
Abstract
Background:
Typical upper limb prostheses may limit sports participation; therefore, specialized terminal devices are often needed. The purpose of this study was to evaluate the ability of transradial amputees to play golf using a specialized terminal device.
Case description and methods:
Club head speed, X-factor, and elbow motion of two individuals with transradial amputations using an Eagle Golf terminal device were compared to a non-amputee during a golf swing. Measurements were collected pre/post training with various stances and grips.
Findings and outcomes:
Both prosthesis users preferred a right-handed stance initially; however, after training, one preferred a left-handed stance. The amputees had slower club head speeds and a lower X-factor compared to the non-amputee golfer, but increased their individual elbow motion on the prosthetic side after training.
Conclusion:
Amputees enjoyed using the device, and it may provide kinematic benefits indicated by the increase in elbow flexion on the prosthetic side.
Clinical relevance
The transradial amputees were able to swing a golf club with sufficient repetition, form, and velocity to play golf recreationally. Increased elbow flexion on the prosthetic side suggests a potential benefit from using the Eagle Golf terminal device. Participating in recreational sports can increase amputees’ health and quality of life.
Background
Golf is a recreational sport enjoyed by millions worldwide. 1 Studies have shown that persons with limb deficiencies who engage in sports and recreation will experience physical and psychological benefits. 2 Terminal devices (TDs) have been developed and studied to assist upper limb prosthesis users when undertaking a number of recreational pursuits, including kayaking,3,4 bowling, skiing, hockey, baseball, and golf. 2
There is a positive relationship between maximizing club head speed, increasing the X-factor, and flexing the elbows correctly on the performance of a full golf swing.5–10 The X-factor (movement of the shoulders relative to the hips) has also been shown as a parameter for measuring golf swing skill.8,10 An increased separation between the pelvis and upper torso at the top of the backswing could lead to greater power generation and, therefore, increased ball velocity. 9 Elbow flexion is also of particular interest to the amputee population as many amputees experience limited range of motion (ROM) due to the fit and capabilities of their prostheses. This may negatively affect their ability to swing a golf club.
Given the importance of swing kinematics to golf performance, the purpose of this study was to examine club head speed, X-factor, and elbow flexion in two transradial amputees using a golf-specific TD (Eagle Golf TD; TRS, Inc., Boulder, CO, USA) before and after formal golf training. A secondary purpose was to compare the prosthesis users to a non-amputee to determine the limiting factors for an amputee during a golf swing.
Case description and methods
The protocol was approved by the University of South Florida’s Institutional Review Board, and all participants provided written informed consent prior to participation.
Study participants
Non-amputee control (C1): 25 years old, male, right-hand dominant
Transradial amputee (A1): 46 years old, male, right-arm amputation (10 years)
Transradial amputee (A2): 34 years old, male, left-arm amputation (8 years)
Both amputee participants were right-hand dominant before amputation and used myoelectric transradial prostheses at the time of participation. A1’s prosthesis utilized a typical self-suspended condylar fit, and A2’s prosthesis utilized a humeral cuff suspension and step-up hinges due to a short residual limb. The control participant reported playing recreational golf about four times a year (no handicap reported), and the amputee participants reported recreational golf experience five to six times a year prior to amputation, but no experience after amputation.
Data collection
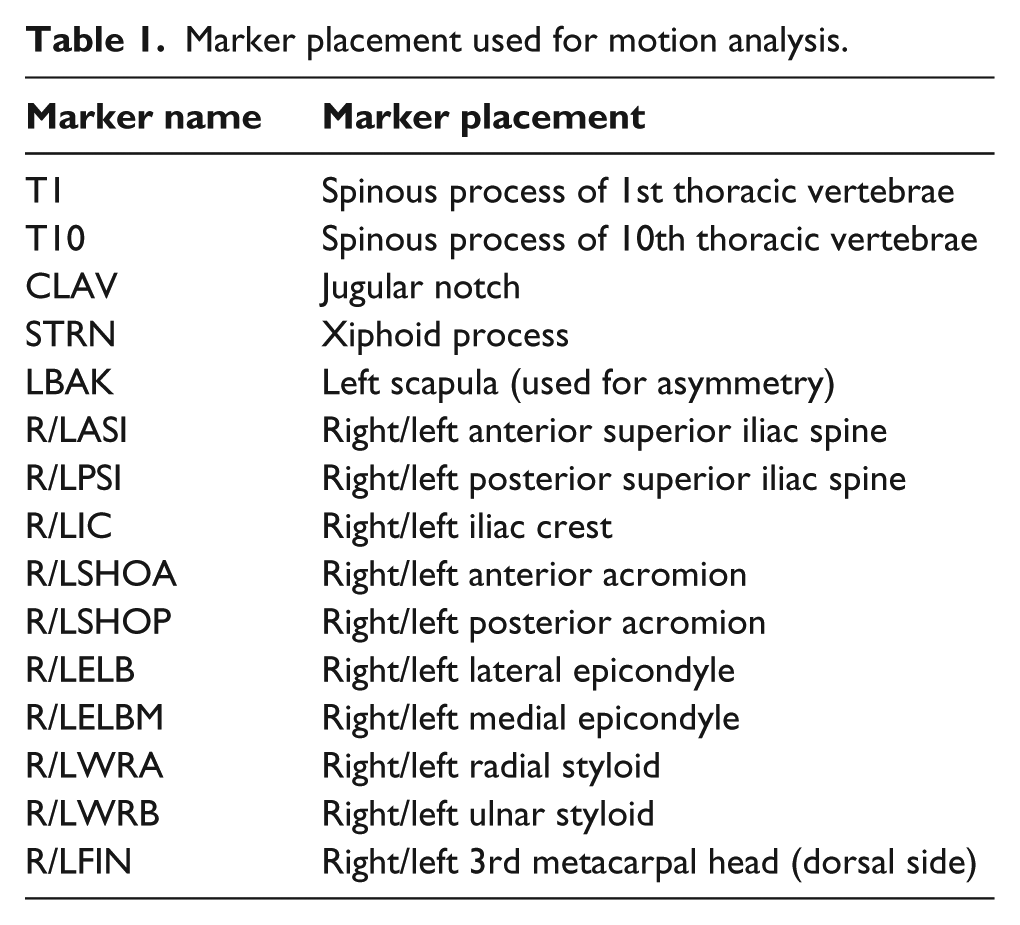
Motion analysis data were collected while participants performed full swings with a driver using an eight-camera Vicon (Oxford, UK) motion analysis system at 120 Hz. (Figure 1). A total of 25 markers were placed on the upper body of the participants (Table 1), and 3 markers were attached to the club. All participants used the same Big Bertha Steelhead 10°, left- and right-handed driver.

Participant A1 with reflective markers collecting data in motion analysis laboratory.
Marker placement used for motion analysis.
Participants performed swings using an Eagle Golf TD (TRS, Inc.) from right- and left-handed stances using standard and cross grips, collecting 10 trials for each combination (Figure 2). The golfers’ right-hand side positioned distal to the left-hand side on the club shaft was defined as the standard grip. Alternatively, the cross grip was defined as the golfers’ left-hand side positioned distal to the right-hand side on the club shaft. Data from the 10 trials were normalized to percentage of swing, averaged, and reported.

Participant A1 using the standard grip with the Eagle Golf TD.
Training with Eagle prosthesis
The two participants with amputations then spent 3 h each on a golf course with a Professional Golfers’ Association of America (PGA)-certified golf professional training coach. The training coach observed the participants while swinging with various stances and grips and provided verbal and manual feedback. The prosthesis was also adjusted during the training session at the course by an American Board for Certification in Orthotics, Prosthetics, & Pedorthics–certified and state-licensed prosthetist. Participants returned to the motion analysis laboratory the following week and completed the same testing protocol as previously described.
Motion data processing and analysis
The data analysis was completed using Visual 3D (C-Motion, Inc., Germantown, MD, USA). Raw marker coordinate and ground reaction force data were filtered using a five-point weighted running average filter. Club head speed at impact was used as the primary measure of golfer performance, as this has been previously shown to correlate with handicap. 11 A linear reconstruction of markers on the club was used in the case of marker dropout, and for this reconstruction, the club was considered to be rigid. Inspection of the marker positions during trials with no dropout verified the accuracy of the reconstruction. Club head speed was calculated by taking the magnitude of the derivatives of the x, y, and z position data of the club head marker with respect to time.
Local coordinate systems or segments were defined for the pelvis, torso, arms, forearms, and hands. 12 The X-factor was calculated by defining the angle between the shoulder vector and the pelvis vector in the transverse plane at the top of the backswing.9,10 The shoulder vector was defined as the unit vector from the average position of the left anterior (LSHOA) and posterior shoulder (LSHOP) markers to the average position of the right anterior (RSHOA) and posterior shoulder (RSHOP) markers. The pelvis vector was defined as the unit vector from the left anterior superior iliac spine (LASI) marker to the right anterior superior iliac spine (RASI). Elbow joint angles were calculated using Euler angle rotations (flexion, abduction, rotation order) of the forearm segment defined by wrist markers (R/LWRA) and elbow markers (R/LELB) relative to the upper arm segment defined by R/LELB, R/LSHOA, and R/LSHOP in Visual 3D. The club head speed, X-factor, and elbow joint angles from all trials were averaged, and the standard deviations (SDs) were calculated.
Findings and outcomes
Comparison of non-amputee golfer to Eagle Golf TD users
The average club head speed at impact and X-factor for each participant with each stance and grip combination before the training session are given in Table 2. Both amputee participants preferred the right stance and cross grip after completing the first data collection session. The control participant preferred the right stance with standard grip. Amputees demonstrated the ability to consistently drive the ball in the laboratory setting, driving the ball into the net 80% (A1) and 100% (A2) of the time while using the TD, while the non-amputee golfer achieved 80% (C1) during the preferred stance.
Mean (SD) club head speed, X-factor, and elbow ROM of each participant for each stance and grip combination before training.
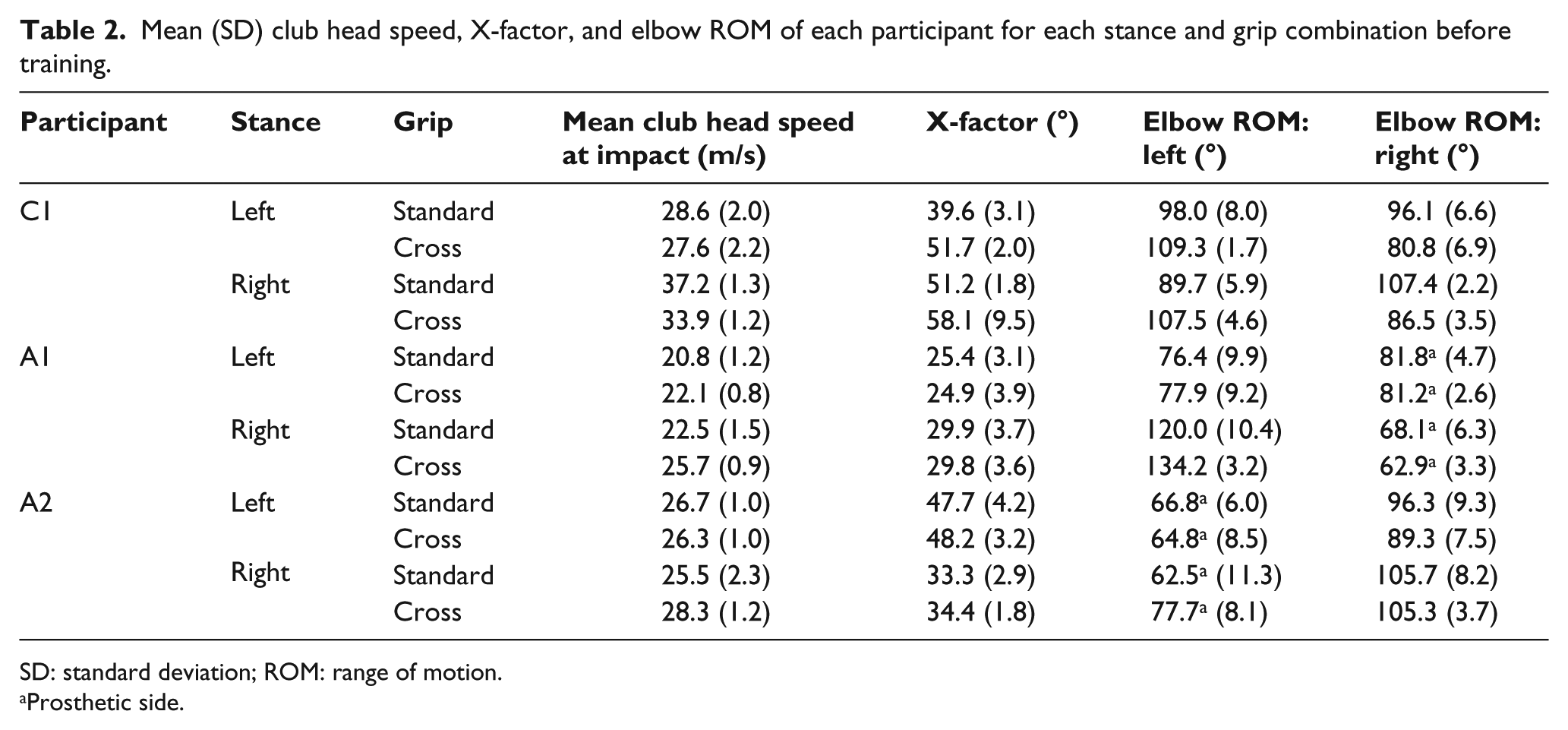
SD: standard deviation; ROM: range of motion.
Prosthetic side.
Comparison of Eagle Golf TD users before and after training session
The preferred stance and grip and the corresponding club head speed, X-factor, and elbow ROM for each user before and after the training session on the golf course are given in Table 3. The first participant (A1), right-hand dominant prior to amputation, and a right-arm amputee, switched his preferred stance to the left-handed stance after practicing with the coach. He preferred the right cross stance prior to the training session because even though he had a right side amputation, he still felt right handed with regard to his golf swing. The second participant (A2), a right-hand dominant male with a left side amputation, preferred the right cross stance both before and after training.
Mean (SD) club head speed, X-factor, and elbow ROM for all participants before and after training with preferred stance and grip.
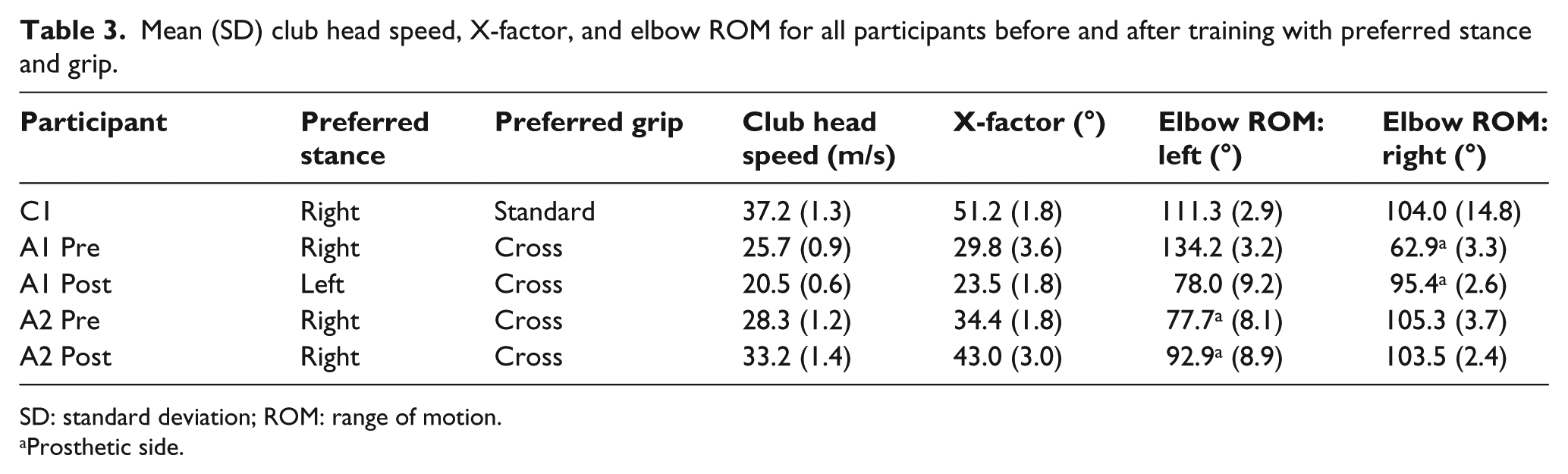
SD: standard deviation; ROM: range of motion.
Prosthetic side.
Discussion
The purpose of this study was to compare club head speed, X-factor, and elbow flexion of two transradial amputees using the Eagle Golf TD (pre/post training) compared with a non-amputee to demonstrate the potential ability to effectively participate in recreational golf. We expected that prior to training, amputee participants would have difficulty using the device effectively and that post training, club head speed, X-factor, and elbow ROM would be close to non-amputee performance. This was not uniformly the case, as the amputee participants were able to use the device effectively without training and training produced varied results. The highest mean (±SD) club head speed at impact for the tested stances of A1 was 25.7 m/s (±0.9 m/s) (pre training) and for A2 was 33.2 m/s (±1.4 m/s) (post training), which were both less than the C1’s club head speed of 37.2 m/s (±1.3 m/s) for right standard (preferred grip). Participant A2 was within the lower range of previously recorded amateur mean club head speeds of 33−58 m/s. 11 This shows that by using Eagle Golf TD, A2 was capable of achieving club head speeds similar to amateur golfers. This club head speed range is further substantiated by Horan et al., 13 who reported a club head speed of 49.1 m/s (±3.6 m/s) in a group of 19 male, competitive, amateur golfers (handicap ≤ 4). While using the Eagle Golf TD, amputees were able to demonstrate club head speeds comparable to high-handicap (>20) amateur golfers, which we consider to be appropriate to engage in recreational golf. Importantly, no consequential prosthetic or dermatological issues arose throughout testing and training, and participants reported the ability to concentrate on their golf swing. Participants were first exposed to the TD at the first data collection, so even without training or instruction, they were able to quickly adjust to the device and repeatedly hit the ball.
The X-factor of C1 was 51.2° (±1.8°) during preferred stance and grip (right, standard) and was comparable to previous studies,10,14 demonstrating that the methods used for this study show similar results to research groups that focus on golf biomechanics. A1 and A2 both exhibited smaller X-factors of 29.8° (±3.6°) and 34.4° (±1.8°), respectively, with their preferred grip. A1 switched his preferred stance after training and had a decreased X-factor of 23.5° (±1.8°), which may have also contributed to his lowered club head speed. A2 increased his X-factor to 43.0° (±3.0°) after training, which may have been a factor in his increased club head speed. X-factor has previously been correlated with club head speed and driving distance, and previous studies have found X-factors of 48°−57° 14 and 70° (±20°) 10 in low-handicap amateur golfers.
Post training, the preferred stance and grip combination for the amputee participants had the prosthetic side as the leading arm (front arm in the stance; arm facing the hole). During a golf swing, the trailing (rear) arm requires more ROM of the elbow and wrist,5,6 which was shown by C1 during right stances (Table 2). The greatest ROM of the elbow of the prosthetic side of A1 and A2 before training (Table 2) occurred when the prosthesis was the leading arm and placed distally (standard grip: right hand placed distally) on the club. The prosthesis may limit the motion of the elbow, which may be why the amputees preferred having the prosthetic side as the leading arm. 15 Improvements in elbow ROM were observed post training for the prosthetic side in all stances, although only the preferred stance data are presented here (Table 3). The increase in elbow ROM of the amputated side post training may suggest that engaging in activities such as golf may improve ROM of the elbow on the prosthetic side, which could have a potential therapeutic value, although the training time of this study was limited. Both participants showed less elbow flexion occurring on the amputated side pre training, with participant A1 showing the greatest degree of asymmetry of elbow ROM between amputated and non-amputated side (Table 3). This restricted motion at the elbow may be indicative of compensation and thus a possible cause of lower club head speed and performance. Using the prosthetic side as his trail arm instead of leading arm may also be a cause.
Participant A1 changed his preferred stance to left after consultation with the golf coach and the prosthetist. Prior to amputation, this participant was right handed and felt more comfortable at first with the right-handed stance even though his prosthesis was on the right side. After training, he preferred the left stance even though in the laboratory, he had a slower club head speed (20.5 m/s) and lower X-factor (23.5°) with this stance compared to the right stance (25.7 m/s and 29.8°). He reported having more control using left-handed stance and ultimately preferred this stance. This suggests that the stance preference should be determined early in the golf training process. Follow-up studies would be required to determine whether further practice and training would demonstrate continued improvement. In this study, it was also noted that placing the club in, and removing it from, the Eagle TD was difficult. The grip material on the golf club was also damaged at times during application or removal of the TD. This should be discussed with amputees interested in golfing, and practice is recommended to avoid foreseeable frustration with this activity.
Further studies with long-term follow-up and more training are needed to determine whether recreational amputee golfers’ performances can be positively influenced over time. As suggested by our participants, experimental designs would be useful in determining how beneficial professional training could be compared with recreational golf exposure in defining the highest potential golf skill of a person with a transradial amputation. As this was a case study, there are limitations to drawing any general conclusions from these data presented. Furthermore, there were no qualifications in terms of accuracy, and therefore, performance was likely to be skewed due to a harder swing correlating to a higher club head speed. Other limitations included the small sample size and focus on the transradial level of amputation.
Conclusion
This study demonstrated transradial amputees’ ability to participate in recreational golf, which may have rehabilitative benefits. While the transradial amputee golfers swung the golf club at a slower speed than the recreational non-amputee golfer, it is the opinion of the authors that this difference would not be enough to prevent participation in recreational golf. Amputees showed a decreased X-factor when compared to a non-amputee golfer, which could potentially be a factor for the lower club head speeds seen and could possibly be overcome with practice. Both amputees increased elbow ROM on the prosthetic side, suggesting a potential benefit in golf participation.
Footnotes
Acknowledgements
The authors acknowledge Bob Radocy, of TRS, Inc., for consultation and for providing Eagle Golf terminal devices (TDs) for comparison and evaluation.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was funded partially by the Florida Department of Education, Division of Vocational Rehabilitation (contract no. 09-128).