
Abstract
Background:
The incidence of foot amputations increased in the Netherlands to 3.3/100,000 people up to 1994. Despite these numbers, only a few basic prosthetic and orthotic devices are available, and all lack functionality to restore ankle and foot mobility.
Objectives:
The aim of this explorative study was to design and test a unique prosthesis for Syme or Pirogoff amputees with the necessary low installation height but restoring ankle and foot mobility.
Study design:
A case study was performed.
Methods:
The new prosthesis was designed and numerically analyzed on aspects concerning strength and deformation. A prototype was tested in a case study to assess the biomechanical behavior of the new foot. As a reference, six Syme/Pirogoff amputees were measured. Additionally, all volunteers filled out a questionnaire to evaluate their prosthetic feet.
Results:
The self-selected and maximum walking speed of the case subject at 0° and 5° slopes was higher using the new foot (0.36 m/s and 0.53 m/s, respectively) comparing to the Low Rider (Otto Bock HealthCare) (0.31 m/s and 0.31 m/s, respectively). Using the new foot, a more symmetrical walking pattern was achieved.
Conclusion:
The case study shows that this new prosthetic foot could be an improvement compared to existing prosthetic feet.
Clinical relevance
Foot amputees with low available installation height still experience daily the inconvenience of missing ankle and foot mobility. Their low velocity and cosmetically poor walking pattern influence on their sound leg and overall walking functionality. A more functional prosthesis would have a great impact on their daily activities.
Background
Between 1988 and 1996, more than 133,000 lower limb losses were reported yearly in the United States, with trauma as the secondary most common cause behind vascular diseases. 1 In 1996, foot amputations and trans-tibial amputations (TTA) per 100,000 habitants were 6.23 and 12.85, respectively. The incidence of foot amputations (transmalleolar to transmetatarsal) in the Netherlands increased in the period 1982–1994 from 1.7 in 100,000 to 3.3 in 100,000 people. 2 Despite the impact, more recent and specific numbers are not available in the literature.
The Syme3,4 and Pirogoff 5 amputations are two ankle disarticulation methods used to preserve as much leg length as possible. A leg length discrepancy of 2–6 cm occurs, with the establishment of a weight-bearing residuum with a large supporting surface.
Changes in the biomechanical characteristics of lower limb amputees (while using a prosthesis) are, for example, reduced self-selected walking speed (SSWS),6,7 increased variability in muscle excitation patterns, 8 increased gait asymmetry,8,9 and increased metabolic costs.7,10 Lower leg amputation also influences the impact forces on the sound limb.8,11–14 Although investigated in trans-tibial amputees, these changes might be explained, besides the various clinical indications for amputation, by the relative stiff character of the ankle–foot prostheses with low installation height. 15 Therefore the mechanical energy needed during walking has to be generated elsewhere. The missing external work is compensated for by the knee 16 and hip joint11,17 musculature of the prosthetic side and by the sound leg, which can lead to additional pathologies.
Ankle mobility and energy returning capacities of a prosthesis may reduce the need for compensation. Based on field experience, the relatively small number of Syme and Pirogoff amputees, together with the small residual space difficulty, can be the main reasons why no functionally good prosthetic feet are available for these patients.
In contrast with the sophisticated prostheses available for TTA, functions reflecting ankle properties are included to a far less degree in the few basic devices with low installation height. The main goal for these prosthetic feet is to restore leg length discrepancy. Functions represented to a lesser extent in these feet, compared to the natural foot, are ankle rotation, energy storage during heel-strike (HS)/mid-stance (MS) and return during push-off, 18 stability on uneven surfaces or slopes, flexibility appropriate to the patients needs, and smooth roll-over dynamics. 19 Especially traumatic amputees, who are usually more active, will profit from a more flexible and energy returning foot. 20 Although these results have been investigated in trans-tibial amputees, the authors believe, based on clinical experience, that the results also hold for Syme and Pirogoff amputees.
The aim of this explorative study was to design and test a prosthetic device for Syme or Pirogoff amputees with an overall installation height of 2 cm. The main focus of this prosthesis was to mimic the natural mechanisms of the ankle and foot in the best way possible with respect to shock absorption, energy storage and return, ankle mobility, and smooth roll-off capabilities with a unique low installation height.
Methods
Prototype
This study consisted of four separate phases. First, the design method of Ullmann 21 was used together with the three-dimensional (3D) drawing software SolidWorks (Dassault Systemes 2009–2010) to design an innovative prosthetic foot, while keeping in mind the three most important requirements: an extremely low installation height (2 cm) ankle movement, and energy storage and return.
The second part of this study contained a finite element analysis (FEA) (Figure 1) to assess structural integrity and to optimize the prototype design using the same software. For the analyses, the socket was left out and the appropriate parts of the feet were constrained. Natural loadings were applied for a static simulation to mimic three phases of the gait cycle: heel strike (HS), mid stance (MS) and toe-off (TO). For all these scenarios, stress, strain, and displacement analyses were performed.
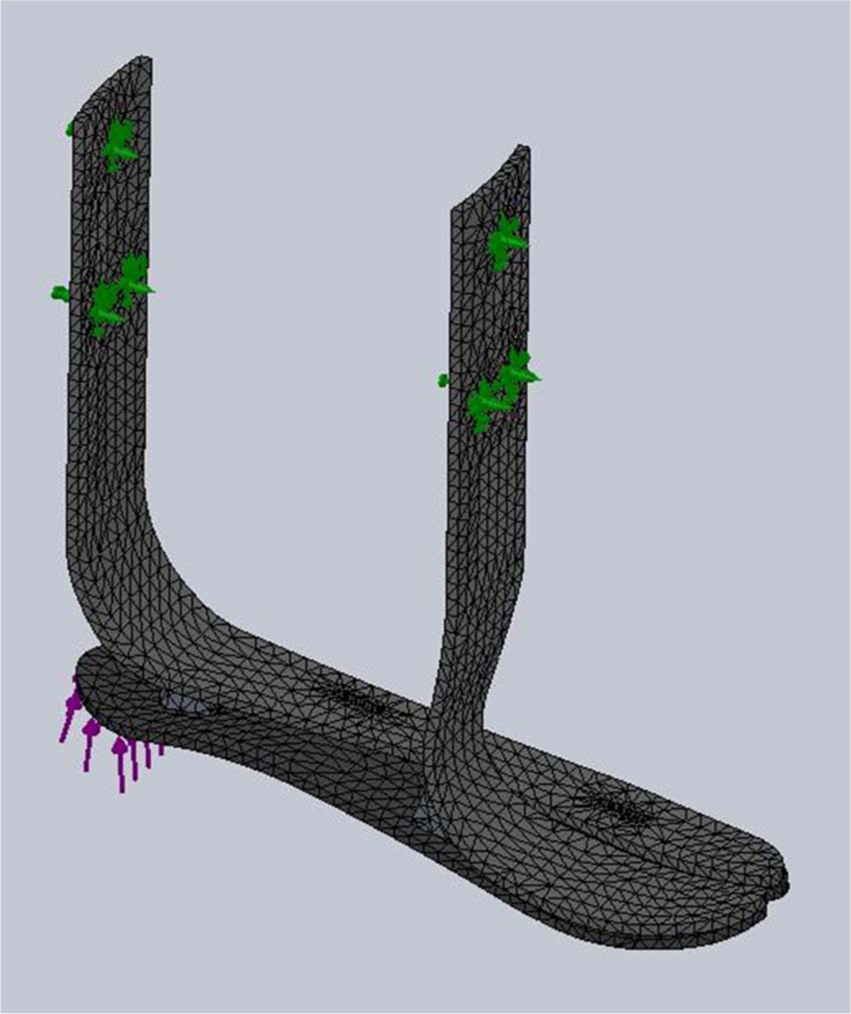
Mesh elements, applied force during HS (thin arrows), and fixation (fat arrows with multiple arrowheads) during finite element analysis of the new prosthetic foot.
The design has been optimized regarding the three phases of the gait cycle: HS, MS, and TO. To investigate whether the theoretical improvements concerning shape indeed increase walking performance, displacement limits were based on existing prosthetic feet properties.22,23
The maximal allowed displacements concerning these phases were under normal loading HS and MS 5 mm and TO 10 mm, under 5× body-weight loads of 10 mm, 20 mm, and 20 mm respectively. Difference between lateral and medial displacement was maximal 5 mm at HS and MS and 10 mm during TO at normal loading. Displacement limits were also set to be sure the foot was stiff enough to be safe. By remodeling the shape and thickness of the different carbon components and therefore manipulating the stiffness and behavior of the device which was verified using FEA, a design was finally obtained with the wanted properties. Due to the shape and composition of the different parts, roll-off is theoretically actuated from the lateral side during MS, toward the medial side during TO as seen in the natural foot. 24 Thereafter, safety calculations using a 5× body-weight load, applied on different areas of the sole of the foot (medial and lateral) were performed.
In the next phase, a 3D prototype (Figure 2) was made using carbon fiber composite material. Standard available vacuum infusion materials were used during this process. The laminate characteristics were optimized using the Laminate Analysis Program. 25 Torayca T300 B 3K 40B carbon fibers (Toray, USA) woven into CD 0286 5H satin fabric (TenCate Advanced Composites, The Netherlands) was used. Araldite LY 1564 SP and Aradur XB 3486 (Huntsman, Germany) were used as a resin and hardener, respectively (ratio 100:34 g).

First prototype of the new prosthetic foot.
Gait analysis
In the fourth phase, a gait analysis study was performed in six amputees (Table 1) during day 1. This group of six volunteers using their own prosthetic foot (i.e. the LP Vari-Flex with EVO from Ossur, the Trustep and Trés from Loth Fabenim, the Seattle Foamer Low Profile from Trulife, and two with the Carbon Copy from Ohio WillowWood) was used as a reference because no comparable normative data are available in literature for this specific group of patients.
Demographic characteristics of the study population.
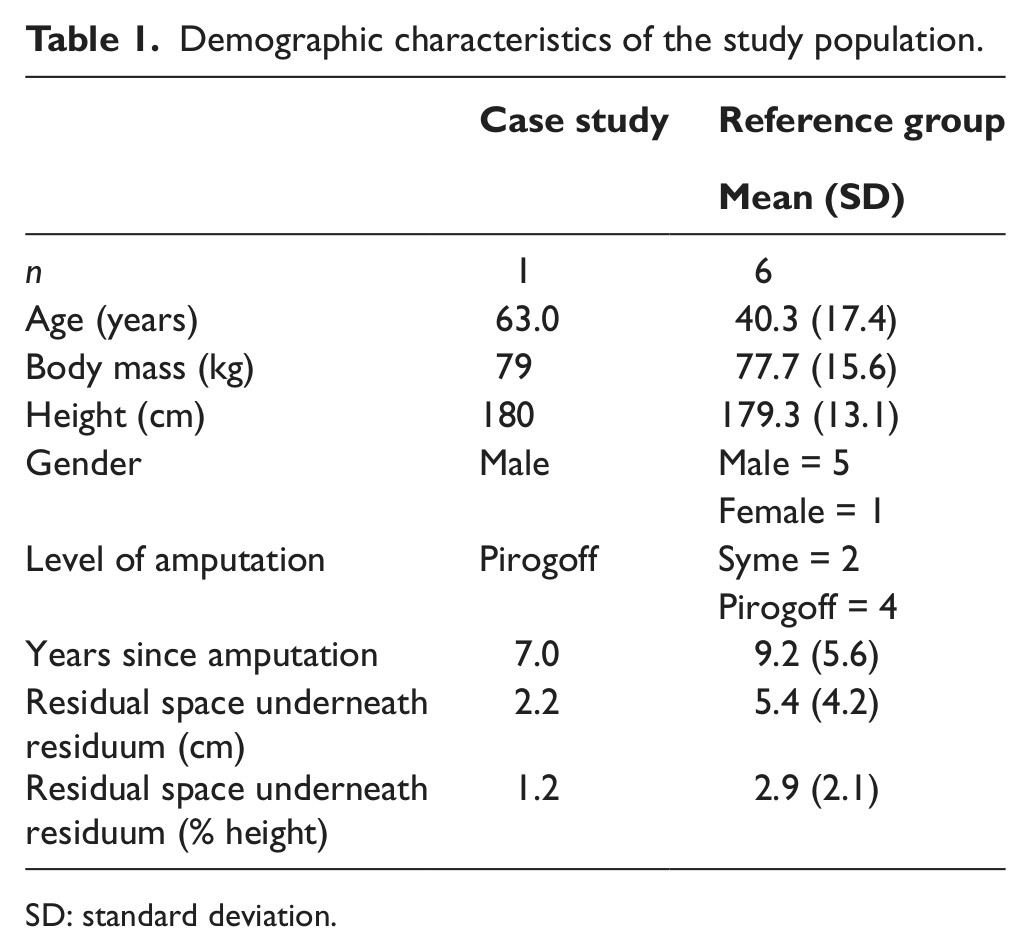
SD: standard deviation.
One of the volunteers, from now on referred to as the “case subject,” also walked with the new prosthetic device to assess its biomechanical behavior and therefore test whether the theoretical design can indeed be an improvement concerning the gait of amputees. Data from days 1 and 8 of our case subject using the new prosthetic foot were compared with the mean data of our reference group. Patients were selected from the databases of Rehabilitation Centre De Hoogstraat and University Medical Centre Utrecht. Amputees who were not able to walk without shoes or an aid, and with additional mental or physical pathologies were excluded. Five volunteers were traumatic amputees, and one underwent amputation surgery after a congenital anomaly. All volunteers gave informed consent, approved by the Medical Ethics Committee of the University Medical Centre Utrecht (nr. 11/471).
A socket was custom made for our case subject with the necessary adjustments needed to enable fixation of the new prosthetic foot. A licensed prosthetist ensured proper fitting of the socket and alignment of the foot. On day 1, the case subject walked with the new prosthetic foot and the Low Rider (LR) from Otto Bock (Germany), his usual prosthetic device for 5 years. The case subject was then allowed to get used to the new prosthetic foot at home, after which, measurements were performed again at day 8. Measurements were done barefoot using a Zebris FDM-T treadmill (Scheinworks, Germany) with accompanying software. In addition, a 10-m walkway with an inlayed ground reaction force (GRF)-platform (AMTI AccuGait Force Plate, 1000 Hz, Advanced Mechanical Technology Inc., USA) was used.
All volunteers performed a walking test using their own prosthetic foot. At a self-selected walking speed (SSWS), volunteers walked multiple times up and down the walkway until six full foot prints of the prosthetic foot were collected. The treadmill measurements included four different speeds on a 0° and 5° upward slope; SSWS, 1.5 km/h, 3.0 km/h, and as fast as possible (AFAP) during 30 s were performed. The 5° slope measurements were done to check whether the new prosthetic foot enables ankle mobility, an important characteristic which today’s prosthetics lack. These conditions resulted in a total of 60 treadmill parameters. Walking speeds were blinded for the volunteers as well as the investigator until the SSWS and AFAP speeds were reached and the volunteer gave a verbal sign. All GRF-plate and treadmill data were averaged across trail for each volunteer. Gait parameters (Figure 3) were compared between the case study using the LR and the reference group, as well as between the LR and the new prosthetic foot. Although no statistics can be calculated from such a case study, a 5% deviation borderline 9 was used while comparing data, assuming that this is indicative of a difference in foot characteristics.
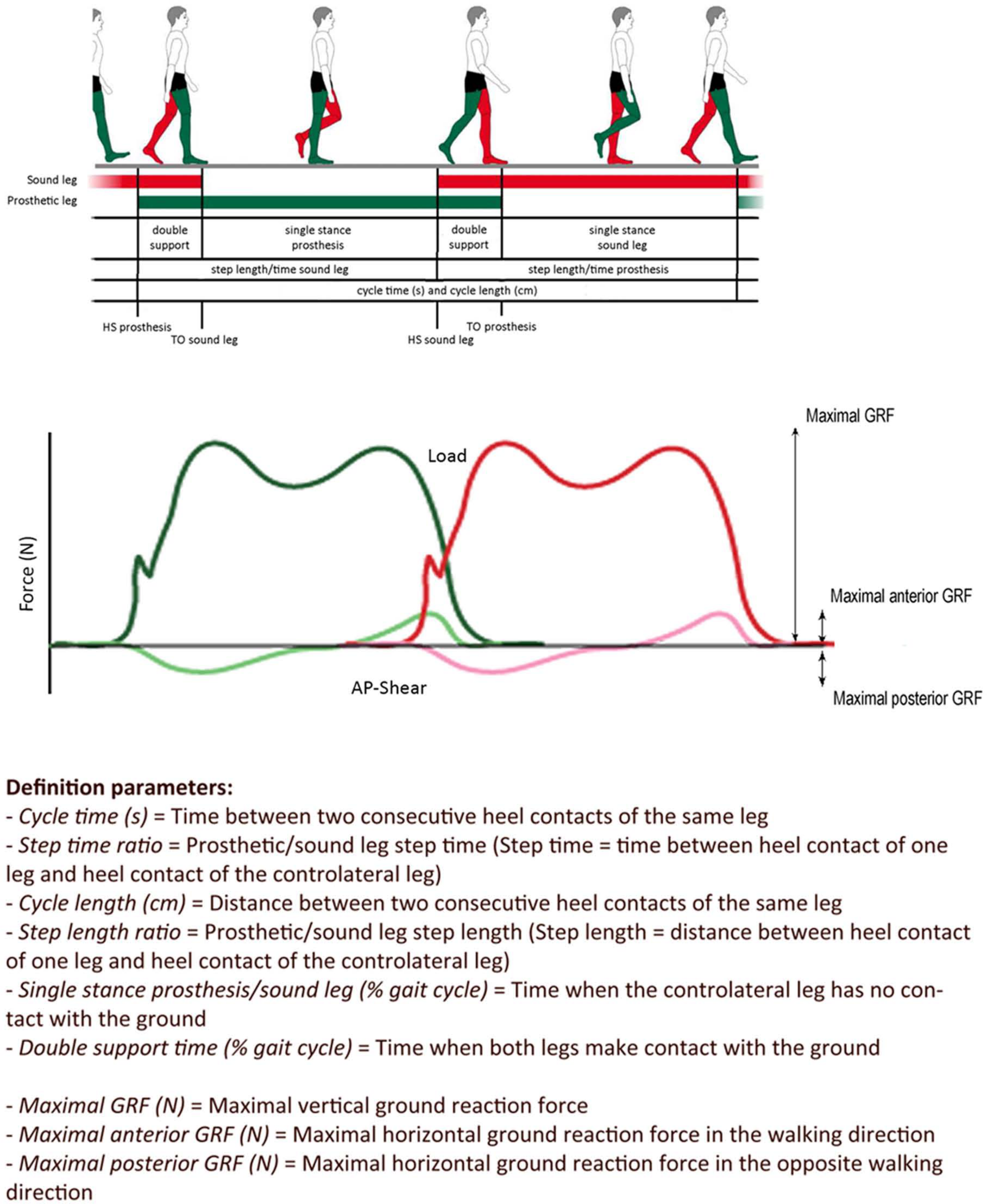
Treadmill and GRF-plate measurement parameters of the gait cycle.
Questionnaire
All volunteers filled out a questionnaire. The volunteers had to grade 30 scenarios concerning 5 categories; stability while standing, stability while walking, functional factors, special activities, and comfort/fitting, 18 to get a better prospective about the prosthetic feet. Additionally, there was room for remarks. Mean scores of the reference group were compared to the difference in score of the LR versus the new foot.
Results
Prototype
This first prototype functions best at a body weight of 80–90 kg. However, computer simulations and strength analyses showed that no material fractures appear if a load of 5× body weight is applied (which mimics for example a misstep). Detailed information about the properties of the material is found in Table 2; deformation analyses are presented in Figure 4.
Specific design properties of the first prototype for each carbon fiber part.

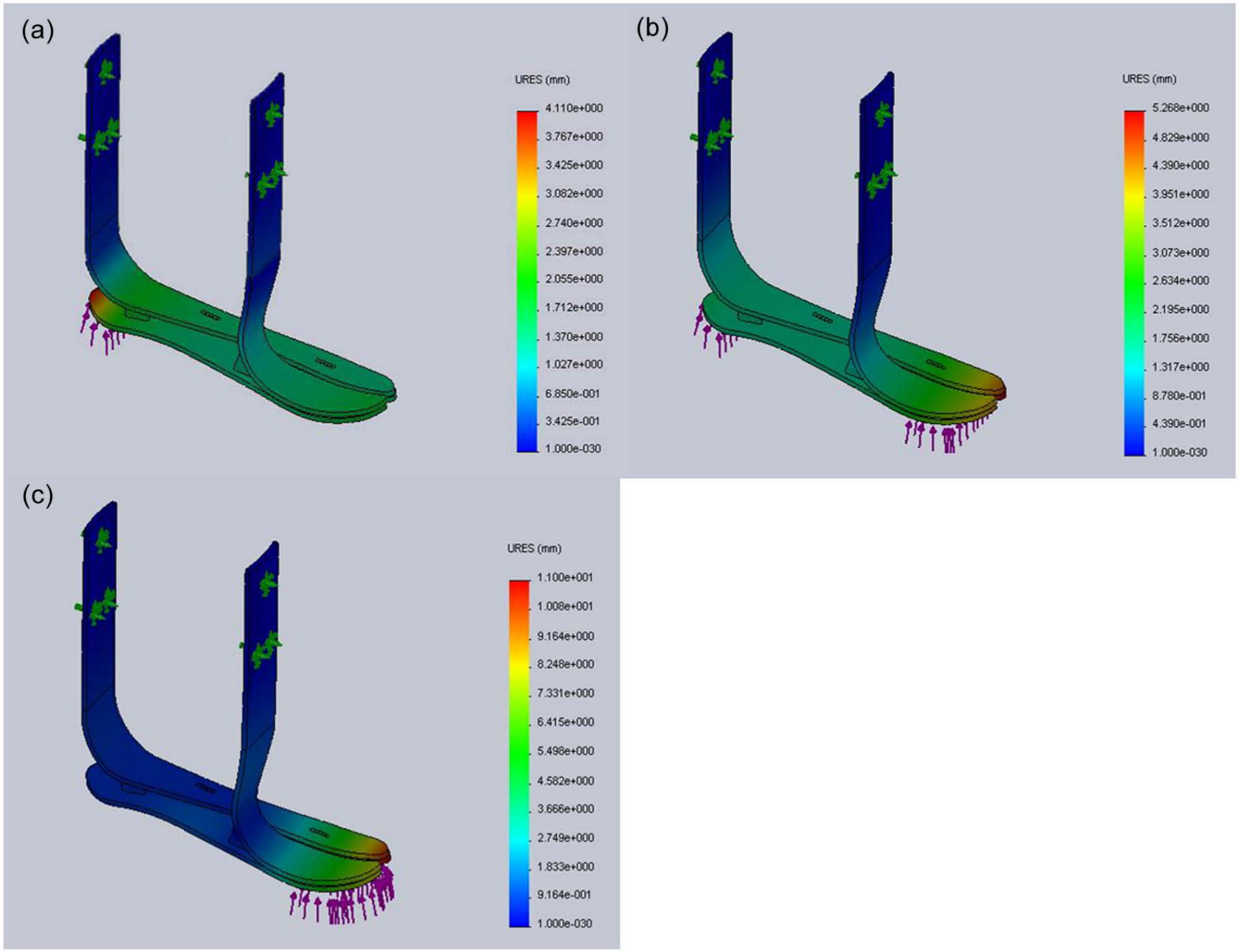
Deformation of the new prosthetic foot (loaded with 1000 N; 1.2× body weight) using finite element analyses. (a) Deformation pattern during heel-strike, (b) deformation pattern during mid-stance (with an equally distributed body weight), and (c) deformation pattern during toe-off. Thin arrows represent applied force, fat arrows with multiple arrowheads represent fixation points.
Gait analysis
All gait parameters of our case subject wearing the new prosthetic foot were compared with the standard LR foot. Mean data of our reference group were only used as a validation of our case subject using the LR foot.
The SSWS of our case subject using the LR foot was below the mean of the reference group, while the AFAP velocity was within the standard deviation (SD) of the reference group. More than 5% deviation was seen in 47% of the treadmill parameters between the mean reference data and the case subject using the LR foot (data not shown). GRF data (Tables 3 and 4) using the LR foot were within the SD of the reference group, except for the maximal anterior GRF, which was lower.
Spatiotemporal gait parameters: treadmill measurement results of the LR versus the new prosthetic foot.
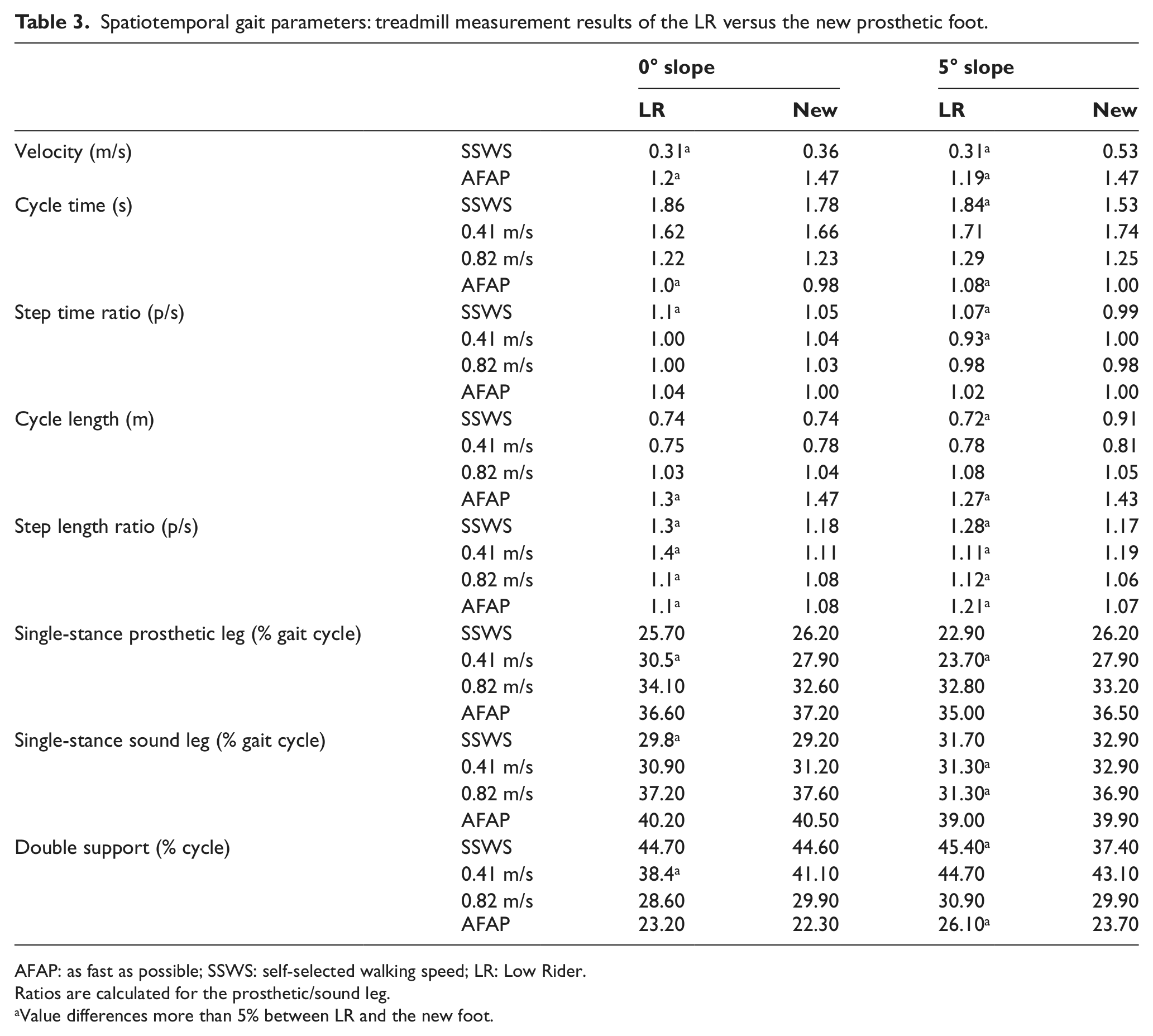
AFAP: as fast as possible; SSWS: self-selected walking speed; LR: Low Rider.
Ratios are calculated for the prosthetic/sound leg.
Value differences more than 5% between LR and the new foot.
Spatiotemporal gait parameters: GRF measurement results of the reference group versus the case subject wearing both prosthetic feet.
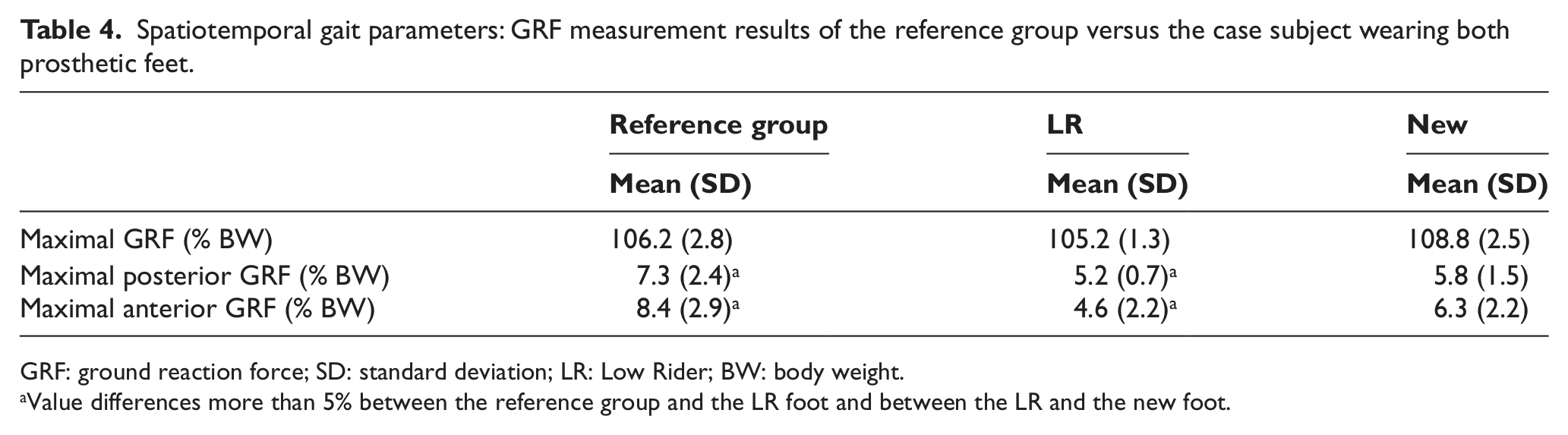
GRF: ground reaction force; SD: standard deviation; LR: Low Rider; BW: body weight.
Value differences more than 5% between the reference group and the LR foot and between the LR and the new foot.
The SSWS of the case subject using the new foot was also lower than that of the reference group on a 0° and 5° slope (Tables 3 and 4). However, the maximal speed of the reference group was higher than the case subject using the LR, but lower than the maximal speed of the case subject wearing the new prosthetic foot, both for the 0° slope and 5° slope.
Step length ratio (prosthetic/sound) for the new foot, for all speeds at both 0° and 5° slopes, indicate an improved symmetry compared to the LR, although not all reach the 5% borderline. Step time ratios (prosthetic/sound) at 0° and 5° slopes at SSWS and AFAP were also closer to 1 for the new foot, where three out of four reached the 5% deviation borderline. The single stance time of the prosthetic and the sound leg were also all higher for the new prosthetic foot compared to the LR, but not all reach the 5% limit. Arising from this, the double support time using the new foot is for all conditions lower than for the LR foot. However, not all reach the 5% borderline. Maximum GRF values (Table 4) of the new prosthetic foot compared to the LR were all higher, but the maximal GRF difference did not reach the 5% borderline.
Questionnaire
The mean data of the reference group were compared with the different outcomes in the case study (data not shown). The scores of the case study using the LR were all within the SD of the reference study, except for five scenarios, which all scored lower: standing still, standing and walking on an uphill slope, shock absorption, and jumping off a stair tread. The mean overall score of the reference study was 6.5 (SD = 2.4) with a mean score for all questions of 6.4 (SD = 1.8). The LR foot was given an overall score of 6 with a mean score for all questions of 5.3 (SD = 1.9) where the new foot scored 7 and 5.4 (SD = 1.4), respectively.
The category stability while walking had an insufficient mean score for the reference group, where the rest had a mean borderline sufficient score. Within the case study, in eleven scenarios, the score remained the same for both feet, and in ten scenarios the new foot scored better than the LR. For seven scenarios, the new foot was given a lower score than the LR.
Five scenarios, walking on even underground, driving a car, cycling, appearance, and stepping on the sidewalk, scored above 7.5 in the reference group. The scores of the LR versus the new prosthetic foot were equal in the first three scenarios. Appearance scored better for the new foot, but stepping onto the sidewalk scored less for the new foot, but still sufficient.
Of all scenarios, which scored insufficient in the reference group, five scenarios stayed the same comparing the LR with the new foot. Other scenarios with an insufficient reference score scored better for the new foot compared to the LR: standing still and walking on upward slope, walking on uneven surfaces, powerful push off, and jumping of a stair, scored better for the new foot compared to the LR. For standing still (sideways) on a downward slope, a lower score was given to the new foot compared to the LR foot.
Discussion
The aim of this study was to design a prosthetic foot with low installation height uniquely combined with functional qualities like shock absorption, ankle mobility, energy storage and return during normal cause of locomotion and a smooth roll-off moment. And, by doing so, to reach the ultimate goal for Syme and Pirogoff patients in obtaining a more natural walking pattern, regain stability and increased walking speed (and thus reduced energy consumption). The gait analysis showed improved SSWS and AFAP walking speed and an improved symmetric walking pattern for all speeds, both on 0° and 5° slopes while using the new prosthetic foot. Although this was tested on one patient under controlled conditions and more research is needed, these results are promising. The questionnaire outcomes also showed improvement using the new prosthetic foot comparing to the LR foot.
Gait parameters are generally tested on the treadmill or during overground walking. Here, the GRF-plate measurements were done during overground walking for logistic reasons and device accuracy. Overground walking, however, is proven to differ under different terrains and surroundings. 26 GRF data of our reference group corresponded with the literature. 9 The other gait parameters were obtained using a treadmill due to its advantages of using a standard protocol and the possibility of multiple steady speed selection in combination with a slope. This could be a limitation of the study; however, literature is inconsistent about the effect of walking on a treadmill. There are reports that it overestimates the SSWS 27 and increases cadence.28,29 In other cases, no significant effect is found, considering healthy subjects30,31 as well as amputees. 32
The results of this case study show that the new prosthetic foot could be an improvement for those patients with high residual limb length. Although the case subject using the LR foot was not completely representative for the reference group, which could be due to his age, the velocity differences between the new and the LR foot are clear. The SSWS and AFAP velocities are important parameters reflecting the effort needed while walking. The SSWS is automatically chosen by people (healthy as well as amputees) and corresponds with the optimal bio-energetic efficiency level.33,34 The maximum velocity measured is useful to detect the capability of the amputee and is also a measure for the energy-efficiency of walking. Amputees modify their walking speed for different situations, in order to keep relative energy costs within normal limits. 34 The authors hypothesize that the higher velocities using the new prosthetic foot could suggest that this foot is a functional energy storage and returning prosthesis, and that it partly compensates for the loss of the plantar flexors. However, to check this hypothesis, mechanical tests of the device are needed.
On day 1, the case subject was able to walk at a speed of 0.33 m/s, while using the new prosthetic foot. After 1 week of practice, this value increased up to 1.47 m/s and a higher SSWS (on both 0° and 5° slopes) was measured (16% and 71% respectively). The AFAP velocity after 1 week was 15% higher on level ground and 24% higher on a 5° slope. The difference between days 1 and 8 can be attributed to familiarisation and rise in confidence. Amputees are known for their high adaptability and become accustomed to a specific “feeling” and “function” of a prosthetic foot. 35 Therefore, a longer familiarisation time might result in even better gait parameters.
Gait parameters of the new prosthetic foot on the slope show the most improvement, probably due to the more flexible characteristics of the new foot compared to the LR. Slope measurements at different speeds were done because it is known that walking on a slope is distinctive for the adjustability of the amputee. 36
Comparison of both legs give useful information about whether the two prosthetic feet induce more or less compensatory behavior of the sound leg, and therefore, gait parameter ratios between the prosthetic and sound leg are a clear way to compare prosthetic feet functionality. 35 The majority of the step length and time ratios of the new prosthetic foot are closer to “1” than the LR foot, indicating a more symmetrical walking pattern. In addition, the higher single stance time of both legs, the lower double support time, and the higher maximal GRF while using the new foot compared to the LR foot suggest higher confidence whilst walking. Although part of this can also be attributed to the higher walking speed.
For some volunteers, a higher velocity was measured while walking on a 5° slope than on level ground, where the opposite was to be expected due to higher energy consumption while walking uphill. 37 This could be explained by the fact that more instability and therefore insecurity is present under these conditions. And, as some volunteers remarked, the solution to get more stability is by walking faster, which is confirmed by Hermodsson et al. 9
Questionnaire outcomes also suggest improvements are made with the new prosthetic foot. However, during the case study measurements and questionnaires, it was not possible to blind the case subject for the type of foot he was wearing. This could also have affected the questionnaire results in a negative way because the “feeling” and “function” of a prosthetic foot affects the amputee’s subjective evaluation. 35
Although the results of this study suggest walking improvement using the new foot, there are some limitations. Information about the response (energy storage and return characteristics) to specific impact loadings and long-term fatigue characteristics have not yet been assessed.
Another point to be taken into consideration is that measurements were all taken barefoot. This was chosen to obtain comparable data between all types of prosthetic feet used and more importantly, to get a better view of the new foot characteristics. This could be a reason for the lower mean walking speeds. Due to logistic reasons, it was not feasible to measure all volunteers using the same kind of footwear. Measuring volunteers using different kind of shoes would not give proper results because shoe properties have a great influence on feet and walking characteristics. 22
Finally, optimizing the design is necessary with respect to the fixation and alignment method of the foot to the socket. Stiffness has been shown to influence the gait parameters of a prosthetic as well as the sound leg to a large degree. 15 That is why stiffness characteristics of the foot at specific areas should be investigated further to design an optimally performing prosthetic foot. Mechanical behavior tests during the gait cycle, material fatigue properties, and energy costs measurements should be done to be able to fully investigate and optimize the characteristics of this new design. Future work should also be directed toward a larger research group to allow for statistical evaluation, and the effect of shoes should be investigated.
Conclusion
The case study shows that this new prosthetic foot could be an improvement to the prosthetics available today with extreme low installation height. This energy returning prosthetic foot enables a faster walking speed on level ground as well as uphill. In addition, a more symmetric walking pattern results using this new device. Optimizing the design, however, is necessary with respect to the fixation and alignment method of the foot to the socket and the stiffness of the foot at specific areas, and material fatigue properties should be investigated. Future work should also be directed toward a larger population, kinetics and kinematics, and energy cost measurements.
Footnotes
Acknowledgements
The authors would like to thank Marcel Conradi of the Orthopedic Technology Department De Hoogstraat for making measurements possible. Orthotic technicians Ronald van der Meer and Jaswant Koendjbiharie for their time, help, and useful input during the design process. Also thanks to Gert Jan Nevenzel, Theo Pünt and Frank de Klein for helping to manufacture the first prototype.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.