
Abstract
Background:
Mandibular reconstruction has been experiencing an amazing evolution. Several different approaches are used to reconstruct this bone and therefore have a fundamental role in the recovery of oral functions.
Objectives:
This review aims to highlight the persistent problems associated with the approaches identified, whether bone grafts or prosthetic devices are used. A brief summary of the historical evolution of the surgical procedures is presented, as well as an insight into possible future pathways.
Study design:
A literature review was conducted from September to December 2012 using the PubMed database. The keyword used was “mandible reconstruction.” Articles published in the last three years were included as well as the relevant references from those articles and the “historical articles” were referred. This research resulted in a monograph that this article aims to summarize.
Results:
Titanium plates, bone grafts, pediculate flaps, free osteomyocutaneous flaps, rapid prototyping, and tissue engineering strategies are some of the identified possibilities. The classical approaches present considerable associated morbidity donor-site-related problems.
Conclusion:
Research that results in the development of new prosthetics devices is needed. A new prosthetic approach could minimize the identified problems and offer the patients more predictable, affordable, and comfortable solutions.
Clinical relevance
This review, while affirming the evolution and the good results found with the actual approaches, emphasizes the negative aspects that still subsist. Thus, it shows that mandible reconstruction is not a closed issue. On the contrary, it remains as a research field where new findings could have a direct positive impact on patients’ life quality. The identification of the persistent problems reveals the characteristics to be considered in a new prosthetic device. This could overcome the current difficulties and result in more comfortable solutions. Medical teams have the responsibility to keep patients informed about the predictable problems related with each elected approach, even understanding that a perfect reconstruction is a secondary goal when compared with maintenance of life.
Keywords
Background
Mandible reconstruction is considered a challenge for the majority of the maxillofacial surgeons. 1 In the basis of this consideration, there are two major factors: On one hand, the anatomical diversity of the region 2 and the complex mandibular movements, 3 responsible for the basic oral functions such as mastication, deglutition, and phonation and for facial mimics, with critical importance on life maintenance and social inclusion; on the other hand, the high prevalence and the reserved prognostic of oral cancer.4–7
This surgical approach is often needed to rebuild the affected bone integrity, not only after trauma, infection, or huge jaw cysts but also after ablative surgery for oral cancer 8 or, in less aggressive situations, after a prolonged use of removable dental prosthesis due to the associated bone reabsorption. 9
Prosthetic devices used for bone tissue replacement or for fixing bone grafts harvested in distant donor sites are still inefficient. They may be exposed, causing infection to the area, and in other cases, bone resorption at the retaining screws can occur, resulting in the loss of stability of the device.
It is important to stress that beyond the mandibular reconstruction, other factors play an important role in the restoration of the previously described oral functions: the dimension and location of the tumor, and the extent of involvement of the tongue, soft tissues, and remaining teeth. However, the approach to these factors does not fall within the scope of this review.
History
The history of mandibular reconstruction cannot be separated from the historical evolution of the precedent bone grafts. The first bone graft was, probably, a xenograft with canine origin, performed by a Russian surgeon, whose name is unknown, related by van Meekeren in 1668, correcting a cranial defect of a soldier, 10 and the first autograft known would have been performed by Von Walther, at Bonn University, in 1821. 10 The discovery of anesthetics and antibiotics, and the development of sterilization and aseptic procedures, together with the growing number of experimental studies, contributed to improved surgical techniques and success rates.
In 1892, Bardenheuer used a pedicle graft of the mandible itself to restore its continuity (Figure 1). 10 However, even though this procedure could recover the mandible continuity, the bone tissue lost was not rebuilt. The next attempts were made with recourse to free, nonvascularized, bone grafts, 11 harvested in distant locations and held in place, at the receptor site, by metallic reconstruction plates, usually titanium. Several bones, such as tibia, iliac crest, or ribs, were often used as donor sites. In 1950, Converse 12 described the utilization of 12 bone grafts and 14 bone and cartilage grafts to restore maxillary and mandible defects. However, the necessary radiotherapy often led to soft tissue fragility with exposure of the immobilization devices and consequent contamination, which led to infection and graft resorption. 1 Another limitation of this approach is the absence of vascularization, which limits the amount of bone that is possible to transfer and, therefore, the size of the defect that is intended to be restored. 13
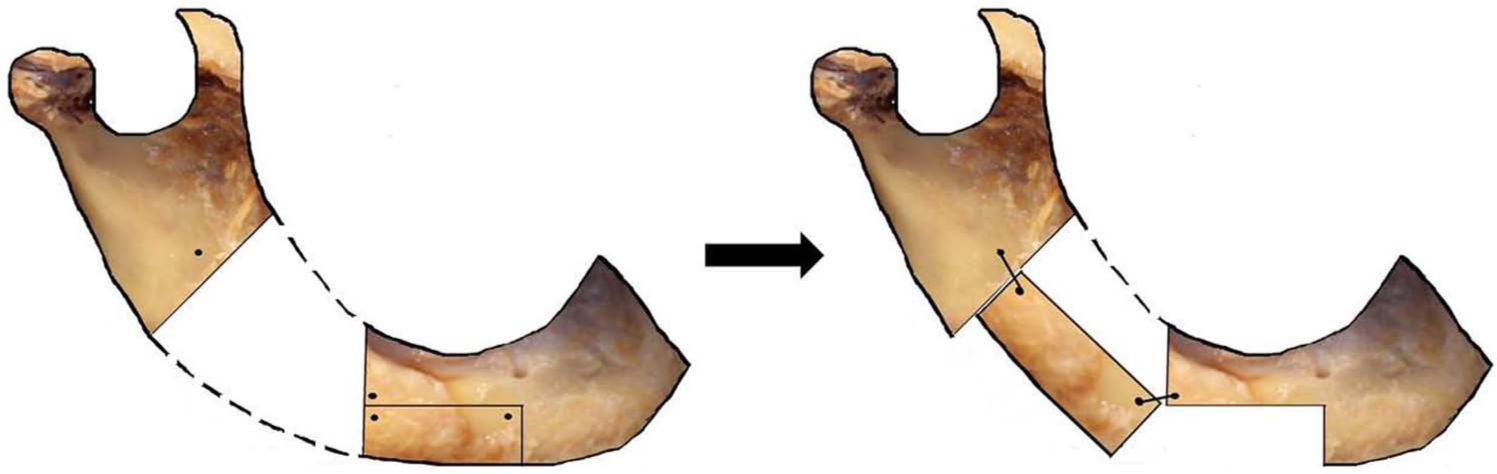
Schematic image of the pedicle bone graft performed by Bardenheuer.
With the emergence of vascular surgery arrived the possibility of supplying vascularization to the bone grafts and therefore restoring larger defects. The first techniques then developed consisted in the transference of different tissues (bone, muscle, skin, blood vessels) that kept the connection with the donor site. Pedicle osteomyocutaneous flaps, the most commonly used, 1 were rib with pectoralis major, 14 clavicle with sternocleidomastoid, 15 and scapula with trapezius. 16 Despite the better outcomes achieved by these approaches, they were limited by the mobility of the tissues, 1 and some aesthetic results were disastrous (Figures 2 and 3).
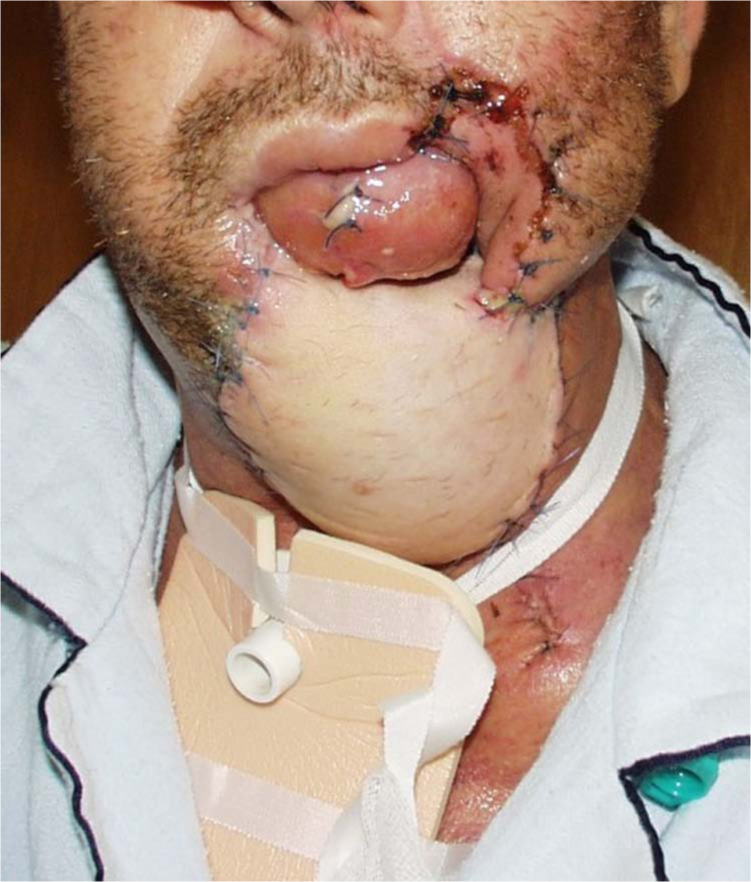
Image of massive tissue transference from the pectoralis major showing a poor aesthetic result.

Clinical image after soft tissue transference with a pediculate flap from the pectoralis major.
The next step in this path arrived with the possibility of using vascularized free flaps, harvested at sites distant from the mandible. Using this approach, not only is bone tissue transferred but muscle, skin, and blood vessels are also included. In 1979, Taylor et al. 17 and Sanders and Mayou 18 described the deep circumflex iliac artery and vein free flap. In 1986, Swartz et al. 19 introduced the scapular osteocutaneous free flap, and 3 years later, Hidalgo 20 reported the possibility of using a fibular osteocutaneous free flap for mandible reconstruction.
State of the art
More recently, different methods are used, including nonvascularized bone grafts, pedicle flaps, and simply titanium reconstruction plates. 21 Nevertheless, the gold standard for the reconstruction of the mandible is the free osteocutaneous flap, fixed in an early phase by a titanium plate, which could be removed at a later stage. 1 The previously described flaps, such as iliac crest, scapula, fibula, and the radial flap, presented by Soutar et al. 22 in 1983, can be used. However, the most common approach is the fibula osteocutaneous free flap.23,24
The choice between the existing possibilities depends on several factors, such as the extension and the area of the mandibular defect; the need of occlusal rehabilitation with dental implants; patient factors, such as age, general medical condition, or tolerance to treatment; and the skills of the medical staff.1,25,26
In recent years, the application of these methods has benefited from digital planning of surgery. With computerized tomography, it is possible to create a virtual three-dimensional (3D) model of the affected mandible. This tool could also help to anticipate surgical difficulties and thereby support preoperatory decisions (Figure 4). The virtual model can be materialized becoming a valuable assistance to surgical planning, surgical guides manufacturing to the donor and receptor beds, titanium reconstruction plates (Figure 5)27-29 and metallic or resorbable trays for bone regeneration30,31
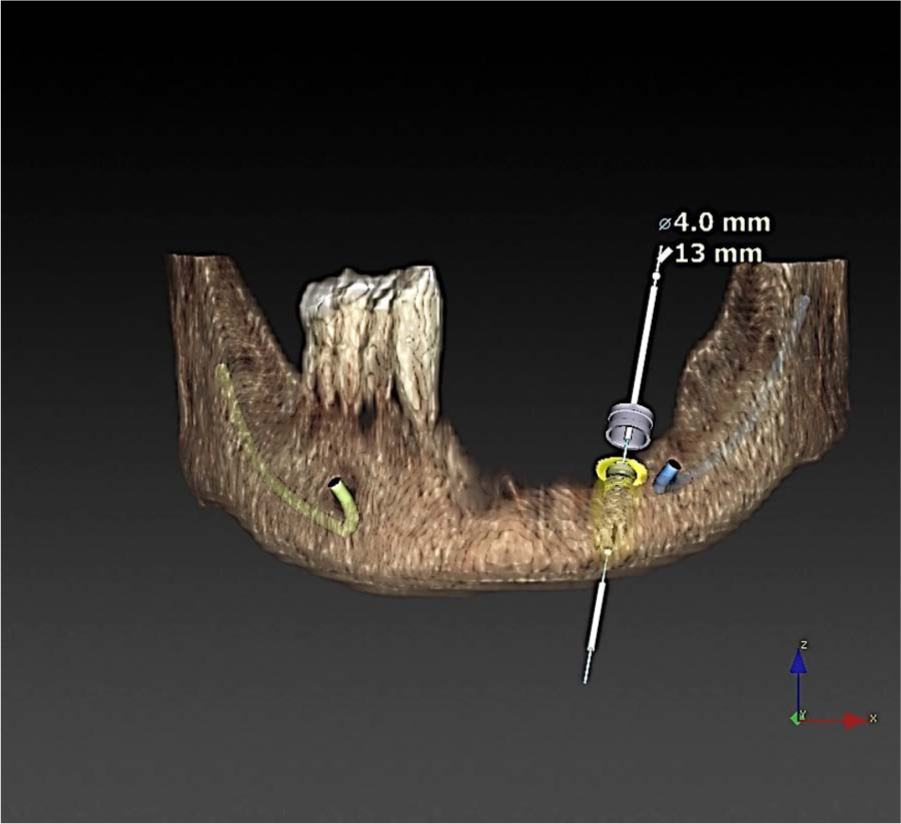
Illustration showing a digital planning of a dental implant placement near the emergence of the mental nerve. Due to a marginal mandibulectomy, the mental foramen is located on the alveolar crest.
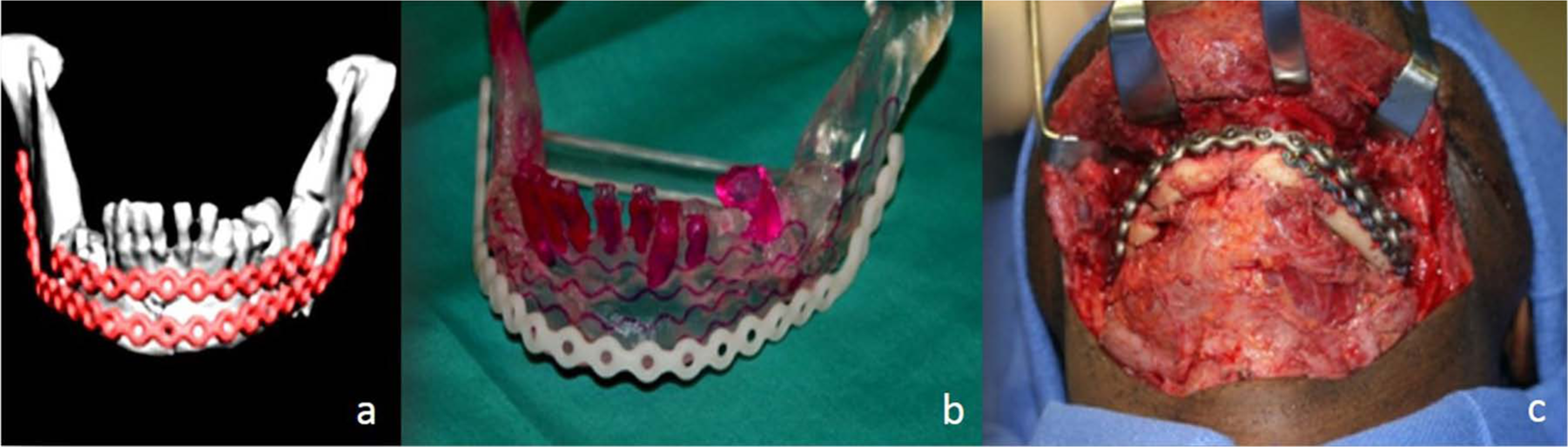
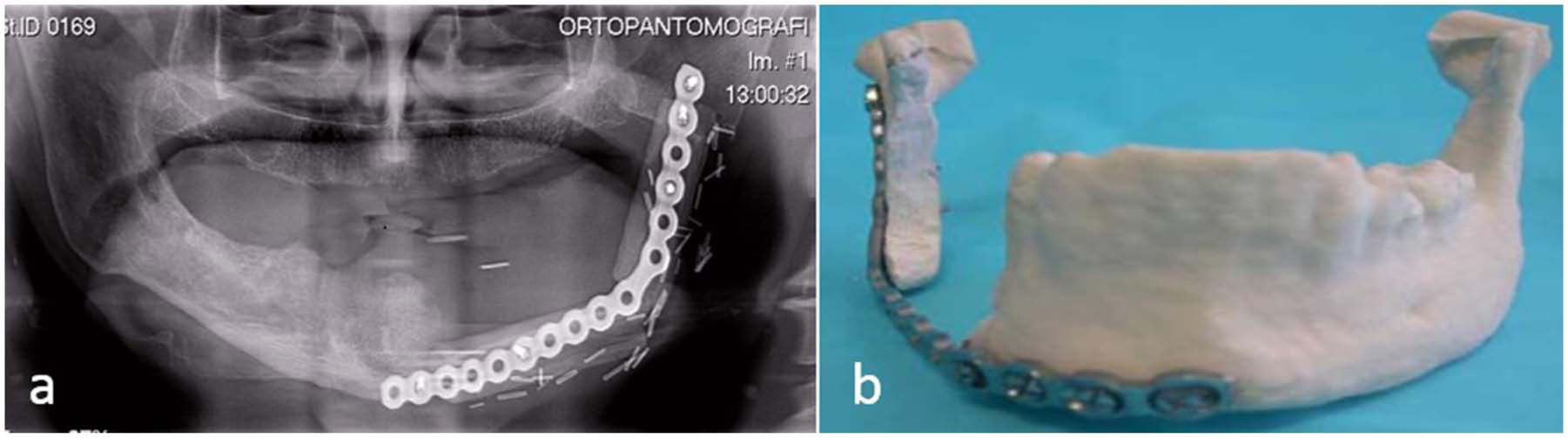
Sequence of images documenting (a) digital planning of titanium plates, (b) materialized model, and (c) surgical application in a mandibular reconstruction.
The surgery preplanning and the prebended titanium plates result in intra-surgical time saving, improved fitting of titanium plates, and increased adaptation of the grafts, with optimization of bone-to-bone contact.32,33
Persistent problems
In the particular case of the mandible reconstruction after ablative surgery related to oral cancer, it is noteworthy that the benefits of current techniques far outweigh the negative aspects since they are able to stop the malignancy evolution and to keep patients alive and autonomously control their oral functions. Nevertheless, and despite the amazing evolution in this field, there are still a few persistent problems.
Prosthetic devices
Titanium plates are used both as fixation devices, to keep the bone grafts in place (Figure 6(a)), and as prosthetic devices, to guarantee the mandible continuity, replacing the removed bone segment (Figure 6(b)). However, mandibular movements (Figure 7) can cause torsions and bending effects on the fixation plates. Also, the mastication forces act as a shearing stress at the fixation devices level. As a result, screw loosening, plate fracture, bone loss, and failure of the reconstruction may occur. 34 Due to these facts, the use of the existent fixation devices, as a permanent solution, is not advised. 3 Likewise, as it is possible to observe on Figure 7, titanium plates replace in an unsatisfactory way the lost bone volume and are not compatible with teeth replacement or with an oral rehabilitation with dental implants.
(a) A bone graft is kept in position by a titanium plate used as a prosthetic fixation device. (b) A titanium plate used as a prosthetic device to replace the removed bone segment. This devices poorly replace the lost bone.
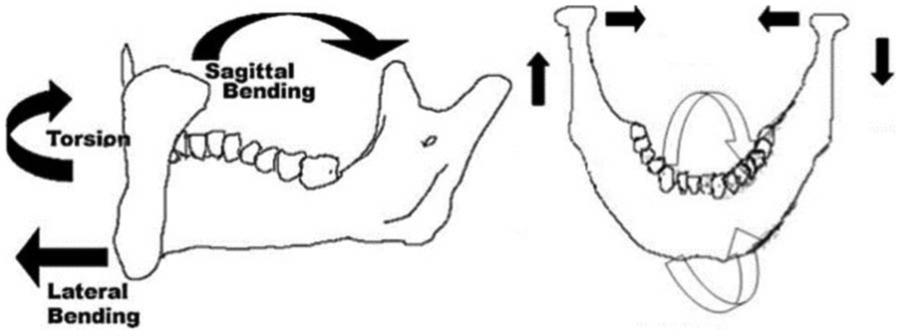
Scheme of the mandibular deformations during the normal function.
Dental implant rehabilitation
Oral rehabilitation with dental osseointegrated implants faces some difficulties in this context. On the one hand, the existing asymmetry on the bone level results in an implant/crown unfavorable relation (Figures 8 and 9), and the success rates of dental implants placed in grafted bone are considered to be lower than in nongrafted bone. 35 On the other hand, the radiotherapy also reduces the dental implant success rates. 36
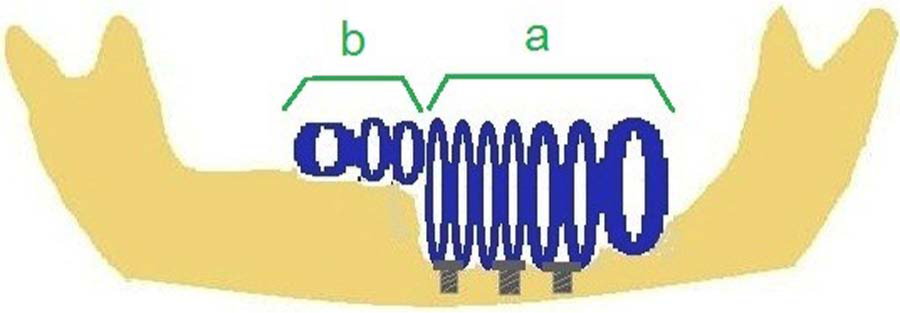
Schematic illustration showing the different crown/implant ratios: (a) unfavorable ratio and (b) favorable ratio.
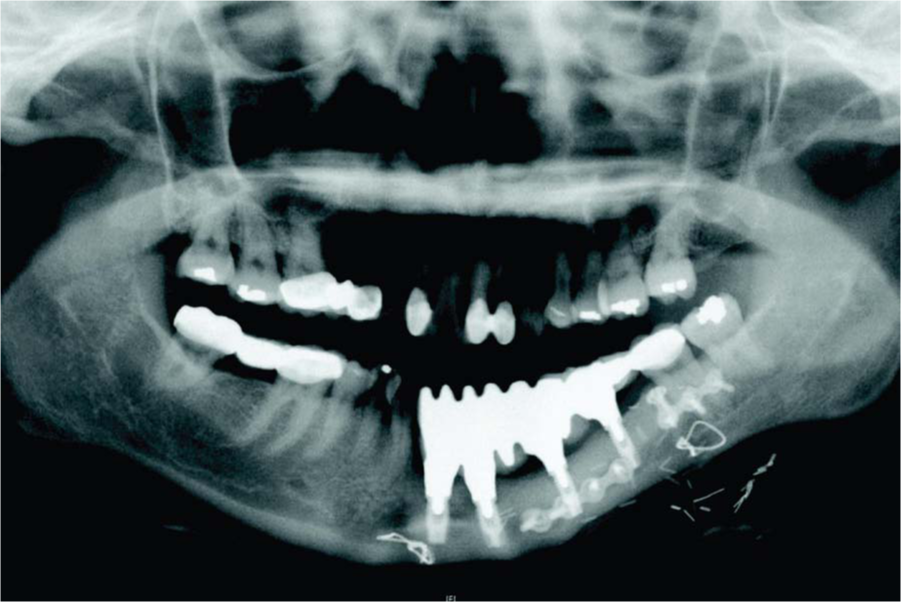
Orthopantomography showing the discrepancy between the native bone and the neomandible.
Radiotherapy
Radiotherapy reduces the amount of cellular mitosis with the aim to control possible tumor recurrence. This effect is also felt in the normal cells of the bone, soft tissues, and salivary glands, with harmful effects. Among them, a reduction in the saliva production 37 contributes to an increase in the number of caries and to a greater susceptibility of lesions in the oral mucosa, which, associated with a lower rate of cell renovation, may cause exposure of the titanium plates with consequent infection.38,39 The hard tissues also have a lower cell division rate with a decreased ability of regeneration, factors that may cause osteoradionecrosis. 37
Morbidity
The donor sites are always associated with high levels of morbidity as shown in Table 1.
Examples of morbidity associated with the donor sites.

A study from Bartaire et al. 40 shows that 24% of the patients who underwent a fibula free flap reconstruction of the mandible still showed some difficulty in walking after 8 years, and 34% could not run after the same period. The same study realized that 21% of the patients regularly took painkillers. Also, the amplitude of the foot movements and the extension and flexion strength were decreased, as well as the sensitivity at the donor area.
Amount of bone
The classical image found after reconstruction shows a significant difference between the bone height of the primitive mandible and the neomandible 37 (Figure 9). In order to solve this problem, a double layer of grafted bone, called double barrel, is necessary, 27 increasing the amount of bone harvested and the associated morbidity. Other approach is the use of iliac crest free vascularized flap, which provides considerable bone height, but with accentuated morbidity.
Amount of soft tissues
The location of the tumor and its size can lead to a massive removal of soft tissues including the tongue. This has a huge impact on speech, swallowing, and aesthetics. Furthermore, the soft tissues are of major importance on mandible reconstruction as, whatever approach is used, the bone graft or the titanium plates must be covered and protected with soft tissues, representing an important source of blood supply for the vitality of the area.
Possible future pathways
New prosthetic devices
One possible approach would be the development of new prosthesis that could replace the bone tissue lost without the recourse to bone grafts and, therefore, sharply reducing associated morbidity and patients’ recovering time. This device should be fixed in a way that could reduce the shearing stress on the retaining screws and should be prepared to be integrated in complex oral rehabilitations, possibly with dental implants.
The customization of the device should go even further by mimicking the original mandible features, particularly geometry and weight, and changing the paradigm from simple titanium plates to customized prosthesis.
Following the trend in product development, the new prosthesis should result from concurrent reverse engineering, computer-aided design and computer-aided manufacturing (CAD-CAM) approaches, and the use of surgical guides. Finally, the device could have a different concept depending on whether a marginal or a segmental mandibulectomy is considered and the volume of soft tissues present.
Tissue engineering
The possibility of regenerating marginal mandibulectomy defects with recourse to tissue engineering strategies is already documented. 31 Some attempts have been made with this goal but without the expected results.42–44 The regeneration of human tissues using stem cells from the patient, seeded in resorbable scaffolds specially designed for each application and subjected to a bioreactor that could simulate the natural conditions,45,46 is an extremely exciting field that will certainly change not only the way in which mandible reconstruction takes place but also how medicine as a whole is practiced. In fact, the new prosthetic device approach proposed could be prepared to include tissue regeneration strategies (Figure 10).

(a) Prosthetic device placed in a mandible model and (b) the prosthetic device including tissue regeneration strategies.
Marginal mandibulectomies
If the continuity of the mandible is not compromised, the reconstruction and rehabilitation procedures are much easier and the clinical and functional outcomes are improved. 47
Some studies comparing marginal with segmental mandibulectomies48,49 showed that the marginal ones were not associated with a worst prognostic. This may be due to the following two reasons:
First, because the majority of tumors have origin in the epithelial tissue, with the squamous cell carcinoma representing up to 94% of all oral cancers. 50 The periosteum and the cortical bone act as a first barrier against the cancer progression. 47
Second, the alveolar bone and the basal bone have two different embryonic origins: The basal bone comes from the ossification of the mesenchyme supported by Meckel’s cartilage, and the alveolar bone appears by induction of the dental follicles.51,52 These different origins also act as a barrier.
Thus, it is predictable that marginal mandibulectomies could be the treatment of choice whenever the surgeon deals with tumors that, including the security margin of excision, do not invade the last centimeter of the mandible, considering this dimension from the lower border of this bone.
Conclusion
It is possible to understand, as described, why mandible reconstruction has been considered a challenge. The historical evolution shows that the demand for new solutions has been a constant concern. The described state-of-the-art approaches are revealing high success rates, allowing to look with optimism for the combat against oral cancer and subsequent reconstruction ability.
However, the identified existing problems associated with the current reconstruction procedures still require to be minimized, in order to offer more predictable, affordable, and comfortable solutions to the patients.
The new pathways leading to mandibular reconstruction strategies combine surgical procedures with digital planning and CAD-CAM technology, gathering engineering and medical competences. Such combination of skills is opening the door to the design of highly customized prosthetic devices, representing a breakthrough at both levels, surgical intervention and patient comfort.
Footnotes
Conflict of interest
None declared.
Funding
This study was cofinanced by the Regional Operational Programme of North (ON.2—The New North) under the National Strategic Reference Framework (QREN) through the European Regional Development Fund (FEDER).