dorsiflexion angles when a moment of 20Nm about the ankle joint was applied. During the Instron test and when the same moment was applied, adopting the equations that were described by Major et al., an error equal to 1.05° was found when the distance between the lower jig and the medial malleolus prominence of the 4.6BCP AFO and the distance connecting the medial malleolus and the upper jig were considered as constants.

The difference in stiffness when the leg is used is noteworthy and it is suggested that results of a study using a leg cannot be compared with similar studies testing isolated AFOs. As suggested by Ross et al., colour additives in the polypropylene sheets will affect the stiffness of the AFO. The difference between the methods is also considerable; it is believed that this variation is due to the creep sensitivity of the manual methods and thus the AFO seems to be more flexible when measured manually. The mathematical data processing of the Instron testing existing in the literature (Major et al., 2004) was found to be imprecise and it is recommended that a camera system (e.g. Bluehill software) should be used to measure the deformations of the AFOs.
[1] Bregman et al., Prosthet Orthot Int, 34(3), 293-304, 2010.
[3] Major et al., Prosthet Orthot Int, 28(1), 44-48, 2004.
[4] Papi, Ph.D thesis, University of Strathclyde, 2012.
[5] Ross et al., Prosthet Orthot Int, 23(1), 63-71, 1999.
305
Marko Markovic (1) presenting Strahinja Dosen (2) Dario Farina (2)
Otto Bock HealthCare GmbH, Duderstadt, Germany (1) University Medical Center Göttingen, Dep. of NeuroRehabilitation Engineering, Göttingen, Germany (2)
Environment aware hand prosthesis: A new paradigm for dexterous control
Controlling multifunctional upper limb prostheses with the conventional myoelectric man-machine interface requires switching between the degrees of freedom in a sequential order, and thus it is cumbersome and slow. We have previously developed a system for semi-autonomous control of upper limb prostheses based on computer vision [1]. Here we advance the concept further by fusing additional sensory information in order to extend the overall system applicability.
The ultimate goal of this research is to simplify the control of a multiple degree-of-freedom prosthesis by endowing the artificial controller with the ability to sense the external environment and make autonomous decisions such as appropriate wrist rotation or grip selection.
The system comprises: 1) Creative Senz3D camera (Creative Technology Ltd.) mounted on the user’s head, implementing the image acquisition, 2) Michelangelo hand prosthesis with a wrist rotator and two 13E200 dry EMG electrodes (Otto Bock Healthcare), and 3) a single MTx inertial sensor (Xsens Technologies B.V.), placed on the prosthesis wrist, for tracking of the 3D prosthesis orientation. When triggered by the user, the system fuses the data acquired from the head-mounted-camera and inertial sensor in order to automatically identify the optimal prosthesis posture (i.e., preshape and orientation) for the given task. It should be noted that, at any moment in time, the user is still able to employ full myoelectric control (semi-autonomous control).

We have evaluated the system in one amputee subject, which was experienced (35 years) and active prosthetic user. After a short introductory session the subject was able to fully understand and employ the presented semi-autonomous control scheme (as depicted in the picture). Additionally, we have designed a custom test to compare the performance of our semi-autonomous to the conventional myoelectric control scheme. The test consisted of 15 grasping trials in which the subject had to employ different hand postures in order to successfully grasp the object. In this test the subject was 40% faster when using the semi-automatic control (on average 6.1±1.7s and 10.5±2s needed to grasp the object in semi-automatic and conventional control scenarios, respectively).
We have demonstrated how an artificial controller can be enriched with an additional, non-conventional information source (vision and inertial sensors) and a high level processing (cognitive-like reasoning) to achieve fully automatic control of both prosthesis preshaping and rotation. Therefore, high-level tasks can be accomplished automatically, which decreases the cognitive burden from the user, with the final goal of making grasping a routine, effortless activity.
[1] Markovic, M., et al. (2014). Stereovision and augmented reality for closed-loop control of grasping in hand prostheses. Journal of Neural Engineering, 11(4), 046001.
306
Sebastian Amsuess (2) presenting Peter Göbel (2) Michael Russold (2) Oskar Aszmann (3) Dario Farina (4) Bernhard Graimann (1)
Otto Bock HealthCare GmbH, Duderstadt, Germany (1) Otto Bock Healthcare Products GmbH, Vienna, Austria (2) Medical University Vienna, Christian Doppler Lab for Restoration of Extremity Function, Vienna, Austria (3) University Medical Center Göttingen, Dep. of NeuroRehabilitation Engineering, Göttingen, Germany (4)
Improved dexterity of transradial prostheses by movement context dependent control
Transradial upper limb amputations constitute severe impairments. In order to alleviate the effects of such trauma, sophisticated multifunctional hand prostheses have been developed. A variety of advanced control strategies, most of them based on surface EMG, have been proposed for suitable control of these devices. These approaches can be categorized into classification and regression techniques. While each of these categories exhibits particular strengths, they also have their drawbacks in certain movement control aspects.
To develop and evaluate a new algorithm for intuitive, simultaneous and proportional control of multifunctional hand prostheses. This algorithm should combine classification and regression techniques in a context dependent way and thus providing either coarse hand positioning or fine object manipulation.
Surface EMG signals from 8 electrode derivations were recorded in 6 healthy and 2 transradial amputee subjects while performing the following (phantom) limb movements: wrist pro/supination, wrist flexion/extension, hand open, tripod pinch, lateral grip, and rest - individual movements only. A linear regression (LR) model was trained on the four wrist movements, allowing for simultaneous and proportional combination of these. Additionally, a proportional classification (PC) method was trained with all 8 classes, allowing for precise single movement actuations. Either LR or PC was selected for each movement based on the distance to the training data.
We propose to intelligently combine regression and classification approaches for surface EMG signals. This combination facilitated simultaneous, proportional control and fine grained precise movement estimations. The quantitative results obtained from tests with able-bodied and amputee subjects, performing online physical tasks with real prostheses, demonstrated that the proposed system outperformed previous state of the art control in transradial prostheses. The seamless fusion of algorithms enabled prosthetic users to intuitively control a complex hand prosthesis.
307
Thomas Schmalz (2) presenting Andreas Samson (1) Herman Boiten (1)
Otto Bock HealthCare GmbH, Duderstadt, Germany (1) Otto Bock Competence Center Göttingen, Göttingen, Germany (2)
Results of biomechanical tests during running with a hydraulically controlled sports prosthesis
In the past years, the development of paralympic sports has been pushed by the athletes’ increasing professionalism and by continuously improved prosthetic components specifically designed for top level competitive sports. These components are not always suitable for leisure, non-competitive sports activities. To date, the growing desire of transfemoral amputees to include running in their sports activities has not been satisfied sufficiently. Now, this discrepancy is considerably reduced by a newly developed sports prosthesis system.
The article presents the results of first biomechanical tests with the new system. The tests aim to define more exactly the possibilities and the limitations for users with different physical conditions.
Components of the sports prosthesis are the 3S80 knee joint (rotary hydraulics without stance phase stability) and the 1E90 sports foot (Ottobock, Germany). The prosthetic alignment was adjusted according to the manufacturer’s instructions. Nine unilateral sports prosthesis users (5 x TF, 4 x KD; 29 ± 10 years; 181 ± 6 cm, 82 ± 14kg) participated in the tests. The study was performed on a 12m walk way in a biomechanics laboratory. After warm-up, the biomechanical data of at least 6 single trials with self-selected running velocity were recorded. The ground reaction forces were measured by means of a force plate (9287A, KISTLER, Winterthur, CH), kinematic measurements were taken with an optoelectronical camera system (12 Bonita cameras, VICONPEAK, Oxford, GB). Based on the kinematic data and the ground reaction forces the joint moments of the lower limb were calculated.
After a short adaptation phase, every runner was able to perform the tests in the lab situation (mean velocity 2.9 ± 0.4 m/s). Comparing the sound and prosthetic sides, the mean maximum of the vertical force on the prosthetic side was higher than on the sound side (270 vs. 258 %BW). The mean horizontal forces on the prosthetic side were lower than on the sound side, both for the minimum (early support phase, -17 vs -28 %BW) and the maximum (late support phase, 24 vs 28 %BW). Over the whole support phase, high external knee extension moments were found on the prosthetic side (mean maximum value 1.70 ± 0.38 Nm/kg). The periodic sequence of flexion and extension moments during the support phase known from non-amputees was seen in the sound limb knee joint of each runner. The mean maximum knee flexion angles amount to 87.7 ± 3.7° (prosthetic limb) and 91.7 ± 15.4° (sound limb).
The tests confirm that the alignment recommendations for the prosthetic system guarantee a high level of safety during the support phase in running. Safety is also supported by the swing phase control of the 3S80 that allows for a flexion angle of nearly 90° independently of the level of physical capabilities of the athlete. As the biomechanical parameters of the sound limb largely correspond to that of non-amputees [1], it can be concluded that the stress to the locomotor system during jogging with a sports prosthesis is not considerably higher than that of non-amputated runners. The missing yielding function, however, prevents this system from being suitable for sports that are associated with knee flexion moments.
[1] Wank et al.: Leistungssport 28 (1998) 1, 48-53.
308
Thomas Schmalz (1) presenting Heiko Drewitz (1) Kerstin Stöcker (2)
Otto Bock Competence Center Göttingen, Göttingen, Germany (1) German Sport University Cologne, Institute of Biomechanics, Cologne, Germany (2)
The use of an AFO as an innovative method within the scope of the conservative treatment of osteoarthritis of the knee
The use of KOs and KAFOs is an established treatment option for patients with osteoarthritis (OA) of the knee and their biomechanical effects and clinical benefits have been demonstrated in numerous studies. However, due to the somewhat difficult handling of the orthoses, their acceptance by patients is compromised. Therefore, an alternative orthotic treatment concept using an innovative AFO has been developed with the goal to improve patient compliance.
The aim of this study was to investigate the biomechanical effects of the AFO in sound subjects and patients with knee OA as well the pain reduction in the patients after 2-week use.
The tests were performed with the AFO Agilium Freestep (Ottobock, Germany). First, sound subjects (n=20) and patients with OA of the knee (n=12, OA stage 2-3 on the KELLGREN scale) were investigated during level walking with and without the orthosis. For the measurements, an optoelectronic camera system (27 passive markers, 12 Bonita cameras, VICONPEAK, Oxford, GB) coupled to two force plates (9287A, KISTLER, Winterthur, CH) was used. The 3D kinematics of the ankle and knee joint and the external joint moments were used as specific evaluation parameters. After having used the orthosis for two weeks, the patients assessed their pain during level walking and walking on stairs on a 10 point NAS scale.
The time-distance- parameters of the two walking situations did not show any significant differences. With the orthosis, the first maximum of the varus moment acting on the knee joint is significantly decreased (p≤0.01) from 0.47 to 0.36 Nm/kg (sound subjects) and from 0.67 to 0.56 Nm/kg (patients). The difference between the knee joint varus deviations at initial contact and at the maximum of the varus moment was not significant in both situations. With the orthosis, the lateralization of COP, i.e. the distance between the centre of pressure (COP) of the ground reaction force (GRF) and the foot length axis during the maximum of the varus moment was significantly increased. This increase was from 7.5 to 17.2 mm (sound subjects) and from 7.3 to 19.7 mm (patients; p≤0.01). This effect correlates with a reduction of the lever arm between the acting GRF and the knee centre by 6.9 (sound subjects) and 11.0 mm (patients, p≤0.01). After two weeks of use, the patients reported significant pain reduction from 7.3 to 2.7 (level ground; p≤0.01), from 8.3 to 3.9 (descending stairs; p≤0.01) and from 7.0 to 2.4 (ascending stairs; p≤0.01).
The biomechanical relief of the knee by the AFO primarily results from a lateralization of the COP. This is due to the rigid bridging of the subtalar joint by the orthosis, resulting in a reduction of foot eversion that causes a shift of the COP [1]. Based on the reduction of the varus moment, a joint relief between 24% (sound subjects) and 16% (patients) has been seen that corresponds to the effect of KOs and KAFOs[2]. This biomechanical effect may explain the remarkable pain reduction in the patients and considerably increases the patient’s acceptance compared to KOs and KAFOs.
[1] Lugade and Kaufmann, Gait Posture 40 (2014).
[2] Pollo et al., Am J Sports Med 30 (2002)3.
309
Thomas Schmalz (1) presenting Malte Bellmann (1) Eva Pröbsting (1) Siegmar Blumentritt (2,3)
Otto Bock Competence Center Göttingen, Göttingen, Germany (1) Otto Bock HealthCare GmbH, Duderstadt, Germany (2) PFH Private University of Applied Science, Göttingen, Göttingen, Germany (3)
Effects of adaptation to a lower limb prosthetic component with new functionality
Biomechanical tests are important for learning to which extent technical developments of prosthetic components may provide additional benefits to the patient. For the methodology of these studies, it is important to know what period of accommodation to new components is required before performing these assessments. In the literature, the length of the adaptation period required to allow for meaningful biomechanical diagnostics is controversial (e.g. [1], [2]).
The present study investigated the adaptation effects observed in TF amputees that had been fitted with a new prosthetic knee joint. The results of the tests performed in ADL situations in two assessment sessions (immediately after fitting and after 3 months of use) are discussed.
Ten unilateral transfemoral amputees (35±10 y, 181±4 cm, 82±12 kg; etiology of amputation: 9 x trauma, 1 x tumour, MG3 to MG4) who had been using a C-Leg (Ottobock, Germany) were enrolled in the study. At baseline, they were fitted with the GENIUM microprocessor-controlled knee joint (Ottobock, Germany). After 7 to 8 hours of use, the first biomechanical assessments were performed in the laboratory (T1): level walking (3 velocities) and walking on ramps and stairs (ascent and descent). Then the patients used the prosthesis for 3 months in their home environment before undergoing a follow-up assessment with the exact same test battery (T2). For the motion capture, an optoelectronic camera system (VICONPEAK, Oxford, GB) coupled with two force plates (KISTLER, Winterthur, CH) was used. Details of the measurement techniques have been reported elsewhere [3].
Level walking at all three velocities did not show any significant differences in the biomechanical parameters between T1 and T2. Walking on ramps, both descending and ascending, was characterized by only slight differences between T1 and T2. The peaks of the biomechanical parameters did not demonstrate any significant differences. For descending stairs step over step, no significant differences were found for the individual parameters between T1 and T2. Important changes between T1 and T2 were seen only in ascending stairs step over step. The inter- and intra-individual variability of test results was considerably higher at T1 than at T2.
The results of the study show that established TF amputees may intuitively utilize the functions of a new prosthetic component after just a few hours of adaptation if the motion pattern required for a given movement is similar to that with the previous component. In such movements or activities, biomechanical tests for functional comparisons between components can be performed after only a short period of acclimatisation. In motion patterns that necessitate motor learning with the new component, objective tests to assess important differences require a longer adaptation and learning period. The present results suggest that a 3-month acclimatisation period may be appropriate.
[1] English et al.: J Rehabil Res Dev 32 (1995) 1, 32-35.
[2] Hafner et al.: Arch Phys Med Rehabil 88 (2007), 207-217.
[3] Bellmann et al.: Arch Phys Med Rehabil 91 (2010), 644-652.
[4] Blischke et al.: Augmented skill in motor skill acquisition. In Psychology for Physical educators. Ed.: VandenAuweele, Y., Bakker, F., Biddle, S., Durand, M., Seiler, R.: Human Kinetics, Champaign, Il, 1999.
310
Aurélie Vouilloz (1) presenting Philippe Vuistiner (1) Christine Favre (1) Yvan Arlettaz (3) Mathieu Assal (4) Olivier Borens (5) Isabelle Loiret (2) Noël Martinet (2) Jean Paysant (2) Vanessa Buhlmann (1) François Luthi (1)
Clinique romande de réadaptation, Sion, Switzerland (1) Institut régional de médecine physique et de réadaptation, Nancy, France (2) Hôpital de Martigny,réseau santé Valais, Martigny, Switzerland (3) Clinique de la Colline, Genève, Switzerland (4) Centre hospitalier Universitaire Vaudois, Lausanne, Switzerland (5)
Cross-cultural adaptation, reliability, internal consistency and validation of the Amputation Body Image Scale (ABIS) for French speaking patients with lower limb amputation
The aim of this study was the French cross cultural adaptation and validation of the ABIS (ABIS-F) and its shortened version ABIS-R (ABIS-R-F).
129 patients (23% women), with a mean age of 62 years, with lower limb amputations for at least 1 year (vascular 75%, traumatic 25%) were recruited in 5 clinical centers. Translation and cross-cultural adaptation (ABIS 20 items; ratings of 1-5; high score indicating high body disturbance, and ABIS-R 14 items, ratings of 0-2) were made according to international guidelines. Internal consistency was calculated by the coefficient of Cronbach. Test-retest reliability was assessed by intraclass correlation in a subgroup of who completed the ABIS on 2 occasions with an interval of 5 to 7 days. Construct validity was estimated through correlations with SF-36 mental component summary (MCS) and SF-36 physical component summary (PCS). Correlations were also calculated with some scales of the Brief Pain Inventory (BPI): pain severity, highest pain and pain interference with activities.
The internal consistency is high (α=0.91 ABIS-F, α=0.90 ABIS-R-F) and satisfying for clinical use. Test-retest reliability was very good for ABIS at 0.87 (95% CI 0.69-0.95) and for ABIS–R at 0.86 (95% CI 0.66-0.94). Correlations with SF-36 were negative for both ABIS questionnaires. More precisely, for SF-36 PCS, they were of -0.40 (CI -0.54 to -0.21) and -0.42 (CI -0.56 to -0.24) with ABIS-F and ABIS-R-F; for SF-36 MCS, they were of -0.40 (CI -0.54 to -0.21) and -0.44 (CI -0.58 to -0.26) with respectively ABIS-F and ABIS-R-F. Correlations with pain were positive for both ABIS questionnaires: respectively for ABIS-F and for ABIS-R-F: pain severity, 0.39 (CI 0.20-0.54) and 0.38 (0.19-0.53): highest pain, 0.39 (CI 0.20-0.54) and 0.39 (CI 0.20-0.54): interference with activities, 0.53 (CI 0.36-0.65) for both. There were no floor or ceiling effects.
The ABIS-F and the ABIS-R-F have the same good psychometrics properties as the original ABIS and ABIS-R (internal consistency, test retest reliability, divergent validity with SF-36, convergent validity with BPI and no floor or ceiling effects) and they could be applied with confidence in patients with lower limb amputation. The ABIS-R-F (the shortened version) is as reliable as the ABIS-F (the longer version) and could be used instead of it with confidence in patients with lower limb amputation.
1. Holzer L. 2014. PlosOne
2. Gallagher P. 2007. Am J Phys Med Rehabil
312
Lauren Flaherty (1) Cristy Wilson (1) Kylie Mines (1) Ipul Powaseu (2) Mary Ikupu (2) Almah Kuambu (3) Dinuk Jayasuriya (4) Lee Brentnall (1) presenting
Motivation Australia, Adelaide, South Australia, Australia (1) PNG Assembly for Disabled Persons, Port Moresby, Papua New Guinea (2) PNG National Orthotics and Prosthetics Service, Port Moresby, Papua New Guinea (3) Australian National University, Canberra, ACT, Australia (4)
Barriers and facilitators of equitable access to mobility services in Papua New Guinea
The number of people experiencing mobility difficulties in Papua New Guinea (PNG) who do not have access to an appropriate mobility device exceeds the number of appropriate devices available. To achieve sustainable and equitable services, it is necessary to understand current requirements of individuals with mobility difficulties and factors contributing to acquiring appropriate mobility devices. This research is the first in PNG to focus on barriers and facilitators to accessing an appropriate mobility device services.
To investigate the barriers and facilitators that exist in relation to accessing appropriate mobility device services for people with a mobility disability in PNG.
A participatory mixed methods approach was applied. A total of 112 women, 104 men and 62 parents of children with a mobility disability completed questionnaires that included both closed and open ended questions. Questionnaires were administered by people with disabilities and participants were selected from four provinces of PNG where mobility device services exist. Six focus groups were conducted in two of the target provinces, using the findings from the quantitative data to identify discussion points. Focus group participants were randomly selected from those who completed the questionnaire. Summary statistics of the quantitative data was analysed and a thematic content analysis was conducted for the qualitative data.
Overall 57% of participants with a mobility device stated it was hard or very hard to get a device. Common barriers related to lack of information and awareness, and lack of financial resources. However, key differences were noted between groups. People aged over 50 experienced the highest level of difficulty accessing mobility services. Two of the top three barriers identified for this group were related to sociocultural issues: being undervalued and lack of family support. Gender related violence and safety was the most common barrier for women accessing services. Further, while there were several facilitators identified for men, no facilitators were identified for women or people aged over 50. Participants recognised the value of being able to access consistent, local mobility device services and felt it was the PNG Government’s responsibility to provide them.
Some of the practical barriers identified through this research can be addressed through various means. Following the project research participants were involved in creating awareness raising resources to be used across PNG. The social barriers however require a more systemic approach to overcome and consideration of the vulnerable groups of women and older people must be considered when designing mobility services in PNG to ensure equitable access to appropriate devices for all.
313
Cleveland T. Barnett (1) presenting Natalie Vanicek (3) David F. Rusaw (2)
Nottingham Trent University, Nottingham, UK (1) Jönköping University, Jönköping, Sweden (2) University of Hull, Hull, UK (3)
Does postural control predict falling and the fear of falling in lower limb amputees?

[1] Vrieling A et al. Gait Posture 2008; 28; 222-8.
[2] Miller WC et al. Arch Phys Med Rehabil 2001; 82(8); 1031-7.
[3] Yardley L et al. Age Ageing 2005; 34(6); 614-9.
315
Qian Wang (1,2) presenting Meng Li (1) Hassan Beygi Beygi (1) Edmond Hok-Ming Lou (3) Chengqi He (2) Ming Zhang (1) Aaron K.L. Leung (1) Man-Sang Wong (1)
Interdisciplinary Division of Biomedical Engineering, The Hong Kong Polytechnic University, Hong Kong, China (1) Center of Rehabilitation Medicine, West China Hospital, Sichuan University, Chengdu, China (2) Department of Surgery, Glenrose Rehabilitation Research Centre, University of Alberta, Edmonton, Canada (3)
Validation of 3-D Clinical Ultrasound Assessments to Scoliosis
The assessment of adolescent idiopathic scoliosis (AIS) can be enhanced with a comprehensive imaging technique to reveal the three-dimensional (3-D) deformities. The recent advancements of 3-D clinical ultrasound (3-D CUS) enable the 3-D reconstruction of spinal images and assessment of spinal curvatures and vertebral rotations in various anatomical planes that could not be accomplished previously. This study is to validate this 3-D CUS technique with Magnetic Resonance Imaging (MRI) measurements.
This study aims to investigate the reliability & validity of using 3-D CUS to assess scoliotic spines in a 3-D approach.
Twenty-four female subjects (10 normal and 14 with moderate AIS) were recruited. The ultrasound examinations were performed using a 3-D ultrasound unit with a SonixGPS system (Ultrasonix Ltd., Canada) while the MRI examinations were accomplished using a 3.0T MR scanner (Philips Ltd., Netherlands). The center of laminae (COL) method was used to measure the spinal curvature in the coronal plane and the apical vertebral rotation in the transverse plane. The spinous process angle (SPA) method was applied to evaluate the spinal curvature in the sagittal plane. Two researchers were involved in data collection and they did the same procedures in ultrasound scanning and measurements after 3-D image reconstructions for all the subjects. The intra-class correlation coefficient (ICC) was used to assess the reliability of measurements, and the Pearson bivariate analysis was applied to assess the correlation between the 3-D CUS and MRI measurements. The Bland-Altman plot was used to examine the agreement between these two sets of measurements. The level of significance was set as 0.05.
The COL method showed high intra-observer and inter-observer reliabilities (both with ICC>0.9, p<0.001) to measure the spinal curvature in the coronal plane and the apical vertebral rotation in the transverse plane. The SPA method presented high intra-observer and inter-observer reliabilities (both with ICC>0.9, p<0.001) to evaluate the kyphosis and lordosis angles in the sagittal plane. In the 3 anatomical planes, the Pearson’s correlation coefficient (r) was high between the 3-D CUS and MRI measurements (r>0.75, p<0.001), and the results of Bland-Altman plots demonstrated an agreement between the 3-D CUS and MRI measurements.
This study showed that 3-D CUS appears to be a reliable and valid method for measuring the spinal curvatures in the coronal and sagittal planes, and the apical vertebral rotation in the transverse plane. To further validate the proposed 3-D ultrasound technique, continuous studies have been initiated to recruit more subjects with different curve severities.
317
Stefania Fatone (1) presenting Michael Dillon (2) Rebecca Stine (3) Robert Tillges (4)
Northwestern University, Chicago, IL, USA (1) La Trobe University, Bundoora, VIC, Australia (2) Jesse Brown VA Medical Center, Chicago, IL, USA (3) illges Certified Orthotic Prosthetic Inc, Maplewood, MN, USA (4)
Coronal plane socket stability during gait in persons with transfemoral amputation: Pilot study
Despite the prevalence of transfemoral amputation (TFA), surprisingly little research describes which transfemoral socket design features are important during gait. Particularly relevant for persons with TFA is the stability between the socket and residual limb in the coronal plane during walking. Since the introduction of the ischial containment (IC) socket and more recent variants such as the Marlo Anatomical Socket (MAS) [1], experts have debated the relative contribution made to coronal plane stability by soft tissue loading and containment of the ischium [2–5].
Our study objectives were to (1) relate socket comfort during gait to a rank order of changes in IC and tissue loading and (2) compare socket comfort during gait when tissue loading and IC were systematically manipulated.
A MAS test socket with a removable IC component and removable panels that allowed tissue compression on the medial aspect of the residual limb, inferior to the ischial level, to be systematically altered was fabricated for each subject. Six randomly assigned socket conditions (IC and tissue compression) were assessed using gait analysis: (1) IC and high, (2) IC and medium, (3) IC and low, (4) no IC and high, (5) no IC and medium, and (6) no IC and low.
Six subjects age 35-81 years with long-term unilateral transfemoral amputation of nonvascular etiology and relatively long residual limbs participated in this study. All subjects wore the MAS as part of their normal prosthesis prior to the study. There was a strong negative relationship between comfort and changes in IC and tissue loading (rho = -0.89). With the ischium contained, tissue loading did not influence socket comfort (p = 0.47). With no IC, the socket was equally comfortable with high tissue loading (p = 0.36) but the medium (p = 0.04) and low (p = 0.02) tissue loading conditions decreased comfort significantly. Coronal plane hip moments, lateral trunk lean, step width, and walking speed were invariant to changes in IC and/or tissue loading.
The results of our pilot randomized cross-over study suggest that socket comfort may be achieved with a variety of transfemoral socket geometries. In an IC socket, medial tissue loading mattered little in terms of comfort. Sockets without IC required high tissue loading to be as comfortable as those with IC and suboptimal tissue loading compromised comfort. The effect on gait of removing IC may be unremarkable in a socket that otherwise fits well and gait adaptations may not be observed until sockets become painful.
[1] Trower TA. Phys Med Rehabil Clin N Am. 2006;17(1):23–30. [2] Dillingham et al. South Med J. 2002;95(8):875–83. [3] Michael JW. Proc 12th World Congress Int Soc Prosthet Orthot; 2007 Jul 29–Aug 3; Vancouver, Canada. p. 54. [4] Uellendahl JE. Proc 12th World Congress Int Soc Prosthet Orthot; 2007 Jul 29–Aug 3; Vancouver, Canada. p. 55. [5] Dillon MP. Proc 12th World Congress Int Soc Prosthet Orthot; 2007 Jul 29–Aug 3; Vancouver, Canada. p. 52.
319
Matthew Quigley (1) Michael Dillon (1) presenting Emily Duke (2)
La Trobe University, Melbourne, Victoria, Australia (1) Royal Melbourne Hospital, Parkville, Victoria, Australia (2)
Comparison of quality of life in people with partial foot and transtibial amputation
Quality-of-Life (QoL) is often thought to be better in people with partial foot (PFA) compared to transtibial amputation (TTA)1. The available evidence is limited to descriptive data and suggests that QoL may be similar in these groups2,3. There are no studies designed to compare QoL in cohorts with PFA or TTA. These data are necessary to help inform difficult decisions about the choice of PFA or TTA from a QoL perspective.
The aim of this study was to compare QoL in people with PFA or TTA secondary to peripheral vascular disease and determine which demographic and health factors influenced QoL.
Persons with either PFA or TTA more than 6 months ago due to peripheral vascular disease were recruited from a major tertiary hospital. A mail-out, mail-back version of the SF-36v2 Health Survey was sent to potential participants along with the demographic section of the TAPES that we adapted to include additional questions about level of amputation and other factors known to influence QoL (e.g., retinopathy). A multivariate analysis of covariance (MANCOVA) was used to compare QoL in the PFA and TTA cohorts (n=33). A multivariate linear regression model was used to identify factors influencing QoL.
Both the SF-36v2 Mental Health Component Score (MCS) and Physical Component Scores (PCS) were comparable in the PFA and TTA cohorts (Figure 1). Age, time with diabetes and presence of retinopathy significantly influenced either the SF-36v2 MCS or PCS whereas amputation level did not.

Comparison of the SF-36v2 Mental and Physical Component scores in cohorts with partial foot (PFA) or transtibial amputation (TTA).
Results of this pilot challenge long-held views that QoL is better in people living with PFA compared to those with TTA. Based on our sample, age, time living with diabetes and the presence of retinopathy had a significant influence on QoL whereas amputation level did not. Given that the level of amputation did not significantly influence QoL, surgeons and patients may instead focus their decision making on factors they can influence, such as the relative risk of ulceration and subsequent amputation.
1 Dudkiewicz et al. The Foot. 2009; 19: 201-4.
2 Boutoille et al. Foot & Ankle International. 2008; 29: 1074-8.
3 Peters et al. Diabetes Care. 2001; 24: 1799-804.
320
Amy Richardson (1) Michael Dillon (2) presenting
George Brown Collage, Toronto, Ontario, Canada (1) La Trobe University, Melbourne, Victoria, Australia (2)
User experience of transtibial prosthetic liners: a systematic review
The liner is an integral part of a transtibial prosthesis designed to protect the residual limb and enhance comfort. Literature comparing different transtibial liners is difficult to interpret and synthesise given the variety of interventions, outcome measures and method designs used. Critical appraisal and synthesize of the evidence is needed to make this literature more useful and better inform decisions about liner prescription based on the user experience.
To critically appraise and synthesize research describing the user experience of transtibial prosthetic liners.
A comprehensive suite of databases were searched using terms related to amputation level, liner type and user experience. Included studies were in English and measured the first person experience of using a transtibial liner. Studies were appraised using the McMaster University Critical Review forms.
18 articles met the inclusion criteria. While the quality of the evidence has improved over time, a number of common issues (e.g., sampling bias, validity of outcome measures, incorrect inferential analysis) reduce our ability to differentiate between the user experience of different transtibial liners.
Despite the number of published studies, there was limited evidence to determine if the user experience differed between transtibial liners. Albeit limited, the available evidence suggests that many aspects of the user experience (e.g., sweating) may be similar between transtibial liners. Focusing on aspects of the user experience that seem to differ most (e.g., ease of donning, the quality of the suspension, the experience of unwanted sounds or rotation within the socket) may help guide discussions about what is important and thereby facilitate more informed decisions about liner prescription based on the user experience.
While the literature documents the user experience of hundreds of people with transtibial amputation, a number of consistent methodological flaws limit what we can learn from these investigations. Future research should utilise validated and reliable outcomes, recruit representative samples and employ statistical techniques appropriate to the number of variables and complexity of the research question. By focusing on these aspects of the reporting and method design, future research will be able to make a more meaningful contribution to our understanding of the user experience of different transtibial liners.
321
Hannah Ozturk (1) Michael Dillon (1) presenting Emily Duke (2) Mary Kennedy-Jones (1)
La Trobe University, Melbourne, Victoria, Australia (1) Royal Melbourne Hospital, Melbourne, Victoria, Australia (2)
Experience of sequential partial foot and transtibial amputation: a narrative enquiry
Following partial foot amputation (PFA), a large proportion of people will experience recurrent skin breakdown, ulceration or wound failure; with one-third requiring further amputation surgery on the same limb.1,2 Anxiety about the prospect of further amputation, depression, and a reduction in quality of life seem to be common experiences following limb loss. Understanding these experiences for people that undergo sequential partial foot and transtibial amputation (TTA) is essential to develop condition-specific education materials that have been shown to establish realistic expectations about the challenges that lie ahead and reduce these negative experiences. While such rich information is available for people living with similarly serious health conditions, (e.g., cancer, spinal compression) there is comparatively little known about the experience of sequential PFA and TTA.
The purpose of this narrative enquiry was to describe the lived experience of people that experienced sequential PFA and TTA.
Participants were recruited through a metropolitan teaching hospital and included adults who had experienced a PFA and then a subsequent TTA on the same limb. Accounts of people’s experiences were obtained via in-depth, semi-structured interviews and common themes generated through narrative analysis.
Three key themes emerged: resolution of enduring complications, improved wellbeing through condition specific knowledge and advice through lived experience.
Participants seemed ill informed about what would happen following their PFA and the likelihood of complications. When these complications did occur, people did not seem well prepared for the challenges that lay ahead. Discussions with other inpatients and allied health professions following PFA were the most common source of information. As participants became better informed about their health condition, they were able to effectively contribute to decisions about their healthcare; leading many to opt for transtibial amputation. For these participants, their experiences following TTA were more positive given that healing was comparatively uncomplicated and they felt they were making progress toward their goals of going home and independence.
This work suggests that patient-specific education material may have a positive impact on wellbeing. Participants in this study recommended that people facing the prospect of PFA be made aware of the potential risks of complications and further treatment, including TTA. Participants recommended that candid conversations with counsellors and clinicians were important to help people facing the prospect of PFA better prepare for their journey and that documenting condition-specific information in brochures was important to aid recall and prompt further discussion. Given the lack of detailed evidence about the experience of sequential PFA and TTA, a shared-decision making model seems appropriate to guide these difficult discussions about the experience.3
1 Dillingham et al. Arch Phys Med Rehabil. 2005; 86:480-6
2 Pollard et al. J Foot Ankle Surg. 2006; 45:91-7
3 Hoffman et al. Med J Aust. 2014; 201:35-9
322
Michael Dillon (1) presenting Richard Fernandez (1,2) Bircan Erbas (1) Chris Briggs (2,3) Matthew Quigley (1)
La Trobe University, Melbourne, Victoria, Australia (1) Victorian Institute of Forensic Medicine, Melbourne, Victoria, Australia (2) Melbourne University, Melbourne, Victoria, Australia (3)
Prediction of the Skeletal ML to improve the accuracy of ischial containment sockets
Accurate measurement of the transfemoral residuum and pelvis is critical for a well-fitting and comfortable socket. One of the most difficult measurements to obtain is the ‘Skeletal ML’ given the need to accurately palpate features of the ischium and locate a calliper in the inter-gluteal cleft. The measurement technique is considered invasive and large variations are common.
As an extension of our initial pilot work1, we sought to improve the accuracy of the Skeletal ML prediction by using input data from Computer Tomography (CT) scans and identifying additional independent variables that might explain part of the variance not described by sex. Without evidence to support which independent variables would be useful predictors of the Skeletal ML, we included several that clinicians could easily record during routine assessment such as the distance between the Anterior Superior Iliac Spines (ASIS) and Greater Trochanters (GT).
To determine how accuracy the Skeletal ML could be predicted and which independent variables contributed significantly to the prediction.
CT-Scans were randomly sampled from a database at the Victorian Institute of Forensic Medicine until minimum sample size of 200 cases was met. Inclusion criteria were: age>25 years, lower-limb alignment that replicated the standing anatomical position, no evidence of osteological trauma, implants or bony growths (e.g., osteophytes). CT-Scans were measured using Vitrea® version 3.1. A measurement protocol was developed to orient the CT-scans into clinical planes of reference and identify discrete landmarks (e.g., apex of the GT) resulting in a high-degree of test-retest reliability for bone-to-bone (ICC>0.9, p<0.001) and soft tissue (ICC>0.8, p<0.01) measures.
Multivariate linear regression models were developed (IBM SPSS ver. 20) to predict Skeletal ML using: sex, age, stature, mass, pelvic depth and height as well as distances between the: ASIS, GT, posterior superior iliac spines and iliac crests.
The regression model explained 79% of the variance in the Skeletal ML (r2=0.786) which was statistically significant (F(10,189)=71.9,p<0.001). Variables that contributed significantly to the prediction of the Skeletal ML included: sex (beta=.553,p<0.001), inter-GT (beta=.396, p<0.001), mass (beta=.238,p<0.001), inter-ASIS (beta=.132,p=0.004), pelvic depth (beta=.100,p=0.033) and age (beta=.082,p=0.023). The Skeletal ML could be predicted with an average error of ±6mm (SEE=6.13). Separate regression models based on sex showed no differences in the accuracy of the prediction in males (SEE=6.09) and females (SEE=6.28).
This work suggests that simple anthropometric measurement could be used to predict the Skeletal ML with an average error of ±6mm. Errors of this magnitude are relatively small and typical of the sorts of adjustments that prosthetists could easily and reliably make during fitting of a check socket. Further work is needed to demonstrate the usefulness of the Skeletal ML prediction in a real-world setting given that in vivo measurement of the predictors may introduce error and reduce the accuracy and usefulness of the prediction.
1 Dillon et al. Prosth Orthot Int. 2014; 38:133-9
323
Tomaž Štajer (1) presenting Gaj Vidmar (1) Helena Burger (1)
University Rehabilitation Institute, Ljubljana, Slovenia (1)
Users’perspective on custom-made orthopaedic shoes
Seventeen to 42 percent of adults have foot pain [1] and half of them have activity limitations [2]. One possibility to decrease these limitations is to use custom-made orthopaedic shoes. However, shoes are only effective if worn. There are several aspects that may influence the use of orthopaedic shoes, such as effectiveness, efficiency and satisfaction [3]. All studies about these factors have been performed in the Netherlands and we do not know whether the same factors are equally important for patients in other countries.
The aim of our study was to find out which factors (and in what ranking order) are important for users of custom-made orthopaedic shoes in Slovenia.
A questionnaire about the importance of various aspects of orthopaedic shoes for their users was devised. All patients using orthopaedic shoes for at least one year, visiting our outpatient clinic for foot problems in summer 2011, who were willing to participate were included in the study. The study was approved by our Institute’s ethics committee.
The participants were 62 women and 66 men, 63years old on average (range 12-92 years). Most of them had used orthopaedic shoes from 1 to 10 years, but some up to 70 years. There was a statistically significant difference between the ranked importance of different factors; the most important was comfort, followed by durability, weight, waterproofness, the way of tying up the shoes, shape, appearance and opinion of other people. Durability was especially important for men; the way of tying up the shoes became more important with increasing age. Orthopaedic shoes statistically significantly decreased foot pain (p<0.001) and improved walking ability (p<0.001).
Similarly to other researcher, we also found out that orthopaedic shoes decrease foot pain and activity limitations [2]. Like in the Netherlands [3], comfort and good fit are the most important factors for users of orthopaedic shoes in Slovenia. Surprisingly, shape and appearance were not deemed very important, even though during their visits to our clinic several patients had complains about those aspects. It seems that decreased pain and better ability to walk overcome the aesthetic issues.
[1] Hawke F, Burns J. J Foot Ankle Res 2009; 2: 1 – 11.
[2] Hawke F et al. Cochrane Database Syst Rev 2008; 83): CD00681.
[3] vanNettenJJ et al. J Rehabil Res Develop 2010; 47: 73 – 82.
324
Helena Burger (1) presenting Ksenija Osrečki (1)
University Rehabilitation Institute, Ljubljana, Slovenia (1)
Effect of posterior leaf-spring ankle foot orthosis on cognitive demand during walking
Posterior leaf-spring ankle foot orthoses (AFO) are used in patients with drop foot in order to assist weak dorsiflexors. Most studies have been performed on stroke patients in whom such AFOs facilitate static and dynamic balance [1] and improve walking. In patients with peripheral ankle dorsiflexor paresis, Geboers and co-authors [2] found that the orthoses did not significantly improve results of walking tests but were safe for use [3]. We could not find any study about the effect of leaf-spring AFO on cognitive demand during walking in any type of patients.
The aim of our study was to assess the effect of posterior leaf-spring AFO on cognitive demand during walking in persons with drop foot due to peripheral ankle dorsiflexor paresis.
All patients with drop foot due to peripheral ankle dorsiflexor paresis visiting our outpatient clinic for orthotic management between September and December 2013 with functional posterior leaf spring AFO and no other impairments who were willing to participate were included into the study. All of them performed 10m walking test with and without AFO in random order first without and then with a cognitive task (subtracting three form 100 during walking). Two-way repeated-measures analysis of variance was used to analyse the data. The study was approved by our Institute’s ethics committee.
Eight men and two women aged 45-80 years old (median 61 years) participated. Nine had peripheral nerve lesion due to various causes (6 spinal disc herniation, 2 injury of peroneal nerve, 1 Guillain-Barré syndrome) and one had dorsiflexor muscle impairment due to compartment syndrome. Three participants were fitted with an AFO for the first time; others had worn it for 3 to 28 years (median 3.5years). The fastest walking was observed using AFO without the cognitive task (mean 0.94m/s), followed by AFO with cognitive task (0.87m/s) and no AFO without cognitive task (0.83m/s); walking without AFO with the cognitive task was the slowest (0.74m/s). Both AFO and cognitive task significantly influenced walking speed (p<0.01); there was no statistically significant interaction (p=0.436). The results were equivalent within the subgroup of participants using AFO for several years.
We found out that posterior leaf-spring AFO improves walking speed during the 10m walking test in patients with peripheral ankle dorsiflexor paresis, both without a cognitive task and with it. Our results differ from the findings of Goebors et al. [2], who did observed no effect of AFO on the results of the 10m walking test. In our participants, walking with AFO while performing a cognitive task was faster that without orthosis and without the cognitive task. We can therefore conclude that in persons with peripheral ankle dorsiflexor paresis posterior leaf-spring AFO improves walking regardless of performing a cognitive task at the same time.
[1] Ramstrand N et al. JPO 2010;22: P4 – P23.
[2] Geboers JF et al. J Rehabil Med 2002;342). 80 – 5.
[3] Geboers JF et al. Arch Phys Med Rehabil 2002; 83(2): 240 – 5.
325
Ksenija Osrečki (1) presenting Imre Cikajlo (1) Helena Burger (1)
University Rehabilitation Institute, Ljubljana, Slovenia (1)
The effect of different ankle foot orthoses on balance – preliminary results
Ankle-foot orthoses (AFO) are the most frequently used orthoses. Nearly one thousand articles can be retrieved from the PubMed database about their use, mainly about their effect on walking in persons with various disabilities. The available literature provides no conclusive evidence about their effect on balance [1, 2], which seems to depend on the design [1]. There is also no evidence about long-term effect of AFO on balance.
The aim of our study was to assess the immediate and long-term effects of different AFO on balance in persons with various disabilities.
All patients visiting our outpatient clinic for orthotic management between January 2013 and June 2014 who needed a functional AFOand had no other impairments willing to participate were included in the study. We assessed their dynamic balance with and without orthosis in a random order using the Postural Response Assessment Device that artificially generates perturbations [3]. The data were compared with normative responses from a healthy population. The study was approved by our Institute’s ethics committee.
We present preliminary results on the first 14 included subjects (8 men), 68 years old on average (range 50-78 years). Five had peripheral nerve lesion, 3 stroke, 2 TBI, 2 were polio survivors, one MS and one neuromuscular disease. Seven were fitted with posterior leaf-spring AFO and 7 with custom-made AFO (three with joints and four without ankle joints). All the included subjects had balance problems without the orthosis. Posterior leaf-spring AFO enabled a postural response more compliant with the norm after forward, forward-lateral, backward and backward-lateral perturbation in both the antero-posterior ant the medio-lateral direction. Custom-made AFO enabled postural response with amplitudes within the norm, especially during perturbations on the impaired side.
Our results for posterior-leaf spring AFO are similar to others [1], but we observed them also in subjects wearing orthosis for several years. The main limitation of the study is the very small number of included subjects. Hence, it was neither possible to analyses custom-made AFOs with joints and without themseparately, nor to study the influence of the duration of using the orthosis. By the time of the presentation, we will have analysed all the data and present the results on 45 subjects.
[1] Ramstrand N et al. JPO 2010;22: P4 – P23.
[2] Guerra Padilla M et al. Neurologia 2014; 29(7): 423 – 32.
[3] Cikajlo I et al. Technol health care 2007; 15: 181 – 93.
326
Helena Burger (1) presenting Liselotte Hermansson (2) Allen Heinemann (3)
University Rehabilitation Institute, Ljubljana, Slovenia (1) School of Health and Medical Sciences, Örebro University, Örebro, Sweden (2) Northwestern University Feinberg School of Medicine and Rehabilitation Institute of Chicago, Chicago, USA (3)
Development of the Orthotic Prosthetic Users’ Survey – Upper Extremity Functional Status module version 3.0 – OPUS-UEFS 3.0
In rehabilitation medicine it is important to have outcome measures with good psychometric properties to evaluate the effects of different interventions, e.g., fitting with prosthesis or occupational therapy. For persons after upper limb amputation the Orthotic Prosthetic Users’ Survey – Upper Extremity Functional Status (OPUS-UEFS) module [1] is suggested. Earlier we found acceptable reliability [2] but several items misfit OPUS-UEFS [2, 4] and the rating scale could be improved [3].
Our aim was to enhance the OPUS-UEFS by taking into account concerns about the current version.
Authors of the original version and the first and second validation study, and representative of the Upper Limb Prosthetic Outcome Measures (ULPOM) group decided on revision of the OPUS-UEFS rating scale and addition of new items. Preliminary data were collected from upper limb prosthesis users in Sweden and Slovenia.
OPUS-UEFS 3.0 consists of 26 activities (15 original, 4 from study 2 and 4, and 7 new). For each activity the person is asked first if the activity is usually done. Next, they are asked to rate difficulty to perform the task with and without the prosthesis using a 4-point scale. Finally, if the person usually performs the activity without prosthesis, follow-up questions address how the activity is performed.
Preliminary results on 44 subjects after unilateral upper limb amputation (31 men) showed that seven activities are done by all, and five by less than half of the subjects. For three activities (drive standard or adapted motorcycle or moped, and drive a car with manual transmission) all who did the activity also used their prosthesis. Two of these activities are done by only 10 – 15% of the subjects.
We developed a revised version of OPUS-UEFS by taking into consideration limitations of the previous version and the suggestions of the ULPOM group. Further studies on the psychometric properties of OPUS-UEFS 3.0 are needed. A multicentre and multinational validation study is underway with centres from Scotland, Sweden, Slovenia and Holland.
[1] Heinemann AW et al. Prosthet Orthot Int 2003; 27: 191-206.
[2] Burger H et al. J Rehabil Med 2008; 40(5), 393-399.
[3] Jarl GM et al. Prosthet Orthot Int 2014; 38(1): 21-6.
[4] Jarl GM et al. Disabil Rehabil Assist Technol 2012; 7(6): 469-78.
327
Longini Mtalo (1) presenting
Kilimanjaro Christian Medical University College, Moshi, Tanzania (1)
Tatcot Contributions and Success in Porosthetic and Orthotic Training
Tanzania Training Centre for Orthopaedic Technologists (TATCOT) was established in 1981 with the aim to address the need of training Prosthetist/Orthotist professional to provide rehabilitation services to people with disability within East Africa. However as the years went by TATCOT continue registering students not only from Eastern part of Africa but even beyond the continent. Furthermore experience gained from training P/O professional over the years drew attention from other non English speaking countries to enrol students at TATCOT. This paper will look at different programmes that are conducted at TATCOT from 1981 to 2014.
This paper is trying to address the training trends in P/O professionals at TATCOT over the 30 years of existence and some challenges associated with P/O training
Student’s register were used in the collection of data ranging from 1981 to 2014. All programmes that are conducted at TATCOT up to one year were included in this paper. These programmes are Diploma course in Orthopaedic Technology (Cat II-ISPO categorization), Certificate course in Lower limb prosthetics/orthotics (LLPT/OT), Certificate course in Wheelchair technology (WTTC), Spinal Orthotic Blended Learning course (SOBL) and Bachelor of Science in Prosthetics and Orthotics (Cat I, BSc P/O)
Over the 30 years of training TATCOT and Kilimanjaro Christian Medical University College (KCMUCO) has managed to graduate 645 professionals of whom 94 Cat I (BSc), 333 Cat II (Diploma in orthopaedic technology),113 certificate in lower limb prosthetics and orthotics (LLPT/OT), 66 Certificate in Wheelchair technology (WTTC)and 39 Spinal Orthotic Blended Learning (SOBL).
Training professional in Prosthetics and Orthotics is a challenging field particularly in low income countries like Tanzania. The majority of training materials, components and consumables are mostly imported from abroad and hence require a huge amount of foreign currency. Looking at enrolment capacity of the different programmes at TATCOT which lies within 10-15 students per each programme per year
328
Céline Lansade (1) presenting Hélène Pillet (2) Coralie Villa (3) François Lavaste (2) Gérard Chiesa (1)
Institut Robert Merle d’Aubigné, Valenton, France (1) Laboratoire de Biomécanique, Paris, France (2) CERAH, Woippy, France (3)
Quantification of the mechanical work performed during the propulsion phase of gait on a population with lower limb amputation: Comparison between five amputation profiles
Amputation involving substantial gait deficits result in greater energy cost. Its quantification appears as a relevant indicator of gait’s quality. The referent method implying oxygen consumption measurement is conflicting with fast clinical gait exam. Calculation of mechanical work easily obtained during conventional gait exam seems a promising way to understand energetic expenditure [1,2]. However, current literature references are limited by the sample size [3].
The aim of this study was to evaluate mechanical work performed by patients with different level of amputation during the propulsion phase of gait for five different populations.
49 patients with different amputation’s level participated in the study. All patients used their own prostheses. The gait analysis exam was realized with an optoelectronic system Vicon and two AMTI forceplates in accordance with plug-in-gait protocol. Each patient adopted their self-selected walking speed. The velocity of the body center of gravity (Cg) was estimated by the velocity of the middle of the two posterior superior iliac spines. Mechanical power was then computed as the dot product of the Cg velocity and the ground reaction forces on each limb [4]. The mechanical work corresponding to limb’s propulsion was assessed by integration of mechanical power profile during the second double support at the end of the stance called Wpropulsion.
The method of Cg velocity calculation has been compared from Pillet’s method [6] using personalized geometrical model from photographs and shows an average error on Wpropulsion of 0.01J/kg [std 0.02] for 24 asymptomatic subjects. Walking speeds of each amputee population and average mechanical work of prosthetic or contralateral limbs are compared in Table 1.
Mean (std) of walking velocity and mechanical works for the five populations. (PLimb = Prosthetic limb ; Climb = Contralateral limb ; TT = Transtibial ; TF = Transfemoral)

In accordance with the literature, average walking gait velocities decreases as the amputation level increases. Mechanical work generated by the prosthetic limb during the propulsion phase is much smaller compared to the contralateral limb’s one. It confirmed the great asymmetry of mechanical production between intact and affected limbs [2,3]. The present study opens the way to a better understanding of amputee compensation and quantification of prosthetic components performance.
1. Kuo AD. Exercise and Sport Sciences Reviews. 2005
2. Houdijk H. Gait and Posture. 2009
3. Bonnet X. Proc Inst Mech Eng H. 2014
4. Donelan JM. Journal of Biomechanics. 2002
5. Pillet H. Gait and Posture. 2010
329
Naveed Ahmed (1,2) presenting Graham Arnold (2)
Pakistan Institute of Prosthetic & Orthotic Sciences (PIPOS), Peshawar, Pakistan (1) Institute of Motion Analysis and Research, Tayside Orthopaedic and Rehabilitation Technology (TORT) Centre, Ninewells Hospital and Medical School, University of Dundee, Dundee, UK (2)
The Impact of Medial Foot Wedge on Tibia Angle in Coronal Plane
The coronal plane motion is less studied compare to sagittal plane motion. However its effect is more diverse and acute. Secondary to knee arthritis, valgus and varus are the two common coronal plane deformities. Medial and lateral wedges are used to reduce the biomechanical changes of the tibiofemoral joint in varus or valgus deformities. There was no evidence found in the literature about effectiveness of the wedges on the tibia alignment. The purpose of this study was to assess the impact of medial foot wedges on the tibia angle in coronal plane.
This research work is specifically focused to find the relationship between the medial foot wedge and the changes that it causes in the tibia angle in the coronal plane.
23 healthy subjects, qualifying the eligibility criteria, underwent the gait analysis without medial wedges and with 6 & 12 mm medial wedges. Different UK size medial foot wedges were manufactured considering thickness of the medial edge covering 2/3rd of the foot length. A modified Helen Hayes Marker placement system was used for the placement of the reflective markers. The tibia motion in coronal plane was recorded using Vicon® motion system. The data from the three groups were compared and analysed using IBM® SPSS® 21.0.
The maximum and minimum angles of the tibia in coronal plane, with the intervention of medial foot wedges, in stance phase were considered for analysis. There were no significant differences in either with and without the wedges (Table-I). Although the mean tibia ROM (Range of Motion) and lower & upper degrees of ROM in the
Significance Difference Between the Variables

Significant p<0.05
This study was the first to specifically assess the impact of the medial foot wedges on the tibial angle. Statistically the results demonstrate no significant change in the tibia angle with the use of the medial foot wedges. As this study showed no change in the measurements of the tibia angle with medial foot wedges, therefore, it is suggested to consider the subtalar joint angulation and knee arthritic patients for the study.
330
Ignacio Gaunaurd (1,2) presenting Robert Gailey (2) Rana Salem (3) Brian Hafner (3)
Miami Veterans Affairs Healthcare System, Miami, FL, USA (1) University of Miami, Coral Gables, FL, USA (2) Universit of Washington, Seattle, WA, USA (3)
Construct Validity of the Prosthetic Limb Users Survey of Mobility (PLUS-M)
Comparison of performance-based and self-report measures by K-Level in people with lower limb amputation

= significant differences among all K-levels; ‡ = significant difference between K-2 and K-3 and between K-3 and K-4; § = significant difference between K-2 and K-3 and between K-2 and K-4. Threshold of significance was p ≤ 0.05.
333
Hans-Rudolf Weiss (1) presenting Sarah Seibel (1)
Spinal Deformities Rehabilitation Services, Gensingen, Germany (1)
Preliminary results of a prospective AIS cohort treated with a recent CAD Chêneau development
A prospective study with a cohort treated with the Gensingen Chêneau brace was started in 2011. Meanwhile we have 72 patients in the database complying with the SRS inclusion criteria.
Purpose of this paper was to analyze the first patients with a follow-up of at least 18 months.
21 patients (12.5 years; Risser 0.89; Cobb 33°; menarche 2.4 months) had a follow up of at least 18 months (21.6 months). Main Cobb angle and ATR angles at the last visit have been compared to the initial values. 7 /21(33%) Patients were already weaned off the brace.
11 Patients (52,3%) improved (>5°), 8 (38.2%) were unchanged and 2 (9.5%) had a progression (>5°). Cobb angle was reduced to 28.4° (p=0,072), ATR thoracic has been reduced from 8.2 to 5.6° (p=0,104) and ATR lumbar from 6.4 to 2.6° (p=0,004). Average brace wearing time as reported was 20.7 hrs. / day.
Compared to other cohorts complying with the SRS inclusion criteria rate of progression was less in this cohort although average Cobb angle was high due to the fact that we also included patients up to 45°. Loss of correction may happen until the end of the follow up and corrections may not be stable until the end. The preliminary success rate of 90%, however is promising compared to the 72% from the BRAIST study by Weinstein et al. Preliminary results as achieved with the Gensingen Chêneau brace seem promising.
Weiss HR, Seibel S, Moramarco M, Kleban A. Bracing scoliosis: The evolution to CAD/CAM for improved in-brace corrections. Hard Tissue 2013 Nov 25;2(5):43.
Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2013 Oct 17;369(16):1512–21.
334
Sheila Clemens (1) presenting Vibhor Agrawal (1) Ignacio Gaunaurd (1,2) Kyoung Kim (1) Robert Gailey (1)
University of Miami Miller School of Medicine, Department of Physical Therapy, Coral Gables, FL, USA (1) Miami Veterans Affairs Medical Center, Miami, FL, USA (2)
Identifying the complexity of the Timed-Up-and-Go Test in unilateral lower limb amputees during specific intervals and mobility improvement
Differences Between TUG Interval Performance

1. Schoppen T; 1999 Arch Phys Med Rehabil
2. Dite W; 2007 Arch Phys Med Rehabil
3. Agrawal V; 2011 Ergonomics
4. Segal A; 2010 Gait & Posture 5. Ventura J; 2011 Gait & Posture
6. Gailey RS; 2008 J Rehabil Res Dev
7. Lemaire E; 1994 Arch Phys Med Rehab
8. Struyf P; 2009 Arch Phys Med Rehabil
334
Sheila Clemens (1) presenting Vibhor Agrawal (1) Ignacio Gaunaurd (1,2) Kyoung Kim (1) Robert Gailey (1)
University of Miami Miller School of Medicine, Department of Physical Therapy, Coral Gables, FL, USA (1) Miami Veterans Affairs Medical Center, Miami, FL, USA (2)
The Functional Lower-Limb Amputee Gait Assessment
The mean and total number of gait deviation observed with the Functional Lower-limb Amputee Gait assessment pre and post 8 weeks of prosthetic training.

336
Manal Al Lawati (1) presenting Sarah Day (1)
University of Strathclyde, Glasgow, UK (1)
Factors Influencing Overuse Syndrome in Persons with Unilateral Upper Limb Absence: A Literature review
338
Kiriakos Daniilidis (1) presenting Christina Stukenborg-Colsman (1) Henning Windhagen (1) Daiwei Yao (1) Eike Jakubowitz (2)
Clinic for Orthopaedic Surgery, Medical School Hanover, Annastift, Hanover, Germany (1) Biomechanical Laboratory, Hanover, Germany (2)
“First clinical and gait analysis results after implantation of a neuroprosthesis for the treatment of the neurogenic drop foot”
In Germany we have yearly about 270.000 strokes per year. From that amount approximately 14.000 patients suffered from a drop foot and about 70.000 from a hemiplegia. This results into a limitation of the physiological gait and is associated with a high risk of fall and high costs for the health care system. In the USA there were about 700.000 strokes per year and in fact of the demographic changes, the treatment of that handicapped patients will be a challenge for the future
The aim of the present pilot study is to gain first insights into the change of gait pattern after implantation of a neuroprosthesis and to detect clinically relevant treatment parameters in patients who suffered from a neurogenic drop foot after stroke.
Four patients (2m / 2w) who suffered from a neurogenic foot drop after stroke were treated with a new neuroprosthetic device (ActiGait®, Otto Bock, Duderstadt). Subsequently a gait analysis with two marker models (Oxford Foot Model and Plug-in Gait full body) was performed. In each case the kinematics and kinetics were compared between the stimulated and the non-stimulated drop foot. Furthermore to evaluate the safety concerning the risk of falls, we measured the ground reaction force. In addition a subjective patient’s evaluation concerning their current situation and quality of life was carried out.

Compared to the non-stimulated foot the data show a clear convergence of the time-distance parameters, the kinematics (upper ankle joint and knee angle, and the head tilt) and the kinetics (ground reaction forces) to the physiological gait cycle. The quality of life was improved because of increased stability, mobility and independence. All patients stated that they had a benefit in their walking stability and would perform the surgery anytime again.
Because of the “ad-hoc” character of the present pilot study a conclusion can not be finally stated. Nevertheless, the obtained data show a clearly measurable correction of gait pattern in patients with neurogenic drop foot after implantation of the neuroprosthesis and a superiority with and without stimulation in the gait pattern.
339
Kiriakos Daniilidis (1) presenting Christina Stukenborg-Colsman (1) Henning Windhagen (1) Bastian Welke (2) Daiwei Yao (2) Eike Jakubowitz (2)
Clinic for Orthopaedic Surgery, Medical School Hanover, Annastift, Hanover, Germany (1) Biomechanical Laboratory, Hanover, Germany (2)
“Unusual endoprosthetic alloarthroplasty in a case of an transfemoral amputee patient to simulate a knee exarticulation”
We report an unusual case of a 38-year-old physically active patient, who suffered of a Ewing sarcoma during his adolescence and therefore was treated with a tumor endoprostheses ex domo (replacement of distal femur and proximal tibia). To date he had to undergo a couple of surgical interventions for revision and currently is suffering with persistent pain of the concerned leg. An aseptic loosening of the tibial component was evident after performing radiologic examinations. Due to his long life of suffering our patient refused further surgeries of retaining the affected limb and he preferred amputation.
We would have taken the risk of a femoral residual limb that is much too short compared with a classical above-knee amputation. In this regard we saw difficulties of the exoprothetic treatment with functional limitations that would have easily influenced the outcome negatively
Consequently, we decoupled the tibial component from the femoral one within the knee joint and thus performed a knee disarticulation leaving the femoral component in situ. Furthermore we performed a gait analysis preoperatively and postoperatively with the interim and the final prosthetic device. We did not determine any differences concerning the clinical outcome.

Postoperatively, we found a mostly harmonious gait pattern with a pure mechanical interim prosthesis regarding time-distance parameters, which may be even further improved by the outstanding final prosthesis. Sagittal joint angles are comparable to those of conventionally knee exarticulated.
To date, no comparable case of such an alloarthroplasty was highlighted in literature, which could regain his mobility with an exoprothetic treatment. As a result, a knee disarticulation within the area of a knee arthroplasty leaving the femoral component is right up with an “ordinary” knee disarticulation.
340
Yasushi Akazawa (1) presenting Hisashi Naito (2) Masao Tanaka (3)
Hyogo Institute of Assistive Technology, Kobe, Japan (1) Institute of Science and Engineering, Kanazawa University, Kanazawa, Japan (2) Graduate School of Engineering Science, Osaka University, Osaka, Japan (3)
Three-dimensional simulation of hemiplegic walking towards characteristics design of ankle-foot orthoses
Ankle-foot orthoses (AFOs) prescribed for hemiplegic patients are required to fit mechanically to them in evidence-based rehabilitation. On clinical sites, the fitting process of AFO functions is often performed by time-consuming trial and error. A novel method of AFO characteristics determination is thus coveted to obtain the proper AFO stiffness lessening burden of trial process participants.
In this paper, investigated is the possibility of AFO stiffness determination by utilizing 3-D simulation of hemiplegic walking with and without a posterior-leaf-spring AFO.
The three-dimensional simulation method [1] of human walking was modified to generate and compare various gaits under different ankle conditions of hemiplegic subjects. The model proposed was a neuro-musculo-skeletal model with hemiplegic characteristics. Plural gait cycles of nearly steady walk were obtained after numerical gait parameter optimization using a small-scale PC cluster. For the affected side, three model conditions for plantar flexion were studied: A00: normal stiffness and normal muscle state; AS02: adding 2% soleus tension of the maximum continuously to A00; AFO: AS02 with the AFO having a plantar flexion resistance of 1.0 Nm/deg. Walking speed, stride length, and coronal thigh angle as circumduction [2] were calculated.
For all conditions, walks of more than 10 strides were obtained. Under the condition AS02, gaits exhibited ankle plantar flexion in swing phase and toe contact at the beginning of stance phase. The walking speed of each condition was 1.07±0.03 [m/s] (A00), 1.16±0.04 (AS02) and 1.05±0.07 (AFO) (average±s.d.) respectively. The stride length was 1.22±0.04 [m] (A00), 1.24±0.03 (AS02), and 1.19±0.05 (AFO) ; and the energy consumption rate was 0.69±0.02 (A00), 0.79±0.02 (AS02), and 0.72±0.04 (AFO). Circumduction of the affected side was observed in all of three conditions, and the circumduction angle was maximum in the condition AS02 (Fig.1).

Maximum circumductions (Boxplot).
Nearly steady gaits were computationally generated by the three-dimensional walking simulation based on a neuro-musculo-skeletal hemiplegic model. The results were biomechanically reasonable because the generated gaits with abnormal soleus tonus of condition AS02 indicated larger compensatory motion of circumduction than that of the non-spastic condition A00. Use of AFO limiting abnormal ankle motion reduced the compensatory motion compared to that in the spastic condition. This demonstrated the potential of such a 3-D walking simulation as a tool for the determination of proper mechanical characteristics of AFOs.
[1] Hase; 2002, JSME Int J Ser C. [2] Kerrigan; 2000, Am J Phys Med Rehab.
341
Ruiqi DONG (1,2) presenting Mansang WONG (1) Wentao JIANG (2)
The Hong Kong Polytechnic University, Hong Kong, Hong Kong (1) Sichuan University, Chengdu, Sichuan, China (2)
Quantitative analysis of arterial morphological changes and muscle atrophy of residual limb after trans-femoral amputation
After limb amputation, blood flow is a crucial factor affecting amputee’s recovery, since it nourishes the entire musculoskeletal system of the residual limb. The surgery makes the arterial structure of residual limb undergo tremendous changes including spatial deformation and volume change which are likely to continue because of muscle disuse and atrophy. Conversely, these changes would cause variation of flow field and hemodynamic parameters, thereby probably giving rise to the development of muscle atrophy.
To investigate the correlation of morphological changes between the arteries and muscles of both thighs of unilateral trans-femoral amputees.
Eight subjects with unilateral trans-femoral amputation (including 2 follow-up cases) were recruited. Computer Tomography (CT) Angiography and Magnetic Resonance Imaging (MRI) scans were performed. The 3-D reconstruction models of femoral arteries extracted from CT images provided the mean values of hydraulic diameter, circumference and sectional area of 5 main arteries, and exported the coordinate matrices of arterial trees to calculate the Hausdorff Distance (HD) for describing spatial deformation. The cross-sectional area of each femoral muscle could be measured using the MRI images. After data collection, the parameters of arteries and muscles between residual limb and sound limb of each subject were compared. The 2 follow-up cases also got comparison between three test intervals within one year after surgery.
The arterial hydraulic diameter, circumference and cross-sectional area, as well as the cross-sectional area of each muscle of the 2 follow-up cases emerged fluctuation within one year after amputation. Nevertheless, the HD values and muscle cross-sectional area decreased in the three follow-up tests of residual limb were larger than that of the sound limb. The indices of each artery and muscle of the 8 subjects showed individual differences. However, in general, the subjects with larger muscle cross-sectional area percentage of residual limb to sound limb exhibited lower HD values between bilateral arterial trees, except for a patient who wore an implantable prosthesis, the vessels of residual limbs with the largest reduction were the superficial femoral artery, lateral and medial femoral circumflex arteries. Corresponding to the nourishing relationship, the atrophies of quadriceps and semitendinosus were the greatest.
Due to different causes of amputation, different types and utilisation rates of the prosthesis, as well as many other factors, the parameters of each artery and muscle of the individual subjects can present variations. Nevertheless, there is a positive correlation between the spatial deformation of arterial tree and the muscle atrophy of residual limb. Generally, with a consistent muscle-blood supply relationship, the arterial reduction degree is positively correlated with the atrophy degree of the muscles nourished by it. Nonetheless, for further quantifying this proportional relationship deserves a larger sample size and a longer duration of study.
344
Boris Dauriac (1,2) presenting Coralie Villa (3) Xavier Bonnet (2) Noël Martinet (4) Hélène Pillet (1) François Lavaste (1,3)
Arts et Metiers ParisTech, Institut de Biomecanique Humaine Georges Charpak, Paris, France (1) Proteor, département recherche et développement, Seurre, France (2) CERAH, Institution Nationale des Invalides, Creteil, France (3) Centre de médecine physique et de réadaptation Louis-Pierquin, IRR-UGECAM Nord-Est, Nancy, France (4)
Prosthetic knee behaviour during slope and stair descent

Moment vs. angular velocity of the prosthetic knee in the sagittal plane for stair and slope descent
Knee damping coefficients varied between individuals from 0.37 to 1.26 N.m.s/° showing the different settings of the hydraulic brake. The coefficients were the same for each patient in both situations. Power absorption profiles in the single support of gait were directly related to this setting.
[1] Silder et al. 2012 Journal of Biomechanics
[2] Riener et al. 2002 Gait & Posture
[3] Schmalz et al. 2007 Gait & Posture
[4] Pillet et al. 2014 IRBM
345
Matthew Wernke (1) presenting Ryan Schroeder (1) Jeffrey Denune (1) Chris Kelley (1) James Colvin (1)
The Ohio Willow Wood Company, Mt. Sterling, OH, USA (1)
Regulation of Temperature and Perspiration within a Prosthetic Socket to Improve Amputee Quality of Life
Heat and perspiration are common complaints leading to a decreased quality of life reported by amputees2. Materials used for prosthetic sockets and liners have poor thermal properties, and therefore insulate the residual limb1, resulting in elevated socket temperatures and increased perspiration. In an effort to Tradiimprove the thermal properties of the prosthetic liner, silicone was modified with a proprietary phase change material (PCM) to increase the heat capacity of the liner.
The purpose of this work is to report results from a crossover study evaluating the PCM liner to a standard silicone liner.
Unilateral transtibial amputees participated in this study. A randomized crossover design was used to evaluate the change in temperature and perspiration during activity between a standard silicone liner and a silicone liner with PCM added. Half of the participants (Group A) began testing wearing a standard silicone liner and the other half (Group B) started the study wearing the PCM liner. Continuous temperature data was collected by thermocouples that were placed on multiple skin surface locations (posterior-medial, posterior-lateral, anterior, and the distal end,) and in the testing room (environment was maintained at 80°F). During the activity a metronome was set to match the participant’s self-selected pace to maintain cadence. Skin moisture was measured immediately after doffing the liner post-activity by wiping the limb and liner and determining the change in weight of the towel. After a 1 hour rest period, the groups changed treatments and the procedures were repeated. The metronome cadence documented during the first activity session was used during the second activity period to ensure consistent cadence between the two. A one tailed, paired t-test was performed on the data.
The rise in temperature during the activity was significantly decreased (p<0.05) when subjects wore the PCM liner compared to the standard liner. More importantly, perspiration within the liner was significantly decreased (p<0.05) when subjects wore the PCM liner compared to the standard liner.
Overall, the results from the testing indicated incorporating PCM into the liner can significantly affect the environment inside the liner. The difference in temperature between the two liners is clinically significant as suggested by Peery3. The results support anecdotal claims made by amputees that a PCM liner creates a more comfortable temperature environment and less perspiration inside the liner. Regulating the temperature in the socket and reducing the amount of perspiration can lead to improved comfort, health and quality of life for amputees.
1. Klute, G. Pros Orthot Int; 31(3), 292-299, 2007
2. Hagberg K. Pros Orthot Int; 25, 86, 2001.
3. Peery J. JRRD; 42(2), 147-154, 2005.
4. Klute, G. AAOP Free Paper, 2013.
346
Matthew Wernke (1) presenting Cameron Rink (2) Surya Gynawali (2) Ryan Schroeder (1) Jayne Kim (2) Heather Powell (2) Jeffrey Denune (1) James Colvin (1) Chandan Sen (2)
The Ohio Willow Wood Company, Mt. Sterling, OH, USA (1) The Ohio State University, Columbus, OH, USA (2)
Elevated Vacuum Dependent Changes in Residual Limb Circulation and Skin Health
Qualitative studies focusing on elevated vacuum suspension sockets have found improvements in skin health1 and wound healing2, 3 on the basis of self-reported questionnaires, clinical outcomes scales, and wound closure studies. The purpose of this work is to provide quantitative results of vacuum dependent changes on residual limb circulation and skin health. Non-invasive measurement protocols were developed that leverage out-of-socket skin health tests (transepidermal water loss (TEWL), surface electrical capacitance (SEC), cutometry (CTY), and torsional ballistometry (TB)), out-of-socket circulation imaging (hyperspectral imaging (HI) and laser speckle imaging (LSI)), and in-socket probe-based circulation tests (transcutaneous oxygen measurement (TCOM), laser doppler flowmetry (LDF)).
The purpose of this work was to employ these techniques to characterize residual limb health in response to long-term use of a vacuum suspension socket.
Ten unilateral amputee subjects (5 transfemoral and 5 transtibial) were enrolled in the study. A crossover design was employed, such that half of the subjects were randomized to begin the study with their current, non-vacuum prosthesis (Group A) while the other half began testing with the vacuum socket (Group B). After 16 weeks, subjects in Groups A and B crossed over to use either the vacuum socket or their original prosthesis respectively. Residual limb measurements were acquired at baseline (week 1), mid-point (week 8), and final (week 16) time points. Skin health data were expressed as mean ± standard error of the mean and statistical significance was established using a student’s t-test (p<0.05).
The use of vacuum socket technology reduced both skin surface hydration and water loss compared to non-vacuum controls in Group A in areas of high socket pressure but the effect was damped within Group B. Skin biomechanics were less strongly affected by vacuum suspension, however some differences in elasticity were found. Reactive hyperemia (increase in blood flow after period of occlusion) was consistently observed when comparing pre- to post-activity StO2 values from the residual limb of amputees. After 16 weeks of use, however, reactive hyperemia was significantly attenuated in subjects under elevated vacuum suspension conditions as compared to suction controls. While not statistically significant, there was a general trend for reactive hyperemia to increase over the 16 weeks under suction conditions.
This work represents first efforts to quantitatively assess skin health and circulation in response to elevated vacuum suspension. The results suggest vacuum suspension leads to improved circulation and skin health. Further work is needed to explore these findings in more detail with a larger study population.This research was funded by the U.S. Department of Veterans Affairs (VA118-12-C-0038).
1. Ferraro C. J Prosthet Orthot; 23, 78-81, 2011.
2. Brunelli S. Orthopadie Technik; 2, 2-8, 2009.
3. Traballesi M. Dis Rehab: Ass Tech; 4, 373-375, 2009.
347
Daniel W. W. Heitzmann (1) presenting Julia Block (1) Merkur Alimusaj (1) Cornelia Putz (1) Sebastian I. Wolf (1)
Clinic for Orthopedics and Trauma Surgery Heidelberg University Hospital, Heidelberg, Germany (1)
A novel prosthetic foot design leads to reduced peak loads of the sound side in unilateral trans-tibial amputees, preliminary results
Individuals with a trans-tibial amputation (TTA) have lost one of the main contributors for forward propulsion, the calf muscles. In prosthetic feet this is addressed via an energy storing and returning (ESAR) design. Though, ESAR feet demonstrate a 2-3 times greater energy return in relation to simple, solid-ankle, cushion-heel feet [1], their push-off is still limited. This limitation, of the prosthetic side can result in higher loading of the sound side during a step to step transition, as e.g. a reduced push-off from the trailing, prosthetic limb can result in greater impact of the leading, sound limb [2].
Aim of the presented study was to verify if a novel prosthetic foot design can reduce sound side stress in unilateral TTA.
Five TTA (all male, 37.7±13.6y; 81.6±10.6kg; 184.4±4.9cm) were fitted with a conventional ESAR foot (CF; Variflex EVOTM) and got two weeks to familiarize. Prior to assessment, TTA were fitted with the novel prototype foot (NF; all feet by Össur, Iceland). With NF, the TTA walked approx. 1.5 km in mixed terrain to adjust. Subsequently, TTA underwent a 3D gait analysis while using first the NF and following the CF during level ground walking at self-selected speed. TTA were equipped with retro reflective markers according to Plugin Gait model (Vicon, UK), kinetics were calculated accordingly [3]. Markers on TTA remained in place for both conditions (NF, CF), except for prosthetic side ankle marker. Ankle marker height and anterior posterior position was duplicated from NF to CF to minimize effects on power calculation [4]. Prosthetic alignment between NF and CF was replicated using a LASAR Posture TM (Otto Bock, Germany). Data of 17 unimpaired subjects served as a reference (NORM; 28.4±5.6 y; 72.6±13.8kg; 178.4±7.9cm). Significance (p<0.05) was tested by a two tailed Wilcoxon Signed-Rank Test (NF vs. CF).
Prosthetic ankle peak power in late stance was significantly higher for NF (p=0.043; NF 2.5±0.4 W/kg vs. CF 1.6±0.3 W/kg; fig.1A). Sound side peak vertical ground reaction force (GRF) was significantly reduced with NF (p=0.043; NF 10.2±0.4 N/kg vs. CF 11.7±0.5 N/kg; fig. 1B) and sound side peak external knee valgus moment in stance was significantly reduced for NF (p=0.043; NF 0.6±0.1 Nm/kg vs. CF 0.7±0.1 Nm/kg; fig. 1C).

Although TTA got a short time to adapt to NF the biomechanical response with NF was similar in all subjects. Major influential factors on the results, e.g. prosthetic alignment and marker placement between conditions were controlled to minimize effects on results. In conclusion NF leads to the proposed higher energy return and the according reduction in sound side stress. Like for Morgenroth et al. our results correspondingly show that a refined design of the established ESAR concept can provide such effect [2]. A larger cohort will be examined to confirm these preliminary results.
[1] Czerniecki JM et al. J of Biom 1991;24;63-75. [2] Morgenroth DC et al. G&P 2011;34;502-7. [3] Kadaba MP et al. J Orthop Res 1990;8;383-92.[4] Rusaw D et al. Clin Biomech 2010;25;713-20.
348
Susan Spaulding (1) presenting Ignacio Gaunaurd (2) Dagmar Amtmann (1) Sara Morgan (1) Robert Gailey (2) Brian Hafner (1)
University of Washington, Seattle, Wa, USA (1) Miami Veterans Affairs Healthcare System, Miami, FL, USA (2)
Prosthetists’ confidence administering outcome measures

Prosthetists’ confidence before training, after training, and at 1-2 years follow-up
1. Duncan EA, Murray J. BMC Health Serv Res; 12, 1-9, 2012.
2. Forsetlund L, et al. Cochrane Database Syst Rev; 2, 2009.
349
Edward Lemaire (1,2) presenting Andrew Smith (1,2)
Ottawa Hospital Research Institute, Ottawa, ON, Canada (1) University of Ottawa, Ottawa, ON, Canada (2)
Biomechanics Analysis of Powered Exoskeleton Gait on Level and Inclined Surfaces
Lower extremity powered exoskeletons have become a viable technology that enable people with lower extremity paralysis to walk and interact with their chosen environment in an upright position. These devices are self-supporting walking frames with powered actuators at the hips, knees, and/or ankles that are controlled in realtime to create motion and resist limb collapse. While these devices are available clinically, little biomechanical research is available on device function.
Biomechanically investigate movement for level and incline walking with a prototype lower extremity powered orthosis (Bionik Labs exoskeleton: ARKE).
Five able-bodied participants were recruited and trained with the ARKE device. Gait testing was performed on the CAREN-Extended virtual reality system (6-DoF movable platform with dual-belt treadmill and integrated force plates, 12-camera Vicon motion capture system, 180° floor to ceiling projection screen). On day one, 300 m of walking data were collected without ARKE over level and 5° inclines/declines, at 0.2 m/s and 0.6 m/s walking velocities. On day 2, participants completed the same protocol as day one while using the ARKE, with short fast and short slow step settings. Ground reaction force and kinematic data were sampled at 1000 Hz and 100Hz, respectively.
For stride parameters, ARKE gait double support time decreased between 35-45%, step time increased from 35-73%, stride time increased from 42-78%, and stride length increased from 45-53%, relative to unassisted walking. Upslope had the largest differences. Foot clearance was 1 cm for unassisted and 4-5 cm for ARKE gait. To achieve foot clearance, ankle, knee, and hip angles were greater when walking with ARKE.
Pelvis angles at foot-off were greater for ARKE gait, with pelvis tilt differences of 13.3° for level, 11.4° for upslope, and 15.6° for downslope. Pelvic obliquity differences were smaller with increases of 0.7° for level and 1.1° for upslope, and a decrease of 0.6° for downslope. Pelvis rotation angles were smaller with ARKE (1.9° for level and 2.5° for upslope, and 1.6° for downslope).
The ARKE exoskeleton uses a similar control approach to other powered bilateral devices, where the person leans forward and laterally to initiate each step. Therefore, increases in pelvic tilt and obliquity were anticipated. However, the lateral tilt differences were less than expected. Also, the results demonstrated that the current biomechanical algorithm did not require a separate “slope mode” to accommodate inclines or declines. However, algorithm improvements could be made to increase double support time, thereby providing a more conservative gait strategy.
350
Brad Poziembo (1,2) presenting
Prosthetic Design Inc, Clayton, OH, USA (1) Dayton Artificial Limb Clinic, Clayton, OH, USA (2)
3D Printing: Engineering Socket Friction to Improve Socket Fit
Movement within a prosthetic socket causes instability and diminished suspension. A common paradigm within the field of prosthetics is a socket must be smooth to achieve a good fit. However, increased movement on a smooth surface is expected since it has a lower coefficient of friction. 3D printing technology has the ability to engineer precise texture to create friction within a socket.
Study the effects of friction on socket fit, in terms of stability and suspension.
Over 30 subjects with a lower extremity amputation wore a conventional socket and 3D printed textured socket that was a duplicate of the conventional socket. Duplication was performed through digitization. Subjects then rated each socket in terms of stability and suspension.
All subjects noted no change to significant improvement in stability and suspension when wearing the 3D printed textured socket. None of subjects noted a decrease in stability or suspension.
By applying friction through texture within a prosthetic socket, it is possible to obtain an better socket fit. The data suggest that the texture increased the static friction the socket, thus reducing movement of the residual limb in relation to the socket. Further studies need to be conducted to obtain objective data on the impact of socket friction on socket fit.
351
Brad Poziembo (1,2) presenting
Prosthetic Design Inc., Clayton, OH, USA (1) Dayton Artificial Limb Clinic, Clayton, OH, USA (2)
Case Report: One clinic’s successful integration with exclusive use of 3D printed lower extremity sockets, liners, and IPOPs
3D printing provides benefits of increased efficiency (cost, time, and labor), mass customization, and ability to produce complex products compared to traditional processes. Limited use in the prosthetic industry is due to inadequate durability, equipment, and software. Thus, a machine overcoming these limitations could significantly benefit prosthetic clinics and their ability to care for amputees.
The purpose is to show that lower extremity sockets, liners, and IPOPs can be fabricated through 3D printing and successfully integrated for exclusive use within a prosthetic clinic.
Over 150 subjects with an amputation were fit with one or more of the following 3D printed devices: lower extremity socket, liner, or IPOP. This case report spans over a three year period at one prosthetic clinic using a Squirt Shape machine. Fabrication of sockets were for transtibial and transfemoral amputees ; silicone liners were off-the-shelf and custom made using printed molds; IPOPs were in the form of two piece ambulatory devices. Success was measured by an amputee being able to wear the device as a definitive weight-bearing product.
All subjects were able to successfully wear one of the three products as a definitive weight-bearing product. Several subjects were able to only wear one of the products due to personal preference or physical limitations.
The findings of this case report show that 3D printed components can be successfully integrated into a prosthetic clinic. With these products, better care can be provided to an amputees through faster fittings and more customized definitive products. Further research is needed to design and develop other prosthetic components.
352
Liang-Wey Chang (1) presenting Chien-Hung Chen (1) Chu-Sheng Hsiao (1)
National Taiwan University, Taipei, Taiwan (1)
Structural and Functional Abnormalities Associated with Mild Anatomical Leg Length Discrepancy
Mild anatomical leg length discrepancy (LLD < 3 cm) is commonly seen in general population but the association between mild LLD and the pathomechanical outcome measures of the sacroiliac joint and muscles is not clear. The clinical evidences of structural and functional asymmetries are essential to establish the relationship between mild LLD and pelvic torsion, which may be a source of functional deficits such as pain in particular.
The aim of this research was to study mild LLD and the structural and functional asymmetries in regard to pelvic torsion, hip joint passive ROMs, and gait kinetics in medial-lateral ground reaction forces and hip joint internally rotating momentduring terminal stance.
Fifteen able-bodied subjects (7 females, 8 males; age = 23 ± 3 yrs) were recruited and took standing radiographic scanographies for LLD assessment. Gait experiments were carried out in a laboratory equipped with Optotrak motion system and three AMTI force plates. Subjects walked barefoot on a 6m walkway at self-selected speed. Kinetic data were collected during terminal-stance, which is from the time of heel lift to the contralateral heel strike. Pelvic torsion was measured with pelvic inclinometer. The ROMs of the hip during clinical tests (FAIR Test and pelvic internal rotation test) were measured with goniometer. Statistical analysis was performed by paired t-test for the shorter leg and the longer leg.
All of the subjects had mild LLD (4.2 ± 3.2 mm; range = 0.7-10.2 mm). The pelvic inclinometer output Pt showed opposite inclined angles for the shorter side and the longer side (p=0.000), which indicated there existed pelvic torsion and the innominate bone of the shorter side rotated anteriorly. The ROMs of hip adduction ROMadd and hip internal rotation ROMint of the shorter leg side were smaller than those of the longer leg side (p=0.002 and 0.000), which might link to muscle tightness. During terminal stance in gait, the medial-lateral ground reaction force impulse If and the internally rotating vertical moment impulse acting on the hip Im of the shorter leg side were larger than those of the longer leg side (p=0.014 and 0.000), which might be also due to structural and functional asymmetries.
Mild LLD coexists with pelvic torsion, abnormality of hip joint passive ROMs and asymmetry of gait kinetics. It was shown that the innominate bone of the shorter side anteriorly rotates and the shorter leg shortens in the Supine to Sit test. The shorter side presents with smaller passive ROM in hip internal rotation and adduciton, but with increased medial-lateral ground reaction force impulse and increased internally rotating moment impulse on the hip during terminal stance in gait. The cause and effect relationship between mild LLD and the associated abnormalities remains to be established.
353
Srood Suad Nafie (1) presenting
ICRC, Erbil/ Kurdistan, Iraq (1)
The International Committee of the Red Cross physical rehabilitation programme in Erbil (Iraqi Kurdistan Region):18 years of more than prosthetic and orthotic service delivery
The International Committee of the Red Cross (ICRC) has established a physical rehabilitation center (PRC) in 1996 in Erbil, capital of the Iraqi Kurdistan region (IKR) in response to extensive needs related to continuous conflicts 1. The objectives of the project are to insure accessibility and provide quality of physical rehabilitation (PR) services in the region. The reintegration of beneficiaries within their communities sought through Micro Economic Initiative projects and by developing the network of associations for people with disabilities (PWD).
This presentation aims to present a comprehensive approach in physical rehabilitation. The constraints and opportunities of such a project will be discussed in light of the current situation in IKR.
Erbil PRC used a result based management method to monitor implementation of the interdisciplinary (IDT) approach, aiming at upgrading existing comprehensive service provision. Close follow up was undertaken by senior staff to enhance capacity to produce adequate quality and quantity prosthetic and orthotic (P&O) devices as well as providing gait and functional training. A twin track strategy included the provision of PR services and upgrading the technical capacity of staff. Developing sustainable services was a cornerstone in the strategy, lobbying for adequate training of qualified P&O technicians and physiotherapists (PTs).
Between 1996 and 2014, the PRC produced more than 12000 P&O devices using the Polypropylene technology for both upper and lower limbs fitting. Since 2008, it is the unique center which performs comprehensive wheelchair prescription and delivery (more than 700 since 2008). Since 2012 the center has implemented the IDT approach to deliver the services, enhancing the sense of collaboration and trust and leading to coherent working procedures. In addition, rehabilitation is fully beneficiary centered and the professionals are using clinical reasoning in all decision stages. The beneficiary satisfaction and trust towards each ID team member is one of the main reasons for the evolution of the project… Erbil PRC is also considered to be the only training center in Iraq to upgrade the scientific, practical and IDT competences of the staff working in the ICRC supported centers (400 trainees since 2006). The Micro Economic Initiative project succeeded in assisting about1200 families by helping the beneficiary of Erbil PRC to start an income generating project.
After 18 years of existence, this project illustrated the importance of staff training, and support to teaching institutions for human resource development within the field of PR. The project also emphasize on the role of management in monitoring and evaluating the project within a framework of comprehensive services. Moreover, early assessment of local regulations and traditions are essential in developing a specific strategy. Many centers supported by non-governmental organizations had faced challenges in assuring quality of services as they did not included a broad approach to the development of the Physical rehabilitation sector in IKR.
1-Physical Rehabilitation services in Iraq by J. Faber& P. Saggurthi, the Lancet, March 2013
355
Dorothy Boggs (1,2) presenting Isabelle Urseau (2)
Handicap International, London, UK (1) Handicap International, Lyon, France (2)
Focusing upon the contribution of P&O and wheelchair service providers to the sustainability of the physical rehabilitation sector in seven fragile countries through multi-stakeholder involvement using a participatory consensus tool
During the joint Sustainability Study and subsequent workshops, ten national level SAP workshops5 with key rehabilitation actors have been held to analyse and measure rehabilitation system sustainability through the participatory development of SIs. National rehabilitation actors have included service providers (inclusive of P&O and wheelchair technicians), professional associations, disabled people, disabled people’s organisations (DPOs), donors, authorities and international organisations.

[1] Nepal, Somaliland, Cambodia, Sierra Leone and Liberia
[2] Blanchet, Karl, Boggs, Dorothy (2012) “The Sustainability Analysis Process: the case of physical rehabilitation” Lyon: Handicap International
[3] Sarriot E., et al (2008). Macro Intl
[4] Six Sustainability Framework components: C1 health & rehabilitation outcomes; C2 service delivery; C3 & C4 Ministry and local organisational capacity and viability; C5 Community capacity; C6 enabling environment http://www.sustainingability.org/about-us/about-sustainability/sustainability-framework-sf/index.html
[5] Cambodia, Liberia, Nepal (x3), Sierra Leone, Somaliland (x2), Burundi and Haiti
[6] Sustaining Ability Case Studies http://www.sustainingability.org/case-studies/index.html
[7] Blanchet, K, Palmer, J (2012) Planning for Sustainability in the Physical Rehabilitation Sector : Report of a 2-year follow-up study in Nepal http://www.sustainingability.org/case-studies/nepal/sustainability-study-part-ii/index.html
356
Lina Magnusson (1) presenting Gerd Ahlström (1)
Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden (1)
Prosthetic and Orthotic Users’ Satisfaction with their Lower-Limb Assistive Device in Malawi and in Sierra Leone
Magnusson L, Ramstrand N, Fransson EI, Ahlström G. Mobility and satisfaction with lower-limb prostheses and orthoses among users in Sierra Leone: a cross-sectional study. Journal of Rehabilitation Medicine 2014; 46:438-446
359
Zeshan Zahid (1) presenting
Rawalpindi Medical College, Rawalpindi, Punjab, Pakistan (1)
Research and Development trends among the World Prosthetist Orthotist Community
360
Coline Martinot-Lagarde (1) presenting Didier Pilliard (2) Frédéric Clavier (1) Nathaly Quintero-Prigent (1) Naïma Brennetot (1) Franck Fitoussi (1)
Hôpitaux de Saint Maurice, Saint Maurice, Ile de France, France (1) Clinique Jouvenet, Paris, Ile de France, France (2)
Interest and use of mechanical prosthesis without control for a population of children with agenesia or traumatic amputation of forearm
The use of mechanical prosthesis without control is a specific technic used in our hospital.
This new study is following the one presented at ISPO 2007. It enabled to expand the range of population by targeting a more precise study population in order to evaluate the evolution and to sharpen and fine-tune our current practice with the use of a mechanical prosthesis without control.
This study is based on a population of 279 children born between 1965 and 2014. They all had agenesia or traumatic amputation of forearm. 49% of this population of patients were once equiped with prosthesis without control. This is a collection of testimonies from children and their parents during multidisciplinary consultations in our department about the use of a mechanical prosthesis without control. The population only focused on children with unilateral involvement forearm. The statement outlines the statistical ages of wearing, years of establishment, wearing time and the activities carried out. Use of pivot tables allows to correlate a particular age, a type of activity on a significant population.
136 out of 279 children (49%) have used a mechanical prosthesis without control. 32 out of these 136 patients are still wearing one in 2014. Between 2000 and 2014, 20 to 32 mechanical prosthesis without control were prescribed per year. The use of this prosthesis was between 1 and 15 years. The duration of the use of the mechanical prosthesis did not exceed 2 years for half of the patients. This prosthesis was usually worn between the ages of 3 years and 7 years, ages in which the child is improving his psychomotor development.
Children mainly use this prosthesis for cycling activity, followed by school handlings (hold a sheet of paper to cut, hold a ruler). After 8 years of age, it is mainly used for specific leisure activities.
This new study confirms and refines results found in our previous study dated from 2007. What changes in our practice were implemented? What is the real need for such type of prosthesis? If it seems inappropriate to wear it before 3 years old, the use of a mechanical prosthesis without control seems to help children to practice some well-targeted activities.
-Chevalier F., Martinot-Lagarde C., Templier D., Utilisation de la prothèse mécanique sans commande chez l’enfant, 2008, ErgOthétapie n°31
- Pilliard D., 2004, KS 43-49
- Sheffler LC & ol, 2009, J Bone Joint Surg Am.
- Crandall RC & ol 2002 Pediatr Orthop.
-Huilzing K. & ol, 2010 Prosthest Orthot Int
362
Kristen Vendeville (1) Matthew Major (1,2) presenting
Northwestern University, Chicago, IL, USA (1) Jesse Brown VA Medical Center, Chicago, IL, USA (2)
Prediction of Frequent Fallers Amongst Lower Limb Prosthesis Users and Effects of Mobility Aid Use on Mobility and Balance Performance
Falling amongst lower limb prosthesis users (LLPUs) is a common event, and has a negative impact on independence in daily living (e.g., social/community engagement and mobility), and consequently quality of life [1]. Clinical outcomes (e.g., performance measures and patient descriptors) may provide an accessible and clinically-relevant means for identifying LLPUs at risk for falls, but research on this topic is limited [2,3]. The ability to clinically determine those at risk for falls is important to guide rehabilitation and safety precautions.
1) Develop a model that classifies LLPU “fallers” (≥2 falls) and “non-fallers” (≤1 falls), and
2) Identify differences in performance between fallers and non-fallers, and mobility aid levels.
A binary logistic regression model was developed through a backward stepwise procedure using data on 29 LLPUs from a previous study [4]. The dependent variable was faller classification (fallers/non-fallers), and independent variables included continuous outcomes on the two-minute walk test, L-Test, and Berg Balance Scale, as well as self-reported fear of falling and community use of a mobility aid. Differences in outcome scores between fallers and non-fallers and between level of mobility aid use (none, crutches/canes, and wheelchair) were statistically assessed with an independent t-test and one-way ANOVA, respectively.
The final model (p=0.008, 86% accuracy, R2=0.43) suggested that the use of mobility aid and fear of falling were significant predictors of falls (p=0.016 and p=0.035, respectively). Those who used a mobility aid fell more frequently than non-users (42% versus 12%). Outcome score differences between fallers and non-fallers were not significant (p≥0.114), but were significantly different between levels of mobility aid across all measures (p≤0.007). An inverse relationship between mobility aid level and performance was observed (i.e. performance was worst for wheelchair users, followed by crutch/cane users, then non-users; see Fig 1 for example).

The model suggests that self-reported use of a mobility aid for community ambulation and fear of falling may predict LLPUs at risk of frequent falls. Use of a mobility aid appears to negatively affect mobility and balance, with wheelchair users demonstrating the most impaired performance. These results suggest that clinicians may use such simple patient-reported information to identify patients that may benefit from closer monitoring and suggest appropriate interventions (e.g. prosthetic components and training) to improve ambulation safety.
[1] Miller, WC. Arch Phys Med Rehabil 2001.
[2] Gremeaux, V. Prosthet Orthot Int 2012.
[3] Wong, CK. J Rehabil Med 2014.
363
Dylan Borrenpohl (1) Matthew Major (1,2) presenting
Northwestern University, Chicago, IL, USA (1) Jesse Brown VA Medical Center, Chicago, IL, USA (2)
A Survey-Based Investigation of the Role of Outcome Measures in the Assignment of Medicare Functional Classification Level for Persons with Lower Limb Amputation
The Medicare Functional Classification Level (K-level) was originally designed to classify functional level and ultimately recommend prostheses for persons with lower limb amputation (LLA) [1]. However, K-level assignment is commonly based on subjective and imprecise methods. Clinically-relevant outcome measures that assess functional mobility have the potential to objectively and consistently assign K-level. To effectively implement these measures, an understanding of how they are currently used and viewed by clinicians must be gained.
Determine how clinicians use clinically-relevant outcome measures for K-level assignment, and how these measures might be integrated into clinical practice to enhance objectivity of this process.
A survey was administered online between October 20th and November 24th of 2014 and distributed via the US-based professional orthotics and prosthetics emailing list, OandP-L. The survey consisted of 20 questions and was divided into three sections regarding: 1) demographics of the respondent sample, 2) methods used to clinically assign K-level, and 3) opinions on potential limitations with the current standard of practice for K-level assignment.
Data was collected on 237 respondents. Most of the respondents were either Certified Prosthetists (34%) or Certified Prosthetist-Orthotists (54%), and the average length of practice was 16.7 years (Range: ≤1-50 years). Regarding responsibility for K-level assignment, 41% of respondents indicated that they were the sole determinate in the assignment process, while 39% indicated that physicians and physical therapists were also included in the decision process. Importantly, 67% of respondents did not believe the K-level classification system is sufficient to accurately assign a level of rehabilitation potential for persons with LLA, with 76% agreeing that incorporation of outcome measures into clinical practice would enhance objectivity of the assignment process. The frequency of different types of outcome measure used by the respondents to facilitate assignment are displayed in Fig 1 (total percentage exceeds 100% as respondents were able to select multiple categories).

A majority of respondents believed that the K-level system was inadequate to accurately classify rehabilitation potential, but that outcome measures may be a useful means for improving this process. These results may facilitate improvement of the functional level assignment process for persons with LLA, and the eventual adoption of a standardized, accurate, and reliable system that is agreed upon by both Medicare and practicing prosthetists. Such a system will allow clinicians to maximize treatment outcomes while minimizing costs to the patient and the payer.
[1] US Health Care Financing Administration Common Procedure Coding System, 2001.
364
Hossein Gholizadeh Vazvani (1,2) Elhamsadat Yahyavi (2) Arezoo Eshraghi (1,2) presenting Hassan saeedi (2) Zahra Safaeepour (3) Mina Arvin (2,3) Noor Azuan Abu Osman (1)
University of Malaya, Kuala Lumpur, Malaysia (1) Iran University of Medical Sciences, Tehran, Iran (2) University of Social Welfare and Rehabilitation Sciences, Tehran, Iran (3)
Clinical assessment of a new prosthetic suspension system
Prosthetic suspension system play a significant role in prosthetic function and amputee’s comfort. Suspension in lower limb prosthesis is attained either anatomically or externally through various components. From the insights provided by the literature reviews and survey studies, designing new suspension system is deemed necessary to enhance the positive qualities of the current systems, while reducing their drawbacks
This study evaluates a new suspension system for lower limb prostheses, and aims to compare the interface pressure and amputees’ satisfaction with the new system compared with a common prosthetic suspension system (pin/lock).
Ten transtibial amputees walked at a self-selected speed on a level ground with two different suspension systems, namely the pin/lock and HOLO system (figure 1). The interface pressure was measured using the F-socket transducers at the proximal, middle and distal sites of residual limb. Furthermore, subjective feedback was logged to compare two systems.

The pressure was significantly higher at the proximal and distal areas with the pin/lock suspension system during the swing phase of gait (P < 0.05). Subjective feedback also showed traction at the stump with the pin/lock system. There were no significant differences in the pressure applied to the mid-anterior and mid posterior stump for both suspension systems. The HOLO system may distribute the pressure more uniformly compared with the pin/lock system, especially during the swing phase of gait
The intention of this study was to deepen understanding on the effect of suspension system on the load distribution over the residual limb. The new coupling system was proved compatible with the pin/lock system in terms of suspending the leg and amputee’s satisfaction. On the other hand, the HOLO system could distribute the pressure more uniformly over the residual limb.
Gholizadeh, H., Abu Osman NA, Eshraghi, A., & Razak, N.A. Clinical implication of interface pressure for a new prosthetic suspension system. Biomedical engineering online, 2014,
365
Emilie Leblong-Lecharpentier (1) presenting Anne-Cécile Barre (2) Isabelle Bonan (1,2) Aleth Perdriger (3)
Service MPR CHU Pontcahillou, Rennes, France (1) Service MPR CHU Hopital Sud, Rennes, France (2) Service rhumatologie CHU, Rennes, France (3)
Compliance of hand orthosis in rheumatoid arthritis : A randomised, comparative, controlled study
Rheumatoid arthritis is a chronic painful rheumatoid illness with deformities and functional handicap and less quality of life. Non pharmacological treatments are recommended until march 2007 in France. Hand positioning orthosis’ efficacy is known on pain, dexterity and quality of life. In literature, the compliance and tolerance of orthosis studied without to study the importance of patients’ information.
The purpose of this study is to assess the impact of patients’ information on compliance of hand positioning orthotic during rheumatoid arthritis.
A comparative, randomised, monocentric, controlled study conducted until April 2012 in the University Hospital of Rennes. Inclusion criteria are voluntary patients with rheumatoid arthritis according to ACR criteria and pain and/or hand deformities. The ethics committee of CHU of Rennes gave his content. All patients received made-to-measure orthosis by trained occupational therapist and either only written information ( group A) or written and oral information (group B) on objectives of orthosis, wearing instructions and maintenance, rules of joint savings and hand exercises.
50 patients (38 women and 12 men) were included and randomised in to comparative groups. Characteristics are according to epidemiological data on this illness. Before this study, 30% have an old orthosis but only a few were reviewed by doctors and only 3 were changed in spite of advice of yearly changed. At 1 and 3 months, in group A, 36% (9/25) wore orthosis more than 50% of prescribed time against 52% (13/25) in group B. There is a statistical difference during two groups. At 1 year, there is no significate difference between two groups with a mean compliance of 25% (12/50). The circumstances which lead to stop where analysed.
This study shows that education and information could increase compliance of orthosis in rheumatoid arthritis but the effect was reduced with time.
With new drug therapy in rheumatoid arthritis, literature dealt less on physical therapy concerning this illness. Nevertheless, also drugs slowed evolution, some patients have real deformities and a lot of them are painful. So orthosis like the other physical treatment keep an important role on care. This study assesses the importance of information and patient’s education during a dedicated time by therapists and confirmed the interest of enhancement of this time near to patients. Some specific educational programs are developed concerning rheumatoid arthritis and they have to include information on orthosis. Last but not least we have to organise the follow up of orthosis.
This study constitutes a first step to evaluate an educational procedure which has to purchase by evaluation of coaching to fight against the decrease of compliance with time.
Silva AC. Effectiveness of a night-time hand positioning splint in rheumatoid arthritis: a randomized controlled trial, J Rehabil Med, 2008,Oct;40(9):749-54
Splints and orthosis for treating rhumatoïde arthritis, Egan M, Cochrane Database Syst Rev. 2003;(1):CD004018. Review
A crossover trial of custom-made and commercially available wrist splints in adults with inflammatory arthritis. Haskett S. Arthritis Rheum. 2004 Oct 15;51(5):792-9.
Use of resting splints by patients with rheumatoid arthritis., Feinberg J, Am J Occup Ther. 1981 Mar;35(3):173-8.
366
Emilie Leblong-Lecharpentier (1) presenting Marie-Christine Cristina (2) Pierre Verschoore (3) Ali Damaj (1)
Service MPR CHU Pontchaillou, Rennes, France (1) Pôle MPR St Hélier, Rennes, France (2) Service amputés, brulés, Rachis, CMRRF Kerpape, Plomeur, France (3)
Sports injuries at athletes with trans-tibial amputation
Lower limb amputation, although rare in young people, can occur especially in traumatic etiology. After early rehabilitation and walking recovery, patients have expectations in return to physical activities. Many advances have been accomplished in the field of materials’ aspects but there are few reports about prosthetic induced injury related to sport practices.
The purpose of this study is to assess the existence of specific traumatic injuries in trans-tibial amputees and suggest specific safety practices and follow-up.
A 8-centers retrospective declarative study conducted between November 2012 and March 2013. An anonymous questionnaire built for this study was sent to 35 trans-tibial amputees playing sports through their PRM practisers or their orthetists in the west of France. Inclusion criteria were patients with trans-tibial amputation all etiologies included,
playing sports with prosthesis, all sports and all levels included, major or with parental consent, agreeing to meet a declarative dedicated survey. We excluded incomplete questionnaires.
24 amputees answered and 3 were excluded due to missing data. Etiology was traumatic in 15 (71%) and amputation was bilateral in 6 (28%).The mean age was 41.5 years old (from 16 to 91). Amputation dated 13,2 years average (3 to 62).
Prosthesis dedicated to sport practice was used by 10(41%).
Residual limb pain during sport practices reported at least once in 15 (71%), completing phantom limb’s pain criteria in 4 (19%). Skin’s wounds occurred in 16 (76%). Muscles, ligaments and tendons’ injuries in 7(33%) involving mostly knees and low back. No bone fracture occurred.
No original anterior study dealt specifically in amputees and sports injuries. Few reports concerned injuries to athletes during Paralympics Games for all kinds of disabilities. They tried to define patterns injury. Nevertheless, comparison is difficult to not disabled athletes and controlled study doesn’t exist.
Concerning biomechanics aspects, some studies dealt with changes due to prosthetic materials especially carbon feet and knee consequences at long term. 3D gait analysis makes it possible to examine specifically times of stance and swing but also impact peak with prostheses. It grows acknowledges on materials and the normal amputee locomotion.
All of these studies tried to propose safety practises to this specific population which grown with the development of adapted physical activities. Some interesting articles bring few elements especially on prevention of knee osteoarthritis. Technics of movement analysis could also advance acknowledges on biomechanics, forces and injuries in specific sports by developing and completed clinical aspects.
The short number of patients is still important in a rather small population. We should follow this work with others rehabilitation centers and with prospective data and joints’ imagery.
H Hobara, B S Baum, HJ Know. Amputee locomotion : lower extremity loading using running-specific prostheses. Gait and Posture 39 (2014) 386-390
M Bragaru, R Dekker, J HB Geertzen. Amputees and sports : a systematic review. Sports Med 41 (2011) 721-740.
K Fagher, J Lexell. Sports-related injuries in athletes with disabilities. Scand J Med Sci Sports (2014).
MS Ferrara, CL Peterson. Injuries to athletes with disabilities : identifying injury patterns. Sports med (2000) 137-143.
367
Rajesh Chandra (1)
Handicap International, Democratic People’s Republic of Korea (1)
Scope of Physical rehabilitation services in the Democratic People’s Republic of Korea- An impact assessment report
Handicap International/EUPS 7in partnership with the Korean Federation for the Protection of the Disabled (A quasi Civil Society Organization under the umbrella of MoPH) is implementing a programme on physical rehabilitation services in DPR Korea since 2001. Various projects have been implemented so far in phased manner aiming to promote contemporary rehabilitation, through professionals capacity building, services equipment and organizational support, and reflection on rehabilitation sector development in the country.
The aim of the study is to analyse the impact made by the programme in the rehabilitation sector of DPR Korea as well as to provide practical recommendations on future strategy planning.
Following methods were used in this study:
Desk review: Project proposals, various internal and external impact related reports, HI and KFPD strategy papers, training reports, end of mission reports from various technical experts, client data etc.
Interviews (semi structured) with key staff of relevant stakeholders.
Self-evaluation and open discussion with key staff members.
Field visits and observation at various health and rehabilitation facilities.
Technological advancement: Before the international organization started supporting the physical rehabilitation sector in DPRK P&O services were provided in only one center, by using local material such as wood, leather and iron, without having well precise measurement, fitting and training for their effective use. The implemented programme has successfully introduced and integrated contemporary technologies (such as CRE, resin, hybrid etc.). Technical capacities: The technical (P&O Cat II and Internationally recognized physiotherapy services) training (Overseas and in-country) provision made through these projects have created a vast positive impact on the quality of service delivery. The programme also introduced the role and importance of physiotherapy services in the P&O sector. Service delivery approach: Besides mitigating scarcity of services through development of outreach actions, the challenge of introducing the patient centered and multi-disciplinary approach of services delivery is being addressed.
So far significant improvement has been made in the field of rehabilitation services (especially in the P&O sector) in the country, but meeting globally recognized standards of physical rehabilitation services (professional competencies, patient centered and multi-disciplinary approaches) requires further efforts. In line with the 2013 signature of the UNCRPD, next steps foreseen include the development of a global rehabilitation strategy for the country, the introduction of intentionally recognized rehabilitation related education programmes, and the diversification of proposed rehabilitation services.
368
Alessandro Marco De Nunzio (1) presenting Sabrina Lemling (1) Marko Markovic (1) Strahinja Dosen (2) Dario Farina (2) Bernhard Graimann (1)
Democratic People’s Republic of Korea, Otto Bock HealthCare GmbH, Duderstadt (1) Germany, University Medical Center Göttingen, Dep. of NeuroRehabilitation Engineering, Göttingen (2)
Vibrotactile feedback to improve force grasping control of myoelectric forearm prostheses
Proportional feedback on grasping force is one of the most important requirements for future improvements in myoelectric forearm prostheses design [1] and vibrotactile stimulation represents an unobtrusive, easily applicable and comfortable method to provide this feedback. Moreover, grasping is a complex task routinely performed in an anticipatory way [2], where sensory feedback is responsible for learning, maintaining and updating the internal model of grasping dynamics.
This study is aimed to evaluate if force feedback information could be used for improving prosthetic grasping force accuracy and learning the model of the prosthesis dynamics to preserve force accuracy without the continuous assistance of feedback information.
Six able-bodied subjects (24.7 ± 5 years, mean ± SD) were enrolled. The subjects myoelectrically controlled a state-of-the-art prosthesis (Michelangelo Hand, Otto Bock Healthcare GmbH) sensorized with position and force sensors. The prosthesis was detached from the subject to avoid indirect feedback and the subject observed the movement of the prosthesis by looking into an animated graphical prosthetic gripper. An array of 3 C2 tactors (EAI, USA), positioned transversally on the forearm, was used to feedback 9 levels of grasping forces. Bursts of 230 Hz delivered at 30 Hz were used as vibrotactile stimulus, and 3 amplitudes of vibration (min, med, max) for each tactor coded the 9 force levels. The vibrotactile stimulus moved from the most lateral to the most medial tactor and from min to max intensity with the increase of the grasping force. Each subject, after a training session, performed two blocks (1st with, 2nd without vibrotactile feedback), of consecutive grasps (1st 70, 2nd 40 grasps) generating a predefined force level. Three force levels (70%, 50%, 30% of the prosthesis maximum force) were tested in three different sessions. The maximum force reached during each grasping trial was used as the trial outcome. The mean relative error, the deviation between the generated and the target force as a percent of the target force, was calculated for each block (Vibro, NoVibro) and session (70%, 50%, 30%). For each session, a paired Student’s t-test between feedback conditions was executed.
The results (Figure) showed no significant accuracy reduction when controlling grasping force to target low and medium force levels (30% and 50%) with and without vibrotactile force feedback. At high grasping force (70%) a significant increase in relative error passing from Vibro to NoVibro condition was reported.

This study highlights the importance of a continuous sensory feedback to achieve high force grasping, while a learning effect can be seen at medium and low levels of force thanks to the previously received vibrotactile feedback. The results speak for the possibility to learn how to control prosthesis grasping force in an anticipatory way. Interestingly this ability may be lost when a high grasping force must be expressed. Since aperture velocity and grasping force of the prosthesis are linearly linked, we can claim that to achieve medium and low grasping forces the trained subject could predict the force levels just taking into account visual information coming from the movement of the graphical prosthetic gripper, while at higher force level, because of the faster aperture velocity, visual information cannot be effectively integrated and used as feedback.
1. Peerdeman, B., et al. J Rehabil Res Dev, 2011. 48(6): p. 719-37.
2. Flanagan, J.R., et al., Curr Biol, 2003. 13(2): p. 146-50.
369
Michael Lang (1) presenting André Müller (1)
Germany, Otto Bock HealthCare GmbH, Duderstadt (1)
Climate socket – focusing on thermal comfort in the prosthetic socket
Microclimate conditions (temperature, humidity, sweat retention) in the prosthetic socket are of large importance for patient satisfaction, comfort and safety. Several publications show the potential drawbacks of retained heat and excessive sweating/perspiration in the socket, e.g. reduction in quality of life, skin irritations and friction blisters [1, 2, 3, 4]. The climate socket is a novel approach to improve comfort by using temperature and humidity controlling materials and technology in the prosthetic socket.
The aim of this study was to show that a newly developed climate socket is able to improve thermal comfort in patients with a lower limb amputation. A case review shows first clinical experience.
The climate socket is a double wall socket system with an inner weight bearing surface that carries temperature sensors and aligned strips of Phase Change Material (PCM). The outer surface of the socket is used as a cosmetic shell. Between these two surfaces an electronic fan system creates an air flow to dissipate heat from the inner socket. In a first clinical test, two unilateral transfemoral amputees were fitted to prove the technical concept of the socket system. Both subjects underwent a 1-hour protocol including 28 minutes treadmill walking, 13 minutes functional testing (2 Minute Walk Test, Timed and go Test, Four Square Step Test) and 13 minutes resting periods after treadmill walking/functional testing, with and without socket ventilation, respectively. Beforehand the subjects were seated for few minutes. Ambient conditions in the room were 22°C and 1001 hPa. The socket temperature was measured continuously during the test period with 1Hz.
During the different phases of the test, the climate socket was shown to stabilize average temperature within the socket (Figure 1). Even during treadmill walking (phase 1), the socket temperature was unchanged, as was during the following functional testing (phase 2). Compared to the condition without socket ventilation, the temperature was up to 4.5°C lower at the end of the 1-hour test period (phase 3). Both subjects reported a noticeable reduction in temperature of the skin during the test with the ventilated socket system.

average temperature in the climate socket with activated and deactivated fan. Phase 1: Treadmill, Phase 2: Functional tests, Phase 3: Resting.
The first test results with the climate socket are promising. The temperature within the socket was kept lower with socket ventilation by preventing heat accumulation. This effect may possibly result in reduced sweating which may, in turn, lead to an improved socket suspension and healthier skin conditions on the long-term. The results justify further studies with more patients and longer use and in a greater variety of environmental conditions.
[1] Hagberg K, et al., Prosthet Orthot Int 2001;25:186-194. [2] Levy SW, Artif Limbs 1956;3:20-35. [3] Akers WA, et al., Mil Med 1972;137: 1-7. [4] Naylor PF, Br J Dermatol 1955;67: 239–48.
370
Therdchai Jivacate (1) M.L.Buddhibongsa Devakula (1) presenting Tipaporn Yesuwarn (1) Vajara Rujiwetpongstorn (1) Boonyou Tipaya (1)
Germany, Prostheses Foundation of H.R.H. the Princess Mother, Chiang Mai (1)
Prostheses Foundation’s Satellite Workshops: Right Solution for Sustainable Accessibility for Prosthetic Services in Thailand
371
Alessia Giangrande (1) Paolo Caravaggi (1) Giada Lullini (1) Lisa Berti (1) Alberto Leardini (1) presenting
Thailand, Movement Analysis Lab, Istituto Ortopedico Rizzoli, Bologna (1)
Functional assessment of orthopaedic shoes for forefoot offloading: traditional baropodometry together with state-of-the-art gait analysis
Forefoot offloading shoes (FOS) are special orthopedic footwear designed to protect and unload the injured part of the foot after surgery and for conservative treatments. While these shoes are intended to be worn only for short periods, a compromise must be found between offloading and comfort from one hand, lower limb functionality and stability on the other hand.
The aim of this study therefore is to integrated traditional baropodometric measurements with pelvis and lower limb joint kinematics and kinetics from standard gait analysis for an overall assessment of the effects on walking of a traditional half-shoe and a novel FOS (Podartis, Treviso, Italy), in a comparison to a standard comfortable shoe (control).
Ten healthy female participants (28.2±10.0 years; BMI 20.4±1.2 kg/m2) were asked to walk in three different footwear conditions for the right/left foot: traditional half-shoe/control, novel/control, and control/control. State-of-the-art gait analysis with three-dimensional rotations and moments at the hip, knee and ankle joints [1] was obtained from three walking trials for each participant in each condition. Simultaneously a sensor insole system (Pedar, Novel GmbH, Munich, Germany) recorded plantar pressure at 100 Hz. Rearfoot, midfoot and forefoot regions, along with the whole foot, were defined a-priori by selecting corresponding pressure capacitive sensors among the 99 available. Normalized root mean square error, determination coefficient, and frame-by-frame statistical analysis were used to assess differences between kinematic and kinetic time-histories.
No significant differences were detected in walking speed and ground reaction force between the three shoes, nor in the spatio-temporal parameters with the exception of the stride length, this being on average 9 cm shorter in the half-shoe condition. From baropodometry, the time-histories of peak pressure (kPa) for each shoe condition revealed different patterns between these shoe conditions at each region. Wearing the traditional and novel FOS resulted in smaller peak pressure at forefoot (kPa, half-shoe 178±90; novel 186±45; control 244±75: p<0.05). The half-shoe showed also the smallest mean and maximum force and force-time integral at forefoot. At rearfoot, mean and peak pressure were the largest in the novel shoe. novel FOS design showed less compensation at the more proximal lower limb joints. Motion at the lower limb joints was similar to control for the two FOS designs, but at the pelvis normalized root mean square error was 68% at the half-shoe, 27% in the novel design. At the ankle, sagittal-plane rotation in the novel FOS had a pattern more similar to control (half-shoe r2=0.85; novel r2=0.93). For joint moments, the largest discrepancy from the control was observed in the sagittal and frontal planes at the ankle joint, root mean square error being 16% in the half-show, 4% in the novel design.
The novel FOS appears capable, though less effective than a traditional half-shoe, in reducing considerably forefoot pressure. However, the good forefoot offloading at the traditional half-shoe was associated to more kinematic and kinetic alterations at the proximal lower limb joints with respect to the control, likely associated to the necessary compensation mechanisms for the peculiar shape of the outsole. The prescription of these forefoot offloading shoes should take into consideration both the required offloading and the overall restoration of normal gait function.
[1] Leardini et al., A new anatomically based protocol for gait analysis in children Gait & Posture, 26:560-71, 2007.
373
Åsa Eliasson (1) presenting Åsa Bartonek (1)
India, Karolinska Institute, Stockholm (1)
Walking ability in children using lower limb prosthetic devices - A systematic literature review
[1] Law M, 1998, Available from: www.srs.mcmaster.ca/Portals/20/pdf/ebp/quanguildelines.pdf.
[2] Bhandari M, 2006, Injury
374
Igor Simanic (1) presenting Igor Popovic (1) Vladimir Jakovljevic (2) Borka Gavrilovic (1) Verica Zivkovic (1,2) Vladimir Zivkovic (2) Fatic N (3)
Sweden, Specialized Hospital for Rehabilitation and Orthopedic Prosthetics, Belgrade (1) Serbia, Department of Physiology, Faculty of Medical Sciences, University of Kragujevac, Kragujevac (2) Serbia, KBC, Podgorica (3)
Orthopedics Prosthetic Rehabilitation Of Patients With Unilateral Lower Limb Amputation And Hyperbaric Oxygenation
Hyperbaric oxygenation (HBO) has been proven to be very effective adjuvant procedure in the multidisciplinary approach to the treatment of gas gangrene, diabetic ulcers and other forms of chronic unhealing wounds and soft tissue necrosis.
The aim of our study was to investigate the effects of HBO on the prosthetic rehabilitation (by evaluating LCI test and Narang’s score) of patients with unilateral lower limb amputation.
Sixty patients with unilateral lower limb amputation were randomly divided into two groups: a group that received HBO treatment (experimental group) and control group. Both groups were subjected to the assessment of functional competence by using LCI test and Narang’s score.
Our results clearly show that in case of a relatively homogeneous group of patients, standard therapy and prosthetic rehabilitation with adjunct of HBO provided better functional capacity of these patients
Adjuvant hyperbaric oxygen therapy (HBO2) for treatment of necrotizing fasciitis reduces mortality and amputation rate. In summary, the results of our study point out to the usefulness of HBO therapy in prosthetic rehabilitation of lower limb amputees. HBO is a relatively safe, non-invasive means of improving healing by enhancing oxygenation, decreasing edema, and modifying healing and immune responses. Although it is expensive, not universally available, and not without risks, limb preservation and speedier healing make this a cost-effective method of wound care, but further research is needed to establish its efficacy and safety in other conditions, such as after amputation.
Narang IC, Mathur BP, Singh P, Jape VS. Functional capabilities of lower limb amputees. Prosthet Orthot Int 1984; 8: 43-51.
Pohjolainen T, Alaranta H, Karkkainen M. Prosthetic use and functional and social outcome following major lower limb amputation. Prosthet Orthot Int 1990; 14: 75-9.
Zgonis T, Garbalosa JC, Burns P, Vidt L, Lowery C. A retrospective study of patients with diabetes mellitus after partial foot amputation and hyperbaric oxygen treatment.
Gauthier-Gagnon C, Grise MC, Lepage Y. The Locomotor Capabilities Index: content validity. J Rehabil Outcomes Meas 1998; 2: 40-6.
Ciaravino ME, Friedell ML, Kammerlocher TC. Is hyperbaric oxygen a useful adjunct in the management of problem lower extremity wounds? Ann Vasc Surg 1996; 10: 558-62.
Zemmel NJ, Amis LR, Sheppard FR, Drake DB. A temporal analysis of the effects of pressurized oxygen (HBO) on the pH of amputated muscle tissue. Ann Plast Surg 1998; 40(6): 624-9.
Lebel D, Gortzak Y, Nyska M, Katz T, Atar D, Etzion Y. Hyperbaric oxygen therapy for chronic diabetic wounds of the lower limbs–a review of the literature. Harefuah 2007; 146(3): 223-7, 244-5.
Bishop AJ, Mudge E. A retrospective study of diabetic foot ulcers treated with hyperbaric oxygen therapy. Int Wound J. 2012; doi: 10.1111/j.1742-481X.2011.00936.x. [Epub ahead of print].
Escobar SJ, Slade JB Jr, Hunt TK, Cianci P. Adjuvant hyperbaric oxygen therapy (HBO2) for treatment of necrotizing fasciitis reduces mortality and amputation rate. Undersea
376
Kenneth Wong (1) presenting Kam Wai Chen (2)
Australia, Queen Mary Hospital, Hong Kong Island (1) Hong Kong, Queen Mary Hospital, Hong Kong Island (2)
A Case Study – A Modified Orthotic Design For Chopart Amputee To Restore The Forefoot Function
Various types of prostheses and orthoses were designed for Chopart’s amputee, for improving their gait function and appearance. This case study was conducted to investigate the biomechanical effect of the modified low-profile orthotic design for Chopart’s amputee by video analysis system and pressure mapping system.
The aim of study was to evaluate the biomechanical effect of the modified low-profile orthotic design for Chopart’s amputee
A 22 year-old female who suffered from left Chopart’s amputation was recruited in this study. An ankle foot orthoses (AFO) was prescribed for her in US and a toe-filler (TF) with leather boot was prescribed for her in Hong Kong, however she felt inconvenient due to the bulkiness. A low profile (below ankle) Chopart’s orthoses (CO) was then prescribed for her and also incorporated with a carbon fiber AFO (CFAFO) for exercising. Totally 4 types of orthotic interventions were compared in this study. Dartfish video motion analysis system was used for comparing the gait pattern with different orthoses and prostheses. Zebris FDM pressure mapping system was used for the evaluation of the biomechanical factors of her gait.
Both gait symmetry, forefoot function at propulsion and CoP pathway were improved in all types of orthoses. High profile (above-ankle) orthoses showed more symmetrical CoP pattern to the sound side and larger force was generated at amputated side during late stance phase. Due to the energy returning property of carbon fiber, highest propulsion force was found in late stance phase in CFAFO. CoP pathway was similar to the sound side in the modified low profile although the forefoot function was lower when compared to high profile design.
High profile design was seldom preferred by the amputee due to its bulkiness. Low-profile design such as toe-filler and foot orthoses can improve the gait stability, but it cannot be expected to improve the forward progression of the CoP as well as the missing lever arm during walking.
1. Dillon MP, Fatone S, Hodge MC. Biomechanics of ambulation after partial foot amputation: A systematic literature review. J Prosthet Orthot 2007;19:P2-P61.
2. Hirsch G, McBride ME, Murray DD, Sanderson DJ, Dukes I, Menard MR. Chopart Prosthesis and semirigid foot orthosis in traumatic forefoot amputation: Comparative gait analysis. American Journal of Physical Medicine & Rehabilitation. 1996;75:P283-P291.
377
Miroslav Janura (1) presenting Zdenek Svoboda (1) Karolina Orechovska (1)
Hong Kong, Palacky University, Faculty of Physical Culture, Olomouc (1)
The effect of residual limb parameters on ground reaction force during walking in unilateral transtibial amputees
Walking is considered to be one of the most important aspects of independence.1 There exist asymmetries in ground reaction force (GRF) parameters between the amputated and intact limb during gait2. Walking in people with transtibial amputation is affected by the stump dimensions and quality of its tissues. The length of the residual limb can have an effect on the energy expenditure level during gait.3
The aim of the study was to describe the effect of the length of residual limb and the residual limb sensation on the GRF in gait.
Sixteen patients with the unilateral transtibial amputation (thirteen males, three females; age 42.8 ± 10.8 years, height 179.6 ± 11.1 cm, weight 88.6 ± 13.9 kg) participated in this study. The length of residual limb, the type of scar, and the residual limb sensation were assessed. All participants completed 5 walking trials at a self-selected speed over a 10 m long walkway, GRF data were recorded bilaterally using two force plates Kistler 9286AA. Statistica v10 was used for statistical analysis (Wilcoxon paired test, Spearmann’s rank correlation, Cohen’s d).
Relative posterior braking (p=0.001, d=1.56), anterior propulsive (p=0.001, d=1.07), and second vertical GRF peaks (p=0.007, d=1.05) were significantly greater on the intact limb. Significant correlation was observed between residual limb length and posterior braking peak (r=0.564, p=0.036) as well as between first vertical GRF peak and the residual limb length (in % of the intact limb length) (r=-0.538, p=0.031).
Posterior braking GRF peak was significantly smaller (d=0.81) for the amputees with hyposensitivity of the stump (n=9). This was also valid for the first peak of the vertical GRF (d=1.01) and for the vertical GRF in the midstance (d=0.88). The maximal values of GRF in anterior-posterior and vertical direction in the group with normal sensitivity of the stump (test for graphesthesia) were significantly greater (d=0.90-1.12) than in amputees with hyposensitivity.
There is a significant positive correlation between the length of the residual limb and the relative anterior propulsive GRF. The smaller vertical GRF in below-knee amputees on the prosthetic limb indicates less propulsion during walking.4 Amputees with the hyposensitivity of the stump loaded the prosthetic limb during walking less than amputees with normal sensitivity. Further studies with a larger number of patients are needed to validate these results.
1. Verhagen AP et al.; 1998; J Clin Epidemiol.
2. Kovač I et al.; 2009; Coll Antropol.
3. Majumdar K et al.; 2008; Online J Health Allied.
4. Vanicek N et al.; 2009; Gait Posture.
380
Rodney Lane (1,2) presenting Paul Chappell (1) Martin Matthews (2)
Saudi Arabia, University of Southampton, Southampton (1) UK, DM Orthotics Ltd., Redruth (2)
Treatment for paediatric dropfoot that combines elastomeric dynamic splinting with functional electrical stimulation (FES)
Standard dorsiflexion socks made by DM Orthotics Ltd. were modified to include panels of a newly developed trans-conductive polymer (EPSRC funded). The material is inert against the skin but allows conduction of FES stimulation from the outer surface, while being fully cleanable on the inner surface. The subjects were a 17 y.o. female with left-hemiplegia and a 14 y.o. male with right hemiplegia. Measurements were taken during walking: without intervention; with the splint without FES; and with both splint and FES. Data were captured for 3 concurrent, timed 10m walks with the steps counted and the physiological cost index (PCI) calculated.


Dynamic splinting showed greatest reduction in walking effort (PCI). The addition of FES increased stride length reducing cadence and further reduced effort of walking.
381
Kawa Hamdi (1) presenting Rozita jahanbin (1) Srood Suad Nafie (1) Ghassan Ali (1)
UK, ICRC, Erbil (1)
Evaluation of SACH foot provided by ICRC
Since 1979 the ICRC is doing a tremendous job to help PWD’s around the globe. In 2000 the ICRC decided to centralize the components production. One of these components is the (SACH) foot, which is used widely, regardless the progress and the recent innovations of different feet. It is the one used in Erbil physical rehabilitation center. Wooden keel in SACH foot was redesigned to adapt the ICRC Polypropylene (PP) technology and made of PP, the rest of the foot is made of polyurethane foam.
During daily prostheses maintenance work, the staff noticed that foot replacement is one of the main tasks. The staff undertook this pilot study to determine the main causes and affecting factors on this phenomena.
This study is carried out in Erbil PRC, the only ICRC run center in Iraq. Two type of factors affecting the foot life cycle were identified; factors related to the service users (age, gender, weight, occupation, living environment, amputation level and type of shoe used). And factors related to the product (prosthesis alignment, shelf life, production year and foot size). These factors were monitored and recorded during 4.5 months.
During the study period, out of 347 repairs done 163 cases were foot failure. The study reading shows that the active people (young 20-40 years old, male, TT amputees who work for 8 hours and more) are the most affected and possible candidates for feet failure. The average usage of foot before breakage was 18 months, which could be considered acceptable. As 44% (72/163) of the breakage happened the first 12 months, an investigation was done to find out the reasons behind that. Accordingly shelf life period, patient occupation and their working hours appeared to be the main affecting factors.

Uncontrolled storing conditions reduces foot life cycle, thus implementing ICRC technical recommendation for 18 months maximum allowed storage period is recommended. Active amputees should instructed to be more careful with their prosthesis. Last but not least, ICRC foot life cycle is within acceptable limit and recommended to be used.
382
Victor Nunes (1) presenting
Iraq, Ortoprotesia, V N Foz Coa (1)
3D Printed Prosthetic Test Sockets - Hi-tech for Low-cost

383
ZDENKA PIHLAR (1) presenting
Portugal, University Rehabilitation Institute, Ljubljana (1)
The effect of graded motor imagery on occupational performance of persons with phantom limb pain
Graded motor imagery (GMI) is a combination of implicit, explicit motor imagery, and mirror therapy. Explicit motor imagery means identifying whether a limb is left or right, implicit motor imagery means imaging movements and posture.Mirror therapy is the use of a mirror to present the reverse image of a limb to the brain, thus »tricking »the brain. The aim of this article is to determine if GMI helps reduce the experience of phantom limb pain ( PLP ) in patients and thus improves execution of activities and patients’ satisfaction in everyday occupations.
The study included 6 patients after unilateral upper limb amputation, who were experiencing PLP. GMI therapy took place over the course of four weeks. PLP was measured with Visual Analog Scale (VAS) prior starting with the GMI and after its completion. Canadian Model of Occupational Performance (COPM), was used to detect change in a patient’s self perception of occupational performance. Activity analysis was used to check performance and satisfaction with performance of activities before and after the implementation of GMI.
PLP has significantly reduced in all 6 patients following the GMI treatment. On average VAS grade has improved by 3.4 points. Average grading of performance and satisfaction with activity performance has risen from 2.9 to 7.2 and 2.9 to 8.6. Activity analysis demonstrated improvement in motor and process skills - energy levels, keeping the pace while carrying out certain activity and being effective.
GMI therapy has proved to be effective and suitable therapeutic treatment in patients with PLP. GMI reduces PLP and it improves patients’ performance and satisfaction with performance in defferent performance areas ; self care, productivity, and leasure.
1. Moseley GL, Butler DS, Beames TB, Giles TJ (2012). The graded motor imagery handbock. Adelaide : Noigroup.
2. Ramachandran VS, Altschuler EL (2009). The use of visual feedback, in particular mirror visual feedback, in restoring brain function. Brain 132 (7): 1693-710.
3. Longo MR, Betti V,Aagliotti SM, Haggard P (2009). 2Visually induced analgesia : seeing the body reduces pain. J Neurosci 29 (39) : 12125-30.4
384
Dominik Hepp (1) presenting Jan Kirsch (1) Thomas Engleder (1) Felix Capanni (1)
Slovenia, Ulm University of Applied Sciences, Ulm, Baden-Wuerttemberg (1)
Development of a smart phone supported upper limb prosthesis with eleven active driven degrees of freedom
State of the art upper limb prosthesis offer up to six active DoFs (degrees of freedom) and are controlled using different grip patterns. This low number of DoFs combined with a machine-human-interface which does not provide control over all DoFs separately result in a lack of usability for the patient.
Design of a novel upper limb prosthesis offering different control possibilities for changing grip patterns depending on the patients’ priorities. Development focused the improvement of grasp capability and the simplification of prosthesis control.
Design development followed the design process requirements given by the European Medical Device Directive 93/42 ECC and was structured into the three main topics mechanics, software and drive technology. First user needs were identified by literature research and by patient feedback. Consequently, concepts were evaluated against technical and usability requirements. Finally, a prototype was manufactured using rapid prototyping technology.
The prosthesis design enables two active (DC-motor) DoFs per finger (one is already realized), a segmented silicone linked mid-hand and a flexible and rotatable wrist. The control unit is connected to an Android based smart phone application using Bluetooth® technology. Two main grip patterns can be preselected in the software application and afterwards changed and used by the EMG signal (high level control). Three different control algorithms can be selected: “all-day”, “precision grip” and “tired muscle”. Further parameters can be adjusted to customize the prosthesis to the patients’ needs. The motor control unit (low level control) receives setpoints from the high level control unit through a bus-system and regulates the grasp-force applied by each DC-motor.

First patient feedback certified the prosthesis an improved level of handling compared to the existing devices.
In a first user feedback test, the smart phone based software application increased the device usability, e.g. the change within preselected grip patterns and the “tired muscle” algorithm.
Although the overall software application was positively rated, the handling of the prosthesis itself needs to be proven within a patient study to be performed next.
385
Wendy Hill (1) presenting Helena Burger (2) Darinka Brezovar (2)
Germany, Atlantic Clinic for Upper Limb Prosthetics, Fredericton, NB (1) Canada, University Rehabilitation Institute, Ljubljana (2)
Updated Version of UNB Test of Prosthetics Function – preliminary results
The UNB Test was developed in 1985 as a clinical and research tool to assess spontaneity and skill in the use of a prosthetic device. It was considered to be a valid, reliable, and clinically useful assessment at that time and continues to be used in many clinics. The test items have recently been updated and the test now includes an older age category for ages 13-21.
The aim of our study was to find out whether subtests of the updated version of the UNB Test were of equal difficulty and if the results could be compared between them.
All children and adolescents who visited the Atlantic Clinic for Upper Limb Prosthetics at the University of New Brunswick and the outpatient clinic for rehabilitation of children following upper limb amputation and upper limb prosthetics at University Rehabilitation Institute of Slovenia were included in this study. All included were randomly tested with all three age appropriate subtests. Results were statistically analysed using SPSS. Descriptive statistic and correlation coefficients were used. Study has been approved by the ethics committees of both institutions.
We had two children (4 tests) in the age group 2 – 4 years, two (5 tests) in the age group 5 – 7 years, four (9 tests) in the age group 8 – 12 years and 17 adolescents (29 tests) it the age group 13 – 21 years. In the age group 2 – 4 years we did not find correlation either for skill or for spontaneity between different subtests. In the age group 5 – 7 years there was correlation between subtests for skill (r1,2=.927, p=.023, r1,3=.822, p=.088, r2,3=.846, p=.071) but not for spontaneity of prosthetic use. In the age group 8 – 12 years there were high correlations between subtests for skill and spontaneity of prosthetic use (all r>.899, p≤.001). In the age group 13 – 21 years there were correlations between subtests for skill (r1,2=.846, p<.001, r1,3=.831, p<.001, r2,3=.787, p<.001) and spontaneity of prosthetic use (r1,2=.882, p<.001, r1,3=.749, p<.001, r2,3=.369, p=.053). Ceiling effect has been observed in up to 11 tests for spontaneity but not for skill of prosthetic use.
We found that in the age groups 8 – 12 and 13 – 21 years, subtest one and two are comparable whereas the comparison with subtest three is not as well correlated, especially for spontaneity, where a high number of included children got the maximal score in subtest three. For the age groups 2 – 4 and 5 – 7 we do not have enough included children to draw any conclusions. More children and further studies are needed to complete all the psychometric testing of the new version of UNB test, but due to these preliminary results it is a promising tool for assessing prosthetic function in children and adolescents.
Sanderson E, Scott R. UNB test of prosthetic function: a test for unilateral amputees (test manual). Fredericton (Canada): University of New Brunswick; 1985.
386
Merkur Alimusaj (1) presenting Daniel W.W. Heitzmann (1) Julia Block (1) Sebastian I. Wolf (1)
Slovenia, Clinic for Orthopedics and Trauma Surgery Heidelberg University Hospital, Heidelberg (1)
Sudden change in walking direction in trans-tibial amputees: Functional effects of a rotational unit in a prosthetic foot
Turning is a mandatory task to move freely within environment. It has been shown that approximately up to 50% of the steps indoors can be recognized as a turning manoeuvre [1]. As conventional prosthetic feet do not offer an explicit degree of freedom in the transverse plane, rotational moments are expected to be a particular challenge for trans-tibial amputees (TTA).
Do TTA benefit from a rotational adapter integrated in a prosthetic foot during a randomized, cued turning task?
Repeated measurements with two feet (Variflex XC Rotate; Össur, Iceland) similar in appearance, geometry, category, size and alignment except for rotational adapter (full functional adapter [FA] placebo adapter [PA]) were conducted to identify differences. 10 unilateral TTA (45y±17; 178cm±8; 76kg±12) were investigated using the PA and FA foot while randomly turning in a 45° angle either left or the right indicated by a visual cue, triggered by a photoelectric switch. Sequence of PA and FA measurements was randomized and TTA were blinded for the foot investigated. Kinematics and kinetics were collected by means of 3D gait analysis (Vicon) [2]. Data of 10 unimpaired subjects (33y±10y; 179cm±9; 72kg±17) served as reference. Statistical significance between feet was tested by using Wilcoxon-Signed-Rank test (p<0.05).
Turning either resulted in a step or spin-turn strategy as previously described in the literature [3]. TTA showed relevant changes in the lower limb positioning while turning compared to reference subjects (p<0.05). A pronounced internal rotated prosthetic foot during step-turns and a pronounced external rotated foot during spin-turns were seen, while pelvic rotation did not change compared to reference group. The rotational adapter showed significant motion during spin and step-turns (p<0.05; fig.1) without a significant effect in involved sides transverse plane moments of the hip, knee and prosthetic ankle (p>0.05). Motion during FA condition (fig.1) could be contributed to noise of marker trajectories [4]. PA condition movement of the rotational adapter is still significant considering this effect.

Kinematic Data shows a significant reaction of the rotational adapter in the FA condition during turning manoeuvres in both, step – and spin turn. As this did not significantly affect transverse plane moments of the hip, knee and ankle joint, neither with the PA nor the FA foot it can be hypothesized, that the changes indicate a reduced rotational motion between socket and stump in FA condition. Therefore a prosthetic component which introduces an additional degree of freedom in the transverse plane might lead to a reduction of rotational movement between stump and socket. This is directly associated to a reduction in shear stress and therefore can be beneficial for the user.
[1] Glaister BC, et al., Gait & posture 2007;25;289-94.
[2] Kadaba MP, et al., J Orthop Res 1990;8;383-92.
[3] Hase K, Stein RB.,J of neurophysiology 1999;81;2914-22.
[4] Richards JG. Human Movement Science 1999;18;589-602.
387
Bernhard Kleiner (1) presenting Anna Grasenack (1) Urs Schneider (1)
Germany, Fraunhofer Institute for Manufacturing Engineering and Automation IPA, Stuttgart (1)
Laser and radar based terrain recognition enables comfort and safety for stair walking with active lower limb prosthesis
Today’s modern prosthetic devices for the knee and ankle joints are actively able to change the gait behavior. These devices are controlled by different states derived from gait speed patterns. States are switched by considering the current motion and the reaction forces on the ground. Despite all of this, approximately 70% of all above-knee amputees still fall once per year. This is mostly caused due to the patient stumbling over undetected obstacles not recognized by the software.
The aim of this paper is to enhance the adaptability of the prosthetic device in unknown terrain through structural information obtained a priori. Such structures are obstacles on the ground, ramps or stairs.
We use wearable distance and inertial measurement sensors inside the prosthetic device to constantly detect different objects in front of the user. Normally a 2D laser scanner generates a three dimensional point cloud using vertical movement of the prosthetic devices during gait. Objects are detected by using shape fitting algorithms. Therefore the position and orientation of the prosthesis is measured continuously using information obtained through inertial measurement sensors and a sensor fusion filter. However laser cannot measure through trousers, which might cover the sensors. Therefore we want to introduce a mobile compact 94GHz radar sensor, which is capable of replacing the laser based system.
We conducted measurement tests to compare the laser and the radar sensor for the task of stair detection. The laser and the radar sensor were mounted on a lower limb prosthesis and moved during a patients gait. On the one hand stairs with a minimum height of 5cm could be detected by the laser sensor. On the other hand the radar sensor with a single lens does not provide rich 3D structure data. But instead it could identify even smaller stairs and the distance of the stairs by analyzing received deterministic reflection patterns. Figure 1 shows the result of a stair depth measurement with an accuracy of 1.5cm.

Radar signal with distance and depth information of 5 stairs
This paper demonstrates the world’s first usage of wearable radar sensors for terrain detection in lower limb prosthetic devices. When the laser sensor approach was introduced in 2011 detecting small stairs was difficult [1]. Therefore wearable radar devices could be complementary or even replace sensor technology for the task of forward-looking terrain adaption.
[1] Kleiner, Bernhard 2011. Foresighted control of active foot prostheses. Technically Assisted Rehabilitation Conference TAR 2011. Technically Assisted Rehabilitation Conference TAR 2011, 2011, in Berlin. http://www.tar-conference.de/.
388
Kate Lancaster (1) presenting
Germany, St Georges NHS Trust, London (1)
Treatment of Phantom Limb Pain using Graded Motor Imagery – a Case Study
Phantom Limb Pain (PLP) is a debilitating and common phenomenon after amputation which in the past has been poorly understood and difficult to treat. Graded Motor Imagery (GMI) evolved as a treatment approach borne from a growing understanding of the underlying neurobiology of complex pain states such as PLP. GMI is a graded treatment approach to re-educate the brain to normalise signals it receives so as not to interpret them as pain when the body is no longer in danger.
To manage PLP by using the GMI treatment technique, give the patient tools to control their pain and manage any future flare ups of PLP.
A case study working with Mr S, who had suffered with extreme PLP since his amputation 8 years previously. He had tried many different techniques to treat PLP but with little / no success other than over medication when experiencing an extreme flare up. The McGill Pain assessment and pain Visual Analogue Scale (VAS) was collected at baseline and regular intervals throughout treatment. Treatment took place over seven months.
Mr S’s treatment included the three different components of GMI: left/right laterality, motor imagery and mirror therapy. Each stage allowed for a gradual increase in the firing of the brain regions involved. Grading occurred from one stage to the next and within each stage.
After seven months of almost weekly GMI treatment sessions plus homework, Mr S’s baseline PLP VAS score reduced from 6/10 to 2/10 and his McGill pain score reduced from 44/78 to 6/78. At initial assessment, the patient reported to being woken around twice a night by PLP, but after four months of treatment, this had reduced to 1-2 times per week. By his final review, he was on reduced pain medications (consultant lead) and reported that the PLP no longer controlled him. His extreme flare ups had reduced from 3-4x per month to approximately 1-2 every 2 months and he was only being woken very occasionally. Mr S also reported more vivid normal sensation in his phantom and was now able to move his phantom limb from full flexion to -30° extension. Previously his phantom limb was fixed in full flexion. At 3 months follow up, these results remained.
GMI can be an effective treatment method for patients suffering from PLP. However, the patient needs to fully understand how the brain interprets pain and that it is the brain that needs to be re-educated to change its interpretation of a perceived threat. The treatment requires patience, persistence, courage and commitment.
Moseley, Butler, Beames, Giles. Graded Motor Imagery Handbook. Adelaide 2012
Neuro Orthopaedic Institute (NOI) – www.noigroup.com
389
Kate Lancaster (1) presenting
UK, St George’s NHS Trust, London (1)
A Balance Circuit Group for Amputees to Reduce Risk of Falls
1 in 3 adults over 65 years fall each year and with the added risk factor of an amputation, amputees are at an even higher prevalence of falling. BACPAR reports 20-53% of amputees experience a fall once a year. Reduced flexibility, strength, reaction time and poor balance are some risk factors which can be addressed through exercise. Otago is an evidenced based exercise programme to reduce falls in elderly and can reduce falls by up to 54%.
To implement a balance circuit class into the week’s timetable to improve confidence, strength, balance and fitness to reduce risk of falls as part of falls prevention management of amputee patients currently receiving prosthetic rehabilitation.
A circuit class based on the Otago exercises was set up for our amputee patients. The Otago exercises have been adapted to ensure that all patients are able to complete each type of exercise regardless of level of amputation or whether they have a prosthesis or not. The class is run once a week for an hour including 10 minutes warm up and down and 2 minutes at each station. There are a minimum of ten exercise stations which try to address all of BACPAR’s recommendations for reducing falls risk.
An outcome measure was initially developed based on Berg Balance Scale and the AmpPro, but it was deemed unsuitable as patients may start the class without a prosthesis, but be discharged with a prosthesis. Also, patients would be performing many of these exercises separately as part of their week’s physiotherapy and therefore there were too many variables to measure the class effectiveness alone. Therefore, a subjective questionnaire was developed for patients to complete at discharge. The majority of patients have reported to enjoying the class, improving their balance and learnt exercises that they will continue with after discharge.
Fear of falling is recorded at initial assessment, at discharge, at 6 week review and 6 month review.
Results from the subjective patient questionnaire have been inconclusive. Patients who report an increase in fear of falling at discharge; it is thought that as their mobility has increased from wheelchair to prosthesis, so their fear of falling has increased. The class has been a fun addition to the week’s timetable and has found that the circuit works the patients harder in a sustained, challenging and safe manner.
390
Claudia Mondragón (2) Julio Reyes Ortega (1) presenting Juan Manuel Zuluaga (1) Claudia Perez (1)
UK, Instituto de Ortopedia Infantil Roosevelt, Bogotá (1) Colombia, Universidad de la Sabana, Bogotá (2)
Reciprocating gait prosthesis for the total transverse deficiency of bilateral thigh: case report
Physical examination: normal neurological development, preserved upper limb mobility, muscle strength 5/5, 0/4 muscle tone, total transverse deficiency of the bilateral femur, sensitive preserved, makes independent movements on stumps.
Reciprocating gait prosthesis fitting was performed; initially received training with the pelvic basket system and stubbies. After that the lap belt was adapted and height increased progressively with balance training. The adaptation of knees was made and the final height with anthropometric tables for age was determined. Finally we designed the cosmetic cover and conducted gait training with anterior walker.

391
Gerwin Smit (1) presenting Maurice A. LeBlanc (2,1) Dick H. Plettenburg (1)
Colombia, Delft University of Technology, Delft (1) The Netherlands, Stanford University (retired), Stanford (2)
Hydraulic transmission applied to body powered upper limb prostheses, as an alternative to the Bowden cable
The operating force an input energy of a Body Powered (BP) upper limb prosthesis should be low, to enable comfortable control of the device by the amputee. The mechanical efficiency of a BP system must be high and therefore internal friction ought to be as low as possible. The Bowden cable used in current BP devices, is a significant source of inefficiency. The internal friction of the Bowden cable increases with an increasing bend angle of the cable. A hydraulic transmission could be a more efficient alternative, as its friction is independent of the bend angle in the tubing [1].
The aim of this study was to measure and compare the mechanical input energy required for a BP system, using either a Bowden cable transmission, or a hydraulic transmission, combined with standard available terminal devices (TD’s).
Two commercially available TD’s were used: a voluntary closing TRS Hook and an Otto Bock VO hand. In the first test both devices were actuated using a Bowden cable (steel cable, Teflon liner). The cable was bended around a cylinder (diam. 150 mm), at increasing angles (0°, 90°, 180°, 270°, 360°). In the second test a hydraulic transmission was used, with custom-made hydraulic cylinders. (bore x stroke = 7.5 x 55 mm). Forces and displacements were measured, using a mechanical test bench. The applied input work was calculated, together with the hysteresis (workin-workreturend).
Table 1 shows the input work of the Bowden cable and the hydraulic transmission, for both TD’s, at increasing bending angles of the cable.
Input work of both terminal devices, combined with the Bowden cable and the hydraulic transmission, at different cable bending angles.

The testing shows that the efficiency of the cable system decreases as the bend in the cable increases, whereas the efficiency of the hydraulic system remains constant. For the OB Hand the required input energy is lower for angles larger than 90° (e.g. in activities like putting something in your mouth). For the TRS the input energy of the Bowden cable is the lowest for all angles.
1. LeBlanc, M, “Current Evaluation of Hydraulics to Replace the Cable Force Transmission System for Body-Powered Upper-Limb Prostheses”, Assistive Technology, Vol. 2.3, 1990.
394
Gordon K. Ruder (1) presenting Joyce Tryssenaar (2) Daniel P Blocka (1)
Iraq, George Brown College P&O Programs, Toronto, Ontario (1) Canada, McMaster University, Masters in Rehab Sciences, Hamilton, Ontario (2)
George Brown College Prosthetic & Orthotic Programs and McMaster University MSc in Rehabilitation Sciences Collaborative Model: Exciting Next Steps
The George Brown College Prosthetic & Orthotic (GBC P&O) programs have supplied professional personnel to the Prosthetic and Orthotic profession for over forty years. In 2010, British Columbia Institute of Technology’s Prosthetics and Orthotics Program, GBC’s P&O post graduate program, and McMaster University’s Masters of Science in Rehabilitation Science program signed a Memorandum of Understanding, and created an optional Cooperative Curriculum model designed to address the emerging educational needs of the Prosthetics and Orthotics profession.
As of 2015, a Masters degree is required to attain professional certification in USA, a tendency that is also occurring globally. There is a recognized need for P&O Schools in Canada to do the same. The aim of this presentation is to present the rationale behind the need and the means to evolve the current educational model to the next phase.
- Review of demographic studies performed across Canada and the United States over the last 2 decades.
- Review of the number and calibre of applicants/graduates to the GBC P&O Programs.
- Past 4 years of “Key Performance Indicators”, collected by the provincial ministry of training, colleges and universities.
- Presentation of new survey based research involving 15 co-enrolled students of the GBC P&O and McMaster MSc (RS) Programs.
- Demographic studies have accurately predicted that there is a growing gap between the supply and demand of clinicians. As more of our work force reaches retirement, this trend will accelerate.
- The number and calibre of applicants to both, but especially the clinical program has steadily increased over the last few years, but the enrolment/graduation rates have been constant.
- Feedback on the student’s educational experience clearly show how well the students perceive their education, value the skills, and find the program prepares them for the P&O profession. They also demonstrate a 100% retention.
- Survey results from 15 current co-enrolled GBC P&O and MSc (RS) students is expected to provide critical information on how the optional cooperative model has faired and directions that should be taken to improve it further.
- Demographic trends collected demonstrate a pressing need to increase enrolment.
- Applicant trends suggest that there would be a high quality applicant pool if the class size increases.
- Give experienced MSc P&O practitioners oppourtunities to take on teaching roles within both educational programs.
- Using the information gathered, complete another mapping exercise to improve collaborative model.
- Host another stakeholders meeting with students, faculty, administrators, employers, patient groups, national and international professional bodies. Use their expertise, and the results of this study to help shape the next phase of a Masters Prosthetics and Orthotics Cat-I Program.
395
Hans-Rudolf Weiss (1) presenting Sarah Seibel (1)
Canada, Spinal Deformities Rehabilitation Services, Gensingen (1)
AIS and the Sagittal Profile – Do modern CAD / CAM Braces increase Flatback?
Scoliosis braces usually increase flatback deformity and lead to a deterioration of the sagittal profile. The new generation of Chêneau based CAD / CAM braces (GBW) includes corrective forces to correct the sagittal profile.
Purpose of this investigation was to test the outcome of the GBW brace with respect to the influence on the sagittal profile.
All patients with Adolescent Idiopathic Scoliosis (AIS) with a CBW brace and a follow-up period of at least 12 months from our data base of patients as evaluated with surface topography (Diers Formetric) have been included. There were 58 patients fulfilling the inclusion criteria (Age 12.9 years; Cobb 32.9°; follow-up 22.6 months.) Kyphosis and lordosis angle before bracing was compared with the last investigation as recorded.
Average kyphosis angle decreased slightly from 45 to 44.5° (p = 0,79), average lordosis angle increased from 37.2 to 38° (p = 0,67). Statistically there was no difference.
There is no influence of the new generation of Chêneau based CAD / CAM braces on the sagittal profile as measured by surface topography. This although these braces clearly provide a correcting force with respect to the sagittal profile. Surface topography, however does not provide comparable measurements of the sagittal profile as the lateral x-ray, therefore the findings from this study may have been compromised by this fact. A study based on x-rays would lead to an unnecessary exposure of the patients. In conclusion, the sagittal profile is not corrected in todays modern scoliosis braces when measured by surface topography. Possibly, surface topography is not appropriate for detecting the real sagittal profile in the region of interest. Surgery is the only treatment leading to a proven correction of the sagittal profile in the x-ray but at the cost of total loss of function in the region fused.
396
Lucas Lincoln (1) presenting Kim Corson (1) Chris Villarosa (1) Michael Orendurff (1) David Boone (1)
Germany, Orthocare Innovations, Mountlake Terrace, WA (1)
Validation of direct measurement of sagittal moments during walking for individuals with transtibial limb loss
Direct measurement of the moments applied to the prosthetic limb during gait offers a novel and comprehensive assessment of the loads applied in real world settings. Currently, the moments applied to the prosthetic limb during gait are usually calculated by inverse dynamics in a computerized gait analysis laboratory. If a method for collecting the moments directly on the prosthetic limb could be validated, measurement of the kinetics of gait in the real world could inform clinical decision-making, outcomes assessments and prosthetic prescription effectiveness.
The aim of this study is to compare the sagittal moments at the prosthetic ankle during walking in a gait analysis laboratory to the moments measured by a sensor directly within the prosthetic limb.
Four individuals with transtibial limb loss gave informed consent to participate in this study. Sagittal moment data for 5 walking trials was collected with an 8-camera Vicon MX (120Hz) with 2 AMTI force plates (1200 Hz). Data were processed in Visual 3D and sagittal moments were calculated at the location of a moment sensor placed directly on the prosthetic pylon just above the prosthetic foot. Stance phase sagittal moment data calculated by inverse dynamics in Visual 3D was compared to stance phase sagittal moment data measured by the sensor (Smart Pyramid) directly in the prosthetic limb using linear regression.
Sagittal moment data across stance phase appears closely aligned when comparing inverse dynamics to direct measurement. R2 values ranged from 0.93 to 0.99 across all participants and all trials (>1900 paired samples total).

The source of difference observed between the two measurements may be a coordinate transformation. Inverse dynamics computes moments at locations estimated by reflective marker placement, whereas the direct measurement tool has its own coordinate system – errors in locating either will propagate. These data suggest that sagittal moment data collected directly on the prosthetic limb during real world ambulation are acceptably similar to sagittal moments collection during walking in the gait analysis laboratory.
400
Vibhor Agrawal (1,2) Robert Gailey (1) presenting Knut Lechler (3)
Thailand, University of Miami, Miami, FL (1) USA, Miami VA Medical Center, Miami, FL (2) USA, Ossur, Reykjavík (3)
A comparison of powered and non-powered prosthetic knees during sit-to-stand and stand-to-sit activities of unilateral transfemoral amputees

[1] Agrawal; 2013 ISPO conference.
[2] Burger; 2005 Prost Orthot Int. 2005.
[3] Agrawal; 2011 Ergonomics
402
Christina Ragnö (1) presenting Anita Stockselius (1)
Germany, RehabCenter Sfären, Bräcke Diakoni, Stockholm (1)
Clinical development and use of AHA-PAD (Assisting Hand Assessment- Prosthetics, Amputations, Deficiencies)
Assisting Hand Assessment (AHA) is an instrument that measures and describes the effectiveness with which the child or adult with one well-functioning hand and one paretic hand uses the effected hand in bimanual activity. Upper extremity unilateral amputations and congenital deficiencies have similar problems.
We were interested in evaluating how patients were using their prosthesis or their affected arm. The original criteria for scoring did however not work well for our patients. Assisting Hand Assessment for Prosthetics, Amputations, Deficiencies
(AHA – PAD) was therefore developed for this patient group.
The aim of the presentation is to describe our material collected during the development of AHA-PAD research version and to describe how the assessment has been useful in clinical work.
In AHA-PAD the patient performs an age-related, standardized activity which is video recorded. The activities are carefully selected to challenge the assessed hand or prosthetic function.
The video is then assessed in 20 different items on a 3-point scale. For adults the two activities are to make a sandwich or a present. For the children toys in a test kit is used for explorative play or to play a board game. The AHA-PAD score form was used to gather data and descriptive analysis were undertaken.
- 53 patients (25 children and 28 adults) from our clinic with below elbow amputation or congenital deficiencies on hand or distal part of the arm, has participated in the study. Of the traumatic amputated 10 was amputated on the right side and 6 on the left side. Unlike the amputated patients the patients with congenital deficiencies were 28 on left side and 9 on the right side. A total of 86 videos were scored. We found that the cosmetic user scored between 44 and 60 % and the myoelectric users between 43 to 74% of the maximum AHA score.
We will also report AHA-PAD results related to:
- Time of prosthetic daily use .
- Different types of prosthesis
- The same patient with different kind of prosthetics or without prosthesis
- Use of armprosthesis on dominant or non-dominant hand
AHA – PAD is an instrument developed for all kinds of unilateral partial hands or below elbow amputations or deficiencies with or without prosthesis. In clinical work, the lack of valid instruments is a weakness when we want to describe our training results and how our patients performed activities.
The instrument gave us a terminology in describing how the patient managed to perform bimanual activities.
We also found that the instrument gave us information of what was needed for further skill training.
403
Lynsey Duff (1,2) presenting David Tang (1) Rhodri Phillip (1)
Sweden, DMRC Headley Court, Surrey (1) UK, NHS Lothian, Edinburgh (2)
Examination of Amputation Technique in Knee Disarticulation Amputees
Knee disarticulation (KD) amputees comprise 1% of the amputee population in the world1. Due to the small number of knee disarticulation amputations performed, the amputation technique is inconsistent.
The purpose of this investigation is to examine the preferred technique for KD amputation with regard to patella preservation and assess if removing the patella reduces the need for revision surgery.
A total of 49 KD amputees were identified; 17 unilateral KD and 32 bilateral amputees with 10 of those being bilateral KD. X-rays following original amputation were examined to confirm amputation technique with regards to preservation or removal of patella. This information was cross-referenced with the surgical notes. Clinical records were then examined to assess if revision surgery was required and the cause of revision surgery noted.
Out of the 61 KD amputations examined, x-rays were available for 43. The patella was left in situ in 60% (n=26) of the KD amputations and 38% (n=10) of those required revision surgery. Of the 38% that had revision surgery, 40% (n=4) had revision surgery due to problems caused by the patella.
The results indicate it is more common to leave the patella in situ than remove it in KD amputation.
If the patellae had been removed in all of those examined, the need for revision surgery may have been reduced by 29%.
There is insufficient data to provide a recommendation of amputation technique in knee disarticulation. A larger population is required to draw more definitive conclusions.
1. The Paediatric Orthopaedic Society of North America (2014) A Manual for the Rehabilitation of People with Limb Amputation [Online] 2004. Available from- http://www.posna.org/news/amputations.pdf [Accessed: 23.05.14]
404
Lynsey Duff (1,3) presenting Hannah Jarvis (1,2)
UK, DMRC Headley Court, Surrey (1) UK, University of Salford, Manchster (2) UK, NHS Lothian, Edinburgh (3)
Walking speed and Oxygen Consumption of a Unilateral Hip Disarticulation Amputee during Level Walking Using a C-leg vs a Genium
With technological advances in prosthetics, more intuitive componentry has been developed that aims to give the user a more natural and energy efficient gait.
It has previously been observed that hip disarticulation amputees use more energy to ambulate than their able-bodied counterparts1-3.
The aim of this investigation is to compare the oxygen consumption and walking speed of a unilateral hip disarticulation amputee walking on level ground with a helix hip joint in conjunction with a C-leg and a Genium.
One unilateral hip disarticulation amputee gave informed consent to participate.
The participant walked for 5 minutes using the C-leg at their self-selected walking speed and oxygen consumption was measured with the last minute used for analysis. The data collection procedure was repeated with the Genium 4 weeks later. The knee unit was the only prescription variable between sessions.
The participant walked at 0.74m/s with the C-leg and 0.80m/s with the Genium. Oxygen consumption was similar with both knee units. The energy cost of walking reduced with the Genium (0.31) in comparison to the C-leg (0.34).

Comparison of walking speed, oxygen consumption, oxygen cost in unilateral hip disarticulation patient wearing C-leg or Genium.
The results indicate that the amputee in this study consumed less oxygen when walking at similar speeds to that previously reported. When walking with the Genium, the participant walked faster and used less oxygen in comparison to the C-leg. The participant also preferred walking with the Genium. Further data collection and a more detailed analysis is ongoing.
1. Schnall et al. Gait characteristics of a soldier with a traumatic hip disarticulation. Phys Ther. 2008; 88:1568-77
2. Chin et al. Energy consumption during prosthetic walking and physical fitness in older hip disarticulation amputees. J Rehabil Res Dev. 2012; 49(8): 1255-60
3. Perry J. Gait analysis: Normal and pathological function. 1st ed. Thorofare, NJ: Slck Inc; 1992
405
Axelle Mokry (1) presenting Isabelle Urseau (1) Graziella Lippolis (2)
UK, Handicap International Federation, Lyon, Rhône (1) France, Handicap International Federation, Brussels (2)
Development And Pilot Testing An Assessment Tool On Human Resources For Prosthetics/Orthotics And Rehabilitation Professions In Developing Countries
The shortage of health workers worldwide is identified as a critical constraint to the achievement of health and development goals. In 2010, a rehabilitation survey, including Prosthetics/Orthotics (P/O), was conducted by Handicap International (HI) and the African Federation of Orthopaedic Technicians (FATO) across 29 countries. This survey explored three areas: country overview, distribution of P/O and rehabilitation services and human resources (HR). The HR component was the least complete in terms of responses, creating limited data opportunity for analysis.
To develop and test a new tool for measuring status, professional development and follow-up of P/O and other rehabilitation professionals within Low and Middle Income Countries (LMICs).
To generate evidence for increasing recognition and training of P/O and rehabilitation professionals.
Based on data from the first survey, gaps identified and international recommendations and guidelines (WHO HRH, UNCRPD) a questionnaire on HR (initial and continuous education, regulation and migration) was developed for P/O, physiotherapists, occupational therapists professions and their respective intermediate levels. A user manual was developed to support the person undertaking the survey in order to improve the quality and quantity of data. The questionnaire and user manual were reviewed and agreed by an expert panel (pre-testing). Focal persons from FATO and HI were identified in Senegal, Kenya and Odisha province (India) and tasked to undertake pilot testing of the questionnaire.
Senegal and Kenya sent completed pilot questionnaires. The tool was updated based feedback from the pre-test and test results. Collating the data collected into a reference table allowed for easier comparison between areas/professions/countries. Data was also collated with existing information from countries, international agencies and some previous rehabilitation profession body survey.
The level of information collected through this tool was of greater quality than the initial survey and satisfaction of the focal persons undertaking the pilot testing was good. However, with countries involved in this test being so few, applicability to other countries may be limited and further adjustments to the tool may be required.
The tool has the potential to be of great application for measuring P/O and rehabilitation HR in low and middle income countries. A second test including a wider and more diverse range of countries is therefore recommended. The creation of a HR P/O data-base would be very useful allowing cross analysis with ISPO standards e.g. education as well as discussion with the International Labour Office (ILO) on the International Standard Classification (ISCO) classification.
406
Helmut Diers (1) presenting Marco Kleist (2) Katrin Gerlach (2) Philipp Drees (3)
Belgium, DIERS Research & Development, Schlangenbad, Hessen (1) Germany, DIERS International GmbH, Schlangenbad, Hessen (2) Germany, Universitätsmedizin Mainz, Mainz, Rheinland-Pfalz (3)
Analyzing Spinal Movement In Patients With Pes Cavus
Two-paired T-Tests for each spinal part comparing sample and normative group resulted in the following p-values: For Lateral Deviation: p(TH): 0.001 (α: 0.999); p(TL): 0.067 (α: 0.9); p(L): 0.66 (n.s.). For Vertebral Rotation: p(TH): 0.108 (α: 0.9); p(TL): 0.582 (n.s.); p(L) 0.383 (n.s.)

[2] Huysmanns, T. (2004); Katholik Universität Leuven
[3] Gipsmann, A. (2014); Advances in Medicine, 2014
407
HORTENSIA MALLYA (1) presenting
Germany, TATCOT, MOSHI (1)
Prosthetics And Orhotics Human Resource Gaps In Tanzania
WHO and ISPO 2005, Guideline for Training for Personnel in Developing countries Prosthetics and Orthotics Services
WHO, 2011, World Report on Disability
408
Xavier Bonnet (1) presenting Francis Djian (1) Boris Dauriac (2) Coralie Villa (3) Isabelle Loiret (4) Noel Martinet (4) Helene Pillet (2)
Tanzania, PROTEOR, Seurre (1) France, Institut de Biomécanique Humaine Georges Charpak, Arts et Métiers ParisTech, Paris (2) France, CERAH INI, Woippy (3) France, IRR, Nancy (4)
Preliminary evaluation of a Microprocessor-controlled Knee Ankle Prosthesis (MKAP) for above knee amputees

409
Saffran Moeller (2) presenting
France, Division of Physiotherapy Department of Medical and Health Sciences, Linköping (1) Sweden, Össur Academy, Uppsala (2)
Can rehabilitation for lower limb amputees be more efficient using an active prosthesis?
solution enhanced rehabilitation, independence and mobility. This offers an alternative to existing traditional solutions for prosthesis component selection during rehabilitation of LLAs.
1. Asano et al (2008) Prosthet Orthot Int.
2. Fortington et al (2012) JAMDA
3. Miller et al, (2004) Disability and Rehabilitation.
410
Veerle Creylman (1) presenting Ingrid Knippels (1) Paul Janssen (1) Evelyne Biesbrouck (1) Knut Lechler (2) Louis Peeraer (1,3)
Sweden, Mobilab, Thomas More Kempen, Geel (1) Belgium, Ossur hf, R&D Medical Office, Reykjavik (2) Iceland, Department of Rehabilitation Sciences, KU Leuven, Leuven (3)
Assessment of transfemoral amputees using a passive microprocessor-controlled knee versus an active powered microprocessor-controlled knee for level walking
In transfemoral (TF) amputees, the forward propulsion of the prosthetic leg in swing has to be mainly carried out by hip muscles. With hip strength being the strongest predictor for ambulation ability, an active powered knee joint could have a positive influence, lowering hip loading and contributing to ambulation mobility. To assess this, gait of 4 TF amputees while walking with the Rheo Knee (Össur, Reykjavik, Iceland), a passive microprocessor-controlled prosthetic knee (P-MPK), was compared to their gait while walking with the Power Knee (Össur, Reykjavik, Iceland), an active microprocessor-controlled prosthetic knee (A-MPK). Furthermore, to assess long-term effects of the use of an A-MPK, a four-week follow-up case study was performed.
The aim of this study was to determine the difference between the P-MPK and the A-MPK in spatio-temporal and kinetic parameters for both the sound and the prosthetic limb during level walking.
The kinetics and kinematics of the gait of 4 TF amputees were assessed while walking with subsequently the P-MPK and the A-MPK. In one case study, a follow-up study was performed: one subject used the A-MPK for four weeks, while gait was measured weekly and the satisfaction over time was evaluated.
The range of motion of the knee was higher for as well the prosthetic as the sound leg in the A-MPK compared to the P-MPK. Maximum hip torque (HT) during early stance increased for the prosthetic leg and decreased for the sound leg with the A-MPK compared to the P-MPK. During late stance, the maximum HT decreased for the prosthetic leg. The significant difference between prosthetic and sound leg for HT disappeared when using the A-MPK. Also, an increase in stance phase duration was observed. The follow-up study showed an increase in confidence with the A-MPK over time. Results here also suggest that a certain time is needed to adapt to the A-MPK: for the first three weeks, the maximum HT during early stance decreased for PL and the maximum HT during late stance decreased for the SL.
Results indicated that, partially due to an induced knee flexion during stance, HT was diminished when walking with the A-MPK compared to the P-MPK. The single case follow-up study showed positive trends indicating that an adaptation time is beneficial for the A-MPK.
411
Jean-Loïc Rose (1) presenting Pascal Genevois (1) Gregory Notin (3) Julie Deceuninck (2) Jean-Claude Bernard (2)
Belgium, Orten, Lyon (1) France, Massues Rehabilitation Center, Lyon (2) France, Lecante, Lyon (3)
Dynamic surface asymmetry analyzing external deformity in scoliosis

[1] Komeli, A. Et al., Surface topography asymmetry maps categorizing external deformity in scoliosis, The Spine Journal, 2013.
[2] Berryman, F. et al., A new system for measuring three-dimensional back shape in scoliosis, European Spine Journal, 2008
412
Kris Cuppens (1) Ingrid Knippels (1) Mario Broeckx (1) Tom Saey (1) Inge Van den Herrewegen (1) Stijn Luca (2) Luc Labey (3) Louis Peeraer (1,4) presenting
France, Mobilab - Thomas More University College, Geel (1) Belgium, KU Leuven - Department of Electrical Engineering, Kasteelpark Arenberg 10, Leuven (2) Belgium, KU Leuven - Mechanical Engineering Technology TC, Geel (3) Belgium, KU Leuven - Department of Rehabilitation Sciences, Leuven (4)
Reliability and usage of clinical parameters for foot assessment
Different methods and protocols are used in clinical practice to analyze feet. The selection of the method mainly depends on the experience of the clinician. Generally, static measurement techniques such as podoscopy or blueprint are used. Furthermore, experts with different clinical backgrounds assess feet differently, not only in terms of methods but also in terminology. We asked nine experts to assess the feet of a single group of healthy subjects and performed a statistical analysis.
We want to get insight in the way different experts analyze feet, and determine which clinical features are the most reliable and the most relevant in our group of subjects.
We recruited 77 healthy subjects (40 male and 37 female) between 19 and 61 years old (average: 33 years). All subjects were clinically investigated by 9 experts: 3 podiatrists, 5 certified prosthetist/orthotists (CPO) and 1 foot surgeon. All experts used the techniques they would normally use in their practice. They noted the results of their analyses on a preformatted form (9 forms per subject) from which clinical foot features were extracted. These clinical features were determined by assessing foot mobility, the static foot (e.g. longitudinal arch height, calcaneus position), and the dynamic foot (e.g. initial contact location, base of gait). In total 67 features were assessed.
First, we investigated the reliability of the different clinical features. To this end, we used kappa statistics and a measure to evaluate the agreement, discriminative power and the relevance of the feature. These quality measures showed that there were 12 reliable clinical features and 9 fairly reliable features. Two of the most reliable features were the pressure area of the midfoot and height of the longitudinal arch, while e.g. the flexibility of the chopart joint and the initial contact location (medial or lateral) showed fair reliability. In a second investigation we searched for differences between the types of experts. In some clinical features, such as the range of motion of the subtalar joint, we found there was good agreement within a group of similar experts, but a clearly lower agreement over all experts combined.
The difference in agreement for some of the assessed clinical features may indicate that the types of experts assess these features differently. However, the number of experts is not large enough to draw strong conclusions. In this study we defined the most reliable clinical features for the clinicians to get more insight in their assessment of feet. In a next step we want to relate the qualitative clinical assessment to quantitative measurements, as we measured the subjects also with different measurement equipment such as a 3D motion capturing system.
413
Ilse M.F. Lankhorst (1) presenting Erwin C.T. Baars (1) Iris van Wijk (3) Wim G.M. Janssen (4) Margriet J. Poelma (5) Corry K. van der Sluis (2)
Belgium, Vogellanden, Center for Rehabilitation, Zwolle (1) The Netherlands, University of Groningen, University Medical Center Groningen, Department of Rehabilitation Medicine, Groningen (2) The Netherlands, Department of Rehabilitation Medicine, Rehabilitation Center de Hoogstraat, Utrecht (3) The Netherlands, Department of Rehabilitation Medicine, Erasmus Medical Center, Rotterdam (4) The Netherlands, Department of Rehabilitation Medicine, de Sint Maartenskliniek, Nijmegen (5)
Living with a short arm: Which problems do young adults experience in transition to adulthood?
Children and young adults with transversal upper limb reduction deficiency (tULRD) generally experience few limitations in daily activities. During transition from childhood to adulthood significant changes occur on different domains of participation. Young adults with disabilities are at risk of experiencing limitations due to changing physical and social requirements, but transitional problems in tULRD have not been studied yet.
The first aim was to evaluate whether young adults with tULRD experience limitations in different domains of participation during transition to adulthood. Second, the method of dealing with these limitations and the influence of people in the environment and the rehabilitation team were examined.
Patients were recruited from 5 Dutch rehabilitation centers. A qualitative study was performed using a semi-structured interview to identify experienced problems on the following domains of participation: education and employment, finances, leisure-time activities, social interaction and friendship, intimate relationship and sexuality, housing and housekeeping, transportation. Interviews were recorded on audio recorder and literally typewritten. A framework approach was used to categorize and analyse the themes assessed.
15 young adults (5 males, 10 females), mean age 21.4 (range 18-24) years with tULRD were included. Current prosthesis use was reported by 4 participants. Aids or adaptations were generally used for specific activities, like car driving or household chores.
Various strategies to deal with the problems were reported. The direct environment like parents and friends mostly had a stimulating role. The rehabilitation team was mainly involved in childhood giving practical advice.
Young adults with tULRD experience limitations in finding a suitable study or job, are in general more insecure about themselves and need some adaptations for specific activities. Their direct environment plays a supporting role. The rehabilitation team could possibly play a more extensive role in advising how to deal with transitional problems.
414
Peter Worsley (1) presenting Josh Steer (1) Chris Smith (1) Alex Dickinson (1)
The Netherlands, University of Southampton, Southampton (1)
Classifying residual limb shape in transtibial amputees
Successful prosthetic adoption and rehabilitation following lower-limb amputation is dependent on a safe and comfortable socket-residual limb interface. This interface is heavily dependent on the shape and quality of the residual limb, with quality being defined using stump shape, bone shape and skin condition factors [1]. Previous research has attempted to characterise residual limb shape in above-knee amputees [2], but this has yet to be attempted for transtibial residual limbs.
Eighty one rectified casts of transtibial residual limbs from were scanned using a VIUScan (Creaform, Canada) laser scanner, with local ethical permission (13/NW/0833). A Matlab (Mathworks, USA) programme was written to extract measures of limb volume, cross-section area (CSA), and shape profiles (sagittal and coronal planes). These measures where used to classify stump shape utilising a Principal Component Analysis (PCA). Here stumps were visually classified into three groups (bulbous, conical and cylindrical) by a physiotherapist using the scanned geometries. Principal components (PCs) were extracted to determine features of shape variation that could be used to quantify differences between the groups.
The 81 rectified casts of residual limbs were scanned and measured, with a mean volume of 3,92l ±2,149cm3 or (3.92 ±2,15L) and were classified into cylindrical (n=38), conical (n=29) and bulbous (n=14). The CSA and shape profiles in the sagittal and coronal planes from all scans were included in the PCA model. The first PC from the coronal data provided the most discriminatory sensitivity of 83%, 77% and 64% for determining cylindrical, conical and bulbous shape respectively. When combined with the second PC of coronal plane and the first PC of the area measures a final discrimination model (Figure 1), accurately separated conical and bulbous stumps (97%) but had less accuracy comparing cylindrical to conical (79%) or bulbous (73%).

3D Scatter plot of principle components
This study has described a technique to use data acquired from high resolution scanning technology to classify transtibial residual limb shape with a modest to high level of accuracy (73-97%). Further research is needed to look at the associations between stump shape and clinical outcomes both with prosthetic fitting and rehabilitation. This would provide the potential to inform best practice across the clinical pathway, from surgery through to rehabilitation.
416
Eric Weertz (2) presenting Frédéric Joyeux (1) Jérôme Canicave (1) Vincent Drouin (3) Isabelle Urseau (1)
India, Handicap International Federation, Lyon, Rhône (1) France, Handicap International Federation, Brussels (2) Belgium, Proteor Handicap Technologie, Dijon, Côte d’Or (3)
Temporary lower limb prosthesis fitting in emergency context in a global multidisciplinary approach by the physical rehabilitation team by Handicap International
A strong earthquake rocked the island of Haiti on 12 January 2010. More than 300,000 adults and children were injured. Based on the assessment of health structures, Handicap International (HI) estimates between 2000-4000 amputations, nationwide, resulted from this earthquake. According to the poor quality of services for orthopedic devices, HI decided in coordination with the French Company, Proteor to develop emergency kits that allow proposing temporary lower limb prosthesis in a short period and with limited infrastructures and equipments.
Propose appropriate and sustainable solutions in terms of lower limb prosthesis in a post natural disaster context through innovative kit for temporary prosthetic fitting by non- formal trained technicians
A first evaluation of the context showed the importance of the needs and expectation of the population, human resources, infrastructures, equipments materials available. According to the situation, a Public Private Partnership was signed between Handicap International and Proteor: it was the occasion to combine the experience of activities in complex situations with the technological experience in term of prosthetic devices. Prosthetics emergency kits were designed and tested on volunteer patients: a study gathering 22 patients (on around 100 fitted) is proposed to evaluate the result of this evidence based approach. Both Handicap International and Proteor were involved in this evaluation.
Regarding functional aspects, the study showed gradually the satisfaction and the improvement of the function for all the 22 patients. The kits have been well accepted despite some beneficiaries have raised the focus on the cosmetic aspects of the prosthesis. Technically, Handicap International and Proteor had to introduce necessary technical adjustments on the kits. Improvements in term of technology were proposed such: brown color for feet, more sizes for the trans femoral sockets, universal connector for the sockets. Through trainings of the technicians and rehabilitation staff, the services have improved. Educational materials are created to facilitate the induction process of the technicians. All those results will lead to the use of this new technology in other contexts: they will be part of a project for the victims of the Syrian crisis.
The use of this technology has been crucial in the service provision of prosthesis in the post-earthquake context of Haiti. Technological improvements have to be proposed to do a transition from temporary devices to definitive.
New projects are in process for the use of emergency kits: a pilot project is in process for the victims of the Syrian crisis. Another challenge is to ensure a remote monitoring of the activities through distance learning tools for deploying this technology in armed conflict zones.
417
Jérôme Canicave (1) presenting Eric Weertz (2) Isabelle Urseau (1)
France, Handicap International Federation, Lyon, Rhône (1) France, Handicap International Federation, Brussels (2)
Innovative solution for prosthetics fitting in complex emergencies and contexts within Handicap International ( HI ) project
HI is developing expertise in provision of functional rehabilitation services in complex emergencies. These contexts call for innovative solutions in order to address ensuing challenges, properly taking into account the needs, expectations, access to services, access to beneficiaries, technology, capacity building and logistics. Using prosthetic kits for lower limbs allows fitting of temporary devices. This is followed by a transition to CAD CAM assisted production of permanent sockets.
-Propose innovative solutions allowing access to prosthetics where expertise, facilities and equipment are scarce.
-Consider the rational of using CAD CAM for provision at distance of lower limb prosthesis
The methodology consists in proposing evidence based practice through a pilot project in Syria using a comprehensive management protocol.
Operational Syrian partners (physiotherapy centers) are trained to fit lower limb amputations using prosthetic emergency kits.
Amputee subjects are fitted with temporary prosthesis until presenting stabilized stumps.
Measurement of stump is done with 3D scanner, digitalized and sent to a remote professional unit.
The latter uses a Cad Cam system for stump rectification and manufactures the definitive socket that is resent to the Syrian partner and assembled on the original components of the emergency kit.
This protocol of treatment using the Cad Cam system targets around 10 subjects . The outcomes are measured by different criteria presented and commented in a follow up frame such as :
- Patient satisfaction questionnaire.
- Orthopedic evaluation of the protocol and its outcomes
- Quality control assessment of the services for further adjustments and improvements
- Evaluation of a distance monitoring system for comprehensive functional evaluation for prosthetic fitting.
- Reliability of partnership in the specific context for further developments
- Economic and costing evaluation of the process.
- Potential for reproduction of this model in other future contexts
- Transition to stable economic and security environments of this model towards more long term developmental models
Necessity to improve ambulation for persons with low mobility in unsecure contexts should lead to explore alternative appropriate technologies and approaches discussing:
- Relevance of fitting definitive sockets versus renewing temporary ones several times until context is stable
- Quality of fitting sockets by available physiotherapists trained on theoretical and practical alignments.
- Tools, processes of distance monitoring in Prosthetic fitting programs, bypassing standardized knowledge versus compliance with international standards.
419
Jérôme Canicave (1) presenting Eric Weertz (2) Isabelle Urseau (1)
Malaysia, Handicap International Federation, Lyon, Rhône (1) France, Handicap International Federation, Brussels (2)
Distance education and blended learning for comprehensive capacity building in prosthetics fitting in complex emergencies within Handicap International ( HI ) projects
Within complex emergencies, innovative solutions are needed to address challenges of upgrading knowledge, managing complex injuries and create remote follow-up capacity to measure increase of knowledge and its impact on beneficiaries. Online modules for training rehabilitation staff were developed by HI in order to acquire in short term tailored knowledge on full assessment, clinical practice and gait training for lower limb amputees.
-To propose innovative solutions for training in prosthetics fitting where classic teaching is compromised.
- Explore the potential of skills upgrading within complex emergencies and existing networks in e-learning.
This methodology consists in drafting course contend for short training of rehabilitation staff in fitting lower limb prosthetics.
This contend is uploaded on an interactive platform on the internet, configuring the knowledge and educational approach to audio visual, blended learning and self- learning modes.
Selection of potential students is done by teachers and project coordinators based on the need to upgrade knowledge within short periods of 3 – 4 weeks.
Courses are delivered on distance using the platform’s features: course scenarios, documentation links, testing knowledge, communication forums for questions and final assessment modules .
This learning method for upgrading knowledge levels for non-formal trained technicians has been under a trial period for up to 6 months.
The basic knowledge delivered to a pool of 3 – 5 staff shows progress in the field of this type of fitting as this is the only type of condition encountered in their clinical practice.
Feedback sessions through Skype meetings and use of forum functions on the distance learning web tool provide additional feed-back on challenges in practice and unmet needs regarding further education.
Use of visual presentation ( in form of video clips demonstrating clinical practice ) in local language have been added to the basic narrative contend . Testing and continuing evaluation of knowledge is compared with minimum knowledge needed for servicing caseloads.
Use of this teaching method, its strengths, challenges and capitalisation is still being monitored and remains the best available way to support learning within the project .
Providing minimum ways of communication and exchange, it is understood that face to face learning remains ideal for full clinical practice transfer. Further exploration is done in adding other fitting technologies as well as comparing education levels with formal education programs.
420
Sevgi Özdinç (1) presenting Serap Ünsar (2) Melahat Akgün Kostak (3)
Belgium, Trakya University Faculty of health Science Physical Rehabilitation Dep., Edirne (1) Turkey, Trakya University Faculty of health science, Edirne (2) Turkey, Trakya University Faculty of health science, Edirne (3)
Determination The Relationship Between Choose of Shoes and Muscle Skeletal Problems Among University Students
421
Peter Kyberd (1) presenting Ali Hussani (1) Ghislain Maillet (1)
Turkey, Institute of Biomedical Engineering, Fredericton, New Brunswick (1)
The Clothespin relocation task as a validated outcome measures for upper limb prostheses

[1] L. A. Miller et al., “Summary and Recommendations of the Academy’s State of the Science Conference on Upper Limb Prosthetic Outcome Measures,” JPO, vol. 21(9), pp. P83-P89, 2009.
[2] A. Simon, B. Lock, and K. Stubblefield, “Patient training for functional use of pattern recognition–controlled prostheses,” J. Prosthet. Orthot., vol. 24, no. 2, pp. 56–64, 2012.
[3] V. Wright, “Prosthetic Outcome Measures for Use With Upper Limb Amputees: A Systematic Review of the Peer-Reviewed Literature, 1970 to 2009,” JPO, 21(9), pp. P3-P63, 2009.
[4] V. Wright, “Measurement of Functional Outcome With Individuals Who Use Upper Extremity Prosthetic Devices: Current and Future Directions,” JPO 18, pp. 46-56, 2006.
422
Conor Sheehan (1) Elaine Figgins (1) presenting
Canada, NCPO, University of Strathclyde, Glasgow, Scotland (1)
A comparison of the mechanical properties between different percentage layups of a single style, carbon fibre AFO
Currently a range of “off-the-shelf” AFO’s are used in clinical practice, of various functions and designs. Their use relates to immediate control over mild conditions.
1. The elastic properties
2. Deflection about the ankle and calculation of stiffness.
3. Failure of each device under compressive forces, (dorsiflexion).
This experimental bench test attempts to increase the understanding and develop the area of testing orthotic devices. This was achieved by comparing carbon fibre, ankle foot orthoses at different percentage layups and the effect this has on the properties. It also outlines a clear and simple setup for obtaining results. With a view to be able to define and compare the mechanical properties of each AFO.
Literature was reviewed for setup and a bench test was then deduced. Two universal Instron testing machines were used to apply the necessary forces. An initial practice device was utilised to establish a baseline of forces and confirm effective setup. Each test was then carried out on nine AFOs, of three different percentage layups. Three AFOs had a standard carbon fibre layup three had 30% reduced layup and three had 30% increased layup. Test were carried out to assess deformation under both compression and tensile forces, and well as finally to ultimate failure of each device.
Elastic properties were proved for all devices. Stiffness exhibited greater resistance in tension, with angular deflection being greatest in the Lite set and least in the Rigid. Failure occurred mainly due to fracture, proximally on the strut, however this was not consistent among the devices. The graph below summarises the results of the project.
The results proved the properties expected of each carbon fibre AFO. This relates to their functional ability and therefore the devices prescription choice. Further work should relate these to specific patient characteristics for better prescription decisions and rationales by clinicians.

Results proved stiffness was significantly different in all cases (p<0.05), other than Rigid vs Standard in compression. It should be noted that the sample size was very small in all cases. Any study with <10 results per set may not truly reflect stiffness. See Appendix 6 for more details.
424
Linda Jenkins (1) Elaine Figgins (1) presenting
Portugal, NCPO, University of Strathclyde, Glasgow, Scotland (1)
Principles of gait analysis for assessing the efficacy of ankle-foot orthoses in patients following stroke
Impaired gait is often seen in adults following a stroke. AFOs are commonly prescribed to restore walking ability and balance. Gait analysis has been used in many studies to assess the efficacy of AFOs.
The objective of this study was to determine the effectiveness of gait analysis in assessing the efficacy of ankle-foot orthoses in adult patients following stroke.
The primary objective of this review was to define the fundamental principles of gait analysis, required when assessing the efficacy of ankle-foot orthoses (AFOs), for adults following stroke. In order to achieve this objective, a review of the literature was conducted to identify the most common methods of gait analysis used and determine which mechanism/parameters yielded the greatest number of statistically significant results. As there is a lack of high quality evidence for the efficacy of AFOs, which may be related to the poor description provided in most papers, a secondary objective of this review was to define the description of AFO characteristics, required within clinical studies.
To define from the literature, effective principles for gait analysis when assessing the efficacy of ankle-foot orthoses (AFOs) in adults following stroke. A secondary objective was to define the description of AFO characteristics, required within clinical studies.
A literature review was conducted using ScienceDirect and Web of Science databases for the period 2004 to 2013. After scrutiny of titles and abstract a final nineteen papers were selected for review.
Each paper was then read, reviewed and quality assessed and importantly outcomes measures. Their effectiveness as an outcome tool for the efficacy of the use of AFO following stroke in adults was documented in tabular form to assess for a thematic analysis across the research under scrutiny. The definitions and description of the AFOs used in all papers was also analysed and assessed for repeatability.
It was found that the most significant measures in gait analysis of adult patient following a stroke were spatiotemporal parameters and ankle joint kinematics, specifically step length of the sound limb. These highlighted the efficacy of AFO as a treatment option. However no conclusions could be reached on AFO design as the results of the description and documentation on the AFO designs used in the studies was so poor and inconsistent. None of the papers reviewed allowed for the results to be repeated accurately due to the poor descriptors of the AFOs used in the trails.
The efficacy of gait analysis has still never been demonstrated in this field. It is hoped that by providing foundations for future studies, the quality of evidence for AFO use in patients with stroke will be improved.
Future studies assessing AFO efficacy in stroke patients should include measurement of spatiotemporal parameters and ankle joint kinematics. AFOs should be fully described in order to increase the quality of evidence for AFO efficacy.
1. NHS Quality Improvement Scotland. Best practice statement: Use of ankle-foot orthoses following stroke. NHS Quality Improvement Scotland; 2009.
2. Tyson SF, Sadeghi-Demneh E, Nester CJ. A systematic review and meta-analysis of the effect of an ankle-foot orthosis on gait biomechanics after stroke. Clinical Rehabilitation. 2013 Oct;27(10):879-91. PubMed PMID: WOS:000323831500003
425
Holly Phimister (1) Elaine Figgins (1) presenting
UK, NCPO, University of Strathclyde, Glasgow, Scotland (1)
Conservative Management of Stage I and II Posterior Tibial Tendon Dysfunction
The posterior tibial tendon primarily maintains the medial longitudinal arch of the foot, damage results in posterior tibial tendon dysfunction (PTTD). PTTD is the commonest cause of acquired adult flatfoot deformity and largely affects middle-aged women of increased body weight. There is a lack of evidence with regard to the most effective conservative treatment of PTTD.
This literature review aims to assess the level of evidence in relation to stage I and II Posterior Tibial Tendon Dysfunction (PTTD) and conclude on the most effective treatment.
The literature surrounding PTTD focuses largely on surgical intervention and there is little available on orthotic management. The aim of this project is to produce a literature review to determine the most effective conservative treatment method of stage I and II PTTD within the adult population. This review may be used by clinicians to aid clinical judgement and encourage evidence-based practice within the field of Orthotics.
A literature review was systematically carried out and studies were assessed for level of evidence, utilising the databases Medline, Embase, Cochrane database, CINAHL and ASSIA. Generally, there was a lack of high quality of evidence with only one randomised control trial.
Ten studies were included in this review, all relating to conservative treatment methods of stage I and II PTTD. Study and population characteristics, interventions and outcome measures were evaluated. Although no restriction was put on the paper search with regard to date, all of the studies used were conducted within the last fifteen years. The Scottish Intercollegiate Guideline Network (SIGN) was used to appraise the literature. There were some cases of bias in the papers, as some of the orthotic devices were provided by companies and this must be taken into account. The mean number of participants was n=27.3 and the median number is 27.5, with a range of 1-64. The sex of the participants is uneven with a total of 218 females as compared to only 54 males. Most of the studies observed the use of an ankle-foot (AFO) or supra-malleolar (SMO) orthotic device. These orthoses are classed as such because they incorporate the talo-crural joint as well as both the subtalar and midtarsal joints. The majority of the orthoses were manufactured from polypropylene thermoplastic. The study with the highest level of evidence used a foot orthoses in combination with an exercise programme. Exercise or stretching as a treatment method was subdivided into either isokinetic, concentric or eccentric exercise. Several of the studies utilised other various forms of treatment including initial immobilisation, rest and ice therapy.
Evidence suggested that the most effective treatment for the treatment of stage I and II PTTD is a custom-made polypropylene foot orthosis in conjunction with an exercise programme consisting of stretches and eccentric strengthening. The most common outcome measure used in the studies was the AOFAS (American Orthopaedic Foot and Ankle Society) ankle/hindfoot scale .This scale measures subjective pain, activity limitations, walking distance, walking distance, walking aids and ability to walk on different surfaces. A full-length semi-rigid foot orthosis with a medial heel wedge and forefoot posting is a suitable prescription for the treatment of stage I and II PTTD. A UCBL is also a suitable treatment method when the deformity is still flexible. Custom-made orthotic devices are most effective at correcting the foot deformity. All the studies used in this review agreed that the use of orthoses in the early stages of PTTD decreased the need for surgery and prevented progression.
Further work includes more studies of a higher level of evidence, specifically in Europe with more comparison between orthotic devices and conservative treatment methods.
427
Benjamin Mundell (1) presenting Hilal Maradit Kremers (1) Sue Visscher (1) Kenton Kaufman (1)
United Arab Emirates, Mayo Clinic, Rochester, MN (1)
Pre-amputation characteristics as predictors for lower-limb prosthetic prescription among adults with above knee amputations: a population-based study

428
Elaine Figgins (1) presenting
USA, NCPO, University of Strathclyde, Glasgow, Scotland (1)
The development and implementation and review of clear objectives and assessment criteria for prosthetic and orthotic clinical placements (Procedure Based Assessments and Clinical Competencies)
Most educational programmes globally in prosthetics and orthotics have a clinical placement element of requirement for clinical experience prior to graduation or certification. The NCPO at Strathclyde University, Scotland undertook a major review of its clinical placement structures, to revise and increase the consistency of their students’ prosthetics and orthotics clinical placements.
To devise a robust methodology to assess undergraduate students as part of a 4 year programme, in their clinical competencies that could be transparent to both students and supervisors, and to review this assessment once implemented.
Literature was searched and a suitable model was found ( from Dundee University medical programme) to construct the new clinical placement evaluations and assessment for undergraduate prosthetic and orthotic students. Stakeholder focus groups were used to help form the assessment protocols, called Procedure Based Assessements PBAs. Paperwork was drafted and further stakeholder were consulted for feedback. Finally the new assessments were implemented, monitored and reviewed.
The results were a pass /fail criteria for assessment of clinical placements. With six prcedure based assessments in each discipline (prosthetics and orthotics), as well as a clinical competencies form to highlight soft skills and interactions. The supervisors and student feedback has been very positive and the assessment methodology is seen as transparent and effective. Supervisors give a pass fail grade with comments if required.
This reviewed assessment affords clearer objectives and removed discrepancies in grading across placement sites, that had caused student anxiety previous ly. Clinical supervisir training has also been adopted to support the new assessment methodology. Supervisor feedback has been that the new PBAs and clinical competencies are more robust and time effective. The assessment method will be shown and as well as an overview of clinical placement supervisors training that has been developed.
Discussions have now been undertaken with the Professional body in the UK (BAPO), to consider the drafting of further competencies and procedures for new graduates in the first two years post graduation as prosthetists/orthotists.
429
Christopher Bennett (1) Andrew Ayers (1) Jennifer Lucarevic (1) Adam Finnieston (1) Robert Gailey (1) presenting
UK, University of Miami Miller School of Medicine, Coral Gables, FL (1)
Length and Speed Matters: The Effects of Prosthetic Limb Length and Walking Speed on Knee Flexion of MPK Prosthesis and the Intact Limb Knee
Results

Significant difference p<.05 **Self-select speed
431
Peter Kyberd (1) presenting Duncan Finlayson (1,2)
France, Institute of Biomedical Engineering, Fredericton, New Brunswick (1) Canada, Glasgow University, Glasgow, Scotland (2)
A sensorised glove for use with an intelligent prosthetic hand

1/ D.Tyler et al. Long-term Peripheral Nerve Interfaces to restore sensation. page 22, MEC’14, 19-22 August 2014, Fredericton, New Brunswick, ISBN 978-1-55131-176-0.
2/ P.J.Kyberd, M.Evans, S.te Winkel An intelligent anthropomorphic hand, with automatic grasp. Robotica, 16 pp 531-536, 1998.
3/ J.M.Nightingale, Microprocessor control of an artificial arm, Journal of Microcomputer Applications, 1985, 8, pp 167-173.
4/ M.Ortiz-Catalan, B.Håkansson, R.Brånemark Osseointegrated human-machine gateway for long-term sensory feedback and motor control of artificial limbs. Sci. Transl.Med. 6(257)re6(2014)
432
Samuel Hamner (1) Vinesh Narayan (1) presenting Nicole Rappin (1) Krista Donaldson (1) Pooja Mukul (2)
UK, D-Rev, San Francisco, CA (1) USA, JaipurFoot Organization (BMVSS), Jaipur, Rajasthan (2)
Evaluating Impact and Effectiveness of the ReMotion Knee – An Affordable Polycentric Prosthetic Knee
[1] Pearlman, J., et al. IEEE Eng. Med. Biol. Mag. 27:12–22, 2008.
[2] Andrysek, J. Prosthet. Orthot. Int. 34:378–398, 2010.
[3] World Health Organization. World Report on Disability, 2011.
[4] Jensen, J., Raab, W. Prosthet. Orthot. Int. 28:141–151, 2004.
[5] Hamner SR, et al. Annals Biomed. Eng., 41:1851-9, 2013.
[6] Radcliffe, C. Prosthet. Orthot. Int. 18:159–173, 1994.
[7] Schoppen, T., et al. Arch. Phys. Med. Rehabil. 80:825–828, 1999.
[8] Condie, E., et al. J. Prosthet. Orthot. 18:13-45, 2006.
435
Raymond Pye (1) presenting
USA, Mobility Outreach International, Seattle, WA (1)
Resourceful Innovation for O&P Design and Manufacturing in Developing Countries
1. Document the needs of the amputee end-users.
2. Observe the function, durability and cosmetic appearance of previously used foot components.
3. Document the most common failure modes and the lifespan of previously used foot components.
4. Identify local suppliers of structural and cosmetic materials as well as delivery capacity.
5. Design foot components to meet the needs of local end-user, using locally available manufacturing tools, locally available materials, and practical quality standards.
6. Test, evaluate and document new foot components with small groups of active users.
436
Takashi Nakamura (1) presenting Nobuya Yamasaki (1) Masaki Nakagawa (1) Ryouzou Tanaka (1) Koji Takahashi (1) Yoshiko Tobimatsu (1)
USA, National Rehabilitation Center for Peraons with Disabilities, Saitama (1)
Prostheses for persons of purpura fulminans with quadruple amputation
The major amputation of all four limbs (referred to as “quadruple amputation”) is a rare occurrence. Persons with quadruple amputation need special improvement for their prostheses not required by persons with unilateral or bilateral amputation. We previously reported two cases of persons who underwent quadruple amputation after suffering from disseminated intravascular coagulation in conjunction with pneumococcemia with purpura fulminans (PF) [1]. Herein we report the third case of a person with quadruple amputation.
The purpose of this report is to provide approaches to solve the problems associated with prostheses for the special requirements of the patient with quadruple amputation.
A 58-years-old male who developed PF from pneumococcal infection and subsequently underwent bilateral transradial and bilateral transtibial amputation. He was initially fitted body-powered upper limb prostheses to enrich his activities of daily living, and then the lower limb prosthesis were fitted for the gait training. The several problems became apparent and we focused on two problems.
1) Control of a wheelchair driving by the upper limb prostheses: As he required a conventional wheelchair in initial stage, he was unable to control a wheelchair because of the slippery surface of the plastic sockets of the upper limb prostheses.
2) Self-donning of the pin-lock liners: He was unable to put on the liner properly, and trying to do so resulted in air being trapped between the end of the liner and the skin of the stump which created a vacuum phenomenon.
The first problem was solved as follows. the rubber sponge pads covered with antiskid polyvinylchloride sheets were attached to the sockets in order to maintain shock absorption and frictional force, and Northwestern-type sockets were fitted in order to prevent rotation of the sockets during wheelchair propulsion.
The second problem was solved with a special assistive device [2] which enables correct positioning of the liner. Trapping of air between the liner and the stump was prevented by use of the device.
In the rehabilitation of persons with quadruple amputation restoration of locomotion and self-donning of the prostheses were common problems we experienced. Not only improvement of prostheses but also use of an assistive device should be considered to solve such problems. Compared to the previous two cases, the rehabilitation of this case was successfully accomplished because he was a person with bilateral transtibial amputation and no skin damage was on the residual limbs.
[1] Yoshimoto et al; 2013 Prothet Orthot Int.
[2] Tamir et al; 2003, Prothet Orthot Int.
437
Shoji Morimoto (1) presenting Haruyuki Yoshida (1)
Japan, Osaka Electro-Communication University, Shijo-nawate, Osaka (1)
Three dimensional rollover characteristics of prosthetic and orthotic foot-ankle units measured on the gait simulated loading device
Various prosthetic foot-ankle units have been developed and improved, and it becomes difficult to select an appropriate foot-ankle unit and adjust its alignment for each amputee for prosthetists. Moreover it becomes difficult to adjust the high functional orthotic ankle unit in which high functional braking unit is installed, for example, MRF brake installed AFO.
To resolve this problem, it is important to develop the measuring method of the foot-ankle unit gait function in which the measured results can be compared.
Based on the rigid body mechanics, f.c.p.(force contact point) is meaningful than c.o.p.(center of pressure). Then, we have developed the measuring method of three dimensional locus of f.c.p. on foot-sole under the fixed stance phase loading from heel contact to toe-off generated by the testing device based on ISO22675 standard. Foot-ankle unit is positioned under the pneumatic servo cylinder which generates the compressive force of double peaks simulating the typical cyclic gait loading, and 6-axis load cell is installed just above the foot-ankle unit. The foot plate positioned just under the foot rolls and generates vertical and shear forces on the foot-sole. Forces and moments measured by 6-axis load cell are positioned on the center of the load cell, and are equally transformed to single force and single moment on the screw line, based on the rigid body mechanics. The cross point of the screw line calculated from the output of 6-axis load cell and the surface of rolling foot plate is the f.c.p.. The locus of this point plotted on the coordinates system fixed at the center of 6-axis load cell shows the rollover characteristics in sagittal, frontal and transverse planes.
Three dimensional rollover characteristics of typical prosthetic foot-ankle units (Single axis foot, SACH foot (1D10, J-Foot) and Tribute) were measured. Locus of f.c.p. in sagittal, frontal and transverse planes were calculated and plotted on each graph. The relation between f.c.p. shift from heel to toeand swing foot plate angle (deg) was plottedon each foot-ankle unit. These results showed distinctive feature on each foot-ankle unit, and useful indicators were obtained. Alignment change (plantar flexion – dorsal flexion, inversion – eversion, toe in – out) of the foot 1D10 was tried and some distinctive marks were obtained.

The method to calculate the three dimensional rollover characteristics as the locus of f.c.p. on the sole of prosthetic foot ankle unit under the fixed gait simulated loading condition was settled. The gait simulated loading device was developed based on ISO22675 and used under the P3 loading condition (corresponding to 60kg body weight amputee). The calculate results of three dimensional locus of f.c.p. showed the possibility to compare various prosthetic foot-ankle unit function.
438
Mohammed Sallak (1) presenting
Japan, King Fahad Medical City, Riyadh (1)
Comparing the gait of children with diplegic cerebral palsy in a clinical environment and an outdoor environment while wearing Ankle-Foot Orthoses
The ankle-foot orthosis (AFO) represents one rehabilitation intervention that may improve gait and reduce functional deficits. However, there is insufficient evidence related to the effect of AFOs on gait in a real environment.
This study aimed to investigate the effect of tuned AFOs on walking ability and energy expenditure of children with diplegic CP, on even surface indoors and outdoors, wearing footwear as baseline.
An experimental pilot study, performing walking trials in random order was done. Trials were conducted in familiar settings where children walked after their AFOs were tuned using a video camera for capturing the shank angle related to the vertical.
Participants were 12 diplegic children with cerebral palsy (7 boys, 5 girls) with a mean age of 9 years 4 months (range 5 years to 13 years). Children ambulated without walking aids. They were fitted with tuned rigid AFOs, and given information to wear AFOs for a period of 4 weeks. Trials were done while children wore accelerometers with a portable microprocessor (Intelligent Device for Energy Expenditure and Activity (IDEEA) monitor) for recording gait parameters.
The main findings of this study that tuned rigid AFOs improved the gait of children with diplegic CP. The study showed that there was a significant difference in the performed trials on flat surfaces indoors and outdoors, in velocity (p = 0.03) and energy expenditure (p = 0.00), but no significant difference in cadence
(p =0.759) or stride length (p =0.216).
The mean values of velocity were lowest when the children used tuned rigid AFOs indoors and highest outdoors while energy expenditure mean values were lowest when the children used tuned rigid AFOs indoors and outdoors and highest when the children used only footwear indoors and outdoors. Stride length and cadence stayed almost the same indoors and outdoors, with and without AFO.
Further research should be focused on different terrains and environments for monitoring children’s gait in a more “real” environment.
439
Yuen Yi Chiu (1) presenting
Saudi Arabia, Tuen Mun Hospital, Hong Kong (1)
New Custom-Made Ankle Brace (CMAB) for stroke patients with equinovarus of the ankle
Stroke is a global healthcare problem and one of the leading causes of chronic adult disability. The stroke survivors may still have functional limitations such as ambulatory abilities are disrupted and hence reduced quality of life. Equinovarus positioning of the foot and ankle complex and sustained plantarflexion of the ankle always the happened after onset of stroke. The deformities will then alter the gait pattern and hence decrease walking speed and increase energy cost.
Equinovarus of the ankle which may decrease walking stability is always neglect by the stroke survivors. An effective orthosis can help improve or minimize functional disability A custom-made ankle brace (CMAB) is designed to increase walking stability after stroke.
Commercial inversion control ankle brace (CICAB) aims to provide better stability of the ankle but has fair conrol of the involuntory movement of the ankle of the stroke patient. Using a CICAB as blue print to design CMAB for better control of the ankle. Using similar technique of making ankle foot orthosis (AFO) but without foot piece and lower proximal trimline. About two third of the ankle is enbraced, which greatly reduce the inversion moment during walking. the heel part of the plastic is removed for better proprioception. But CMAB is only suitable for patient with mild drop foot and spasticity less than 2.
CMAB is applied for stroke patient with equinovarus ankle and mild drop foot. It is able to reduce the ankle inversion and mild drop foot and used for barefoot walking. The walking stability of the patient is increased as the heel is landed in a neutral position during heel strike and the transition from heel strike to foot flat is more smooth.
Patient who are not preferred to wear shoe for indoor walking can still use the CMAB as without the plastic piece of the sole part which reduce the chance of slippery. There are more choices of footwear for CMAB over AFO as no foot piece of the CMAB and hence more space inside the shoe.
The evaluation of the CMAB will be done in later stage to see how much
Improvement can be done to the stroke patient by using the CMAB.

There is a poor compliace of the AFO as not all the stroke patients using
AFO for indoor walking and even outdoor walking. People usually take off their shoes or wear slippers in the house and poor fitting slippers are frequently associated with a fall and fracture.
CMAB can be used to tackle the slippers problem and increase the compliance as CMAB reduce the ankle inversion and mild drop foot.
Munro BJ, Steele JR. Household-shoe wearing and purchasing habits. A survey of people aged 65 years and older. J Am Podiatr Med Assoc 1999; 89: 506-14.
Sherrington C, Menz HB. An evaluation of footwear worn at the time of fall-related hip fracture. Age Ageing 2003; 32: 310-4.
440
Laura Huinink (1) presenting Hanneke Bouwsema (2) Dick Plettenburg (3) Corry van der Sluis (4) Raoul Bongers (1)
Hong Kong, University of Groningen, University Medical Center Groningen, Center for Human Movement Science, Groningen (1) The Netherlands, Adelante Rehabilitation Centre, Centre of Expertise in Rehabilitation and Audiology, Hoensbroek (2) The Netherlands, Delft University of Technology, Faculty of Mechanical Engineering, BioMechanical Engineering, Delft (3) The Netherlands, University of Groningen, University Medical Center Groningen, Center for Rehabilitation, Groningen (4)
The development of motor skills in novice body-powered prosthesis users over time
A recent study examined how people learn to use a myoelectric prosthesis (Bouwsema et al., 2014). With this knowledge a foundation was laid for an evidence-based training program for myoelectric prostheses. However, body-powered prostheses differ from myoelectric prostheses, regarding the control regime and the feedback provided from the prosthesis. Due to the cable-based control of the body-powered prosthesis via body-movements, more proprioceptive feedback is provided. These differences might have consequences for how body-powered prostheses need to be trained.
The aim of this study is to describe the learning processes and performances over time of novice body-powered prosthesis users during practice of goal-directed tasks.
Thirty able-bodied participants were randomly assigned to one of four experimental groups, and practiced with a body-powered prosthesis simulator, equipped with a voluntary closing TRS hook, for five sessions during a period of two weeks. Groups had to perform either indirect grasping (IG), handing over the object from the sound hand, direct grasping (DG), fixation (FIX) or a combination of all three tasks (COM). Prior to the learning sessions the Southampton Hand Assessment Procedure (SHAP) was performed, as well as during the posttest, 2-weeks retention and 3-months retention test. During grasping tasks deformable objects with a different compliance were used which had to be manipulated. Movement kinematics were examined, as well as grip force control which was derived from the magnitude of compression of the objects.
All four experimental groups improved on the SHAP over training. Interestingly there were no significant differences between groups. Total reach time and hand closing time decreased during the training sessions. Importantly, the IG group showed a shorter time in which the hook was fully open (i.e. the plateau time) compared with the DG and COM group. The data showed a trend in that the IG group also showed a faster performance in reach time and hand closing time and showed a higher peak velocity of hand closing. In general, when object rigidity decreased, overall movement times increased. As expected, low-resistance objects were more compressed than high-resistance objects. It was remarkable that compression did not change over the learning sessions.
The data on the reaching and grasping profile clearly showed that motor skills of novice body-powered prosthetic users improved during a two-week training period. Interestingly, the IG group, which handed over the object from the sound hand, had shorter plateau times than the other groups. We hypothesized that proprioception of the sound hand might have helped perceiving object properties. Comparing these data with improvement over training in myoelectric prostheses showed that overall movement times with a body-powered prosthesis were faster.
Bouwsema, H., van der Sluis, C. K., & Bongers, R. M. (2014) Changes in performance over time while learning to use a myoelectric prosthesis. J Neuroeng Rehabil,11, 16-0003-11-16.
441
Imad Sedki (1) presenting Keren Fisher (1)
The Netherlands, The Royal National Orthopaedic Hospital/ Stanmore, London (1)
Developing Prescribing Guidelines for Microprocessor Controlled Prosthetic Knees
Microprocessor-controlled prosthetic knees have gained increasing popularity over the last decade. Research supports their provision to address specific problems or to achieve certain rehabilitation goals. However, there are yet no agreed protocols or prescribing criteria to assist clinicians in the identification and appropriate selection of suitable users.
The aim is to reach professionals’ agreement on specific prescribing guidelines for microprocessor-controlled prosthetic knees
The study involved multidisciplinary teams from the Inter Regional Prosthetic Audit Group, representing nine Prosthetic Rehabilitation Centres in the South East England region. We used the Delphi technique with a total of three rounds to reach professionals’ agreement.
Professionals were able to agree MPK definitions, suitability criteria, indications and contraindications, in addition to details of trial and outcome measures.
(See table below)


The prescribing guidelines were agreed and will be reviewed and updated depending on new research evidence and technical advances.
Sedki I, Fisher K. Developing prescribing guidelines for microprocessor-controlled prosthetic knees in the South East England. Prosthet Orthot Int. Onlinefirst 2014 March 25
443
Pooja Mukul (1) presenting Vinesh Narayan (2)
UK, BMVSS-JAIPUR FOOT ORGANIZATION, JAIPUR (1) India, D-Rev, San Francisco (2)
Jaipur Knee – Remobilizing transfemoral amputees in India and the developing world
The World Health Organization (WHO) estimates that 30 million amputees i.e. 80% of the global amputee population lives in low income countries (LICs) . 31% of these are transfemoral. This puts the need of prosthetic knee joints close to 10 million. WHO in its latest disability report also states that only 5% of these patients’ needs are met . Those that are provided with prostheses are traditionally fitted with a single axis knee joint with a manual lock or constant friction, largely because of nonavailability of better options resulting in an ergonomically inefficient and cosmetically awkward gait .
To design a high performance, affordable prosthetic knee joint conforming to ISO 10328 standards to meet the occupational, sociocultural, religious, climatic and psychological needs of transfemoral amputees in India and the developing world.
The design of the Jaipur Knee was based on the versatile Polycentric concept. The development progressed through foam core modelling to 2D-CAD simulation of polycentric geometry to 3D-CAD modelling. The first prototype was ready for trial in August 2008. In 2009 the Jaipur Knee was hailed as one of the 50 best inventions of the world in that year. From 2008 to 2014 extensive clinical trials were conducted. Over 5000 transfemoral amputees were fitted with the Jaipur Knee in India and 1500 amputees across 12 different countries including Afganistan, Iraq, Columbia, Sri Lanka, Sierra Leone, Liberia, Pakistan etc.
The performance and impact of the design was studied using both categorical and descriptive outcome measure tools, including self reports, physical performance measures, time distance tests and QOL measures.
The immediate post fitting observations showed full extension at heel strike, voluntary stability through stance, knee flexion at toe off and through swing. Feedback in terms of patient acceptance, compliance and durability of the joint was very encouraging. However, there were issues of concern like the overly stable position at the end of stance, clicking sound at the end of swing, inability to carry out dynamic alignment and adaptors that only interfaced with the Jaipur technology. These problems were addressed and a modified version, renamed as the ReMotion Knee evolved. A pilot study of the ReMotion Knee is currently underway. It is being tested to ISO 10328 standards ; will be maufactured in an ISO 1345 certified facilty and will transition from clinical trials to market distribution by the second quarter of 2015.
The Jaipur Knee was the first polycentric knee, made accessible to transfemoral amputees from the bottom of the pyramid. Amputees in LICs are young, largely rural, from the lower socio-economic strata, mostly post traumatic, K3 –K4 level, are bread earners for their families and live in a physically and economically challenging environment. By remobilizing them with a high performance prosthesis we also provide an opportunity to break the cycle of poverty and disability
445
Impact of Dynamic Orthotic Approach on Fine Motor Development in Cerebral Palsy
Children with more severe paresis in upper limb muscles have a higher risk of developing contractures of the wrist and finger flexor muscles. Dynamic orthoses allow hemiparetics to participate in the latest treatment advances by incorporating their affected hand repeatedly for task-specific training. Using dynamic orthosis, repetitive task-specific training can be offered, challenging traditional neuro-rehabilitative concepts, including a paradigm shift from “proximal to distal” recovery to “distal to proximal” recovery.
The aim of this study was to evaluate the effect of dynamic hand orthosis on fine motor development in congenitally hemiparetic cerebral palsied children.
Thirty spastic hemiparetic children of both sexes participated in this study, selected from the outpatient clinic, Faculty of Physical Therapy, Cairo University. Their age ranged from three and six years and spasticity ranged between 1 to 1+ grades. Control group received specially designed rehabilitation program. Study group received same program but all fine motor skills were learned with using the dynamic hand splint. Peabody Developmental Motor Scale (PDMS-2) and JAMAR hand held dynamometer were used for assessment. Each treatment session was conducted for one hour. Sessions were conducted for 3 times/week for a period of three successive months.
Results showed significant difference for all measured variables. Post-treatment mean value of handgrip strength for control group was 3.81±1.3 Kg., while for study group, it was 5.09 ± 1.22 Kg. (P<0.05). Post-treatment mean value of fine motor quotient for control group was 48.2±1.78, while for study group; it was 51±2.17 (P<0.001). Post-treatment mean value of age equivalent for grasping for control group was 8.33±1.29 months. While for study group, it was 10±2.035 months (P<0.05). Post-treatment mean value of age equivalent for visual motor integration (months) for control group was 12.8±0.676 months. While for study group, it was 13.4±0.91 months (P<0.05).

From functional perspective, dynamic splints are most effective with children who have muscle weakness and those with mild increased tone. This means that, splints can maximize functional hand use. Dynamic orthotic approach with low profile, lightweight construction, is less likely to interfere with hand function.
It is concluded, dynamic orthotic approach is considered as complement to the traditional therapeutic modalities that are conducted for spastic hemiparetic cerebral palsied children.
446
Isao Ojima (1) presenting Akio Nakagawa (1) Satoshi Okubo (1)
Egypt, Kobe Gakuin University, Faculty of Rehabilitation, KObe, Hyogo prefecture, (1)
Non-amputee prosthetic gait training - energy consumption change from the first to the third training -

447
Vibhor Agrawal (1,2) Robert Gailey (1) presenting Ignacio Gaunaurd (1,2) Michael Greene (1) Shijia Geng (1)
Japan, University of Miami, Miami, FL (1) USA, Miami VA Medical Center, Miami, FL (2)
Comparing the symmetry of external work measure with traditional force plate parameters for differentiating prosthetic feet in unilateral transfemoral amputees
Mean (SD) symmetry indices for P1, P2, LR and SEW are presented in the accompanying table, where a symmetry index of less than 100% indicates a greater value of the parameter, for the intact limb. Preliminary results demonstrate that both feet had similar symmetry indices for peaks P1 and P2. LR values were numerically different between feet and noticeable differences between feet were evident for the SEW values.
Mean (SD) symmetry of assessed parameters

[1] Agrawal; 2009. Prosthet Orthot Intl.
[2] Hofstad; 2004. Cochrane Database Syst Rev.
[3] Agrawal; 2013. Prosthet Orthot Intl.
448
Vibhor Agrawal (1,2) Robert Gailey (1) presenting Ignacio Gaunaurd (1,2) Christopher Bennett (1) Gheiman Reyes (1) Adam Finnieston (1)
USA, University of Miami, Miami, FL (1) USA, Miami VA Medical Center, Miami, FL (2)
Changes in symmetry of external work due to prosthetic foot design characteristics during unilateral transtibial and transfemoral amputee gait

[1] van der Linde; 2004. J Rehabil Res Dev
[2] Agrawal; 2013. Prosthet Orthot Int.
[3] Agrawal; 2009. Prosthet Orthot Int.
450
Ban MASUHARA (1) presenting Akinobu SAKAMOTO (1) Kazuya IKOMA (2) Toru MORIHARA (2) Katsutoshi TACHIIRI (3) Torao KUSAKABE (3) Taku YAMASHITA (3) Shiro ISHII (3) Makoto TAKAHASHI (3) Masaharu OKUMURA (3) Haruo SOEDA (3)
Republic of Korea, Rehabitech, Kyoto (1) Japan, Kyoto Prefectural University of Medicine, Kyoto (2) Japan, Subcommittee of model projects for locomotorium school physical examination in Kyoto Medical Association school health committee, Kyoto (3)
Development of a device for simultaneous recording of rear foot alignment and footprint configurations in a static standing posture
Foot deformities such as pes planus and pes cavus are reported as risk factors which may cause sports injuries of lower extremity. From a view point of injury prevention, screening both rear foot alignment (RFA) and foot print configuration (FPC) at the same time contains useful information. Especially since use of X-ray observation still have a hazardous problem, it is preferred to employ a way which avoid use of X-ray and still perform an effective screening.
The objective of this study is to develop a device to record and store an individual RFA and FPC as digital photo data. There are three constraint conditions in the device design, which are 1) Any operator can operate the device easily without a special training. 2) The device is kept hygienic and safe to examinee. 3) The device can be set up and perform at any places.
Two cameras which are an USB video class type, were selected, because a real time subject posture can be checked on PC display. The developed software enables to display a view of RFA and FPC simultaneously on a laptop screen. To evaluate a performance of the device, error values between the screen shot and a real measurement were measured.
Four healthy male subjects are fully informed and consented to participate in this research. In Leg Heel Alignment (LHA) measurements, three markers of phi-8mm were placed at the posterior-coronal midpoint at the level of 1/3 height of lower limb, the insertion of Achilles tendon and Tuber Calcanei.
The foot length, foot width and LHA are calculated from captured image and compared with the actual values. There are errors of -3.1+/-2.2mm (Ave. +/-SE) in the foot length,1.0+/-2.0 mm in foot width and -0.8+/-1.2 degree in LHA. It is found that clarifying the border line of a contact area of foot and the background in the image happened to be difficult in some cases. To solve this problem, the room lights have to be turned off or the device has to be covered with black curtain to eliminate the unclear border in the image.

A device which captures a RFA and FPC are developed and its performance is tested. The test result shows this device obtains an accuracy of within 10 % error to actual measured values. In future work, an evaluation of accuracy of the device by comparing with CT and X-ray images will be necessary.
452
Marwa Ismaeel (1) presenting Amira El-Tohamy (1)
Hong Kong, Faculty of Physical Therapy, Cairo University, Cairo (1)
Flatfeet in response to Intensive Physical Therapy Approach in Egyptian School Aged Children
Foot is being to support the body weight and to serve, as a lever to propel the body forward in walking and running. Flexible flatfoot is foot, with a depressed medial longitudinal arch and a pronated subtalar joint underweight bearing conditions. Orthoses are seldom needed in the early years of growth. If supple flatfeet are seen to persist beyond ages six or seven, custom-made, flexible orthotics is appropriate.
This study determines effect of intensive physical therapy program based on orthotic approach as well as specially designed exercise program on changing the planter pressure in children with flat feet.
Thirty flatfeet children of both sexes selected from Egyptian governmental schools at Cairo. Their age ranged from 7 – 8 years. They followed normal average of weight and height (According to Egyptian scale for normal boys and girls). Weight and height scale, Toe standing and Jack toe-raise test and Foot scan using plate system were used for assessment. Designed rehabilitation program was based on Shoe insert, Non-Weight Bearing Exercises (from sitting position) and Weight Bearing Exercises (from standing position). Treatment session was conducted for about one hour as 6 sessions/week for three successive months as intensive Physical Therapy.
Comparing pre and post treatment mean value of study group revealed significant differences for all measured variables as shown in the table except that, pressure over 3rd right toe. It was estimated (p<0.05). Mean differences and percentage of improvement were calculated also for all measured variables.

Flexible flat foot due to ligamentus laxity and muscle weakness can be improved by strengthening the muscles that can help on forming longitudinal arch. Effect of shoe insert is momentary as it gives negative support to the arch without treating the cause. So it can be concluded that wearing shoe insert and performing intensive strengthening exercises are beneficial for the child having flat feet rather than using the insert alone.
454
Prasanna Kumar Lenka (1) Aratatran Patra (1) presenting
India, National Institute for the Orthopaedically Handicapped, Kolkata (1)
Analysis of Postural Parameters and Asymmetric Stability Margin in Persons with Transtibial Prosthesis by piezoresistive 3D Force Plate
455
Abedelkareem Elsabea (1) presenting
India, ALPC, Gaza (1)
A Polypropylene Partial Foot Prosthesis with Ankle Articulation
Because of recent armed conflict in Gaza there are numerous people with amputations, including partial foot amputations. Inspired by the designs of Groner (2013) and Wening (2008) and research by Dillon and Fatone (2008), the author has produced a novel design of Partial Foot Prosthesis (PFP) with supra malleoli suspension and dorsal wrap reinforcement which prevents bending of the Polypropylene (PP).This design has been developed and found useful for active partial foot amputees.
To describe a design of PFP that allows normal movement of the Talocrural joint, prevents PP bending in the mid foot area and allows for some PP bending at the MetaTarsal Head (MTH) area to simulate MTH dorsiflexion. This design suspends positively through an anterior supra malleoli shell with good comfort and function and is appropriate for K3 and K4 activity levels.
A person with Tarso-metatarsal amputation secondary to trauma was selected. A metallic free range ankle joint was used to allow free Dorsi and Planter Flexion. Casting and rectification was done according to PFP principles. The distal end was extended using Ethyl Vinyl Acetate (EVA). After draping PP with a dorsal join, trim lines were made in such a way that PP covers the dorsal foot proximal to the estimated MTH, stiffening this area. To simulate normal toe-break function this dorsal coverage does not extend past the MTHs allowing for some dorsiflexion. The device is donned from posteriorly.
The user’s performance was tested using this prosthesis based on International Classification of Functioning for activities and participations (d450-475). This includes brisk walking, running, climbing stairs and running with different speeds and on inclines, demonstrating excellent results. The user could walk more than 3km without getting tired. The rollover from heel strike to toe off was very smooth. The movement at the ankle joint and controlled toe break area simulated natural angular movements in normal gait. Three millimetre rubber sole pasted on the sole area with a heel strap attachment enabled the user to walk barefoot. This enabled him to use the prosthesis with shoes outdoors and without shoes at home as is the local custom.

The PFP design with use of ankle joint and controlled toe break encourages a natural gait pattern which demonstrates a higher functional outcome in the selected case. A more controlled study and biomechanical analysis are needed to generalize the functional benefits of this design over various available PFP designs, specifically to test the anterior excursion of the Centre of Pressure. The design also offers appropriate locally produced and economical alternatives to more expensive silicone and carbon fibre PFPs.
-Dillon MP, Fatone S, Hansen AH. Effect of prosthetic design on center of pressure excursion in partial foot prostheses. J Rehabil Res Dev. 2011;48(2):161–78.
-Groner 2013 http://lermagazine.com/article/debating-the-complexities-of-partial-foot-amputation accessed 20th September 2014
-Wening J, Ruzich J, Nunez R, Partial Foot Device for High-Level Ambulators. Academy Today http://www.oandp.org/academytoday/2008feb/3.asp Accessed 10th December 2014
-International Classification of Functioning http://apps.who.int/classifications/icfbrowser/
457
Masayuki Onuma (1) presenting Akira Magara (1) Yukio Agarie (1) Hironori Suda (1) Yu Maeda (1)
Occupied Palestinian Territory, Niigata University of Health and welfaew, Niigata-city (1)
Assumption of optimal compression value for the UCLA IRC trans-femoral socket in a Japanese amputee who has average residual limb length and average soft tissue consistency
Trans-femoral prosthetic suction socket needs certain amounts of compression. It is said for UCLA IRC sockets that 5 % circumferential reduction at ischial level is for amputee whose stump length is in average and has moderate soft tissue consistency. However, Some Japanese prosthetists have realized the fitting problems of soft tissue volume. Therefore we doubt about 5% compression value (CV). We apply rather less than 5% and assume Japanese trans-femoral amputees need a modified guideline of CV.
Making a proposal of the optimal CV of UCLA IRC trans-femoral prosthetic sockets for Japanese amputees, that was found out through the each socket fittings of patients whose stump is of average length and soft tissue consistency.
10 male trans-femoral amputees were recruited. All the subjects have average stump length and moderate soft tissue consistency. First, the UCLA IRC trans-femoral socket with 5% CV was provided for all the subjects. Then socket adjustments including changing volumes were done. Afterwards, a new plaster positive of each fitted sockets was made and the circumferential measurement of that renewed plaster molds was carried out to find out actual reduction from the nature stump. It is difficult to measure the ischial level circumference precisely. Therefore, the circumference of ischial level was calculated by the special formula we made. This is the result, which we have derived to circumference of level 25mm below, and we call then the optimal CV for Japanese amputees.
The average CV was 5% at the ischial level, which was uniformly used for calculation to goal circumference for our 10 subjects when modifying plaster mold at first. At that time, the CV at level 25 mm below was 4.3±0.2% before fitting process. After fitting, the CV at ischial level is 3.7±0.8% and there is significance differences (p<0.01) compared which was used at first to determine so called goal circumference. Furthermore, the CV at 25mm below level is 3.0±0.8% and there is also significance differences (p<0.01) compared which was used as the guideline before fitting.
It is surmised that the reason why the CV has become smaller at 3.7% might be influenced by some diffences in amount of soft tissue between Japanese and Western amputees. Japanese have smaller body mass index(Walpole et al. 2012) and subcutaneous adipose tissue at abdominal(Azuma et al, 2009). In addition, stratum corneum is also thinner (Komaore and Tsuruta, 1993). Because of those, we assume that the stump of Japanese amputee’s has mach less soft tissue than of the Westner’s. Therefore the socket might be too tight if 5% CV is applied.
458
Tamer El-Saeed (1) presenting Faten Abdel-Azeim (1) Ehab Ragaee (2)
Japan, Faculty of Physical Therapy, Cairo University, Cairo (1) Egypt, National Center for Research, Cairo (2)
Impact of Distal Static Orthotic Approach on Back Geometry in Cerebral Palsy
Hemiplegia comprises several pathological entities that result in limb weakness on one side of the body. Deformities of spine (scoliosis, kyphosis, and lordosis) are associated. As children gain ambulatory ability, main goal of orthoses becomes preventing plantar flexion. Formetric 3D measurement system dynamically scans and reconstructs human back surfaces. Automatically detectable fixed points and invariant features on surface correlates to a high degree of accuracy with spinal processes and pelvis.
The primary aim was to evaluate effect of different forms of static AFO on back geometry in hemiplegic cerebral palsied children. A secondary aim was to compare between these forms.
Thirty children of spastic hemiplegia between ages of six to eight years were studied. They were recruited from out clinic of Pediatrics, Faculty of Physical Therapy, Cairo University. They were assigned into two groups. Group A received specially designed rehabilitation program in addition to solid AFO while Group B received same designed rehabilitation program in addition to spiral AFO which was used for successive 3 months. Children of both groups received especially designed therapeutic exercise program based on the neurodevelopmental technique principles. Each treatment session lasted one hour and was conducted at 3 times/week basis for 3 successive months.
Comparing the pre and post treatment results of children of both study groups revealed significant improvement of all measured variables (p<0.05) including fontal profile parameters {Trunk length, Trunk imbalance, Pelvic tilt, Pelvic torsion and Surface rotation (rms)} and sagittal profile parameters {Trunk inclination and Kyphotic Apex} which may be attributed to effect of the designed rehabilitation program including orthotic approach as well as exercise program. On the other hand, there was no significant difference (p>0.05) when comparing post treatment means values of both groups which mean that, there is no significant difference between using either solid or spiral AFO.
Ankle Foot Orthoses correct the position of the foot. So base of support will improve and make standing easier. As a whole, we can conclude that wearing an AFO improves the static postural control significantly. Researchers consider significant value of using either solid or spiral AFO as complement to traditional therapeutic exercises that are conducted for hemiplegic children as long as the treatment conducted for suggested period of study.
459
Kathy Mak (1) presenting Alexander Au Yang (2)
Egypt, Princess Margaret Hospital, Hong Kong (1) Hong Kong, Prince of Wales Hospital, Hong Kong (2)
The Effect of Soft Lumbar Corset on Postural Stability in Patients with Chronic Low Back Pain during Standing
Soft lumbar corset is one of the common conservative interventions for patients with low back pain (LBP). The efficacy of lumbar orthosis in pain reduction has been shown previously but there is not much information about the mechanisms of how soft lumbar corset improve postural stability. The mechanisms of action of lumbar orthosis remain a matter of debate.
The study was designed to investigate the effect of soft lumbar corset on postural stability in patients with chronic low back pain (CLBP) during standing by the interpretation of center of pressure (CoP) measurement.
The study recruited 15 subjects with LBP for more than 3 months, without neurological disorders, vestibular diseases or deformity of spine. The subjects performed upright standing on a force platform for 70 seconds for the measurement of CoP parameters, which were used to evaluate the postural stability. Paired- t test was used for the comparison of stability with and without a soft lumbar corset.
The results showed significant decrease in total mean speed (p = 0.001), mean speed in antero- posterior (AP) (p = 0.006) and medial – lateral (ML) (p = 0.047) directions while using a soft lumbar corset. There were also significant decrease in AP range (p = 0.025) and ML range (p = 0.016) of CoP when using a soft lumbar corset.
The information provided by a force platform suggested that using a soft lumbar corset may help CLBP patients to improve postural stability in upright stance. More large scale study is suggested to confirm the beneficial effects of using soft lumbar corset in stability in LBP group.
461
Richard Collins (1) Greg Bowring (1,2) presenting
India, The Prince of Wales Hospital, Randwick, NSW (1) Australia, The University of NSW, Kensington, NSW (2)
Let’s go hiking: learning to walk again using microprocessor-controlled prosthetic knee joints. A five case series
Potentially, new generation microprocessor-controlled prosthetic knee joints (MPKs) provide significant functional benefits for amputees. However, they are costly in comparison to most other components. Consequently, clinicians need strong arguments to justify such requests to funding bodies. Much publicity has concentrated on high end functionality such as advanced stair climbing and running.
Subject 1: Crushed between 2 cars. Right through-knee amputation.Other injuries included: compound fracture (L) tibia requiring open reduction internal fixation and skin grafting. Prolonged period prior to fitting.Two school age children.
Subject 2: Type 2 diabetic with peripheral vascular disease. Right trans-femoral amputation (TFA) and left below knee amputation. Prolonged period immobile prior to TFA. Initially told he would never walk again.
Subject 3: Motorbike accident. Right TFA and right trans-radial amputation.
Subject4: Run over by a garbage truck. Right TFA. Other injuries included a fractured left acetabulum requiring total hip replacement and left knee lateral ligament injury. Significant pre-existing medical problems.
Subject 5: Right TFA. Right femoral nerve palsy and multiple failed orthopaedic procedures prior to amputation, including three total knee replacements.

MPKs have been shown to benefit all patients in this small but varied sample. Both K4 subjects rapidly obtained independence even after prolonged periods of immobility. Arguably, subjects two and four moved up a K level as a direct consequence of MPK use. Subject two was mobilising outdoors when he had initially been advised that he would never walk again. Subject four achieved goals which until that time had proved impossible with a NMPK. Prior to revision surgery, subject five was mobilising outdoors without crutches for the first time in many years. One patient fell during prosthetic training.
Case studies have limited generalizability. Resources and subject numbers limit the practicality of an independent study providing higher levels of evidence in this instance.
462
Donna Fisher (1) presenting
Australia, Ottobock, Dublin (1)
The Effect Of Alignment On The Balance And Confidence Of Trans Femoral Prosthesis Users
The alignment of a trans-femoral prosthesis is crucial and may affect socket pressures, stability and the function of lower limb components. Traditionally alignment is performed using observation, clinician experience and feedback from the prosthesis user (1).
A stable prosthesis can promote comfortable gait and function for the prosthesis user and may increase user confidence. Falling and fear of falling, is a recognised issue for trans-femoral prosthesis users and can be linked to balance and confidence (2). A clearer understanding of the effects of prosthetic alignment on this lower limb absent population could lead to improvements in balance and confidence (3).
The purpose of this pilot study was to assess the effect of prosthetic alignment on the balance and confidence of trans-femoral prosthesis users.
The prosthetic alignment of five non-vascular trans-femoral prosthesis users were recorded using a bench alignment apparatus. The hip range of motion of each participant was assessed using the Thomas Test to establish the recommended socket flexion angle for bench alignment and compared to the socket flexion in the original prosthesis alignment.
The Activities-specific Balance and Confidence Scale ABC was used to determine user baseline balance and confidence with the original prosthetic alignment.
Each prosthesis was then re- aligned using two pre-determined angles of initial socket flexion. Dynamic alignment was conducted without adjustment to socket flexion or extension above the knee joint and the effect of compensatory adjustments noted. The resulting dynamic alignment of each configuration was compared using the bench alignment apparatus.
Each participant was assessed using the L-Test and Four Step Square Test in each of the alignment configurations of their everyday prosthesis.
Results showed a high level of balance confidence (Mean ABC = 86.6, s.d. = 8.1), walking ability (Mean L-Test = 24.77 seconds) and balance (Mean FSST = 12.43 seconds) in all alignment configurations. No statistically significant differences were found in the times recorded for the L-Tests and FSST, for any participant, in any alignment configuration.
The participants were able to function to a high level, even with significant changes in the initial angle of flexion of the prosthetic socket. This indicates healthy, active prosthesis users can adapt using compensatory movements to accommodate for changes in prosthetic alignment. The clinical significance of these compensatory movements requires further investigation.
Future research to promote understanding of the influence of prosthetic alignment and the effects of compensatory movements on balance and confidence is required. Such work is important to facilitate long-term optimal functional ability of the prosthesis user.
1. Radcliffe CW. The Knud Jansen Lecture: Above-knee prosthetics. Prosthetics and Orthotics International. 1977;1(3):146-60.
2. Miller WC, Deathe AB, Speechley M, Koval J. The influence of falling, fear of falling, and balance confidence on prosthetic mobility and social activity among individuals with a lower extremity amputation. Archives of Physical Medicine & Rehabilitation. 2001;82(9):1238-44.
3. Blumentritt S. A new biomechanical method for determination of static prosthetic alignment. Prosthetics & Orthotics International. 1997;21(2):107-13.
463
Isabelle Loiret (1) Philippe Vuistiner (2) Yvan Arlettaz (3) Mathieu Assal (4) Olivier Borens (5) Laure Huchon (6) Noël Martinet (1) Jean Paysant (1) presenting François Luthi (2)
Ireland, Centre de rééducation Louis Pierquin, UGECAM Nord-Est, Nancy (1) France, Clinique Romande de réapdaptation, Sion (2) Switzerland, Hopital de Martigny, Martigny (3) Switzerland, Clinique de la Colline, Genève (4) Switzerland, CHUV, Lausanne (5) Switzerland, CHU, Lyon (6)
Cross-cultural adaptation, reliability, internal consistency and validation of the Trinity Amputation and Prosthetic Experience Scales-Revised (TAPES-R) for French speaking patients with lower limb amputation
The Trinity Amputation and Prosthetic Experience Scales-Revised (TAPES-R) is a self-reported multidimensional amputee-specific questionnaire [1]. The 33 items evaluate psychosocial adjustment (3 subscales), activity restriction (1 subscale) and satisfaction with prosthesis (2 subscales). This measurement has been translated into several languages such as Swedish, Italian, and Persian [2].
The aim of this study was the French cross cultural adaptation and validation of the TAPES- R (TAPES-R-F) in a lower limb amputation population.
129 patients (23% women) with a mean age of 62 years and with lower limb amputations for at least 1 year (vascular 75%, traumatic 25%) were recruited in 5 clinical centers. Translation and cross-cultural adaptation were made according to international guidelines. Internal consistency of each subscale was measured with Cronbach’s alpha. Test-retest reliability was assessed by intraclass correlation in a sub- group of 24 subjects who completed the TAPES-R twice with an interval of 5 to 7 days. Construct validity was estimated through correlations with two main components of SF-36. Correlations were also calculated with some scales of the Brief Pain Inventory (BPI): pain severity, highest pain and pain interference with activities.
Cronbach’s alpha was high, ranging from 0.85 for the Adjustment to limitation subscale, to 0.95 for the Aesthetic satisfaction with prosthesis subscale. Reliability was acceptable to high (ICC=0.72 to 0.91) for all subscales with the exception of the Social adjustment (ICC=0.67) and Adjustment to limitation (ICC=0.42) subscales. The PCS component of SF-36 was significantly correlated with all subscales (r=0.24 to 0.66) as was the MCS (r=0.30 to 0.58), except with Aesthetic satisfaction and Adjustment to limitation. Regarding the BPI, significant correlations were found for all subscales (r=-0.20 to-0.68) with the exception of Adjustment to limitation. Ceiling or floor effects (>15%) were found for all but Activity restriction and Functional satisfaction scales.
The TAPES-R-F has acceptable psychometric properties for most of its subscales. Our results may suggest that the French version is more useful in a population research perspective than in an individual perspective. Other studies are necessary to clarify the role andthe psychometric properties of this measurement.
[1] : Gallagher et al., Arch Phys Med Rehabil;85 :730-6,2004
[2] : M. Mazaheri et al., Disability and Rehabilitation,33(19-20):1737-1745,2011
464
Yukio Agarie (1) presenting Hironori Suda (1) Hiroshi Otsuka (2) Fumiko Tayama (3) Akihiko Hanabusa (3) Shinichiro Yamamoto (3) Masayuki Onuma (1) Yu Maeda (1)
France, Niigata University of Health and Welfare, Niigata (1) Japan, University of Human Arts and Sciences, Saitama (2) Japan, Shibaura Institute of Technology, Saitama (3)
A Casting Technique Which Makes Well-fitting Ischial-Ramal-Containment (IRC) Socket - Manual Compression Casting Technique :MCCT IRC Socket-
Fabrication of UCLA IRC sockets focus mainly on positive model modification. Proximal two-thirds of length of positive model is shaved to match aim circumference calculated with compression value, and 4cm distal to ischial tuberosity (IT) level is shaved to match specific shape of socket. Thus, shape of residual limb is damaged. Moreover, soft tissues of residual limb elongate when compression value is applied, which causes incongruity between residual limb and socket and makes fitting difficult. Since 1994, we had been developing a casting technique which compression value was directly applied and socket was shaped by manual technique.
MCCT was expected to decrease the time spent on socket fabrication and fitting, which reduced the loading of both prosthetists and amputees.
MCCT was based on the concepts of UCLA IRC socket. The following principles were essential:
1. Compression casting: elastic plaster bandages were used, and compression value was directly applied to residual limb. At the same time soft tissues elongated and this shape could be captured.
2. Mechanical elements of casting and manual technique: forces were applied to anteroposterior and mediolateral directions to increase stability in stance phase, which were known as AP and ML lock. The skeletal ML lock was the force vector from medial aspect of IT to femur shaft as skeletal AP lock was from Scarpa’s triangle to IT. The ML lock of soft tissues was the force vector from adductors/hamstrings to femur shaft as AP lock was from Scarpa’s triangle to hamstrings.
3. Accurate capture of residual limb’s shape: anatomical structures of residual limb should be clearly captured so that socket could accurately match.
Compare MCCT negative model with UCLA model, the former showed the shape nearly the same as aim shape of socket which made less time cost on positive model modification. Also, elongation of residual limb was captured so that volume of socket corresponded to the residual limb and fit well. AP and ML locked properly, which maintained the stability in ambulation even when trim lines of anterior and posterior walls were low. MCCT also did well with liner.

The development of MCCT reduced the time spent on prosthesis fabrication and socket fitting compared with original method. However, wrapping of elastic plaster bandage and manual technique during casting depended on each prosthetist’s experiences. Therefore, further improvement was expected in the future. Deta analysis of MCCT is now in progress.
465
Tetsuo Yamada (1) presenting Hisato Sasaki (1) Kazusige Iisihara (1) Sigeru Morinaka (1) Nobuo Nakanisi (1)
Japan, Hiroshima International University, higasihirosimasi (1)
The effect due to the difference in height position of the joint of the anterior cruciate ligament injuries therapeutic knee orthosis
More of knee brace for ACL injury treatments aim to control knee extension, or to keep location between tarns-femoral (btt) and trans-tibial. Effect of those knee brace have been not substantial observed for treatment of ACL injury because occurred slipping btt by propagate threw soft tissue.(1,2)
We developed knee brace which can change btt by change upward shift joint location from physiological knee joint, and force tibial tuberosity by shell of knee brace from anterior for reducing stress of ACL
The idea of this ACL knee brace is setting its joint anterior to physiological joint. In this study we modified its setting area to vertical direction. Its range of adjustment is 2 cm superior to physiological joint position. Pressure measurements have done on tibial tuberosity, posterior 15 cm down from knee and posterior from thigh knee axis. FSR-400 Pressure sensors (Interlink Electronics Inc.) have used and sampling rate was 10Hz.
2 subjects who are physically unimpaired were measured by tree passion that physiological knee joint, forward 1 and 2cm from physiological knee joint with the brace what peak of pressure during repeated each flexion and extension movement.
It was observed he more axis of knee joint was shifted to anterior, the more the pressure increased significantly.
These changes can be considered trans-tibial slide to backward against trans-femoral when flexion more than extension of knee by knee joint of the brace was set up above physiological knee joint. ACL is developed maxim tension between from full extension of knee to 30°knee flexion, it is declined tension over 30°knee flexion.(3) Liability relief of ACL is very important for treatment at initial flexion. We will masseur more subjects for to research relationship between location of knee joint of the brace and pressure, and develop the brace for ACL injury.

(1)Tomoo Kato: knee anterior cruciate ligament damage and brace, Public Interest Incorporated Orchestra Japan American Physical Therapy Association, Physical Therapy 19 (3), 276-281, (1992)
(2)Harilainen A, Sandelin J, Vanhanen I, et al : Knee brace after bone-tendon-bone anterior cruciate ligament reconstruction. Randomized, prospective study with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc. 1997;5(1):10-3
(3)Hirokawa Shunji :Biomechanics of the knee joint influenced by agonist and antagonist muscle contractions Society of Biomechanisms Japan (SOBIM) Bio mechanism 11, 153-165(1992)
466
Ejaz Ali Khan (1) Zia Ur Rehman (1) presenting Shazia Asif (1)
Japan, Pakistan Institute of Prosthetic and Orthotic Sciences, Peshawar (1)
Problems And Causes Of Explosive Remnants Of Armed Fighting- A Kpk/Fata Case Study
The study focuses on recent surge in the landmines and Unexploded Ordnance incidents to civilian population in KPK/FATA areas. The exact extent of the problem is far from known due to various reasons including access issues to affected areas, absence of a centralized authority at the government level to recognize and encourage Mine Action activities and so on and so forth. The research study strives to collect, as much as possible, the tiny bit of information to highlight the scope and the causes of landmines and other Unexploded incidents in Pakistan, particularly in KPK/FATA.
To highlight the suffering of people, living in conflict and post conflict areas of KP and FATA, in relation to weapon contamination and understand the existing knowledge, attitude and practice of people exposed to threat of landmines and UXOs
The research study drew on both primary and secondary data. Primary data was acquired from the physical rehabilitation center in Peshawar whereas secondary data was obtained from research study on the topic, newspaper incident reports, ICBL and other mine action In addition, a well-structured questionnaire was developed to interview survivors of either landmine or other unexploded ordnance. The aim of this process was to collect data from victims/survivors on the circumstances in which incidents occurred. Before the final use of questionnaire, a pilot test was conducted with two victims at PIPOS. A few shortcomings in the questionnaire were noticed and rectified reports and the researcher’s own experience on the subject.
Discussion with people living in potentially dangerous areas and with survivors reveal the extreme vulnerabilities of civilian population to landmines and unexploded devices in the study areas. In addition, the most recent incident of UXOs in Buner (where two children and a woman were killed due to explosion of a suspicious item that they tampered with) indicates that the UXOs are extremely dangerous even long after the hostilities end and become utmost sensitive and unpredictable with time
Study explores different causes of landmines and unexploded ordnance incidents to common people, which could be/have been avoided in the first place. Some of the causes include lack of knowledge about the risk of explosive remnants, economic necessities that force people to take risk, misperception about explosive devices and so on.
Each new explosive remnants incident means someone killed or injured (injuries mostly end up in amputation) somewhere in FATA/KPK. The situation is alarming as more and more people are incapacitated by the landmines and UXOs incidents in the FATA/KPK. There is an urgent need for giving a proper heed to this menace before a big chunk of population in the study areas become huge burden on our sluggish economy
467
Eva Haggstrom (1,2) presenting Kerstin Hagberg (1,2) Roy Tranberg (1)
Pakistan, Dept. of Orthopaedics, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Sahlgrenska University Hospital, Gothenburg (1) Sweden, Dept. of Prosthetics and Orthotics, Sahlgrenska University Hospital, University of Gothenburg, Gothenburg (2)
Implant loading during walking and riding a stationary bicycle with a bone-anchored transfemoral prosthesis - a pilot study using the iPec instrument
1. Branemark, R., et al., A novel osseointegrated percutaneous prosthetic system for the treatment of patients with transfemoral amputation: A prospective study of 51 patients. Bone Joint J, 2014.
2. Koehler, S.R., Y.Y. Dhaher, and A.H. Hansen, Cross-validation of a portable, six-degree-of-freedom load cell for use in lower-limb prosthetics research. J Biomech, 2014.
3. Lee, W.C., et al., Kinetics of transfemoral amputees with osseointegrated fixation performing common activities of daily living. Clin Biomech (Bristol, Avon), 2007.
468
Sarah Day (1) presenting Nurnazlyna Mohd Bahtiaraffandi (1)
Sweden, University of Strathclyde, Glasgow, Scotland (1)
Employing International Classification of Functioning, Disability & Health (ICF) in the comparison of use and acceptance between trans-radial body-powered and myoelectric prostheses
The difference in use and acceptance between upper- and lower-limb prostheses is recognized but it is less so between the two functional types of upper-limb prostheses – body-powered and myoelectric. Additionally, majority of upper-limb prosthetics research greatly involves trans-radial prosthesis users thus facilitating a comparison of both types of prostheses at this level. In doing so, the International Classification of Functioning, Disability and Health (ICF) which has three activity domains – activities of daily living, employment or education, and recreation & social activities – could establish the level of activities & participation as well as activity limitation/participation restriction achievable by each trans-radial prosthesis.
To investigate the actual use, perceived usefulness and inherent limitations, all of which contribute towards activities & participation, and activity limitation/participation restriction, of trans-radial body-powered and myoelectric prostheses in the three activity domains of the ICF. These investigated aspects would therefore be analysed to understand the difference in use and acceptance patterns between them.
Literature review – Literature published between 1980 and 2014 was searched across five databases using 52 relevant keyword combinations. Four inclusion and two exclusion criteria were applied in selecting relevant papers. Neither reviews of references from the included articles nor consultations with experts were made to acquire further literature. Papers were graded using NICE 2012 and SIGN50 guidelines prior to being reviewed to elucidate the results of the research objectives .
The literature search retrieved 8799 articles but only 23 were included for review. Specific activities emerged under each type of ICF activity domain (Table 1), which were relevant only to two of the investigated aspects of actual use and perceived usefulness. For the final investigated aspect of inherent limitations, eight factors relating to financial, functional and physiological factors were featured.
Specific activities under each type of ICF activity domain

Use patterns of trans-radial body-powered and myoelectric prostheses were similar in activities of daily living, education and hobbies while each type was suitable for specific employments. Body-powered was used greater in sports/outdoor recreation whereas myoelectric had superior use in social activities.
Myoelectric was generally more accepted than body-powered although this deduction could vary accordingly.
World Health Organization. International Classification of Functioning, Disability & Health. Geneva, Sweden: World Health Organization; 2001.
469
Heidi K W Mak (1) Rie Nagai (1) Tsurayuki Murakami (1) presenting
UK, Tan Tock Seng Hospital, Singapore (1)
Efficacy of early cranial orthotic intervention in the treatment of deformational plagiocephaly in Singapore
There is emerging evidence that cranial orthotics (COs) can effectively manage deformational plagiocephaly (DP) with appropriate timings of intervention. Intervention periods vary among the different literature but there is a consensus that early intervention gives greater results within the first year of birth. Currently, there is no literature reporting on results within the Singaporean or South-east Asian population.
The aim of this study is to analyse the effectiveness of COs in the management of DP based on timing of intervention and to report on results within the Singaporean population.
Retrospective clinical data were gathered from discharged patients seen at Tan Tock Seng Hospital. Anthropometric measurements were done by qualified orthotists, according to a standardised, valid and reliable protocol.1 The CO was casted, manufactured, and fitted on-site in the same facility. Paired samples t-test comparison of overall pre to post-treatment measures, and independent 2-tailed t-test comparison between early (≤6months age) and late (>6months age) intervention groups were done.
30 patients were discharged between 2013 and 2014. Mean cranial vault asymmetry index (CVAI) decreased from 9.3% (S.D. 3.5%) to 3.8% (S.D. 2.9%) at discharge, and overall CVAI percentage correction was 57.7% (p<0.0001). Pearson corrélation of CVAI percentage correction and percentage growth was moderate (r=0.38). Early intervention allowed slightly shorter (mean 3.0months; n=15) but insignificant (p=0.23) treatment lengths compared to late intervention (3.4months; n=15). CVAI percentage correction was similar in early (58.1%) and late (57.2%) intervention with no significant difference (p=0.47).
The number of CO referrals for DP is negligible in proportion to the birth rate in Singapore; the prévalence of DP may not be comparable to Western countries or there is a poor awareness of orthotic interventions in Singapore. Overall correction achieved with COs was significant, although it was difficult to analyse the extent of correction directly due to CO usage alone without doing a controlled trial, as most patients had adjunct physical or repositioning therapy. Patients were also discharged when parents were pleased with the acquired head shape, regardless of whether further correction was possible. Correlation of correction achieved and head growth was moderate, and other factors need to be further investigated such as compliance, sternocleidomastoid tone, cervical range of motion, extent of adjunct treatments and orthopaedic or neurological conditions.
Early intervention did not allow shorter treatment lengths or greater correction as expected, compared to late intervention. Treatment lengths could be influenced by decreased compliance with late intervention and hence treatment could not be continued as intended. As the infant grows older, he/she will be able to actively remove the CO, affecting compliance. However, correction achieved was still similar in both groups. The initiation of CO treatment could possibly be deferred to 6months of age while less invasive interventions are trialed.
1. Wilbrand JF, Wilbrand M, Pons-Kuehnemann J, et al. Value and reliability of anthropometric measurements of cranial deformity in early childhood. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2011; 39: 24-9.
471
Marcelo Lofiego (1) presenting
Russia, Ortopedia Alemana, Buenos Aires (1)
Effect of an EXTENSION ASSIST DEVICE on knee extension in patients fitted with stance control orthoses
KAFO: No knee flexion in swing phase.
SCKAFO WITHOUT ASSISTED-EXTENSION: Flexion curve was similar to normal subjects.
SCKAFO WITH ASSISTED-EXTENSION: Peak knee flexion of 45% compared to normal, reaching 30º as compared to 70º observed in curve of normal subjects.
GRAPH SHOWING KNEE KINEMATICS

Lower limb fitted with orthosis
An extension assist device is frequently used initially to achieve knee extension, without providing the necessary training in the SCKAFO rehabilitation protocol. Hence, these patients lose some of the benefits that SCKAFO provides regarding knee flexion, since it decreases to 45% compared to SCKAFO without extension assist.
We have fitted 137 SCKAFO, 34 with extension assist and 133 without gnee.
472
G.M. (Clemens) Rommers (1,2) presenting Barbara Engelen-Schouten (1,2) Hans Emmen (3) Ronald JAM Slegers (1) Martijn PM Dremmen (2) Nicolaas C Schaper (1)
Argentina, Maastricht University Medical Center, Maastricht (1) The Netherlands, Adelante Rehabilitation Center, Hoensbroek (2) The Netherlands, Smeets Loopcomfort, Sittard (3)
Partial foot amputation in diabetes mellitus: what can orthopaedic footwear accomplish?
The treatment of a diabetic foot ulcer (DFU) is challenging and complex. The team approach of the doctor, podiatry expert and orthopedic shoe technician are important in the multidisciplinary diabetic foot team.
The aim of this audit was to determine the recurrence rate of a DFU after a partial foot amputation when high shaft shoes with rigid counterfort and rocker bar, guided by in shoe-plantar pressure measurements (Pedar-X ®), are prescribed.
Patients with a recent partial foot amputation because of a DFU in 2011-2014, and treated by our multidisciplinary team were identified and their electronic records reviewed. All patients were prescribed therapeutic footwear with the aim to reduce peak plantar foot pressure below 250 kPa. The ulcer free period was calculated as the time between shoe prescription and recurrence of a DFU.
Nineteen diabetic patients with a recent partial foot amputation were included. The mean duration of diabetes was 22 years; 32% were female with a mean age of 63 years. The level of amputation varied between a ray and a Chopart amputation. The post-operative pressure measurements suggested that especially the more proximal amputations were adequately offloaded by the prescribed shoe-wear. All patients had a recurrent ulcer during a mean duration of follow-up of 20 months, with a mean ulcer free period of 166 days. One patient had a transtibial amputation.
From partial foot amputation to orthopaedic footwear

The results of pressure guided prescription of therapeutic footwear after partial foot amputations were disappointing given the relative short ulcer free period. We did not measure compliance in wearing the prescribed shoes, but several patients informed us that they were incompliant. Further research is needed on to guide amputation level selection in an individual patient, to improve off-loading of the therapeutic footwear and in particular to develop strategies to improve compliance.
473
Sandra Sexton (1,2) presenting
The Netherlands, Rehabskills Ltd, Wishaw (1) UK, ISPO, Brussels (2)
Using the evidence base to improve professional practice in a prosthetic and orthotic service in Malawi, a Low Income Country
Evidence based clinical practice is about using the best available evidence in decision making in clinical services. Where professional development needs are identified for specific conditions, the published evidence can provide a rich source of information about how to assess, prescribe and design prosthetic and orthotic devices. In Malawi, a Prosthetics and Orthotic Centre has been using the evidence as part of a quality improvement effort.
The aim was to understand the scope and complexity of clinical presentations in Lilongwe, Malawi and to encourage evidence based practice to improve the quality of prosthetic and orthotic provision.
During 10 months in 2014, the 500 miles Prosthetics and Orthotics Centre, Kamuzu Central Hospital, Lilongwe, Malawi hosted a mentor Prosthetist/Orthotist. This was during the fourth of a five year development plan in the Hospital as part of an agreement with Sophies Minde Hospital, Oslo, funded by FK Norway, the Norwegian Peace Corps.
Throughout the period, a number of clinical and technical practice development needs were identified relating to the prosthetic and orthotic care of patients attending the Centre. Selected published reports and scientific papers were sought and shared with the team and improved clinical and technical practices introduced.
Early in the project, the need to improve the management of children with cerebral palsy was identified. Discussions in the local team were augmented by two formal continuing professional development days when two of the Malawian 500 miles national services were brought together in a larger group and considered published literature for gait analysis and tuning of AFOs.
Other evidence about proximal focal femoral deficiency, traumatic spinal fractures and spinal TB was also introduced to the teams.
Following this, appropriate practice was encouraged. The teams were able to demonstrate improved techniques resulting in more appropriate device provision. Two of the clinicians presented associated case series at national conference and won two of the five available awards for best presentation. They continue to learn more by reflecting on their practice.
The published evidence can be used as an effective lever to change practice in services. Both the mentor and mentees benefitted from a deeper understanding of assessment and treatment methods resulting in more appropriate prosthetic and orthotic devices. Significant limitations exist, however, in the low income setting where clinicians lack skills in how to find and read evidence and rely too heavily on knowledge gained in pre-professional training alone.
Ramstrand and Brodtkorb, 2008. Considerations for developing an evidenced-based practice in orthotics and prosthetics. Prosthetics and Orthotics International . 32 (1). 93-102.
474
Rowan English (1) presenting
Belgium, International Committee of the Red Cross, Dhaka (1)
Building P&O in Developing Countries – A New P&O Education Program in Bangladesh
Bangladesh is a densely populated country in South Asia with many physically disabled. The Bangladesh Health Professions Institute (BHPI) has established the first school of P&O in the country. Developing the educational program within organizational limitations, national requirements and international guidelines has created numerous challenges. The International Committee of the Red Cross (ICRC) partnered with BHPI to help meet these challenges with a practical approach, combining previous experience with modern educational practices.
To partner with, assist and mentor the development of a sustainable educational program in P&O. It should have a national impact and meet ISPO guidelines at a category 2 level.
ICRC identified the need to provide P&O services for Bangladesh and that to ensure sustainability an education program was required. It was decided to partner with a local organisation to develop and run an educational program. BHPI had been keen to run a P&O course alongside its other allied health programs for some time. Governmental approval had been provisionally received for the P&O course in 2013. Detailed curriculum was developed, physical infrastructure built, equipment procured and suitable staff hired. Students were selected and began their study in the common first year of the course this year, 2014. A second cohort has been selected for 2015.
While the national curriculum was approved provisionally, it did not meet the ISPO guidelines and a substantial reworking was required to meet these and national guidelines. A full curriculum was redeveloped and final approval was received. Physical facilities were built and fitted out in a partnership with ICRC and the German government: a two storied school built above the existing P&O clinical service. The clinical service is being refurbished to allow accommodation of students in their internship year. Expatriate staff members are teaching and developing detailed teaching material. The first intake of 10 students (5 male, 5 female) for 2014 are undertaking their studies with provisional results showing a 100% success rate. The second intake of 10 students (8 male, 2 female) have been selected for 2015 entry.
There is an established need for P&O services in Bangladesh. It is essential that any educational programs are sustainable to have any chance of meeting the long terms needs. The first P&O school in Bangladesh is now operational, with a curriculum that is designed to satisfy national and international criteria. There are new custom built physical facilities and a commitment of ongoing support from the ICRC.
475
Zala Kuret (1) presenting Helena Burger (1)
Bangladesh, University Rehabilitation Institute, Republic of Slovenia - Soca, Ljubljana (1)
Quality of life in lower limb amputees
Rehabilitation following a lower limb amputation usually involves restoring function with the use of prosthesis. Amputation has an important impact on physical and psychosocial functioning and influences quality of life. Quality of life is not well researched but there is an increasing acknowledgement, since clinical practice is becoming more patient-centred and evidence based.
The aim of our study was to evaluate patient satisfaction with the prosthesis for lower limb amputations and how amputation influences their quality of life.
We included patients with lower limb amputation who were examined in our outpatient clinic in July and August 2013. To evaluate function of the prosthesis and the major health related quality of life domains we used Prosthesis Evaluation Questionnaire and 5-item World Health Organization Quality of Life Assessment (WHOQoL-5).
We included 25 patients. Most of them (twenty-two) had transtibial amputation, two had transfemoral amputation and one patient had knee exarticulation. The majority of amputations were due to trauma (44%), followed by peripheral artery disease (28%) and diabetes (16%).
PEQ is composed of 9 validated scales, highest scores were achieved in Perceived Responses (91), followed by Social burden (79), Frustration (77), Well-being (75), Utility (66), Sounds (65), Appearance (65) and scores were the lowest in Ambulation scale (61). Similarly results of WHOQoL-5 were also all quite high; the highest was satisfaction with home environment (7.9) and personal relationships (7.8), the lowest was health status satisfaction (6.7).
Patients in our study report good results on all PEQ subscales and also on WHOQoL-5. It is known that greater satisfaction with the prosthesis and lower levels of phantom limb pain and stump pain are associated with positive adjustment to limb loss (1). Also satisfaction strongly correlates with the PEQ scales, particularly ambulation, prosthetic utility, frustration, perceived response and social burden (2).
1.Horgan O; 2004, Disabil Rehabil.
2.Kark L; 2011, Prosthet Orthot Int.
476
Yuji Nagakura (1) presenting Hironori Hamamoto (1) Toshihiro Nagao (1)
Slovenia, 325 Izumi-machi, Kumamoto,Kumamoto (1)
The relationship between the physical performance and walking speed for trance femoral amputees
Procedures: Physical performance measurement for Amputees
1. Walking time and steps for maximum and usual waking speed at 10m distance.
2. Timed up and go test walking time and steps (TUG).
3. One leg standing time on prosthetic side in open eyes.
4. One leg stand up from a chair 10 repetition times.
Muscle strength measurement by JTECH Medical co. Power Track 2. The non-stretchable of isometric muscle strength muscle of the target for 3 seconds around the hip joint to use the fixing belt was measured
Data analysis: SPSS statistical package, non-parametric one-way ANOVA for muscle strength. We calculated the maximum walking speed and a correlation with each physical performance measurement using a Pearson product-moment correlation coefficient.

477
Sharah Abdul Mutalib (1) presenting Etienne Burdet (1) Alessandro Allievi (1)
Japan, Imperial College London, London (1)
An Instrumented Toy for the Assessment of Hemiplegic Cerebral Palsy Infants
Table 1 summarises the performance of each subject during the bimanual lifting tasks. The duration of completion time, maximum grasping force, and presence of any reversed movement (downward motion of the cube before lifting) or impact during unloading the cube was monitored. Younger subjects demonstrated poorer performance in terms of force coordination and movement stability than the older subjects, denoted by the higher amount of grasp force and longer duration to complete the task than older subjects.

479
Franz Landauer (1) presenting Karl Vanas (1) Alexander Henhapl (1)
Thailand, University Clinic of Orthopedics (PMU), Salzburg (1)
The Insole-concept to compensate the equinus component after arthroereisis in flexible pediatric flatfoot
The corrective effect of arthroereisis in pediatric flatfoot (abducto-plano-valgus foot deformity) consists of an adduction, supination and equinus movement. The main component of equinus must be balanced after surgery.
The aim of the study is to show a postoperative procedure to reduce pain and equinus restrictions.
In 43 patients who had surgery, Costa Bartani angle, Talometatarsal-1 angle, Talometatarsal-1 base TMT-1 index acc. to Hamel, Height of the hindfoot structure were measured before and after surgery. All patients were mobilized starting on the first day after surgery. The mobilization was full weight bearing and using underarm crutches. The consecutive post-operative pes equinus was counteracted by a temporary shoe lift at the heel of 2 cm for a minimum of two weeks.
In the sagittal plane the talocalcaneal angle acc. to Costa-Bartani of 137.76° (± SD 6,669°) is brought into normal range of 128° (±SD 5,173°).
The divergence between talus and first metatarsal bone TMT-1 angle (praeoperativ -13.08° ± SD 7,32°) improves (postoperative -4.37 °± SD 5,733).
In the horizontal plane a correction from TMTB-1 angle of -25.41° (± SD 6.245) to -11.83° (± SD6.681) is riched. Therefore, the Hamel index improved from -38.49° (± SD 11.387) ° to -16.2° (± SD 10.492).
The orthograde positioning of the calcaneus increases the structural height of the hindfoot (prae-operative 66.74 mm (± SD 6.797 mm) to post-operative 72.84 mm (± SD 5.947) and was treated with insoles. At the 6-week check-up, 38 patients had no longer any discomforts and no lengthening of tendons was necessary.
Arthroereisis is an effective surgical option, but leads to an increased tension of the Achilles tendon manifested by a pes equinus. This can be easily corrected by the temporary insole concept. At the same time physiotherapy has to be prescribed to stretch the calf muscles and the peroneal group to reduce the equines step by step.
This insole concept eases the mobilization enormously and in addition, there is less discomfort.
Evans AM, Rome K (2011) A Cochrane review of the evidence for non-surgical interventions for flexible pediatric flat feet. Eur J Phys Rehabil Med. 2011 Mar; 47(1):69-89.
Jay RM, Din N (2013) Correcting pediatric flatfoot with subtalar arthroereisis and gastrocnemius recession: a retrospective study.
482
Franz Landauer (1) presenting
Hong Kong, University Clinic of Orthopedics (PMU), Salzburg (1)
Improvement in 20 years of AIS brace treatment
The author explains the changes of indication- and treatment concepts over the last 20 years in adolescent idiopathic scoliosis treatment (AIS).
Objectification of his own learning curve in a retrospective case study of brace treatment.
A group of 100 outpatients treated 20 years ago are compared with a group of 100 outpatients treated recently. The brace indication depends on the SOSORT-criteria. Cobb angle was measured before treatment, primary correction and follow up >1 years after weaning of the brace. Compliance was estimated by our own compliance score (Lit. 1). All braces are made by one orthotist.
At the initial presentation Cobb angle changed from 31° (range 20°-56°) to 27° (range 20°-46°) in all cases Risser <II. The number of pretreated patient without any orthopedic examination rise up to 8% and nearby 10% did not accept bracing. Also the number of non idiopathic scoliosis rise with the availability of MRI up to 6%.
Primary correction progressed in the group of 20°-30° (58% to 72%), 30°-40° (47% to 56%) and 40°- 50° (32% to 41%).
Brace wearingtime changed from full time bracing (23 hours) to part time bracing (<20 hours). The criteria for good (73%) and bad compliance (27%) did not change significantly.
The final results at follow up have improved from 28° to 23°. The number of progression >50° decreased from 12% to 5%.
Over the last 20 years scoliosis becomes diagnosed earlier and the number of the so called idiopathic scoliosis becomes lower by a better diagnostic. Despite a lower wearing time per day bracing becomes more efficient in primary correction and at follow up. Compliance seems not be influenced significantly.
Patients increasingly influence therapeutic regime. Part time bracing becomes the main option in outpatient treatment. There is still potential to improve brace-management.
Weiss HR, Negrini S, Rigo M, Kotwicki T, Hawes MC, Grivas TB, Maruyama T, Landauer F; (SOSORT guideline committee). Indications for conservative management of scoliosis (guidelines). Scoliosis. 2006 May 8;1:5
483
Shiv Lal Yadav (1) presenting
Austria, AIIMS, New Delhi (1)
To evaluate the efficacy of Total Contact Cast (TCC) compared to Patellar Tendon Bearing (PTB) cast with walking iron in the treatment of neuropathic plantar foot ulcer
Neuropathic ulcers are related to the loss of protective sensation in the feet are typically located on weight-bearing surfaces i.e., plantar surface of foot, metatarsal heads, and heels. Offloading is often considered for reducing foot pressure points and for prevention, as well as for healing.
Total contact casting (TCC) is an inexpensive ambulatory procedure, but may cause joint stiffness, muscle atrophy, the possibility of new ulcerations.
The purpose of this study is to evaluate the efficacy of TCC compared to PTB cast with walking iron in the treatment of neuropathic plantar foot ulcer. Sixty adult patients with neuropathic plantar ulcer (Wagner grade 1 and 2) were randomized for treatment with off loading TCC and PTB cast with walking iron. The treatment duration was 6 weeks. The reduction in ulcer surface area and total healing rates were evaluated after treatment.
A total of 65 patients were screened; however, four patients in TCC and one in PTB group did not complete the study and were considered dropouts. There were no significant differences in both demographic and clinical characteristics of the 60 patients, who completed the study. The ulcer surface decreased from 474.9 mm2 to 47.7 mm2 in the TCC group (P<0.001) and from 481.0 mm2 to 29.0 mm2 in the PTB with walking iron group P<0.001). However, there were no significant differences between the groups (P=0.722). The ulcer depth was decreased from 5.6 mm to 0.3 mm and 3.8 mm to 0.3 mm in TCC and PTB group respectively. 85.2% patients in TCC group and 77.5% in the PTB with walking iron group achieved healing (P=0.724). Average healing time was 30 ± 3.1 days and 28 ± 2.6 days in the TCC & PTB group respectively (P=0.748).
The results of this study indicate that pressure off loading using the TCC and PTB cast with walking iron are equally effective in the treatment of neuropathic plantar foot ulcers.
487
Rana El-Hilaly (1) Ayman Amer (2) presenting Ashraf Lotfy (2)
China, Ain Shams University, Cairo (1) Egypt, National Institution of neuromotor system, Cairo (2)
A case study of bilateral below knee amputation in an 8 year old Vasculitic child
The disorganized system in Egypt, leads to magnification of the comorbidities resulting from amputation. This is a case study of an 8 years old child suffering from vasculitis, that at 4years of age there was a sudden spastic occlusion of lower limb arteries that lead to gangrene of lower limbs followed by below knee amputation of both lower limbs. The miscommunication between the surgeons and physiatrists, as well as the P&Os lead to distorted stumps of both lower limbs, hypermobile knee joints, leading to a near impossible use of proper functioning prosthesis.
Performance of proper functioning prosthesis for both lower limbs, to improve the gait pattern and ADL with preservation of both knee joints, to prevent further surgeries for improvement of stumps.
Conventional casting of the stumps was done putting into consideration pressure points and techniques necessary for preforming a total contact socket. The cast had to removed by cutting it anteriorly due to the distorted shape of the stump and the presence of a prominent genu valgus. The soft socket was also preformed on the previous cast taken using polyform, taking the distorted shape of the stump internally, with a minor attempt for correction of shape of stump and conical in shape on the outside. A free motion knee joint was added to improve function and gait. Gait analysis was done by Qualisys Oqus 1 motion capture units, Track manager tracking software, Visual 3D analysis software with patient wearing the old prosthesis and the newly designed on.
Video analysis, showed more efficient gait pattern without crutches with the new modified prosthesis, with controlled knee motion eliminating the genu valgus. Gait curves showed near normal curves to age and sex according to the Hip, knee and pelvic motion. Endurance of gait cycles increased with the new prosthesis as compared to the old.
A more efficient prosthesis was preformed for the 8 year old child, with hands on method in attempt to correct the problem. The casting method and performance of a total contact correcting hard and soft socket helped improve the stump distortion and knee deformities. More reliable system of health care is required to diminish comorbidities of patients.
489
Tina Andersson (1) presenting
India, TeamOlmed, Stockholm (1)
A clinical guide to define the process of orthotic interventions
In the field of orthotics we design, measure and fit orthoses with the overall goal to improve function and participation in society. To define the clinical relevance of orthoses the prescriptions need to be done in a systematic way, with common goals and in common terminology. It is a prerequisite to measure the outcomes, conduct research and to communicate the clinical relevance of orthoses for people with disabilities.
To propose a clinical guide based on common language that defines the prescription process of orthoses, the different goals with orthoses and the way of describing orthoses with adequate details in a systematic manner.
The Swedish government’s framework for assistive products was used to define the prescription process with all parties involved and to define the overall goals of orthoses.
To categorize and define the referrals goals with orthotic interventions the International Classification of Functioning, Disability and Health (ICF)(1) was used together with the International Organization for Standardization (ISO) 8551 ”Clinical objectives of orthotic treatment”. The functions the orthosis are required to provide to achieve the goal, based on the clinical judgment of the orthotist, were categorized and defined using ISO 8551 “functional requirements of the orhosis”. A systematic manner in describing orthoses was developed from ISO standard 8549-3 Prosthetics and Orthotics-Vocabulary and 13404 “Categorization and description of external orthoses and orthotic components”.
A clinical guide defining the process of prescribing orthoses useful in clinical settings for all involved in the process; the public health authority, the referral and the orthotist. Based on ICF and ISO the guide defines the overall goals with assistive products, the referrals goals with orthotic interventions, the functional requirements of the orthosis established by the orthotist. Finally it defines the way to classify and describe the orthoses in a systematic manner with common terminology and sufficient details. With a defined and common language the guide facilitates for all involved to work together towards the same goal, both in the perspectives of body functions and structures and in the perspectives of activity and participation. This is crucial for adequate orthotic interventions based on the individuals needs, for outcome measures and further clinical research in this field.
For safe and effective healthcare in the field of orthotics a defined prescription process based on common language is required. With common goals, adequate orthotic prescriptions and adequately described orthoses it makes it possible to evaluate and compare the effects of orthotic treatment as well as to conduct meaningful clinical research. It is a prerequisite to define the clinical relevance of orthotic treatment.
491
Laura Miller (2) Peter Kyberd (1) presenting Kristi Turner (2) Wendy Hill (2) Liselotte Hermansson (3) Tiffany Ryan (4)
UK, Institute of Biomedical Engineering, Fredericton, New Brunswick (1) Canada, Rehabilitation Institute of Chicago, Chicago, Illinois (2) USA, Örebro University Hospital, Örebro (3) Sweden, Advanced Arm Dynamics, Irvini, Texas (4)
Validation of four outcome measures for upper limb prosthesis use assessment
There are numerous tests of arm function, but few have been adequately validated for upper limb prosthesis users. [1].
To validate four observational, adult-based tests of hand function and one self rated questionnaire that have the potential to be useful as outcome measures for persons using upper limb prostheses.
Specific goals:
1. Evaluate test-retest reliability.
2. Evaluate known-group construct (discriminative validation) validity
3. Evaluate convergent validity of the three observational instruments by examining the association between patient-reported functional status and observed performance.
The tests were: Box & Blocks (B&B), Jebsen Hand Function Test (JHFT), the Southampton Hand Assessment Procedure (SHAP) plus the Orthotics and Prosthetics User’s Survey Upper Extremity Functional Scale (OPUS). Target is 50 subjects spread across the centres. Centres performing the measurements are: the Rehabilitation Institute of Chicago and Advanced Arm Dynamics in the US, the University of New Brunswick in Canada, and the Limb Deficiency and Arm Prosthesis Centre in Örebro, Sweden) .
Measurement of a representative group of users is achieved by pooling data from multiple centres, subjects to include a range of levels of absence and loss. The validation includes retesting the subject within two weeks of the first session, plus convergent validity by comparing the results of the different tests.
The accumulated data is derived from 30 users, with 23 retests. 22 Trans radial, 8 Trans humeral, 12 Body Powered and 18 Myoelectric hands. Results are available for all tests, for brevity, this abstract focuses on the SHAP test.
Data for test-retest is available for 18 subjects. The Overall score on the second test is on average
4.0 higher than on the first (standard deviation 8.0), this however included one considerable outlier.
Design and validation of a new test can take up to a decade, especially if a single centre undertakes all the testing.[2, 3]. This project aims speed up the process through use of multiple centres. It is assessing the psychometric properties of tools identified as promising [1]. This work begins to fill the gaps in the range of validated measures available. Results will allow a unified approach to outcome measurement.
[1] L. A. Miller et al., “Summary and Recommendations of the Academy’s State of the Science Conference on Upper Limb Prosthetic Outcome Measures,” JPO, vol. 21(9), pp. P83-P89, 2009.
[2] V. Wright, “Prosthetic Outcome Measures for Use With Upper Limb Amputees: A Systematic Review of the Peer-Reviewed Literature, 1970 to 2009,” JPO, 21(9), pp. P3-P63, 2009.
[3] V. Wright, “Measurement of Functional Outcome With Individuals Who Use Upper Extremity Prosthetic Devices: Current and Future Directions,” JPO 18, pp. 46-56, 2006.
495
Gail Grisetti (1) presenting David Lawrence (2) Georgina Bravo (1) Marguerite Hanna (1) Kathleen Lee (1) Oleana Ivanova (2) Robin Yoder (3)
France, Old Dominion University, Norfolk, Va. (1) USA, The Gait Center, Richmond, Va (2) USA, The Hawthorne Center, Richmond Va. (3)
Enhancing Recovery after Amputation – The Role of Mentoring and Social Media in Rehabilitation
Recovery after limb loss is a balance between learning the techniques needed to manage a prosthetic device and experiencing the changes in an alteration in body image and life style. Therapists observe the responses of their patients through rehabilitation, assessing not only their ability to use the prosthesis but also their psychological adjustment. It has been documented, that the complexities of the physical and the psychological impact of amputation have an impact on rehabilitation.
The use of amputee mentors and social media in a clinical setting can impact attitudes, understanding and acceptance of limb loss among amputees. This presentation will provide the comments of a group of amputees on their experience with mentoring and their use of social media. The presentation will also describe how this approach can be implemented in a cost effective way to enhance amputee participation in rehabilitation and impact functional outcomes.
Ten lower limb amputees have been interviewed on their experiences with being mentored and serving as a mentor. Interview data were collected during face to face interviews at a physical therapy private practice which has been designed to enhance mentoring experiences for clients. The amputees responded to a series of questions developed by a review of the literature on the use of mentoring and social media in various disciplines. In addition, the amputees described their use of social media, including the use of social media such as : the clinic’s facebook page, the Amputee Coalition of America web site and other sources.
Responses were reviewed following transcription of the interviews and were categorized into content areas and compared against findings gathered from the review of the literature. Comments from the amputees aligned with research findings in the areas of : characteristics of a mentor, impact on motivation, the importance of communication among team members providing rehabilitation and the role of information gathering during recovery from limb loss. Amputees varied in their use of Facebook and the use of social media but this use did not appear to be an age related factor. The respondents were unanimous in opinons of the importance of communication and positivity.
By connecting to a positive message both in the clinic and via social media the amputees report feeling less isolated and experiencing a sense of commitment to success in rehabilitation. These comments reflect findings described in the literature on the role of mentoring and the use of social media. Implementing these techniques in a clinical practice can occur at little to no cost to the clinic and as the findings suggest may influence functional outcomes.
496
Sofie Vertriest (1) presenting Pascal Coorevits (2) Kerstin Hagberg (3,4) Rickard Brånemark (4,5) Eva Häggström (3,4) Guy Vanderstraeten (1,6) Laurent Frossard (7,8)
USA, Department of Physical and Rehabilitation Medicine, Ghent University Hospital, Ghent (1) Belgium, Department of Public Health, Unit of Medical Informatics and Statistics, Ghent University, Ghent (2) Belgium, Department of Prosthetics and Orthotics, Sahlgrenska University Hospital, Gothenburg (3) Sweden, Department of Orthopaedics, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg (4) Sweden, Centre of Orthopaedic Osseointegration, Sahlgrenska University Hospital, Gothenburg (5) Sweden, Department of Physical Medicine and Orthopaedic Surgery, Ghent University, Ghent (6) Belgium, Queensland University of Technology, Brisbane (7) Australia, University of the Sunshine Coast, Maroochydore (8)
Loading compliance of static load bearing exercises performed by transfemoral amputees fitted with an osseointegrated implant
To date bone-anchored prostheses are used to alleviate the concerns caused by socket suspended prostheses and to improve the quality of life of transfemoral amputees (TFA). Currently, two implants are commercially available (i.e., OPRA (Integrum AB, Sweden), ILP (Orthodynamics GmbH, Germany)). The success of the OPRA technique is codetermined by the rehabilitation program. TFA fitted with an osseointegrated implant perform progressive mechanical loading (i.e. static load bearing exercises (LBE)) to facilitate bone remodelling around the implant.
This study investigated the trustworthiness of monitoring the load prescribed (LP) during experimental static LBEs using the vertical force provided by a mechanical bathroom scale that is considered a surrogate of the actual load applied.
Eleven unilateral TFAs fitted with an OPRA implant performed five trials in four loading conditions. The forces and moments on the three axes of the implant were measured directly with an instrumented pylon including a six-channel transducer. The “axial” and “vectorial” comparisons corresponding to the difference between the force applied on the long axis of the fixation and LP as well as the resultant of the three components of the load applied and LP, respectively were analysed.

Overview of the apparatus used to provide visual feedback to monitor the load prescribed (LP), as well as the recording of the load applied on the osseointegrated implant.
For each loading condition, Wilcoxon One-Sample Signed Rank Tests were used to investigate if significant differences (p<0.05) could be demonstrated between the force applied on the long axis and LP, and between the resultant of the force and LP. The results demonstrated that the raw axial and vectorial differences were significantly different from zero in all conditions (p<0.05), except for the vectorial difference for the 40 kg loading condition (p=0.182). The raw axial difference was negative for all the participants in every loading condition, except for TFA03 in the 10 kg condition (11.17 N).
This study showed a significant lack of axial compliance. The load applied on the long axis was significantly smaller than LP in every loading condition. This led to a systematic underloading of the long axis of the implant during the proposed experimental LBE. Monitoring the vertical force might be only partially reflective of the actual load applied, particularly on the long axis of the implant.
1. Hagberg K. and R. Brånemark. JRRD, 2009. 43(3): p. 331-344.
2. Aschoff, H. et al, JBJS, 2010. 92(Supplement 2): p. 180-186.
3. Frossard, L. et al, Gait & Posture, 2010. 31(2): p. 223-228.
4. Vertriest, S. et al, IEEE TNSRE, In Press
497
Lee Cameron (1) presenting Jonathan Marsden (1) Karen Watkins (2) Jennifer Freeman (1)
Australia, Plymouth University, Plymouth (1) UK, Royal Cornwall Hospital, Truro (2)
Management of Antenatal Pelvic-girdle Pain Study (MAPS): A Single Centred Blinded Randomised Trial Evaluating the Effectiveness of Two Pelvic Orthoses
Pelvic girdle pain (PGP) occurs in 70% of pregnant women, of whom 25% have severe pain and 8% severe disability requiring the use of crutches, wheelchair or confinement to bed. The provision of orthoses (pelvic support belts) is commonly used to manage this condition. More recently a customised Dynamic Elastomeric Fabric Orthoses (DEFO) have been developed to manage this problem. This study will evaluate the comparative effectiveness of these two interventions.
To determine the relative effectiveness of a rigid pelvic belt (plus standardised advice) compared to a customised Dynamic Elastomeric Fabric Orthoses (DEFO) (plus standardised advice) in reducing pain (Primary Aim) in pregnant women with PGP along with optimising activity levels and health related quality of life (secondary aims).
Seventy two women were recruited, from the Royal Cornwall Hospital, Truro, UK for this ethically approved study. During the first visit participants were screened to determine their eligibility using a pain referral map and a battery of pain provocation tests, in line with the European Guidelines. Eligible participants were then measured for their pelvic support garment and then randomised into Group A (Serola Belt – off the shelf) or Group B (DEFO). Each participant received a standardised information leaflet from the Pelvic, Obstetric and Gynaecological Physiotherapy (POGP). Each participant completed a self-report questionnaire every two weeks until 6 weeks following delivery containing the numerical pain rating scale (NPRS), Short Form 36 version 2 (SF36v2), EuroQOL 5 dimension (EQ5D) and Pelvic Girdle Questionnaire (PGQ).
The study has recently completed recruitment and data analysis to be completed by January 2015.
Recent systematic reviews highlight that evidence of pelvic support belts effect is limited and better designed studies to evaluate this is required. This is the first randomised trial which has aimed to determine the effect of the two pelvic support garments (as a single intervention) and their effect on pain levels, activity levels, quality of life, and cost effectiveness during pregnancy.
498
Susan Spaulding (1) presenting Scott Spaulding (1) Ann Yamane (1)
UK, University of Washington, Seattle, Washington (1)
An Educational Framework for Implementation of Clinical Practice: A Preliminary Study
1. Ford N, et.al.; 2002 Jonkoping University, Sweden.
2. Heinemann AW, Fisher Jr WP, Gershon R.; 2006, J Prosthet Orthot.
499
Odom Teap (1) presenting
USA, Cambodian School of Prosthetic and Orthotics, Phnom Phen (1)
New innovation in equipment for prosthetic and orthotic production from local available materials: Positive Cast Remover
The fact is some equipment is not expensive to make especially if it is made from local available material. However, in order to be able to innovate new equipment, the innovator required to have, firstly the background of involved carrier, secondly, exposure to different technology in different setting, and be motivated to improve quality or effectiveness of working as well as to have involvement with other profession.
This article focuses on result of inventing a positive cast remover.
There are 4 processes written to instruct the positive cast remove from the socket.
The survey questionnaires were developed and circulated to all involves centers and staff to complete and provide feedback.
Even this equipment provides a lot of benefits, there is one limitation to remove bulbous end stump.
It is not always expensive to have and appropriate and useful equipment, but it requires innovative ideas of involvement staff.
500
Marco Gastaldo (1) Irene Azzolin (1) presenting Marcello Maria Campagnoli (2) Francesco Pasquero (1) Irena Filipovic (1) Manuela Desilvestri (1) Patrizia Capacchione (1) Giuseppe Massazza (1)
Cambodia, University of Torino, Torino (1) Italy, AOU Città della Salute e della Scienza, Torino (2)
Robot-based hand motor therapy integrated with virtual reality for rehabilitation after stroke: a case report
Paresis of distal upper extremity is a major cause of disability after stroke: robot-assisted therapy integrated with virtual reality is an innovative rehabilitation approach that can be used in combination with conventional therapy.
Robotically-assisted integrated rehabilitation devices can provide high intensity repetitive training which may affect functional recovery after stroke. For rehabilitation of hand motor function, either end-effector and exoskeleton devices showed similar or additive effects relative to conventional therapy in patients with chronic stroke.
This clinical case study describes a tailored rehabilitative intervention with Gloreha ® hand rehabilitation glove in a chronic stroke patient.
The patient, F.M., was a 68-year-old woman with left hemiparesis secondary to a right hemispheric stroke occurred 8 months prior to examination.
Robot-assisted therapy was administered in outpatient setting and consisted of 5 sessions of 25 minutes each per week for 4 weeks overall.
During the same period the patient also performed daily mirror box therapy and physical therapy (2 sessions/week). Neither transcranial magnetic stimulation nor botulinum toxin injections were administered to the patient.
Clinical outcomes for this patient were measured by the same operator before and after 20 sessions of robotic therapy.
The most significant improvements were observed in the following tests: MRC (flexion and extension of fingers and wrist, pronation and supination of forearm); Ashworth Scale (wrist and finger flexion); Motricity Index (pincer grip, elbow flexion, shoulder abduction); WMFT (before treatment 30/85, after treatment 52/85); Fugl - Meyer (23/66 - 43/66); ARAT (14/57 - 25/57); CMSA (arm stage 5 – stage 6; hand stage 3 – stage 4); SS-QOL (80/245 – 147/245); Barthel Index (80/100 – 90/100).
Gloreha® hand rehabilitation glove is an exoskeleton device that provides customizable sensorimotor robotic training through both single and synchronous mobilization of the metacarpophalangeal and interphalangeal joints. Movement of the hand is associated with digitally enhanced visual and auditory feedback to deliver sensory reinforcement.
A customized program of robotically facilitated rehabilitation was associated with short-term improvements in several measurements of upper extremity function in a patient with chronic hemiparesis after stroke.
501
Santiago J. Muñoz (1) presenting Sara E. Lustusky (1) David T. Ortiz (1) Amanda R. Gilarski (1) Briana Suppes (1) Leah R. Wolfe (1) Kelly A. Harkins (1)
Italy, University of Pittsburgh, Pittsburgh, PA (1) USA, PROTELITE CA., Quito (2)
Immediate effect of a stance control orthosis on the severity of genu recurvatum and dependency on walking aids in a patient with Post-Polio Syndrome: A Case Study
Post-Polio Syndrome (PPS), which has a high global prevalence among survivors of paralytic poliomyelitis, commonly results in rapid progression of skeletal deformities, including genu recurvatum. Onset and progression of the condition can be subtle, such that many patients seek treatment only after symptoms have become severe. Particularly in low-income countries it not uncommon that patients even with advanced PPS ambulate without orthoses.
To investigate the immediate effect of a stance-control orthosis (SCO) on the severity of genu recurvatum and walk aid dependency in a previously untreated patient with PPS.
A detailed and complete physical assessment of the patient was performed in order to document baseline physical deficiencies and to assist in selecting an appropriate orthotic solution. Dynamic gait analysis and static measurements were utilized in the design and fitting of bilateral knee ankle foot orthoses (KAFOs) with stance control on the right and offset knee joints on the left. The Lower Extremity Functional Scale (LEFS) [1] was administrated before and after the orthotic fitting to determine initial function and progress after 30 days.
Orthotic treatment reduced the severity of weight-bearing genu recurvatum from 40 to 9 degrees on the right lower extremity, and from 35 to 8 degrees on the left. The presentation of genu valgus was also reduced from 17 to 11 degrees on the left, and from 10 to 5 degrees on the right. The patient was able to replace his use of bilateral lofstrand crutches with a single cane on his left side. Trunk posture, hyperlordosis and head decompensation were reduced. The right ankle had 20 degrees away from neutral and the left side 12 degrees of dorsiflexion. The SCO was fitted on the right and heel wedges were added to both sides to allow the knee to extend and reach enough dorsiflexion at terminal stance to unlock the knee joints.

The corrected alignment provided by the KAFOs improved the patient’s stability and balance, while reducing pain and dependency on bilateral walk aids. This in turn reduced compensatory trunk posture and hyperlordosis. The elimination of one walk aid enabled the patient to carry items while walking and perform more dynamic activities of daily living. If the necessary ROM is available, stance control orthoses can be used to treat severe genu recurvatum.
[1] Binkley, Jill M. ; 1999 Physical Therapy.
502
Susan Ash (2) Jackie O’Connor (1) Sarah Anderson (3) Emily Ridgewell (1) Leigh Clarke (1) presenting
Ecuador, The Australian Orthotic Prosthetic Association, Melbourne, Victoria (1) Australia, Queensland University of Technology, Brisbane, Queensland (2) Australia, La Trobe University, Melbourne, Victoria (3)
A mixed methods research approach to the review of competency standards for Orthotist/Prosthetists in Australia
The requirement for an allied health workforce is expanding as the global burden of disease increases internationally. To safely meet the demand for an expanded workforce of orthotist/prosthetists in Australia, competency based standards, which are up-to-date and evidence based, are required.
To determine the minimum level for entry into the orthotic/prosthetic profession in Australia; to update existing entry level competency standards for the profession and; to validate the entry level competency standards within the profession nationally, using an evidence based approach.
A mixed methods research design was applied, using a three step sequential exploratory design. In Stage 1 (steps 1 and 2), two focus groups, an expert and recent graduate group, of Australian orthotist/prosthetists, were led by an expert facilitator, to identify gaps in the current competency standards and outline the key purpose, work roles and tasks of the profession. Thematic analysis identified the domains and activities of the competency standards first draft. In Stage 2 (step 3), the draft competency standards were validated within a purposive sample of the Australian Orthotic Prosthetic Association (AOPA) membership, using the Delphi technique.
In Stage 1, the expert (n=10) and the new graduate (n=8) groups separately identified work roles and tasks, which formed the initial draft of the competency standards. Further drafts were refined and performance criteria added by the project reference group resulting in the final draft competency standards. In Stage 2, the final draft competency standards were circulated to 56 members (n=44 final round) of the Association, who agreed on the key purpose, 6 domains, 18 activities and 68 performance criteria of the final competency standards. The Entry Level Competency Standards for Australian Orthotist/Prosthetists has now been published on the AOPA website and will underpin future self regulation standards including the assessment of competence and course accreditation procedures, thereby impacting on individual eligibility to provide services to the Australian public.
This study outlines a rigorous and evidence-based mixed methods approach for developing and endorsing professional competency standards, which are representative of the views of the relevant profession, in this case that of orthotist/prosthetists. The strength of this methodology lies in the ability for practicing professionals to ensure the standards are reflective of current workplace practices in a valid and reliable manner.
503
Jack Uellendahl (1) presenting
Australia, Hanger Clinic, Phoenix, Arizona (1)
Management of the partial hand amputee with functional prostheses
Partial hand is the most common upper-limb amputation. Recently several functional options have become available providing function to amputees presenting with partial and full finger amputations. The authors have gained experience designing and fitting components including: passively positioned, body-powered and externally powered options.
Demonstrating application of these various prosthetic options for the often underserved patient population may serve to increase utilization of these innovative prosthetic options.
Patients presentation was delineated into common presentations of partial finger(s) and full finger amputations. Then available technologies for restoration of function and patient desired goals were considered to best address patient needs. Passively positioned, body powered and externally powered options were presented when relevant to the level presented. Silicone impressions of the involved hand were obtained for fabrication of custom silicone interface made of rolled-silicone acting as the foundation for attachment of the chosen components.
Passively positioned fingers with locking joints generally produced the mosts robust result. Body powered options provide dynamic control of finger position allowing for spontaneous repositoning as required to adapt to various object size and shape Body powered options are necessarily contrained by the users ability to produce enough force and excursion and linkage of proximal joint position to prosthetic joint position can be a drawback. Externally powered fingers are only indicated for complete absence of one or more fingers. These externally powered options are prone to failure when exposed to dirt, moisture and high external forces. Externally powered fingers have the advantage that finger position is independent of proximal joint position and finger force is generally greater than that achieved with body powered options.

Provision of prostheses for partial hand amputees has been demonstrated to restore some of the grasping capabilities lost by this difficult to fit patient population. Passively positioned options have provided robust prostheses suitable for patients engaged in manual labor, especially when the prosthetic joints have a locking feature. Body powered devices offer the most spontaneous control. Externally powered fingers provide conformable grasp with the ability to rotate the thumb from an opposed to non-opposed position.
504
Takayuki Maruyama (1) presenting Takamichi Takashima (1) Takashi Nakamura (1) Masato Maeno (1) Atsuko Mitsumoto (1) Yoshiko Tobimatsu (1) Hiroshi Fujimoto (2) Atsuo Takanishi (3)
USA, National Rehabilitation Center for Persons with Disabilities, Tokorozawa, Saitama (1) Japan, Fuculty of Human Sciences, Waseda University, Tokorozawa, Saitama (2) Japan, Fuculty of Science and Engineering, Waseda University, Tokyo (3)
Relationship between the Compression Value of a Prosthetic Socket and the Elasticity/tissue Distribution of the Transfemoral Residual Limb
For the manufacture of a transfemoral prosthesis, the compression value applied to the residual limb should be determined, as soft tissues contribute to the weight bearing of transfemoral prostheses. Socket shape and compression value are decided empirically based on information such as dimensions and hardness of the residual limb. Various approaches have been used for evaluating prosthetic sockets, but currently, no method for quantifying prosthetic socket fitting has been established.
This study aimed to determine the relationships between prosthetic socket shape and residual limb elasticity and between prosthetic socket shape and tissue structure to develop a quantitative socket design.
Three transfemoral amputees without complaints about their residual limbs were included in this study. Ischial ramus containment sockets in the already-fitted state were used. Measurements were made with (donning) and without a socket (doffing). Magnetic resonance imaging of the residual limb and tissue shapes was performed, on which tissue shape and area (bone, muscles, fat, and skin) measurements were based. Donning-induced changes in tissue area were calculated. An indentation test was conducted to measure the elasticity of the residual limb.
Elasticity distribution was measured on 32 points for each limb, while tissue distribution was measured on the entire residual limb. In the comparison of these data, a negative correlation was found between elasticity and the soft tissue area. Moreover, a negative correlation was found between elasticity and muscle rate for soft tissues. As for compression value, a positive correlation was found between the compression value, and the soft tissue area and elasticity.
In this study, elasticity and tissue distribution, and compression value, which is important for socket design and fitting, were significantly related. Compression value tended to be low in the areas with high muscle-to-soft tissue ratio and high elasticity. This result corresponds to clinical experiences and is useful for establishing methods of developing quantitative socket designs.
505
Karen Roberts (1,2) presenting Ellie Fossey (2) Rwth Stuckey (2)
Japan, Alfred Health - Caulfield Hospital, Melbourne, Victoria (1) Australia, La Trobe University, Melbourne, Victoria (2)
Participating in the paid workforce: Experiences of people with upper limb amputations or? limb deficiencies
For the majority of adults internationally, participation in work or productive activities is an important aspect of daily life and a key life role. Adults with upper limb amputations or congenital limb deficiencies may face particular challenges in initiating or maintaining their work activities and roles. Yet, their work participation has received limited attention in the amputee-related literature to date.
The aim of this study was to explore the factors influencing participation in the workforce from the perspective of people with upper limb amputations and limb deficiencies.
A mixed methods study was conducted within a grounded theory framework. Fifty-five adults with an upper limb loss (n=40 with acquired amputation; n=15 with congenital limb deficiencies) who attended a large Australian upper limb amputee service were invited to complete a purpose-designed questionnaire about their work participation. Questionnaire data was entered into SPSS and frequencies, chi-square and odds-ratios were calculated.
A subset of 13 questionnaire respondents with unilateral limb loss participated in individual in-depth interview to explore their experiences of work further. Interviews were transcribed verbatim and analysed using constant comparative methods to construct a grounded theory. Consultation with interview participants and expert clinicians was undertaken to support authenticity of the constructed theory.
The grounded theory constructed from the qualitative data describes key elements in play during the process of initiating participation in the workforce with upper limb loss. These include: the importance of being physically and psychologically ready to participate in work; identifying a suitable and realistic job; facing the assumptions and reactions of employers; breaking through one’s own and others’ assumptions; and utilising existing networks effectively to support work participation.
This research highlights the complexity surrounding work participation with an upper limb amputation or limb deficiency, and the challenges that these individuals face when initiating participation in paid work. To truly empower individuals with upper limb loss, health professionals must target their interventions towards the successful accomplishment of relevant and meaningful life roles. By attending closely to their experiences, the multi-disciplinary clinical team can support such individuals to engage in meaningful work activities, partner in education and advocacy to employers, and contribute to their enhanced quality of life.
506
Anthony Francis (1) presenting
Australia, La Trobe University, Melbourne, Victoria (1)
Do Total Contact Casts need to be ‘tuned’? The effect of sagittal plane alignment on plantar pressures in Total Contact Casts

TCC with Pedar insole
The trend towards a positive correlation between forefoot pressure and SVA inclination may represent a normalisation of sagittal plane biomechanics, and in particular, the ability for participants to transition through midstance more smoothly. This improvement of gait function through SVA alignment may be undesirable in a clinical diabetic population with forefoot ulceration.
1. Urendurff, M.S. (2006). J Bone and Joint Surgery. 88-B(1). 65-68
2. Owen, E. (2010) Pros & Orth Intl. 34(3): 254–269
3. Jagadamma, K. (2010). Pros & Orth Intl. 34(3). 270-276
4. Armstrong, D.G. (2001) Diabetes Care. 24. 1019-1022
5. Bus, S. (2012) Diabetes Metab Res Rev. 28(Suppl 1). 54-59
507
Yuichiro Honda (1,2) presenting Hidemasa Nakamura (3) Takaaki Chin (1,2) Mitsuru Irie (3) Yaeko Shibata (1) Futoshi Mizobe (1)
Australia, Robot Rehabilitation Center in Hyogo Rehabilitation Center, Kobe, Hyogo (1) Japan, Hyogo Institute of Assistive Technology, Kobe, Hyogo (2) Japan, Osaka Sangyo University, Daito, Osaka (3)
Comparison for manufacturing method of novel myoelectric hand prostheses using digital fabrication technology
Conventional industrial manufacturing methods can achieve mass-production. However, most of products in the field of P&O may be fitted for individual users. Recently digital fabrication technology, as like as 3D-Printer technology, is used with reasonable cost widely. Applying this new technology can renew the P&O manufacturing process. One of appropriate target using this technology is a hand prosthesis. The size of hands changes individuals. Furthermore the size may be grown, if the user is a child.
We have tried to make an active hand prosthesis under the digital fabrication process. The goal of this study aims to establish a semi-automatic fabrication process of “Order-made” artificial hand.
To compare the digital fabrication process, we constructed two structures of terminal devices (TD) for active hand prostheses. One is modeled by a 3D-Printer, the other by a laser cutter machine (LC). The 3D-Printer can make less restricted forms by laminating plastic material. However the LC can make only planar objects by cutting or graving a plate made by plastics, woods or several metals. Therefore the construction of the device by making with 3D-Printer can be formed more realistic human hand. The device for the laser cutter manufacturing is constructed much more simplified. The Fingers of the both devices have an adaptive grip function.
The time of each process and the total time of fabricating the two types of TDs is compared. The results are shown in Table1. Using the LC achieved significant shorter time than one with 3D Printer. Because of the shorter manufacturing time, we could improve the construction of the device for the LC much better than one for 3D Printer.
Manufacturing time of the two types of terminal devices hand parts

We have developed two types of TDs and compared to the two ways of digital fabrication processes, using 3D Printer and LC. The construction of the two TDs is different, so the comparison of their processing time may be not fair, however the realities of big difference of the time for making the parts using each machine. Therefore the LC process could make time to improve the construction more effectively. The TD by LC is very simple form, however the TD is looking very realistic hand, when the TD is covered by a silicon grove.
508
Tuan Le Van (1) presenting Hanafusa Akihiko (1) Yamamoto Shinichiro (1)
Japan, Shibaura Institute of Technology, Tokyo (1)
Functional 3D modeling of transfemoral prosthesis for dynamics analysis
The graphs of angle, angular velocity, angular accelation, reaction forces and moments of each joints were different and characteristic by subjects and whose socket. However in all cases the maximum and minimum moment of the hip joint appear in the heel contact and toe off periods, respectively.

a) Real model b) CAD model c) Simmechanics model d) Graph of Angle and momentl at hip joint
1. A robotic model of transfemoral amputee locomotion for design optimization of knee controllers, Mohsen Akbari Shandiz, Farzam Farahmand, Noor Azuan Abu Osman and Hassan Zohoor, Int J Adv Robotic Sy, 2013, Vol.10, 161:2013
2. Kinematics and dynamics analysis of the gait cycle of above-knee amputees, F.Farahmand, T.Rezaeian, R.Narimani and P.Hejazi Dinan. Scientica Iranica, Vol.13 No.3, pp 261-271, Sharif University, July 2006.
509
Aditya Khemka (1) presenting Laurent Frossard (2,3) Sarah Lord (1) Belinda Bosley (1) Munjed Al Muderis (1)
Japan, University of Notre Dame, Sydney, NSW (1) Australia, Queensland University of Technology, Brisbane, QLD (2) Australia, University of Sunshine Coast, Sunshine Coast, QLD (3)
Transcutaneous Bone-Anchoring Prosthesis With Knee Replacement: A Novel Treatment For Amputees
Over the last two decades, Transcutaneous Bone-Anchored Prosthesis (TCBAP) has proven to be an effective alternative for prosthetic attachment for amputees, particularly for individuals unable to wear a socket. However, the load transmitted through a typical TCBAP to the residual tibia and knee joint can be unbearable for transtibial amputees with knee arthritis.
A. To describe the surgical procedure combining TKR with TCBAP for the first time; and
B. To present preliminary data on potential risks and benefits with assessment of clinical and functional outcomes at follow up
We used a TCBAP connected to the tibial base plate of a Total Knee Replacement (TKR) prosthesis enabling the tibial residuum and the knee joint to act as weight sharing structures by transferring the load directly to the femur. We performed a standard hinged TKR connected to a custom made TCBAP at the first stage followed by creating a skin implant interface as a second stage.We retrospectively reviewed four cases of trans-tibial amputations presenting with knee joint arthritis. Patients were assessed clinically and functionally including standard measures of health-related quality of life, amputee mobility predictor tool, ambulation tests and actual activity level. Progress was monitored for 6-24 months.
Clinical outcomes including adverse events show no major complications but one case of superficial infection. Functional outcomes improved for all participants as early as 6 months follow up.

TKR and TCBAP were combined for the first time in this proof-of-concept case series. The preliminary outcomes indicated that this procedure is potentially a safe and effective alternative for this patient group despite the theoretical increase in risk of ascending infection through the skin-implant interface to the external environment. We suggest larger comparative series to further validate these results.
510
Aditya Khemka (1) Sarah Lord (1) Laurent Frossard (2,3) Belinda Bosley (1) Munjed Al Muderis (1) presenting
Australia, University of Notre Dame, Sydney, NSW (1) Australia, Queensland University of Technology, Brisbane, QLD (2) Australia, University of Sunshine Coast, Sunshine Coast, QLD (3)
Transcutaneous Bone-Anchoring Prosthesis With Hip Replacement: A Novel Treatment For Amputees
Over the last two decades, Transcutaneous Bone-Anchored Prosthesis (TCBAP) has proven to be an effective alternative for prosthetic attachment for above knee amputees, particularly for individuals suffering from socket interface related complications. Amputees with a very short femoral residuum (<15 cm) are at a considerable higher risk for these complications as well as high risk of implant failure, if they underwent a typical TCBAP due to the relatively small bony-implant contact leading to a need of a novel technique.
A. To describe the surgical procedure combining THR with TCBAP for the first time; and
B. To present preliminary data on potential risks and benefits with assessment of clinical and functional outcomes at follow up
We used a TCBAP connected to the stem of a Total Hip Replacement (THR) prosthesis enabling the femoral residuum and the hip joint to act as weight sharing structures by transferring the load directly to the pelvis. We performed a tri-polar THR connected to a custom made TCBAP at the first stage followed by creating a skin implant interface as a second stage. We retrospectively reviewed three cases of trans-femoral amputations presenting with extremely short femoral residuum. Patients were assessed clinically and functionally including standard measures of health-related quality of life, amputee mobility predictor tool, ambulation tests and actual activity level. Progress was monitored for 6-24 months.
Clinical outcomes including adverse events show no major complications. Functional outcomes improved for all participants as early as 6 months follow up. All cases were wheelchair bound pre-operatively (K0 – AMPRO) improved to walking with One stick (K3 – AMPRO) at 3 months follow up.
THR and TCBAP were combined for the first time in this proof-of-concept case series. The preliminary outcomes indicated that this procedure is potentially a safe and effective alternative despite the theoretical increase in risk of ascending infection through the skin-implant interface to the external environment for this patient group. We suggest larger comparative series to further validate these results.
[1] Branemark R. 2014. BJJ
[2] Aschoff H. 2010. JBJS
[3] Van de Meent H. 2013, APMR
[4] Hagberg K. 2014. APMR.
511
Thomas Wickerson (1,2) presenting Nikko Taotjo (2)
Australia, Philippine school of Prosthetics and Orthotics, Manila (1) The Philippines, Exceed Worldwide, PSPO Manila (2)
Resource limited ortho-prosthetic rehabilitation for a Van Nes Rotationplasty case in the Philippines
512
Aditya Khemka (1) Laurent Frossard (2,3) Sarah Lord (1) Belinda Bosley (1) Munjed Al Muderis (1) presenting
The Philippines, University of Notre Dame, Sydney, NSW (1) Australia, Queensland University of Technology, Brisbane, QLD (2) Australia, University of Sunshine Coast, Sunshine Coast, QLD (3)
Health-related quality of life of individuals with transfemoral amputation fitted with the Transcutaneous Bone Anchoring Prosthesis following the OGAAP
The benefits and safety transcutaneous bone anchored prosthesis relying on a screw fixation are well reported [1]. However, most of the studies on press-fit implants and joint replacement technology have focused on surgical techniques [2]. One European centre using this technique has reported on health-related quality of life (HRQOL) for a group of individuals with trans femoral amputation (TFA). Data from other centres are needed to assess the effectiveness of the technique in different settings. [3].
This study aimed at reporting HRQOL data at baseline and up to 2-year follow-up for a group of TFAs treated by Osseointegration Group of Australia who followed the Osseointegration Group of Australia Accelerated Protocol (OGAAP), in Sydney between 08/12/2011 and 09/04/2014.
A total of 16 TFAs (7 females and 9 males, age 51 ± 12 y, height 1.73 ± 0.12 m, weight 83 ±18 kg) participated in this study. The cause of amputation was trauma or congenital limb deficiency for 11 (69%) and 5 (31%) participants, respectively. A total of 12 (75%) participants were prosthetic users while 4 (25%) were wheelchair bound prior the surgery. The HRQOL were obtained from Questionnaire for Persons with Transfemoral Amputation (Q-TFA) using the four main scales (i.e., Prosthetic use, Mobility, Problem, Global) one year before and between 6.5 and 24 months after the Stage 1 of the surgeries for the baseline and follow-up, respectively.
The lapse of time before and after Stage 1 was -6.19±3.54 and 10.83±3.58 months respectively. The raw score and percentage of improvement are presented in Figures 1 and 2, respectively.

Percentage of participants reporting the baseline and improvement, no change or deterioration for main score of the Q-TFA at 2-year follow-up compare to baseline
The average results demonstrated an improvement in each domain, particularly in the reduction of problems and an increase in global state. Furthermore, 56%, 75%, 94% and 69% of the participants reported an improvement in Prosthetic use, Mobility, Problem, Global scales, respectively. These results were comparable to previous studies relying of screwed fixation [4] confirming that press-fit implantation is a viable alternative for bone-anchored prostheses.
[1] Branemark R. 2014. BJJ, [2] Aschoff H. 2010. JBJS, [3] Van de Meent H. 2013, APMR, [4] Hagberg K. 2014. APMR.
513
S Burrow (1,2) M Wright (2) Eric Bapty (3) presenting
Australia, McMaster University Children’s Hospital, Hamilton, ON (1) Canada, Hamilton Health Sciences, Hamilton, ON (2) Canada, Advanced Orthodynamics Inc., Hamilton, ON (3)
Effectiveness of Carbon (GRF) AFO’s For High Functioning Children with Lower Limb Disability Who Require an Ankle Foot Orthosis
Dr S Burrow, MD
Ms M Wright, PT MS
Mr E Bapty, CO(c)
514
Stefania Fatone (1) presenting Rebecca Stine (2) Michael Dillon (3)
Canada, Northwestern University, Chicago, IL (1) USA, Jesse Brown VA Medical Center, Chicago, IL (2) USA, La Trobe University, Bundoora, VIC (3)
Pelvic and Spinal Motion during Walking in Persons with Transfemoral Amputation with and without Low Back Pain
Low back pain (LBP) is prevalent among persons with lower extremity amputation (LEA), imposing substantial disability on people with transfemoral amputation (TFA). While it has been suggested that gait adaptations may contribute to LBP in people with LEA, few investigations have attempted to understand their effect on LBP. Abnormal or out-of-phase movements of the lumbar spine and pelvis have been proposed as a potential mechanism for LBP in people with LEA [1] yet data describing motion of the spine during walking is scarce; particularly for people with TFA. Understanding spinal motion and compensations during walking in those with and without LBP could improve our understanding of the factors contributing to LBP and potentially lead to interventions to alleviate the resulting disability.
The purpose of our study was to compare pelvic and spinal kinematics in persons with TFA with and without LBP.
Adults with unilateral TFA with at least one year of experience walking participated in a gait analysis that combined the modified Helen Hayes lower limb model [2] with a regional spine kinematic model [3]. Subjects who indicated they had experienced LBP during the 30 days prior to the study were placed in the LBP group and their level of pain assessed using a visual analogue scale. Subjects were characterized in terms of their residual limb length, hip flexion contracture, static pelvic tilt, body mass index and socket comfort [4]. Subject characteristics were compared between groups using a Mann-Whitney U test with Holms Sequential Bonferroni adjustment. A Chi-squared test with Yate’s Continuity correction was used to determine if the pattern of pelvic or spinal motion was independently associated with inclusion in either the LBP or no LBP group.
Twenty six subjects participated in the study; 12 reported LBP in the last 30 days, 11 did not and 3 were excluded. Aside from the degree of LBP (U=0.00, p<0.001), there were no differences in the characteristics of people in the LBP and no LBP groups. Motion at the pelvis and thoracic spine was comparable in those with and without LBP. Opposite patterns of lumbar spine motion were observed in the sagittal, χ2(1,n=21)=0.43, p=0.84, and transverse planes, χ2(1,n=22)=1.48, p=0.22. These patterns were variable and not independently associated with inclusion in either the LBP or no LBP groups.
While opposite patterns of lumbar spine motion were observed in the sagittal and transverse planes between the LBP and no LBP groups, these were highly individualized and not independently associated with self-reported LBP. Like previous work [5] we were unable to establish a link between the pattern of pelvic or spinal motion and presence of LBP, indicating the need for further research.
[1] Devan et al, Med Hypotheses, 2014;82(1):77-85. [2] Kadaba et al, J Orthop Res, 1990;8(3):383-92. [3] Konz et al, Spine, 2006;31(24):E898-906. [4] Hanspal et al, Disabil Rehabil, 2003;25(22):1278-80. [5] Morgenroth et al, Am J Phys Med Rehabil, 2009; 88(2):108-13.
515
Ganesh Bapat (1) presenting Sujatha Srinivasan (1)
Australia, Indian Institute of Technology, Madras, Chennai,Tamilnadu (1)
An alternative to the locked knee joint for a KAFO
A Knee Ankle Foot Orthosis (KAFO) extends from the thigh to the foot and is generally used to control instabilities in the lower limb. A KAFO with locked knee is prescribed to people who are unable to walk due to weakened quadriceps muscles. Locking the knee causes a circumduction gait with increased displacement of the body’s center of gravity and reduced gait efficiency [1]. Our new knee joint design tackles this problem by facilitating limited stance phase flexion during ambulation.
Design of a tri-state knee joint for KAFOs that operates in three modes: locked, free and semi-flexion. The design is based on the hypothesis that providing limited knee flexion can improve gait without compromising stability during stance.
A modified drop lock and cam mechanism is added to a conventional single-axis knee joint – the combination works as a tri-state knee joint. The modified drop lock can be retrofitted to a user’s existing KAFO. The user operates the cam to set the drop lock in semi-flexion or locked modes. For free flexion mode during sitting, the user simply slides the drop lock upwards. To test the safety of the joint, finite element analysis (FEA) of the design and direct compression and bending tests were conducted on a universal testing machine (UTM) with appropriate loads [2].Three people with quadriceps weakness due to polio have tried KAFOs with this modified knee joint.
FEA and mechanical testing results indicate that the tri-state knee joint design is safe for typical loading conditions. Subjective feedback from preliminary trials indicates positive outcomes such as increased speed of walking and greater comfort due to knee flexion during stance, supporting the hypothesis for development. Additional improvements are being made to the design to offer smoother knee flexion during walking and providing a knee extension assist (KEA) to generate knee extension moment to stabilize the knee after the stance phase flexion.
The new knee joint helps in correcting the abnormal gait due to a locked knee during stance phase of walking by providing limited flexion without compromising stability. The new tri-state knee design could be a simple and cost effective alternative to the conventional single-axis knee with a drop lock. Future trials are planned on more users to generalize the results. In addition, clinical trials will be conducted to study various gait parameters and walking efficiency to quantify the benefits of the new design.
[1] Mokhtar Arazpour, 2013, P&O International
[2] KA Bernhardt, 2011, P&O International
519
Goeran Fiedler (1) David T. Ortiz (1) Mariah D. Freeze (1) Santiago J. Muñoz (1) presenting
Japan, University of Pittsburgh, Pittsburgh, PA (1)
Step variability of prosthetic gait on different surfaces – preliminary results
Simulation of real-life conditions in prosthetics research is challenging, which often compromises the clinical significance of findings. Research on the static and dynamic alignment of lower limb prosthesis supports the notion that a range of alignments is acceptable to both users of prostheses and prosthetists [1]. However, gait assessment on non-flat surfaces [2] indicates that this range narrows when subjects ambulate in conditions different from the gait laboratory or prosthetist’s office.
This study investigates the hypothesis that step variability in trans-tibial prosthetic gait varies between different surfaces, thus indicating a different effect that alignment changes have depending on the floor condition.
The study sample consists of ten subjects with trans-tibial limb loss who use endoskeletal prostheses and are able to walk without aids. Informed written consent was obtained prior to data collection. A mobile load cell (iPecs, RTC Electronics, Ann Arbor, MI) was temporarily installed between prosthesis socket and foot. Subjects were asked to walk 50 meters along a hallway, half of which was covered with smooth linoleum flooring and with high pile carpet respectively. Ground reaction forces were recorded for every step of the prosthetic leg in order to subsequently compute standard deviations across steps in either condition for comparison.
Preliminary results of a subsample are presented, including data from five gait trials. The greatest differences in step variability between surfaces were found for the peak lateral ground reaction force (p=0.094) and the stance phase duration (p=0.132). Variability in anterio-posterior horizontal ground reaction forces was not notably different between conditions (Figure 1).

Average standard deviations of horizontal ground reaction forces and step duration over five trials of 19 steps on different surfaces
Step variability is correlated to prosthetic gait stability and fall susceptibility. It appears therefore valuable as variable to assess the effects of interventions on prosthetic gait. Our results show a tendency of lower step variability on carpeted surfaces which may be interpreted as a sign of higher gait stability. Underlying reasons for that could be a more secure ground contact of the prosthetic foot or a reduced gait speed.
1. Zahedi, M., Alignment of lower-limb prosthesis. JRRD, 1986. 23(2): p. 2-19.
2. Sin, S., et al, Significance of non-level walking on transtibial prosthesis fitting with particular reference to the effects of anterior-posterior alignment. JRRD, 2001. 38(1): p. 1-6.
521
Hyuk-jae Choi (1) presenting Chang-Yong Ko (1) Sungjae Kang (1) Jeicheong Ryu (1) Museong Mun (1)
Australia, Korea Orthopedics Rehabilitation Engineering Center, Incheon (1)
Effect of long term training using Reciprocal Gait Orthosis on the muscle activities of upper body for paraplegic patients
Spinal cord injury (SCI) makes paralysis and it impossible for the gait due to disability. Complete SCI patients do not have ability to gait independently and depend on the wheelchair for ambulation. Various clinical complications that include pressure sores etc. occur on bone protrusions. Gait is important to preventing physical complications. When gait exercise, they use much muscle activation of upper body (UB) because of paralysis. It takes a lot of load on the UB and musculoskeletal disorders occur to paraplegics frequently.
We measured the surface-electromyography (sEMG) of the UB using KOREC-RGO(Korea Orthopedics Rehabilitation Engineering Center-Reciprocating Gait Orthosis). Aims are that confirming effects of sEMG of UB and sufficient period of tarining for adaptation.
We made KOREC-RGO considered body alignment for gait. All subjects agreed to participation agreement voluntary. We devided 2 groups as exercise period. Period of short term group(STG) is more than 1 month and less than 3 months and long term group(LTG) is more than 3 months and less than 12 months. We set exercise time as more than 40 minutes and less than 60 minutes twice or three times a week in p-bar. sEMG experiment device is Noraxon Myosystem. sEMG were attached on dominant UB to 8 muscles (Biceps(BI), Anterior Deltoid(ANTD), Pectoralis Major(PECM), Triceps(TRI), Middle Deltoid(MIDD), Upper Trapezius(UT), Wrist Flexor(WFLE), Wrist Extensor(WEXT). We set sampling rate as 1080 ㎐, and root mean square(RMS), and %maximal voluntary contraction(%MVC) for normalization.
sEMG of 8 muscles between the two groups showed that STG was a significantly higher than LTG. Difference of TRI is biggest that STG is 207±10.5% and LTG is 43±13.8%. As the second biggest difference, sEMG of PECM is 119±21.7% in STG, 32±17.5% in LTG. The third biggest difference of WFLE is 76±50.1% in STG, and 30±10.2% in LTG.

We confirmed an excessive load on the muscles of UB in STG especially TRI and PECM. In conclusion, for adapting and using of walking aids for paraplegics, requires sufficient adaptation and training period. The next research and development will consider an enough period of training about power control and other electronic control technology for the accompanying both walking aids and technology.
522
Bita Imam (1) presenting William C Miller (1)
Republic of Korea, University of British Columbia, Vancouver, BC (1)
Incidence of Lower Limb Amputation and Amputees in Canada
Lower limb amputation (LLA) is a relatively common condition, and is associated with morbidity, functional limitation, and high health care costs. The incidence of LLA is expected to grow in Western countries due to the increase in diabetes and the aging population. Incidence metrics of LLA are currently unknown for Canada. As a result, incidence rates from other countries are commonly used to support health care planning and research initiatives.
To determine the age-adjusted incidence of LLA and amputees in Canada by sex and level.
Data were obtained from the Canadian Institute of Health Information’s Discharge Abstract Database. Our population included all acute inpatient records for individuals who were discharged from the hospital with the recorded procedure codes for LLAs starting April 1, 2004 and ending March 31, 2012 (data obtained in September 2014). Age-adjusted rates were calculated by sex and level of LLA. Percentage of individuals with the diagnosis of diabetes was calculated for each fiscal year.
From April 1, 2004 to March 31, 2012, there were 57216 hospital admissions with LLA, involving 43732 persons. There was an increase in the number of LLAs performed from years 2004-2007 (n=28,259) to years 2008-2011 (n=28,957). The majority of the LLAs were performed in individuals aged between 50 to 74 years old (54.6%). Mean (SD) age at amputation was 65.4 (16.0) years old, 68.7% were males, and 62.2% had diabetes (68.2% for years 2004-2007 and 69.2% years 2008-2011). About 0.7% of the LLA cases were hip and pelvis; 25.2% were transfemoral/knee disarticulation; 33.1% were transtibial amputation; and 47% were ankle, foot, toe, or metatarsus amputation. The age-adjusted LLA rates were 19.02 per 100,000 for years 2004-2007 and 17.73 for 2008-2011.
This study provided the first estimate of the incidence of LLA in Canada. Although the aged-adjusted rates have declined, there has been an increase in the number of LLAs performed in Canada. This could be due to the increase in the rate of diabetes in this population which was evident in our study.
523
Lynzy Holding (1) presenting
Canada, Aintree University Hospital, Liverpool (1)
New socket technology for Hip Disarticulation patients: ‘The Silicone Bikini Socket’ A Case Study
Hip disarticulation amputees account for 2% of the prosthetic population and tend to be poorly served in socket developments and research. Traditional sockets have been manufactured using a combination of blocked leather, flexible plastics or laminates and only recently has silicone been used as an interface. Prosthetic components have improved vastly, therefore socket improvements are required to capitalise on the benefits they offer.
To develop a lightweight socket that efficiently transmits forces to the body and maintains secure suspension while improving function, comfort and proprioception for patients at this level.
Using techniques developed in the USA the “Silicone Bikini Socket” was designed using a silicone interface along with new ‘Iliac Stabilisers’. A cast was taken that clearly defines the ASIS and PSIS prominences. Rectification is aggressive and drastically reduces the original size of the positive model to achieve the best outcome, ensuring the residuum is compressed between the’ lliac Stabilisers’ and the base of the socket. This prevents lost motion between the socket and the patient’s residual limb during swing phase therefore reducing energy expenditure.
Stability of the new socket relies primarily on the alignment, comfortable axial support, and suspension. Test socket(s) is/are required for a dynamic trial within the parallel bars.
The presentation is a case study of one male patient, current prescription is a silicone socket and the Ottobock Helix hip and C Leg. He reported his silicone socket to be very comfortable but found during swing phase the socket would lose purchase resulting in a slight visible ‘drop off’. To combat this the patient supported his prosthesis with dorsal palm, leading to callous hard skin on his hand.
The final socket consisted of silicone with a rigid core plate and flexible socket edges cut back to the shape of a ‘bikini’ to provide support to the bony anatomy allowing the soft tissue to expand into the open sections.
The socket was effective in greatly improving range of motion, proprioceptive feedback and cosmetic appearance underneath clothing. The patient immediately reported that the prosthesis now felt ‘a part of him’ it was much more comfortable to wear and visibly improved his gait. It can be donned and doffed at the flick of a clip. His confidence has improved and he no longer feels he needs to support the limb with his hand at swing phase.
We now have a strong, comfortable socket which supports the patient throughout the gait cycle.
We have solved the ‘drop off’ issue at swing phase, the flexibility of the proximal edges allows a greater range of movement and is more forgiving when the patient is sitting down. The advances made are presented for consideration by other teams as a possible solution for Hip Disarticulation patients.
524
Bita Imam (1) presenting William C Miller (1)
UK, University of British Columbia, Vancouver, BC (1)
Status of Inpatient Rehabilitation for Individuals with Lower Limb Amputation in Canada
Lower limb amputation (LLA) is a relatively common condition. The incidence of LLA is expected to grow in Western countries due to the increase in diabetes and the aging population. Post amputation, rehabilitation is required to facilitate restoring lost function, regaining independence, and participation. Given the escalating healthcare costs, it is becoming increasingly difficult to provide rehabilitation. Little is known about the status of LLA rehabilitation in Canada.
To determine the; i) proportion of individuals who received inpatient rehabilitation in Canada, ii) length of inpatient rehabilitation, and iii) level of independence at discharge.
LLA surgical records in Canada starting from April 1 2004 to March 31 2012 were obtained from the Canadian Institute of Health Information (received Sept 2014). For each LLA record obtained, the National Rehabilitation Reporting System (NRS) determined whether the individual received inpatient rehabilitation. For individuals who had inpatient rehabilitation, the NRS provided data on length of rehabilitation, and the Functional Independence Measure (FIM) scores at baseline and discharge. The frequency (%) of individuals who received inpatient rehabilitation as well as the means (SDs) length of their inpatient rehabilitation and their FIM change score at discharge were calculated.
There were 8034 records of inpatient LLA rehabilitation from April 1 2004 to March 31 2012. This indicates that only 14.6% of LLA cases in Canada were followed by inpatient rehabilitation. For those who received inpatient rehabilitation, the mean length of their stay was 36.2 (24.6) days. The mean (SD) FIM score at baseline was 91.9 (19.4) whereas at discharge was 106.7 (33.3) / 126.
This is the first study to provide data on the status of inpatient rehabilitation and the independence level at discharge for Canadians with LLA. Understanding the status of inpatient amputee rehabilitation in Canada is essential for managing preventive and rehabilitation services provided to individuals with LLAs. The results of this study indicate that only 14.6% of individuals with LLA received inpatient rehabilitation in Canada.
525
Yunhee Chang (1) Presenting Shinki Kim (1) Jongkwon Kim (1) Jinho Son (1)
Canada, Korea Orthopedics & Rehabilitation Engineering Center, Incheon (1)
Comparison of the vertical GRF of two types of microprocessor-controlled prosthetic foot and energy storing feet during treadmill gait
Many research studies have been devoted to developing feet that enable automatic angular control of the ankle and active power output from the ankle. Among those, the microprocessor-controlled prosthetic foot (MCPF) has the advantage of inducing gait patterns that increase energy input and thus facilitate a more natural gait on various surfaces. However, biomechanical characteristics of microprocessor-controlled prosthetic foot during treadmill gait are unknown.
This present study was to investigate differences of the vertical ground reaction force (vGRF) between an energy storing foot (ESF) and two types of MCPF in transtibial amputee during treadmill gait.
The subject of this study was a male unilateral traumatic transtibial amputee. His functional classification was K4 level and he had no other musculoskeletal problem other than the amputation. vGRF and spitiotemporal parameters were obtained using the Zebris FDMT Treadmill (Zebris Medical GmbH, Germany). In this study, we use an ESF (Renegade) and two types of MCPF (Elan, Proprio-foot). Prior to the measurement phase, subject participated in an adaptation-familiarization trial in order to establish speed level. Data was obtained during 30 second, except for the 30 seconds before and after, while the subject has walked consecutively on the treadmill for 1.5 minute at the comfort speed.
Velocity (3.6km/h), cadence (96.6±1.51steps/min), stride length (125.0±1.75cm), and step width (11.9±0.3cm) in all prosthetic foots during treadmill gait were no different. The results of vGRF are as shown in Figure. vGRF of the prosthesis limb of all prosthesis foot showed a similar pattern. However, different pattern was observed in vGRF of the intact limb. The vGRFs of intact limb of MCPF in the early stance phase were relatively large than the end of the stance phase; whereas, ESF showed a tendency of the opposite. vGRF of the intact limb of MCPF in the early stance phase were about 240N larger than that of the ESF.

The vertical ground reaction force of two microprocessor-controlled prosthetic foots and energy storing feet on treadmill gait.
We found that the vGRF of the intact limb of MCPF in the early stance phase during treadmill gait were large than that of the ESF. It means that the MCPF exerts a large shock in intact limb than when an ESF used during treadmill. MCPF price is at least 3 times higher than ESF. Also, when considering the impact of an intact limb during treadmill gait, MCPF is not efficient than ESF. Thus, there must be research on the effectiveness of MCPF use of in a variety of environments.
526
Fumiko Tayama (1) presenting
Republic of Korea, Shibaura Institute of Technology, Saitama (1)
The Quantitative Analysis and Evaluation of Prosthetic Sockets for Trans-Femoral Amputees Using Finite Element Methods
The prosthetic sockets were produced by manually Prosthetist and Orthotist (PO). The beginner of PO was necessary a long time experience to get product skill. Therefore, the produced sockets depended on PO’s empirical knowledge. We made finite element (FE) model using residual limb’s internal tissues from MRI data, simulated the pressure occurring residual limb’s surface. Therefore, the purpose of this study was to compare the relationship between FE analyzed pressure and experimental result from pressure sensor.
To reproduce the upright standing and the gait stance phase situation in the simulation.
And to evaluate the adequacy and availability of the simulation.
Additionally, to compare the different type of the sockets.
The geometries of residual limb surface and the internal soft tissues and bone were captured from a male trans-femoral amputees, 38 years old, 169[cm] and 65[kg] who had more than 8 years experience using his prosthesis IRC (UCLA/AG)socket. The former UCLA socket is one of the IRC socket.It isn’t added pressure while taking the limb’s shape.So, it has to file off a lot of plaster. The latter AG socket is also one of the IRC socket. It is added pressure while taking the limb’s shape. So it doesn’t have to rectify the plaster.Magnetic resonance images (MRI) were obtained from the residual limb in supine lying and hip extended position with axial cross-sectional images at an interval of 10[mm] and 10[deg]. The mechanical properties of the materials were assumed to be linearly elastic, C.Mario et al .(2006) and J.C.H.Goh et al .(2005). We compared the pressure value of residual limb between the simulation from FE model and the experiment result from force sensor measurements.
In the upright standing simulation, the high pressure distributed anterior-proximal and medial-proximal area. The force sensor measurements indicated similar results, compared the FE analysis. The correlation between FE analysis and force sensor measurements indicated significantly high coefficient. In the gait stance phase simulation, the high pressure distributed anterior-distal and posterior-proximal area. The force sensor measurements indicated similar results, compared the FE analysis. However, the correlation between FE analysis and force sensor measurements indicated significantly high coefficient in the all distal position of residual limb, but there were no correlation in any position of side.
The purpose of this study was to compare the relationship between FE analyzed pressure and experimental result from pressure sensor. In the upright standing simulation, we obtained the high correlation between FE analysis and force sensor measurements. However, in the gait stance phase simulation, we have not yet obtained enough results. In the future study, we will try to improve FE analysis of the pressure of residual limb during gait of trans-femoral amputee gait.
527
Karine Langlois (1) presenting François Lavaste (1) Patricia Thoreux (2,1) Helene Pillet (1)
Japan, Arts et metiers Paris Tech.LBM/institut de biomecanique humaine Georges Charpak, Paris (1) France, Service de Chirurgie Orthopédique Hôpital Avicenne, Paris (2)
In vivo evaluation of the knee brace OdrA® on symptomatic knees with medial compartment osteoarthritis
Knee braces are recommended in physical treatments to manage knee osteoarthritis [1]. The OdrA brace is designed to unload the knee by creating a distraction between femur and tibia, and applying an external rotation by means of Rack pinion design inversed between medial and lateral sides is used to impose this kinematics to the brace.
The purpose of the study is to quantify the mechanical effects of the OdrA brace settings on symptomatic subjects, in order to understand the mechanisms explaining the pain’s relief when subjects wear the brace [2].
The experimental procedure consists in biomechanical assessment in laboratory combining low dose irradiation stereoradiographies with the EOS® system and motion analysis on an instrumented walkway by an optoelectronic system Vicon (gait and sit-to-stand). 10 symptomatic subjects will participate in the study after informed consent and undergo the protocol with and without the brace (7 static positions in the radiographic system and 4 kinematic conditions for the motion analysis). Data analysis of motion capture includes kinematic and kinetic parameters, center of pressure (CoP) displacements. From EOS data, femur and tibia positions as well as the displacement of soft tissues are calculated.
Preliminary results concern a control subject and a symptomatic subject. For the symptomatic subject, the amplitude of the postero-anterior displacement of the CoP increases in the condition “with the brace” compared to the condition “without the brace”, especially on osteoarthritis side during sit-to-stand (2.6 cm). In the same time, the peak of vGRF (at 33 % sit-to-stand cycle) also increases with the brace of 0.25 N/kg. The ratio between the peak of vGRF on the osteoarthritic and on the healthy sides is 0,93 without the brace and 1.04 when symptomatic subject is wearing the brace during sit-to-stand task.
The increase of the vGRF of the affected side, showed in the present study, could be related to a decrease of the pain, resulting in a better confidence on the affected lower limb. In addition, this parameter differs from the knee load, which must take account the distribution on forces compression by the brace. The instrumentation of the orthosis with strain gauges will test the hypothesis of unloading of the knee due to the orthosis [3].
From further analysis of radiographic images, it should be also possible to estimate the strain of the soft tissues. This deformation is expected to participate also to the pain decrease [2] according to two mechanisms: the transmission of the mechanical unloading of the knee and the sensitivity resulting of the stretching of the thigh skin.
[1] :Zhang Y and al. OARSI recommendations for the management of hip and knee osteoarthritis. Osteoarthritis and cartilage 2008; 16:137-62.
[2]: Laroche and al. Biomechanical effectiveness of a distraction-rotation knee brace in medial knee osteoarthritis : Preliminary results. The Knee, 2014;
[3] :FantiniPagini C. et al. The effect of valgus bracing on the adduction moment during gait and running in male subjects with varus alignment. Clinical Biomechanics, 2010; 25:70-76.
529
Raphael Dumas (1,2) presenting Catheryne Robert-Leblanc (5) Pierre-Marc Beaulieu (5) Laurent Frossard (3,4)
Hong Kong, Université de Lyon, Université Claude Bernard Lyon 1, Lyon (1) France, Laboratoire de Biomécanique et Mécanique des Chocs, IFSTTAR, Bron (2) France, Queensland University of Technology, Brisbane (3) Australia, University of the Sunshine Coast, Maroochydore (4) Australia, University of Quebec In Montreal, Montreal (5)
Errors in the knee joint forces and moments during gait depending on the foot and knee prosthetic components
Previously studies showed that inverse dynamics based on motion analysis and force-plate is inaccurate compared to direct measurements for individuals with transfemoral amputation (TFA). Indeed, direct measurements can appropriately take into account the absorption at the prosthetic foot and the resistance at the prosthetic knee [1]. However, these studies involved only a passive prosthetic knee.
The objective of the present study was to investigate if different types of prosthetic feet and knees can exhibit different levels of error in the knee joint forces and moments.
Three trials of walking at self-selected speed were analysed for 9 TFAs (7 males and 2 females, 47±9 years old, 1.76±0.1 m 79±17 kg) with a motion analysis system (Qualisys, Goteborg, Sweden), force plates (Kitsler, Winterthur, Switzerland) and a multi-axial transducer (JR3, Woodland, USA) mounted above the prosthetic knee [1,2]. TFAs were all fitted with an osseointegrated implant system. The prostheses included different type of foot (N=5) and knee (N=3) components.
The root mean square errors (RMSE) between direct measurements and the knee joint forces and moments estimated by inverse dynamics were computed for stance and swing phases of gait and expressed as a percentage of the measured amplitudes. A one-way Kruskal-Wallis ANOVA was performed (Statgraphics, Levallois-Perret, France) to analyse the effects of the prosthetic components on the RMSEs. Cross-effects and post-hoc tests were not analysed in this study.

A significant effect (*) was found for the type of prosthetic foot on anterior-posterior force during swing (p = 0.016), lateral-medial force during stance (p= 0.009), adduction-abduction moment during stance (p = 0.038), internal-external rotation moment during stance (p = 0.014) and during swing (p = 0.006), and flexion-extension moment during stance (p = 0.035).
A significant effect (#) was found for the type of prosthetic knee on anterior-posterior force during swing (p = 0.018) and adduction-abduction moment during stance (p = 0.035).
The RMSEs were larger during swing than during stance. It is because the errors on accelerations (as derived from motion analysis) become substantial with respect to the external loads. Thus, inverse dynamics during swing should be analysed with caution because the mean RMSEs are close to 50%.
Conversely, there were fewer effects of the prosthetic components on RMSE during swing than during stance and, accordingly, fewer effects due to knees than feet. Thus, inverse dynamics during stance should be used with caution for comparison of different prosthetic components.
[1] Dumas et al., Gait Posture 30: 560–562, 2009.
[2] Lee et al., Med Eng Phys 30: 825-33, 2008.
530
Dymphy van der Wilk (1) presenting Roy Reints (1) Klaas Postema (1) Tom Gort (3) Juha Hijmans (1) Bart Verkerke (1,2)
Canada, Department of Rehabilitation Medicine, Center for Rehabilitation, University of Groningen, University Medical Center Groningen, Groningen (1) The Netherlands, Department of Biomechanical Engineering, University of Twente, Enschede (2) The Netherlands, Noppe Orthopedietechniek, Noordwijkerhout (3)
Design of a SMART ankle foot orthosis for people with paretic ankle muscles

Functions of the smart AFO
[1] Perry J; Gait analysis: Normal and pathological function. Slack; 1993.
[2] Radtka SA; The kinematic and kinetic effects of solid, hinged, and no ankle-foot orthoses on stair locomotion in healthy adults. Gait Posture. 2006;24(2):211-218.
[3] Verkerke GJ; Design of biomedical products. In: Biomaterials in modern medicine: the Groningen perspective. Ed by Rakhorst G, Ploeg R. World Scientific Publishing, Singapore; 2008:23-38.
531
Thanyaporn Rakbangboon (1) presenting Kasun Kithsiri Rupasinghe (1) Loganayaki Ramakrishnan (1) Stephney Weerasinghe (1) Jeewantha Sasika (1) Pham Thi Hoa (1) Sunee Bovonsunthonchai (2) Manunchaya Samala (1) Cathy McConnell (1)
The Netherlands, Siridhorn School of Prosthetics and Orthotics, Mahidol University, Bangkok (1) Thailand, Faculty of Physical Therapy, Mahidol University, Bangkok (2)
The Effect of Three Prosthetic Knee Joints on Vertical Ground Reaction Force Patterns in Transfemoral Amputee Gait

1. Zdenek Svoboda, et al., (2012). ISPO Prosthetics and Orthotics International.
2. Thomas M, et al.,(1997) Journal of Orthopaedic Sports Physical Therapy.
3. C. SJÖDAHL, et al., (2002) Prosthetics and Orthotics International.
4. Jacquelin P. and Judith M., (2010), Gait analysis Normal and Pathological function, 2nd edition, California USA.
5. H. Goujon, et al., (2006) Prosthetic and Orthotic International.
6. Margrit S., (2012) Human Movement Science, January 2012.
532
Michael Ceder (1) presenting
Thailand, Teamolmed AB, Jönköping (1)
Vacuum positioning method for CAD-CAM manufacturing of hand and ankle foot orthoses
When treating these patients there are many difficulties to overcome, and as always an important part is a good shape of the orthosis which lead to good acceptance and comfort, otherwise the orthotic device will tend to be used only occasionally and consequently with poor outcome. Traditionally these orthoses are made by using a plaster mold or manufactured directly on the patient with a low temperature plastic. Both ways have their difficulties in getting the desired final position of the hand- and finger joints and is time consuming for both the patient and the manufacturer.
This method has giving us new possibilities to produce different kinds of orthotics, for upper and lower limbs and in different patient cases using scanning. Other advantages that we have found out are that, even if we were not scanning at the perfect angle, the software makes it possible to alter and produce orthoses in the desired position. For example, children with the diagnosis of CP are also growing individuals who frequently require new molds for manufacturing that often have been relating to new casting using Plaster of Paris. This method gives us a better initial approached of the problem, it’s better documented, easier adjusted and produced. The use of foam molds instead of plaster has also forced us to consider new materials and manufacturing methods. Moldeable felt, made of 100% polyester (Nordifa AB) is a material we have found suitable for these kind of hand orthoses. Felt is easily shaped, washable, has good breathability, and also good acceptance and comfort. The patient’s reaction of this new method in manufacturing of orthosis has been very promising.
533
Dymphy van der Wilk (1) presenting Pieter Dijkstra (1,2) Klaas Postema (1) Bart Verkerke (1,3) Juha Hijmans (1)
Sweden, Department of Rehabilitation Medicine, Center for Rehabilitation, University of Groningen, University Medical Center Groningen, Groningen (1) The Netherlands, Department of Oral and Maxillofacial Surgery, University of Groningen, University Medical Center Groningen, Groningen (2) The Netherlands, Department of Biomechanical Engineering, University of Twente, Groningen (3)
Effects of Ankle Foot Orthosis on Body Functions and Activities: A Systematic Review

Text box 1: Effects of AFOs on body functions and activities in people with paretic ankle muscles placed in the ICF framework [3]. ① elastic AFOs (rubber band connecting shank and shoe), ② circular AFOs made of fabric, ③ circular AFOs made of silicone, ④ dorsal AFOs, ⑤ hinged AFOs,
[1] Brehm M, Bus SA, Harlaar J, Nollet F. (2011) A candidate core set of outcome measures based on the international classification of functioning, disability and health for clinical studies on lower limb orthoses. Prosthet Orthot Int 35:269-77.
[2] Harlaar J, Brehm M, Becher JG, Bregman DJ, Buurke J, Holtkamp F, de Groot V, Nollet F (2010) Studies examining the efficacy of ankle foot orthoses should report activity level and mechanical evidence. Prosthetics and Orthotics International 34:327-35
[3] World Health Organization (2001) International classification of functioning, disability and health (ICF). Geneva, Switzerland
535
Babak Hassan Beygi (1) presenting MS Wong (1)
Malawi, The Hong Kong Polytechnic University, Kowloon (1)
Evaluation of a purpose-design assessment frame utilized in the casting procedure of patients with adolescent idiopathic scoliosis
[1] Landauer F; 2003 J Pediatr Rehabil Med
[2] Wong MS; 2005 Prosthet Orthot Int
[3] Li M; 2012 Eur Spine J
[4] Chan SL; 2014 scoliosis
536
Philippe Ferreira (1,2) Dominik Raab (2) presenting Dietmar Rosenthal (2) Mario Siebler (3) Harald Hefter (4) Andres Kecskemethy (2,1)
Hong Kong, ITBB GmbH, Neukirchen-Vluyn (1) Germany, University of Duisburg-Essen, Duisburg (2) Germany, MediClin Fachklinik Rhein/Ruhr, Essen (3) Germany, University of Düsseldorf, Düsseldorf (4)
A Numerical Approach to Evaluate Stroke Patients Walking Disorders Based on Instrumental Gait Analysis
A consistent scoring method for evaluation of walking disorders after stroke is very desirable in order to quantify the functional impairment and to evaluate the outcome of the rehabilitation. Traditional internationally recognized scores are widely used but fail to assess the functional mobility or to assist clinicians in their choice of rehabilitation methods.
In this context, a team of medical experts developed a scoring method, referred to as ReHabX-score, that evaluates six functional gait motion criteria, namely “Posture”, “Leg movement”, “Arm movement”, “Gait speed”, “Gait flow”, “Stability/risk of falling”.
In order to enhance objectivity and reproducibility of the scoring result, a numerical approach was developed, based on motion capture (MoCap) data.
The gait of 47 stroke patients was measured using MoCap technology. 261 kinematical parameters (called “features”) were identified and extracted from each measurement. According to their nature, those features can be grouped in 5 categories: patient anthropometric data, standard parameters from instrumental gait analysis, discretized joint angles, ReHabX-features (novel gait features developed in the context of this study), derived features such as interlimb coordination and normalized features.
The patients were rated using the ReHabX-Score and stepwise linear regression was used to select and weight the features in order to numerically reproduce the functional average scores provided by five medical experts.
The model accuracy of all the gait motion criteria is above 80% (Fig. 1.a) with the exception of the arm movement because paretic and spastic arms are significant stroke deficits with very different kinematical effects. Fig. 1.b shows the individual medical scores (blue circles) and the corresponding numerical ones (red crosses) plotted against the average medical score for each patient, in the case of “Posture”. The variability of the numerical score is much smaller than the medical scorings and much fewer outliers fall outside the desirable matching zone (green area).

Final results: (a) Numerical model accuracy (b) ReHabX-score “Posture”: medical vs. numerical scores.
The numerical scoring based on measured motion parameters allows reproducible assessment of gait disorders based on quantitative criteria. This offers a valuable support for the objective assessment of movement disorders and provides a valuable tool to support the selection of the most appropriate rehabilitation measure, thus accelerating the recovery of the gait ability after stroke.
538
Munjed Al Muderis (1) presenting Aditya Khemka (1) Sarah Lord (1) Henk Van De Meent (2) Jaun-Paul Frolke (2)
Japan, University of Notre Dame, Sydney, NSW (1) Australia, Radboud university medical center, NIjmegen, Netherlands (2)
Safety of Osseointegrated Prosthesis for trans-femoral amputees
Although osseointegration has been proven to significantly increase walking ability and prosthesis-related quality of life, the risk of potential infectious complications prevents further introduction to a larger scale, so far.
In this study we report on infectious complications to determine potential risk factors in the first two years after implantation
After IRB approval, two university hospitals in Australia and The Netherlands conducted a prospective clinical cohort study to analyze all consecutive subjects with trans-femoral amputation (3 bilateral) who underwent implantation of osseointegrated femoral prosthesis (ILP Ortho Dynamics GmbH Lubeck Germany).
Infectious complications were prospectively registered and classified. Potential risk factors for complications were determined including gender, age, duration after amputation, cause of amputation, comorbidity including BMI, smoking behavior and length of stoma.

Infectious complications occurred in; Australian group (n= 22): 7 grade 1A, 5 grade 1C, one grade 3C. Netherlands group (n= 24); 15 grade 1A. 8 grade 1C, one grade 2C. Risk factors that might have contributed to these complications included smoking, and female gender.
Complications related to the osseointegrated leg-prosthesis do occur but the suffering and disabilities are relatively mild. Infectious events are superficial and can be managed with intensive local irrigation and antibiotics. Strict patient selection and adherence to exclusion criteria, may reduce complication rate.
Tillander J1, Hagberg K, Hagberg L, Brånemark R. Osseointegrated titanium implants for limb prostheses attachments: infectious complications. Clin Orthop Relat Res. 2010 Oct;468(10):2781-8
540
Motonori HOSHINO (1) presenting Shun SASAGAWA (2) Yoshiko TOBIMATSU (1) Kimitaka NAKAZAWA (2)
National Rehabilitation Center for Persons with Disabilities, Tokorozawa, Saitama (1) Japan, University of Tokyo, Meguro, Tokyo (2)
Evaluation of postural control during quiet stance using center of mass acceleration in bilateral transtibial amputees
Many standing posture control studies in transtibial amputees have been using center of pressure (COP) as the evaluation indicator. However, single inverted pendulum is a prerequisite in evaluating the posture control of the whole body by COP. Meanwhile, total body center of mass(COM) acceleration can be easily calculated by dividing the ground reaction force by body mass and can be used to evaluate the posture control of the whole body.
The purpose of this study was to evaluate the posture control in bilateral transtibial amputees by using COM acceleration in the sagittal plane during quiet standing.
The experiments were carried out with four traumatic bilateral transtibial amputees and four healthy subjects who were asked to stand quietly for 30s on two force platforms with their eyes open or closed. We derived the actual CoM acceleration by dividing A–P share force by body mass. Root mean squre (RMS) and time frequency of the amplitude about the COM derived were analyzed.Simultaneously, Angular displacements and accelerations of the ankle, knee, and hip joints were calculated from kinematic data obtained by a motion capture system (MAC3D).
We found that RMS of the acceleration of COM showed a greater trend in the amputee group than the healthy group.As for frequency characteristic, the healthy group exhibited a monomodal pattern with a peak at about 0.8Hz while the amputee group exhibited a bimodal pattern with a second peak at 1.4~2Hz in addition to the peak frequency of the healthy subjects.
From the fact that the natural frequency increases as the number of joints involved in standing posture control increases, the second peak at high frequency which was not seen in the healthy subjects shown in COM acceleration of the amputee group is a sensitive evaluation indicator against the changes of the posture control strategy of transtibial amputees and suggests the posture control strategy is changing at a whole-body level.
541
Malte Bellmann (1) presenting Marc Kraft (4) Siegmar Blumentritt (2,3)
Japan, Otto Bock Competence Centre Göttingen, Göttingen (1) Germany, Otto Bock HealthCare GmbH, Duderstadt (2) Germany, PFH Private University of Applied Science, Göttingen (3) Germany, Technical University Berlin, Berlin (4)
Biomechanical Investigation of Principles of Load Transfer in Transfemoral Sockets: An Innovative Study Design and Preliminary Results
Ischium containment socket technologies have established in the past for the treatment of transfemoral amputees. They differ from other technologies in shape and functionality (1,2,3). The main difference is to be found in the proximal functional area that is responsible in different proportions for the force transmission between the residual limb and the bony pelvis structures. Socket technologies without force transmission in the tuber ischium region are available as well (sub-ischial sockets).
Within the scope of this biomechanical study, force transmission principles between residual limb and the main functional elements of different transfemoral prosthetic socket technologies are discussed.
The sockets are segmented according to the four main areas (ischium containment, lateral wall, anterior wall, control area) and implemented in a CFK frame that includes load sensors which are able to record three forces in the corresponding segments and their centres of pressure. A self-developed mobile wireless LAN system measures data synchronically to a stationary gait analysis system (Kistler, Vicon).
Three different sockets (CAT-CAM, MAS, sub-ischial socket) were measured each with 5 transfemoral amputees while standing with different socket adduction and flexion angles (sockets tightly installed on a stationary fixture), level walking, descending stairs and ramps (sockets installed on a prosthetic knee joint and foot).
The results suggest that the principles of force transmission within the four main socket areas do not differ significantly from each other between a CAT-CAM and MAS socket - neither in standing position nor during walking. With both socket types, a high degree of axial force is transferred by the medially located containment area. Furthermore it becomes obvious that the contribution of the lateral socket wall for stabilization between residual limb and socket during the stance phase is very low. With the sub-ischial socket that does not contact the pelvis, significant differences can be identified, however. They are to be found in the position of the total force running through the socket leading to the conclusion that the force transmission principles are different compared to both ischial or ramal containment sockets.
In the literature, the force transmission principles of transfemoral socket technologies have been discussed exclusively on the basis of fitting experiences (1,2,3). Theoretical models assumed that - also with ischial containment total contact sockets - an axial force can only be transferred by the soft tissue cover of the residual limb. The method described in this study allows for the first time to objectify by comparison which socket areas are involved in force transmission and to what extent.
1. Sabolich J. Contoured Adducted Trochanteric-controlled alignment method (CAT-CAM): introduction and basic principles. Clin Prosthet Orthot 1985;9:15-26.
2. Ortiz RM. M.A.S.-Construction for Above Knee Prostheses. Orthopädie-Technik 2007; 58:240-247.
3. Schuch CM et al. Current transfemoral sockets. Clin Orthop Relat Res 1999;361:48-54.
543
Bjoern Altenburg (1) presenting Malte Bellmann (1) Thomas Schmalz (1) Siegmar Blumentritt (2)
India, Otto Bock Competence Centre Göttingen, Göttingen (1) Germany, Otto Bock HealthCare GmbH, Duderstadt (2)
Biomechanical investigation of currently available microprocessor controlled prosthetic feet
Since the introduction of microprocessor controlled knee joints in the nineties their market share has constantly increased. Advantages such as the functional range and the safety have been proven repeatedly. These knee joints are accepted by users and technicians and have become an indispensable part of today’s prosthetic treatment options of the lower limb. Considering, however, the development of electronically controlled prosthetic feet, acceptance and use is significantly lower.
The study investigates the performance of microprocessor controlled prosthetic feet currently available on the market.
Five microprocessor controlled prosthetic feet and the everyday feet (all of them carbon spring feet, different models) of the subjects are tested. The prosthetic alignment is standardized and documented. The study is performed with 10 subjects (5 transfemoral, 5 transtibial). The focus is on everyday situations such like level walking at different walking velocities, walking on ramps, on stairs, on changing terrain, walking with small steps, walking with different heel heights, walking backwards and stepping on objects. In addition swaying is measured during standing on 10° inclines. For the measurements a stationary gait analysis system with 12 Vicon Bonita cameras and 2 Kistler force plates is used.
First results suggest that some features of these microprocessor controlled prosthetic feet such as speed adaptation play a rather secondary role. Considering the measuring data and the user feedback any clear positive effects cannot be identified. Other characteristics, however, such as ramp adaptation show clear effects and a functional gain. The same applies to the heel height adaptation and to standing on inclined ground. In addition to the individual functional range, the feet basically differ from each other in the real time adaptation to the terrain and in the incremental adaptation whereas the real time adaptation offers clear advantages.
In contrast to the functional gain, disadvantages of these microprocessor controlled prosthetic feet can be identified too. The extra weight compared to conventional prosthetic feet should be mentioned here primarily
The new generation of prosthetic feet shows a clear functional gain with respect to terrain and heel height adaptation. Dependent on the functional principle, however, the quality and thus the usability of the new functions strongly differ from each other.
For prosthesis users often moving on changing terrain or often varying their heel height (other shoes, walking barefoot), microprocessor controlled prosthetic feet of high functional quality offer a high potential to make a contribution to an improved prosthetic treatment and to an increased quality of life.
544
Andrea Giovanni Cutti (1) presenting Ilaria Parel (1) Martina Luchetti (2) Tiffany Ryan (3) Rinaldo Sacchetti (1) John Miguelez (3)
Germany, Centro Protesi INAIL, Vigorso di Budrio (BO) (1) Italy, University of Bologna, Bologna (BO) (2) Advanced Arm Dynamics, Irving (TX) (3)
Changes in shoulder and trunk biomechanics during a standardized manipulation task performed with a multi-grip prosthetic hand
Min, max and median values for the ROM, comparing the tri-digital (TD), Michelangelo (M) and sound side (S)

[1] Carey (2008) Clin Biomech
[2] Greitemann (1996), Z Orthop Ihre Grenzgeb
546
Pitchaya Rayothee (1) presenting Jackrit Suthakorn (2)
Thailand, Sirindhorn School of Prosthetics and Orthotics (SSPO), Bangkok (1) Thailand, Center for Biomedical and Robotics Technology (BART LAB), Bangkok (2)
Requirement and Recommendation for Development of New Assistive Device in Spinal Cord Injury Patient (SCI): A Baseline Study
Currently, a number of patients who suffer from gait impairment are increasing causing from many reasons, such as, traumatic accidence, cerebrovascular disease (CVA) and spinal cord injury (SCI). Assistive devices might be recommended to enhance and increase their functional ability, such as, crutch, cane and wheelchair. Moreover, the orthoses are also recommended in term of promoting the lower limb movement and minimizing the pathologic gait.
The aim of the study is to find the requirement and recommendation for development of new assistive device in spinal cord injury patient from expert opinions who involve with SCI treatment.
The research style is descriptive study. There are 31 participants including rehabilitation doctors, certified prosthetists and orthotists (CPO), PO lecturers, physical therapists (PT), PT lecturers, nurses and SCI patients. The survey questionnaire was sent to the participants by private online questionnaire and document papers. The questionnaire contained of 7 sections which are general information, comment to current assistive device for walking, currently treatment way for SCI, assistive device prescription, efficiency of assistive device for walking, problem in currently assistive device for walking, and other recommendations. After 2 weeks, the documents and online questionnaire was sent to non-responders with a follow-up telephone call.
There are 31 participants’ responded (62%) and an average of age is 40.6 years. Approximately 150-200 cases come to the public hospital per year. The goal of rehabilitation treatment is “to promote walking without risk of falling”. Currently, treatments are focused on increasing muscle function and strength, balance control, activity dairy living with/without assistive devices and environment modification. For assistive devices, AFO, KAFO and HKAFO are the most common of medical prescription for standing and walking purposes. However, the common devices are passive orthosis and patient walk with unnatural of gait. Concerning the recommendation, hip and knee joints are the major part which should be controlled and followed by ankle and trunk respectively. Moreover, the assistive device should be automation and do not specific for only SCI patient.
Multidisciplinary team included patient and relative is an important team work for promoting the treatment to reach the optimal goal. While, many design of orthoses are available in the clinic, but, most of them are passive and patients walk with unnatural of gait pattern. In concerning point, hip and knee are the most important part that should be controlled and followed by ankle and trunk. Finally, assistive device should function automatically and do not specific for only a group of patient.
547
Aditya Khemka (1) presenting Sarah Lord (1) Belinda Bosley (1) Munjed Al Muderis (1)
Thailand, University of Notre Dame, Sydney, NSW (1)
Osseointegrated Prosthetic Limb for Amputees - Over Hundred Cases
The Osseointegrated Prosthetic Limb (OPL) was introduced in 2011. Prior to its advent all prostheses consisted of stump and socket mechanisms which did not changed dramatically since Ambroise Pare lower limb prosthesis in 1525. These socket prostheses failed to address a few major requirements of normal gait. Our hypothesis was that using an Osseointegrated Prosthetic limb will result in superior function of daily activities, without compromising patients’ safety.
A. To describe the surgical procedure of the OPL; and
B. To present data on potential risks and benefits with assessment of clinical and functional outcomes at follow up
This paper presents our first 100 cases operated between 2011 and 2015 in a single centre, Sydney, Australia by a single surgeon. The criteria for inclusion was strict including a formal interview with the team including the surgeon, radiologist, anaesthetist, pain physician, psychiatrist, physiotherapist, rehabilitation physician and the prosthetist. Patient characteristics and demographics were collected. Outcomes assessment included health related quality of life questionnaires (SF 36 and Q-TFA), Mobility Predictor (K Levels – AMPRO), functional testing (6MWT and TUG) and evaluation of energy expenditure. The data was collected at all stages of the patient journey and statistically analysed.
The total number of patients was 101 with 107 implantations. 7 patients were blateral amputees. Average age at amputation was 33 years (range 3-76), at implantation 44.3 (range 17-76). Average period from amputation to implantation was 13 years (range 0-46). Traumatic amputations occurred in 61 patients (77%). Infection was the second most common cause for amputation consisting 12%. Neoplasia was the cause for amputation in 10% of the cases. 30% of the patient included in the study were wheelchair bound. Both K scores, Time Up and Go and 6 MWT tests showed a statistically significant improvement, with high significance p=0.0006, and p=0.0149, respectively. HRQOL improved dramatically for all patients. The energy expenditure increased at an average 4 fold after the surgery at their final follow up.
This study shows favorable results for OPL treatment for above knee as well as below knee amputees, compared to Socket prosthesis. Our experience of over 100 patients has revealed encouraging results with a major improvement in patient’s functionality and quality of life, and a low rate of complications.
549
Eric Versluis (1) Mona Hichert (1) Dick Plettenburg (1) presenting
India, Delft University of Technology, Delft (1)
Normative values for maximum voluntary applied grip and pinch forces in healthy subjects as a baseline for hand prosthesis design – a systematic review
During the design of a prosthetic hand, information is needed about the requirements the prosthesis should meet. Information about the desirable maximum voluntarily applied forces with a prosthetic hand is of great help when composing these requirements. Unfortunately no clear reference values exist for this purpose. Therefore it will be of value to know how much force a healthy person can exert with the hand. This information can then be implemented in the design requirements.
The aim of this review is to provide information about the maximum grip and pinch strength of healthy subjects without upper extremity defects, and to serve as a basis for composing the design requirements of a prosthetic hand.
The databases Scopus and Pubmed were searched with the words ‘grip’, ‘pinch’, ‘norm* data’, ‘norm* values’, and ‘reference values’, while excluding results on ‘disorder’, ’syndrome’ or ‘deficiency’. The identified articles were selected for the comparative analysis using the following criteria: written in English; contain data about grip, tip, key, or palmer pinch forces; clear description of protocol, instruments used, and calibration; healthy subject group size >100; subject age 20-60 years; subjects from Europe or North America.
A total of 137 articles were identified. After the application of the selection criteria 11 articles were included: of which 9 articles contained data on grip strength comparison, and 7 articles on pinch strength. Inter-subject variability of grip and pinch strength was found to be influenced by the following variables: age; gender; anthropometry; occupational manual strength; hand dominance; and race. Only on age and gender data was reported throughout the included articles. Furthermore, the acquired results were influenced by method related variables, including: posture, instrumentation; calibration; measurement type; and fatigue. However, the influence of these method related variables was reported to be small.
Male grip strength was found to vary between the included studies between 270 N and 740 N; female grip strength varied between 120 N and 430 N. Key pinch strength varied between 55 N and 150 N for males, and 25 N and 115 N for females. Tip pinch strength varied between 40 N and 125 N for males, and 25 N and 85 N for females. Palmar pinch strength varied between 70 N and 150 N for males, and 45 N and 110 N for females.
Differences found between different age groups within the studies are statistically significant. The age group 30-39 years has the highest average grip strength.
To compose the design requirements of a prosthetic hand device the maximum voluntarily applied forces with the device are of interest. For this a comparison is made with the maximum applicable grip and pinch forces by healthy individuals. The maximum average grip strength is about 550 N for male subjects and about 340 N for female subjects. Male average maximum pinch forces range, depending on pinch type, from 80 N to 100 N. Female average maximum pinch forces range, depending on pinch type, from 55 N to 80 N. The designer of a hand prosthesis can use the values found to formulate the requirements for his/her design.
552
Jutamanee Poonsiri (1) presenting Tippawan Junthadech (1) Thanatat Jaratrungolan (1) Nattapong Polharn (1) Satreerat Siripachote (1) Tullathorn Tullatharn (1) Poompong Tiangtam (1)
India, Sirindhorn School of Prosthetics and Orthotics, Mahidol University, Bangkok (1)
A New Design of Tracing and Casting Positioning Tool for Lower Limb Orthoses

The results showed that the ML measurement and the desired knee and ankle angles in the sagittal plane with the conventional methods had greater errors than that of the new design tool. With the designed tool, the time spent for tracing, casting and modification was also reduced. The questionairs showed the orthotists satisfied with the proposed design, however the weight of the tool should be improved. The prpoposed tool can help the orthotic casting and tracing more accuracte, and faster, and facilitate orthotists work outside facility or in wards because its mobile design. design.
555
Sebastian Wolf (1) presenting Julia Block (1) Cornelia Putz (1) Daniel Heitzmann (1) Merkur Alimusaj (1)
India, Clinic for Orthopedics and Trauma Surgery Heidelberg University Hospital, Heidelberg (1)
Functional effects of a new carbon prosthetic foot with hydraulic ankle
There are a host of carbon fiber prosthetic feet on the market. Commonly they are designed to enable a natural roll-over while returning energy via elastic deformation of carbon forefoot and hindfoot springs. However, the deformation of the carbon foot in fact offers no plantar- or dorsal motion as such but allows for energy take-up in mid-stance which ideally would be given back for push-off but which in practice typically is hardly achieved [1]. The newly released prosthetic foot Kinterra© (Freedom Innovations, USA) combines the functionality of a carbon foot with a hydraulic joint unit to act as a prosthetic ankle joint allowing for12° of range of motion. The resistance of the hydraulic damper may be adjusted to individual conditions.
To monitor the functional consequences of this new prosthetic foot when used by trans-femoral amputees in combination with a Plié II knee joint© (Freedom Innovations) in different walking conditions.
Six transfemoral amputees (45y± 11y; 178cm ± 8cm; 82kg ± 15kg) were provided with a Plié II knee and a Kinterra foot using their current socket. After four weeks adaption time the subjects underwent a 3D-gait analysis walking on level ground and on inclines (inclination of 2.5°, 5.0° and 7.5°). Kinematics and kinetics were calculated using standard modeling procedures [2]. Additional markers were used to calculate the motion of the prosthetic foot. Gait data of 17 unimpaired subjects (28y ± 6y; 178cm ± 8cm; 73kg ± 14kg) served as reference.
The prosthetic foot showed on level ground:
1) a large range of motion (ROM 23.8º±3.4º), with the hydraulic unit contribution of 5°
2) reduced internal plantarflexion moment in late stance
3) limited ankle power generation in late stance.
On inclines: 4) slight increase in total dorsiflexion, 5) almost no adaptation via hydraulic ankle dorsiflexion

Even though the ROM of the hydraulic ankle is small, the overall ROM of the foot is adequate. However, the hydraulic ankle angle does not improve adaptations to ascends due to the limited dorsiflexion. In descends, the prosthetic ankle should promote an adaptation to an incline via knee knee flexion [3] by offering a larger dorsiflexion ROM.
[1] Fey NP, Klute GK, Neptune RR., Clin Biomech 2011; 26(10):1025-32
[2] Kadaba, MP, Ramakrishnan HK, Wootten ME, J Orthop Res, 1990; 8(3):383-92
[3] Hansen AH, Childress DS, Miff SC, Hum Mov Sci 2004; 23(6):807-21
556
Tom Saey (1) Ingrid Knippels (1) Eveline De Raeve (1) Luiza Muraru (1,3) Louis Peeraer (1,2) presenting
Germany, MOBILAB, Thomas More University College, Geel (1) Belgium, Department of Kinesiology, Musculoskeletal Rehabilitation, KU Leuven, Leuven (2) Belgium, Biomechanics section, Mechanical Engineering Department, KU Leuven, Leuven (3)
The effect of prosthetic misalignment in the sagittal plane on trans-tibial amputee gait
If a lower leg prosthesis is not well aligned or its configuration is not adapted to the patient’s anatomy and characteristics, this will result in pain, discomfort and, ultimately, even loss of function. Despite the clear importance of the alignment process, it is currently based primarily on the expertise and experience of the orthopedic technologist, with a rather small evidence base.
The fact that a similar change in alignment can have different effects for different individuals is an additional problem.
The aim of this study is to investigate the influence of alignment changes of the prosthetic foot to anterior or posterior on the knee during gait.
For 5 active, healthy subjects with a trans-tibial amputation, experienced in walking with their prosthesis, gait was recorded in a specialized gait lab. Measurements were performed on kinematics (marker based), and ground contact forces (force plate). The anterior/posterior translation of the foot with respect to the socket was varied randomly in steps of 2.4cm to 4.8 cm from reference (bench alignment) in each direction. For each alignment 3 trials were recorded, results were averaged for these 3 trials.
The effect of shifting the prosthetic foot in the sagittal plane on mean knee kinematics is depicted in Figure 1. Results from our patient study show that anterior-posterior shift of the prosthetic foot results in increased knee extension-flexion moments respectively while dorsi-plantarflexion of the prosthetic foot results in increased knee flexion-extension moments during midstance.

Mean knee flexion/extension moment for anterior-posterior translation (A) and dorsi-plantarflexion tilt (B) of the prosthetic foot.
Our study indicated that linear and angular changes of the prosthetic foot alignment influence knee moment. Schmalz et al. [1] investigated the effect of different prosthetic alignments on knee moments and metabolic parameters and reported similar results related to knee kinematics.
Our final goal is to correlate kinematic data with comfort parameters in an effort to predict individualized optimal prosthetic alignment.
Schmalz et al. 2002, Gait and Posture.
557
Kerstin Caine-Winterberger (1) presenting Rickard Brånemark (1) Max Ortiz-Catalan (1)
Belgium, Sahlgrenska University Hospital, Gothenburg (1)
Outcome measures following implanted electrodes in an osseointegrated trans-humeral patient
559
Chih-Kuang Chen (1,2) presenting Weng-Pin Chen (3) Shih-Cherng Lin (1) Sih-Chen Huang (3) Simon Fuk-Tan Tang (1,2)
Iceland, Department of Physical Medicine and Rehabilitation, Chang Gung Memorial Hospital, Taoyuan (1) Taiwan, School of Medicine, Chang Gung University, Taoyuan (2) Taiwan, Department of Mechanical Engineering, National Taipei University of Technology, Taipei (3)
Changes in Plantar Pressure Distribution in Response to Different Metatarsal Pad Designs and Placements during Walking - a Dynamic Finite Element Analysis
Forefoot pain and discomfort within the plantar soft tissue beneath the metatarsal (MT) heads is referred to metatarsalgia. The MT pad is commonly prescribed for patients with metatarsalgia in clinical practice. Although the effectiveness of MT pad on the plantar pressure reduction had been investigated in previous studies using plantar pressure measurement system, no clear conclusion on the MT pads design and placement that can achieve best effectiveness in plantar pressure reduction so far.
This study aimed to investigate the effects of different placements and geometrical designs of MT pad on the plantar pressure distribution through dynamic finite element analysis.
A three-dimensional FE model of the foot-shoe complex, including the foot bony and ligamentous structure, soft tissue, MT pad, insole, outsole and shoe cover, was adopted in this study. The trajectory of the reflective markers and the kinematic data of the foot obtained from gait analysis were used to define the boundary condition in the FE analysis. After validation of the model, the effects of MT pad on the plantar pressure distribution beneath the metatarsus and the second MT head were investigated by changing five different placements, two different heights, and three different sizes of the MT pad.
When the pad was placed 10 mm proximal to the second MT head, better efficacy of pressure reduction than other placements was found. Under the appropriate placement, the efficacy would be further improved by raising the height of the pad from 5 mm to 10 mm, but causing high pressure concentration beneath the metatarsus. However, increasing the pad size by 10% would relieve the concentrated high pressure.
According to the results, it is found that increasing the height as well as area of MT pad properly may enhance the efficacy of plantar pressure reduction beneath the second MT head, and relieve high pressure concentration beneath the metatarsus. More subjects with different size and structure of foot should be recruited in the future in order to provide a more comprehensive recommendation on the prescription of MT pad.
560
Jai Kulkarni (2) Dominic Hannett (1) presenting Steven Purcell (1)
Taiwan, opcare, Oxfordshire (1) UK, Disablement Services Centre (DSC), University Hospitals of South Manchester, Manchester (2)
Bariatric amputee: A growing problem?
This study reviewed prevalence of patients with lower limb amputations with above normal weight profile, with
body mass index over 25, in seven disablement services centres managing their amputee rehabilitation in the United Kingdom
To review two clinical standards of practice in amputee rehabilitation. Ambulant lower limb amputees should have their body weight recorded on an electronic information system, with identification of cohort with body weight >100 kg. Lower limb amputees to be provided with suitable weight-rated prosthesis.
Data were collected from the Clinical Information Management Systems. Inclusion criteria – subjects were ambulant prosthetic users with some prosthetic intervention in the last 5 years and had at least one lower limb amputation.

In 96% of patients, the weight record profile was maintained. In addition, 86% were under 100 kg, which is the most common weight limit of prosthetic componentry. Of 15,204 amputation levels, there were 1830 transfemoral and transtibial sites in users with body weight over 100 kg. In 60 cases, the prosthetic limb build was rated to be below the user body weight.
In 96% of our patients, body weight was documented, and in 97%, the prosthetic limb builds were within stated body weight limits, but this may not be the case in all the other disablement services centres in the United Kingdom. Also, the incidence of obesity in the United Kingdom is a growing problem, and the health issues associated with obesity are further compounded in the amputee population.
1. Dalton M, Cameron AJ, Zimmet PZ, et al. Waist circumference, waist–hip ratio and body mass index and their correlation with cardiovascular disease risk factors in Australian adults. J Intern Med 2003; 254: 555–563.
2. Yusuf S, Hawken S, Ounpuu S, et al. Obesity and the risk of myocardial
infarction in 27,000 participants from 52 countries: a
case-control study. Lancet 2005; 366: 1640–1649.
3. The NHS Information Centre, Lifestyles Statistics. Statistics on obesity, physical activity and diet: England,
2012, 23 February 2012. Leeds: The Information Centre,
2012.
4. Tzamaloukas AH, Leger A, Hill J, et al. Body mass index in patients with amputations on peritoneal dialysis: error of uncorrected estimates and proposed correction. Adv Perit
Dial 2000; 16: 138–142.
5. National Amputee Statistical Database (NASDAB). Edinburgh: Crown Copyright, 2005. Available at: http://www.limbless-statistics.org/
562
Zdenek Svoboda (1) presenting Zuzana Kovacikova (1) Karolina Orechovska (1) Miroslav Janura (1)
- , Faculty of Physical Culture, Palacky University Olomouc, Olomouc (1)
Balance assessment during drop jump landing in subjects with transtibial amputation
Ground reaction force (GRF) measures during drop jump landing were presented as a useful simple tool for dynamic balance assessment in subjects with ankle [1,2] or knee[3] deficits. We hypothesized that drop jump landing would be sensitive and reliable tool for dynamic balance assessment also in subjects with transtibial amputation.
The aim of the study was to assess reliability of selected variables derived from GRF during drop jump landing and compare values between subjects with transtibial amputation and controls.
Research sample consisted of subjects with transtibial amputation (n = 14, age = 43.4 ± 9.8) and control subjects (n = 12, age = 43.9 ± 9.5). Three trials of drop jumps landing was assessed for each subject. From ground reaction force data stability index scores for anterior-posterior (APSI), medial-lateral (MLSI) and vertical (VSI) directions, composite stability index (DPSI)[1] and time to stabilization (TTS) were computed[3]. To determine between-session reliability, ICCs (3,1) were computed independently for group of subjects with transtibial amputation (TTA) and control group. Differences between groups were assessed by one way ANOVA.
For both groups ICC values of stability index scores varied from 0.77-0.88. ICC values of TTS were 0.55 for TTA and 0.63 for control group. Mean vaules of measured avriables and p values are presented in table 1.

Reliability of measurement is acceptable for stability index scores, but relatively low for time to stabilization. Comparison of groups suggests that this test is insufficiently sensitive for subjects with transtibial amputation. Future research would consider using of multiple jump directions[1].
[1] Brown, C. N. et al. (2010). Med Sci Sports Exerc, 42(12), 2258-63.
[2] Ross, S. E., et al. (2009). Med Sci Sports Exerc, 41(2), 399-407.
[3] Colby, S. M., et al. (1999). J Orthop Sports Phys Ther, 29(8), 444-54.
563
Joseph BASCOU (1) Coralie VILLA (1) presenting Didier JACQUOT (1) Alexandre TONNELIER (1) Denis MANGENOT (1) Nourredine EL FETTAHI (1) Xavier DREVELLE (1) Pascale FODE (1)
Czech Republic, Institution Nationale des Invalides/CERAH, Paris (1)
External measurement of 3D interactions between the residual limb of an amputee person and the socket
The socket usually links the residual limb and the prosthetic components. As it transmits the efforts from the residual limb to the prosthesis, the socket provides proprioceptive informations but can induce pain and injuries.
Interactions forces measurement within the socket could enhance both socket fitting and rehabilitation [1]. However few methods only were yet designed to access pressure and shear forces within the socket during gait [2] [3], Particularly Sewell et al. designed a protocol to measure pressure forces by external measurements [4].

[1] Reger et al. 2010. London: Wounds International
[2] Sanders et al. 2006. Prosthetics and Orthotics Int.
[3] Laszczak et al. 2014. Medical eng & Physics
[4] Sewell et al. 2012. Artificial Intelligence in Medicine
564
Futoshi Wada (1) presenting Kenji Hachisuka (1) Yasuhiro Watanabe (2) Kenji Tateishi (3) Mitsuo Arai (4) Taisuke Sakaki (5)
France, University of Occupational and Environmental Health, Japan, Kitakyushu, Fukuoka (1) Japan, Fukuoka Industrial Technology Center, Kitakyushu, Fukuoka (2) Japan, I-Quark Corp., Kasuya, Fukuoka (3) Japan, Arai’s PO Ltd., Kitakyushu, Fukuoka (4) Japan, Kyushu Sangyo University, Higashi-ku, Fukuoka (5)
Development of an advanced stance control system with bi-directional wireless data transfer

565
Deepak Sharan (1) presenting Mathankumar Mohandoss (1) Rameshkumar Ranganathan (1)
Japan, RECOUP Neuromusculoskeletal Rehabilitation Centre, Bangalore, Karnataka (1)
Bone mineral density in children with cerebral palsy: effect of sequenced rehabilitation protocol following a single event multilevel surgery
566
Hilde Ploeger (1) presenting Merel-Anne Brehm (1) Sicco Bus (1) Frans Nollet (1)
India, Academic Medical Center, Department of Rehabilitation, University of Amsterdam, Amsterdam (1)
Gait pattern and impairment characteristics in polio survivors with calf muscle weakness

Relation between impairment (IMP) and gait clusters. Thicker lines represent more limbs. PF: plantarflexor, KE: knee-extensor, contr: contracture, K/A: knee and/ or ankle, AA: ankle angle, KA: knee angle, AM: ankle moment (external), DF: dorsiflexion, FL: flexion, EX: extension.
567
Nobuo Nakanishi (1) presenting Hisato Sasaki (1) Shigekazu Ishihara (1) Kosuke Morinaga (1) Sigeru Morinaka (2) Shigeyuki Akiyama (3)
The Netherlands, Hiroshima International University, Higashi-Hiroshima,Hiroshima (1) Japan, Shiyomigishi CO;LTD., Touon,Ehime (2) Japan, Obarakogyo CO;LTD., Setagaya,Tokyo (3)
Develop of usable knee joint for ACL・PCL injure
Some patients with anterior cruciate ligament (ACL) injury complain of pain in the knee while walking and climbing stairs, despite the use of a brace. On investigating the cause of this pain, we found that the pain caused by forward movement of the tibia could be alleviated by shifting the knee joint axis of the brace further forward than the physiological joint axis. Basically, it is regarded as one geared-link mechanism. Therefore, when joint is moved to forward, moment of lower link become increased. (Fig1-a)

Therefore, we manufactured a brace where the knee joint axis can be moved and conducted the experiment.
By shifting the knee joint axis of the brace used by a patient with ACL injury further forward from the physiological joint axis, forward movement of the tibia at the knee belt during knee flexion and tension of the anterior cruciate ligament are suppressed, thereby alleviating knee joint pain.
The subject was experienced partial tear of ACL injury 8 years ago. Changes in pressure were measured in a single gait cycle. The knee joint axis of the brace during these measurements was set at (1) physiological joint axis, (2) 1cm in forward of the physiological joint axis, and (3) 2cm in forward. Pressure was measured at 1.on the tibial tuberosity, 2. about 15cm below of 1., and 3. posterior of trans-femoral (above 6cm from popliteal fossa). The brace was put while sitting position, then belts were adjusted in the standing position. Pressure from belt to body was measured with thin pressure sensor (FSR-402, Interlink Electronics).Sampling rate was 10Hz.
Pressures were compared between 3 variations of brace joint axis (physiological joint, 1cm, 2cm forward). Fig.1 shows the difference at tibial tuberosity. Pressure was increased along with joint location. When brace joint was set at physiological joint, the peak pressure to the body was 662.4g/cm2 at the heel’s initial contact to the floor. Respectionly 670.8g/cm2 at 1cm forward set, and 745.4g/cm2 at 2cm forward.
Also, similar result was observed at integral value of pressure during cycle of walking. (p<0.01) (Fig1-b)
A backward force pulling on the physiological joint axis is applied on the knee joint axis during knee flexion as a result of the adjustment of the knee joint axis so that it is further forward than the physiological joint axis. On generating this force, the belt fastened at the portion of the brace proximal to the lower leg pushes the tibial tuberosity forward. It appears that we were able to suppress tibial movement by applying force from the front.
Hirokawa Shunji :Biomechanics of the knee joint influenced by agonist and antagonist muscle contractions Society of Biomechanisms Japan(SOBIM)Bio mechanism 11,153-165(1992)
568
Deepak Sharan (1) presenting Mathankumar Mohandoss (1) Rameshkumar Ranganathan (1)
Indian, RECOUP Neuromusculoskeletal Rehabilitation Centre, Bangalore, Karnataka (1)
Orthopedic Selective Spasticity Control Surgery for treatment of spastic upper extremity in cerebral palsy
569
Deepak Sharan (1) presenting Mathankumar Mohandoss (1) Rameshkumar Ranganathan (1)
India, RECOUP Neuromusculoskeletal Rehabilitation Centre, Bangalore, Karnataka (1)
Virtual Reality Based Therapy: three different methods and its effect on balance and weight shifting ability of children with cerebral palsy
570
Hong-Wei Hsiao (1) presenting Hsiu-Chen Lin (1) Hung Yen (1) Kaisheng Chang (1)
China, Department of Physical Therapy, China Medical University, Taichung City (1)
Effects on foot pressure during walking using custom-made foot orthosis in patients with hallux valgus
Hallux Valgus (HV) is a common foot condition. It demonstrates valgus deformity at the first ray and causes pain during walking and even affects the activities of daily living. Most patients would firstly seek for conservative treatment (e.g. foot orthosis, toe separator, hallux strap etc.) before surgical intervention. Studies showed foot orthosis could alleviate pain, improve ambulation ability and reduce progression of the deformity. One study showed reduced plantar pressure over the medial forefoot using prefabricated arch support foot orthosis (1). However, there was limited information about the alterations in load distribution wearing custom-made foot orthosis.
The purposes of this study were to investigate the differences of foot pressure during walking between healthy controls and HV patients, and also the effects of using customized-made foot orthosis in HV patients.
Five HV patients (mean age: 20.4±0.6 years; BMI: 20.26±1.98) and four healthy controls (mean age: 21.7±1.25 years; BMI: 20.24±2.28) have been enrolled in this study. The inclusion criteria for HV patients were HV angle between 20~40°, independent walking ability, and no other neuromuscular diseases. The custom-made EVA insole was processed with foam box imprint and plaster mold, following biomechanical principle to correct the force distribution by the reinforcements of (1) forefoot medial wedge, (2) metatarsal pad and (3) medial arch support. After fitting, the foot pressures during walking with barefoot, in standard shoe, and in shoe with insole were recorded by RSscan Footscan® system. Then the patients were asked to wear the insole for at least 2 month, and the same foot pressure testing was performed again for comparison.
The results showed that the HV patients would have larger force distribution at forefoot region compared to the healthy controls. After fitting the custom-made insole, the force distribution under the first toe and metatarsal regions were reduced compared to the barefoot condition immediately. After using the custom-made insole for two months, the center of forces (COF) during walking showed larger variances over the lateral foot region.
This study showed custom-made insole following biomechanical correction principle could reduced the force distribution under the first toe and metatarsal regions, suggesting the remedy effects for the painful symptom and correction of the loading distribution over the medial forefoot region. The trajectories of the COF during walking after wear insole showed larger variances over the lateral foot region, indicating the lateral shift of the loading and further supporting the thepateutic effects.
1. Farzadi, M., et al. “Effect of medial arch support foot orthosis on plantar pressure distribution in females with mild-to-moderate hallux valgus after one month of follow-up.”
571
Erik Prinsen (1,2) presenting Juha Hijmans (3) Daan Brandenbarg (3) Turgay Kahraman (4) Jaap Buurke (1,2) Aline Vrieling (3) Bart Koopman (2) Hans Rietman (1,2)
Taiwan, Roessingh Research and Development, Enschede (1) The Netherlands, University of Twente, Enschede (2) The Netherlands, University Medical Centre Groningen, Groningen (3) The Netherlands, Roessingh, Centre for Rehabilitation, Enschede (4)
Restoration of walking ability in the early stages after transfemoral amputation. Preliminary results of an ongoing trial
Regaining walking ability is challenging for persons who recently underwent a transfemoral amputation. However, scientific literature focusing on how walking ability is regained in the early stages after transfemoral amputation is generally lacking. This is especially the case for the restoration of the gait pattern in terms of kinematic variables. Knowledge of this process is of clinical importance as it may aid in improving rehabilitation programs.
Quantification of the restoration of walking ability in terms of kinematic variables in the early stages after a unilateral transfemoral amputation.
Participants were measured at three moments after amputation: (1) two weeks after the provisional prosthesis is prescribed; (2) two weeks after the definite prosthesis is prescribed; (3) at the end of the outpatient rehabilitation.
There was no intervention on prosthetic prescription and participants received the regular treatment. Measurements included 3-dimensional gait analysis using an opto-electronic 6-camera Vicon system. We used the modified Helen-Hayes marker set, which was placed according to the Vicon lower-body Plug-in-Gait model. Participants completed trials at self-selected walking speed and were allowed to use a walking aid if needed. A minimum of 10 strides were analyzed and averaged.
Three participants completed the first two measurements. The age of the participants were 68, 70, and 73. Reason for amputation were vascular (n=2) and infection (n=1). At the time of the first measurement the time since amputation was 7 (n=2) and 12 (n=1) weeks. The prescribed prosthesis with which the second measurement was completed were Total Knee (n=2) and 3R93 (n=1). The time in between measurements was three weeks for all participants.
Walking speed in both measurements increased from 0.15 to 0.23 m/s, from 0.14 to 0.34 m/s and from 0.13 to 0.49 m/s.
During the first measurement, there is very limited movement in the hip, knee, and ankle joint of the prosthetic leg. In contrast, the intact leg show increased but almost fixed hip and knee flexion, and ankle dorsal flexion in stance phase. During the second measurement, movement of the prosthetic leg comparable to the first measurement, while the movement of the joints of the intact leg show much more similarities to the movement patterns of persons without an amputation.
These preliminary data indicate that there might be a substantial restoration of walking function in the first weeks after (provisional) prosthetic prescription. This was most evidently reflected in the increase in walking speed. In addition, the preliminary kinematic data showed remarkable differences, which may partly be explained by differences in walking speed. More data will be collected to see whether these preliminary statements can be validated.
572
Rémi Rebour (1,2) presenting Lisette Arsenault (1,3) Ludovic Delporte (1,3) Françoise Caillet (3) Gilles Rode (1,3) Yves Rossetti (1,4)
The Netherlands, Plateforme « Mouvement et Handicap », HCL, Saint Genis Laval 69230 (1) France, Service de Neurorééducation, Hôpital Pierre Wertheimer, HCL, Bron 69500 (2) France, Pôle de Rééducation et de Réadaptation Fonctionnelles, Hôpital Henry, Saint Genis Laval 69230 (3) France, ImpAct, Centre de Recherche en Neurosciences de Lyon, Inserm, CNRS, Bron 69500 (4)
Short term therapeutic effect of a peroneal nerve Functional Electrical Stimulation (FES) orthosis on gait kinematics of patients with footdrop
FES orthosis elicits a muscular contraction by a peroneal nerve stimulation to produce a functional movement of ankle dorsiflexion. Its orthotic effect has been well documented. Several scientific studies show its therapeutic effect on gait performance on patients with foot drop ([1], [2]). These studies were designed to compare gait parameters without wearing FES before and after long term training (from 3 to 12 months).
Quantify the therapeutic effect of FES orthosis on distal kinematics of patients with foot drop, after a short term training (1 month), using a motion capture system.
4 patients with foot drop (more than 1 year post stroke or with Multiple Sclerosis) were fitted with FES orthosis (Walkaide®) undergoing a one month training program (FES used on a daily basis for walking). Two clinical assessments and two gait motion captures were performed without orthosis, at pretest and after one month of use.
Gait speed, ankle angle at initial contact, peak of dorsiflexion at swing phase, peak of plantar flexion and maximum ankle range of motion at third rocker were computed.
Our following analysis used paired Student tests, between the pre and the post training values. Significance threshold was set for p values lower than 0.05.
After the month of training, all patients were satisfied of the FES orthosis and found their gait improved even with the FES off. Clinical exams showed an improvement of active dorsiflexion. Between the first and the second gait analysis, the walking speed significantly increased (mean differences: 0.07m/s, t(3)=6.56, p=0.007). The peak of ankle dorsiflexion at swing phase was increased (mean differences: 3.50°, t(3)=3.12°, p=0.05), whereas the peak of dorsiflexion at initial contact only showed a trend towards normalization. All the other gait kinematic parameters were not significantly modified.
The improvements in walking speed are as reported in literature. The increased peak of dorsiflexion at swing phase, facilitating foot clearance, is probably induced by increased in dorsiflexion muscles strength, and the strengthening of residual neural connections as reported by Everaert et al. [3]. Considering the therapeutic effect obtained on such a short term use, it might be relevant to consider using FES as a therapeutic tool, as mentioned in the literature [4].
[1] Laufer Y. et al. ; 2009 J Neurol Phys Ther
[2] Stein R. B. et al. ; 1997 Artif Organs
[3] Everaert D. G. et al. ; 2010 Neurorehabil Neural Repair
[4] Israel S. et al. ; 2011 Top Stroke Rehabil
573
Tuna Orhanli (1) presenting Atila Yilmaz (1)
France, Hacettepe University, Electrical and Electronics Engineering, Ankara (1)
Implementing Phase and Velocity Estimation for Finite State Based Control of Pneumatic Above Knee Prosthesis

a) Determined knee angles, b) Automatically adjusted motor positions
574
Akihiko Hanafusa (1) presenting Noriyasu Maruyama (2) Tomozumi Ikeda (2) Tsuyoshi Nakayama (3)
Turkey, Shibaura Institute of Technology, Saitama, Saitama (1) Japan, Polytechnic University, Kodaira, Tokyo (2) Japan, Research Institute, National Rehabilitation Center for Persons with Disabilities, Tokorozawa, Saitama (3)
Dynamic Finite Element Analysis of Different Width Ankle Foot Orthoses that is Incorporated with Human Lower Leg Model
It is important to adjust the shape of plastic shoehorn-type ankle foot orthoses (AFOs) to improve the gait of the individual patients. By changing the width of ankle part, bending stiffness of AFO that affects the gait can be altered. In general, those adjustments are done by prosthetist by trial and error using their knowledge and experience. However, it is advisable if the effect is able to be assessed before fabrication.
The aim of the study is to simulate deformation of AFOs whose width of ankle part is changed, because deformation and contact on the AFO with the lower leg affect gait.
The finite element (FE) model of the human right lower leg is composed with 6,650 elements, including bones, muscles, and fat models. Material properties as described in the literature1) were assigned to the model. The ankle joint and 5 MP joints were defined as rotatable joints. Two wide and narrow types of AFO FE models including belts whose ankle part width were 0.5 and 0.4 times of circumference were composed. The same weight as a subject was loaded onto the bone model at the center of gravity of the human body, and the motion and deformation from the moment of heel contact until the heel-off position were simulated using the dynamic FE analysis program LS-DYNA (LSTC Corp.).
Two types of orthosis with strain gauge sensors were manufactured and gait experiments were performed. The composed lower leg model including bones and time variation of simulation results are shown in the figure. The lower leg model, the AFO and its belt were in contact with each other, and a movement was similar to the human gait. The time variation of simulated strain was also similar to that of measured except after heel-off phase and strain was larger in narrow type orthosis.

Simulated human model and comparison of time variation of strain
The results indicate the qualitative validity of the dynamic FEM for analyzing an AFO by using a human lower leg model and the usability for adjusting the shape of AFO. Still, the difference of strain distribution between simulation and measurement exists as for the peak value and their position and further improvement of the simulation model and their conditions are necessary.
1) R.E. Tannous et al. “A Three-Dimensional Finite Element Model of the Human Ankle: Development and Preliminary Application to Axial Impulse Loading,” Proc. of Stapp Car Crash Conf., Vol.40, pp.219-238, 1996.
575
Nicky Seymour (1) presenting
Japan, STELLENBOSCH UNIVERSITY, Cape Town (1)
The role of community-based rehabilitation (CBR) in effective wheelchair service provision
SMETs from 2013 and 2014 were reviewed and results compared with the WHO Wheelchair Guidelines to determine if weaknesses existed in areas where CBR organizations and/or workers could have a role to play.
The results showed that collaborations between wheelchair services and CBR organisations are either absent or ineffective. However, for service provision to be in line with best practice and to meet the needs of both the WHO Guidelines and, importantly, wheelchair users themselves, there needs to be a focus on strengthening this.
1.‘Guidelines on the Provision of Manual Wheelchairs in Less-Resourced Settings’, WHO 2008
576
Lena Quisth (1) presenting Inge Beuschau (1) Ane Simony (2)
South Africa, Ortos, Odense (1) Denmark, Sector for spine surgery and research, Middelfart Hospital, Middelfart (2)
Initial experience with the Providence Nighttime Bracing in adolescent idiopathic scoliosis
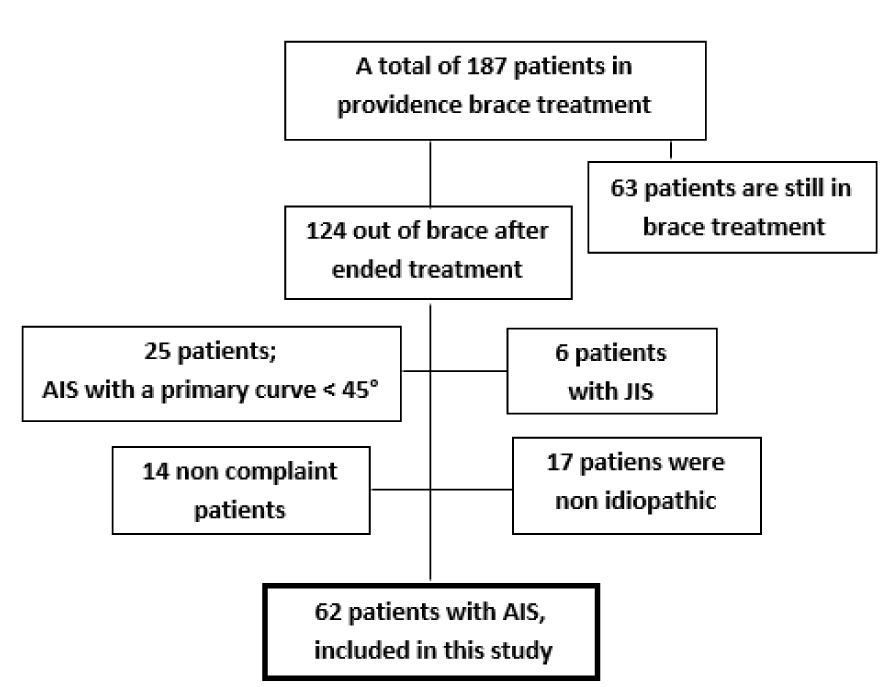
577
WAI CHIU CHOI (1) presenting
Denmark, The Chinese University of Hong Kong, Hong Kong (1)
Effects of Footstrike on the Loading and Heart Rate in a Group of Top Amputee Runners with Running-Specific Prosthesis in Hong Kong
Running-Specific Prosthesis (RSP) facilitates amputee run faster and longer. There are more and more amputee participating in long distance running race. Greater loading on intact limb of amputee runner while running put the intact limb under higher risk of injury like osteoarthritis knee and tibial stress fracture. Forefoot strike is a running strategy to minimize loading for normal subject. It is unknown if forefoot strike can also reduce loading on intact limb for amputee. Also energy cost may be affected by altering the footstrike in running.
The aim of this study is to investigate the effect of forefoot strike and rearfoot strike on the loading and heart rate of a group of top Hong Kong amputee runners while running with RSP.
It is case study design, repeated measures. Five unilateral amputee runners with different amputation levels will be invited. They will run in a comfortable speed on a Zebris treadmill with force sensors. Polar watch will be used for heart rate monitoring. The plantar force, temporal parameter and heart rate will be recorded when amputee run in forefoot strike and rearfoot strike condition. The variable will be compared between the different footstrike conditions. Heart rate will be used for estimating the running energy cost.
Result is pending and it will be completed in March 2015. It is hypothesized that forefoot strike will decrease the loading on intact limb of amputee runner and will increase their heart rate and energy cost is estimated to increase.
Pending
0580
Nadine Stech (1) presenting David Moser (1) Andy Sykes (1) Joe McCarthy (1) Alan McDougall (1) Saeed Zahedi (1)
The Philippines, Endolite Technology Centre, Basingstoke (1)
Ramp Descent Ambulation using Different Control Strategies with an Integrated Transfemoral Prosthesis
Ramp ambulation has not been considered to a great extent in transfemoral amputee gait studies. Although it is known that gait is influenced to a high degree by the surface inclination (Lay et al., 2006).This study investigated the effects of different joint braking strategies using an integrated transfemoral knee-ankle prosthesis. Non-amputee studies have shown a negative net energy for ramp descent (Schwameder et al., 2001). It was expected that incorporating a combined knee-ankle brake strategy would be beneficial.
Different braking scenarios for ramp descent ambulation were considered to gain a deeper understanding in the under lying biomechanics. The aim was to quantify the biomechanical effects of different control strategies.
Four transfemoral K3 amputees participated in the study. Signed consent was given. The integrated prosthesis consisted of a microprocessor controlled hybrid knee joint and a microprocessor controlled hydraulic ankle. Overall limb control was coordinated by a single controller. Changes in the braking strategy were done wirelessly and the same alignment was used during the whole data collection session.
Four braking strategies were measured: a) no braking action, b) braking action of the ankle, c) braking action of the knee, d) braking action of the whole limb.
Kinetic and kinematic data was collected using a Codamotion Gait Analysis System and a Kistler force plate on a 5° ramp at self-selected normal speed.
Additionally subjective feedback from the participant and the prosthetist was collected.
Ground reaction forces were clearly influenced; especially the peak value, timing and quantity of the braking impulse.
The ankle showed its influence from early-mid stance on the anterior-posterior ground reaction force and the ankle moment in sagittal plane, whereas the knee provided braking influence in mid/late stance.
Most participants described the ramp descent ambulation with the limb brake as beneficial. They perceived to have more control over their gait. Temporal spatial stride data also showed a reduced self-selected speed which was lowest using the complete limb brake. When the limb brake effect was reduced there was a tendency for amputees to accelerate during ramp descent suggesting less controlled stepwise momentum. All subject responses seemed to correlate perceived improvements in function with lower gait speeds.
We conclude that the control of walking speed on ramps can be markedly influenced by dynamically altering stance phase damping settings at both the ankle and knee. In our preliminary study the participants when walking down ramps perceived the braking action of both the knee and ankle during ramp descent as most beneficial.
A larger and more detailed follow-up study is required to investigate effects of the integrated limb brake on different speeds and different gradients.
LAY, A. N. et al. 2006. Journal of Biomechanics, 39, 1621-1628.
SCHWAMEDER, H., et al. 2001. SPECTRUM Suppl., 98-105.
0581
Kristjan Finnsson (1) presenting
UK, Össur, Reykjavik (1)
Activity monitoring and data collecting for Össur Bionic Prosthetics
Physical inactivity is the fourth leading cause of death (1). Within amputees physical activity can improve psychological, social and physical status (2) and individuals with limb amputations appear to benefit both physically and psychologically from participation in sports and/or regular physical activity as found in a comprehensive review (3) and shows an increase in enrichment of social contacts and attitude.
By collecting information about the mobility of a user, analysing it and presenting it back to the user in a motivational manner we will encourage the user to be more mobile thus helping with the healing process and improve psychological, social and physical status
The Össur RheoKnee sends data via Bluetooth Low energy to a mobile device, iPhone/Android Phone. The mobile device processes the data, logs it and presents the user with motivational representation of it. The mobile device can also relay the data onward to a Össur cloud based data central where data can be processed
Through the data collected we can determine the current level of mobility and evaluate gait parameters. In real time the user can be motivated with the app and data can be shared with a doctor or trainer to monitor the progress. By collecting data we can compare mobility and gait information of a larger user population.
By displaying data to the individual patients the user improves awareness about his status of physical activity
Giving remote access to mobility and gait data makes it possible for doctors and trainers to keep track of day to day progress of a patient.
1. Lee, I-Min, et al. “Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy.” The Lancet 380.9838 (2012): 219-229.
2. Deans, Sarah A., Angus K. McFadyen, and Philip J. Rowe. “Physical activity and quality of life: A study of a lower-limb amputee population.” Prosthetics and orthotics international 32.2 (2008): 186-200.
3. Bragaru, Mihail, et al. “Amputees and sports.” Sports Medicine 41.9 (2011): 721-740.
0582
Trevor Law (1) Tim Bryant (1,2) presenting Stacey Hildebrand (1) Greg Esau (1) Heinz Trebbin (3)
Iceland, Queen’s University, Kingston, ON (1) Canada, Kingston General Hospital, Kingston, ON (2) Canada, DOI ortho-innovativ GmbH, Kempten (3)
Effect of Structural Modifications on Mechanical Properties of a Novel Prosthetic Foot Keel
The objectives of this study were to: (1) Determine the range of mechanical performance that could be achieved using the design approach of a modifiable keel, and (2) Identify how keel modification protocols relate to mechanical performance changes.
Sample devices (Niagara Foot™ Model 2, Version 21; Niagara Prosthetics and Orthotics International, St. Catharines, Canada) were obtained from the manufacturer. The single piece flexible keel (DuPont™ Hytrel™) is comprised of heel, toe, and C-spring elastic features that can be modified by the removal of layers of material (Figure 1a). Seven keel conditions were studied that spanned the permutations of the modifications possible at each of the features. Each keel was tested in an Instron™ 5500 compression testing machine in which loads of 1200N were applied at a rate of 200N/s to the heel and toe at angles of 15deg. and 20deg. respectively. Resulting force-displacement curves were analyzed to determine the defection, stiffness, and energy stored at peak force; stiffness was determined by the slope of the force-displacement curve at the peak force and energy by the computing the area under the loading curve.

Displacements, stiffnesses, and energy storage for the test conditions at peak load are indicated in Figure 1b.
Each modification produced a unique combination of mechanical properties, indicated by the points in the Energy-Stiffness and Energy-Deflection graphs. Heel deflection ranged from 3-9 mm; toe deflection 23-45 mm; heel stiffness 350-580 kN/m;, toe stiffness 70-100 kN/m; heel energy 1-4 J; and toe energy 11-14 J.
0583
Kardem Soyer (1) presenting Nilgün Bek (1)
Germany, Health Institution, Ankara (1)
The effects of shoulder retraction harness orthosis on perception of pain, quality of life and depression
Factors like postural disturbance related to working position, breast size and decreased body awareness may give rise to reduction in muscular structure of upper back which may result with postural kyphosis. Any damage to joints, muscles and connective tissues may lead to an abnormal posture causing symptoms such as pain. Vicious circle may be formed within chronic pain, quality of life and emotional tides.
The aim of this study is to investigate the effect of basic shoulder retraction harness orthosis which is used for maintaining postural feedback on perception of pain, quality of life and depression.
Fifteen women, aged between 18-45 who had a normal body mass index between 16 and 29.9 kg/cm2, were recruited. The volunteers were subjected to the assessment protocol which included demographic data. Pain assessment was done with McGill Pain Questionnaire, quality of life with SF-36 and depression with Beck Depression Inventory. The treatment protocol included retracting their shoulder with retraction harness orthosis for maintaining postural correction for 6 weeks. After 6 weeks the volunteers were subjected to the same assessment protocol. SPSS 21and Paired-Samples T Test was performed to compare before and after treatment protocol data. The level of significance was set at p < 0.05.
The mean of demographic data of patients were, age (31.33±0.33 years), body mass index (22.79±3.30 kg/m2). There was statistically significant difference between the pre and post-intervention mean values of tender pain and frequency, respectively (p=0.001, p=0.001) (p<0.05). There was significant difference between the before and after mean values in SF-36 Health Survey (p<0.05) (Table 1). There was no statistically significant difference between before and after mean values of Beck Depression Inventory (p>0.05).
Results of comparison of pre and post intervention values of subscale of SF- 36 Health Survey.

: p<0.05
It was possible to confirm a statistically significant association between retraction of the shoulder, pain and quality of life. Retraction band is useful and aesthetic but in literature there is limited knowledge about the effects of retraction harness. In the present study there was statistically significance between retraction of the shoulder with retraction band and pain and quality of life in women.
0584
Charla Howard (1) presenting Chris Wallace (1) Dobrivoje Stokic (0)
Turkey, Methodist Rehabilitation Center, Jackson, MS (1)
Mechanical Knee Users Improve Motor Function with Rheo3 Knee: Single-Subject Design
Justifications for prescribing advanced prosthetic components are becoming more stringent. Thus, the benefits of advance components, such as microprocessor knees (MPK), should be more systematically evaluated for evidence of functional improvement over less expensive mechanical components.
To evaluate the impact of MPK (RheoKnee® 3) in long-term mechanical knee users based on standard clinical measures, user preferences, and objective gait parameters.
Subjects: Seven mechanical knee users (6 K3, 1 K2) novice to MPK.
Study Design: ABA (n=3) or BAB (n=4) design was used (A-mechanical knee, B-MPK, 4 weeks each), preceded by a baseline evaluation and with a 2-week transition period between phases (14-16 weeks total).
Protocol: Berg Balance Scale (BBS), Amputee Mobility Predictor (AMP), 6-minute walking distance with pre-post heart rate to derive physiological cost index (PCI) were administered at baseline and the end of each phase. Knee preference was assessed using a visual analog scale at the end of each phase after wearing MPK. Temporo-spatial footfall data were collected at each weekly session by an electronic walkway (Zeno®, length 6m) while subjects walked at normal and very fast self-selected speeds (
While using MPK, the majority of subjects increased BBS (6/7), AMP (5/7), K-level (4/7), and 6-minute walk distance (6/7) and decreased PCI (5/7). All but one subject expressed strong preference toward MPK, both overall and for specific activities (walking in narrow spaces, uphill). Although a few subjects increased normal self-selected speed on MPK (3/7), all increased very fast speed (7/7). The median changes are reported in the table.

Clinical measures of balance, mobility, and endurance improved while using MPK. Those with a lower baseline BBS and AMP scores showed the greatest improvement, whereas limited improvement in subjects with higher baseline scores could be due to ceiling effect of these measures. An increase in AMP score allowed 3 K3 subjects to cross the K4 threshold, but more importantly the only K2 subject moved from low K2 to K3 level. A consistent increase in fast walking speed on MPK suggests improved neurocontrol of gait and/or higher confidence during walking. Improvements on the 6-minute walk and PCI show increased endurance while walking with the MPK. These objective clinical results substantiate strong preference toward MPK and anecdotal reports of better daily functioning. The single-subject design proved useful for objectively demonstrating individual benefits of MPK.
0585
Joshua Young (1,2) presenting Simon Lalor (1,2)
USA, St George’s Healthcare NHS Trust, London (1) UK, Opcare, Oxford (2)
A comparative review of prosthetic and orthotic care pathways for the management of partial foot amputation in a single centre
People who undergo a partial foot amputation, or have a congenital absence of part of the foot, will frequently become long term users of either prosthetic or orthotic devices. These devices aim to restore walking function, or to prevent further complications such as ulceration. Prosthetic and orthotic management of partial foot amputation can be challenging and a wide variety of approaches may be used.
This study aimed to define and compare current prosthetic and orthotic care pathways for the management of partial foot amputation in a multidisciplinary rehabilitation centre.
New and existing partial foot amputees were identified by searching the clinical software system and surveying prosthetists and orthotists at the centre. To be included subjects needed to have at least one metatarsal head absent through acquired amputation or congenital absence. Adults and children were included. Clinical notes for identified subjects were reviewed. Data was collected between October 2013 and April 2014.
In total 31 subjects (34 amputations) were identified. Various aspects of the care pathway are different when comparing prosthetics and orthotics, including use of and access to x-rays, patient diagnoses, amputation level and cause, treatment, treatment cost, reviews and outcome measures. Most more proximal partial foot amputations were treated in prosthetics while most more distal amputations were treated in orthotics. Radiographs were accessible to most orthotists while no prosthetists reported access to imaging reports. The most common prescription in prosthetics was a silicone prosthesis while the most common prescription in orthotics was therapeutic footwear and foot orthoses, often combined with a carbon ankle foot orthosis. Reviews and outcome measures were performed less often in prosthetics.
Little is known about current prosthetic and orthotic care pathways for the management of partial foot amputation in the UK. Defining current care has enabled this centre to make centre specific recommendations for improvement. The cause of much of the variation between prosthetic and orthotic pathways is unclear and could be related to differences in the patient groups, professional differences or other factors.
0586
Philip Jefferies (1) presenting Pamela Gallagher (1) Mark Philbin (1) Malcolm MacLachlan (2)
UK, Dublin City University, Dublin (1) Ireland, Trinity College Dublin, Dublin (2)
Being ‘just normal’: A new theory of prosthesis use
The psychosocial aspects of prosthesis use have become a focus for research in recent years, including explorations of adjusting to an artificial limb and quality of life following fitting (Sinha et al., 2014). Theory is now needed to help understand divergent outcomes in research as well as to provide useful perspectives and recommendations for practice (Dunn et al., 2008). This research sought to develop theory grounded in the experiences of prosthesis users in order to support further inquiry and the development of evidence-based practice.
The aim of this project was to develop theory capturing the varied ways through which a main concern of prosthesis users is processed and resolved.
Data from participants that used upper and/or lower-limb prostheses (n=24) were collected using an in-depth and flexible interviewing style. Data were also collected via internet forums, weblogs and autobiographical texts. These were systematically analysed in accordance with the established procedures of Grounded Theory methodology (Glaser et al., 1967; Glaser 1978, 1998) in order to determine a main concern of prosthesis users and to establish the ways this concern is resolved. Through adherence to the constant comparison process of analysing incidents within the data, patterns were identified and conceptualised, and variations within these were explored. These patterns of concern-resolution formed the present theory.
A main concern of being ‘just normal’ emerged through analyses. ‘Just normal’ is the condition of prosthesis users being and living in ways that they perceive are variously ‘about right’; that are sufficient, fair, and generally how things ‘ought to be’ for them, as they see it. Three modes of resolving this concern were identified: (1) ‘preserving’ being just normal, where persons manage threats to their ability to be this way, such as threats to their ongoing use of a prosthesis; (2) ‘redressing’ to just normal, such as persons seeking or petitioning for a limb that is ‘good enough’; and (3) ‘persevering’ with just normal, accounting for how prosthesis users keep going with living just normally, despite ‘normal’ difficulties that may accompany this, such as particular issues in the use of a limb.
The theory provides a novel understanding of what compels prosthesis users to act in particular ways and elucidates the benefits and challenges of living with artificial limbs, as persons make efforts to live in ways they see as fitting with what they consider is ‘just normal’ for them. Such an understanding has the potential to facilitate appropriate fitting of prostheses and to inform goal-setting in rehabilitation. It also has the transferrable potential to related areas of living with assistive technologies, the experience of disability more broadly, and beyond.
Dunn, D.S., et al. (2008). The place and promise of theory in rehabilitation psychology research. Rehabil. Psychol.
Glaser, B., et al. (1967). The discovery of Grounded Theory: Strategies for qualitative inquiry. Aldine.
Glaser, B. (1998). Doing Grounded Theory: Issues and discussions. Sociology Press.
0587
Yanga Sibidla (1) presenting
Ireland, PE Provincial Hospital, Eastern Cape (1)
Prevalence of peripheral neuropathy on the contralateral limb of unilateral diabetic amputees
Sensory and motor defects are known to contribute to incidence of foot ulceration which increases the risk of amputation. It is suspected that the contralateral limb on diabetic mellitus (DM) patients after unilateral amputation are at risk of peripheral neuropathy (PN) but there is little knowledge on the extent of the problem, and hence a study in gaining an understanding in determining the extent in which the contralateral limb is exposed to this risk is of vital importance.
This study will determine the prevalence of PN in the contralateral limb and it will also look at demographic characteristics of the study population such as patient’s life style, sex and age to assess whether any of these have any influence on the peripheral neuropathy on the contralateral limb of the subjects to be included in this study and also look on whether patients were educated on appropriate foot wear for diabetic patients.
This is a clinical cross sectional study of first time unilateral diabetic amputees who were amputated in KCMC between November 2009 and January 2010, only diabetic unilateral subjects with no other major medical conditions were part of the study. Subjects that were amputated due to trauma, tumors and other medical condition that were amputated during this same period were not included on the study. The number of patients that took part on the study is 32
Mean (±SD) overall peripheral neuropathy score was 1±0.3 indicating mild peripheral neuropathy to majority of patients. Average overall PN showed that slightly more than ninety percent (90.6%) scored Grade 1, 2 (6.3%) Grade 0 and only one Grade 2.There was no statistical significant relationship found between the medication used and life style of the respondents.
Peripheral neuropathy does exist on the contralateral limb of diabetic patient unilateral amputees. Majority of patients loose the protective sensation and this puts them on risk of pressure sores which could lead to amputation of the contralateral limb. There is no patient education on the appropriate foot wear and limb care in our set ups.
0588
TAE SOO BAE (1) HAN WOOL SEO (1) presenting DAE DONG KIM (1) Cheol Woong Ko (3) Hyung Tae Kim (3) Joon Hmm Lee (2)
South Africa, Jungwon University, Goesan-gun, Chungcheongbuk-do (1) Republic of Korea, OX korea, CheonAn, Chungcheongnam-do (2) Republic of Korea, Korean Institute of Industrial Technology(KITECH), CheonAn, Chungcheongnam-do (3)
Structural Stability Analysis of Adjustable Connector Types in Electric Handbikes
Wheelchair users are participating in more frequent outdoor activities, and the demand for aids to retain their mobility is emerging as a significant social issue. Several handbikes are recently being developed to ensure the free and active mobility. Installation-type handbike can easily be converted into motorized wheelchairs when required by their users, and they have the advantage of adjustability according to the size of the manual wheelchair.
The purpose of this study was to compare the structural stability according to connector types in the area that connects the wheelchair and the motorized aid, based on a static and dynamic stability tests.
We selected a snatch lock, a slide latch, and a fastener that are not easily loosened, have simple combining methods, and have strong fixation power. The design of an overall model was performed using Solidworks and commercial models were used for the connectors. By referring to durability test for electric wheelchair based on ISO 7176, loading condition for static and dynamic analyses were set based on a human with a weight of 70 kg. Simulations were performed using finite element method(ANSYS) for the static analysis and Multi-Flexible Body Dynamics(Recurdyn) for the dynamic analysis.

The static analysis was conducted on the three types of connectors and their joints under static loads. As a result, the maximum stress for all types of connectors was lower than the yield stress of the connectors’ materials (552 MPa). The stress in the each frame, the motor’s adjustable area, and the upper latch when using the snatch lock were lower than when using the other connectors.
In addition, a multi-flexible body dynamic analysis in the joint of each connector was performed for durability test of electric wheelchair. The maximum stress was 216 MPa in the snatch lock, 575 MPa in the slide latch, and 1443 MPa in the fastener. Therefore, the snatch lock showed the lowest von Mises stress among the three types of connectors.
This study aimed to analyze the static and dynamic structural stability and the results after comparing their stress values showed that the use of the snatch lock resulted in the lowest stress Therefore, the use of snatch locks is considered most efficient. This study may become the basic data for selecting the most efficient connector for the production of actual handbikes.
0589
Musa Zia (1) presenting
Republic of Korea, Ministry of Public Health, Kabul (1)
Quality of life of women with lower limb disabilities using prosthetics or orthotics devices in Kabul, Afghanistan
In present study conducted in Kabul, Afghanistan women with lower limb disabilities using orthotics or prosthetics devices were compared to no disable women. The main aim of this study was to examine and compare the quality of life score of two groups of women with lower limb disabilities and compare non disable women. In developing and post conflict countries women are suffer from triple discrimination due to their disabilities, gender and socio-economical position in society. Therefore it’s assumed women are having lower quality of life.
The main aim of this study was to examine and compare the quality of life score of two groups of women with lower limb disabilities using prosthetics/ orthotics devices and compare non disable women.
Socio-demographic data was collected from 211 participants and WHOQOL-BREF was used to measure the quality of life of disable and no disable women in four domains, physical, psychological, social relationship and environment.
Statistically differences (p>0.05) were found in the means score of the four domains between the two groups of participant of the study. The physical health and social relationship domain significantly higher in no disable women compared to disable women. In the socio-demographic factors differences were found.
Quality of Life is determined to be low when living with physical disability. Marriage and life with children have a greater impact on the quality of life of women with disabilities. For full integration and participation in the society higher education help to improve the quality of life and their status. Satisfaction from the devices was high and to increase the daily uses of the appliances by women it is required to consider the environmental factors and women needs into account during the designing and fabrication of devices.
It was found that prosthetics and orthotics devices provide opportunity to earn income which affects the quality of life women with disabilities. Also socio-demographic variables play a significant role in determining the Quality of Life- education, income, and children affect domains scores.
0590
Felix Starker (1) presenting Florian Blab (1) Florian Dennerlein (1) Urs Schneider (1)
Afghanistan, Fraunhofer IPA, Stuttgart (1)
Simulation of ramp and stair walking with a prosthetic foot test machine
Prosthetic feet are complex designed lightweight series of spring elements with a determined flexibility and durability. Therefore several endurance tests are developed within the last decade (ISO 10328; ISO 22675). New standards and methods for mechanical characterization of prosthetic feet are in development (AOPA 2010; ISO/TC 168 2014). Neither of these takes into account that everyday walking is not only limited to level walking but also contains stairs and ramps.
Aim of this study is to investigate the feasibility of a dynamic prosthetic foot test machine to perform beside standardized dynamic level gait, stair and ramp gait profiles.
Initial data was captured with one subject (m, 31 y, 75 kg, cat 4, TT amputee) in a motion lab walking a predefined course containing a forceplate instrumented level, ramp (12%) and stairs parcours (AMTI AccuGait) at self- selected walking speed with the shoed daily used prosthetic foot (Össur Vari Flex, 27 cat 3) recorded with a motion capture system (Qualisys, 9 cameras).
The data was processed (Matlab 2014b) and edited to be transmitted on the prosthetic foot test machine (Shore Western, KS-07).
The test machine successfully simulated individual user data of stair up- and down, ramp (12 %) up- and down as well as level walking. Captured data needed to be filtered and fit by a polynom 11th order to lead to a smooth automatic adaptation to the force levels by the test machine (example data for downstairs walking see figure below).

With help of the prosthetic foot test machine different gait situations were simulated. Force and moment data was recorded above the prosthetic foot. This method is useful for design decisions of prosthetic feet and helps to broaden the functional understanding. Further research needs to deal with generation of standardized input data for stairs and ramp profiles especially with respect to user activity groups for comparable results.
ISO 10328, 2004: ISO 10328. Prothetik. Prüfung der Struktur von Prothesen der unteren Gliedmaßen. Anforderungen und Prüfverfahren. ISO/DIS 10328.ISO 22675, 2007: ISO 22675. Prothetik - Prüfung von Knöchel-Fuß-Passteilen und Fußeinheiten.AOPA (2010): AOPA’S PROSTHETIC Foot Project. What It Is, What It Is Not, and What Patient Care Facility Providers/Practitioners Need to Know…, zuletzt geprüft am 27.11.2014.ISO/TC 168 (2014): ISO/DIS 16955.2 - Prosthetics – Quantification of physical parameters of ankle foot devices and foot units. Hg. v. DIN.
0591
Kristleifur Kristjansson (1) Thorvaldur Ingvarsson (1) Magnus Oddsson (1) presenting Melissa Evangelista (2) Morten Hansen (2)
Germany, Ossur, Reykjavik (1) Iceland, Alfred Mann Foundation, Valencia (2)
Mind control for leg prosthesis. Is it useful?
Microprocessor controlled prosthetics have been available for more than a decade. Direct control through surface myoelectric sensing is conventional technology for upper extremity prosthetics. Electromechanical sensors and logic processes are primarily used for lower extremity control. Difficulties of acquiring consistent bio signals that the microprocessor control system can properly interpret human intent may be one of the reasons why direct control has not proven to be commercially successful so far for lower extremity. By using wireless intramuscular myoelectric electrodes the greatest obstacle of inconsistent signal quality can be avoided.
The study describes how quality myoelectric signals can be used to supplement existing microprocessor control with information directly from the patient and how it vastly expands the possibilities of control.
Two subjects, one transfemoral amputee and one transtibial amputee were implanted with two electrodes each into non intact muscles of the residual limb. The transfemoral subject received one sensor in vastus lateralis and another in biceps feomoris. The transtibial subject received one sensor in gastrocnemius and the other in tibialis anterior. A coil built into the prosthetic socket was used to deliver power to the sensors through electromagnetic induction. A secondary function of the coil is to act as an antenna to receive data from the sensors representing myoelectric activity.
The data from the sensors is processed parallel to the information generated by the conventional sensors and then used to control the actuation of the prosthesis.
After a healing period post implantation the subjects performed a series of tasks controlling the prosthesis using the myoelectric sensors. The tasks were designed to provide data where the response and accuracy of the control system could be evaluated. Both subjects performed the series of tasks successfully despite very short learning period. Signals from the transfemoral subject showed that during level ground walking there is measureable muscle activity pattern that can be used to trigger events driving a state machine for prosthetic control, resulting in a more precise and intuitive control. Similar signals were not observed from the transtibial subject although the myoelectric signals proved to be useful performing cognitive actuation tasks adjusting a motorized prosthetic ankle. The subjects also used the myoelectric control system in real life situations and it proved to a positive improvement over the previous control.
Implanted myoelectric electrodes for prosthetic control proved to be an improvement over a state of the art lower extremity control system. Subjects claim that the system is more responsive and consistent than their previous prosthesis. The direct capture of user intent for the control may lead to simplification of control algorithms while vastly expanding the range of tasks that can be performed with the prosthesis.
0592
Richard Lombard Vance (1) presenting Pamela Gallagher (1) Fiadhnait O’Keeffe (2) Deirdre Desmond (3) Robert Coen (4) Nicola Ryall (2)
USA, Dublin City University, Dublin (1) Ireland, National Rehabilitation Hospital, Dún Laoghaire (2) Ireland, Maynooth University, Maynooth (3) Ireland, St James’s Hospital, Dublin (4)
The Impact of Cognition on Physical and Psychosocial Outcomes at Discharge from a Lower Limb Prosthetic Rehabilitation Programme
The majority of lower limb amputations in industrialized countries are of vascular or diabetic etiology; both have been linked to cognitive impairment. Cognition has been linked to prosthetic rehabilitation outcomes such as mobility and prosthesis use (O’Neill & Evans, 2009). Comprehensive neuropsychological assessment could facilitate understanding the impact of cognition on physical and psychosocial rehabilitation outcomes at discharge from rehabilitation.
To determine the effects of impaired cognitive functions on physical and psychosocial outcomes collected at discharge from rehabilitation.
Comprehensive neuropsychological assessment of memory, attention, executive function, visuospatial cognition, and language was undertaken at admission to an LLA rehabilitation programme at a national rehabilitation hospital. Physical and psychosocial rehabilitation outcome data was collected at discharge. Outcome measures included SIGAM Mobility Grades (SIGAM), Trinity Amputation and Prosthesis Experience Scales (TAPES), WHO Disability Assessment Schedule 2 (WHODAS) and Hopkins Rehabilitation Engagement Rating Scale (HRERS). Data analysis investigated the relationship between cognitive tests and physical and psychosocial rehabilitation outcomes.
Data from T1 are presented here. 3.5% (SIGAM grade A) and 12.9% (grade B) of people wore their prosthetic limbs for cosmetic or therapeutic reasons only, respectively. 24.7% achieved SIGAM grade C (walking <50 metres), 54.1% grade D (>50m, outdoors, level ground), and 4.8% grades E or F (independent of walking aids, except occasionally or normal gait). WHODAS scores ranged from 0 to 89.6 (mean=58). Mean TAPES scores for general, social, and limitation adjustment were 2.9, 3.2, and 3.0 respectively. Mean TAPES aesthetic, and functional satisfaction scores were 3.3 and and 4.6 respectively. The mean HRERS score was 27.8 (SD=2.63). Impaired general cognition (RBANS total) was related to poorer mobility (SIGAM) and rehabilitation engagement (HRERS) (p<.05). Impaired executive function (DKEFS colour-word switching) was related to poorer adjustment to limitation (TAPES) (p<.05).
Variation in physical and psychosocial outcomes was seen in this sample. This was evidenced, e.g. by wide variation in self-reported disability (WHODAS), and in mobility, with 16.4% of people using prostheses for cosmetic or therapeutic reasons only. Mean adjustment, prosthesis satisfaction, and rehabilitation engagement levels were relatively high. Impaired cognition was linked with rehabilitation outcomes, such as poorer mobility, and adjustment to amputation. Knowledge of the impact of cognition on rehabilitation outcomes will aid the improvement of prosthetic rehabilitation programmes, and ultimately improve the well-being of persons with LLA. Further longitudinal research is on-going to predict role of cognition at 6 and 12 months post discharge.
0593
Felix Starker (1) presenting Florian Blab (1) Florian Dennerlein (1) Urs Schneider (1)
Ireland, Fraunhofer IPA, Stuttgart (1)
A low-cost prosthetic foot based on a leaf spring design
There is a high demand for prosthetic components such as prosthetic feet in developing countries (Arya et al. 2008; Salmond et al. 2010). Current available low-cost products are compared to high priced state of the art prosthetic feet in developed countries inadequate in terms of functionality( Lenka et al. 2010). Reports showed a high gap of these devices between durability (half a year) and energy return (< 50%)(Jensen and Treichl 2007).
A new prosthetic foot is presented that is based on a leaf spring design and with several features to achieve a robust design with high functionality at a low price.
A first prototype is presented that allows easy adaptation to user weight and mobility.
The prototype was tested and refined with a prosthetic foot test machine (ISO22675) to assure safety and functionality. Initial subject data (m, 31 years, 75 kg, TT amputee, cat 4) was recorded to validate the findings from the machine and compared with a state of the art carbon fiber foot (Össur, Variflex, 27, cat 3). Therefore a subject walked with the prosthesis a course containing an instrumented (AMTI, AccuGait) floor, slopes and stairs in a motion lab (Qualisys, 9 cameras).
Motion lab data reveals that force and moment values of the low-cost foot are in a comparable range compared to the carbon fiber foot (see figure below). Furthermore roll-over shape shows a shortened effective foot length. Subjective perceived comfortable gait progression and a safe stance phase that results from the bi-modal designed spring blades.

Based on the results the leaf spring based prosthetic foot design seems capable of providing on the one hand side high functionality like energy return we currently see in carbon fiber feet on the other hand side to achieve a low price for an affordable prosthetic foot that shall be used for developing countries.
Further optimization regarding roll-over shape and effective foot length will be integrated within next design iterations.
ISO22675, 2007: ISO 22675. Prothetik - Prüfung von Knöchel-Fuß-Passteilen und Fußeinheiten.A. P. Arya, L. Klenerman (2008;): The Jaipur foot. In: J Bone Joint Surg,.
J. Steen Jensen; Sandra Sexton (2010): Appropriate Prosthetic and Orthotic Technologies in Low Income Countries (2000-2010). A report of the activities under the Agreement provided by the United States Agency for International Development (USAID) to the International Society for Prosthetics and Orthotics, zuletzt geprüft am 20.11.2014.
Jensen, J. Steen; Treichl, Henning B. (2007): Mechanical testing of prosthetic feet utilized in low-income countries according to ISO-10328 standard. In: Prosthetics and Orthotics International 31 (2), S. 177–206. DOI: 10.1080/03093640701210986.
Layne Hancock Salmond: Transtibial Prosthetics for Developing Countries, P Lenka, R Kumar (2010): Gait Comparisons of Trans Tibial Amputees with Six Different Prosthetic Feet in Developing Countries. In: IJPMR (21), S. 8–14,
0594
Theerapat Kangkasomboon (1) presenting Nuttapol Assarut (1) Tipnara Sakaew (1) Warinthorn Gatephong (1) Pruesarash Phukitviraskul (1) Wissarut Kehasuwon (1)
Germany, Chulalongkorn University, Bangkok (1)
Self-image and attitude on prosthetic cosmetic cover in lower limb amputee in Thailand
There are approximately 35,000 lower-limb amputees in Thailand requiring prostheses. Limb amputation causes a tremendous loss in terms of function, sensation and body image. Amputees suffer from feeling of social discomfort with symptoms of depression. A relationship between body image and prosthetic satisfaction was reported; prosthetic cosmetic cover aesthetic plays an importance role to prosthetic satisfaction. For standard prosthetic treatment in Thailand, prostheses are generally provided with one standard color.
The purpose of this study was to investigate the attitude on body image, prosthetic experience and prosthetic cosmetic cover of the lower limb prosthetic user in Bangkok, Thailand.
This study was conducted in mixed-method approach; in-depth interview and cross-sectional questionnaire survey. The convenient sample of 43 and 6 lower limb amputees, who visit the public and private prosthetic clinics for prosthetic service, was recruited from three major public and private prosthetic clinics in Bangkok, for questionnaire survey and in-depth interview, respectively.
Questionnaire composed of 54-item questions on a 1-5 Likert scale and one opened-end question. Items were focused on body image with/without prosthesis, prosthetic experience in daily life and prosthetic cover satisfaction. The in-depth interview composed of questions on attribution, consequence and value received from prosthetic cosmetic cover.
Demographic data of survey study was shown in table 1. From questionnaire survey, overall average self-perception score was 3.04, with lowest score in self-confident and social interaction section of 2.75 (1 means very dissatisfied and 5 means very satisfied). Experience in daily life and prosthetic satisfaction scores were both moderately satisfied (average 3.64 and 3.58, respectively). Eighty-six percents of participants prefer their prostheses to have natural look in color and detail.
Demographic data

Result from the in-depth interview demonstrated that the most concern attribution of cosmetic cover is natural look and color matched to skin tone. The consequence is that amputees did not want to be noticed as amputee or disable and wanted to be accepted by society. The main core value for them is social belonging and self-esteem.
Returning to society was the major concern of participants. By having prostheses with natural look and color matched skin tone would help them participating to society more confidently. Despite of the need of cosmetic cover with natural skin color, participants are satisfied with current prosthesis cover aesthetic. Possible rationales were discussed. Further investigation on the relationship among various factors and the larger sample size are recommended.
Murray CD, Fox J., Body image and prosthesis satisfaction in the lower limb amputee. Disabil Rehabil. 2002 Nov 20;24(17):925-31.
Cairns N, Murray K, Corney J, McFadyen A. Satisfaction with cosmesis and priorities for cosmesis design reported by lower limb amputees in the United Kingdom: Instrument development and results. Prosthet Orthot Int. 2014; 38(6):467-73.
0595
Richard Lombard Vance (1) presenting Pamela Gallagher (1) Fiadhnait O’Keeffe (2) Deirdre Desmond (3) Robert Coen (4) Nicola Ryall (2)
Thailand, Dublin City University, Dublin (1) Ireland, National Rehabilitation Hospital, Dún Laoghaire (2) Ireland, Maynooth University, Maynooth (3) Ireland, St James’s Hospital, Dublin (4)
Profiling Cognitive Functions in People with Lower Limb Amputations in a Prosthetic Rehabilitation Programme
Peripheral vascular disease and diabetes are the leading causes of lower limb amputations (LLA) in industrialized countries. As both have been linked with cognitive impairment, it suggests people with LLA are more likely to have impaired cognitive functioning. O’Neill and Evans (2009) found that memory and executive function are related to mobility and hours of prosthesis use respectively. However, cognitive functioning is assessed infrequently or with screening tools only. Coffey et al. (2012) recommended comprehensive neuropsychological assessment to determine the nature of cognition and associated impairment in people with LLA.
To investigate cognitive functioning (i.e. memory, executive functioning, attention, processing speed, visuospatial cognition, language) in people with LLA and to determine whether cognitive impairment was prevalent in a sample of people with LLA in a prosthetic rehabilitation programme.
As part of a quantitative, prospective cohort study, a cross-section of neuropsychological functioning in adults with LLA was obtained. Participants were engaged in inpatient or day patient rehabilitation services at a national rehabilitation hospital. Participants completed a comprehensive neuropsychological assessment battery.
Eighty-seven participants with LLA were recruited. When compared to normative data, evidence of impaired (≥1.5 SD below the mean) global cognitive functioning (e.g. 34% were impaired on the RBANS), executive functioning (e.g. 38% impaired, DKEFS Color Word Interference), learning (e.g. 21.4% impaired, CVLT-II-short immediate free recall), episodic memory (e.g. 33.9% impaired, WMS Logical Memory II), attention and processing speed (e.g. 57.5% impaired, RBANS Coding, 33.3% impaired WAIS-IV symbol search), and visuospatial cognition (e.g. 42.9% impaired, RBANS Figure Copy) was observed. Chi2 tests of expected frequencies showed significantly (p<.05) greater numbers of this sample were impaired on a range of tests, compared to the normative population. Significant correlations (p<.001) between cognitive functions were also observed, indicating high incidence of participants having a range of cognitive impairments.
Cognitive impairments are significantly more prevalent in this sample of people with LLA than the general population. The range of impairments observed in this sample may hinder rehabilitation by affecting ability to plan, organise, and learn to use prostheses. Building a profile of cognitive strengths and impairments may aid in understanding the relationship between cognition and outcomes in LLA rehabilitation.
Coffey, L., Gallagher, P., Desmond, D., O’Keeffe, F, & Lombard-Vance, R. (2012). Disabil Rehabil.
O’Neill, B.F. & Evans, J.J. (2009). Disabil Rehabil.
0596
Kardem Soyer (1) presenting Nilgün Bek (1)
Ireland, Health Institution, Ankara (1)
Does usage of the shoulder retraction orthosis effect the shoulder movements, strength and scapular symmetry?
In clinical practice, postural correction is a common treatment approach for individuals with neck and shoulder pain. As chronic static muscle use and postural misalignment are thought to be associated with the onset of some neck and shoulder pain syndromes, it is important to understand the postural correction program might have an impact on muscle activation and posture alignment in the neck and shoulder regions.
The aim of this study is to investigate the effects of the shoulder retraction osthosis on range of motion of shoulder, muscle strength and postural symmetry among 18-45 year old women.
Fifteen women, aged between 18-45 who had a normal body mass index between 16 and 29.9 kg/cm2, were recruited in the study. The volunteers were subjected to the assessment protocol which included demographic data. Manual muscle test was applied bilaterally to the rhomboid muscle, trapezius muscle, pectoral muscles, and upper back erector spinal muscles by the same clinician before and after the treatment protocol. Range of motions of shoulder flexion and external rotation movements were assessed by using a standard goniometry. The Scapular symmetry and shoulder protraction was evaluated with measurement of acromion-wall distance bilaterally, occiput-wall distance, T3-Spina Scapulae, T7- Inferior Angle of Scapulae. The treatment protocol included retracting their shoulder with retraction band in order to maintain postural correction for 6 weeks. After 6 weeks the volunteers were subjected to the same assessment protocol. SPSS 21 and Paired-Samples T Test was performed to compare before and after treatment protocol data. The level of significance was set at p < 0.05.
The mean of demographic datas of patients were, age (31.33±033 years), body mass index (22.79±3.30 kg/cm2). According to results of our study, there was statistically significant differences between the before and after mean values of both right and left shoulder flexion and external rotation (p<0.05). There was no statistical significance in the other motion ranges (p>0.05)(Table 1).
Comparison of the before and after orthotic usage ROM of shoulder movement and muscle strength.

: p<0.05
For the scapular symmetry measurements there was statistically significant difference between the before and after mean values of both side T3-Spina Scapulae, T7- Inferior Angle of Scapulae distances, acromion-wall distance and occiput-wall distance respectively (p<0.05) (Table 2).
Comparison of muscle strength and scapular symmetry measurements.

: p<0.05. **: Strong correlation
Shoulder retraction orthosis is useful and aesthetic but in literature there is limited knowledge about the effects of usage. It was possible to confirm a statistically significant association between retraction of the shoulder, normal range of motion, muscular strength and scapular symmetry. In the present study, it was statistically proven that orthosis has no effects on muscular strength nevertheless by maintaining postural alignment and normal range of motion muscles may contract more effectively. As conclusion, shoulder retraction orthosis affects retraction of the shoulder, range of joint motion and postural symmetry.
0597
Marina Pogosian (1) Mona Hichert (1) Dick Plettenburg (1) presenting
Turkey, Delft University of Technology, Delft (1)
Hand opening and grip force - a literature study that investigates healthy humans ability to control hand opening and grip force with proprioceptive feedback
Upper limb amputation causes several functional disabilities and hampers patient’s body image. Similar to unimpaired humans, the amputees want to be able to adapt and control their motion with the same level of ease. The development of prostheses has increased the level of functionality, but the user acceptance of these prostheses is currently low among others due to the lack of or limited sensory feedback. Studies have shown that feedback about hand opening and grip force are two important requirements and by including these into the prostheses the user acceptance can be increased by reducing the effort needed to control the prosthesis visually.
The purpose of this literature review was to investigate healthy humans ability to control the hand opening and grip force with proprioceptive feedback. No comparison was done with current prostheses.
The relevant literature was searched through PubMed and Scopus. The keywords used for hand opening were; (Hand opening OR Grip aperture) AND (Visual Feedback OR Proprioception);and for grip force: (Grip force OR Grip strength OR Pinch force) AND (Visual Feedback OR Proprioception). This search returned over 900 articles. A first selection of articles was done based on the titles and abstracts. Abstracts containing more than one keyword from the “AND” operator were selected for further analysis. If the articles contained only two keywords from the “OR” operator then these were not selected. References cited in these articles and citations were also examined. A total of 37 articles was selected for further analysis for hand opening and 32 articles for grip force.
Two different visual feedback conditions were investigated; visual and no visual feedback. Visual feedback of the force level was provided to the subject on a computer screen. The data presented for hand opening and grip force showed a significant difference between the two visual feedback conditions. The results suggest that healthy humans will have a grip size and force level closer to the target with visual feedback than with proprioceptive feedback. This result is valid under certain experimental conditions. The grip aperture increased by 10% in the no visual feedback condition (NVFC) compared to the visual feedback condition (VFC). Here the initial hand position was seen in the VFC, the same room light level was used for both conditions and the conditions were not in random order. For grip force there was a difference of 4-6% between the two conditions. In the VFC the subject could see their real-time force level on a screen and in the NVFC only the target force and/or time was displayed.
It can be concluded that if experimental methods as mentioned above are used, healthy humans will have a 10% better grip size (closer to object size), and the grip force will also be closer to the target force level, difference 4-6%, with visual feedback than with proprioceptive feedback (no visual feedback).
0598
Cornelia Putz (1) presenting Julia Block (1) Daniel Heitzmann (1) Thomas Dreher (1) Marcus Egermann (1) Sebastian Wolf (1) Merkur Alimusaj (1)
The Netherlands, Clinic for Orthopedics and Trauma Surgery, Heidelberg University Hospital, Heidelberg (1)
Structural changes of the thigh muscles in trans-femoral amputation, preliminary results
The configuration of the residual limb soft tissue is of high relevance after trans-femoral amputation (TF). A firm soft tissue configuration of the residual limb will potentially result in a superior stabilisation of the residual femur within soft tissue and therefore result in an improved control of the prosthesis. However, clinical experience shows that atrophy of residual-limb muscles lead, beside a loss in strength (1), to a change in residual limb soft tissue characteristics. In general, instability of the stump-socket interface has to be avoided because it could generate e.g. shear forces, pain and friction sores (2). To date little data exists about the structural changes of the residual limb after TF over time, especially of surgical interventions like a myoplasty.
The purpose of the study was to analyse how structural changes of the residual limb after TF amputation can be depicted by using magnetic resonance imaging (MRI).
In this retrospective clinical study 47 patient aged 18-70 years following a TF amputation on the basis of a bone neoplasm or metastasis between 2000 and 2014 were identified. In line with the aftercare program and the adjustment of the prosthesis all patients obtained clinical evaluation and postoperative MRI every three months. Using the Goutailler Classification (3) the fatty degeneration of the thigh muscles (adductor muscles, medial and lateral hamstrings and quadriceps muscle) were analysed in the middle and at the distal end of the residual limb. MRI images of a first preliminary analysis (female, 40y, left side, TF due to a synovial-carcinoma) are presented.
Figure 1 illustrates a typical course after 4 years, that the proportion of intramuscular fat based on MRI signal intensities is graded 1 (1- 25% of fat) in adductor muscles and the gracilis muscle (Fig.1B) compared to grade 4 (degenerated) in the quadriceps and hamstring muscles with an amount of 75%-100% fat. In comparison to the MRI image shortly after amputation (Fig.1A) this clearly demonstrates a fatty degeneration and atrophy of hamstring and quadriceps muscles. Preliminary results also indicate that myoplasties lead to a high amount of fatty degeneration with a decrease of muscular tissue and increase of fatty soft tissue at the end of the stump.

MRI is an excellent diagnostic tool to evaluate fatty degeneration after TF amputation. The degeneration of myoplasties and muscular soft tissue and an increase of fatty soft tissue at the residual limb possibly contribute to instability of the stump-socket interface. Further studies are necessary to evaluate if improved surgical techniques or conservative treatment (e.g. socket design, level of activity) may positively influence the structural changes of the amputated limb.
1. Jaegers SM, et al., Clin Orthop Relat Res 1995;276-84 2. Isakov E, et al., Prosthet Orthot Int. 1996 Aug;20(2):96-100. 3. Goutallier D, et al., J Shoulder Elbow Surg 2003 ;12(6):550.
0599
Abdul Nasir (1) presenting Saad Saleem (1) SivaKugan Kuhanantharajah (1) Sophary Met (1) Shin Sasaki Sasaki (1) Jutamanee Poonsiri (1) ThanatatCharatrungolan Charatrungolan (1)
Germany, SSPO, Bangkok (1)
Analyzing Improvement in Upper Limb Function for GMFCS Level III & IV CP Patient Using Appropriate Assistive Seating
Cerebral Palsy (CP) is a non-progressive lesion that results in disorder of posture arising due to severely disturbed motor functions of a child and creates number of involuntary movements around body.
Assistive Seating devices are used for improvement in life of CP children by preventing disabilities, provision of functional position and accessibility to surroundings. All these factors are supposed to be achieved with no compromise to the comfort of CP Child. Assistive Seating should be such that patients could adopt to use it throughout their daily life. Another important aspect of Assistive Seating is its effect on upper limb function
The purpose of this study was to analyze effectiveness of upper limb function for GMFCS level III & VI CP patients with use of appropriate assistive seating.
Another objective of our research was to compare pressure around hip
For the first objective i.e. effectiveness of upper limb function on the Assistive Seating as compared with using common wheelchair; we asked selected volunteers to perform following activities
Activity-1: Picking cylindrical object and placing it at desired place.
Activity-2: Picking cup to desired level.
Activity-3: Reaching to distant objects.
For the 2nd objective i.e. Pressure distribution on assistive seating as compared to common wheelchair; we performed following activity on patients.
Activity-4: Pressure mapping both on assistive seat and common wheel chair using FSA.
First three activities were reflecting ADL while 4th activity was used to compare pressure distribution around hip and specially Ischial tuberosity.
As hypothesized the results were decidedly in favour of using assistive seat to enhance upper limb function. First three activities performed on assistive seat were improved by a major percentage when compared to wheelchair. These activities in general reflect the Activities daily life (ADL).

Results from Activity-4 shows that total area of contact was increased by a significant percentage in all 6 subjects. Peak pressure at IT in assistive seat was reduced considerably as compared to wheelchair.
Results also showed that average pressure around weight bearing area was distinctly reduced while using assistive seat as compared to wheel chair.
As hypothesized the results were decidedly in favour of using assistive seat to enhance upper limb function. total area of contact was increased by a significant percentage in all 6 subjects. Peak pressure at IT in assistive seat was reduced considerably as compared to wheelchair.
Appropriate assistive seat provides better support to the lower limb and trunk by keeping them in aligned position and by controlling unwanted movements. Assistive seat not only reduces peak pressure on Ischial tuberosity but also reduces average pressure on the whole buttock region because it increases the area of contact and reduces risk of pressure sore on Ischial tuberosity.
0600
Julia Block (1) presenting Daniel W. W. Heitzmann (1) Merkur Alimusaj (1) Cornelia Putz (1) Sebastian I. Wolf (1)
Thailand, Clinic for Orthopedics and Trauma Surgery, Heidelberg University Hospital (1)
Functional assessment in lower limb amputees with different level of amputation in therapy routine
Patients following a lower limb amputation have to regain everyday functionality with their prosthesis. Several factors like socket fit, prosthetic components, physical and mental conditions are influencing progress and outcome. Quantifying the outcome serves a valuable response for all professions involved.
A compact assessment is introduced in every day routine to monitor development and functional outcome. Aiming at a middle way between completeness and necessary extend.
53 patients (36 male, 17 female, median age 51 y range:16–75 y), following a unilateral lower limb amputation took part in this ongoing study. Median time since amputation was 1 year (range 0,25 - 41y). Cause of amputation was in 51% tumor, 30% trauma and 10% pAVK/sepsis. According to the level of amputation three groups consisting of 13 transtibial (TT); 28 transfemural-/ knee-disarticulated (TF) and 12 hip-disarticulated/ hemi-pelvectomied (HX) were formed. The program consisted of prosthetic fitting (36 patients with their first prosthesis), strengthening and stretching exercises as well as functional- and gait training. Patients attend a mean of 26 therapy units. Assessment started in the second unit (T1) with the Locomotor Capability Index [1] (LCI), followed by the Two-Minute-Walk-Test (2Min), 10-Meter-Walk-Test (10m) and Timed-Up&Go-Test (TUG). The use of walking aids was documented and ranked. Changing one rank was counted as one point. The assessment was repeated at the last unit (T2). Group means are calculated and compared between groups and dates.
LCI score in TT at T1 was already at maximum in their basic activities (BS) and gained in the advanced activities (AAS), only the 2Min showed a functional progress. The TF displayed the most all over improvement in the assessment. The HX were limited in their LCI high score and improved in the functional tests. The use of walking aids was most reduced in the TF with -0,7 points in average followed by the HX (-0,4). Wereas the TT barely used any aids therefore just reduced -0,2 points.
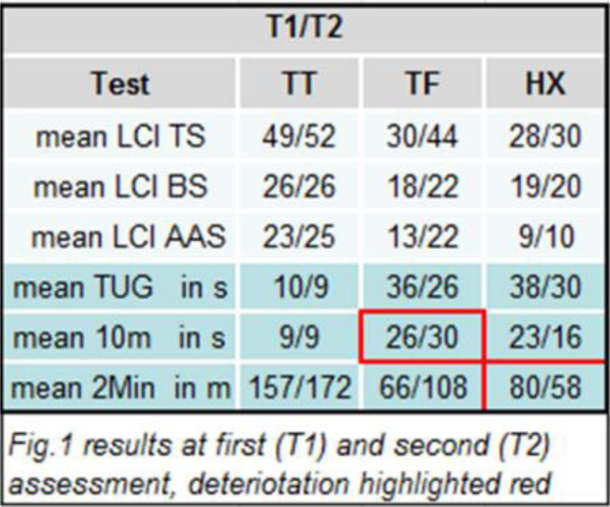
Deterioration in the functional tests (highlighted in red) are directly related to a reduction in the us of walking aids. LCI results are in accordance with the functional test results and aids ranking. Subjects starting with high scores need more sensitive tests for propper documentation. Performing standardized tests at defined points in the rehabilitation serves as feedback for patients as well as the interdisciplinary caregiver team.
1. Franchignoni, F. Arch Phys Med Rehabil, 2002.
0602
HORTENSIA MRANGA (1) presenting
India, KILIMANJARO CHRISTIAN MEDICAL UNIVERSITY COLLEGE, KILIMANJARO (1)
The Need of Category I Prosthetist and Orthotist in Africa
Sub-Saharan Africa has approximate population of 874,841,049, comprising 131,226,157 people with disabilities (WHO 2011). In few selected countries in Africa the study shows that the unmet need of assistive devices including prostheses and Orthoses is still high, for example Zambia(38.9%) and Namibia(47.7%)
Due to an increased number of disabled people with higher level of disability due to war conflicts in some African countries there is a need of training CAT I P/O.
To determine the demand of CAT I Prosthetist and Orthotist professionals in Africa in the provision of prostheses and orthoses for disabled people with higher level of disability.
Descriptive, Qualitative and Quantitative Methods were applied. The study was done in Tanzania at Kilimanjaro Christian Medical University College of Tumaini University Makumira. This is the only University which train CAT I ISPO recognised prosthetist and Orthotist in Africa. Student statistics from KCMUCO, Faculty of Rehabilitation Medicine in the Prosthetics and Orthotics programme was used to obtain the number of prosthetist and orthotist trained so far in Africa. Inclusion criteria were prosthetist and orthotist graduated from 2002 to 2013 at KCMUCO. The exclusion criterion was Prosthetist and orthotist graduated from unrecognized universities by ISPO in Africa.
The number of graduates so far from KCMUCO who are included in the study are 90. Among them 75 are from African Countries.
CAT I Prosthetist and Orthotist graduates in Africa and their number in the brackets are Tanzania(29), Kenya(7), Uganda(1), Rwanda(1), Ethiopia(3), Zambia(5), Malawi(1), Namibia(3), South Africa(19),Mozambique(1), Nigeria(2), Siera Leonne(1), Togo(3), Senegal (1)
Countries like DRC, Somalia, and Liberia just to mention few examples are still affected by civil war and they don’t have any graduate from KCMUCO. The main reason being low level of sponsorship support. The table below shows the trend for three years

Considaring the above results, there is a need of the sponsorship support agencies to increase their support to the countries affected by civil war
Secondly, the University should find means of increasing the facilities so that it can accommodating high number of students
Thirdily, if there is adropout of the candidates from the earmarked countries then the vacancies should be filled by applicants from other developing countries including Tanzania.
0605
S Walkay (1) presenting William Munro (1) Martin Buchan (1)
Russia, The Inverclyde Royal Hospital, Inverclyde Greenock Scotland (1)
A clinical outcome study of the Varus – Valgus stress adjustment knee brace in the management of knee Osteoarthritis- A district general hospital experience in the West of Scotland
The off loading knee brace is a known treatment for varus gonoarthritis of the knee. Literature has shown that these braces reduce pain and increase walking distance. These braces can be used as non surgical management of knee osteoarthritis. This study was conducted to evaluate the clinical out come of varus –valgus stress adjustment stress knee brace (V-VAS) used for in our district general hospital for treatment of knee osteoarthritis.
To study the clinical outcome of Varus – Valgus adjustment knee brace in the management of knee osteo-arthritis.
A total of 147 patients included in study who had been prescribed varus off loading knee brace for osteoarthritis . Of these 86 patient were followed retrospectively and 61 patient were followed prospectively. The mean follow up was 3.4 years in retrospective group and 1.2 years in prospective group .Oxford knee scores, Visual analogue score for pain, Walking distance before and after the brace, Patient satisfaction and Statistics were evaluated.
Average oxford scores before the brace was 19 and after the brace was 32 (P<0.01). The pain scores before and after the brace was 8 and 3 respectively (p<0.01). The walking distance had improved to 900 yards. The patient satisfaction was 78%. Thirteen of eighty six patients in the retrospective group discontinued the brace, of these two had high tibial osteotomy, six patients had total knee replacement, one had unicondylar knee replacement, one patient had dislocation of patella and two elderly patients were house-bound because of medical problems.
The Off loading knee brace is effective in the management of osteoarthritis of the knee. Patient satisfaction is high when using the brace. However compliance may be an issue in some of the patients . Education and early appointment for brace re-fitting increases patient compliance.
0606
Mark Currie (1) Elaine Figgins (1) presenting
UK, NCPO, University of Strathclyde, Glasgow, Scotland (1)
Prosthetic Charities: Prosthetic Rehabilitation Professionals Opinions on their Function & Role
A primary amputee is treated by a multi-disciplinary team (MDT). The team must see that all the patients’ needs and wishes are taken into consideration when making any decisions about their treatment. This may include putting patients in touch with charities or user groups for further support after their initial care is complete. It is documented that in any area where treatment of ill health is concerned, charities are founded to help support patients and their families. Charities aim to help the patients involved and support the health service wherever possible.
As the role and function of many other charities that support different sectors of the health service are so widely understood, it is important to grasp the current situation that surrounds prosthetic charities. Much of the literature related to prosthetic charities and their role involves patient’s satisfaction of their care. No literature exists that takes into account the prosthetic rehabilitation professionals opinions of the charities. Currently there are eight prosthetic charities that work in Scotland; BLESMA, The Douglas Bader Foundation, The Limbless Association, Limb Power, Reach, STEPS, The Murray Foundation and PORT-ER.
This study utilised a nine question survey that was taken around Scotland to the Prosthetic Rehabilitation Centres. The survey aimed to gain an insight into clinician’s opinions regarding various aspects of prosthetic rehabilitation charities. It also attempted to gauge the level of interaction currently and possible interactions in the future between clinicians and charities. Four of the questions were audio recorded to ensure all qualitative information was documented. All information was put into the analysis software Qualtrics. Qualitative data was analysed using Grounded theory and open coding to form themes in the information.
22 participants took part in the study from 4 of the prosthetic rehabilitation centres in NHS Scotland. Of these; 16 prosthetists, 2 prosthetic managers, 2 physiotherapists, a prosthetic technician and a clinical nurse were included.
Table showing areas participants would consider future interactions with prosthetics charities

Charities want to be more involved in supporting professionals, but taking current opinions into account, this does not seem to the happening effectively at the moment. There is a need for charity run events, but better tailored to the general amputee population for them to be more successful. Charities need to advertise their services and availability of grants for patients and clinicians to interact more easily with them. Charities could be key to a brighter future.
0607
John Eyley (1) Elaine Figgins (1) presenting Anthony McGarry (1)
UK, NCPO, University of Strathclyde, Glasgow, Scotland (1)
Pilot Study: Measuring the Reliability of the Modification of Ankle-Foot Orthosis Models Using TracerCAD Software
Computer aided design (CAD) systems such as TracerCAD have become more prominently used in orthotic clinics across the world in recent years. CAD can be used as a method of shape capture and rectification tool for the manufacture of ankle foot orthoses (AFO). Historically, plaster modification techniques have been used in orthotics and prosthetics but these methods have been described as time consuming and difficult to quantify. After shape capture, modification is required to alter the shape prior to the manufacture of an ankle-foot orthosis (AFO).
The benefits of the use of Computer-Aided Design (CAD) systems in orthotics had been mentioned within many previous studies, yet no studies had been able to validate these claims.
The intra-reliability and inter-reliability of the CAD modification of ankle foot orthosis models by three orthotists was attempted to be quantified within this study.
The main questions that were asked in this study were:
Is there sufficient evidence of intra-reliability of the rectification process using OMEGA software?
Is there sufficient evidence of inter-reliability of the rectification process using OMEGA software?
Do the results show differences between the inter-reliability and intra-reliability?
It was planned for the three orthotists to each modify, each of the thirteen AFO models three times and therefore creating 9 repetitions for each model and a total of 117 rectified models. It was intended for each of the orthotists to attend three sessions at weekly intervals; therefore the intra-reliability over time and inter-reliability between orthotists could be compared.
The number of models was chosen to create statistically significant evidence for intra-reliability with the power level of 80% and a significance level of 5%. The models were based on patient presentations that were fabricated to represent thirteen typical orthotic patients treated using a rigid AFO. Data at 6 landmarks on each model was collected for analysis. The inter-reliability and intra-reliability of results were calculated using the intra-class correlation formula. SPSS was used to analyse the results.
From the results it was deduced that there was more evidence of ‘sufficient’ intra-reliability than there was to suggest there was ‘insufficient’ evidence of intra-reliability. There was also some evidence of inter-reliability but the evidence was not compelling enough to be able to draw any certain conclusions.

Participant fatigue may have been a factor that could have affected the results. The sessions were carried out at differing times of day. A larger study with a greater number of participants would be required to validate the conclusions made from the results of this study. There is an immense need for more research and greater standardisation of orthotic processes.
0608
Guðfinna Halldórsdóttir (1) presenting Christophe Lecomte (1) Knut Lechler (1)
UK, Össur, Reykjavik (1)
A novel prosthetic foot design shows anatomical like stiffness properties
The range of motion and the stiffness of the biological ankle during stance phase of gait is very important for proper locomotion. Conventional energy-storing and -returning (ESAR) prosthetic feet try to mimic this with carbon fiber leaf springs which require the amputee to charge the spring with his residual limb. If the spring is too stiff the socket can potentially put excessive pressure to the residual limb.
Describe the design and mechanical stiffness results of a novel prosthetic foot that has more ankle range of motion and stiffness closer to biological ankles than conventional ESAR feet.
The design intention of the ankle was to design a passive ankle with range of motion and stiffness closer to the biological ankle than previously seen in ESAR feet. The prototype consists of three carbon fiber
Stiffness curves (load vs. displacement) were plotted for both feet. The stiffness was calculated for the first linear part of the curve (A). The stiffness for the prototype was 40% lower than for Vari-Flex. Energy storage was 26,5J for the prototype compared to 14,7J for Vari-Flex. Energy return for the prototype was 23,2J compared to 14,1J. At maximum load applied (1230N) the Graph 1: Stiffness curves for prototype and Vari-Flex

displacement for the prototype was 37mm compared to 32mm for Vari-Flex.
The results show much lower stiffness for prototype compared to Vari-Flex during the first part of the loading phase (A). Clinically this indicates smaller resistance to initial dorsiflexion for the prototype and less moment needed from the residuum of the amputee to load the prototype. Prototype stores much more energy than Vari-Flex and despite more energy loss it returns more energy. The high energy return along with progressive stiffening, similar to what seen in anatomical ankle [1], is an indication of a more powerful push-off during late stance.
1. Takahashi, K. Z., & Stanhope, S. J. (2013). Mechanical energy profiles of the combined ankle-foot system in normal gait: insights for prosthetic designs. Gait & Posture, 38(4), 818–23.
0609
Alistair Vardy (1) presenting Dick Plettenburg (1)
Iceland, Delft University of Technology, Delft (1)
Development of a shoulder-worn prosthetic interface to control an upper limb prosthesis
Body-powered prostheses remain the most cost-effective upper limb prosthesis, and have the advantage of providing proprioceptive feedback to the controlling limb and thereby a high level of control compared to externally powered devices. Unfortunately high control forces have led to abandonment [1,2]. Control forces for externally powered prostheses are low, but control has proven difficult without appropriate feedback and most users rely on vision to manipulate objects.
Our study aims to develop a prosthetic interface to control an externally powered prosthesis which is controlled by shoulder movements and applies proprioceptive feedback to the user.
We conducted two pilot experiments to investigate shoulder control using a single shoulder. First, we determined which shoulder movements would yield the largest deflection between two points on the shoulder, anticipating the use of skin anchors [3]. To this end, the 3D positions of 25 points on the back, and the acromion, were recorded during protraction, retraction, elevation, depression, and a combination of elevation and protraction. Second, we determine to what extent participants were able to control low forces levels (2-10 N). This experiment utilized a haptic robot programmed to simulate grasping either a solid or a deformable object by moving the shoulder.
The first experiment revealed the combination of elevation and protraction that yielded the largest displacement between two points on the back. Due to excessive movement of the skin over the underlying tissue for points near the shoulder blade, a combination of points near the 7th thoracic vertebrae and the acromion were selected for the second experiment. The second experiment illustrated that forces between 2 and 10 N could easily be controlled by elevation and protraction, however, forces between 4 and 6 N were preferred by most participants.
Shoulder control using low control forces seems promising. The low level of force will likely reduce the abandonment rate and hopefully reduce the over-use complaints of prosthetic users while retaining a high level of control. Our next step is to determine the most comfortable level of feedback from a prosthesis, and develop of a mobile prosthetic interface (control and feedback) that can be worn underneath clothing and connects to existing externally powered prostheses. This research was funded by Fonds NutsOhra.
[1] E. A. Biddiss and T. T. Chau, “Upper limb prosthesis use and abandonment: A survey of the last 25 years,” Prosthetics and Orthotics International, vol. 31, pp. 236-257, 2007.
[2] G. Smit, R.M. Bongers, C.K. van der Sluis, and D.H. Plettenburg, “Efficiency of voluntary opening hand and hook prosthetic devices: 24 years of development?,” Journal of Rehabilitation Research and Development, vol. 49, pp. 523-34, 2012.
[3] D. Latour, T Sabolevski, K Lajoie-Weaver. “Ipsilateral scapular cutaneous anchor” 12th World Congress of the International Society for Prosthetics and Orthotics, Vancouver Canada, July 29 - August 3, 2007
0611
Liselotte Hermansson (1) presenting Lena Krumlinde-Sundholm (2) Christina Ragnö (3) Anita Stockselius (3)
Russia, Faculty of medicine and health, Örebro university, Örebro (1) Sweden, Karolinska Institutet, Stockholm (2) Sweden, bRÄCKE dIAKONI, stockholm (3)
Development of the Assisting Hand Assessment-PAD: A Rasch-built performance measure for people with unilateral upper limb prosthesis, amputation or reduction deficiency
Hand function assessment for people with unilateral upper limb amputation or congenital deficiency commonly fails to measure how effectively the affected limb is used in bimanual daily life tasks performance. The Assisting Hand Assessment (AHA) has successfully used this perspective in children with congenital hemiplegia. Some studies have tried to use the original scale also for people with other diagnosis, but considerable adjustments of the scale were needed to make the measures valid for people with unilateral upper limb prosthesis, amputation or deficiency.
To evaluate the validity of Assisting Hand Assessment - PAD for use in people with unilateral upper limb prosthesis, amputation or deficiency. More specifically to report the evidence of content, response processes, and internal structure for the AHA-PAD.
In total, 222 assessments of children and adults with unilateral upper limb prosthesis, amputation or deficiency were used for this study. The relevance of the original AHA test items, and the generating and evaluation of new test items were evaluated by Rasch measurement analysis according to a rating scale model. Internal scale validity was investigated by evaluating rating scale functioning, item and person goodness-of-fit and uni-dimensionality of the scale. Furthermore, targeting and scale reliability was evaluated.
The resulting AHA-PAD includes 20 items scored on a 3-point rating scale. Internal scale validity was confirmed and the AHA-PAD scale distributed the person ability measures well with high separation.
The results from this study show that the AHA-PAD can be used to measure functionally important, bimanual aspects of hand-use for both children and adults with unilateral upper limb prosthesis, amputation or deficiency.
The use of the AHA-PAD has the potential to significantly broaden the knowledge of how effectively individuals perform bimanual tasks with or without prosthesis or when using different types of prosthesis. The AHA-PAD may also be used to guide functional approaches to training that target effective assisting hand use in daily activities.
0614
Kristin Zhao (1) presenting Ryan Breighner (1) Amanda Theuer (1) Sasha Blue Godfrey (3) Matteo Bianchi (3,4) Manuel Catalano (3,4) Giorgio Grioli (3,4) Marco Santello (2) Antonio Bicchi (3,4) Karen Andrews (1)
Burkina Faso, Mayo Clinic, Rochester, Minnesota (1) USA, Arizona State University, Tempe, Arizona (2) USA, Istituto Italiano di Tecnologia, Genova (3) Italy, Centro E. Piaggio, Università di Pisa, Pisa (4)
Application of a novel robotic hand as a myoelectric prosthetic prototype: Proof of concept in a single patient
The Pisa/IIT SoftHand (SH) is a novel under-actuated robotic hand which combines soft robotics and the first grasp synergy (determined by principal component analysis of grasp postures1) to guide grasp movements. The SH is anthropomorphic and has a single actuator that drives simultaneous motion at all joints of the five digits. Because of the versatility and anthropomorphic design, the SH is an ideal platform for the development and translation of the novel, robotic principles into a breakthrough upper limb myoelectric prosthesis.
The aim of our research team is to convert a novel, robotic hand (SH) into an easily-controlled, anthropomorphic, versatile myoelectric upper limb prosthetic prototype. As a proof of concept, we will demonstrate its potential in a single patient with upper limb loss.
Design and control changes were implemented to transform the SH robotic hand into a prototype upper limb myoelectric prosthesis. Specifically, we addressed several objectives, including portability, battery requirements, motor specifications, size/weight, and wrist connector design changes necessary for integration with a prosthetic socket. Further, we integrated the SH with a custom prosthetic socket for use in an existing upper limb myoelectric prosthesis user. Clinical tests (Box and Block2, AM-ULA3, Jebsen-Taylor4) and biomechanical data (grasp forces and kinematics) were obtained on the subject during initial use and following 6 hours of training with the new prosthesis.
The design changes allowed for the prototype to include on-board, wireless control of the two commercial EMG electrodes, a single on-board light-weight 12V lithium-ion polymer battery, a single on-board, low-profile motor, and a custom quick disconnect wrist connector. These changes allowed for seamless integration of the prototype prosthesis into a prosthetic socket for the subject. There were noted improvements in the Box/Blocks and AM-ULA tests from pre- to post-training, and improvements in some aspects of the Jebsen-Taylor. Qualitatively, the subject reported satisfaction with the initial use of the prosthesis. Force measurements from an instrumented grip device showed a maximum grip force consistent with the hand’s design specifications. From the kinematic data it was seen that post-training, the subject executed preparatory closure of the SH in anticipation of a grasping task, when appropriate.
Efforts to convert the novel, robotic hand (SH) to a myoelectric terminal device for persons with transradial limb loss are extremely promising. Design changes allowed for on-board EMG, power, and motor and integration with a prosthetic socket. Further, reports from a single user indicated satisfaction with the hand. In addition, clinical and biomechanical tests indicated improvement in outcomes following a short training session.
1. Santello M, Flanders M, Soechting JF. Postural synergies for tool use. Journal of Neuroscience. 1998; 18: 10105-10115.
2. Mathiowetz V, Volland G, Kashman N, Weber K. Adult norms for the Box and Block Test of manual dexterity. Am J Occup Ther. 1985; 39(6):386-91.
3. Resnik L1, Adams L, Borgia M, Delikat J, Disla R, Ebner C, Walters LS. Development and evaluation of the activities measure for upper limb amputees. Arch Phys Med Rehabil. 2013; 94(3):488-494.
4. Jebsen RH, Taylor N, Trieschmann RB, Trotter MJ, Howard LA. An objective and standardized test of hand function. Arch Phys Med Rehabil. 1969; 50(6):311-9.
615
Lucy Topaloff (1) presenting
Italy, miraclefeet, Chapel Hill, NC (1)
Parent and clinic staff feedback from pilot testing a low-cost brace for clubfoot
Out of 15 patients:
12 said the shoe was easier to put on
8 said the child never cried when parents tried to put the brace on, whereas they did when parents but the other brace on
10 said the brace appeared more comfortable
4 said the brace allowed them to carry their child, whereas the other did not
8 said the child could stand more easily than in another brace
6 said the child could walk in the brace, whereas children couldn’t in the other
5 said children could crawl more easily in this brace
3 said the child could not remove himself from the brace, whereas he could before
6 said it took under 5 min to put the brace on, instead of 10 minutes
Though the sample size is small, results indicate that parents find the miraclefeet brace more comfortable and practical than other braces. Miraclefeet expects the brace compliance rate to be higher with the miraclefeet brace than with other braces, and therefore for the relapse rate to decrease. To test this hypothesis, miraclefeet will test the miraclefeet brace on a larger scale.
Dobbs MB. Pediatr Orthop.2007;
Thacker MM J Pediatr Orthop. 2005
0616
Yeongchi Wu (1) presenting Christopher Robinson (1) Larissa (Conner) Sletto (1) John Michael (1) Steven Gard (1) Desmond Masterton (1)
USA, Northwestern University Prosthetics-Orthotics Center, Chicago (1)
Dilatancy TLSO System for Fabricating Thoraco-Lumbar-Sacral Orthoses
There are three commonly used methods for fabricating custom spinal orthoses: plaster-based, CAD-CAM-based, and measurement-based approaches. Following successful development
The project aimed to develop an appropriate procedure based on dilatancy technology for custom fabricatio
n of spinal orthoses that is suitable for services in resource limited environments.
Development of the dilatancy TLSO casting system started with re-designing of the dilatancy prosthetic system for laboratory testing on a plaster model in order to select suitable casting materials and test the casting procedure. It was a continuous problem-solving process with many unexpected technical challenges. After developing a workable casting system, we conducted clinical evaluation on consented healthy adults to continue refining the casting system and procedure. At this time we are testing the system on consented individuals with disabilities.
After numerous design changes to overcome technical barriers, we have arrived at a workable casting system and procedure. We use two large Spandex casting bags filled with polystyrene (PS) beads sealed in large thin plastic bags (garbage can liners) for casting the front and back panels of the negative mold (Figure: transverse plane, superior view of supine subject). The formed light-weight negative PS mold is then converted to a positive sand model for modification and thermoforming the TLSO. Since the positive sand model is relatively heavy, a simple model stand was made to reduce the stress of lifting and allow easy rotation of the sand model during modification and thermoforming of TLSOs.

This dilatancy TLSO casting system is inexpensive to set up and easy to use. Being plaster-less, it is easy to clean up and does not create plaster waste. Clinical evaluation on healthy subjects revealed good comfort level during casting and fitting evaluation. We believe this dilatancy TSLO casting system is potentially an appropriate technique for providing services in resource-limited environments. Further independent field evaluation is highly desirable.
1) Mead WJ; 1949. U.S. Patent 2,472, 754.
2) ;2003, Prosthet Orthot Int, 27(2):146-152.
3) ;2009, Prosthet Orthot Int, 33(1):1-9.
4) Jensen J ; 2005, Prosthet Orthot Int, 29(2):165-175.
5) Thanh NH; 2009, Prosthet Orthot Int, 33(2):130-134.
6) Jivacate T; 2012, Prosthet Orthot Int, 35(1): 70–75.
0618
Ann Yamane (1) presenting
USA, University of Washington, Seattle, WA (1)
Developing a Prosthetics-Orthotics Professional Learning Community Using Portfolios as a Tool: An Action Research Project Proposal
Clinical degree programs in prosthetics and orthotics (P&O) require the learner to build on acquired knowledge and skills across the curriculum in preparation for entry-level clinical practice. The use of portfolios, a collection of student work over a course of study, is reported to be effective in achieving varied objectives in classrooms, programs, and professional settings.1 From a learner’s perspective, portfolios are reported to facilitate the integration of acquired knowledge across an educational program.2 Professional learning communities (PLC) focused on student learning have a positive impact on both teachers and students.3 The evidence indicates through collaborative efforts, sharing student work has the potential to improve both student and faculty learning, promote reflective dialogue, and deprivatize practice. 4
The aim of this action research study is to answer the question: Will the implementation of a student portfolio with a focus on collaboratively using “looking at student work” protocols provide the foundation for the development of a P&O professional learning community at the University of Washington?
A literature search was conducted to define the attributes of a PLC and describe the use of portfolios in the development of a PLC. Baseline and post intervention data of the faculty and students will be gathered through formal interviews, surveys, field notes, and a self-reflective journal. Data analysis will entail identification of themes and concepts based on the current literature identifying the characteristics (reflective dialogue, deprivatized practice, collaboration, shared norms, teacher beliefs, focus on student learning, tension between learning content and practice) of a PLC.
The barriers encountered in the initial introduction of the student portfolio included 1) no specific guidelines for material inclusion, 2) a lack of established portfolio review guidelines, and 3) no designated faculty time for collaborative review of student work. These issues are addressed in the current study proposal.
The development of a PLC in a clinical prosthetics and orthotics program may be challenging. The faculty’s varied expertise and responsibilities in the areas of teaching, clinical care, and research may be one contributing factor. The collaborative structured protocol of “looking at student work” can potentially encourage reflective dialogue, sharing of beliefs and practices, and ultimately enhance student learning.
1. White CP.; 2004, New Directions for Teaching and Learning
2. Bowers SP; 2005, College Student Journal
3. Vescio V, Ross D, Adams A.; 2008, Teacher and Teacher Education
4. Bryk A, Camburn E, Louis KS.; 1999, Educational Administration Quarterly
0619
Sajid Muhammad (1) presenting zeshan Zahid (2)
USA, Rawalpindi Medical College, Rawalpindi (1) Pakistan, Rawalpindi Medical College, Rawalpindi (2)
A Descriptive Review of Lower Limb Amputation Cases in Allied Hospitals Rawalpindi of Five Years
Amputation is removal of body extremity either surgically or accidentally. There are also another type of amputation know as congenital amputation that occurs within the uterus. Body extremities are very important in daily living activities. In developing countries the physical disability is higher than the developed countries due to multiple pathological and environmental reasons. Modern Science has replaced the missing body limbs with closely resembling mechanical limbs know as Prosthesis. Prosthesis helps an amputee to resume social and professional life.
To find out most common causes of lower limb amputation in Benazir Bhutto hospital Rawalpindi, with the distribution of lower limb amputation according to age, gender, and amputation level. This study is also aimed to predict the need of different types of prosthesis required after the amputation.
Retrospective data of five year (January 2007 to December 2011) was collected that fulfilled the requirement of questionnaire, data of 401 cases were recovered from the record registers of Orthopaedic operation theatre, General surgery Operation theatre and causality operation theatre of Benazir Bhutto Hospital. 401 patients were included in our study out of which 303 (75.6%) were male and 98 (24.4%) were female.
Among 401 lower limb amputees, peripheral vascular disease associated with diabetes was leading cause of lower limb amputation and it was 78.8% (316), Trauma 11% (44), Infection 7.5% (30), and least value is tumour 2.7% (27). Transtibial amputation 45.6% (183), ray amputation 34.9% (140), knee disarticulation 1.0% (7), syme amputation 1.0%(4) and partial foot amputation .5% (2). Unilateral amputation was more with Right side was 69.8% (280), left side 24.9 (98) and bilateral amputation .2% (1). Yearly amputation rate was 12.7% (51) in 2007, 21.2% (85) in 2008, in 2009 it was 22.7% (91), in 2010 19.9% (78) and in 2011 it was about 23.9% (96). In gender distribution males are 75.6% and females 24.4%. Mean age of patients was 49.2 with SD
Result showed that most common cause of lower limb amputation at Benazir Bhutto Hospital was peripheral vascular disease associated with diabetes and least common was tumour. Male were more involved than females, it could be due to the more exposures of males to external environment and professional activities. Most common level of amputation was transtibial level. This retrospective study also showed that amputation rate increasing yearly. Re-amputation was observed and that was 6.0% which can be considered significant because re-amputation shift the level of amputation more proximal. It was also concluded that pre-amputation and post amputation prosthetics care was not taught to the patients.
0620
Yeongchi Wu (1) presenting
Pakistan, Northwestern University Prosthetics-Orthotics Center, Chicago (1)
CASE REPORT: Stump care and Prosthetic Fitting of A Transfemoral Residual Limb with a Large Open Wound
In the presence of a traumatic open wound, determining the type of wound care and timing of prosthetic fitting is a multifactorial decision. This paper presents the experience of managing a traumatic transfemoral amputee with a large skin defect using elastic stockinette and a simple compression device for stump shrinkage and an early preparatory prosthetic fitting for gait training even with a large open wound.
The paper presents the benefit of using compression dressing, compression device and early prosthetic fitting for promoting wound healing and gait training of a traumatic transfemoral amputee with a large open wound.
Proper application of layers of elastic stockinette can be a very effective method to provide gradient compression to promote shrinkage of any residual limbs

The adult transfemoral traumatic amputee was seen during an out-of-state consultation when the caring team was deciding whether to do skin graft first and refer him to rehabilitation program six months later. After a short discussion, the patient was transferred to our out-patient rehabilitation program. Besides regular wet-to-dry wound dressing changes, layers of elastic stockinette were applied, and, a compression device was made for wearing outside the pants while up in the wheel chair. Three weeks later, when the residual limb became less bulbous, a preparatory prosthesis was fabricated for him to start gait training. Another three weeks later, the open wound reduced in size and the surrounding tissue became looser, he was sent back to his orthopedic surgeon for secondary wound closure closure.
1. ; (2003), pps.1183-1190, Haimovici’s Vascular Surgery, 5th Edition, Blackwell Scientific Publications, Inc, Cambridge, MA.
0621
Nima Befrui (1) presenting Annie Horng (1) Oussama Jarousse (1) Tuan Nam Le (1) Simon Weidert (1)
USA, Clinic for General-, Trauma- Hand- and Reconstructive Surgery of the LMU, Munich, Bavaria (1) Germany, Institute for Clinical Radiology, Munich, Bavaria (2)
Vibroarthrography: non-invasive early detection of cartilage degeneration in comparison to MRI
Vibroarthrography (VAG) analyses the vibrations emitted from articulating joint surfaces during joint movement. It is expected that knee joint pathologies, such as the degeneration of articular cartilage, affect the vibroacoustic characteristics of the joint and correlate with detectable variations of the VAG-signals. Unlike the high cost and time consuming MRI or invasive arthroscopy, VAG could provide a cheap and easily accessible assessment of knee joint function in motion and cartilage status.
Our aim was to evaluate the accuracy of VAG in the diagnosis of different stages of chondromalacia/ osteoarthritis in comparison to MRI.
Patients with knee joint symptoms and recent MRI data and healthy volunteers with no knee joint complaints were assessed and compared within this study. Symptoms were evaluated with the Oxford Knee Score.
VAG-signals were measured/ recorded by a setup consisting of accelerometers placed upon the patella and medial plateau of the tibia, as well as a piezoelectric sensor placed upon the lateral tibia plateau, as the patient performed a series of extensions and flexions of the knee joint. A potentiometer mounted to a knee orthosis measured the angle of joint flexion.
Patient MRI data was assessed by a radiologist and classified according to Outerbridge.
Out of 31 patients (m=14, f=17, mean age : 55± 13 years), 32 knee joints were evaluated : chondromalacia grade II : n=3, grade III : n=10, grade IV : n=19. Three joint signals with bone degeneration visible in X-ray imaging were discarded to focus on early detection of cartilage degeneration only. The control group consisted of 40 healthy knee joints (m=22, f=18, Oxford Knee Score within normal limits, no symptoms/ complaints, mean age : 29± 10 years).
Pathological and healthy VAG-signals were analysed via machine learning algorithms and statistical parameters (standard deviation, zero crossig rate) were selected for their performance to distinguish healthy vs. non-healthy knees. In 4 automated randomised sequences, 75% of data was used as software training with remaining 25% used to test classification accuracy, producing an average sensitivity of 82% and a specificity of 70%.
This is the first evaluation of VAG-technology using MRI-data for control and focusing on early diagnosis of cartilage damage. Encouraging data has been found for sensitivity and specificity. We see great potential of VAG to provide a quick, low-cost assessment of knee function and cartilage status, which could reduce possibly unnecessary diagnostic procedures. It also provides a possibilty of objective longitudinal intra-individual joint evaluation. It is expected that the evaluation of a larger case number will increase the machine learning accuracy and thus sensitivity and specificity.
0622
Innes Boland (1) Aurelio Gomes (1) Laura Gwathmey (1) presenting
Germany, Physicians for Peace, Norfolk, Virginia (1)
An Innovative Approach to Global Prosthetic and Orthotic Training and Education: Lessons-Learned from a Blended-Learning Approach in the Dominican Republic
More than one billion people in the world live with some form of disability, yet access to high quality rehabilitative services is limited for many of those living in the developing world. Building the capacity of in-country healthcare professionals to provide quality prosthetic and orthotic (P&O) care is essential to narrowing the gap in appropriate services and treatment, but access to education and training is often extremely limited. Since 2001 Physicians for Peace (PFP) has been addressing this need by providing training and education to rehabilitative healthcare professionals in collaboration with in-country partners in the Dominican Republic.
To address a gap in P&O training and certification available in the Dominican Republic, PFP collaborated with Asociación Dominicana de Rehabilitación (ADR), a local clinical partner providing P&O services, and the International Society for Prosthetics and Orthotics recognized certification program at the University Don Bosco in El Salvador to offer a blended- learning training curriculum to P&O technicians while they continued working full-time in the Dominican Republic.
Blended learning is a multi-modal approach to education that complements distance learning with hands-on training. Volunteer international medical educators from PFP supplemented the online curriculum with regular hands-on training in the facilities where the technicians worked.
Recently, an external evaluation was conducted on this blended learning approach to assess the strengths, challenges, and optimal resources for program delivery. The evaluation sought to gain an understanding of the benefits and challenges in executing this blended learning approach. Three primary evaluation questions were established. 1.How has blended learning affected the participating program technicians (prosthetists and orthotists)? 2.What have been the strengths and challenges of the online and hands-on learning components? 3.What resources, partnerships or inputs are needed for effective implementation? Data was collected via surveys, interviews, observations, and artifacts.
This model of integrating a distance-learning curriculum, with consistent and supportive hands-on training has resulted in the completion of the first class of seven student technicians from the Dominican Republic in 2014. Key findings from the evaluation included : improved confidence, quality of work, knowledge of specific orthotic and prosthetic topics, productivity, and teamwork in an interdisciplinary setting ; increased knowledge through participating in demanding online and hands-on training ; shared learning and communication with fellow students ; difficulty accessing computers and reliable internet connections ; challenges in maintaining a work-life-school balance ; and challenges in timely communication and responsiveness to questions.
Primary limitations of the data collection methods include small sample size, selection and language bias. Despite these limitations, carrying out an evaluation was very important to determine if replication and sustainability of a blended-learning approach is effective in training employed technicians as Internationally Certified Prosthetic and Orthotic Category II Level technicians.
0623
Pairat Tangpornprasert (1) presenting Chanyaphan Virulsri (1)
USA, Chulalongkorn University, Bangkok (1)
Thickness Distribution Improvement of Prosthetic Socket by Thermal Vacuum Forming with Pre-Vacuum Technique
Nowadays, the prosthetic legs are still not available for every leg amputees in Thailand. The important component of a prosthesis leg which is hard to fabricate is prosthesis socket. In Thailand, there are two socket fabrication methods that are resin casting and thermal vacuum method. The thermal vacuum forming method which can rapidly fabricate has more advantage than the resin casting method that ruins prosthetists’ health from the volatile matter. Nevertheless, the thermal vacuum forming method can fabricate the socket with poor wall thickness distribution.
The purpose of this paper is to develop techniques to improve thickness distribution of the prosthetic socket by thermal vacuum forming using high density polyethylene (HDPE) plastics.
The high density polyethylene (HDPE) plastics of 38 cm x 40 cm with 7 mm in thickness were fabricated by thermal vacuum forming process. The proposed techniques use pressure different of the inside and outside of closed system (pre-vacuum), causing uniform stress and strain all over the plastic cross sectional area before vacuum forming process. In the experiment, pre-vacuum were applied to produce different heated plastic sag with 0, 1/5, 2/5 and 3/5 of stump length. The fabricated sockets were cut through the middle plane and were measured the thickness along the cutting plane for evaluation.

The plastic around 0-5 cm. of height position is in direct contact with the stump mould. Heat in the plastic was then transferred into the stump mould resulting in higher thickness. The heated plastic sag with 1/5 and 2/5 of stump length can increased the direct contact area with the stump mould and reduce tension in plastic between vacuum forming process. Therefore, the thickness distribution can be improved. However, the thickness heated plastic sag with 3/5 of stump length let the plastic elongate too much before vacuum forming process resulting in less thickness. In conclusion, the proposed technique can improve the thickness distribution of the socket. The heated plastic sag with 2/5 of stump length is the most suitable and provides most uniform condition.
0624
Atila Yilmaz (1) Tuna Orhanli (1) presenting
Thailand, Hacettepe University, Electrical and Electronics Engineering, Ankara (1)
Improving Test Platform for Kinematic Analysis of Above Knee Prostheses
Various mechanically or electronically driven problems may occur during long testing stages and even regular uses during the lifecycle of above knee prostheses. Developing knee prostheses require special tests under some extreme circumstances otherwise difficult even unsafe for human patients before they can be introduced as a prototype. Therefore, many design and development centers may consider allocating a reliable test platform that is inevitable for testing every single components and the functionality of whole system.
The main goal to improve the test platform is to regenerate predefined and controllable periodic movement specifically hip vertical displacement and thigh angle motion applied to above knee prosthesis so that test studies will be less dependent to human trials in any development phase.
The mechanic frame of the proposed test platform has been modified from a simple card drill machine. The system includes two alternative current motors providing two dimensional movements for gait simulation, a rotary encoder, and a pulse counter for each motor control unit, a reducer used for decreasing the speed of the electrical motor to appropriate levels, and driver for motor control. The system is improved by better control unit with software for real-time control and drive requirements. Different gait velocities can be provided through this test platform by adjusting speed and torque parameters manually or by means of software interface. The system will increase its performance with integrated load cells to measure the stance phase reaction force.
Performance tests were conducted with both an image based measurement system (IBMS) and a direct type measurement (DMS) system. In the hip simulator performance evaluation phase, accelerometer and video signals were collected simultaneously from the experimental system for kinematic analysis. The evaluation of generated motions from test platform has been subject to streaming information from two channels gathered by two motion measurement system methods simultaneously.
The graph of the thigh angle signals between the natural gait and simulated gait was shared for image based measurement system (Fig. 1.a) and direct (sensor) measurement system (Fig. 1.b).

a) Knee Angles from IBMS b) Knee angles from DMS
0625
Agnes Sturma (1,2) presenting Tanja Stamm (5,2) Malvina Herceg (4) Oskar Aszmann (1,3)
Turkey, Christian Doppler Laboratory for Restoration of Extremity Function, Medical University of Vienna, Vienna (1) Austria, University of Applied Sciences FH Campus Wien, Vienna (2) Austria, Division of Plastic and Reconstructive Surgery, Medical University of Vienna, Vienna (3) Austria, Department of Physical Medicine and Rehabilitation, Medical University of Vienna, Vienna (4) Austria, Department of Internal Medicine III, Division of Rheumatology, Medical University of Vienna, Vienna (5)
Phantom Limb Pain in patients with high upper limb amputations
Phantom limb pain (PLP) is defined as a painful perception of a limb or parts of a limb that has been amputated and occurs in 50%-80% of all amputees. Although much effort was put in understanding and relieving PLP in the past, neither pharmacological approaches nor psychological interventions have succeeded in improving pain intensity in the majority of affected patients. Since less than 10% of all amputations in Europe account for the upper limb, most of the recent research focuses on the lower limbs and very little is known especially from transhumeral or glenohumeral amputees.
The aim of the study was to explore the occurrence of PLP and contributing factors in people with high arm amputations.
Transhumeral and glenohumeral amputees visiting the “Christian Doppler Laboratory for Restoration of Extremity” at the Medical University of Vienna, Austria, between July 2012 and June 2014 were assessed concerning their PLP. Patients with peripheral nerve injuries or cognitive impairments were excluded. The authors used semi-structured interviews and analyzed them with qualitative content analyses.
17 Men and 5 women were included (age range between 9 and 63 years). Time since amputation was from 3 months to 40 years. 18 amputations were caused by trauma, 3 by tumor and one patient had a congenital absence of the arm. There were 12 transhumeral and 12 glenohumeral amputations (2 patients had bilateral upper arm amputation).
Only 1 of the 22 amputees reported not to feel a phantom limb at all, 16 of them also reported PLP.
PLP was not influenced by the level of amputation and the time since amputation. There were no gender differences. Interestingly, also young patients (e.g. 9 and 16 years of age) reported PLP. A slight tendency was observed to develop PLP when the dominant hand was amputated and if someone else was responsible for the amputation.
Many different types of pain (burn, electric shock, squashing…) and pain triggers (changes in the weather, stress, absence of distraction…) were described by the patients.
Little is known about the occurrence of PLP in high arm amputations. To our knowledge this is the first qualitative study especially focusing on pain perception of transhumeral and glenohumeral amputees. The prevalence of PLP in this sample was 72%, which fits to current literature. However, some patients may have come for consultation because of PLP. This may have caused a selection bias.
Flor, H., Phantom-limb pain: characteristics, causes, and treatment. Lancet Neurol, 2002. 1(3): p. 182-9.
Subedi, B. and Grossberg, G.T., Phantom limb pain: mechanisms and treatment approaches. Pain Res Treat, 2011. p. 86460-5.
0626
Sandra Sexton (1,2) presenting
Austria, Rehabskills Ltd, Wishaw (1) UK, ISPO, Brussels (2)
The impact of training personnel to the minimum standards ISPO Category I and II
Working in partnership with the USAID Leahy War Victims Fund since the 1990s, the International Society for Prosthetics and Orthotics has promoted international standards of professional practice. Today, ISPO has well established professional standards for the clinical personnel who provide prosthetic and orthotic devices as treatment interventions. ISPO certifies these professionals as Prosthetist/Orthotist (ISPO Category I) and Orthopaedic Technologist (ISPO Category II) professionals when they graduate from ISPO evaluated courses.
We wished to determine the impact of training personnel to the minimum standards ISPO Category I & II. Our main interest was to test a hypothesis in developing countries.
Our hypothesis is that “Training personnel to ISPO Category I and II standards provides basic knowledge, skills and experience to enable them to provide and/or improve prosthetic and orthotic services for persons with physical disabilities”.
We developed a causal model and framework of assessment and conducted field visits to thirteen countries. There we listened to service users, hearing the stories of how services had impacted upon their lives. We interviewed Ministry officials, Heads of Hospital Services and Heads of Prosthetic and Orthotic Departments and conducted a partial audit of graduate clinical skills and competencies whilst determining graduate professional development needs.
No matter the country, we found that prosthetic and orthotic provision enabled people with disabilities to have greater independence in their lives. This included accessing all kinds of education and employment.
ISPO Category I and II graduates were found to have a positive impact on access to services. ISPO Category I graduates worked at a more senior level, were able to lead and advise ISPO Category II graduates, and were able to handle more complex cases.
The majority of graduates were able to correctly appraise their own work and knew where improvements could be made. In general the quality of treatment was found to be satisfactory with graduates conducting their professional work to the expected standards.
We found compelling evidence that the ISPO evaluated professional training programs prepare the graduate to provide and/or improve prosthetic and orthotic services. Most importantly, graduates enabled the end user of prosthetic and orthotic devices to be included in and participate in society. ISPO certified graduates were able to demonstrate an appropriate quality of prosthetic/orthotic treatment and recognised where they needed and wanted to develop their professional practice.
WHO/ISPO (2005). Guidelines for training personnel in developing countries for prosthetics and orthotics services: World Health Organization/ISPO ISBN 92 4 159267 2.
0627
Larissa (Conner) Sletto (1) presenting Christopher Robinson (1) Yeongchi Wu (1)
Belgium, Northwestern University Prosthetics-Orthotics Center, Chicago (1)
Dilatancy-Based, Plaster-Less System for Fabricating Ankle Foot Orthoses
There are three methods commonly used by orthotists to take impression for ankle foot orthoses: plaster bandage, fiberglass casting tape, and scanner. A new impression and fabrication technique utilizing the dilatancy principle, initially investigated by WJ Mead1, has been developed and field tested for transtibial prostheses.2, 3, 4, 5 This “plaster-less” dilatancy prosthetic technique has now been modified for orthotic fabrication, as presented here for ankle foot orthoses.
The purpose of this development project was to redesign the dilatancy-based plaster-less transtibial prosthesis impression technique for fabrication of custom ankle foot orthoses.
The development project involved: design of the casting system and fabrication process, laboratory testing using a plaster model, clinical evaluation on consented able-bodied subjects and individuals with disabilities, review of data, and knowledge translation.
The process of taking an impression and converting into a positive sand model is a simple, multi-step procedure utilizing a sand-filled bag in a wood frame. The patient’s limb is placed on top of a plastic bag in the frame and after alignment has been verified, the bag is filled with sand and vacuum is applied. The negative sand mold is then converted to a positive sand model. Modifying the positive sand model by flattening the bottom of the foot, realigning the forefoot-hind foot relationship, or realigning the ankle joint alignment can be done by varying the vacuum pressure. Clinical evaluations on able-bodied subjects and individuals with disabilities have shown promising results for the casting process and fitting comfort of the fabricated orthoses.

This plaster-less system is inexpensive to set up and easy to use. It utilizes plastic bags filled with clean sand in a wood frame for taking impressions and forming positive sand models. The plastic bags are recyclable while the wood casting frame and sand are re-usable, thereby minimizing waste. In short, this “faster, cheaper, and greener” dilatancy-based system is potentially a viable and appropriate technique for use in resource-limited environments.
1. Mead WJ; (1949), U.S. Patent 2,472, 754.
2. ; (2003), Prosthet and Orthot Int, 27:146-152.
3. Jensen, JS; (2005),Prosthet and Orthot Int, 29(2):165-175.
4. ; (2009), Prosthet and Orthot Int, 33(1):1-9.
5. Thanh NH; (2009), Prosthet and Orthot Int, 33(2):130-134.
0629
Kengo Ohnishi (1) presenting Makiko Nakakita (1) Kazuhiro Kawabe (1) Teppei Mochizuki (1) Hibiki Takami (1) Tomoki Mita (2) Takashi Nakamura (2)
Iran, Tokyo Denki Univeristy, Hiki, Saitama (1) Japan, National Rehabilitation Center for Persons with Disabilities, Tokorozawa, Saitama (2)
Inner socket hydrothermal measurement of quasi-transradial prosthetic socket under controlled environmental hydrothermal condition
There are requests from upper limb prosthesis user to reduce the discomfort caused by the heat and humidity within the socket. Heat transmission characteristic of the socket materials are investigated[1] and residual limb temperatures of the lower limb is measured [2], however, very little is reported as systematical evidence on the hydrothermal reaction between the upper limb prosthetic socket and skin surface.
This research targets to measure the temperature and humidity variation inside the socket, when a resin socket is donned on the forearm. Our focus is to prepare instrumentation system and systematically measure the heat transmission characteristic between the skin, socket, and the ambient environment, while non-amputee subjects are donning a socket under a controlled room temperature and humidity.
Quasi-Northwestern type Surlyn sockets were created for each 3 able-bodied subjects (male, aver. 23 S.D.0.8 year-of-age). The digits were contained in a full-extended and adducted posture within the socket. Two temperature sensors, on the palm and forearm, and 2 hydrothermal sensors were mounted on the forearm skin. The socket was donned on the arm and measured in a controlled room temperature and humidity of 3 conditions: 20, 25, and 30 deg.C., at 38%R.H. The subjects were seated at resting condition with the socket worn forearm resting on an insulated tabletop. The sensor signals were sampled for 30 minute at 100Hz period and outer socket surface temperature image were captured with infrared radiometry camera at 5-minute interval. An approved University and Institute Human Subjects Review Committee protocol was followed for consent.
Figure shows the result of the 3 room temperature condition. The plotted data of the skin surface temperature were computed by spatially and temporally averaging the intersubject average of every 100 msec. The outer socket surface temperatures are intersubject average. The increasing rates of skin surface temperature changed after 500 sec., while the outer socket surface temperatures’ rates decreased between 300 and 600 sec. in all 3 room temperature conditions. The humidity gradually increased in the socket and reached 100%R.H. for 30 deg.C., and 90%R.H. for 20 and 25 deg.C.

The greater slant of temperature rise of the skin and outer socket surface before 500 sec. indicate that the heat transfer in this phase is to warm the socket. The temperature difference between the skin and outer socket surface of the post 500 sec. phase gradually decreases, indicating that the heat transfer to warm the socket has saturated. This 500 sec. period is similar to the residual limb temperature variation of the transtibial socket [2], yet the increased skin temperature in the able-body subject’s upper limb were different then the decreased case of lower residual limb. Further experiments are required on transradial amputee, under different socket, environmental, limb posture and activity conditions.
0630
Melissa Evangelista (1) Paul Pasquina (2) Paul Demers (1) presenting
Japan, Alfred Mann Foundation, Santa Clarita (1) USA, Walter Reed National Military Medical Center, Bethesda (2)
Clinical Demonstration of Prosthetic Control Using Implantable Myoelectric Sensors
Advanced myoelectric prosthetic arms are currently controlled using EMG signals recorded by surface electrodes. Limitations of surface electrodes include inconsistent and unreliable signals, particularly when there is poor skin contact, socket movement, or residual limb sweating. In addition, surface electrodes are unable to record signals from deeper muscles, thereby limiting their ability to capture user intent. More sophisticated prosthetic devices require a stable, reliable, and intuitive control interface between the user and terminal device to improve prosthetic function. Implantable Myoelectric Sensors (IMES®) are small electrodes that can be placed within residual limb muscles to detect EMG activity and wirelessly transmit these signals to control a prosthetic hand. The implanted electrodes are powered via an electromagnetic coil built into the prosthetic socket and are able to record signals from multiple residual limb muscles, enabling more intuitive, simultaneous control over multiple degrees of freedom.
To demonstrate the feasibility of using the IMES® System in three individuals with transradial amputation to provide intuitive simultaneous control a 3-Degree of Freedom biomechanical upper limb prosthesis.
Prospective, non-blinded, single group, interventional, three subject feasibility study conducted at a single investigational site, the Walter Reed National Military Medical Center. Once subjects recover from surgical implantation of IMES, they practice IMES control using a bench-top IMES trainer for approximately a month. As soon as the subject’s custom–fit IMES Prosthesis is available, it is fitted and programmed. Subjects then begin six months of prosthetic training. After training, subjects are given the option to continue using their IMES Prosthesis for another sixteen months. The usability and functionality of the prosthetic system is evaluated throughout the study using standard measures.
Three subjects have been enrolled and implanted without complication. The first subject has used the IMES system for a year and a half and demonstrated good initial control that continues to improve with time and training. The second subject has used the IMES System for more than six months. This subject shows good control over prosthetic wrist and finger function, but struggles with control over prosthetic thumb movement. The third subject was recently implanted and will initiate prosthetic training in the next few weeks.
At present, the limitation of advanced myoelectric prostheses is not their ability to reproduce near-normal human function, but rather their inability to control the multitude of actions they are capable of in a natural and repeatable way. A core issue is extracting multi-channel biological signals that are stable and reliable over long periods of time. Implanted electrodes present a potential solution.
631
Michelle Hall (1) presenting Michael Schwartz (1)
USA, Gillette Children’s Specialty Healthcare, St. Paul, Minnesota (1)
Comparison of the Barefoot and AFO Margins of Stability in Children with Cerebral Palsy Diplegia
1. Hsue BJ, Miller F, Su FC. “They dynamic balance of the children with cerebral palsy and typically developing during gait. Part I: Spatial relationship between COM and COP trajectories.” Gait & Posture. 2009; 29: 465-470.
2. Hof AL, Gazendam MGJ, Sinke WE. “The condition for dynamic stability.” Journal of Biomechanics. 2005; 38: 1-8.
632
Salomé Silva (1) Ana Margarida Rodrigues (1) Fani Ferreira (1) Samanta Pacheco (1) José Pedro Matos (1) presenting
USA, ESTeSL, Lisboa (1)
Professional situation of the graduates in Orthotics and Prosthetics in ESTeSL since 2004/2005 to 2012/2013 – Sociological Portrait
The Orthopedics is a degree with a recent academic history and hence with a weak knowledge of the labor market. The uncertainty experienced by newly graduated after completion of degree led to the need to deepen the existing employability. The Diagnostic and Therapeutic Technicians is defined as a young professional, which in the Portuguese market, the major employer is the National Health Service, however in the case of orthopedics this is referred to as a minority employer.
Make a sociological portrait of the population of the graduated population in Orthotics and Prosthetics in Escola Superior de Tecnologia da Saúde de Lisboa (ESTeSL), serving as reflection about employability of this technicians.
The research is part of a descriptive study using a questionnaire, a total of 22 questions. Those were applied using the LimeSurvey® software.
In order to implement the questionnaire to the graduates there was a collection of electronic mail for which would be sent the access link. In a universe of 150 graduates in ESTeSL, the questionnaire was sent to 140 (93,3%). The response period was between June 11 and July 25 of 2014.
There was a return of 103 questionnaires, of which 11 were incomplete.
Only 92 were considered completed and used for statistics - these represent approximately 61% of all licensed formed by ESTeSL.
Most of the population of graduates surveyed are young – 57.6% are between 25 and 30 years, there are more graduates females than males. The males graduates takes less time in getting their first job than women’s. 78.3% of the graduates are working on orthopaedics area and the unemployment rate stands at 8.7%.
Only 17% of respondents were or are in the course of a graduation. The major employer are orthopaedic (private companies) - 63.1%. Of the total population surveyed, 41.7% had internship experience abroad, in Spain or Finland, either exclusivity or together with one semester internship in Portugal.
It is also noted that most of the graduates who had internship abroad, had exercised his first job also there.
The emigration of graduates represents 16.7% of the total, leading to the concept of “brain drain”.
Getting the first job requires a search up to six months, which is lower search time among males . There is a direct relationship and a confirmation that the academic internship abroad can influence the permanence and getting their first job also abroad. From all the graduates surveyed, 41,7% had internship experience abroad.
Unlike most health courses, the National Health Service proves to be a minority employer this sample.
633
Stefan Salminger (1) presenting Aidan Roche (1) Agnes Sturma (1) Marina Ninkovic (2) Gerhard Pierer (3) Adam Chelmonski (4) Jerzy Jablecki (4) Oskar Aszmann (1)
Portugal, Christian Doppler Laboratory for Restoration of Extremity Function Division of Plastic and Reconstructive Surgery, Department of Surgery, Vienna (1) Austria, Department of Physical Medicine and Rehabilitation, Medical University of Innsbruck, Innsbruck (2) Austria, Department of Plastic and Reconstructive Surgery, Medical University Innsbruck, Innsbruck (3) Austria, Hand Trauma Center St. Hedwigs’s Hospital, Trzebnica (4)
Hand transplantation compared with prosthetic reconstruction in below elbow amputees: an investigational study of functional outcomes
Composite tissue transplantation and improvements in the field of prosthetics have opened new frontiers in restoring hand function in upper limb amputees. These two concepts aim at supporting amputees in their daily life, however, the indications, advantages and limitations for each treatment must be carefully considered depending on level and extent of amputation. Here we report our findings of a multi-center study comparing hand function of transplanted and prosthetic hands.
To compare functional outcomes of hand transplantation with that of prosthetic reconstruction using standardised objective hand function tests.
12 patients aged 22-60 years with either hand transplant (n=5) or prosthetic reconstruction (n=7) after bi- (n=2) or unilateral (n=10) amputation below the elbow were enrolled in this study.
The global extremity function of all patients was tested with Action Research Arm Test (ARAT), Southampton Hand Assessment Procedure (SHAP) and the Disabilities of the Arm, Shoulder and Hand measure (DASH) and the results of both groups compared.
The transplanted patients achieved a mean ARAT score of 40.86 ± 8.07 out of 57 and an average SHAP score of 75 ± 11.06 points. In comparison, prosthetic patients achieved a mean ARAT score of 39 ± 3.61 out of 57 and an average SHAP score of 75.43 ± 10.81 points. No significant difference between transplanted and prosthetic hands in ARAT and SHAP could be identified. In unilateral patients, the reconstructed hand (transplant and prosthetic) could achieve a score of 76.45% in SHAP and 69.12% in ARAT in relation to their healthy hand.
The indications for hand transplantation and prosthetic reconstruction in below elbow amputees must be carefully weighed for each patient. As the functional outcomes were not significantly different between the two groups, treatment should be guided by what exposes the patient to the least harm. Due to the side effects of immunosuppression the indication for allotransplantation must still be restrictive, the best being bilateral amputees.
634
Roger V. Gonzalez (1,2) presenting Aaron Nystrom (1,2)
Austria, The University of Texas at El Paso, El Paso, TX (1) USA, LIMBS International, El Paso, TX (2)
Improving Prosthetic Outcomes in the Developing World Through a Complete Transfemoral System
Since 2004, researchers with LIMBS International (formerly LEGS) have been developing locally sustainable prosthetic knee and foot components with high levels of functionality for amputees in the developing world. While these components are the cornerstones of a successful transfemoral prosthetic device, on their own they cannot meet the needs of amputees and prosthetists in countries with limited resources. There is a great need throughout the developing world for appropriate systems that include a pylon and quality adapters.
LIMBS has created the LIMBox, a complete transfemoral prosthetic leg system to meet the needs of the developing world. Deployment of the LIMBox has begun with ongoing review of the system planned in key countries of Asia.
A survey of prosthetic solutions for trans-femoral amputees in developing countries indicates that most options currently available are poorly engineered with inadequate incorporation of basic biomechanical principles for the attainment of high quality gait outcomes. A number of efforts have been made to meet those needs through improved knee and foot components, but without a complete integrated system the parts cannot be used by those for whom they are intended. The development of the LIMBox seeks to fill the gap between providing clinics with appropriate components and fitting amputees with a quality prosthesis.
The LIMBS Knee is a 4-bar polycentric knee specifically designed for implementation in the developing world [1] with proven beneficial outcomes in patient functionality [2]. LIMBS is now manufacturing an injection molded version of the knee that builds on the success of the M3 knee while adding functionality, cosmetic appeal, and a K2 rating. This will allow an increase in production and economies of scale backed by standards that far exceed common practice in the target market environment. The LIMBox combines proven knee technology with the low cost, durable, energy recovery Niagara foot and a high quality set of adapters to create a complete system to meet the needs of the most demanding environments in the world’s poorest countries.
To date, the LIMBox has been deployed in Bangladesh, Mexico, Guatemala, Philippines, and Kenya and has proved to be a very successful high-quality, affordable leg system. With additional deployment of the system planned throughout SE Asia and Africa, the LIMBox is expected to continue improving the efforts of LIMBS to restore mobility to the world’s neediest amputees.
[1] Ayers, S., et al. (2006). Journal of Biomechanics
[2] Rispin, K., et al. (2010) 13th World Congress of the ISPO.
635
Joshua Bowen (1,2) Roger V. Gonzalez (1,2) presenting
USA, The University of Texas at El Paso, El Paso, TX (1) USA, LIMBS International, El Paso, TX (2)
Development of a Variable Stiffness Locally Adjustable and Repairable Low-Cost Energy Storage and Return Carbon Fiber Prosthetic Foot: A Feasibility Study
Modern advances in prosthetic technology in the Developed World have significantly outpaced technology in the Developing World, where nearly 30 million people need a prosthetic device [1]. Prosthetic technology available in the Developing World often does not meet international test standards and fails to meet specific challenges of the developing world, especially regarding reliability, reparability, and patient-specificity [2].
The goal of this study was to demonstrate the feasibility of a low-cost (materials less than $100), tunable (patient-specific), repairable, modular composite prosthetic foot that passes static ISO standard tests.
The prosthetic foot was manufactured from plain weave 3k carbon fiber fabric and laminated together with AdTech 820 epoxy with medium hardener using compression molds. Once cured, components were trimmed and sanded to their final sizes. Three different toe layers were developed with high, intermediate and low stiffness levels. The overall stiffness of the foot was varied by assembling the toe section using different combinations of layers. Static Proof and Ultimate tests were performed with a foot consisting of the three layer types. Two subject case studies were conducted to assess the foot’s performance during gait.
The foot was built using approximately $73.00 of materials and 12 man hours to manufacture. Three toe layers could be interchanged using varying stiffness levels in order to change the overall stiffness of the foot. Two feet underwent testing and withstood the static proof and ultimate test loads with no visual damage. In the subject trials, changes in temporal parameters and variations in ground reaction forces were within the expected values. Walking in the prototype compared to their standard foot, both subjects’ changes were less than 3% - within 7% changes observed from altering foot stiffness within ESAR feet [3]. The subjects’ qualitative evaluation of the foot was similar, citing that the prototype was noticeably lighter and toe stiffness felt adequate although it was less stiff than their standard foot.
This study demonstrates the feasibility of manufacturing a low-cost, tunable, modular prosthetic foot that passes ISO static test. The prototype passed the ISO static tests while allowing the stiffness to be tailored and the components to be replaceable without the need for specialty tools or the need to realign the prosthesis. The modularity of the prototype enables field repairs and maintenance to occur without the need for a highly-trained clinician benefitting patients living in rural areas.
[1] WHO (2005). Guidelines for training personnel in developing countries for P&O services.
[2] Cummings, D. (1996). Prosthetics and Orthotics International.
[3] South, B. J., et. al. (2010). Journal of Biomechanical Engineering.
636
Heinz Trebbin (1) presenting Stacey Hildebrand (2) Christopher Wilson (2) Greg Esau (2,3) Tim Bryant (2,3)
USA, DOI ortho-innovativ GmbH, Kempten (1) Germany, Queen’s University, Kingston, ON (2) Canada, Kingston General Hospital, Kingston, ON (3)
Development of a Clinical Protocol for Fitting a Modifiable Foot Keel

637
J. Chad Duncan (1) presenting
Canada, Alabama State University, Montgomery, Alabama (1)
Effect of prosthetic intervention on activities of daily living, balance, health status, and patient self-efficacy in individuals with Type II diabetes who have had a unilateral transtibial amputation secondary to the disease
Historically prosthetic patient management has not been quantified nor based on any specific outcome measure. Self-efficacy has been used in cardiac surgery to assist in prediction and intervention of patient care. With outcome measure being more and more prevalent a systematic and thoughtful application is needed in the field of prosthetic and orthotics.
To determine what outcomes are best to assist in developing effective interventions and patient management among individuals with Type-II diabetes with unilateral trans-tibial amputation.
Certified Prosthetic clinician assessed balance and activity of new unilateral trans-tibial amputee due to diabetes using the Activities-Specific Balance Confidence Scale (ABC) and Timed Up and Go (TUG), Lower Extremity Functional Scale (LEFS), Patient Reported Outcome Measurement Information System (PROMIS-29) and the General Self-Efficacy Scale (GSE) assessments at the times provided below:
Data collection using battery of assessments (ABC, TUG, LEFS, PROMIS-29, and GSE) at initial consultation, delivery (week 6-7), post delivery (weeks 7-9), and post-delivery (weeks 11-15) were explored.
The pilot-study sample (N=10) was primarily African-American (90%) and Caucasion (10%) with a mean age of 62.2 years and mean weight of 231.3 pounds. Gender was evenly divided into Female(N=5)and Male(N=5). The mean height of subjects was 5 feet 6 inches. At pre-delivery GSE score was 37.3 while the PROMIS-29 was 29 (below-average) with standard error of 4.2. At delivery the GSE score was 36.3. One week post delivery (N=2) the average ABC score 34 %, the LEFS score 25, and GSE 33.5.
Preliminary data shows individuals GSE, ABC, and LEFS scores increase during the process of obtaining a prosthesis. Patient’s who reported high indicative pain and low GSE scores tend to score low on ABC, LEFS and TUG throughout the process. It may suggest that individuals with low GSE scores may need targeted interventions than individuals with high GSE scores. More data needs to be collected to confirm current findings.
O’Neil, A., Berk, M., Davis, J., & Stafford, L.(2013). Cardiac-self efficacy predicts adverse outcomes in coronary artery disease (CAD) patients. Vol. 5, No.7A3, 6-14 Creative Commons http://dx.doi.org/10.4236/health.2013.57A3002
Schwarzer, R., & Jerusalem, M. (1995). Generalized Self-Efficacy scale. In J. Weinman, S. Wright, & M. Johnston, Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35-37). Windsor, England: NFER-NELSON
Web sites :
http://www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=949 http://www.physio-pedia.com/Lower_Extremity_Functional_Scale_(LEFS)
http://www.rehabmeasures.org/PDF%20Library/Timed%20Up%20and%20Go%20Test%20Instructions.pdf http://www.nihpromis.org
638
Michaela M. Pinter (1) presenting Othmar Schuhfried (2)
USA, Danube-University, Krems (1) Austria, Medical University Vienna, Vienna (2)
Predictor for positive response to a selective implanted drop foot stimulator (ActiGait) post stroke
Drop-foot is a common problem following stroke. Functional electrical stimulation is one intervention that is used to stimulate the ankle dorsiflexor muscles during the swing phase to correct drop-foot. Recent studies indicate that functional electrical stimulation of the peroneal nerve with a selective implantable stimulator (ActiGait) is an effective intervention in improving functional gait outcomes in the chronic stroke population.
The aim of this study was to investigate the extent to which functional electrical stimulation with surface electrodes can predict the functional effect of ActiGait stimulation.
Ten post-stroke hemiplegic patients were included in this study. Functional electrical stimulation was delivered to the peroneal nerve during the swing phase via single foot switch in combination with surface electrode or implanted stimulator. Kinematic data were collected using a computerized motion analysis system with force plate. Data of functional electrical stimulation with surface electrode (FES) and with selective implantable stimulator (ActiGait) group were compared among each other. In order to examine the relationship between kinematic data under FES and ActiGait a ranked correlation, respectively a Pearson correlation was computed.
In all patients preoperative FES was applied for a period of at least 3 months. The evaluation of the functional outcomes among ActiGait stimulation followed at 6 months after activation of the implant. Improvements were seen in all gait parameters under stimulation with both FES and with ActiGait, even if no statistically significant differences in improvements could be detected between the two stimulation modalities (Table 1).
Temporal data during gait cycle

To investigate the effect of FES as a predictor of the effect of ActiGait stimulation, a Pearson correlation was expected between individual kinematic parameter. There was found a close correlation with the kinematic data between FES preoperatively and ActiGait stimulation 6 months after activation of the implant (r=0.81, p<0.001).
In the preliminary study, we showed that FES with surface electrodes can very well serve as a predictor of functional outcome of ActiGait stimulation. In light of these results, we see it as essential to perform FES with surface electrodes for a period of at least 1 month prior to implantation of the ActiGait system.
641
Jacinte Bleau (1,2) presenting Stephane Savard (2) Sebastien Hinse (1)
USA, Medicus, Montreal, Quebec (1) Canada, Savard Ortho Confort, Quebec, Quebec (2)
A new approach for the treatment of drop foot
There is a need for a new type of ankle and foot orthosis that could allow drop foot patients to remain active and participate in sports and physical activities. Such an orthosis would have to be resistant enough to sustain larger constrains created by higher intensity activities. No available studies have estimated the resistance of materials used in the design of conventional ankle and foot orthoses for the treatment of drop foot.
This study aims at testing the resistance of material of an ankle and foot orthosis used in the treatment of drop foot. Specifically, the study will verify the number of cycles of flexion and extension at the ankle joint before breakage of material.
A test bench was created to verify the resistance of the TurboMed ankle and foot orthosis. The test bench was conceived and fabricated in order to simulate ankle joint flexion and extension movements at variable angular velocities, according to technical and morphological data of the subject. The test was realized at a simulated running speed of 4 min/km, a stride length of 1.4m, an angular range of 47° and a room temperature of 20.4°C at the beginning of testing. These parameters represent a number of 90 cycles per minutes for the displacements of the air cylinder.
The average number of cycles per minute was estimated at 91.4. This would represent an average running speed of 15.2km/h. A first breakage of material (figure 1) representing 4/5 of the diameter of the rod was observed after 179.1 hours of testing, which represents a number of 977988 cycles and a running distance of 2738.4 km. The test was pursued until complete breakage of the rod, which occurred after 193.7 hours of testing, representing 1059209 cycles and a running distance of 2965.8 km. At that time, the test was stopped, since breakage was sufficient to impair proper functioning of the orthosis. No changes in color or properties of the orthosis were noticed other than those observed at breakage point.

Breakage point.
The TurboMed orthosis was designed to allow patients with drop foot to practice in more intense physical activity or return to a physical activity level that was existent before the presence of drop foot. After verification of resistance of the material composing the rod of the orthosis, it was concluded that breakage first occurs after 977988 cycles of flexion and extension at the ankle joint and complete breakage of the rod occurs at 1059209 cycles.
642
Stacey Hildebrand (1) Matthew Faris (1,3) Martin Robertson (4,1) Qingguo Li (1,2) Tim Bryant (1,2) presenting
Canada, Queen’s University, Kingston, ON (1) Canada, Kingston General Hospital, Kingston, ON (2) Canada, St. Mary’s of the Lake Hospital, Kingston, ON (3) Canada, Motion Specialities, Kingston, ON (4)
Ground Reaction Force and Shank Angle Waveforms for Prosthetic Foot Mechanical Characterization


[2] Haberman, A (2008). Mechanical properties of dynamic energy return prosthetic feet. M.Sc. Thesis, Queen’s University, Kingston, ON, Canada.
643
Kengo Ohnishi (1) presenting Fumiya Takemasa (1) Hibiki Takami (1)
Canada, Tokyo Denki Univeristy, Hiki, Saitama (1)
Development of baseball fielding terminal device for bilateral upper limb amputee
Baseball is one of the popular recreations for persons with disability in Japan to participate and improve the physical ability and regain confidence through team play. Clamp-like terminal devices to fit a glove on or a Lacrosse cross-shaped terminal device for catching a ball is developed for use of unilateral upper limb amputee. However, the function of these terminal devices is limited to catching.
The aim of the project was to design a new device with catching and throwing function to meet the requirements for a bilateral upper limb amputee with a single arm with short transradial residual limb.
Impact absorption of 20 m free-fall of a 72 mm in diameter, 135-gram rubber baseball and stiffness to throw a baseball in the target direction and distance, 30 m, were set as design specification. The arm motion for catching and throwing were set to shoulder and elbow motion in anteroposterior direction in a sagittal plane since the pronation-supination could not captured in the short residual limb. Therefore, the device is designed to function in sequential series of underarm catching motion, and underarm throwing motion. Further requirements were weather resistance, dust tightness, easy maintenance and low cost to meet the durability of 1-year outdoor use.
A Lacrosse cross-shape frame of overall length 430 mm and width 150 mm was produced by defroming 114-mm diameter rigid polyvinyl chloride plastic thin-wall pipe. The natural rubber belt and flexible polyurethane form sheet was used to compose a cross-type web of a baseball glove and attached to the frame with a nylon banding band. To increase impact absorbtion function, a natural rubber belt loops were attatched on the frame aroud the pocket of the web. Eight prototypes were systematically created toexperimentally investigate and optimize the shock absorbing effect . Two prototype inheriting the dimentions of shock absorption design with different stiffness property were produced, and tested for the catching and throwing function by a able-body subject. As for the test result, the stiffer prototype had a better performance and the average stabilization time of 4-m ball drop catch was 0.48 sec. and the average throw distance with upper extrimity motion was 18m.

Test result indicate that the device needs further modification to meet the specification. However, the performance of the device is dependent on the user’s physical ability and skills gained by repeated pratice, and therefore, the device should be practicle at the current condition for higher physical ability amputees. Meanwhile, the test was conducted by a single able-body subject and further testing is required.
644
Arun Jayaraman (1,2) presenting Susan Deems-Dluhy (1) Luca Lonini (2) Shenan Hoppe-Ludwig (1,2)
Japan, Rehabilitation Institute of Chicago, Chicago, IL (1) USA, Northwestern University, Chicago, IL (2)
Micro-processor controlled Knee-Ankle-Foot Orthosis (C-Brace) vs. Stance-control Knee-Ankle-Foot Orthosis (SCO) and conventional Knee-Ankle-Foot Orthosis (KAFO): Functional Outcomes in Individuals with Lower Extremity Impairments due to Neurologic or Neuromuscular Disease, Orthopedic Disease or Trauma
645
Sydney Low (1) Stacey Hildebrand (1) Tim Bryant (1,2) presenting
USA, Queen’s University, Kingston, ON (1) Canada, Kingston General Hospital, Kingston, ON (2)
Effect of Cosmetic Cover on Mechanical Properties of a Prosthetic Foot System


648
Thomas Schmalz (1) presenting Eva Pröbsting (2) Hartmut Stinus (3) Andreas Kannenberg (2)
USA, Otto Bock Competence Centre, Göttingen, Göttingen (1) Germany, Otto Bock Healthcare Products GmbH, Clinical Research & Services, Vienna (2) Austria, Orthopaedicum Northeim-Göttingen, Northeim (3)
A randomized controlled cross-over trial to investigate locomotor capacities when using an electronic stance control orthosis
The functional disadvantages of locked KAFOs [1] have been significantly reduced with the development of stance control orthoses (SCO). E-MAG Active is a SCO system comprising a double sensor system, a gyroscope, an accelerometer, a microprocessor and an electromagnetic locking system. E-Mag Active has been CE marked since 2008 and routinely used for subjects with lower limb paralysis. The patient benefits of the device have not yet been studied.
To demonstrate the biomechanical and clinical patient benefits of the stance control mode of E-MAG Active as compared to the locked knee mode .
The study was approved by the ethics committee of the medical doctors association of the federal state of Niedersachsen, Germany. Subjects actively using E-MAG Active were invited to participate in the study by their orthotist. After baseline assessment (QUEST), subjects were randomized to perform a 6MWT and gait analysis with the orthosis in either the locked or unlocked (stance control) mode. After 2hrs of rest, a crossover of the device condition was performed. For gait analysis, an optoelectronic camera system (17 passive markers, 12 Bonita cameras, VICONPEAK, Oxford, GB) coupled to two force plates (9287A, KISTLER, Winterthur, CH) was used. Kinematics of the lower limb joints and the external joint moments were used as specific evaluation parameters.
8 subjects (5 male) were enrolled, mean age 46 ± 20ys. Indications included incomplete spinal cord injury (3), poliomyelitis (2) and muscular disease (1). Two subjects were excluded as they were unable to perform the functional measurements. The subjects’ satisfaction with the everyday use of the device ranged from 3.9 (safety) to 4.9 (Follow-up service). In the locked mode, patients walked a significantly shorter distance in the 6MWT with 298,7 ± 54,3m as compared to 338,9 ± 48,5m in the unlocked (stance control) mode (p ≤ 0.05).
In the SCO mode, subjects walked with a significantly higher speed (0.94 vs 0.88 m/s, p ≤ 0.05) and showed a tendency to reduced step length asymmetry (difference between the step length on the orthotic and sound side: 0.03 vs 0.05 m). A mean swing phase knee flexion angle of 56 ± 16° was measured for the SCO mode. During the complete stance phase, higher external joint moments acting on the sound side ankle, knee and hip joint were measured when walking with the locked knee joint.
Subjects showed a high level of satisfaction with their stance control orthoses. The functional assessment showed a significant improvement in locomotive capabilities as confirmed by joint kinematics and kinetics as well as the distance walked the 6MWT when subjects were used the unlocked mode. The study confirms that E-MAG Active provides functional benefits over locked KAFO’s.
[1] B. Zacharias, A. Kannenberg, Clinical benefits of Stance Control Orthosis Systems: An analysis of the Scientific Literature, JPO 2012; Vol 24, Num1; p 2
649
Maurizio Petrarca (1) presenting Enrico Castelli (1)
Germany, Bambino Gesù - Children’s Hospital, Palidoro, Rome (1)
The next step will leave the print: towards a new generation of robotized orthosis for gait recovery
Elastic components can be utilized for the functional recovery of gait [1] The coupling of elastic components with tunable stiffness allows the realization of dynamic personalized orthosis with variable joint rest point and tunable stiffness [2]. This orthosis has a main limitation: it is impossible to set different rest point and stiffness in the different functional phase. Robotic device seem to offer the opportunity to overcome this limitation [3], but remain unclear the success of these device for improving the function.
The aim of the present project is to individuate the critical correction needed for the gait reeducation and the development of a new generation of smart orthosis.
In this abstract is illustrated the use of two different orthoses one applied to the knee (a dynamic device with elastic component [2]) on a child ( age 7 years) with hemiplegia as a consequence of a CP and the other applied to the ankle (a motorized device [3] on a child (age 9 years) with hemiplegia acquired after a TBI. In the first case the orthosis was set in order to control the knee hyper extension in stance. In the second case the orthosis was utilized to control the increased plantar flexion at the contact with the terrain, i.e. for the recovery of the ankle first rocker. Gait analyses were conducted with an opto-electronic system (Vicon MX).

In the figures are shown the correction induced on the two joints during gait. D illustrates the knee flexion extension of the child with CP, gray band – control, black line – free walking and dotted line – walking with the elastic component. a, b, c, illustrate the free walking of the child with TBI. a, gray band – control, black line – free walking and gray line contralateral ankle. b, the same of a, but with traditional ankle orthosis. c, the same of a, but with robotic orthosis. The arrows illustrates a voluntary induced instability (functional to motor learning principles) realized introducing a spring between the actuator and the joint of the orthosis. Both orthosis improved walking velocity (CP from 0.8 m/s to 1.0 m/s and TBI from 1.0 m/s to 1.2 m/s)
Dynamic orthosis with tuneable both rest position and stiffness, can be utilized in order to manufacture personalized orthoses able to determine specific gait corrections that can follow and drive the function maturation in child, tuning the orthosis rest position and stiffness. This perspective can really open the path for a new generation of modular and personalized devices for gait recovery and support.
[1] Petrarca M, et al. Gait Posture 2009;29(January (S1)):e28–9. [2] Petrarca M, et al. Gait Posture 2011;33S:S7–9.[3] Petrarca M, et al. Gait & Posture 40 (2014) S1–S31.
650
Yvette Kerkum (1) presenting Merel-Anne Brehm (1) Josien van den Noort (1) Jules Becher (1) Annemieke Buizer (1) Jaap Harlaar (1)
Department of Rehabilitation Medicine, MOVE Research Institute Amsterdam, VU University Medical Center, Amsterdam (1)
A spring-hinged Ankle Foot Orthosis can normalize knee kinematics and kinetics while preserving push-off power in children with Cerebral Palsy
Mean (SE) gait parameters, net EC and walking speed for different walking conditions (N=14).

s,r and h represent shoes only, rigid AFO and hinged AFO resp.
3 Kerkum et al. (2014), J Appl Biomech.
651
Seema Radhakrishnan (1,3) Friedbert Kohler (1,2) presenting Carolina Schiacappasse (4) Veronica Fialka-Moser (5) Jianin Li (6) Christoph Gutenbrunner (7) Arun Jayaraman (8)
Mobility post amputation from patient’s perspective: An International comparison using the International Classification of Function, health and disability(ICF)
Amputation of the lower limb results in limitations in mobility which are amenable to multiple rehabilitation interventions. The participation restrictions as a result of lower limb amputations may vary significantly depending on the etiology of amputation, geographic location and socioeconomic situation of the amputee. The International Classification of Function, health and disability (ICF) provides a common language that may be used to compare the function of amputees a across various countries and cultures .
To compare the concepts in mobility important to persons with lower limb amputation across six countries using ICF
Focus groups and individual interviews of persons with lower limb amputation were done across six countries to identify the issues faced by patients with an amputation during and after their amputation, subsequent rehabilitation, and on an ongoing basis. Meaningful concepts from these focus groups and individual interviews were extracted from the responses and linked to suitable 2nd level and where applicable 3rd level ICF categories. ICF categorical frequency analysis was performed to determine the prevalence and spread of ICF categories by location.
133 patients were interviewed..93percent of the concepts could be matched to ICF categories for quantitative analysis. The concepts in activity and participation that were important to the participants included walking especially walking on different surfaces, climbing, moving around with equipment, driving using transportation, washing self and doing house work. There was a difference in the frequency with which these concepts were recorded between individual countries. Assisstive devices including prosthesis, walking aids and wheelchairs, as well as design of public and private buildings were identified as facilitators or barriers to mobility
The important concepts in mobility were similar across the different countries. Some mobility concepts, like squatting in China and climbing mountains in Argentina,. varied between countries The People living in remote towns had less access to suitable services and either had to relocate or travel long distances to access appropriate prosthetic services. This was true across all countries. The comprehensiveness of ICF as a classification system for human function and its universality across the globe is demonstrated by the huge proportion of the concepts contained in the interviews from across the study centres that could be matched to ICF categories
The International Classification of Functioning, Disability and Health (ICF). Geneva: WHO. 2001: World Health Organisation.
652
Paul Charlton (1) presenting
USA, Peacocks Medical Group, Newcastle upon Tyne (1)
The use of KAFOs for management of Inclusion Body Myositis (IBM)
Often the use of KAFOs with gross global weakness is discarded as many consider weight and impact on function to be to great
The presentation will consider how assessment and intervention may be introduced to these patients as well as biomechanical needs, careful orthotic design and material selection.
The aim of this paper is to highlight the problems associated with any orthotic intervention in this debilitating condition and the considerable benefits if successful
Beginning with a description of the disease and resulting changes in biomechanical demands imposed. The presentation will then show by means of a case study the need to balance intervention whilst allowing other necessary compensations to optimize function.
Outcomes include biomechanical changes from gait analysis and the effect on ground reaction force vector. A reduction in visual analogue pain score from 9 to 2, medication change and interview.
This presentation raises the need to consider the psychological aspect of intervention as well as ethical considerations. The paper also questions how such help can be made more readily accessible to those who may benefit
Whilst the presentation is specific to IBM; the principles could be extrapolated to any condition resulting in global weakness