
Abstract
Background:
Collateral ligament shortening causes extension contractures of the metacarpophalangeal joint, and dynamic flexion splinting has been widely used to treat these contractures; however, there are various problems with these approaches. We developed a novel, pneumatic-type dynamic traction and flexion splint to solve these problems.
Case description and methods:
A total of 25 fingers were treated with the dynamic traction and flexion splint for 8 weeks. Every 2 weeks, the average metacarpophalangeal joint flexion angle, total active motion, grasp strength, and pain scores were assessed.
Findings and outcomes:
The finger flexion angle was significantly greater at the final evaluation, starting after 6 weeks of treatment (p < 0.05), than prior to treatment. Similarly, the total active motion results improved significantly over 8 weeks.
Conclusions:
Our results show that use of the dynamic traction and flexion splint improves patient finger functioning and flexural angle.
Clinical relevance
The dynamic traction and flexion (DTF) splint appears to be effective for treating patients.
Background
The metacarpophalangeal (MCP) joint is critical for the proper functioning of the hand. Contracture of these joints, often resulting from trauma and burns,1,2 causes significant disorders in the activities of daily living. These common 3 contractures may be caused by collateral ligament shortening. Thus, continuous stretching is an effective treatment, 4 and the treatment efficacy is improved through the use of a dynamic orthosis,5–7 which is a well-accepted modality used to regain hand joint motion. 8 The clinical success of treatment is better and results in less joint stiffness if the interval between injury and treatment is minimal. 9
Dynamic flexion splints have been widely used for MCP joint extension contracture treatment.10,11 However, this type of flexion splint can negatively impact the articular surface of the joint, leading to pain when the finger is flexed for an extended period. 3 As a result, range of motion improvements is difficult to obtain. 11 The conventional dynamic flexion splint pulls at right angles to the proximal phalanx and, as such, does not compress or distract the MCP joints. However, the manufacture of the splint is time consuming, and the splint durability is problematic. Furthermore, problems have been associated with the appropriate regulation of the traction power to elicit maximal improvement. Hence, a dynamic splint, using pneumatic artificial muscle (PAM), has been manufactured from a more durable material that is flexible and has easily adjusted traction power. However, the use of PAM splints has not been previously reported for improving joint contracture. We devised a novel pneumatic-type dynamic traction and flexion (DTF) splint. 12 This study investigated whether the DTF splint is an effective device for treating MCP joint extension contracture.
Case description and methods
The trial protocol was approved by our hospital’s ethics committee. Prior to their enrollment in the study, written informed consent was obtained from each patient participating in the research protocol.
Patients
We evaluated nine patients (25 fingers; average age = 49 (range: 33–62) years) with MCP joint extension contractures diagnosed less than 6 months earlier. A total of five men (11 fingers) and four women (14 fingers) were treated with DTF splints. The contractures developed as a result of proximal phalangeal fractures (one patient, one finger), metacarpal bone fractures (two patients, three fingers), proximal phalangeal and metacarpal bone fractures (two patients, five fingers), extensor tendon injuries (three patients, eight fingers), distal radius fractures (two patients, eight fingers), and complex regional pain syndrome type II (one patients, four fingers) (Table 1). As part of their splint therapy, the patients were directed to wear the assigned splint for their range of motion exercises by their occupational therapist. The authors helped the patients perform the exercises for 20 min, three to five times/week. Each patient started wearing the splint when the elastic traction was 200 gf.4,13–15 The splint was worn by the patients three times/day (morning, noon, and night) for 30 min/session. An occupational therapist checked each patient’s traction power and appropriate wearing of the splint every 2 weeks.
Characteristics of the patients with extension contractures of the MCP joint.
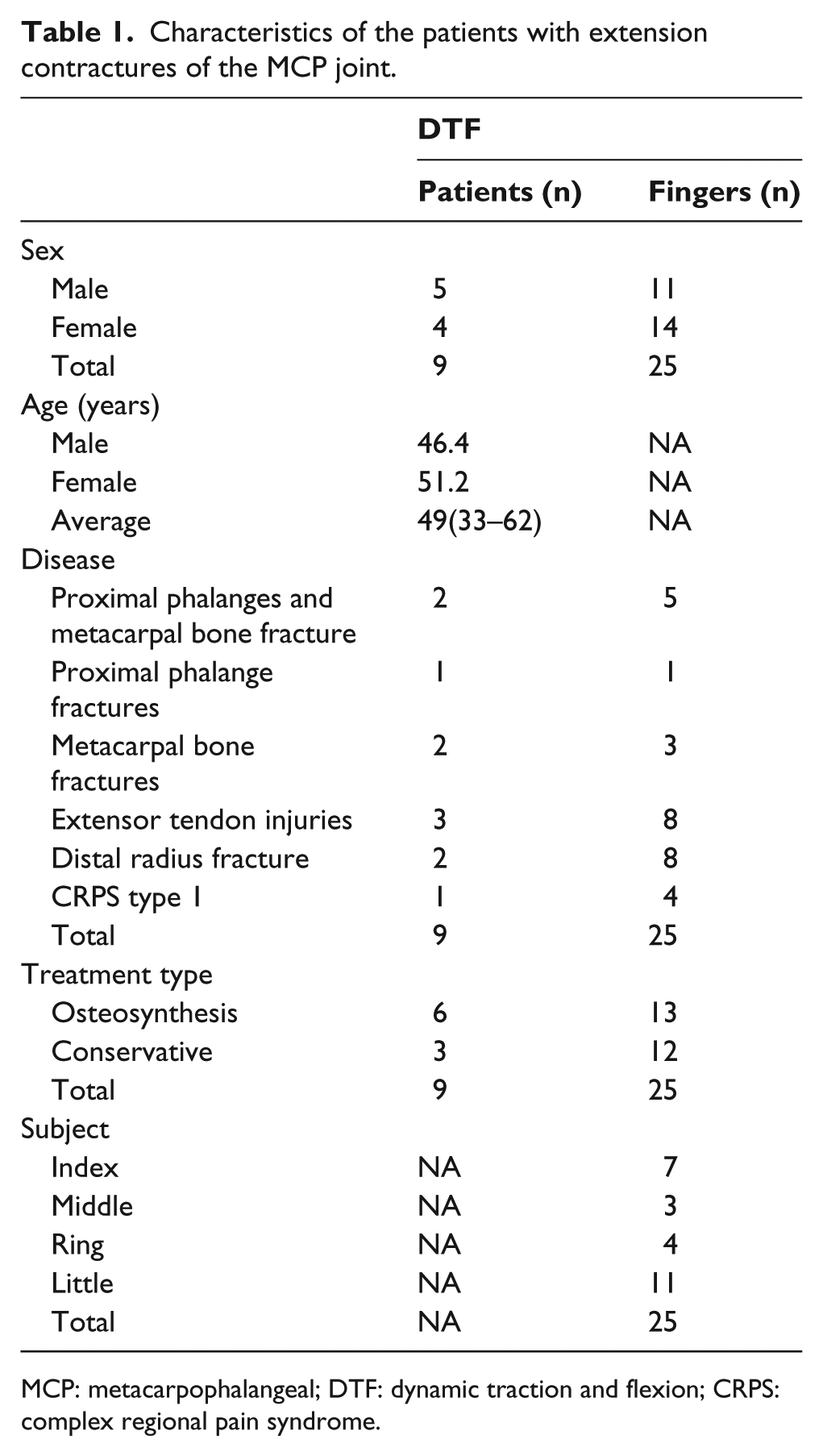
MCP: metacarpophalangeal; DTF: dynamic traction and flexion; CRPS: complex regional pain syndrome.
Measurements
We evaluated the progress of the finger function tests (TAM scores) and MCP joint flexion angles, every 2 weeks, over an 8-week period. Furthermore, we compared the two groups for their ability to grasp and their experience with sharp pain (Visual Analog Scale (VAS) score) when they started their treatment sessions, and after 8 weeks of progress. The evaluator was an occupational therapist, blinded to the purpose of the research.
Structure and characteristic of the DTF splints
The DTF splint comprised a wrist joint dorsiflexion instrument, a curved PAM and a wrist joint-arthrodesis belt (Daiya Industrial, Okayama, Japan), a miniature gas cylinder (74 g, Nippon Tansan Gas, Tokyo, Japan), a Velcro strap, and an elastic band (Figure 1). A profile view of the splint (Figure 2) shows the characteristics of this splint, which pulls the articular surface and corrects the flexural direction by applying a PAM to the dynamic splint; the splint permits the treatment of two or more fingers, simultaneously. The PAM used in this study was made of curved rubber (Figure 3(a) and (b)), and comprised a rubber tube covered with a bellows sleeve that only extends or contracts axially. By inhibiting the extension of one side, with the fiber reinforcement, the bending motion in the desired direction occurs after supplying compressed air to the rubber tube. As shown in Figure 3(a), the curved tube is covered with an inner, noncontracting cloth and an outer, rubber cloth. The curved, rubber PAM bends when the rubber tube expands as a result of the differences in the lengths of the rubber and cloth (outer and inner) covers. The bending motion was used to flex the joint, and the extension movement was used for joint traction (Figure 3(b)). The subject finger was wrapped to avoid any possibility of local ischemia.

The dynamic splint used in this study. Pneumatic-type dynamic traction and flexion splint: the characteristic motion of the artificial muscle allows extension and bending of the finger. The bending motion was used for flexion of the joint, and the extension movement was provided by joint traction.

The pneumatic artificial muscle used in this study involves a curved pneumatic rubber artificial muscle.
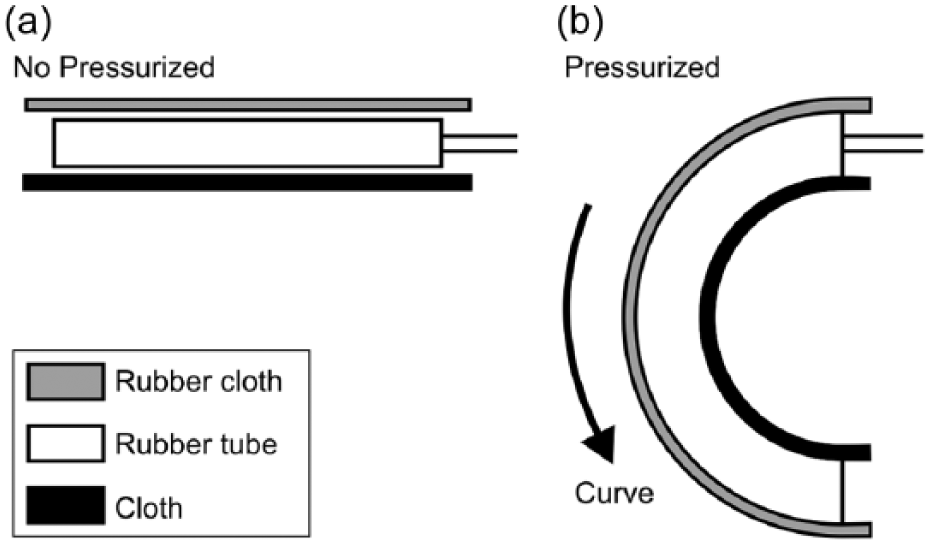
Structure of the curved-type pneumatic rubber artificial muscle: (a) non-pressurized rubber tube and (b) pressurized curved rubber tube.
Statistical methods
The Kruskal–Wallis and Bonferroni methods were used for within-group comparisons. The significance of the differences between mean values was calculated. All statistical analyses were performed using SPSS Base 11.0J statistics software (SPSS Japan, Tokyo, Japan); p values <0.05 were considered statistically significant.
Findings and outcomes
Table 2 describes the effects of wearing the DTF splint over the 8-week treatment period.
Evaluation results in relation to the use of pneumatic-type dynamic traction and flexion (DTF splint).
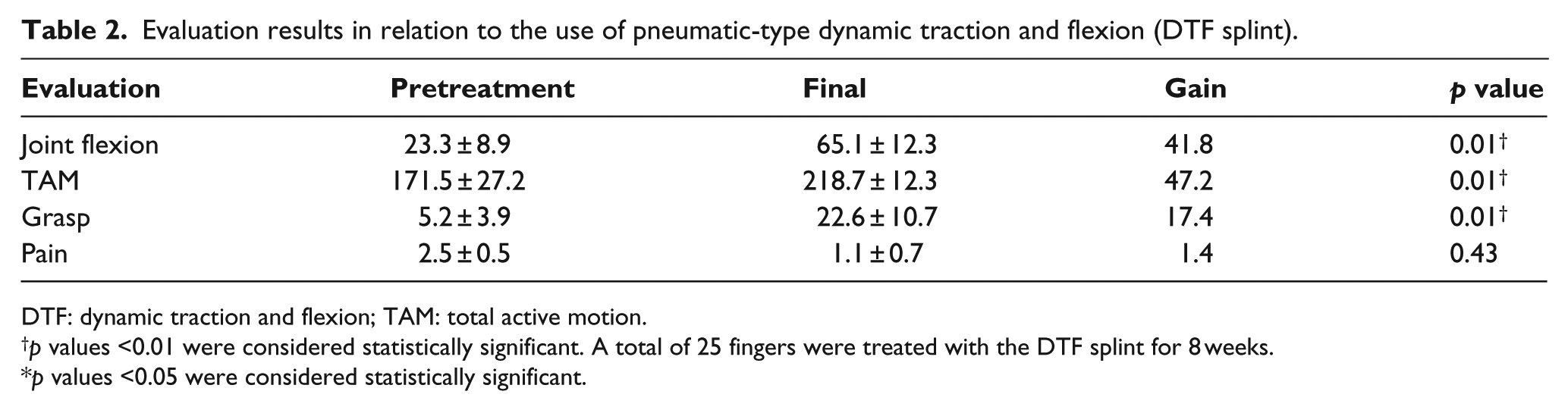
DTF: dynamic traction and flexion; TAM: total active motion.
p values <0.01 were considered statistically significant. A total of 25 fingers were treated with the DTF splint for 8 weeks.
p values <0.05 were considered statistically significant.
MCP joint flexion angle
The mean pretreatment MCP joint flexion angle was 23.3 ± 8.9°; at the final evaluation, the angle was 65.1 ± 12.3°. Furthermore, the MCP joint flexion angles improved by an average of 41.8°. Over the 8-week treatment period, the splint showed significantly improved flexion angles (p < 0.01) (Table 2). As shown in Figure 4(a), there was a significant improvement started after 6 and 8 weeks of treatment (p < 0.01).
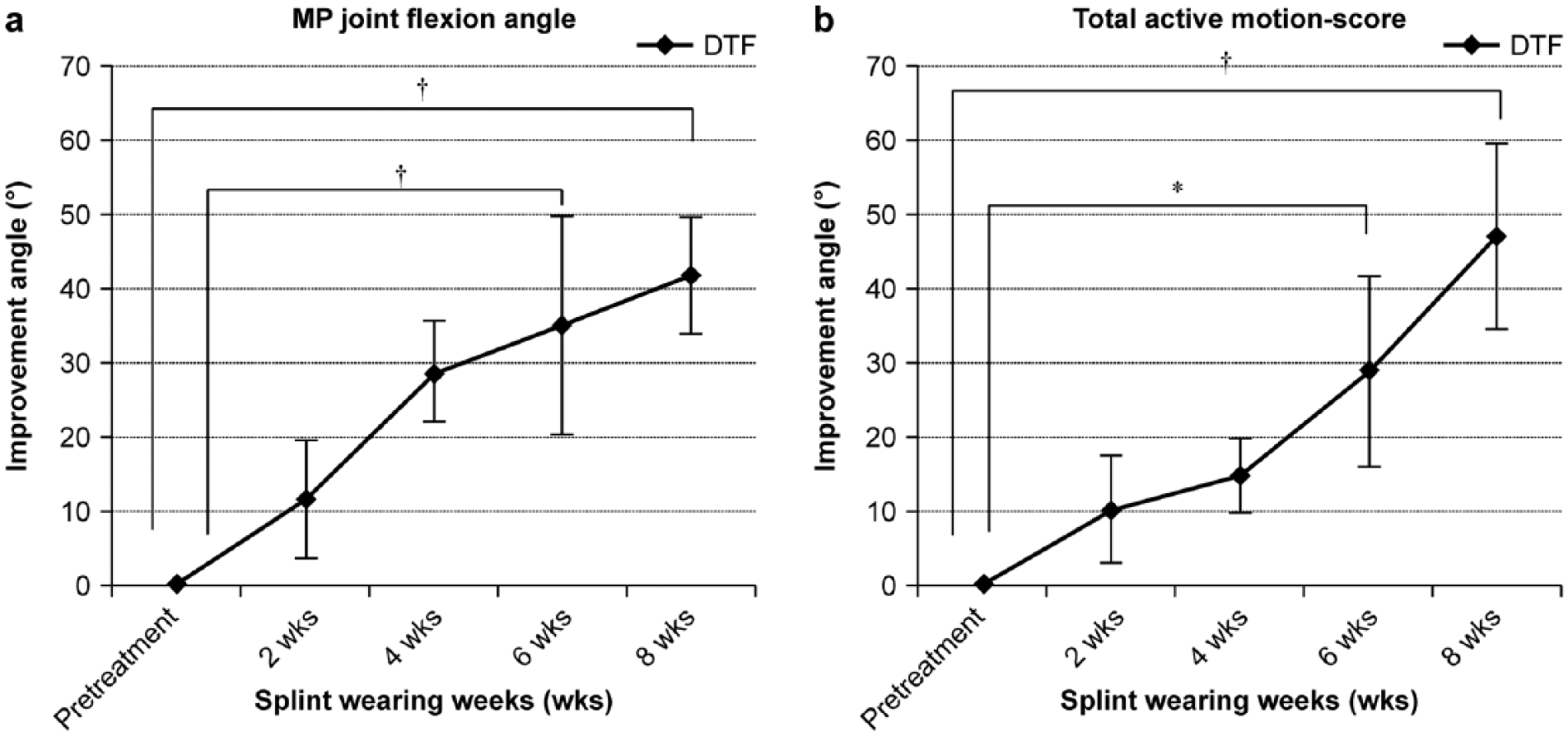
The 2-week improvement rates in patients wearing dynamic traction and flexion splints. We treated 21 patients (52 fingers). The level of significance was set at *p < 0.05, †p < 0.01: (a) metacarpophalangeal joint flexion angle and (b) total active motion score.
TAM scores
The TAM scores for the pretreatment and final evaluations were 171.5 ± 27.2° and 218.7 ± 12.3°, respectively. Over the 8-week treatment period, the splint produced significant improvement in the total finger function (p < 0.01), improving by an average of 47.2° over the 8-week treatment period (Table 2). The significant improvement began after 6 and 8 weeks of treatment (p < 0.01, Figure 4(b)).
Grasp strength
The pretreatment grasp strength was 5.2 ± 3.9 kg and was 22.6 ± 10.7 kg at the final evaluation. Over the 8-week treatment period, the muscle strength improved significantly (p < 0.01), increasing by an average of 17.4 kg over the 8-week treatment period (Table 2).
VAS score
There were no significant differences in the VAS scores between the pretreatment and final evaluations. The 2-week rates of improvement for the patients wearing splints are shown in Figure 4(a) and (b).
MCP joint flexion angle improvement angle
As shown in Figure 4(a), there was a significant improvement starting after 6 weeks and 8 weeks of treatment (p < 0.01).
TAM score improvement angle
For the TAM scores, there was a significant improvement starting after 6 weeks and 8 weeks of treatment (p < 0.01, Figure 4(b)).
Discussion
Contracture of the MCP joint is a common clinical condition, 12 but the treatment is difficult and is prolonged if the contracture is fully formed. Of the several causes of joint contracture,16,17 the most common cause of MCP joint extension contractures is shortening of the collateral ligament. 11 The dynamic splint has been a well-accepted modality used for restoring joint motion to an injured hand. However, in extension contractures that involve a bent MCP joint, such treatment may not only be ineffective, but may also injure the articular cartilage causing greater damage. More recently, conventional dynamic flexion splints have been used to pull the proximal phalanx at right angles, to neither compress nor distract the MCP joints. Generally, a PAM enables effective treatment to be delivered under conditions of relatively low pressure and reduced tension; PAM provides powered torque to the splint in the DTF splint. Additionally, the utilization of PAM enables the use of a splint that is flexible, light-weight, easily maintained, easily adjusted to provide appropriate traction power, and inexpensive. Recent studies have quantified the detailed force-length, force-velocity, force-activation, and bandwidth properties of such artificial pneumatic muscles.18–21 The PAM is well suited for mimicking natural movements19,20 and, in the current orthosis, for providing a power-assisted glove. 13
This study assessed the DTF splint as a device for treating MCP joint extension contractures. The results indicated that the DTF splint resulted in recovery of approximately 40° in both the joint flexion angle and finger function within 8 weeks. Specifically, the range of motion of the joint flexion angle improved significantly, starting after 6 and 8 weeks of treatment. As a result, the TAM scores in the DTF splint-treated joints also improved significantly, starting after 6 and 8 weeks of treatment. According to another study that investigated 14 hands, including interphalangeal joint mergers, the dynamic splint wearing period averaged 2 months; the resulting percent improvement was 32.5°. 22 In the current study, the flexion angle improved 41.8° after DTF splinting, suggesting this splint’s potential clinical effectiveness.
The DTF splint allows finger extension and bending. According to our preliminary research, the joint space in the most palmar part of the MCP joint increased by approximately 1.7 mm, using the DTF splint, compared with a joint not receiving orthotic treatment. 13 Thus, the DTF splint allows extension of the extensor tendon as well as the application of traction. The improved flexion angle of the whole finger, into the interphalangeal joint, was accomplished using the PAM along the full length of the finger. As a result, there was improvement in both joint extension and the function of the whole finger, including the interphalangeal joint. The traction force of the DTF splint extended the collateral ligaments of the MCP joints. This may indicate an improvement in the overall function of the finger as well as an improvement in the flexural angle. Therefore, the DTF splint may be an effective tool for improving a patient’s digital range of motion during the early stages of treatment.
Study limitations
Each patient used the splint for only 8 weeks, rather than over a longer period. Hence, we were unable to determine the required period of treatment. Additionally, only a limited number of patients, with MCP joint contractures diagnosed within 6 months of the start of the study, were enrolled. In future studies, we plan to increase number of patients and test the long-term effects of the splint and its usefulness for treating contractures diagnosed more than 6 months prior to the start of therapy. Furthermore, we want to show the clinical usefulness of DTF in comparison with the conventional dynamic flexion splint.
Conclusion
Our results show that use of the novel DTF splint allows improvement in overall finger functioning and in the MCP joint flexural angle in patients with MCP joint extension contractures.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This study was funded by a 2011 grant from the Okayama Prefecture Industrial Promotion Foundation.