
Abstract
Background:
Limb loss negatively impacts body image to the extent that functional activity and societal participation are affected. Scientific literature is lacking on the subject of cosmetic covering for prostheses and the rate of cosmetic cover utilization by cover type, gender, amputation level, and type of healthcare reimbursement.
Objectives:
To describe the delivery of cosmetic covers in lower limb prostheses in a sample of people with lower extremity amputation.
Study design:
Cross-sectional design
Methods:
Patient records from an outpatient practice were reviewed for people who received a transtibial or transfemoral prosthesis within a selected 2-year period.
Results:
A total of 294 records were reviewed. Regardless of the amputation level, females were significantly (p ≤ 0.05) more likely to receive a cover. Type of insurance did not affect whether or not a cover was used, but Medicare reimbursed more pull-up skin covers.
Conclusion:
There were differences regarding cosmetic cover delivery based on gender, and Medicare reimbursed for more pull-up skin covers at the transtibial level than other reimbursors did. This analysis was conducted in a warm, tropical geographic region of the United States. Results may differ in other parts of the world based on many factors including climate and local views of body image and disability.
Clinical relevance
Cosmetic covering rates are clinically relevant because they provide insight into which gender is utilizing more cosmetic covers. Furthermore, it can be determined which type of covers are being utilized with greater frequency and which insurance type is providing more coverage for them.
Background
There are numerous attributes that contribute to poor cosmesis in a prosthesis. For instance, interface materials may be bulky or colored such that they are highly visible to onlookers. Suspension systems may require buttons, straps, buckles, or other such devices that appear somewhat obviously through clothing and are inconsistent with normal anatomy, thereby also drawing attention. Uncovered pylons lack the required material bulk and shape to provide matching symmetry and anatomic contouring of the involved side. The intersection between prosthetic foot shell and pylon represents another place with captivating and abrupt shape transitions that stand out visibly. 1
Gallagher et al. 2 reported that limb loss has a negative impact on body image to the extent that functional activity and societal participation may be adversely affected in some. Cosmetic covers can assist in prosthesis acceptance, promote functional recovery, and have been shown to positively affect patient outcomes. For instance, Donovan-Hall et al. 3 reported that persons with transtibial amputation (TTA) significantly increased their frequency of engagement in activities that involved revealing their body after 12-week use of a cosmetic cover. Additionally, subjects’ perception of comfort improved. Thus, cosmetic covers can serve an important role in the rehabilitation of persons with lower limb amputation.
Body image may be particularly affected acutely following amputation including initial “preparatory” prosthesis delivery. Preparatory prostheses may contribute to disappointment with prosthetic cosmesis. This is because cosmetic covers are not routinely applied or reimbursed with preparatory prostheses, the limb provided to patients at a time when most are still coping with limb loss. 1 In our practice, cosmetic covers are not provided with the preparatory prosthesis but are offered as part of definitive prostheses. This demonstrates at least one point when reimbursement may directly impact cosmetic cover delivery and indirectly impact body image.
Cosmetic covers begin with a shaped foam block to match the sound leg. Following shaping (Figure 1(a) to (c), (f), and (g)), one of three protective, cosmetic covers may be applied. These include a nylon stocking (Figure 2(c) and (i)), a pull-up skin (Figure 2(d)), or a customized spray-applied cover (Figures 1(d) and (e), and 2(e) and (j)). Nylon stockings are commonly used when alignment changes are anticipated, allowing easy access to components. They are further used as a temporary protective layer for the foam block prior to more permanent covering such as a pull-up or spray skin. Finally, nylon stockings are used in cases where a particular insurer may limit cosmetic options revealing a second point where reimbursement may impact delivery of cosmetic covering and potentially body image. Pull-up skin covers provide a more permanent, durable, and seemingly more acceptable cosmetic finish. Challenges to providing a pull-up skin cosmetic cover include additional labor and higher cost. Finally, custom spray skin can be the most aesthetically pleasing but possibly the most fragile and costly cosmetic alternative. Factors that affect patient preferences for use of a cover or selection of a specific type of cover are unknown.
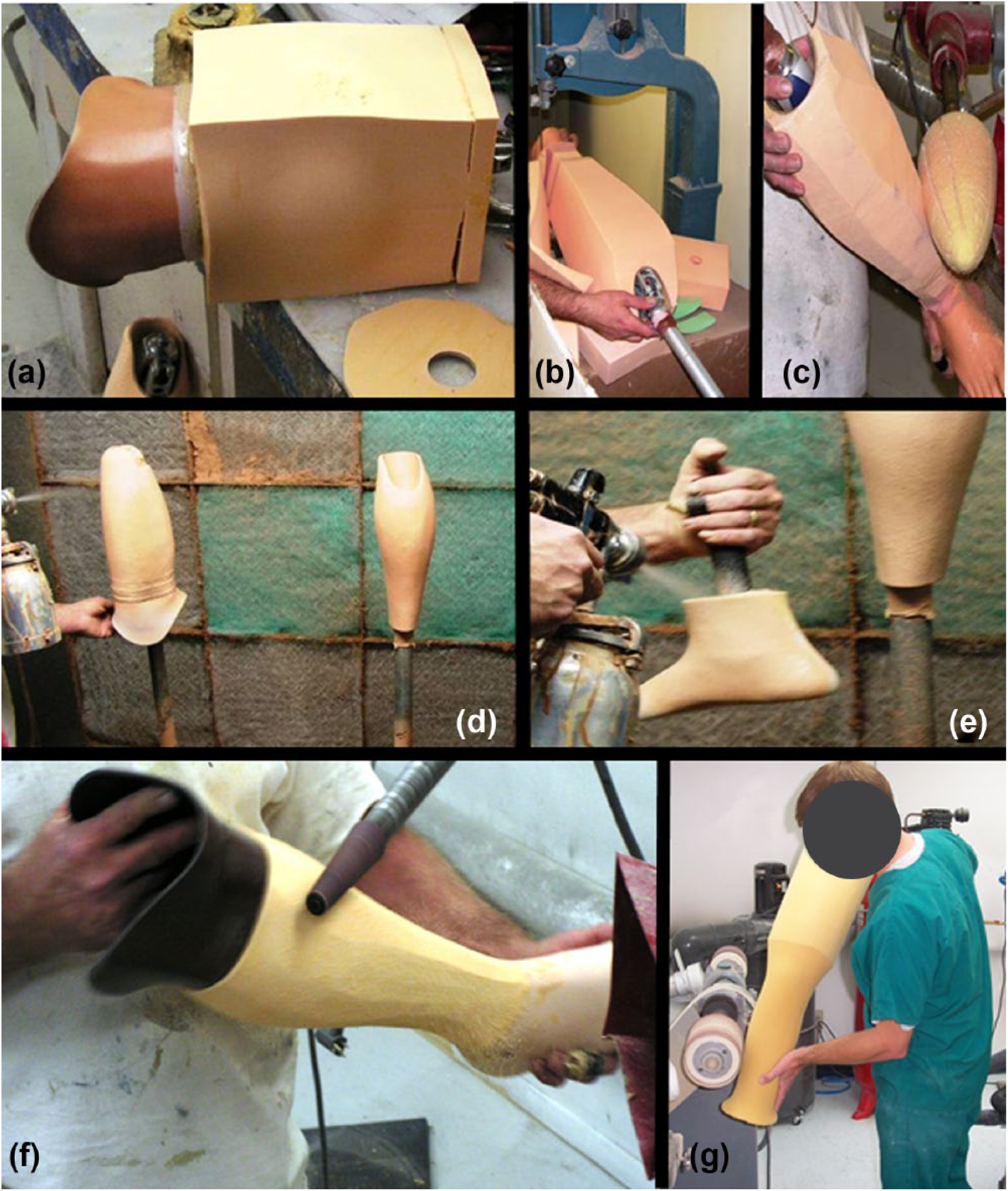
Technical steps in cosmetically covering a prosthesis: (a) fitting a socket into a foam block, (b) preliminary shaping—in this case, this includes sawing away excess material bulk, (c) further shaping via ablation, (d) initial spray layers for a custom spray-applied skin finish, (e) spraying skin onto a foot to assure final color and texture matching, (f) shaping a transtibial prosthesis, and (g) shaping a transfemoral prosthesis.

Cosmetic covering options. Transtibial covers are 1(a) to (e). Transfemoral covers are 1(f) to (j). (a) Laminated cover, (b) foam block with preliminary shaping, (c) nylon stocking over shaped foam block, (d) pull-up skin over shaped foam block, (e) custom spray-applied skin over shaped foam block, (f) some patients prefer or lack reimbursement for a cosmetic finish as shown here—this is a finished prosthesis, (g) some patients prefer only to have a pigmented lamination as their final cosmetic finish, (h) foam block for transfemoral prosthesis prior to shaping, (i) nylon stockings over shaped foam block, and (j) custom spray-applied skin over shaped foam block.
Prosthetic acceptance is influenced by comfort, function, and cosmesis.4,5 Similarly, body image is influenced by social values including vitality, fitness, and physical appearance (i.e. cosmesis). 6 Use of a cosmetically covered prosthesis may improve body image, self-acceptance, and social acceptance in part by providing a means of presenting one’s self to others and allowing the individual to be seen first before potentially revealing a disability (i.e. amputation). 5 It is unclear whether there are differences in body image perception among persons with amputation based on gender, amputation level, or other demographic variables as results are presently conflicting. For instance, Miller 7 found no significant difference between males and females in terms of reported differences in body image perception. Breakey found no difference based upon age or amputation level; however, Zidarov et al. reported poorer body image perception at more proximal amputation levels (i.e. transfemoral compared with transtibial levels).7–9 Through qualitative analyses, Murray 5 reported that cosmesis may be prioritized partially in relation to etiology and gender, with the latter being counter to Miller’s 7 findings, but in agreement with Elnitsky et al. 10 It seems plausible that certain demographic variables are related to body image perception. However, based on previous studies which used standardized survey instruments and qualitative analyses, demographic differences are not eminently clear. Nevertheless, if cosmetic cover utilization can potentially improve body image, then rates of cosmetic cover delivery may be related and should be part of the discussion. Unfortunately, scientific literature on the subject of cosmetic covering for prostheses, including the rate of cosmetic cover delivery by type, gender, amputation level, and type of healthcare reimbursement is not presently available. Therefore, this study’s purpose was to describe the delivery of cosmetic covers in lower limb prostheses in a sample of persons with lower extremity amputation with regard to demographic factors including level of amputation, gender, age, and insurance type. We hypothesized cosmetic cover delivery would be higher among females and persons with TTA.
Methods
The study protocol was approved by the University of South Florida’s Institutional Review Board. A cross-sectional design was utilized for the study. Patient records from an outpatient prosthetic practice in Tampa, Florida (USA) were reviewed and included for all persons with TTA and transfemoral amputation (TFA) who received a prosthesis within a pre-selected 2-year period based on convenience. Records were excluded if patients had amputations other than TTA or TFA or were bilaterally involved. The following data were collected from patient records that were included:
Gender;
Insurance or payment source;
Utilization of a cosmetic cover or not within the study period;
If a cosmetic cover was documented in the record, which type of cover was utilized.
Statistical analysis
Nominal (i.e. gender, type of insurance) and continuous (i.e. age, frequency counts) data were collected. Where possible, descriptive statistics (frequencies, means, and standard deviations) were calculated and stratified by amputation level (TTA or TFA). Comparisons were first made across whether a cover was delivered. Then, comparisons were completed to determine whether there was a difference between type of cover delivered and demographics. To determine whether significant differences existed regarding delivery and demographics, chi-square/Fisher’s exact tests were used for categorical variables (e.g. gender and type of insurance) and analysis of variance (ANOVA) or independent samples t-tests for continuous variables (age). Analyses were completed using SPSS v22.0 (Armonk, NY, USA). Significance was set, a priori, at p ≤ 0.05. To determine whether cover delivery could be predicted by demographics, logistic regression models were completed using the predictors that were significant in the univariate analysis.
Results
In total, 294 records met eligibility and were reviewed. Of these, 221 were TTA and 73 were TFA (Table 1). The overall mean age was 58.9 ± 16.0 years. By gender, 18 of 73 TFAs and 50 of 221 TTAs were female. Overall, significantly more people did not receive a cover (χ2: p < 0.001). As shown in Table 1, males were significantly less likely to receive a cover for both TTA (p = 0.003) and TFA (p = 0.02). Type of insurance did not affect whether or not a cover was delivered, regardless of amputation level.
Use of cover by demographics.
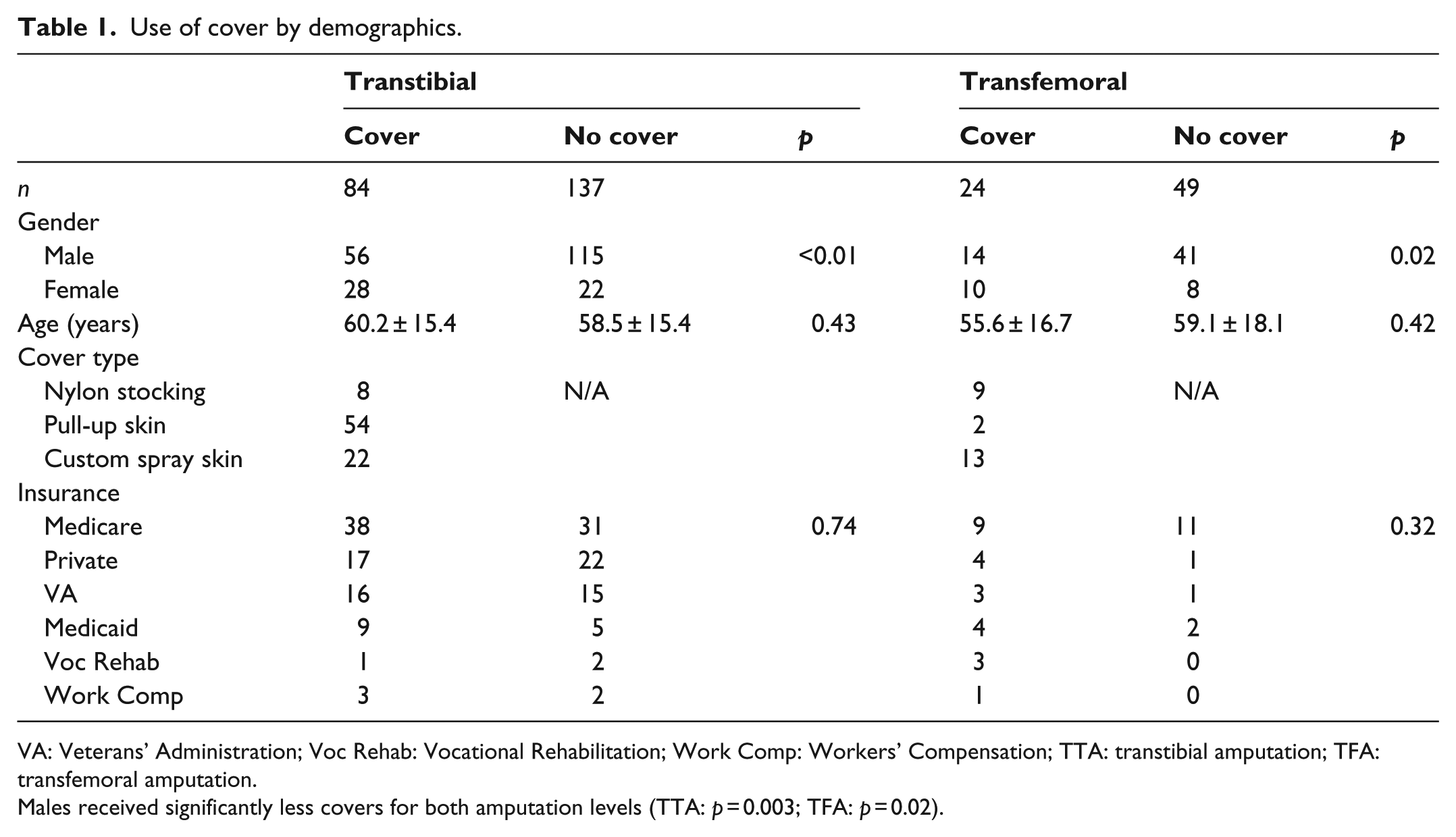
VA: Veterans’ Administration; Voc Rehab: Vocational Rehabilitation; Work Comp: Workers’ Compensation; TTA: transtibial amputation; TFA: transfemoral amputation.
Males received significantly less covers for both amputation levels (TTA: p = 0.003; TFA: p = 0.02).
Regarding persons with TTA who received covers (Table 2), the majority of the individuals (64%) received a pull-up skin cover. There was no relationship between gender or age and type of cover received among TTAs. However, a greater proportion of those with Medicare insurance received a pull-up skin cover compared to those with other forms of insurance (p = 0.02).
Cover type by demographics for patients who received covers.
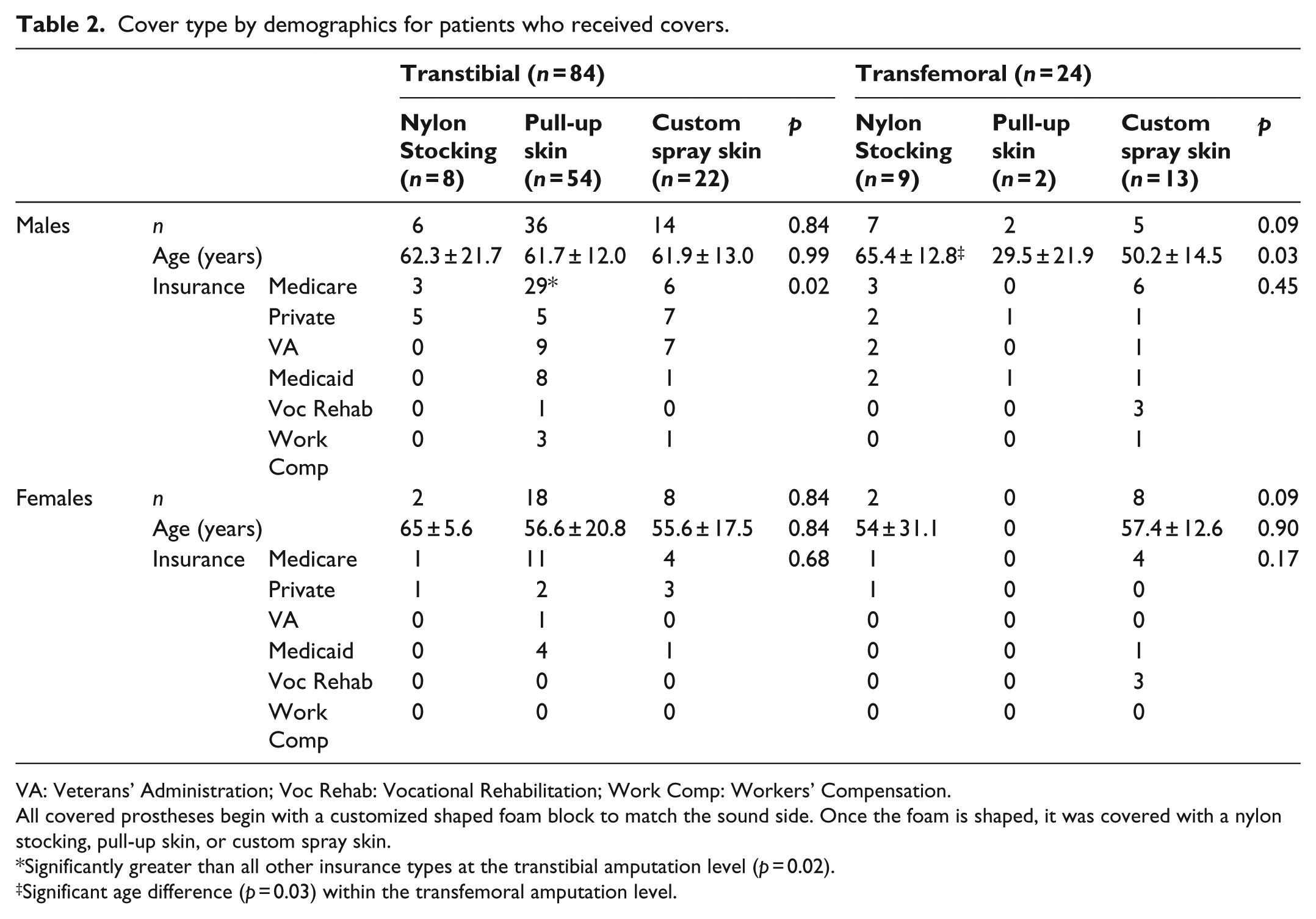
VA: Veterans’ Administration; Voc Rehab: Vocational Rehabilitation; Work Comp: Workers’ Compensation.
All covered prostheses begin with a customized shaped foam block to match the sound side. Once the foam is shaped, it was covered with a nylon stocking, pull-up skin, or custom spray skin.
Significantly greater than all other insurance types at the transtibial amputation level (p = 0.02).
Significant age difference (p = 0.03) within the transfemoral amputation level.
For individuals with TFA (Table 2), there was no relationship between type of cover and gender or insurance coverage. There was a statistically significant difference (p = 0.03) in age between the group of persons with TFA receiving a pull-up skin cover (29.5 ± 21.9 years) compared to those receiving a nylon stocking cover (65.4 ± 12.8 years). Results from the logistic regression indicated that women were more likely to receive covers than men in both the TTA (p = 0.003) and TFA (p = 0.02) groups. (Table 3)
Logistic regression to predict whether or not a person uses a cover.
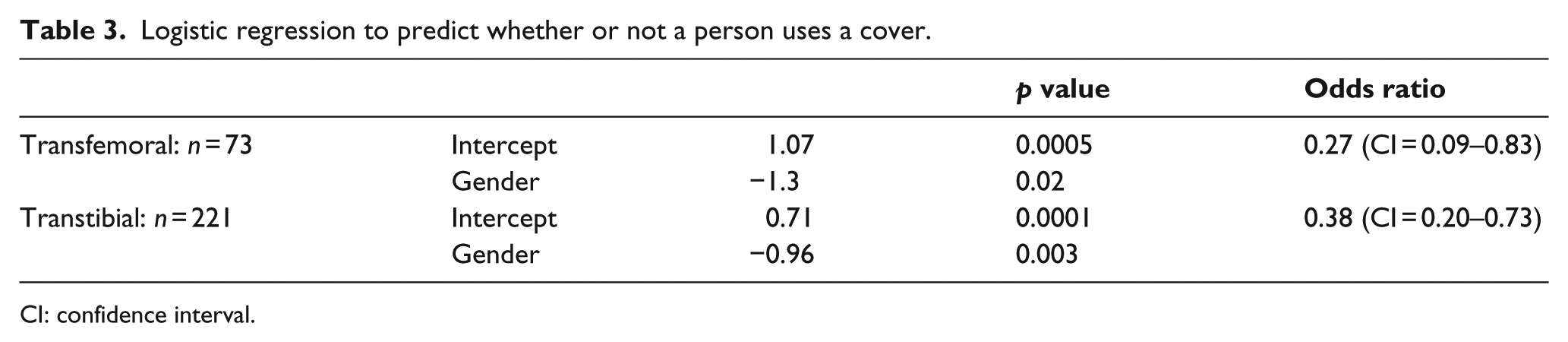
CI: confidence interval.
Discussion
This sample comprised 75% TTA and 25% TFA with 20% female representation and mean age of 58 years. With regard to sample distribution characteristics, this is comparable to a study of psychological adjustment in persons with lower limb amputation whose cohort was 64% TTA, 24% TFA, 24% female representation, and mean age of 64 years. 11 Similarly, another study investigating issues of importance to persons using prostheses had 63% TTA, 25% TFA, 14% female representation, and mean age of 55 years, which was also comparable to this study sample. 12
We hypothesized that more females than males would receive cosmetic covers. This was indeed the case. In this sample, 56% of females with amputation received a cover, while only 31% of males did. This is consistent with Elnitsky et al. and Murray, who both report that females may have a heightened concern about body image. Moreover, females rated utility/usefulness, appearance, smell, and sound of their prosthesis as being more important than males did. 12 In another study, overall prosthetic satisfaction and body image disturbance were inversely correlated for both males and females. However, in the same study, increased functional satisfaction of the prosthesis and lower body image disturbance had a statistically significant inverse correlation for males, whereas for females, functional, aesthetic, and weight satisfaction all had statistically significant inverse correlations with body image disturbance. 13 The study’s findings and the literature support the study’s hypothesis that females with lower limb amputation would have a higher percentage of covers delivered.
The hypothesis that more covers would be delivered at the TTA level was generated in collaboration with participating clinicians. Clinicians anecdotally reported a greater number of persons with TTA requesting cosmetic covers due to the desire to wear shorts in the local temperate climate (Tampa, FL, USA). Regarding less cover utilization in persons with TFA, also anecdotally, participating clinicians conveyed that patients would at times feel that a discontinuous cover, necessary to access knee componentry for charging or to permit uninhibited knee movement, was more visually notable than a non-covered prosthesis. This hypothesis could partially support an explanation as to why persons with TTA reportedly wear their prosthesis for longer periods compared to those with TFA. 14 Body image is a reported concern at more proximal amputation levels. 9 Thus, if cosmetic covers cannot be utilized as efficiently by persons with TFA, then this is a plausible, contributing explanation for why these individuals might wear their prosthesis less. Further research is required to determine whether a discontinuous TFA cover (Figure 2(i) and (j)) is more bothersome to users, notable to onlookers, and whether full-length transfemoral cosmetic covering would alter prosthetic knee functionality.
Regarding insurance coverage, given that the majority of patients accessing prosthetic care at the study practice were of Medicare age and would likely have met other Medicare eligibility requirements, it was hypothesized that Medicare would comprise the largest percentage of reimbursement for cosmetic covers. Demographic data show that majority of persons with amputation are older with an age range of 55–64 years11,12 and that Medicare eligibility in the United States includes individuals aged 65 years or older as well as younger individuals with disabilities. Except for the group of subjects with TFA who received pull-up skin covers, the mean age per sub-group by amputation level and type of cover delivered was 50.2–65.4 years. The former group of persons with TFA who received pull-up skin covering, while significantly younger (p = 0.03), may be a spurious finding as this was the smallest group (n = 2). Government agencies such as Medicare, Medicaid, Department of Defense, and Department of Veterans Affairs provide 40%–50% of reimbursement for prosthetic services and devices in the United States. 15 Thus, the hypothesis that significantly more covers (p = 0.02) were reimbursed by Medicare was supported.
Finally, concerning cosmetic covering type, we hypothesized that the cover providing the optimal balance of durability, aesthetics, and economy would be most commonly selected and utilized. In our estimation, that combination of parameters would best be met with a commercially available pull-up skin cover. The nylon stocking cover would have been a less costly option but less protective and less aesthetically pleasing. At the highest end of cost, time to finish, but most aesthetically pleasing would be the custom spray-applied skin. Overall, there were significantly more pull-up skin covers delivered (χ2: p < 0.001), thus confirming our hypothesis.
Limitations
Study limitations included limited information availability in patient records. For example, no record of removable foam covers existed, so it is unclear how these are classified. Furthermore, only third party reimbursements were found in the records, and it is thus unclear whether any patients paid out-of-pocket for cosmetic covers. Another consideration may be that persons with amputation may get part of the prosthetic cover at one provider and then get final customization at another. This may be due to preference for specific artistic finishing (e.g. tattoo) or that specific services were not available at the first location. Records of cosmetic work provided by another facility would not have been available as part of this review. The convenience sample likely creates some limitations to a longer view of cosmetic cover delivery patterns and thus could limit generalizability of findings.
Multiple aspects of cosmesis were not considered in this study, for example, the selection and impact of adjustable heel height feet and cosmetic socket finishes. Finally, the limitation bearing the greatest consideration is that the demographics and frequency of cosmetic cover delivery and climate of the study site may not be representative of or generalizable to other practices, so caution should be exercised when attempting to do so. Future work should consider a multi-site study and perhaps a study of cosmetic cover utilization to extend findings beyond delivery patterns.
Conclusion
Because society values physical appearance, limb loss adversely impacts body image. In persons with lower limb amputation, cosmetic covers can facilitate presentation of person prior to presentation of impairment. Thus, cosmetic cover usage may favorably impact body image. Previous survey and qualitative studies disagree on the influence that demographic variables such as amputation level and gender have on body image. This study used rates of delivery of cosmetic covering to determine the influence of the aforementioned demographic variables. Regardless of amputation level, fewer males received covers compared to females. In persons with TTA, Medicare reimbursed for pull-up skin covers more than other cover types. Using these methods, it seems that gender, reimbursor, and cover type may be important to consider when discussing or studying cosmetic covering and body image in persons with lower limb amputation.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.