
Abstract
Background:
The halo orthosis is a treatment option currently used in Australia for cervical spine immobilisation following trauma, fracture and post surgical stabilisation. In a previous study, the authors reported halo pin replacement to be a common complication. The aim of this study was to investigate the potential correlation between routine halo pin re-torquing and the incidence of pin replacement.
Case description and methods:
A retrospective case series study was undertaken. A total of 258 charts were reviewed, with 170 patients included in the study. Patients were fitted with a Bremer HALO System with the initial application torque maintained by routine re-torquing throughout the duration of wear.
Findings and outcomes:
A total of 680 pins (4 per patient) were inserted during the initial application of the halo orthoses, with only six pins replaced (0.88%) throughout the duration of the study.
Conclusion:
The findings from this study demonstrate a potential correlation between routinely re-torquing halo pins and decreasing the incidence of pin replacement.
Clinical relevance
This case series study has identified a potential improvement in clinical management of patients wearing a halo-thoracic orthosis.
Keywords
Background
The use of a halo-thoracic orthosis for the treatment of cervical spine immobilisation was first reported in 1959 by Perry and Nickel. 1 Since its introduction, it is used to manage traumatic cervical spine injuries. These injuries can include Jefferson fractures (C1), odontoid fractures (peg injury of C2), hangman’s fracture and single column cervical spine injuries (bone and ligamentous). A halo-thoracic orthosis may also be used following surgical intervention for cervical arthrodesis, immobilisation of an unstable cervical spine following tumour resection or the management of cervical fractures in patients with ankylosing spondylitis. 2
There are numerous complications associated with the wearing of a halo-thoracic orthosis, including pin loosening, pin site infection, pin discomfort, dural penetration, ring migration/failure of fixation of the ring to the skull, loss of reduction or progression of spinal deformity, pressure sores and prolonged bleeding at pins sites.3 –5 Despite the advancements made in materials and halo design, pin loosening and pin-site infection still present as complications associated with the wearing of a halo-thoracic orthosis.5 –9
Pin loosening rates have been recorded varying from 7% to 100%.10,11 Inconsistencies appear in the literature pertaining to the most effective and safe management of loose halo pins. Skull penetration and increased erosion through the outer table of the skull have been suggested as possible complications; however, to date, no studies have looked at the possible benefits of routine pin re-torquing, which may reduce the incidence of pin loosening.
The purpose of this retrospective case study was to examine the role of pin re-torquing while wearing a halo orthosis. It was hypothesized that routine pin re-torquing would result in a reduction in the incidence of pin loosening, the need for pin replacement and subsequent soft tissue scarring.
Case description and methods
A retrospective case series study was carried out. This involved reviewing all medical records of patients fitted with a halo-thoracic orthosis between 1999 and 2006 at the Princess Alexandra Hospital (PAH), Brisbane, Queensland, Australia. Ethics approval was obtained prior to reviewing medical charts.
In all, 170 patients (132 males and 38 females) were included in the study. The mean age of the sample was 39.8 years. All patients sustained a cervical spine injury (single or multiple level), with causes being trauma (97%), inflammatory (1.8%), congenital (0.6%) and sarcoma (0.6%).
Patients were excluded from the study if upon medical record review, it was noted that
Duration of wear was less than 42 days/6 weeks;
Osteoporotic bone or skull fractures were present at the time of halo application, thus effecting pin placement and initial application torque;
Incomplete patient record, or patients moved or were transferred to another facility.
All patients were fitted with a Bremer HALO System as per manufactures guidelines. Pre-calibrated torque limiting caps supplied by Bremer were used during the initial fitting of the halo-thoracic orthosis to obtain an initial application torque of 8 in lbs (0.90 N m). A pre-calibrated, non-sterilised, torque wrench (Torqueleader; M.H.H Engineering Co. Ltd, England) was used to subsequently re-torque the pins to 8 in lbs, 24 and 48 h post halo application. A review regime every 2–3 weeks was then carried out, with distance travelled and clinic availability taken into consideration.
At each review, all pins were checked for loss of torque using the pre-calibrated torque wrench. Any pin displaying a loss of torque was re-torqued to 8 in lbs. Patients were encouraged to attend additional reviews if they experienced headaches, pain, a clicking noise or sustained a knock or fall. Pins were replaced only if they failed to meet with resistance while being checked using the pre-calibrated torque wrench.
Findings and outcomes
The mean duration of wear was 69 days, with an average of five reviews during the treatment period. During the follow-up review appointments, only 5 of the 170 patients in the study (2.9%) presented with pins that demonstrated no resistance to re-torquing and therefore required replacement.
Table 1 shows the details of the pin(s) which were replaced, at what stage during the duration of wear of the halo-thoracic orthosis they were replaced and the potential cause of loosening which subsequently resulted in pin replacement. In all, 680 pins were initially inserted during the study (4 pins per patient). A total of 6 pins (0.88%) were replaced.
Pin replacement during halo-thoracic orthosis treatment in 170 patients.
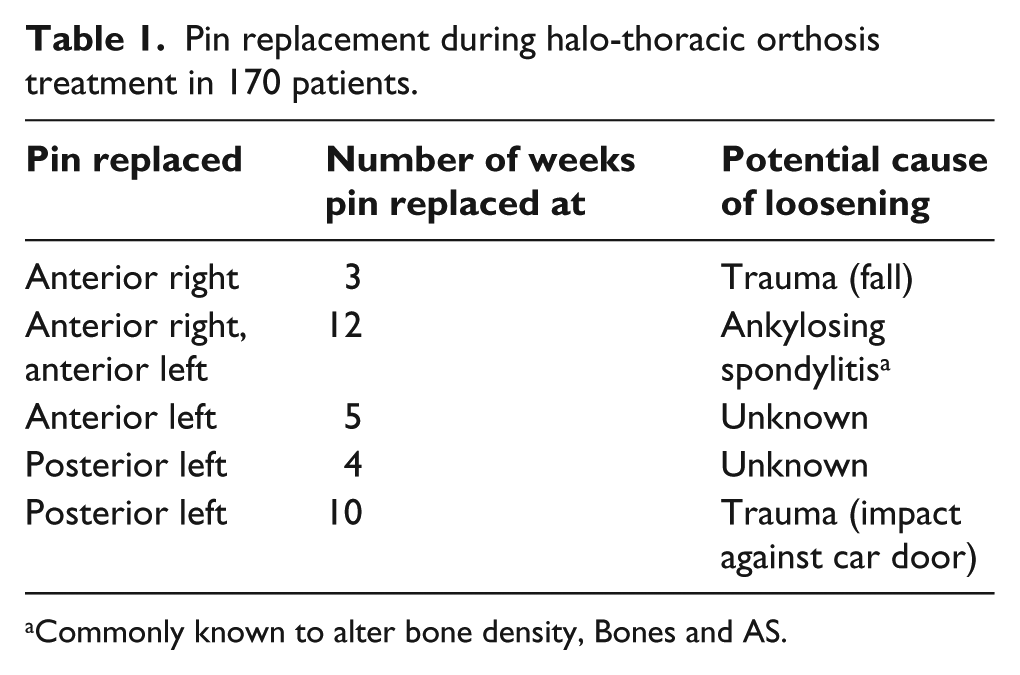
Commonly known to alter bone density, Bones and AS.
Discussion
Previous studies describe ‘loose pins’ as only needing to be ‘re-tensioned’ if resistance is met during the first couple of turns. If no resistance is met, the loose pin should be replaced. Pin loosening has been described as
Being able to freely twist the pin greater than one complete revolution;
The tip of the pin is visible at the edge of the skin rather than being secured against the skull;
The patient complains of feeling the pin move or hearing a clicking sound. 9
These descriptions are all subjective and open to interpretation, and therefore do not clearly provide a reliable and consistent way of recording ‘pin loosening’. This may be a contributing factor when considering that previous studies have indicated such large variations in pin loosening rates, ranging from 7% to 100%.8 –10
This study based the need to routinely re-torque halo pins following any reduction in torque from the initial application of 8 in lbs, in an endeavour to provide a more consistent and reliable term of reference. Torque is defined as force applied to rotate an object about an axis, whereas ‘tension’ is a pulling force exerted by a string, cable or chain. The term ‘tension’ is therefore not accurate when referring to the initial application of pins, nor is it a relevant unit of measure when reviewing pins. Pin tension is not a variable that can be measured with torque wrenches which are commonly supplied with halo-thoracic orthosis and used when reviewing loose halo pins. 13
There has been limited research looking at the effect of regularly re-torquing halo pins while wearing a halo-thoracic orthosis. This study highlights the potential role of regular re-torquing of halo pins and maintaining the initial application torque during the duration of wear of a halo-thoracic orthosis. By regularly reviewing halo pins using a torque wrench, torque was monitored and pins were re-torqued to 8 in lbs if a reduction had occurred. Consequently, the incidence of pins reaching the previously defined ‘loose’ stage appeared to be minimal.
In comparison, a study by Garfin et al., 9 a total of 716 pins were inserted, with 75 pins being replaced (10.47%). Pins were retightened at 24 and 48 h post application and only thereafter if the pin was found to be ‘loose’. In this study, the substantially lower pin replacement rate of 0.88% (6 pins replaced out of a total of 680 pins inserted), highlights the potential benefit of regularly reviewing and re-torquing halo pins in an endeavour to avoid pins becoming ‘loose’ and thus requiring replacement.
In the past, loose pins have been replaced rather than re-torqued due to the belief that skull penetration may occur as a result of excessive bone deformation at the pin/skull interface during the process of re-torquing. However, minimal clinical evidence exists pertaining to the physiology of the pin/skull interface. Garfin et al. 14 stated that proper halo fixation requires the pin tip to penetrate the outer 2 mm cortical bone table, without completely perforating the 3 mm cancellous middle layer and 2 mm inner cortical table which makes up the cranial bone wall. To achieve adequate depth and maintain fixation, large pin forces are required against the skull. Pin forces are generated by applying torque to the halo pin as it passes through the soft tissues and then penetrates the skull. The high forces and consequently high stresses at the pin site may contribute to pin loosening as a result of bone resorption, excessive microfracture in the region of concentrated stresses or possible bone necrosis. 9
Voor et al., 15 investigated the stress distribution in the cortical bone of the skull immediately adjacent to the pin tip upon insertion. Their study demonstrated that there is an area of localised deformation of bone of approximately 3.8 mm3 following the insertion of a halo pin, which created an actual hole volume of 0.3 mm3. A Von Mises stress contour plot of human skull bone model demonstrated a radial decrease in bone deformation from the insertion point. Voor et al. further discussed the influence axial creep (time-dependent deformation) at the pin-bone interface has on axial pin force. While creep will occur, it has been found that a higher insertion force of 0.09 N m (8 in lbs) as opposed to 0.68 N m (6 in lbs) may help reduce the incidence of pin loosening and infection. Although maintaining the initial insertion force of 0.09 N m (8 in lbs) will not avoid axial pin creep, it may result in enough residual fixation force after creep has occurred, to avoid some of the complications associated with ‘loosening’.
While the above two studies looking at pin-bone interface (all utilising cadaveric skull specimens) endeavour to match the characteristics of living bone, they are limited in what conclusions can be drawn as a living bone model with the forces, motions and biological process normally occurring on a halo pin are not present. 4 Further research into the reactions of bone at the interface of the halo pin in vivo may lead to a greater understanding of the causes of ‘loosening’. A radiographic study may assist in the further investigation as to the extent of penetration of the pin at the cranial bone wall following the fitting and consequent review process while wearing a halo-thoracic orthosis. The low percentage of pins required to be replaced in this study suggests that the risk of pin penetration may be minimised if the initial application torque is maintained and regularly reviewed.
Conclusion
The findings from this study demonstrate a potential correlation between routinely re-torquing halo pins and the incidence of pin replacement. This should be considered when determining the clinical management of patients wearing a halo-thoracic orthosis. To further investigate the findings of this study, a prospective study using a randomised population with a control sample (no re-torquing) should be carried out.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.