
Abstract
Background:
Higher plantar pressures at the medial forefoot are reported in hallux valgus. Foot orthoses with medial arch support are considered as an intervention in this pathology. However, little is known about the effect of foot orthoses on plantar pressure distribution in hallux valgus.
Objectives:
To investigate the effect of a foot orthosis with medial arch support on pressure distribution in females with mild-to-moderate hallux valgus.
Study design:
Quasi-experimental.
Methods:
Sixteen female volunteers with mild-to-moderate hallux valgus participated in this study and used a medial arch support foot orthosis for 4 weeks. Plantar pressure for each participant was assessed using the Pedar-X® in-shoe system in four conditions including shoe-only and foot orthosis before and after the intervention.
Results:
The use of the foot orthosis for 1 month led to a decrease in peak pressure and maximum force under the hallux, first metatarsal, and metatarsals 3–5 (p < 0.05). In the medial midfoot region, peak pressure, maximum force, and contact area were significantly higher with the foot orthosis than shoe-only before and after the intervention (p = 0.00).
Conclusion:
A foot orthosis with medial arch support could reduce pressure beneath the hallux and the first metatarsal head by transferring the load to the other regions. It would appear that this type of foot orthosis can be an effective method of intervention in this pathology.
Clinical relevance
Findings of this study will improve the clinical knowledge about the effect of the medial arch support foot orthosis used on plantar pressure distribution in hallux valgus pathology.
Background
Foot orthosis has been considered as a conservative intervention in hallux valgus (HV) treatment. The findings of several studies have reported improvement in pain, symptoms, and morphological aspects of the foot in patients with HV.1–4 Tang et al. 5 showed the reduction in the HV angle and pain in HV feet with usage of a foot orthosis incorporating a toe separator and arch support. Landsman et al. 6 reported the effectiveness of a foot orthosis in reducing foot pain and inter-metatarsal angle. However, Reina et al. 7 showed no significant differences in the HV angle and inter-metatarsal angle between orthosis and control group after 1 year of follow-up.
Studies have shown that collapsing the medial arch could orient the first metatarsal axis from the transverse plane to the vertical orientation. This could result in the first ray hyper-mobility in the late stance and may attribute to HV development.5,8,9 Additionally, investigations have revealed an altered pattern of plantar pressure in HV deformity, especially higher pressure under the medial metatarsal heads compared to normal feet.10–14 Studies have also shown an increased loading beneath the hallux in HV patients.11,12 Martínez-Nova et al. 12 suggested an association of first ray angular deviation with an altered pattern of plantar pressure in this region in women with mild HV.
It is suggested that foot orthosis with medial arch support may mechanically reorientate the first metatarsal axis from the vertical to the transverse orientation and prevent first ray hyper-mobility.4,7–9,15 However, the majority of studies have examined the effect of the insole on pain, morphology, and symptoms in HV patients,2,5–7 and our knowledge about the efficacy of the arch support foot orthosis in distribution of plantar pressure in this pathology is insufficient.
Therefore, the aim of this study was to investigate the effect of a foot orthosis with medial arch support on pressure distribution in females with mild-to-moderate HV. It was hypothesized that peak plantar pressure, maximum force, and contact area would be different in participants with mild-to-moderate HV after wearing a foot orthosis with an arch support for 1 month compared to the baseline measurement.
Methods
Participants
Sixteen female volunteers with mild-to-moderate HV with a mean age of 26.1 ± 5.7 years, height of 161.5 ± 5.6 cm, and weight of 56.9 ± 4.6 kg were recruited for the study. At first, the procedures were explained to the volunteers and all the participants completed the consent forms. The study was approved by the Human Research Ethics Committee of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. The participants were chosen among the female students and staff of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. The reason for selecting women participants was that the HV is more common in female than male population. 16
All participants met the inclusion criteria of having mild-to-moderate flexible HV (no severe rigid deformity). The presence and severity of HV were examined using the Manchester scale. This scale consisted of four standardized photographs to classify HV including none, mild, moderate, and severe which were matched to the participant’s feet. 17 This has been shown to provide a valid and reliable tool for HV assessment.17–19 Participants were excluded from the study if they had experienced traumatic injuries or surgery to the lower limbs, leg length discrepancy, pathologic condition or neurologic disorder in feet, and deformities other than HV in the forefoot. All the examinations were performed by an orthopedic surgeon.
Protocol
For each participant, a pair of prefabricated foot orthosis was provided. Each orthosis extended from the heel to the metatarsophalangeal joints and included a heel cup and longitudinal arch support. The orthosis was semi-rigid and constructed of 5-mm-thick polypropylene (Figure 1).

Prefabricated arch support foot orthosis.
Plantar pressure was assessed using Novel Pedar-X® (Novel GmbH, Munich, Germany) at the sampling frequency of 50 Hz. This system has been shown to be a repeatable tool for measuring plantar pressures.20,21 The system includes pressure insoles comprising 99 capacitive sensors. Four sizes of Pedar insoles were used to accommodate the range of foot sizes in this study. The pressure insoles were calibrated according to the manufacturer’s manual for each participant prior to the study.
At the beginning of the study, plantar pressures were collected in two conditions with participants wearing first the shoe-only and then shoe with foot orthosis. At each condition, participants walked for four laps of a 9-m walkway at a self-selected normal speed. Afterward, using the Pedar-X step analysis software, turning and acceleration steps were deleted and three intact steps were selected for each lap. In total, 12 steps were identified per participant at each condition.
Participants were asked to wear the foot orthosis for 4 weeks. The participants were recommended to use the foot orthosis for at least 7 h a day, 5 days a week. Telephone follow-up was conducted every week to check the correct use of the devices. After 4 weeks, plantar pressure was measured again using the same protocol as the first session.
Data analysis
Using the Pedar-X “Automask” and “Create a Mask” programs, the plantar surface of the foot was divided into eight anatomical regions: hallux, lesser toes, first metatarsal (1st MTH), second metatarsal (2nd MTH), third to fifth metatarsals (3rd–5th MTHs), medial midfoot, lateral midfoot, and heel (Figure 2). 21 For each region, peak pressure (kPa), maximum force (N), and contact area (cm2) were calculated. The walking speed (m/s) was computed by dividing the distance by time for each trial.
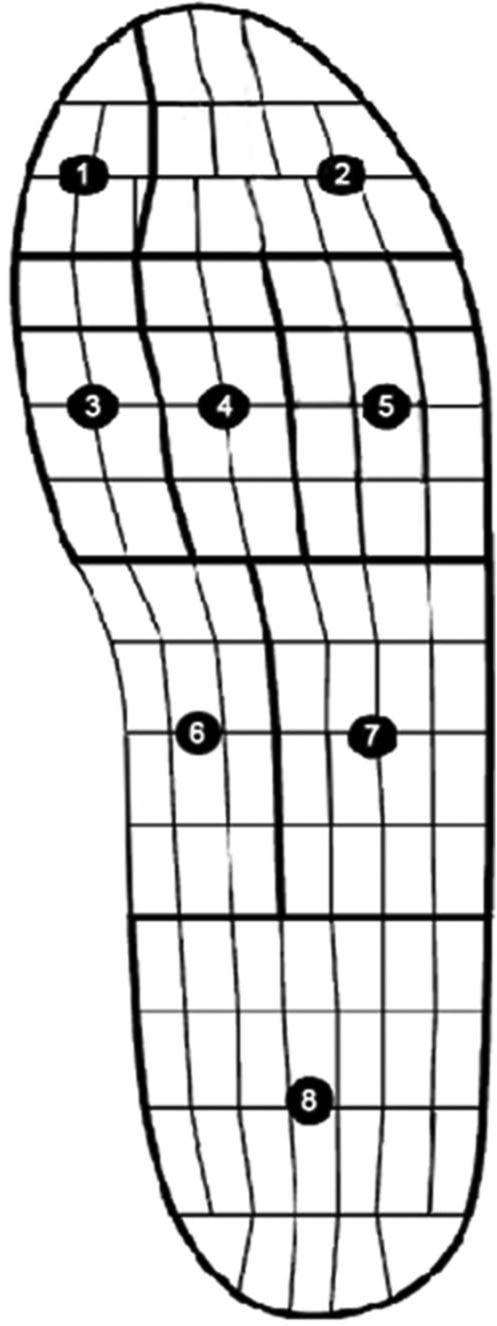
Anatomical divisions of foot from the first to eighth region are hallux, lesser toes, first metatarsal, second metatarsal, third to fifth metatarsals, medial midfoot, lateral midfoot, and heel.
The reliability of peak pressure values between multiple trials on the same participant while wearing shoe-only was examined using intraclass correlation coefficient (ICC). The Kolmogorov–Smirnov test was performed to assure the normal distribution of the data (p > 0.05). Independent t-tests were applied to assess the differences between right and left feet. 22 A repeated measures analysis of variance (ANOVA) with Bonferroni-adjusted post hoc test was applied to compare the variables in four conditions. Alpha levels were set at 0.05 for all tests. All the statistical analyses were performed using SPSS version 20 (SPSS Inc., Chicago, IL, USA).
Results
The level of ICCs was greater than 0.9 for peak pressure values. The mean and standard deviation (SD) values of gait speed (m/s) for shoe-only and foot orthosis conditions at the first and second sessions were 1.01 ±0.17, 1.04 ± 0.22, 1.03 ± 0.16, and 1.05 ± 0.27, respectively. No significant differences were found between walking speed at two sessions of data collection (p > 0.05).
Statistical analyses showed no significant differences in peak pressure, maximum force, and contact area between the right and left feet, and therefore all the analyses were performed on the right feet (p > 0.05). Tables 1 to 3 represent the mean values and SD of peak pressure, maximum force, and contact area in four conditions including shoe and foot orthosis in the initial and after 1 month of follow-up.
Mean (SD) values of peak pressure (kPa) for the four conditions in all regions.
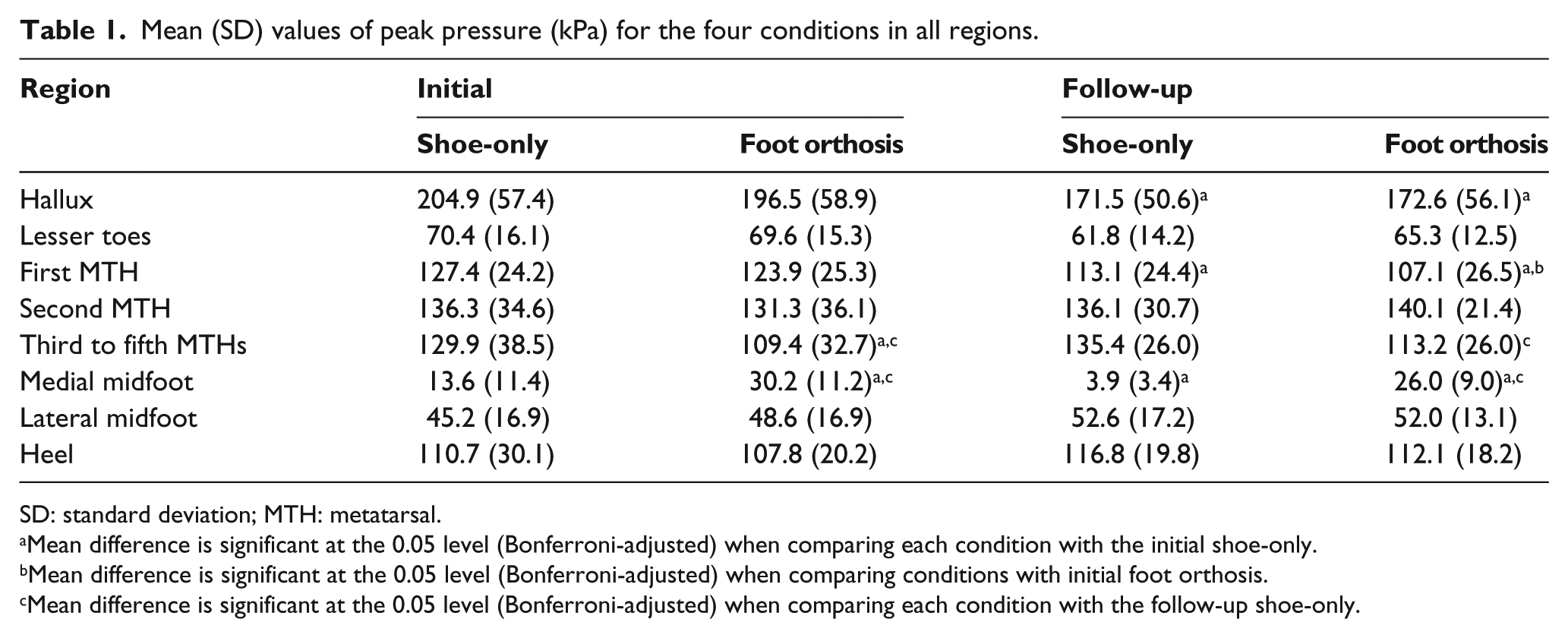
SD: standard deviation; MTH: metatarsal.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing each condition with the initial shoe-only.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing conditions with initial foot orthosis.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing each condition with the follow-up shoe-only.
Mean (SD) values of maximum force (N) for the four conditions in all regions.
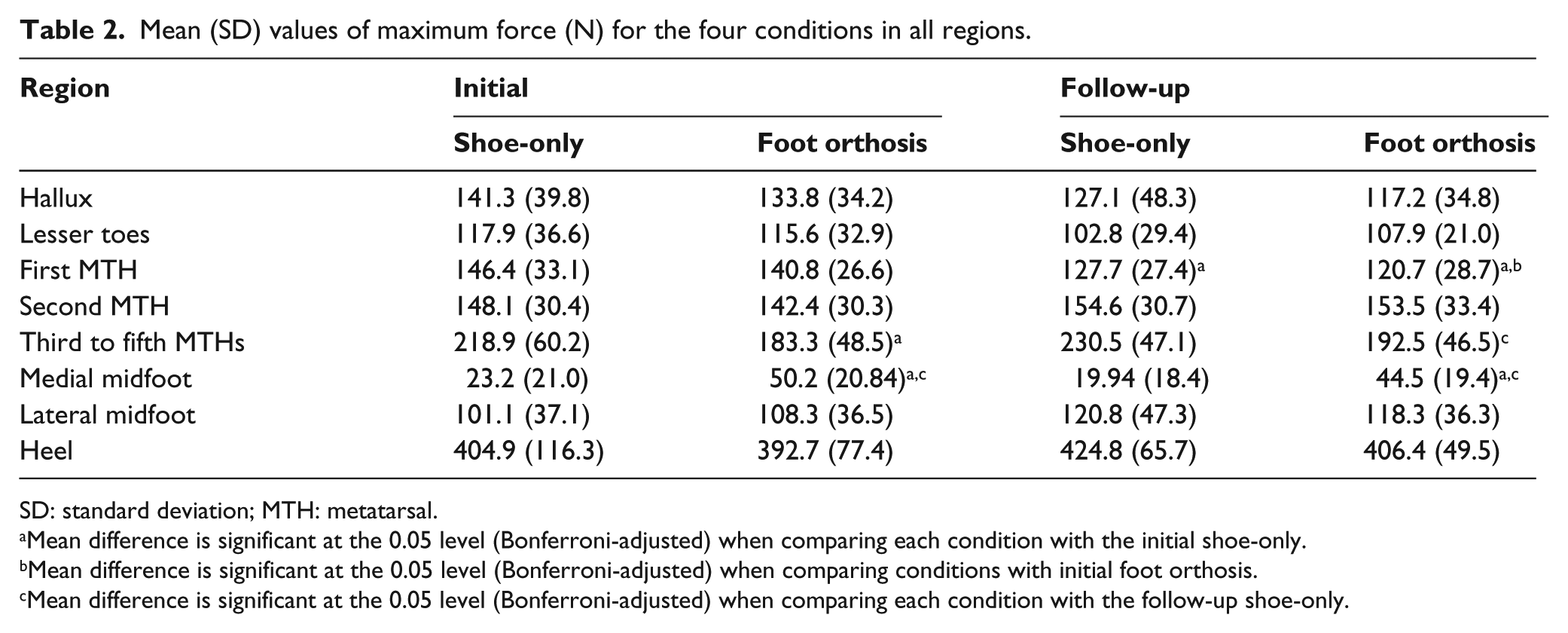
SD: standard deviation; MTH: metatarsal.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing each condition with the initial shoe-only.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing conditions with initial foot orthosis.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing each condition with the follow-up shoe-only.
Mean (SD) values of contact area (cm2) for the four conditions in all regions.
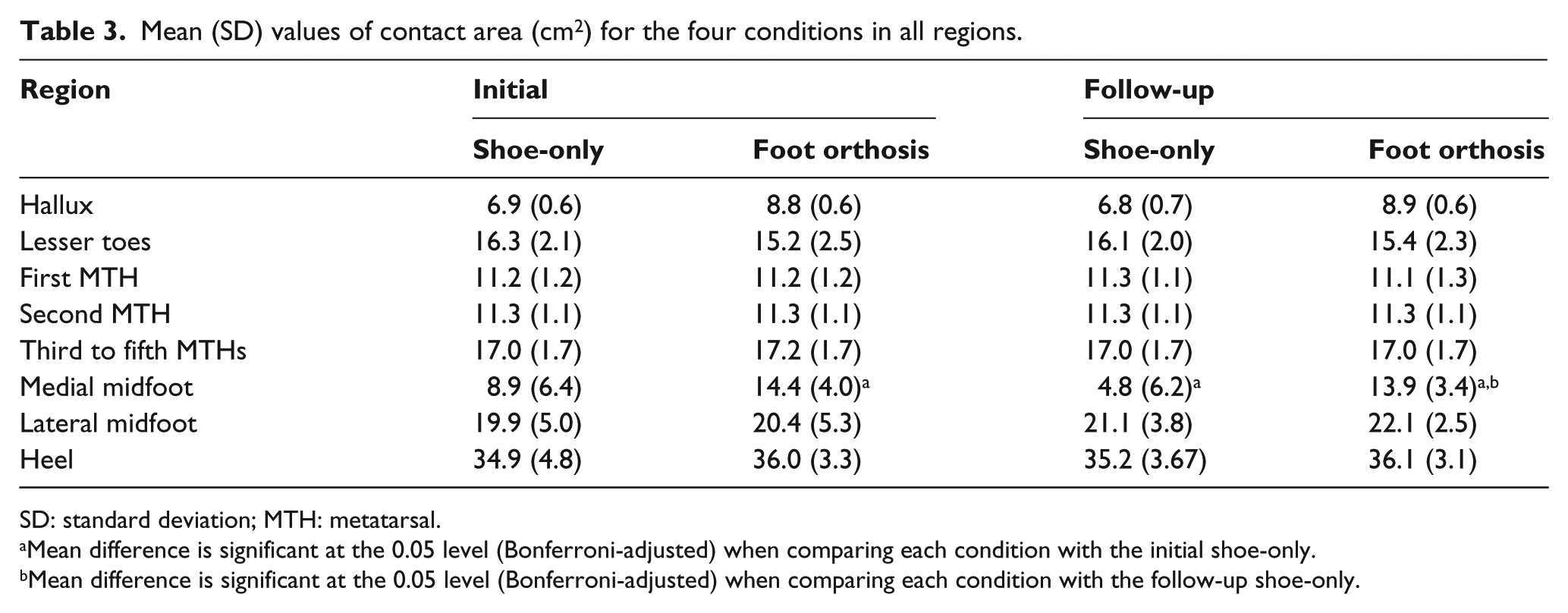
SD: standard deviation; MTH: metatarsal.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing each condition with the initial shoe-only.
Mean difference is significant at the 0.05 level (Bonferroni-adjusted) when comparing each condition with the follow-up shoe-only.
According to the Tables 1 to 3, hallux presented significantly lower peak pressure in the follow-up assessment compared to the initial shoe-only condition (p = 0.02). However, no significant differences were observed between four conditions in the maximum force and contact area at this region (p > 0.05). There was a significant decrease in peak pressure and maximum force values in follow-up assessments comparing to the initial shoe-only assessment at the 1st MTH (p = 0.03, p = 0.02). Moreover, peak pressure and maximum force were decreased in the follow-up orthosis in comparison with the initial orthosis condition (p = 0.00, p = 0.03). At the 3rd–5th MTH, the mean of peak pressure and maximum force were significantly decreased by wearing orthosis at initial and follow-up assessments compared to the shoe-only conditions (p = 0.00). In the medial midfoot region, peak pressure, maximum force, and contact area were significantly higher with foot orthosis than shoe-only at both sessions (p = 0.00). Contact area was significantly smaller in the follow-up than initial shoe assessment (p = 0.00). No significant differences in variables were seen for the other regions.
Discussion
The findings herein support the hypothesis that the wearing of foot orthoses with a medial arch support for a period of 1 month could change peak plantar pressure, force, and contact area in females with mild-to-moderate HV. While it has been suggested that arch support orthosis is beneficial in HV management,2,5,6 the results of this study support this concept by usage of plantar pressure method.
In this study, peak pressure and maximum force underneath the hallux, first, and 3rd–5th metatarsal heads were reduced after 1 month of using the orthosis. Additionally, a significant increase in these variables at midfoot with foot orthosis compared to the shoe-only was observed. Based on the previous studies, increased pressure under the hallux and 1st MTH head displays a pathological condition which is positively associated with the first ray angular deviation.11,12,23 It is demonstrated that arch support foot orthosis can improve or control the hallux deviation.2,4–6,24 Theoretically, foot orthosis with medial arch support may mechanically reorient the 1st MTH axis from the vertical to the transverse orientation. This could prevent the excessive pronation of first ray which is attributed to HV development and progression.4,7–9 Considering the pressure distribution, arch support orthosis should transfer the load under medial forefoot to the midfoot area.22,25,26 In accordance with this concept, the results of this study showed that the pressure and force were reduced in the forefoot and increased in the midfoot. Generally, it can be concluded that a foot orthosis with medial arch support may be served as an effective intervention in correcting high plantar pressure under the forefoot areas in HV.
In line with the previous studies,22,25,27 findings showed no significant differences in variables in the 2nd MTH region after using the orthosis. However, Tsung et al. 26 suggested the greatest peak pressure reduction at this region by the orthosis. This might be attributed to the metatarsal pad that was not applied in the present orthosis structure.
The results of this study are limited to the effectiveness of a foot orthosis with a medial arch support in altering pressures in females with mild-to-moderate HV after 1 month of follow-up. It is also acknowledged that participants with mild and moderate HV were grouped together. The authors did not present the results as two separated groups since the pressure did not significantly differ between the two groups. This might be as a result of limited number of participants on each group (6 participants with mild and 10 with moderate HV). Thus, further investigation is needed to assess the longer term biomechanical effect of the insole in a wider range of HV participants with mild and moderate HV.
Conclusion
This study has demonstrated that using a foot orthosis with medial arch support for 1 month decreased peak pressure in the forefoot region, but increased it in medial midfoot in females with mild-to-moderate HV. Thus, foot orthosis with a medial arch support mechanism could be considered as an effective method in the redistribution of pressures underneath the foot in HV.
Footnotes
Acknowledgements
The authors would like to thank the Prosthetics and Orthotics Department, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research was supported by the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.