
Abstract
Background:
Hallux limitus is one of the most common disorders affecting foot biomechanics. Custom-made foot orthoses can improve the function of the first metatarso-phalangeal joint.
Objectives:
The objective underlying this study was to test whether custom-made foot orthoses increased the range of mobility of metatarso-phalangeal joint in patients with hallux limitus.
Study design:
Randomized, double-blinded, and clinical trial.
Methods:
The study consisted of 20 participants (40 feet) diagnosed with hallux limitus. A control group and an experimental group both wore the same custom-made foot orthoses and, in the experimental group, a support element under the first metatarso-phalangeal joint was added to the orthoses. Two measurements were made with both groups: the relaxed position of the first metatarso-phalangeal joint and the maximum extension of the hallux. These measurements were made before first placing the foot orthoses and 6 months after application of the treatment.
Results:
In the experimental group, the results showed an improvement of 4.5° in the relaxed position and 22.2° in the maximum extension being statistically significant (p < 0.001) for both measurements.
Conclusion:
Custom-made foot orthoses with added support under the first metatarso-phalangeal joint were proved to be an effective treatment to restore functionality of this joint in hallux limitus patients.
Clinical relevance
Limitation of hallux movement in the joints propulsive phase of gait negatively affects the biomechanics of the lower extremity, causing changes in the rest of the joins. The use of foot orthoses designed in this study restores range of motion of the first metatarso-phalangeal joint.
Background
Over the years, many authors have proposed values for what should be the normal range of mobility of the first metatarso-phalangeal joint (MPJ) in the sagittal plane. It is known that a minimum of 60°–65° metatarso-phalangeal extension is required in the propulsion phase for gait to develop normally.1–11
There are several biomechanical and morphological factors that can adversely affect the normal function of the first MPJ and reduce the range of extension of the hallux. These factors are as follows: retraction of the plantar soft tissue extending to the transversal axis of the first MPJ; 12 a dorsiflexed first ray or metatarsus primus elevates 13 and hypermobility of the first ray (these last two abnormalities cause first ray insufficiency); alterations in the length of the first metatarsal; an excessively long hallux; alterations of the gleno-sesamoid system; square, or square with central ridge, first metatarsal head 14 and insufficiency of the peroneus longus muscle (PLM). 15
Even quite recently, a new perspective on the etiology of hallux limitus (HL) has been provided in the demonstration of a relationship between this pathology and a reduced capacity for internal rotation of the lower limb by Lafuente et al. 16 Moreover, it is noticed that the most important of the phases of the gait cycle is the propulsive phase of toeoff, thus the load capacity of the first metatarsal and the extensor capacity of the hallux. To produce adequate plantarflexion of the first metatarsal during this phase, it is important that there be proper functioning of the PLM which, as it is known, is inserted into the plantar aspect of the first cuneiform and the base of the first metatarsal.17,18 Therefore, insufficiency of this muscle in the propulsive phase will entail improper loading of the first metatarsal on the ground.
If the subtalar joint experiences a movement of excessive pronation during the stance phase of gait, as is regularly the case in individuals with HL, 19 part of the mechanical advantage provided by the spatial arrangement of the PLM tendon is lost. From a frontal view, the distance between the ground and the passage of the PLM tendon through the cuboid canal in normal conditions is less than the distance between the ground and the insertion of the tendon into the base of the first ray. This provides the muscle with a fulcrum effect that is essential to stabilize the first ray. 2 In addition, the calcaneocuboid joint also becomes important in the plantarflexion of the first ray since, on locking, it becomes a fixed and immobile zone for the PLM tendon to use as a pulley or resistance point to produce movement in the first metatarsal. If the fulcrum is lost, the muscle does not stabilize the first ray, there is an increase in ground reactive forces under the first metatarsal head during toe-off, and the first ray becomes hypermobile and dorsalflexed. The proximal phalanx adopts a position in flexion so as to compensate for the lack of support of the first ray, the loading point of the first metatarsal shifts distally to the interphalangeal joint of the hallux,13–15 and the progression of articular limitation is triggered. This makes proper PLM function indispensable for the adequate plantarflexion and stability of the first ray.
There are many foot orthoses designed for conservative treatment of HL, including orthotics type root to control the subtalar pronation, orthoses medial heel skive type, orthoses blake type inverted, or orthoses with kinetic wedge; but there is no scientific evidence that any of they have improved the extension of the hallux.
This study seeks to show that continued use for 6 months of custom-made foot orthoses with pathomechanical control and added support for the first MPJ improves the hallux capacity for extension in HL patients. This is because the support limits hindfoot pronation, making the action of the PLM more effective. This muscle acts earlier and for longer in the gait cycle, favoring the first metatarsal’s plantarflexion, which is essential for the correct extension of the hallux. Therefore, we shall find an increased metatarso-phalangeal angle in relaxed position.
Methods
Study participants
The participants in this double-blind clinical trial were patients who were presented at the Area of Clinical Podiatry at the University of Seville and who were diagnosed with HL. The total sample comprised 40 feet (n = 40) of 20 individuals (8 women, 12 men) aged between 16 and 63 years (mean 43.35 ± 16.47 years).
The foot was used as the unit of analysis rather than the individual since the parameters measured of the two hallux MPJs (right and left) usually differ in the same individual. With this choice, any concomitant statistical interferences were avoided. 20
The characteristics of the participants in both the control and the experimental groups are listed in Table 1.
Characteristics of the participants in the two groups.
The inclusion criteria for the participants in the study were to belong to the age range described above, to present physeal closure,21,22 and to present hallux MPJ mobility in extension of less than 65° and more than 15°. 23 The exclusion criteria were suffering degenerative osteoarticular diseases or neuromuscular imbalances, both of systemic origin, having undergone any type of foot trauma or osteoarticular surgery, or experiencing pain or functional disability in any region of the foot which could affect the normal mobility of the first MPJ, except for the joint under study.
The study was approved by the Research Ethics Committee of the University of Seville. Also, since it involved clinical practice, it was approved by Area of Clinical Podiatry at the University of Seville.
Procedure
Data acquisition was conducted in three phases by two of the authors (Researchers 1 and 2) other than the lead author. Under no circumstances did they cross their data, so that there was full compliance with the double-blind masking of the study.
In the first phase, Researcher 1 performed on all the participants who presented at the center a biomechanical examination in seated, static, and dynamic situations following the standard protocol used in the Area of Clinical Podiatry at the University of Seville. The dependent variables of the study were the Relaxed Position of the first MPJ and the Maximum Extension of the hallux. For these measurements, we used a two-armed goniometer,24,25 with the participant seated on the examination table with the knee extended and the foot in a relaxed position. 26 In this relaxed position of the foot, the center of the goniometer was placed on the center of the metatarsal head. The proximal arm was placed parallel to the bisection of the first metatarsal and the foot was held steady with one hand. The distal or mobile arm was placed parallel to the bisection of the proximal phalanx and held fixed to the toe with the other hand. The first of the measurements was taken corresponding to the relaxed physiological position of the first MPJ. From this relaxed position, the toe together with the distal arm of the goniometer was drawn to the maximal extension, allowing the first ray to plantarflex so that the movement of extension would be entire. 27 At this point, the second measurement was taken (Figure 1). Subsequently, the first phase of application of the treatment was initiated, consisting in making molds on phenolic foam under load, neutralizing the rearfoot. 28

Goniometer measurement of the maximum extension of the hallux.
In the second phase of the process, Researcher 2 prepared the custom-made foot orthoses and assigned each individual to one of the two study groups—control or experimental—following a computerized randomization procedure without informing the participant of the group to which they belonged. The orthoses were made with retrocapital thermoplastic polypropylene of 3 mm thickness and 3-mm-thick ethyl vinyl acetate (EVA) top cover of 45 Shore A hardness 29 (Figure 2). All the foot orthoses were the same for both the control and the experimental groups except that, for the latter, a supporting element was added, also of 3-mm-thick EVA of 45 Shore A hardness, covering the entire first metatarsal head and the base of the proximal phalanx of the hallux, without reaching the distal interphalangeal joint (Figures 3 and 4).

Plantar view of the orthoses with the first ray unsupported.

Plantar view of the orthoses with the first ray supported.

Lateral view of the foot orthoses with the first ray supported.
For the third and final phase of the process, after 6 months, the participant was scheduled for a further appointment at the Area of Clinical Podiatry at the University of Seville, and received by Researcher 2. After removal of the footwear and orthoses, the participant was directed for re-measurement of the foot parameters to a room conditioned to that effect. These measurements were again carried out solely by Researcher 1.
Finally, the data obtained before and after application of the treatment were provided to the Lead Researcher, who was responsible for their processing and analysis, and who had at no time participated in the processes of group allocation, measurement, or data acquisition.
Statistical analysis
A descriptive analysis is made of the data, providing the means; standard deviation; minimum, maximum and the 25th, 50th and 75th percentiles for the quantitative variables; and frequencies and percentages for the qualitative variables. For the analysis of the specific variables of the study, normality tests are performed in accordance with each group so as to select the appropriate statistic (a t-test or the Wilcoxon signed-rank test) to use for related samples. A 95% confidence level is used in all cases. Statistical calculations are performed with the IBM SPSS Statistics 20 program package.
Results
Relaxed Position of the hallux
The values of the Relaxed Position of the hallux of the two groups are listed in Table 2. As it is observed, in the control group, the 6-month use of custom-made foot orthoses with biomechanical control improved the Relaxed Position in extension of the hallux by 0.9° (p < 0.001). In the experimental group who wore the same custom-made foot orthoses but with added support for the first ray, the improvement was 4.5° (p < 0.001). The difference between the two groups was statistically significant (p < 0.001).
Variable: relaxed position, comparing the control and the experimental groups.

Maximum Extension of the hallux
The values of the Maximum Extension of the hallux of the two groups are listed in Table 3. The 6-month use of the custom-made foot orthoses with improved biomechanical control improved the Maximum Extension of the hallux by 5.65° (p < 0.001). In the experimental group who wore the same custom-made foot orthoses but with added support for the first ray, the improvement was 22.2° (p < 0.001). The difference between the two groups was statistically significant (p < 0.001).
Variable: maximum extension, comparing the control and the experimental groups.

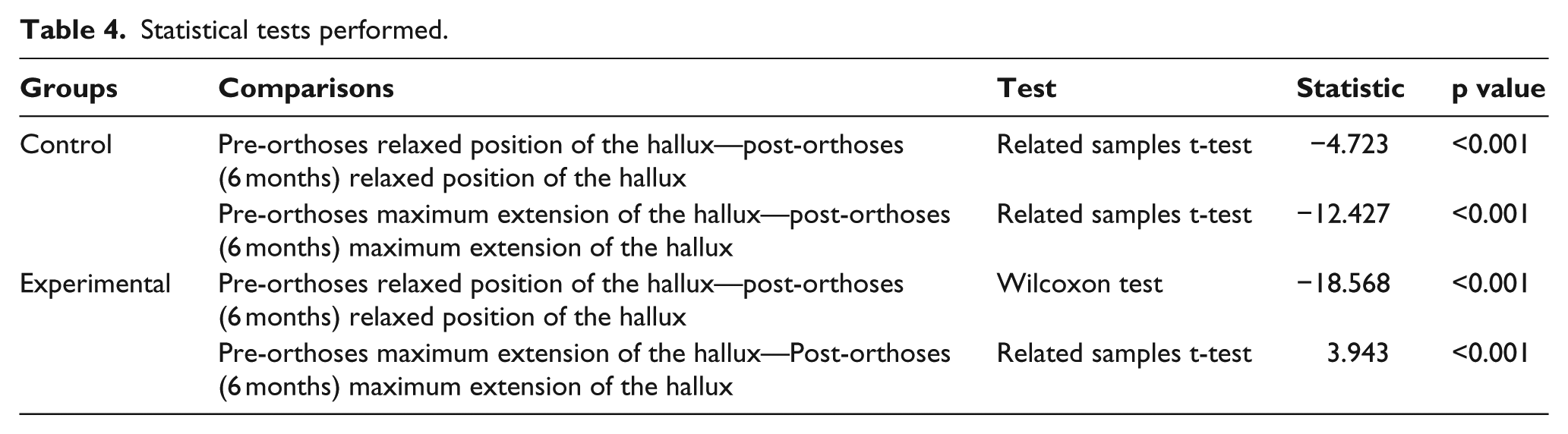
The statistical tests are presented in Table 4. There are significant differences in the two measurements for each of the two variables in both the control group and the experimental group.
Statistical tests performed.
Discussion
The principal objective of this clinical trial was to improve the extension capacity of the hallux in HL patients by using custom-made foot orthoses for that purpose, favoring plantarflexion of the first metatarsal in the propulsive phase of gait. The results indicated that the experimental group, who used the foot orthoses with added support under the first MPJ, obtained after 6 months a significantly greater increase in mobility of the hallux than the control group.
Many studies in the literature that we analyze below discuss foot orthoses use and its relationship with improvement in the range of mobility of the first MPJ. However, most have focused on improving the symptoms of the condition with orthoses that act at different levels of the foot.
At the hindfoot level, root-type foot orthoses have been used, modified in order to control pathological pronation of the subtalar joint, attempting thereby to restore the functionality of the hallux. Using this type of orthoses, Kilmartin et al. 30 failed to improve the extension of the hallux either in HL patients or in healthy participants, but Munuera et al. 31 achieved an improvement of 8° after 5 months of treatment in patients of ages from 25 to 32 years. According to Nawoczenski and Ludewig, 32 control of pronation and increasing the medial longitudinal arch of the foot did not imply any improvement in the range of dorsiflexion of the hallux. One of the conclusions drawn in that study was that the degree of plantarflexion of the first metatarsal is directly proportional to the dorsiflexion of the hallux, thus coinciding with the purpose of our first measurement (relaxed position of the first MPJ). Hogan and Kidd, 33 besides controlling subtalar pronation in HL patients, studied inverting the hindfoot with medial heel skive type orthoses, finding no better extension of the hallux. Scherer et al. 34 applied orthoses to control hindfoot pronation by favoring the windlass mechanism. They obtained an extra 8.8° extension in HL patients, although their data were determined by making measurements on the same day under load before and after application of the orthoses. This demonstrates the importance of biomechanical control of the foot as a causative factor of the limitation of the extension of the hallux, a control that we applied with all the foot orthoses, both for the experimental and for the control groups. However, this biomechanical control alone is insufficient to achieve the minimum range of hallux extension necessary for normal function.
Munteanu 35 applied Blake-type foot orthoses with 30° inversion, without positive results. At the forefoot level, Dananberg 4 applies a kinetic wedge to favor transmission of the load in the direction of the first metatarsal, but makes no reference to the extension of the hallux, instead describing improvement of the symptoms of the musculoskeletal system in general. Camasta 36 and Dananberg et al. 37 describe the biomechanical concept of a cut-out under the first metatarsal, leaving space in the orthoses under the first metatarsal head to allow its plantarflexion. Clough 38 designed a 6-mm-thick material glued to the insole of the shoe under the hallux, with the aim of favoring the windlass mechanism and achieving plantarflexion of the first metatarsal. Three cases were studied and two of them showed improved plantarflexion. This study neither concluded with any improvement in the extension of the hallux.
The studies reviewed above together demonstrate that control exclusively applied to the forefoot or to the hindfoot in isolation fails to improve the extension of the hallux, so that various authors have considered the association of control of pronation with orthotic elements for the forefoot. Chang and Camasta 39 used foot orthoses with subtalar inversion and cut-out of the first metatarsal when this is flexible. In the case of metatarsus primus elevatus in hallux rigidus, those authors used orthoses to lock the joint by means of a Morton extension plate, with a ‘rocker’ bar ahead of the MPJ. However, the purpose behind the use of all these elements is palliation of the deformity, and there is no evidence that they improve the range of mobility of the first MPJ.
Grady et al. 6 studied 362 HL patients. Of these, 215 were fitted with functional orthoses, 32 of them being fitted with Morton extension plates. The other 87 were fitted with Shaffer devices involving elevation of the medial longitudinal arch of the foot, with 28 of them having a combination of the above elements. A 47% success rate was achieved after 7 years of treatment, although the objective was not to restore the functionality of the joint but to treat the corresponding pain. This same objective was pursued in the work of Welsh et al. 40 in which 6 months of treatment improved the pain symptoms of the first MPJ of the patients. The treatment applied consisted of prefabricated orthoses with a medial wedge to control pronation, a cut-out under the first ray and 3-mm-thick, high-density support under the second, third, fourth and fifth metatarsals. This work neither marked any reference to the degree of correction of the extension of the hallux.
In summary, therefore, the scientific literature as yet has included no conclusive studies ensuring the restoration and functionality of the first MPJ in HL patients. The present work has proposed new foot orthoses as a valid treatment for the definitive correction of this pathology.
The results of this study suggest that the use of custom-made foot orthoses to control the pathomechanics of the foot with added support under the first MPJ significantly improves the maximum extension of the hallux, evaluated as non-loadbearing. This increased joint range-of-motion may favor the normal functionality of the first MPJ in the toe-off phase of gait, with the consequent benefits which this brings to other joints of the locomotor apparatus. Nonetheless, this aspect needs to be analyzed in future studies in which the hallux’s dynamic extensor capacity is evaluated.
The increased extension of the hallux is accompanied by an increase in plantarflexion of the first metatarsal, thanks to the proper functioning of the PLM. Before, this functioning had been insufficient, but now it is effective following the added support provided by the foot orthoses designed in the study.
One limitation of our study is that although it have been recruited more participants than those required on the sample size calculation, we consider that it is a small sample because it is a pilot study. We understand that a larger sample is required to make our results more conclusive.
Another limitation of our study is the treatment time of 6 months. We understand that it would be interesting to have a longer follow-up treatment (1 year) to see whether these results can still improve.
With these limitations, we would not accomplish a proper comparison of results depending on the sex of the subjects, which could be realized in the future with a larger sample.
Conclusion
The use of the custom-made foot orthoses designed for this study, with added support in the first MPJ, significantly improved maximum passive extension of the hallux in individuals in the experimental group after 6 months of treatment.
Awaiting of the increment of the sample size and analyzing the results over a period of at least 1 year of treatment, we propose these custom-made foot orthoses designed in this study as an effective method of conservative treatment that improves the extension of the hallux in patients with HL.
Footnotes
Acknowledgements
This study was made possible because of the cooperation and continued support of the Department of Podiatry at the University of Seville. We would also like to express our gratitude to the Area of Clinical Podiatry at the University of Seville for the use of their facilities, materials, and human resources without which the research would have been impossible. Finally, we are sincerely grateful to all the participants who voluntarily participated in the study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None of the authors have any financial affiliations or competing interests to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.