
Abstract
Background:
Major amputations are indicated for curative treatment of some tumors of the pelvis. Previous literature suggests that patients with a hemipelvectomy amputation are more efficient walking with crutches than using a prosthesis.
Objectives:
The purpose of this study was to evaluate whether modern prosthetic use after hemipelvectomy may be a viable option for patients than in the past.
Study Design:
Case control trial.
Methods:
We identified five patients who underwent hemipelvectomy amputation and fit with high-level prosthetic components. Patients were evaluated using a timed up and go, 5-m walk, 400-m walk, and stair climb tests to evaluate functional performance with a prosthesis and without. Short Form–36 scores were collected as well. These results were compared to matched controls.
Results:
There was a trend for faster locomotion using crutches over wearing a prosthesis in the timed up and go, and 5-m and 400-m walk; no difference was seen in stair climbing. Short Form–36 scores showed decreased physical component score, but equal mental component score compared to the general population.
Conclusion:
Our results show that in addition to advances in surgical techniques, prosthetic rehabilitation and management are beginning to optimize functional mobility with the prosthesis.
Clinical relevance
Patients who use a modern prosthesis following hemipelvectomy demonstrated good clinical function with and without their prosthesis. Although health status scores were decreased in the physical component, mental component scores were equal to healthy controls.
Background
External hemipelvectomies are often indicated for curative treatment of primary pelvic tumors.1,2 Due to the complexity of bony anatomy, relationship of the viscera, nervous, and vascular structures, hemipelvectomies are one of the most invasive and technically demanding surgical procedures in the modern surgical era.2,3 Early on it was reported that half of patients undergoing a hemipelvectomy died from complications related to the surgical procedure; 4 however, through advances in surgical technique and anesthesia, this number has decreased to 0%–10%.1,5–7 With more patients surviving their malignancies, there is an increase in the need for rehabilitation for these patients following a high-level lower extremity amputation.8,9
It has previously been shown that the ability to walk following amputation is determined by the level of amputation.10–12 The gait velocity selected by patients with amputations is significantly lower than normal and decreases with more proximal amputations. 12 Waters and colleagues showed that the gait velocity for traumatic amputations was 87% of able bodied individuals for below-knee amputations (BKA) and 63% of able bodied individuals for above-knee amputations (AKA); hemipelvectomy level amputations were not studied. 12 Similarly, the rate of oxygen consumption, heart rate, and respiratory quotient were significantly increased in all groups of amputees (hemipelvectomy level not tested) when walking with their prosthesis and when walking with crutches without a prosthesis compared to controls. 12 Nowroozi reported that patients with hemipelvectomy level amputations walked about 50% slower and spent about 125% more energy than able bodied people of the same age. 13 Due to the level of amputation, it becomes difficult to control swing, stance, and stabilize a prosthesis, while balancing the body.1,14 With these difficulties, some patients are unable to successfully use a prosthesis for activities of daily living (ADL).8,9,15,16
While recent studies have looked at functional outcomes following hemipelvectomy, the conclusions are based on subjective patient data collected from surveys.15,17 We sought to objectively evaluate patient function with and without a prosthesis following hemipelvectomy surgery and to compare it to matched controls. Additionally, we evaluated health status using the Short Form–36 (SF-36) instrument in this population.
Methods
Patients
The research protocol was approved by the Institutional Review Board. Over a 10-year period (2000–2010), 135 patients underwent a pelvic level amputation (hip disarticulation or external hemipelvectomy). A total of 120 (89%) of these patients were excluded from the study. Exclusion criteria included: (1) elected to carry out their rehabilitation and follow-up care at another institution (n = 72, 53%), (2) patients who were dead at the time of the study (n = 32, 13%), (3) underwent a hip disarticulation (n = 14, 10%), and (4) patients who had pre-existing neurologic dysfunction on the contralateral side, that is, paraplegia (n = 2, 1%). Following the exclusion of these patients, 15 (11%) were available for review. Five of these patients had the ability to easily return to our institution for inclusion in this study. All patients included in this study had undergone a unilateral hemipelvectomy for a malignant process in the pelvis, and were using a high-level prostheses consisting of a polycentric hydraulic hip joint, microprocessor knee, and dynamic response foot following rehabilitation at our institution. All patients had a minimum 6-month prosthetic use and used identical prosthetic components (C-Leg and Helix 3D Hip; Otto Bock, Dunderstadt, Germany). Patients’ medical records were examined for their age, sex, body mass index (BMI) without prosthesis, type of pelvic malignancy, hours of daily prosthetic use, length of hospital stay, length of in-patient rehabilitation stay, recurrence of disease, and if there were any postoperative complications. Once the patients were selected, controls of similar ages, BMI, and sex were selected from the community.
There were four males and one female with a mean age of 46 years (range: 33–58 years) and BMI of 23.2 (range: 16–26) (Table 1). Three patients underwent surgery for recurrent chondrosarcoma, one for a recurrent osteosarcoma, and one for a primary fibrosarcoma (Table 1). The mean length of stay in the hospital was 12 days (range: 8–14 days), with a mean in-patient rehabilitation stay of 8 days (range: 0–17 days). The patients have used their prosthesis for a mean of 18 months (range: 6–42 months) and for a mean of 10 h per day (range: 6–12 h). At last follow-up, at an average of 26 months (range: 8–72 months) following surgical resection there were no local recurrences. Three patients used a single forearm crutch on the contralateral side to their prosthesis, one patient used two forearm crutches, and one patient did not use any gait assistance devices. When the patients were not using their prosthetic limb, all ambulated with two forearm crutches.
In our cohort of patients who have undergone hemipelvectomy, the most common indication for surgery was recurrent chondrosarcoma.
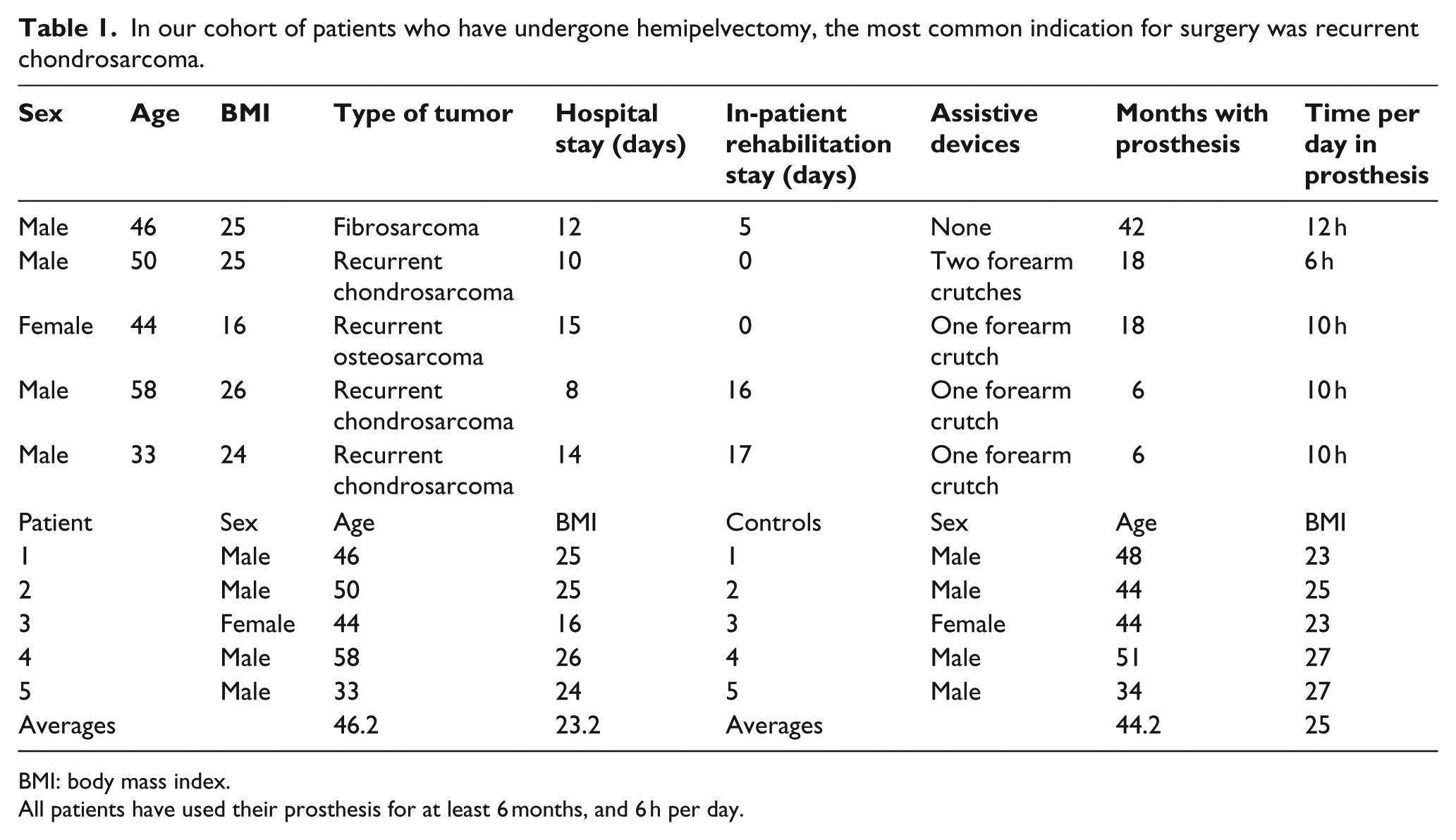
BMI: body mass index.
All patients have used their prosthesis for at least 6 months, and 6 h per day.
The control group included four males and one female with a mean age of 44 years (range: 34–51 years) and BMI of 25 (range: 23–27). The control subjects were matched with patients of a similar age, sex, and BMI (Table 1). There was no statistical significance between the ages and BMI between the two groups (p > 0.10).
Measures of outcomes
Prior to testing, a certified prosthetist checked the prosthetic alignment and gait of the patients to confirm an optimal gait pattern for each prosthetic component. Gait speed (5-m and 400-m brisk walking pace), stair climbing time, and the timed up and go (TUG) test were obtained (Figure 1). Patients were asked to complete these tasks once while wearing their prosthesis and once while not wearing their prosthesis and only using forearm crutches. A random number generator was used to determine whether the patients would ambulate with the prosthesis first or the crutches first.
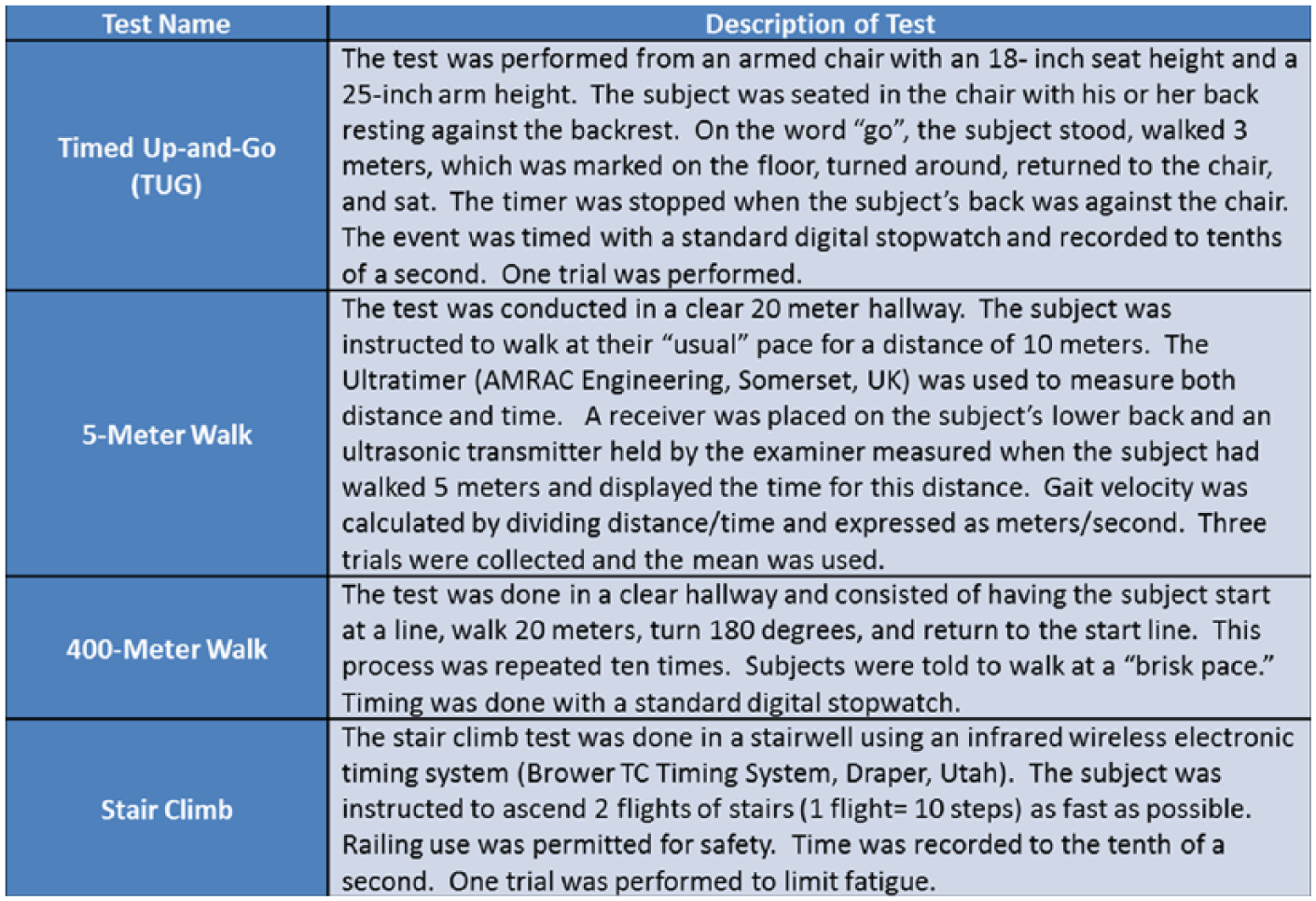
Timed up and go, 5-m and 400-m walk test, and stair climb are functional outcome measures used to assess patients who have undergone hemipelvectomy level amputation as well as a control group of sex matched, age and body mass index (BMI) similar study subjects.
General health status was assessed using the SF-36 (version 1). The SF-36 is a validated outcome measure to assess the burden of disease on the patients’ physical as well as mental health, comparing it to normal values of the general population, with higher values indicating better function. 17
Statistical analysis was performed using the Wilcoxon sign-rank test. Statistical significance was set at p < 0.05, and nonsignificant trend was defined as a p value < 0.10.
Results
Functional outcome
Patients with hemipelvectomies showed a trend toward faster ambulation with crutches over a prosthesis for the 400-m brisk walk (p = 0.06), 5-m walk (p = 0.06), and TUG test (p = 0.06) (Figure 2(a)). There was no statistical difference in stair climbing (p = 0.44) between the two groups (Figure 2(a)). When comparing the patients to controls selected from the community, as expected, the control group functioned at a higher level in all tasks when compared to the patient group when they were using their prostheses (p = 0.06), and when they were using crutches (p = 0.06) (Figure 2(a)).
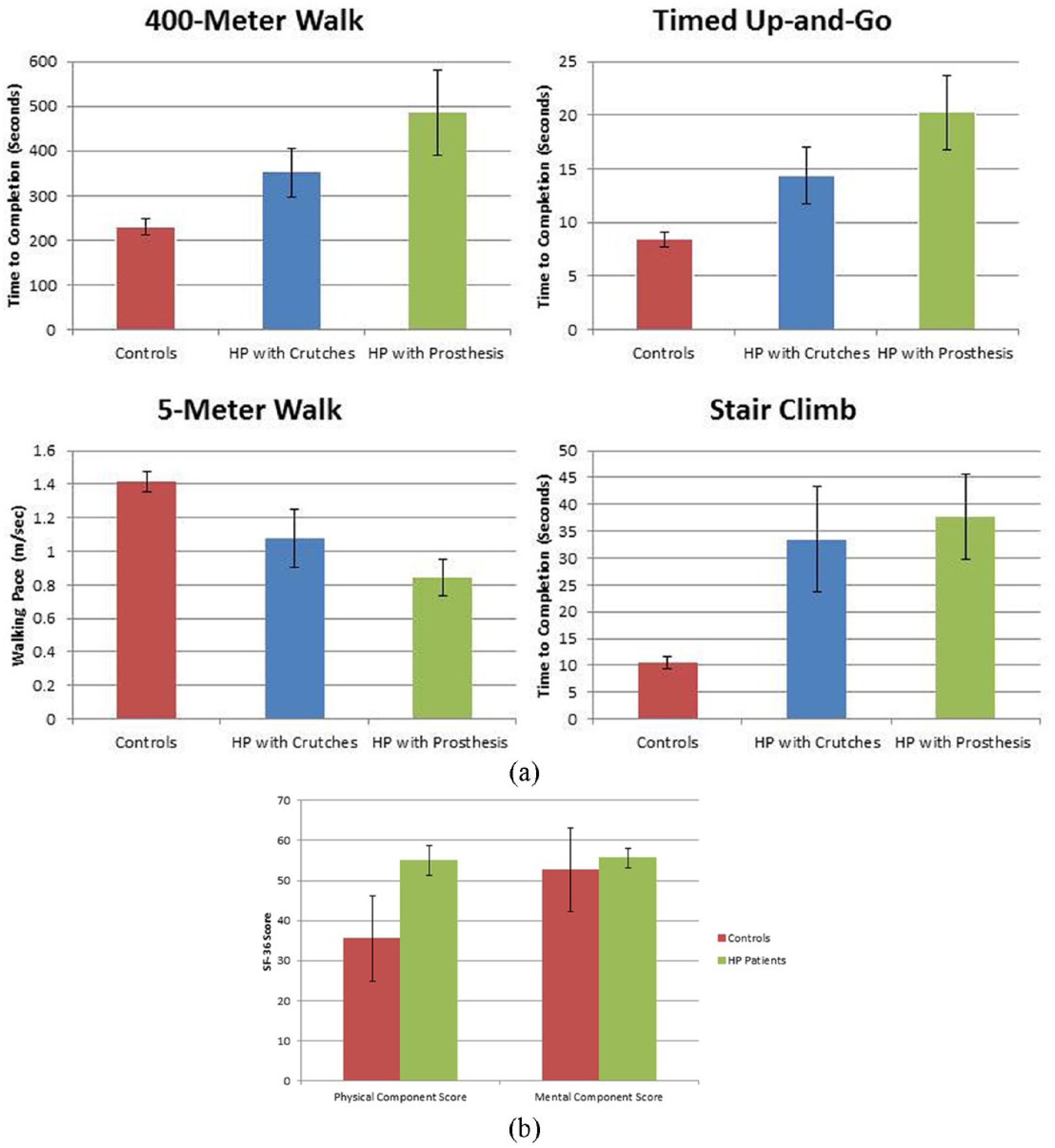
Results of functional outcome measures (a) showing that control subjects were able to perform all measures at a higher level compared to patients who have undergone hemipelvectomy. (b) When comparing Short Form–36 (SF-36) scores, again the controls physically performed at a higher level; however, there was no difference in the mental component of the test.
Health status
In comparing the results of the patients’ SF-36 scores to that of the control group, the control group scored statistically higher (p = 0.008) on the physical component summary; however, there was no statistical difference (p = 1.0) between the controls and the patients on the mental component summary scores (Figure 2(b)).
Discussion
The effect amputations of the lower extremity have in relation to functional ability and energy requirement is one of the best studied of all disabilities. 18 That being said, these studies frequently only include below knee amputations (BKA) and above knee amputations (AKA),12,13,18,19 with limited reports of patient function following a hemipelvectomy level amputation.13,15 Hemipelvectomy level amputations are routinely performed in young patients for oncologic processes, who frequently survive their malignancies, have a well-functioning contralateral limb, request a prosthesis over a wheelchair, and as such are potential candidates for prosthetic rehabilitation.2,3,13,17,20 We sought to objectively evaluate a group of patients using modern prostheses following hemipelvectomy to compare gait function with and without a prosthetic as well as health status.
There are several limitations to our study. The sample size is small, related mainly to the rarity of the procedure and the need to recall patients back for testing to participate in the study. Nevertheless, all patients were treated and rehabilitated at a single institution, with four of the five patients treated by one surgeon (PSR). Second, we only examined these outcome measures in patients with hemipelvectomies who ambulate with a prosthesis. Likewise, all patients used the same prosthetic components, and as such we are unable to comment on how the use of other components would compare to our results. Due to this, we are unable to comment on the functional status of patients who underwent a hemipelvectomy and now only ambulate with crutches. That said, this is the only study we are aware of that objectively evaluates function in a group of patients following hemipelvectomy using modern prosthetic limbs in a civilian population.
Following a hemipelvectomy, patients have been shown to have greater oxygen consumption and a slower gait speed with a prosthesis than when they use crutches and versus control patients. 13 It is thought that these differences are due to the weight of the prosthesis and also the difficulty to control swing phase of gait, stance, and stabilize the prosthesis; 15 because of this, many patients choose to use crutches instead of a prosthesis. 13 Given that performance and self-reported outcomes are frequently used to determine the quality of a patient’s life following orthopedic procedures,21–25 we chose to use the TUG, 5-m walk, 400-m walk, and stair climb tests, all which have been shown to adequately evaluate a patient’s mobility, balance, and lower extremity strength. 21 The results of our study show a trend toward faster locomotion with crutches compared to a prosthesis in the TUG, 5-m walk, and 400-m walk; there was no difference between the use of crutches and prosthesis in stair climbing (p = 0.44), which to our knowledge has never been previously reported.
The development of microprocessor knees and polycentric hip prostheses (such as the C-Leg and Helix 3D Hip used in this study; Otto Bock) have increased amputees independence and functional mobility following amputations.26,27 Microprocessor knees are equipped with sensors which continually detect the position and forces on the knee during swing and stance phases, allowing the prosthesis to rapidly adapt to changes in the walking environment. 26 Similarly, advances in prosthetic polycentric hips have shown to improve hip and knee extension during stance phase and increased hip and knee flexion during swing phase, the combination of which has led to greater control of hip motion. 27 The combination of microprocessor knees and polycentric hips appears to improve high-level amputee function to allow greater ability to safely and predictably negotiate environmental obstacles such as stairs and inclines while allowing the ability to walk at variable cadence, provide stumble recovery to avoid falls, and allow safer walking while minimizing the need for gait aids.26,27
Although the patients in this study showed a nonsignificant trend toward slower function with a prosthesis than with crutches, they did show better function compared to controls than has been reported in previous studies of hemipelvectomy level amputees. Patients in our study walked at a speed 40% slower than normal controls, similar to prior studies where walking speed was 50% slower than controls. 13 Gait velocity in this study (0.84 m/s with a prosthesis) was faster than previously reported walking speeds of vascular amputees of both BKA and AKA, and similar to traumatic above-the-knee amputations. 12 Functionally, this gait speed is sufficient to safely cross a street with traffic lights. 28
The TUG test has previously been shown to correlate well with the risk for falling, clinical outcome scores, and use of ambulatory aids in an elderly population, and has been used in amputees.22,29,30 Falling is a major problem and concern for patients with lower extremity amputations. 31 The TUG has been used to assess risk of falling in elderly patients, with patients who require greater than 30s were more likely to need assistance with ambulation and are at increased risk for falls.29,32 All of the patients within our cohort using their prosthesis were under the 30-s time point, and none had reported a serious fall. While using crutches as opposed to their prosthesis, the patients were faster at the TUG test (14.4 s vs. 20.2 s); patients were faster than previous reported times of vascular patients with above and below knee level amputations and in elderly patients with a history of orthopedic conditions, including total joint arthroplasty and hip fractures.30,33
The 400-m walk is frequently used to assess cardiopulmonary fitness, lower extremity power, and predict mortality in elderly patients.34–36 In large studies of elderly patients, patients who were unable to complete, or stopped to rest during the 400-m walk test were at increased risk of future mobility limitations and disability, require assistance with ADL, and future mortality.35,36 In our study, none of the patients stopped during the test, and all of the patients using their prosthesis completed the 400-m walk test, albeit in a slower time than with the use of crutches or versus controls (Figure 2(a)).
Negotiating stairs is a common goal for the end of rehabilitation for many patients following lower extremity injury or surgery.23,37 In order to complete the stair climb test, patients need to be able to function at a “higher” level compared to those who are unable to complete the task, and since it is more challenging, it does not have a ceiling effect which has been shown to be a problem with the TUG test. 38 In the patients in our cohort, there was no difference (p = 0.44) in the time it took patients to negotiate the stairs when they were using their prosthesis or crutches (Figure 2(a)). The time it took patients to climb and descend the stairs (mean: 37.6 s) was similar to published data of patients who were awaiting and recovering from a total knee replacement.38,39
Physical ability is only part of the rehabilitation process and subsequent quality of life following an amputation. In accordance with previous studies, our results show that a hemipelvectomy has a substantial impact on the physical components of a patient’s health status.15,17 Based on their functional scores, and also the physical component of the SF-36, patients were physically impaired from their hemipelvectomy; however, mental health scores were comparable to the general population. This was based on the patients’ mental component score of the SF-36 compared to the controls (Figure 2(b)). This is similar to previous reports of patients undergoing a hemipelvectomy, which showed similar physical and mental component scores of the SF-36. 17 Other studies examining lower extremity amputation (transfemoral and transtibial) for oncological conditions have shown worse mental component scores in patients undergoing a transfemoral amputation than the patients in our study. 40 Likewise, patients who undergo a limb-salvage procedure have a similar mental component of their SF-36 score to the patients in our study. 41
Conclusion
Patients who successfully use a modern prosthesis following hemipelvectomy demonstrated good clinical function with and without their prosthesis. A trend was observed for increased function using crutches as compared to a prosthesis. The results observed were comparable to or better than those reported outcomes following lower level leg amputations. Patient health status showed decreased physical component scores but equal mental component scores compared to healthy controls. Modern prosthetic designs appear to improve function following pelvic level amputation.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.