
Abstract
Background:
An ankle–foot orthosis is suggested to actively assist dorsiflexion of the foot by induction of a positive proprioceptive impact to ankle dorsiflexor muscles. However, an objective proof is missing.
Objectives:
To assess the proprioceptive impact of an ankle–foot orthosis application by Hoffmann reflex recordings of the soleus muscle under static conditions. It was hypothesized that the use of an ankle–foot orthosis facilitated dorsiflexor motor function and thus a decreased the soleus Hoffmann reflex.
Study design
Experimental study in healthy volunteers, pre–post test design.
Methods:
In all, 20 healthy volunteers were enrolled in order to assess the proprioceptive impact of orthosis application. The Hoffmann reflex was recorded before, during, and after orthosis application.
Results:
Under orthosis application, the Hoffmann reflex significantly decreased as compared to before (p < 0.05) and after application (p < 0.05).
Conclusions:
Findings indicate an inhibition of plantarflexors probably induced by facilitation of ankle dorsiflexors under static conditions. At first glance, it seems that foot orthoses primarily have a stabilizing effect on ankle joints in terms of simple mechanical bandages. However, the present results suggest an additional active impact on proprioceptive control.
Clinical relevance
The putative neuromodulatory effect on motor control may support the application of such ankle–foot orthoses in, for example, drop foot. Furthermore, the objective assessment of a neurophysiological mode of action of orthoses by Hoffmann reflex recordings might be an appropriate primary outcome parameter in clinical trials.
Background
Drop foot is caused by peripheral or central neuropathy, leading to weakness of dorsiflexor muscles.1,2 Symptomatic treatment of drop foot includes strength training, ankle–foot orthoses, and implantable medical devices.3–8 The ankle–foot orthosis of this study is proposed to stabilize the ankle and to actively assist dorsiflexion by induction of excitatory proprioceptive input to the ankle dorsiflexor muscles.
The proprioceptive impact of external factors can be examined by the Hoffmann reflex (H-reflex).9–11 Previous studies applied H-reflexes of lower limb muscles to assess proprioceptive impact of brace application.12,13 Upon electrical stimulation of peripheral nerves above motor threshold, a short-latency M-wave reflects direct activation of efferent α-motoneurons, and a long-latency H-reflex, reflecting activation of Ia-proprioceptive fibers. 10 At high intensities, the M-wave predominates, while the H-reflex disappears due to antidromic collision. 10 The M-wave is generally accepted as an indicator of stable stimulation conditions in H-reflex studies.11,14
H-reflex recordings from tibialis anterior muscle (tibialis anterior) at rest are known to be highly variable within and between individuals.15,16 The antagonistic soleus muscle (soleus) is the standard muscle for H-reflexes.17–20 Reciprocal inhibitory projections between motoneurons of soleus and tibialis anterior physiologically control the balance of activity between these antagonists. 21 Thus, assessing the soleus H-reflex may also indicate changes of motoneuron excitability of tibialis anterior. The aim of this study is to examine the proprioceptive impact of an ankle–foot orthosis in healthy volunteers.
Methods
In all, 20 healthy volunteers (10 females and 10 males; 22.8 ± 1.7 (standard deviation (SD)) years) were recruited for three experiments and a total of 32 experimental sessions. The research was approved by the appropriate regional research ethics committee. All investigations were in accordance with the protocol and followed the ethical and humane principles of research. Subjects gave their informed consent prior to inclusion in the study according to the Declaration of Helsinki. Volunteers were without any lower extremity injuries or ankle pathologies.
This study consisted of three experiments: two preliminary experiments and one main experiment (Figure 1). One preliminary experiment was designed to investigate effects of agonistic or antagonistic muscle preactivation on the H-reflex of the soleus (ExpPreact). The other preliminary experiment was designed to test proprioceptive impact of two different orthosis prototypes, using H-reflex recordings of the soleus (ExpProto). The main experiment was designed to assess and quantify a possible proprioceptive effect of orthosis application (ExpOrthosis). The orthosis chosen for ExpOrthosis was based on results from ExpProto.
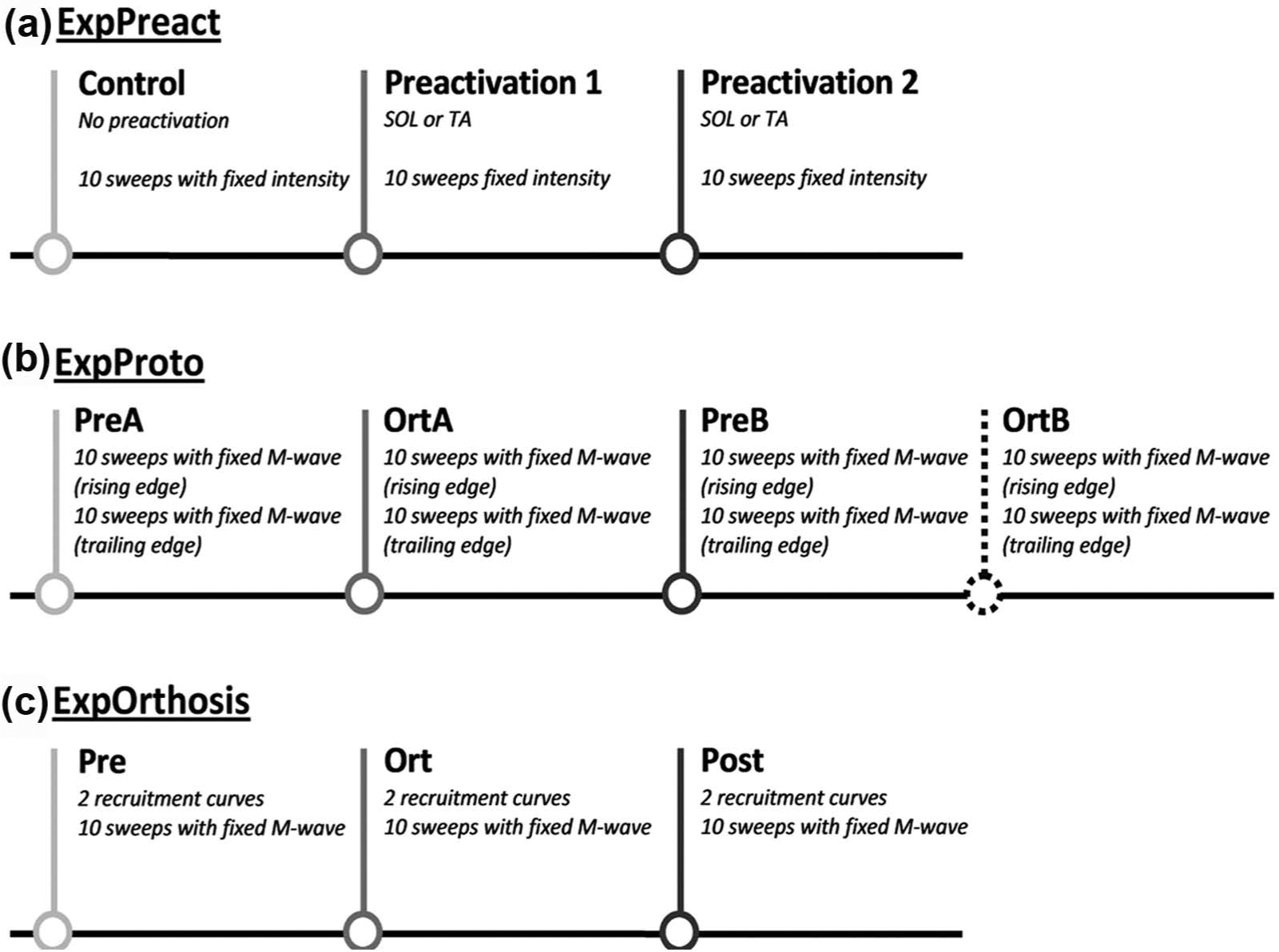
A schematic illustration of experimental conditions within two preliminary experiments ExpPreact and ExpProto, and the main experiment ExpOrthosis. ExpPreact had three experimental conditions: an initial control condition without muscle preactivation (Control) and two subsequent conditions with preactivation of either soleus (SOL) or tibialis anterior (TA). ExpProto had four experimental conditions: one before wearing orthosis prototype A (PreA), one while wearing orthosis prototype A (OrtA), one before wearing orthosis prototype B (PreB), and an additional condition while wearing orthosis prototype B (OrtB). The main experiment, ExpOrthosis, had three experimental conditions: one before wearing the orthosis (Pre), one while wearing the orthosis (Ort), and one after having worn the orthosis (Post).
Volunteer positioning
Volunteers were asked to adopt a prone position on a level examination bed and to turn their head to either left or right, whichever proved most comfortable. Volunteer’s hands were placed next to their waist. The lower leg was raised with a cylindrical, padded, supporting bolster, placed under the tibia, slightly proximal to the ankle (approximately 20°–25° knee flexion). Position was documented in order to verify this prior to each stage of the experiment.
Electrode attachment
In all experiments, two electromyography (EMG) surface electrodes were fixed on both tibialis anterior and soleus bellies, each with defined recording sites. Two reference electrodes were fixed on the anterior border of the tibia: one for tibialis anterior and other for soleus. The anode of a pair of stimulation electrodes was fixed to the anterior aspect of the distal thigh. A mobile cathode was then used to search for optimal cathode position for stimulation of tibial nerve. The stimulus was a 1-ms rectangular pulse, with an intensity suited to elicit a H-reflex response. The optimal cathode location, producing a significant H-reflex with no M-wave, was marked, and the mobile cathode was substituted with a surface electrode.
ExpPreact
The experiment addressed the influence of plantarflexor (soleus) or dorsiflexor (tibialis anterior) preactivation on the soleus H-reflex. It was hypothesized that slight preactivation of the agonistic soleus muscle facilitated the soleus H-reflex, and that slight preactivation of the antagonistic tibialis anterior muscle inhibited the soleus H-reflex. Both hypotheses were crucial for definition and interpretation of the subsequent experiment ExpOrthosis that investigated a possible impact of the ankle–foot orthosis on the soleus H-reflex.
Five volunteers participated in two experimental sessions each. In each experimental session, only one leg was tested in randomized order. Initially, the soleus response was recorded upon stimulation of the tibial nerve with increasing stimulation intensities from 0 to maximum 20 mA, with incremental steps of 0.5 mA (Figure 2). From these recordings, two recruitment curves (RCs) were generated. RC generation was interrupted before 20 mA, when M-wave was estimated to have reached its maximum. Thresholds for local sensation at site of stimulation and sensation of projection in the nerve’s receptive field were assessed during RC recordings.
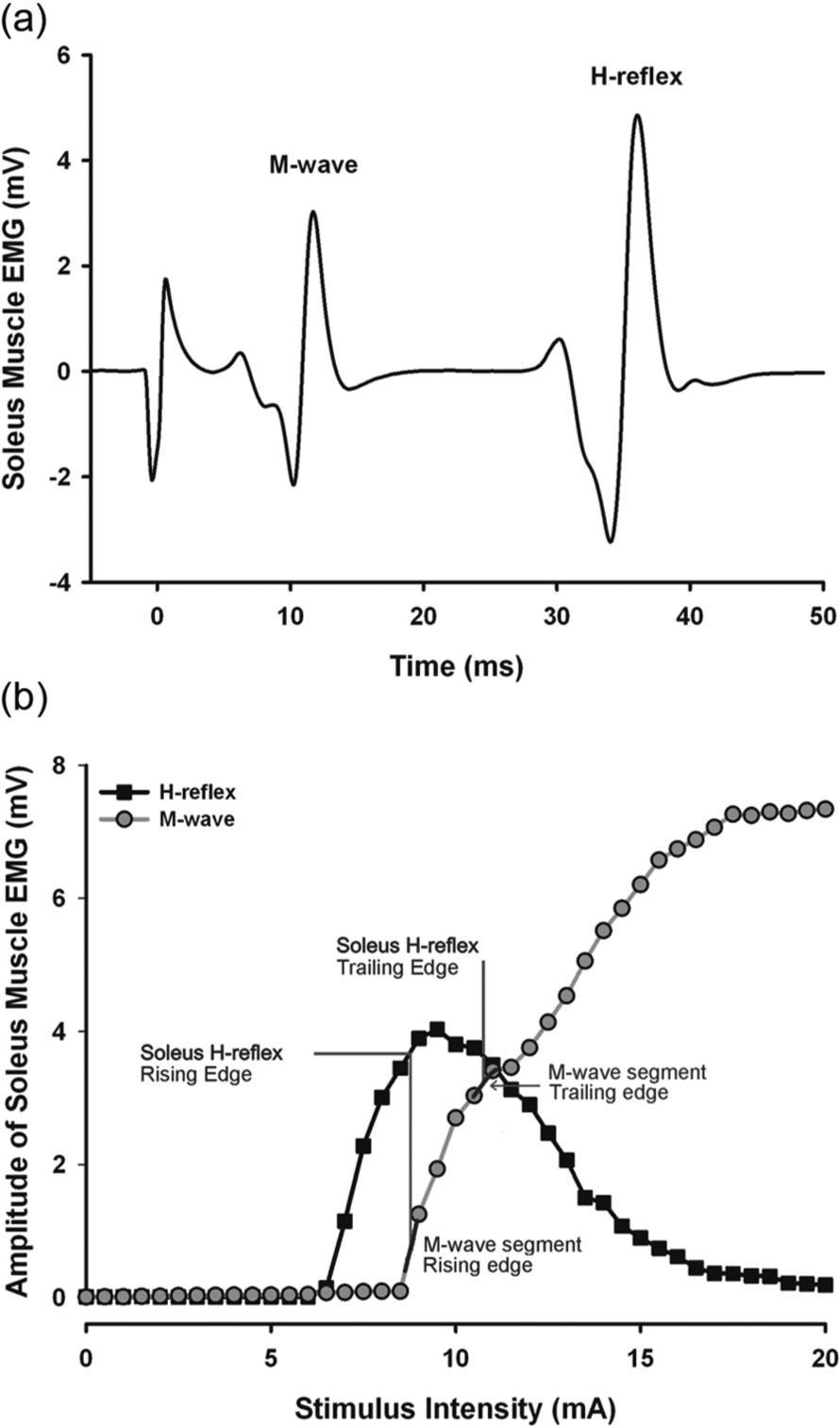
(a) An example of an original EMG recording of the soleus muscle upon stimulation of the tibial nerve in the popliteal fossa with a stimulation intensity of 9 mA. An early response can be identified as the M-wave, and a late response can be identified as the H-reflex. (b) A schematic illustration of M-wave segments corresponding to H-reflex amplitudes on the rising and trailing parts of the H-reflex recruitment curve, respectively. The fixed M-wave segments were determined on the basis of a fixed procedure, which differed between ExpProto and ExpOrthosis.
Stimulus intensities evoking the maximum H-reflex amplitude (Hmax) in RC were determined. Second, the lowest of these two stimulus intensities, −0.5 mA, was selected for the remaining experiment. This procedure was followed to remain on the rising edge of the H-reflex RC.
The selected fixed intensity was used to record soleus H-reflex 10 times under three experimental conditions: without any muscle preactivation (Control), with soleus preactivation (SOL), and with tibialis anterior preactivation (TA) (Figure 1). Control condition was always recorded first, while the subsequent order of SOL and TA preactivation was randomized. Interstimulus interval (ISI) was fixed to 6 s during these recordings. Depending on the condition, preactivation of SOL or TA was adjusted to 20% of voluntary maximum contraction monitored by EMG. The level of preactivation was kept stable through 60 s. Muscle contraction was performed isometrically, with the ankle flexion angle being kept stable as the contraction was performed against a plate parallel to plantar foot surface.
ExpProto
In ExpPreact, fixed stimulus intensity was used to examine the influence of muscle preactivation on the soleus H-reflex. However, this design showed abundant M-wave variation. Generally, fixation of stimulation intensity should provide for activation of the same amount of nerve fibers with each electrical stimulus, as the amount of fibers activated constitutes a significant independent variable in H-reflex recordings. While stimulation intensity may correlate to the amount of fibers activated within the nerve trunk, the M-wave is a closer and more precise correlate of the amount of fibers activated. Therefore, the study design was adapted and the M-wave was fixed instead of the stimulus intensity, based on the experiences made in ExpPreact. In order to provide for further stabilization of the M-wave, the impact of different stimulus intensities on rising or trailing edges of RC was investigated.
Two volunteers participated in one experimental session each in order to look for differences between two orthoses (A and B). The major difference between the two orthoses was the structure of the plantar support, as only Orthosis A had a tongue-like extension, which extended into the proximal metatarsal region of the plantar foot surface. Each experimental session had four conditions: before (PreA) and while wearing orthosis prototype A (OrtA), before (PreB), and while wearing orthosis prototype B (OrtB) (Figure 1). The experimental procedure was identical for all conditions.
Prior to onset of experimental conditions, volunteers had two RC recorded with increasing intensities ranging from 0 to maximum 25 mA, with incremental steps of 1 mA. Subsequently, the aim was to fix M-wave amplitudes during H-reflex recordings. Two sets of recordings were performed within each condition: 10 sweeps with fixed M-wave amplitude on the rising edge of H-reflex RC and 10 sweeps with fixed M-wave amplitude on the trailing edge of H-reflex RC. Prior to these recordings, acceptable fixed M-wave segments were determined using a fixed procedure (Figure 2).
The M-wave on the rising edge of the H-reflex RC was determined using the intensity evoking Hmax, during the prior RC recordings, −2 mA. The M-wave evoked by this intensity during prior RC recordings was noted. These two M-wave amplitudes were averaged.
The same procedure was followed to find a fixed M-wave segment on the trailing edge of H-reflex RC. Here, the intensity used to evoke Hmax plus 2 mA was used. Again, M-wave amplitudes evoked with this intensity during the prior RC recordings were averaged. During subsequent recordings within each experimental session, M-waves were accepted if it was within 7% of the M-waves determined from the above-mentioned procedure.
ExpOrthosis
In all, 20 healthy volunteers participated in a screening session and one experimental session each. Screening sessions had the purpose of familiarization of volunteers with the experimental environment and determine whether volunteers met inclusion criteria.
Each experimental session consisted of three conditions: before wearing (Pre), while wearing (Ort), and after having worn the orthosis (Post) (Figure 1). The procedure was identical for all conditions. During each of three conditions, volunteers had two initial RC recorded, with increasing intensities ranging from 0 to maximum 25 mA, with incremental steps of 1 mA. The ISI was randomized between 5 and 10 s. Thresholds for local stimulus detection and sensation of projection in the nerve’s receptive fields were noted. Subsequently, 10 recordings, with fixed M-wave amplitude on trailing edge of H-reflex RC, were performed. The procedure for M-wave determination was fixed: (1) 75% of average Hmax during preceding RC recordings was determined; (2) an intensity, clearly on the trailing edge of H-reflex RC, evoking this H-reflex amplitude ± 10% was determined; (3) this intensity was used for five stimulations; (4) amplitudes of M-waves evoked during these stimulations were averaged; and (5) this average M-wave amplitude ±5% was the acceptable M-wave reference segment for fixed M-wave recording in the remaining experiment.
Instrumentation
Signal acquisition was performed with Power1401 (Cambridge Electronic Designs Ltd, Cambridge, UK) and 5 mm Ag/AgCl unipolar surface electrodes. The signal was interfaced to a computer and recorded with the software Signal (Version 3.00; Cambridge Electronic Designs Ltd). For monitoring and determination, the preactivation level of muscles in ExpPreact, an oscilloscope (Analog Digital Scope HM1507; HAMEG Instruments GmbH, Germany), was used to determine the force of activation. Electrical stimulation was performed using a constant current high-voltage stimulator (Digitimer Model DS7A; Digitimer Ltd, Hertfordshire, UK). The orthoses used in ExpProto and ExpOrthosis were right-footed ankle–foot orthoses (Bauerfeind AG, Zaulenroda-Triebes, Germany) (Figure 3). To record appropriate muscle activity, during H-reflex recordings, settings of EMG were adjusted accordingly. High-pass and low-pass filters were set at 100 Hz and 1 kHz, respectively. The sampling rate was set to 10 kHz. The duration of each recording was 100 ms, with recording starting 20 ms prior to the stimulus.
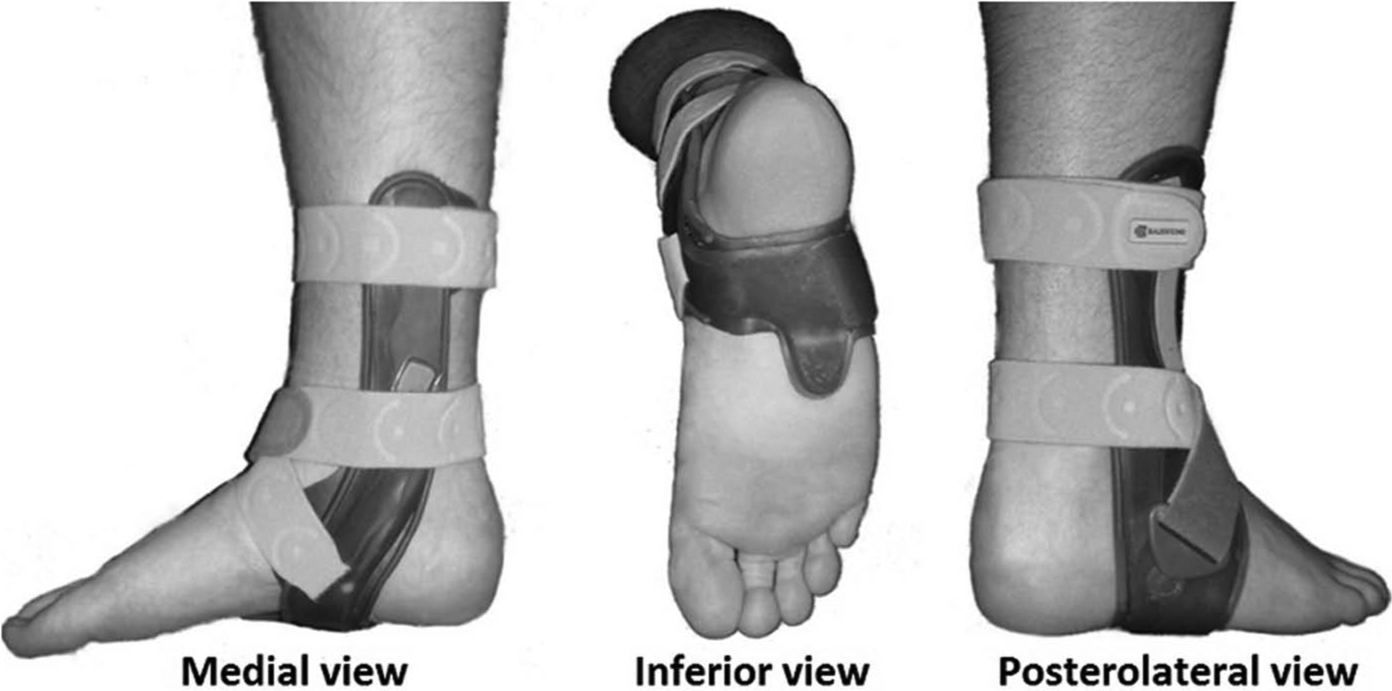
Orthosis A from ExpProto, and the orthosis used in ExpOrthosis from a medial, inferior, and posterolateral view, respectively.
Data analysis
Amplitudes of H-reflexes and M-waves refer to the peak-to-peak amplitude. H-reflex and M-wave amplitudes were expressed as absolute data. Statistical analysis was performed using SigmaPlot (version 11.0; Systat Software Inc., San Jose, CA, USA). Amplitudes were described as means of all volunteers ± SD or of all recordings ± SD. Mean H-reflex and M-wave amplitudes were analyzed in one-way repeated measures (RM) analyses of variance (ANOVAs), with experimental condition as the only factor. In the cases of nonparametric data distribution, Kruskal–Wallis one-way ANOVA (H-value) or Friedman RM ANOVA (χ2-value) was applied. Student–Newman–Keul’s post hoc test was used to address individual group differences. Significance was expressed at three levels: p < 0.05, p < 0.01, and p < 0.001.
Results
ExpPreact
Stimulus intensity was adjusted and kept fixed while H-reflex recording in each of the three conditions of ExpPreact: without muscle preactivation (Control), with preactivation of the soleus muscle (SOL), and with preactivation of the tibialis anterior (TA). Preactivation of tibialis anterior significantly suppressed soleus H-reflex compared to both SOL (p < 0.05) and Control (p < 0.05) (Figure 4). Mean M-wave amplitude of Control was 0.96 ± 1.18 mV, 2.19 ± 2.17 mV for SOL, and 1.79 ± 1.54 mV for TA. There were no significant differences between M-waves recorded in the three experimental conditions.
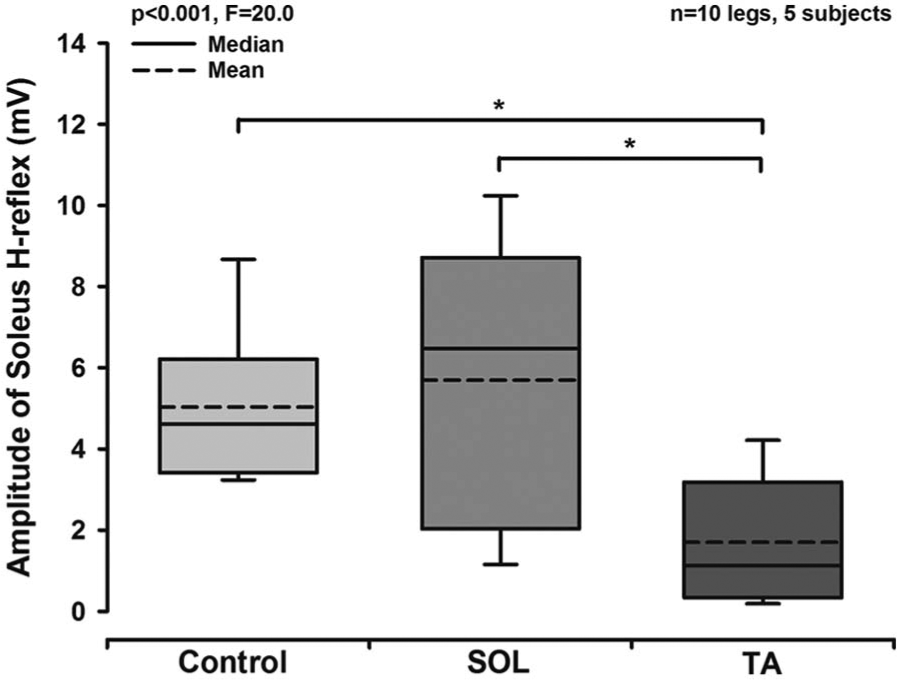
Box plot diagram based on mean H-reflexes recorded from all experiments in ExpPreact, while stimulus intensity was kept fixed, during each of the three experimental conditions: no muscle preactivation (Control), soleus preactivation (SOL), and tibialis anterior preactivation (TA). A one-way repeated measures ANOVA revealed significant differences between conditions (p < 0.001; F = 20.0). Subsequent post hoc testing revealed that during TA, a significantly decreased soleus H-reflex was observed compared to both Control and SOL.
ExpProto
Under controlled stimulus conditions (M-wave fixation), H-reflexes were recorded on both rising and trailing edges of RC. Two M-wave segments were determined: one segment with a corresponding H-reflex on the rising edge of RC and other with a corresponding H-reflex on the trailing edge (Figure 2). Data from ExpProto were analyzed separately for each subject (n = 2). H-reflex data from both subjects recorded on the rising edge of RC revealed no significant differences between any of the four conditions: before (PreA) and while wearing orthosis prototype A (OrtA), before (PreB), and while wearing orthosis prototype B (OrtB) (Figure 5(a)). H-reflex recordings on the trailing edge, however, revealed a significant suppression of H-reflex during OrtA compared to PreA (p < 0.05), PreB (p < 0.05), and OrtB (p < 0.05) in both subjects (Figure 5(b)). For subject 2, a significant suppression of H-reflex was observed during OrtB compared to PreA (p < 0.05) and PreB (p < 0.05). Upon M-wave fixation, no significant differences were observed in the M-wave data.
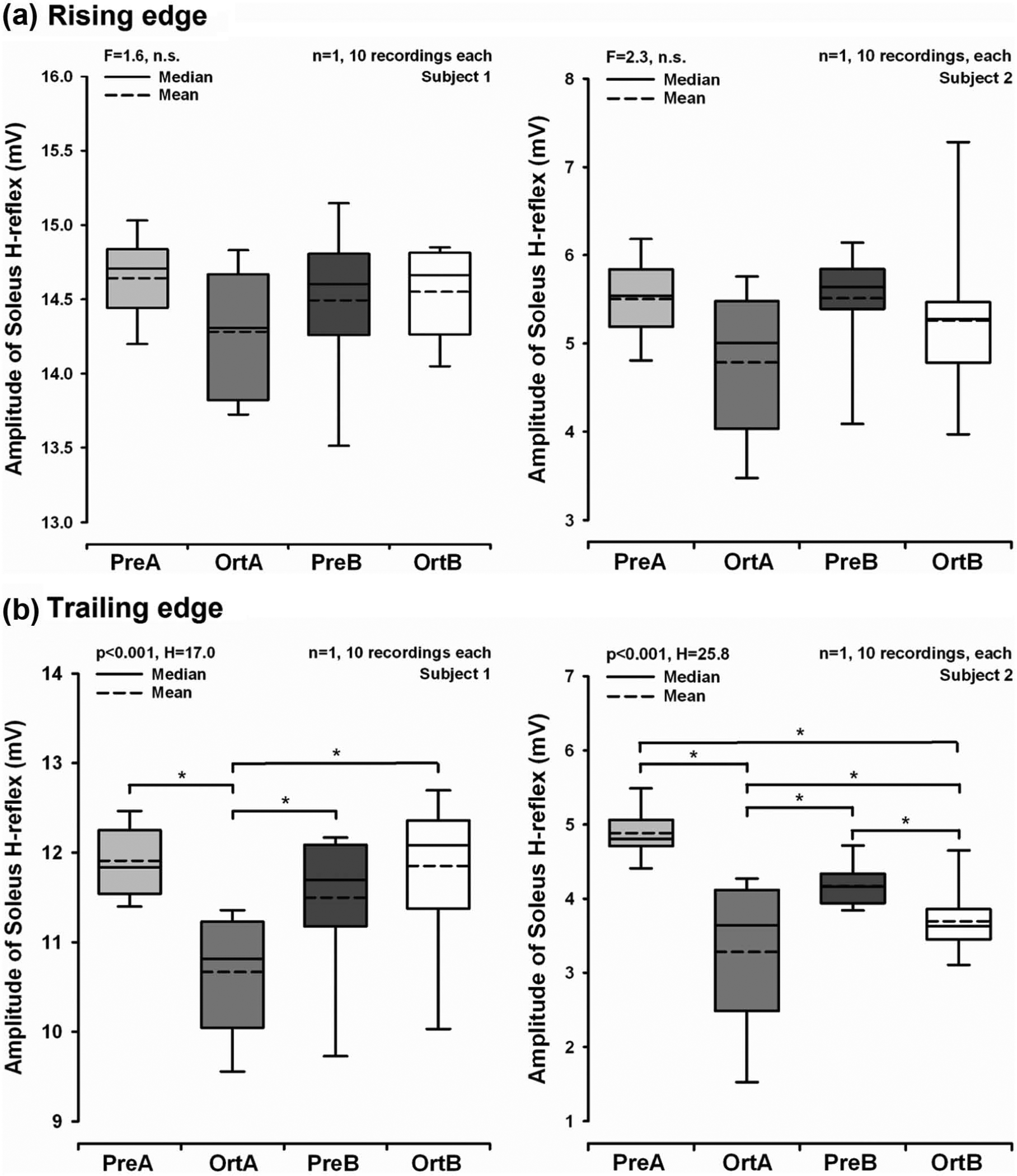
Box plot diagrams based on H-reflexes recorded in ExpProto in each of the four experimental conditions: before wearing orthosis prototype A (PreA), while wearing orthosis prototype A (OrtA), before wearing orthosis prototype B (PreB), and while wearing orthosis prototype B (OrtB). (a) Graphs are based on H-reflex data recorded, with fixed M-waves on the rising edge of the H-reflex recruitment curve, from subjects 1 and 2, respectively. (b) Graphs are based on data recorded on the trailing edge of the H-reflex recruitment curve. When H-reflex recording was performed on the trailing edge of the H-reflex recruitment curve, a significant more pronounced inhibition of the soleus H-reflex was observed for OrtA, compared to PreA, PreB, and OrtB for both subjects. For subject 2, the soleus H-reflex was significantly lower during OrtB compared to PreA and PreB. The p-values in the upper left corner of figures refer to the results of the one-way ANOVA performed on the data sets. F-values are given in case of a parametric one-way ANOVA, and H-values are given in case of a nonparametric Kruskal–Wallis one-way ANOVA.
H-reflex data from ExpProto revealed increased sensitivity when recordings were performed on trailing edge of RC. Additionally, an average of 32 stimulations was needed to obtain 10 recordings meeting the M-wave criteria when performed on the rising edge of the curve, while an average of 22 stimulations was needed on the trailing edge. This clearly suggested fixation of the M-wave with a corresponding H-reflex on the trailing edge of RC.
ExpOrthosis
RC recordings (Figure 6(b)) revealed stable stimulus condition as reflected by sensory thresholds (Table 1). However, significant differences were observed in H-reflex (p < 0.001) and M-wave thresholds (p < 0.001) between the three conditions. Maximum H-reflexes recorded during RC assessments were significantly lower in the Ort condition (4.67 ± 2.21 mV) compared to both Pre (5.58 ± 2.37 mV, p < 0.05) and Post (5.37 ± 2.37 mV, p < 0.05), as derived from post hoc testing.
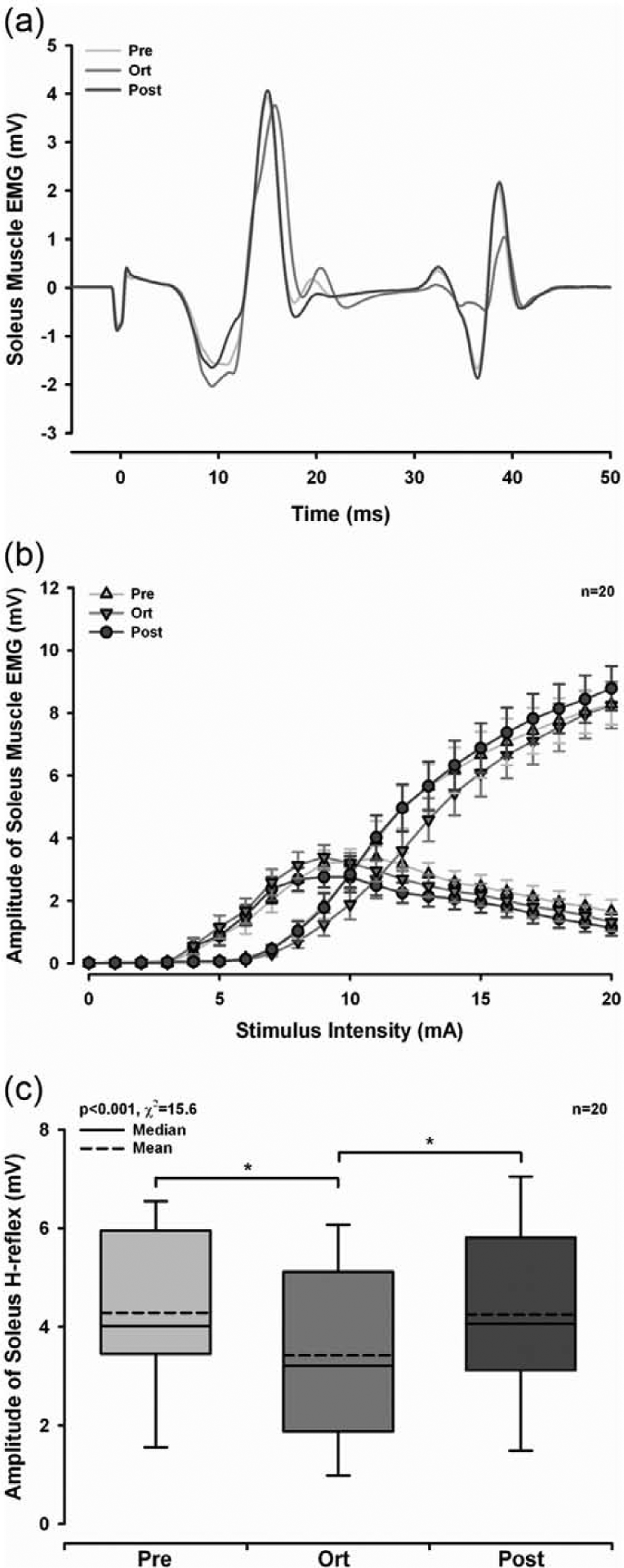
Graphical illustrations of the data from ExpOrthosis. (a) Schematic example of three raw EMG recordings, with fixation of the M-wave, from each of the three experimental conditions in ExpOrthosis: before wearing the orthosis (Pre), while wearing the orthosis (Ort), and after having worn the orthosis (Post). It is noticeable how changes in the H-reflex occur without any change in the M-wave. (b) Recruitment curves generated of data from 20 volunteers recorded in ExpOrthosis, in each of the three experimental conditions. It is visible how the H-reflex appears at intensities lower than the M-wave, and how it decreases at higher intensities, due to increased influence of antidromic collision. Data are presented as means ± standard error of mean. (c) Box plot diagram based on mean H-reflexes recorded with fixation of the M-wave in ExpOrthosis for all 20 volunteers, during each of the three experimental conditions. H-reflexes recorded in the Ort condition were significantly lower than both Pre and Post.
Mean stimulation intensities (mA) ± SD evoking different sensory thresholds, H-reflex threshold, M-wave threshold, and the maximum H-reflex (Hmax) during recruitment curve recordings across all three experimental conditions in ExpOrthosis: before wearing the orthosis (Pre), while wearing the orthosis (Ort), and after having worn the orthosis (Post).
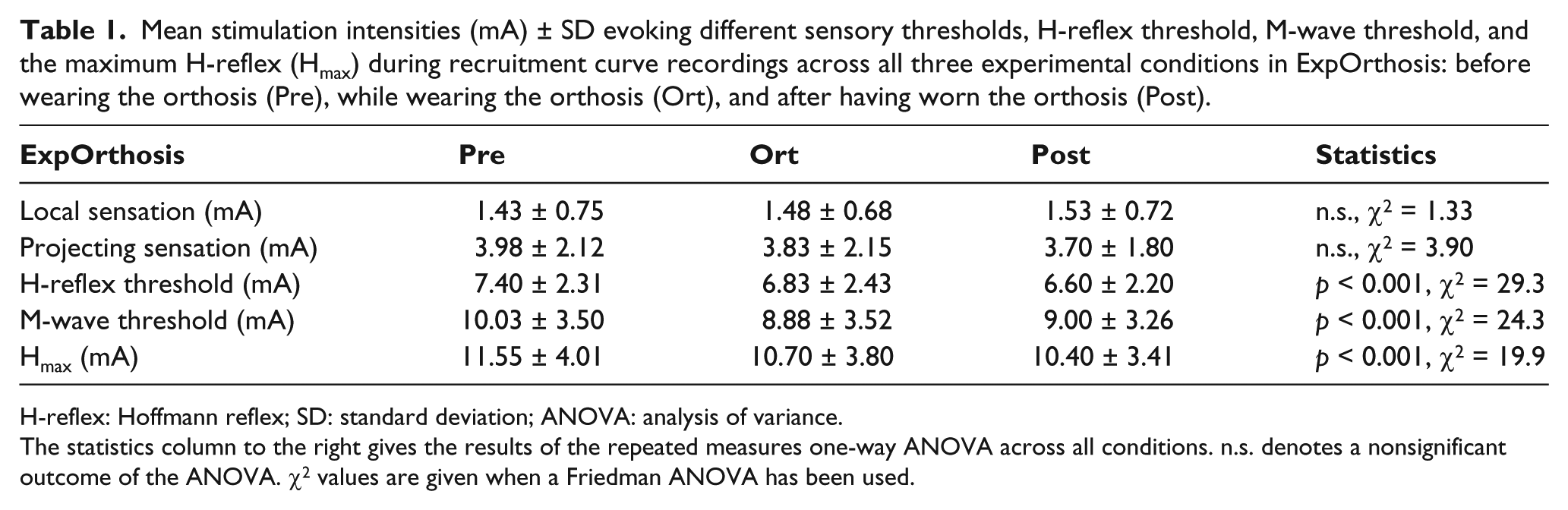
H-reflex: Hoffmann reflex; SD: standard deviation; ANOVA: analysis of variance.
The statistics column to the right gives the results of the repeated measures one-way ANOVA across all conditions. n.s. denotes a nonsignificant outcome of the ANOVA. χ2 values are given when a Friedman ANOVA has been used.
Data recorded with M-wave fixation revealed a suppression of H-reflex in Ort condition compared to both pre (p < 0.05) and post (p < 0.05) (Figure 6(a) and (c)). M-wave fixation resulted in a stable stimulus condition (mean M-wave amplitudes were 3.48 ± 1.34, 3.43 ± 1.25, and 3.47 ± 1.35 mV for Pre, Ort, and Post conditions, respectively), suggesting that reduced H-reflexes seen in Ort condition can be attributed to the application of the orthosis. To maintain a stable M-wave in each condition, stimulus intensity was adjusted slightly, but significantly (p < 0.001), over the three conditions.
Discussion
Three experiments were designed to address proprioceptive impact of an ankle–foot orthosis. Two initial preliminary experiments (ExpPreact and ExpProto) provided knowledge allowing more precise interpretation of the results obtained in ExpOrthosis. Application of an ankle–foot orthosis reduced the H-reflex in this study. Based on well-documented antagonistic relationship between soleus and tibialis anterior muscles, and further supported by results from ExpPreact, this may indicate a facilitation of the motor function of ankle dorsiflexors, principally the tibialis anterior muscle.10,21
Physiological impact of the orthosis
Data from ExpOrthosis revealed a clear suppression of soleus H-reflex during orthosis application. While two preliminary experiments were performed mainly to adjust the experimental design of ExpOrthosis, they also provided hints relevant to the interpretation of the results from ExpOrthosis. In ExpProto, the main intention was to select an orthosis type for ExpOrthosis. The results indicated that Orthosis A exerted a greater reflex inhibition than Orthosis B, whereby Orthosis A was selected for further investigation in ExpOrthosis. The major difference between the two orthosis prototypes was the structure of the plantar support, as only Orthosis A had a tongue-like extension, which extended into the proximal metatarsal region of the plantar foot surface, indicating that tactile stimulation of this area inhibits soleus muscle excitability. Previous studies have investigated this sensory-motor interaction using physical loading and electrical stimulation of both innocuous and noxious nature. Innocuous electrical stimulation of the metatarsal region of the foot resulted in a reduction in soleus excitability, while similar stimulation in the heel region had the opposite effect. 22 Innocuous tonic mechanical loading in both healthy volunteers and spinal cord injured patients evoked reduction in soleus H-reflex. 23 Despite limitations, the present results in healthy volunteers under static conditions demonstrated an inhibition of soleus motoneurons probably indicating ankle dorsiflexor facilitation during orthosis application. Cutaneous afferents play a crucial role in the initiation of dorsiflexion during gait. Thereby, the tongue-like extension of the orthosis in the plantar sole may act as an enhancer of the naturally occurring tactile stimulation during gait.
M-wave as an indicator of stimulus consistency
In ExpOrthosis, the proprioceptive influence of an ankle–foot orthosis was evaluated with H-reflex recordings performed while the M-wave was fixed within a segment on the trailing edge of the H-reflex RC. While H-reflex recordings previously have been performed with fixed stimulus intensity, in order to assess influence of conditioning stimuli, strict M-wave fixation by continuously adjusting the stimulus intensity is another well-supported option.12,14,22,24 In ExpPreact, fixed stimulus intensity was used to examine the influence of agonistic and antagonistic preactivation on soleus H-reflex. However, even with fixation of stimulus intensity, abundant M-wave variation was observed. As the M-wave reflects direct activation of α-motoneuron axons without any descending modulation, it can be assumed that a change in the M-wave either is due to a change in the stimulus or recording geometry, for example, site of stimulation electrode relative to the tibial nerve or site of the recording electrodes relative to soleus. During the experimental procedure, it was especially noticeable that precise and careful positioning of the stimulation electrode was required. It is apparent that even small changes, such as preactivation, minor movements, or application of orthosis, may influence stimulus condition. When stimulation intensity is fixed, it is done in the desire to activate the same amount of nerve fibers with each electrical stimulus, as the amount of fibers activated constitutes a significant independent variable in H-reflex recordings.11,14 While stimulation intensity may correlate to the amount of fibers activated within the nerve trunk, the M-wave is a closer and more precise correlate of the amount of fibers activated. Therefore, the study design was adapted and the M-wave was fixed instead of the stimulus intensity, based on the experiences made in ExpPreact. Thereby, changes in soleus H-reflex observed while wearing the orthosis cannot be attributed to a change in the amount of fibers activated, but may rather be attributed to the orthosis itself.
It was recommended to examine the H-reflex on the rising edge of RC due to increasing influence of antidromic collision on the trailing edge, which could mask influence of conditioning stimulation, such as application of an orthosis. 11 Therefore, the initial experiment, ExpPreact, examined the effects of agonistic and antagonistic preactivation on soleus H-reflex on the rising edge of RC. This resulted in pronounced M-wave variability. In some cases, it was not even possible to obtain a significant M-wave before Hmax was reached. In contrast, fixing the M-wave on the trailing edge of the RC yielded a significant M-wave with less variation, making the H-reflex recordings more reliable.
Clinical implications of orthosis induced facilitated dorsiflexor function
Orthoses are primarily applied in order to support joints passively. However, the orthosis under study proved to inhibit ankle plantarflexion under static conditions in healthy volunteers. This may indicate a facilitatory impact of the orthosis on ankle dorsiflexors. Thereby, its application could be feasible in the treatment of patients suffering from dorsiflexor weakness, such as in drop foot, where it may facilitate rehabilitation. Facilitation of motor function may additionally prevent or reverse muscle wasting, which is often observed in neuropathy-induced muscle weakness. It is emphasized that these experiments were performed in healthy volunteers under acute conditions. The predictive value of the outcome for patients under chronic conditions is questionable and should be carefully discussed. Finally, the experiments could justify future clinical trials in patients applying reflex recordings in order to objectify clinical outcome.
Conclusion
At first glance, it seems that foot orthoses primarily have a stabilizing effect on ankle joints in terms of simple mechanical bandages. However, the present results suggest an additional active impact on proprioceptive control. The putative neuromodulatory effect on motor control may support the application of such ankle–foot orthoses in, for example, drop foot. Furthermore, the objective assessment of a neurophysiological mode of action of orthoses by H-reflex recordings might be an appropriate primary outcome parameter in clinical trials.
Footnotes
Acknowledgements
Dr Rainer Scheuermann trained the investigators in order to provide for correct application of orthoses in volunteers.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by a research grant from the Bauerfeind AG (Zeulenroda, Germany).