
Abstract
Background:
Immobilization of the wrist joint with a splint is an established approach for ulnar-sided pain due to ulnocarpal abutment syndrome. However, patients have a tendency to stop wearing the splints because of its inconvenience and there have been no reports based on splint therapy.
Objective:
We investigated the usefulness of a newly designed custom-made aluminum splint for ulnar-sided wrist pain.Study design: This was a cohort study of the aluminum splint therapy for the patients who had been primarily treated with a conventional splint but ceased to use it because of the inconvenience in activities of daily living.
Methods:
The subjects included 10 female patients (mean age = 44.2 years). The outcome was assessed using the visual analogue scale score for pain, the disabilities of the arm, shoulder and hand score, range of motion of the wrist, and the grip strength. The mean follow-up period after wearing the aluminum splint was 8.8 months.
Results:
All parameters, including the visual analogue scale pain and disabilities of the arm, shoulder and hand scores, improved significantly (p < 0.05) following use of the aluminum splint relative to the pretreatment scores. Seven patients continued to use the aluminum splint, and three of the seven had complete remission from related pain.
Conclusion:
Constant use of the aluminum splint during the study period was associated with improvement in the ulnar-sided wrist pain scores, which reconfirmed that increased adherence to splint use in daily activities is an important intentional behavioral strategy.
Clinical relevance
Although the custom splint is effective for alleviation of wrist pain in ulnocarpal abutment syndrome, continuity of splint use is a key element of conservative treatment. This study showed that a splint that patients were willing to wear in their daily life was a useful device for alleviation of pain.
Background
Ulnocarpal abutment syndrome is a degenerative condition that induces ulnar-sided wrist pain. 1 Repeated excessive load on the ulnocarpal joint causes pathological changes, including tear of the degenerative triangular fibrocartilage complex (TFCC),2,3 chondromalacia of the lunotriquetral bony structure or the ulnar styloid, and ulnotriquetral ligament disruption, in addition to causing certain bony morphological characteristics, such as positive ulnar variance. 4 When ulnar-sided pain becomes intractable, it is exacerbated by ulnar flexion, which restricts wrist motion and leads to severe interference with the activities of daily living. For patients in the early phase of the symptoms, conservative treatment comprising activity modification, medication with nonsteroidal anti-inflammatory drugs (NSAIDs), steroid injections into the ulnocarpal joint, or immobilization with a wrist splint has been recommended.1,5–7 When these are no longer successful, surgical procedures may be proposed. Although medication is not always necessary, pain is exacerbated when patients forcefully use their hands with the wrist in ulnar deviation or when ulnar deviation of the wrist is occasionally caused by, for example, carrying heavy luggage. Ulnar-sided pain is therefore a significant setback with regard to everyday activities. Immobilization of the wrist joint with a splint to limit motion is an established approach and has been described in several textbooks.1,5,6,8 Although the symptoms of ulnocarpal abutment syndrome are sometimes severe in the acute phase, acute flare-up symptoms may often resolve with time for most patients. Such splints comprise a thermoplastic material, or they are commercially made for the wrist joint, but to date, there have been few follow-up studies that have assessed such splint therapy following application.9–11 Most patients affected by this disease are active young or middle-aged individuals, and many are engaged in occupations that require frequent use of both hands. Recent articles reported that patients have stopped wearing hand splints because they interfered with daily activities. There have been no reports on the use of custom-made splints for ulnocarpal abutment syndrome in contrast to reports of studies that examined rheumatoid arthritis of the wrist12–17 and osteoarthritis of the thumb carpometacarpal (CMC) joint. 18
In this study, a newly designed custom-made aluminum splint (AL splint) was used to treat patients with ulnar-sided wrist pain due to ulnocarpal abutment syndrome, who underwent primary treatment using a conventional standard thermoplastic splint (CST splint) but who could not continue using the CST splint because of its inconvenience. In this study, we investigated the outcomes of the treatment using the AL splint and discuss its usefulness for ulnocarpal abutment syndrome.
Methods
The newly designed custom-made AL splint is constructed of a thin, light, rod-shaped aluminum wire (diameter 4.0 mm), which can be bent to fit the forearm and hand with multiple support points to mainly restrict ulnar deviation of the wrist. The newly designed custom-made AL splint is shown in Figure 1.
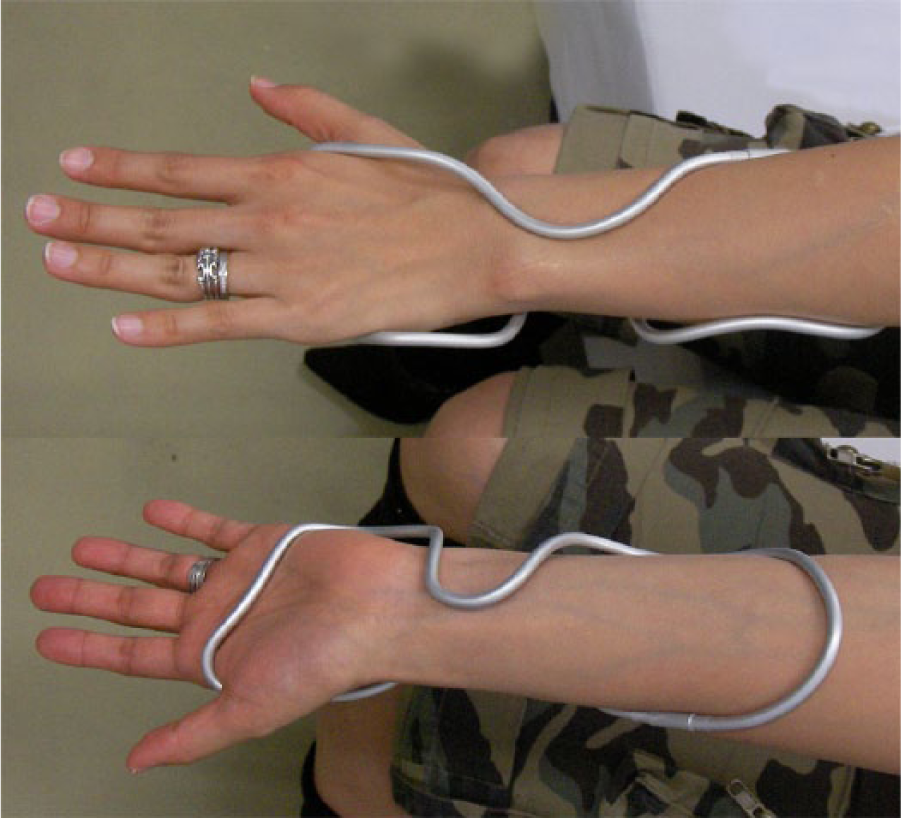
Custom-made aluminum wrist splint.
The bony prominence around the wrist, especially the ulnar head, should not make contact with the wire. The point of support at the dorsal side of the wrist is the soft area just proximal to the distal radioulnar joint. The points of support at the palmar side are at the palm and mid-forearm. Ulnar deviation is restricted by the bar in the first web and the bar adjacent to the hypothenar. The rod is bent round and smoothly well fit to the contour of the wrist. Until the AL splint is properly adapted to the wrist, fitting and remodeling are repeated several times. This splint is light, rigid, and impervious to water, which is the main advantage because it is like a rigid aluminum string twined around the wrist. The splint can be easily applied and removed. We designed the AL splint, but manufacturing was outsourced.
A total of 10 patients who complained of ulnar-sided wrist pain and had been diagnosed with ulnocarpal abutment syndrome based on the basis of symptoms, clinical signs, initial anterior–posterior and lateral radiographic findings, and magnetic resonance imaging (MRI) findings were enrolled in this study. All patients were females, nine of whom had right wrist pain and one had left wrist pain. Their ages ranged from 25 to 60 years, with an average age of 44.2 years. Prior to visiting our institution, the duration of symptomatic ulnar-sided wrist pain due to ulnocarpal abutment syndrome had ranged from 1 to 9 months, according to the patients’ recollections. Seven patients had no history of trauma. Three had onset of symptoms after a fall, one of whom had a history of distal radius fracture. Plain radiographs of the wrist joint showed an average of +1.1 mm positive ulnar variance. Two patients had a degenerative TFCC tear detected by MRI (Table 1).
Demographic data of the patients.
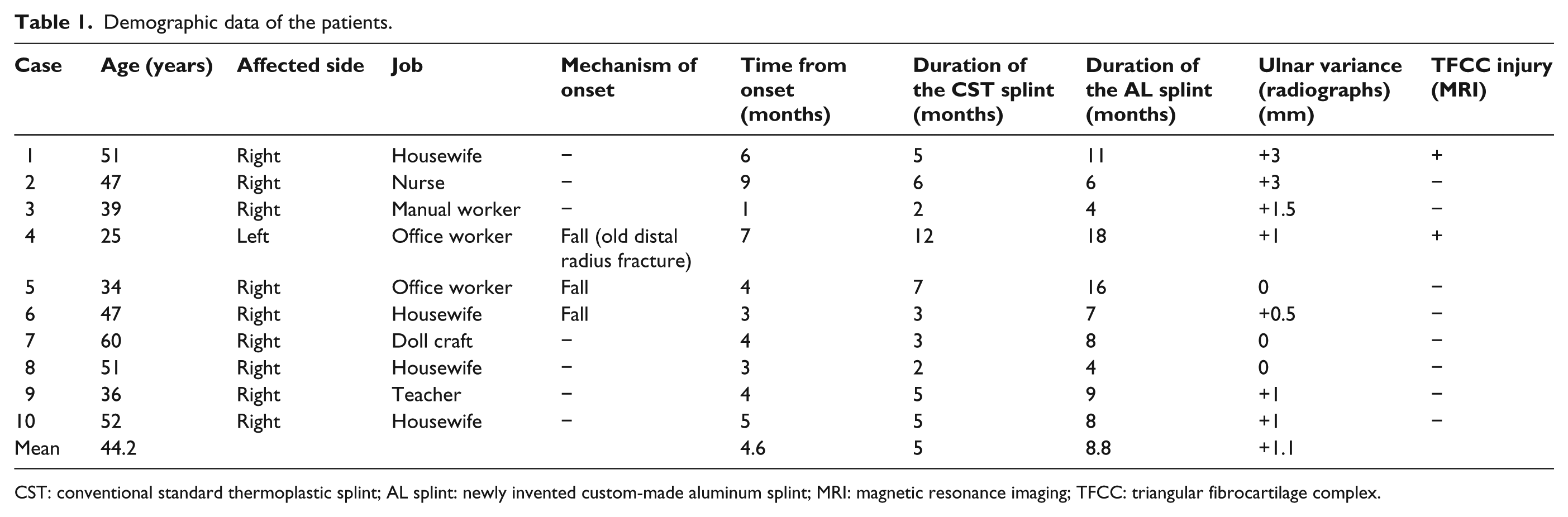
CST: conventional standard thermoplastic splint; AL splint: newly invented custom-made aluminum splint; MRI: magnetic resonance imaging; TFCC: triangular fibrocartilage complex.
All patients were treated with a CST splint at first, and they were instructed to wear the splint preferably the whole day until the pain would subside. However, all had ceased to use the CST splint for an average of 5 months because of its inconvenience in activities of daily living, before the pain would improve. Thus, the AL splint was used instead of the CST splint.
The patients were instructed to wear the AL splint all day but were allowed to remove it at will because of discomfort. The patients were also permitted to stop wearing the splint once symptoms had subsided. Even with decreased but persistent pain, the patients continued to wear the splint for some time or were allowed to wear it, depending on the severity of their symptoms. Reciprocal use of both types of splints was permitted on occasion. While the patients were participating in this study, they did not partake in combination therapy with NSAIDs.
Treatment outcome assessments following use of the CST and AL splints included interviews with patients and physical examination, including range of motion (ROM) of wrist and grip strength, as well as subjective pain assessments using the 100-mm visual analogue scale score for pain (VAS pain) and disabilities of the arm, shoulder and hand (DASH) score for the assessment of upper extremity functions. Assessments were performed three times; before treatment, post-treatment after cessation of CST splint use and at commencement of AL splint use, at final assessment after using AL splint. The follow-up period after commencement of AL splint use ranged from 4 to 18 months, with an average of 8.8 months. The Wilcoxon signed-rank test was used to compare the improvements in the VAS pain score, DASH score, ROM of the wrist, and grip strength of all patients at all three assessments. Differences with p < 0.05 were considered to be significant.
Improvement in VAS pain was expressed as the percentage of reduction in the post-treatment value relative to the pretreatment value according to the following equation: %VAS pain improvement = [(pretreatment value − post-treatment value)/pretreatment value] × 100.
Ethical approval was granted from the institutional review board of Tokai University School of Medicine, and informed consent was obtained from all patients.
Results
In this series, because of ulnocarpal abutment syndrome, most subjects at pretreatment had mild to severe motion pain on ulnar deviation during daily living activities, and some had mild swelling on the ulnar side with an average of 56.0-mm VAS pain and disablement of upper extremity function with an average DASH disability/symptom score of 30.1 points. After treatment using the CST and AL splints, pain symptoms in all patients improved (Figure 2). At the time of post-treatment following use of the CST splint, only the VAS pain and DASH scores showed statistically significant improvement relative to the pretreatment scores. However, following use of the AL splint, all evaluated parameters, including the VAS pain score, DASH score, ROM, and grip strength, showed statistically significant improvement relative to the pretreatment status. The improvement in %VAS pain was 44.3% for the CST splint and 51.7% for the AL splint relative to the pretreatment scores, both of which were statistically significant (Table 2). However, except for wrist flexion, there were no significant differences in any of the parameters between the two splints at post-treatment.
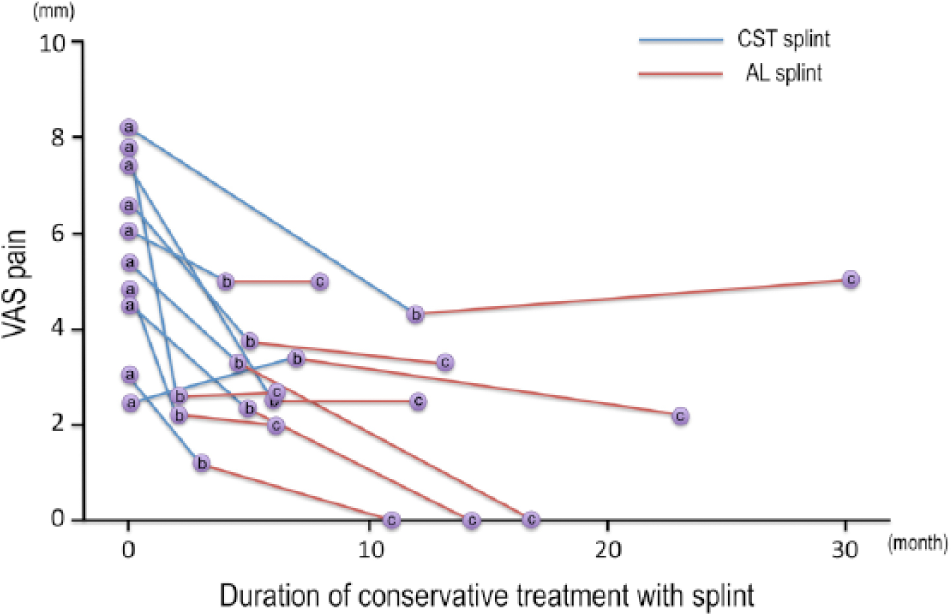
Relationship between VAS pain and duration of splint therapy. The blue line represents the period of CST splint therapy, and the red line represents the period of AL splint therapy. VAS pain was measured at three times: (a) before treatment, (b) post-treatment at cessation of CST splint use and at commencement of AL splint use, and (c) at final assessment after AL splint use (c).
Patient data.
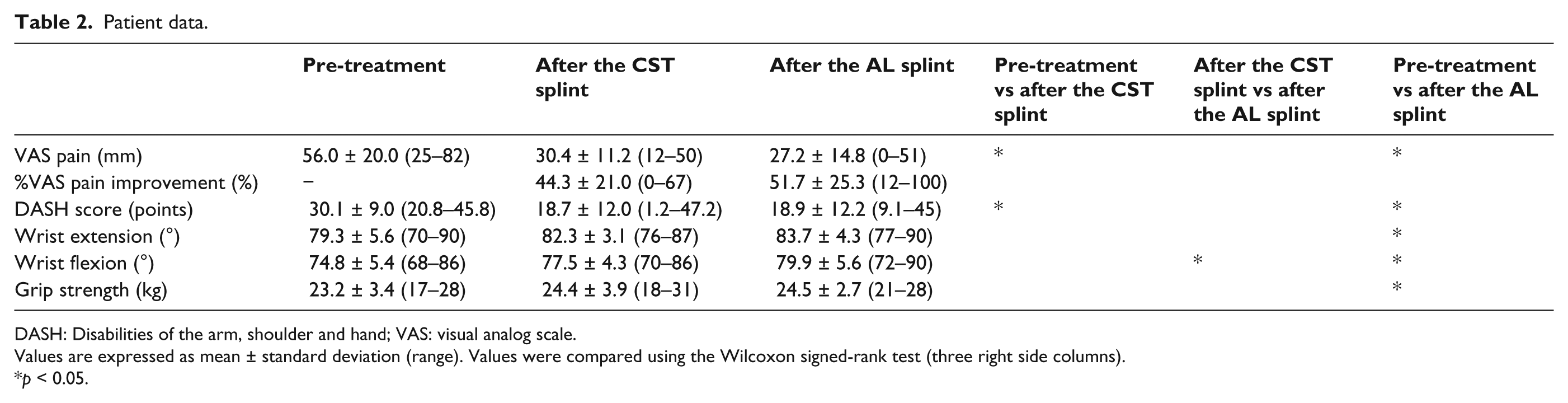
DASH: Disabilities of the arm, shoulder and hand; VAS: visual analog scale.
Values are expressed as mean ± standard deviation (range). Values were compared using the Wilcoxon signed-rank test (three right side columns).
p < 0.05.
The main reasons for patients not continuing to wear the CST splint were that they could not wear it during wet or dirty activities such as washing, cleaning or bathing; discomfort from sweating; because of the weight of the splint material, its unsightly appearance, or inconvenience. After changing to the AL splint, most patients had no complaints about its appearance during an average of 8.8 months of follow-up. All patients accepted the design, appearance, and feeling of the splint and were willing to wear it. No patients reported removing the splint during social occasions, and no skin symptoms from wearing the AL splint were noted. At final follow-up, seven patients continued using the AL splint, five used it all day long, and two used it when symptoms became worse or when in contact with water. The other three patients had complete remission from ulnar-sided wrist pain and were able to conduct all daily activities without the splint. One patient was able to play tennis without painful restriction. Unexpectedly in this series, all patients were female, and they were willing to wear the AL splint as if it was a bracelet. One patient reverted to using the CST splint on an occasion because of the reduced rigidity of the AL splint relative to the CST splint. No patient complained of loss of ulnar-sided palm sensation while wearing the AL splint. Two patients reported loosening of the splint when working with soap and water. One patient reported that the advantages of the splint’s design were evident while performing fine manual activities, such as pinching movements, picking up small objects, or turning a page. Three patients reported reduced functional ability when grasping an object because the aluminum bar across the palm compromised performance. These patients reported that they had removed their splint to accomplish gripping movements such as grasping a knife or using a computer mouse.
Discussion
As described previously, conservative management, such as medication, intra-articular steroid injection, heat therapy, and splint fixation, have been advocated as initial treatments for ulnar-sided wrist pain due to ulnocarpal abutment syndrome. 19 Few evidence-based recommendations for splint therapy for this syndrome have been proposed, because there have been few reports on randomized controlled trials that have examined this therapy. 11 According to previous studies that examined use of hand splints in osteoarthritis of the CMC joint and wrist joints, the primary focus was patient motivation for and compliance in using splint.11,10,15,16,18,20 The authors of these studies concluded that the adherence determinants were support and protection, appearance, comfort, fitting, and problems with attachment and removal of the splint in addition to symptom relief, such as relief from pain and swelling. To our knowledge, there have been no reports of case series or comparative studies examining wrist joint splints as applied to ulnocarpal abutment syndrome.
In this series, the CST splint was proven to be effective in all patients for reducing ulnar-sided pain, as measured by the VAS pain and DASH scores. However, patients ceased to use the CST splint because of the high degree of inconvenience in daily use. Therefore, after a long period of CST splint treatment and eventual discontinued use, the CST splint was changed to the custom-made AL splint that we devised; therefore, this study was not a comparison of the CST and AL splints.
After the improvement of ulna-sided wrist pain following use of the CST splint, the AL splint that we devised did not exacerbate the pain symptoms, as assessed by the VAS pain score, DASH disability/symptom score, and other objective measurement parameters. The AL splint also enabled a greater degree of functionality in daily activities in addition to providing rigid support.
One limitation of this study was that it was not clear whether the improvements in pain measures resulted from spontaneous recovery after longstanding observation or from use of the custom-made AL splint.
Other limitations were the lack of strict criteria for splint therapy and for strict diagnosis of ulnocarpal abutment syndrome. Moreover, there were no critical objective evaluation methods to measure the appearance, fit, comfort, and functionality of the AL splint, and some results are subjective because of the method of analysis of patients’ interviews.
The advantages of the AL splint are numerous. It is simple to custom-fit the splint to a patient’s arm, and it can be used when in contact with water. Similar to the CST splint, the custom-made AL splint provides rest and immobilization for pain relief and can also be used for support or protection against accidental subconscious wrist motion in daily activities. However, the custom-made splint has certain disadvantages. Several attempts may be necessary to fit the splint adequately to the patient’s arm, with a concomitant time requirement. The splint can easily detach when the patient is working with soap and water. For some individuals, it can be difficult to exert strength with the palm of the hand, thus rendering it necessary to remove the splint for certain situations where otherwise there would be reduction in functional ability. In particular, gripping or grasping movements are very difficult because the aluminum bar across the palm obstructs performance, but this criticism can be leveled at all types of wrist splint.
Although the outcome parameters at post-treatment following use of the AL splint do not prove the functional superiority relative to that of the CST splint, we concluded that the design of the AL splint enabled a greater degree of functionality in daily activities, which enabled much better long-term compliance with the goal of continual use and led to improvement in the symptoms. Even if the wrist splint is useful for alleviation of pain, its use does not guarantee that all patients can achieve satisfactory function of the upper extremity. This fact underlies the important conclusion that the continuity of splinting or prescribing the splint to be used in daily living is a key element of conservative treatment.16,21,22
Conclusion
The AL splint is an effective symptom modifier because it can be used in intentional behavioral strategies to increase adherence to the goal of continual use of the splint. Therefore, until abatement of symptoms in ulnocarpal abutment syndrome, patients are free to apply or detach the splint in the course of their daily lives. It is desirable to provide splint configurations that will be worn by patients much more often than will be a conventional splint when performing daily activities.
Footnotes
Acknowledgements
The authors wish to thank Mr. Hidehiro Suda and Mr. Toshiaki Katori at Katorigishi Co., Inc. (Tokyo, Japan) for their valuable support in the production of the custom-made wrist splint.
Author contribution
First author (Masayoshi Ikeda) prepared the article and the other authors accepted the contents.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.