
Abstract
Background:
The Milwaukee brace is an efficient method for correcting hyperkyphosis before skeletal maturity. However, loss of correction in long-term follow-up is inevitable.
Objectives:
To determine loss of correction and factors affecting the loss of correction.
Study design:
Retrospective study.
Methods:
A total of 49 corrected patients by Milwaukee brace participated minimum 2 years after treatment completion. The participants were categorized into two groups based on their roentgenograms: Group 1 (n = 36) had kyphotic curves of 45° or less and Group 2 (n = 13) had kyphotic curves of more than 45°.
Results:
The mean loss of corrections for Group 1 and Group 2 were 3.80° (ranges = 0°–13°) and 12.92° (ranges = 8°–22°), respectively. Group 1 showed no significant difference between the average hyperkyphosis of the patients for the part-time and full-time treatment duration (p = 0.02). By contrast, a significant difference was observed between the average hyperkyphosis of patients in Group 2 for the part-time and full-time treatment duration (p < 0.05).
Conclusions:
Patients with kyphosis of 60° or less who can save the correction in full-time orthotic treatment in part-time treatment may have the least loss of correction over time.
Clinical relevance
As the orthotic treatment is a time-consuming method that needs the close collaboration of patient and treatment team, it is possible that clinicians predict the probable result of treatment and efficiency of orthotic treatment. Thus, a clinician can abandon orthotic treatment and refer the patient for an operation.
Background
“Thoracic hyperkyphosis” is the term used when the degree of the kyphotic curve of the thoracic spine increases. The Scoliosis Research Society defines that a normal kyphosis is between 20° and 40°. However, Fon et al. 1 and Stagnara et al. 2 disputed this figure and claimed that the range is too narrow.
Hyperkyphosis results from several conditions. Scheuermann’s disease is a common reason of hyperkyphosis with an incidence rate of 4%–8%, and it has no gender predominance. The sign of this disease is the existence of at least three consecutive wedged vertebral bodies of at least 5°.3–6 Besides Scheuermann’s disease, spinal fracture, neuromuscular diseases, posture, and unknown reasons can also cause hyperkyphosis. In general, if no plausible scientific reason can explain an existing hyperkyphosis, the term “idiopathic hyperkyphosis” is used.
Two approaches are available in treating hyperkyphosis: orthotics management and surgery. Surgery is an easy and quick method for curve correction, but it comprises the risk of death, postoperative neurologic deficits, infections, fixator failure, pseudarthrosis, loss of correction, progression of kyphosis, pulmonary emboli, and persistent back pain. 7 The Milwaukee brace is an efficient orthosis in flexible hyperkyphosis and is still prescribed for hyperkyphosis correction. In this case, bracing should start before the curve exceeds 50°, 8 and the patient needs to have at least 1 year of growth before skeletal maturity is reached. Bracing must continue for a minimum of 18 months to have an effect on hyperkyphosis.9,10 Milwaukee brace has a pelvic basket in the distal end that is connected to a cervical ring in the proximal end through an anterior bar and two posterior bars. Two kyphotic pads are installed to push the hyperkyphosis anteriorly. 28
Bradford et al. analyzed the effectiveness of the Milwaukee brace on adolescents suffering from Scheuermann’s hyperkyphosis. Among 75 patients, only 19 had worn the brace for a minimum of 18 months. They concluded that the Milwaukee brace is an effective method of managing hyperkyphosis in adolescents. 11, 28 A number of published studies have confirmed the positive outcomes of the nonoperative management of Scheuermann’s hyperkyphosis by using orthoses.8,11,13–21 The issue mentioned in the literature is loss of correction after orthotic treatment of hyperkyphosis. Few retrospective studies have worked on this issue. Montgomery and Erwin 17 studied long-term outcomes of Milwaukee brace in a group of 39 patients with Scheuermann’s disease and found a mean correction loss of 15° over time. 17 Farsetti et al. 21 compared the results of using the Milwaukee brace in patients who suffered from Scheuermann’s hyperkyphosis with those who suffered from idiopathic hyperkyphosis. They demonstrated that loss of correction occurred in both groups of patients, but the average loss of correction in patients with idiopathic hyperkyphosis was more than that observed in patients with Scheuermann’s hyperkyphosis. Bracing in Scheuermann’s hyperkyphosis can provide 50% correction in the brace, and approximately two-thirds of cases may maintain partial correction at long-term follow-up.22,23
At present, there are few studies available on the loss of correction in idiopathic hyperkyphosis. Most studies of bracing outcome in Scheuermann’s hyperkyphosis about loss of correction in long-term follow-up lack a control group. In addition, the level of kyphosis which would increase the risk of deformity progression has not yet been determined. We conducted a retrospective research to study the results of orthotic treatment in idiopathic hyperkyphosis after some years of treatment completion. The main goal was to identify the factors that may affect the treatment results. This study looked for any key point that can predict the results before the end of the orthotic treatment for making the decision whether orthotic treatment should continue.
Methods
A total of 117 subjects (93 females and 24 males) who used to have hyperkyphosis were selected to participate in a retrospective study based on their files in a spine center. The exclusion criteria were hyperkyphosis with known reasons such as Scheuermann’s hyperkyphosis, postural hyperkyphosis, spinal fracture, neurological, musculoskeletal hyperkyphosis, and scoliosis of 5° or more. The medical files of patients were investigated and 70 of 93 treated patients with Milwaukee brace were chosen randomly. Based on medical files, it was found that all participants had kyphotic curves of less than 45° in their last examination and had completed their orthotic treatment at least 2 years before this study.
All 70 subjects were contacted, and those who accepted to attend the study were clinically examined and sent to radiography. The kyphotic curves of 49 participants who delivered their radiographs were measured. Other variables, including initial kyphosis, kyphosis in brace, kyphosis at the end of full-time wearing brace, kyphosis at the time of ending treatment, age of beginning treatment, age of finishing treatment, and gender, were extracted from medical files of subjects.
This study was approved by the medical ethics of the Faculty of Rehabilitation Sciences of Iran University of Medical Sciences. All the patients signed the consent form before participating in the study.
Data analyses were performed by using SPSS software version 11.0 for Microsoft Windows. The alpha level of 0.05 was defined as statistically significant for all the tests. Repeated-measure analysis of variance (ANOVA) and Student’s t-test were used to compare the data.
Results
A total of 49 subjects participated in this study. An orthopedic surgeon measured the curve severity on the standing anterior–posterior and lateral roentgenogram on the basis of standard 24 procedures used in other studies.1,14,25 The evaluation of kyphotic curves of participants showed that all subjects had lost some of correction after two or more years (range = 2–8 years) without the brace, while they had hyperkyphosis of 45° or less when they discontinued using the brace.
Among the 49 subjects, 36 had hyperkyphosis of 45° or less and 13 had hyperkyphosis of 46° or more. To simplify the analysis, the subjects were divided into two groups, namely, Group 1 and Group 2, according to the severity of the kyphotic curve during the final follow-up examination. The following findings were provided based on medical files of participants and measurement of kyphotic curves of participants at the time of this study.
Roentgenographic findings
Group 1
Group 1 consisted of 36 subjects (11 males and 25 females) who had completed the full treatment duration wearing the Milwaukee brace consistently. The participants had hyperkyphosis of 45° or less at the time of treatment completion and after a minimum of 2 years of treatment completion. The average of the initial hyperkyphosis was 58.28° (range = 46°–76°). The average age at the time of initial examination was 13.06 years (range = 8–16 years). Among the total patients in Group 1, 67% followed the prescribed exercise program completely. Patients wore brace for 16.97 months (range = 6–51 months) 23 h a day and wore brace part-time for 20.28 months (range = 5–46 months). The kyphotic curve of patients in each group is shown in Figure 1.
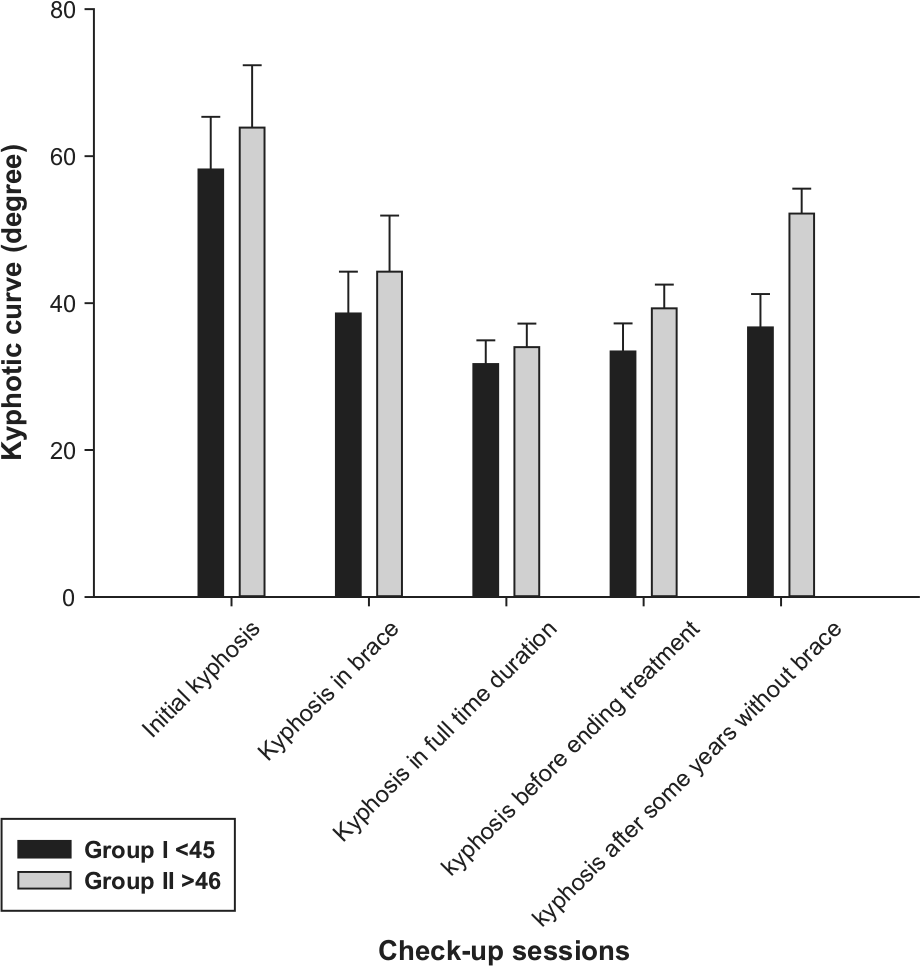
The orthotic treatment results in patients who saved their orthotic correction, Group 1, and who lost some of the correction, Group 2.
Group 2
Group 2 consisted of 13 patients (4 males and 9 females). Each of the patients had hyperkyphosis of 46° or more at the time of this study. These patients had a greater loss of correction during treatment on the basis of the status of their kyphotic curves at the time of this study. The average initial hyperkyphosis was 63.92° (range = 50°–80°). The average age of the Group 2 members at the time of initial examination was 13.27 years (range = 10.5–15 years). The average duration for full-time brace use was 17.57 months (range = 6–32 months). Among those involved in the study, 36% completed the exercise program consistently during treatment. Figure 1 shows the trend of decrease of hyperkyphosis during the treatment.
Statistical analysis
Results show that the most effective reduction in hyperkyphosis was observed in patients who wore the brace over a long time. However, a significant difference was not observed between the two groups. The effects of the exercise program and gender were measured across each group, but no significant differences were found. We compared the severity of hyperkyphosis in each group during treatment. We found that a significant difference exists between the average hyperkyphosis and initial hyperkyphosis in Group 1 and between hyperkyphosis during brace use and hyperkyphosis at the time of treatment completion (p < 0.05). No significant difference was observed among the average hyperkyphosis at the end of full-time brace use, at the time of treatment completion, and years after treatment completion (p = 0.02).
In Group 2, the severity of hyperkyphosis significantly differed in all evaluation points (p < 0.05); however, no significant difference was observed between the hyperkyphosis of patients during treatment and the hyperkyphosis of patients at the time of treatment completion (p = 0.17).
Discussion
In this retrospective study, the results of treatment after more than 2 years of follow-up of patients with idiopathic hyperkyphosis who were treated with Milwaukee brace showed a loss of correction in almost all patients. This result is consistent with other studies on Scheuermann’s hyperkyphosis.5,11,16 In this study, 74% of patients still had a kyphotic curve of 45° and less. The long-term outcomes of bracing in idiopathic hyperkyphosis are more stable than those in Scheuermann’s hyperkyphosis reported by Tribus. 22 Since in his study approximately two-thirds of treated patients maintained correction during long-term follow-up.
Because of difference in definitions of a normal kyphotic curve,1,2 it is difficult to compare our results of loss of correction with other studies. The overall mean for loss of correction in Group 2 was 12.92° in long-term follow-up, while it was 15° in Scheuermann’s hyperkyphosis. 17
A total of 13 participants who had consistently used the Milwaukee brace were recognized to have hyperkyphosis after ending treatment for at least 2 years; however, their hyperkyphosis severity was less than their initial hyperkyphosis. We concluded that if any intervention has not been used, their initial hyperkyphosis would have increased. Two studies on untreated hyperkyphosis8,16 showed an increase of hyperkyphosis in 7 out of 43 patients.
Bracing can provide best results in mild hyperkyphosis. The average of initial kyphosis severity of Group 1 was less than 60°, while it was less than 70° in Group 2. This is consistent with results of orthotic treatment in Scheuermann’s and postural hyperkyphosis.13,23,26,27
Patients who show a gradual decrease in hyperkyphosis severity during bracing have the least loss of correction over the time. In this study, patients in Group 1 could save correction in brace when they were wearing brace part-time, whereas patients in Group 2 lost an overall mean of 5° achieved in full-time treatment when they were wearing brace part-time.
This study focused on the statistical differences between hyperkyphosis severities in each group. We discovered that the patients who maintained correction in full-time and part-time duration experienced the least loss of correction even after treatment completion. We assumed that the longer the brace was worn over a part-time or full-time basis, the larger the effect observed during the final follow-up examination. However, our analysis did not confirm whether the duration the brace was worn is statistically significant. Some patients maintained correction after treatment completion time and even during follow-up examination several years after doffing the brace, wearing brace for 8–10 months full-time.
Other variables include exercise, gender, age, full-time treatment duration, and part-time treatment duration. The statistical analysis was not significant for these variables. Therefore, we concluded that these variables do not have a significant influence on the treatment outcome.
Although we originally hoped to find effective variables which made orthotic treatment inefficient, we were unable to do so. Accordingly, no control group (untreated patients) and few numbers of patients made it difficult to compare results of treatment. So, a future study with higher number of subjects and a control group are required for precise conclusion.
Conclusion
On basis of the results of this study, we concluded that Milwaukee brace has good long-term results of treatment in patients who have idiopathic kyphosis. The results show that all treated patients demonstrated loss of correction over time, but kyphotic curve was in range of normal in 74% of the patients who were followed for more than 2 years. However, an initial kyphosis of more than 60° was associated with a higher loss of correction in long-term follow-up. Comparing two groups, it was found that patients who could save the correction in brace in part-time treatment duration, might have the least loss of correction some years after treatment completion. Future studies should include a control group in order to find the reasons behind the loss of correction with the Milwaukee brace with time.
Footnotes
Acknowledgements
We would like to thank Dr. Shahin Goharpay and Dr. Mohammad Kamali for their comments on the statistical analysis of the experimental data.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by UM/MOHE/HIR Project no. D000014-16001.