
Abstract
Background:
Prosthetic foot prescription guidelines lack scientific evidence and are concurrent with an amputee’s concurrent with an amputee’s Medicare Functional Classification Level (K-Level) and categorization of prosthetic feet.
Objective:
To evaluate the influence of gait training and four categories of prosthetic feet (K1, K2, K3, and microprocessor ankle/foot) on Symmetry in External Work for K-Level-2 and K-Level-3 unilateral transtibial amputees.
Design:
Randomized repeated-measures trial.
Methods:
Five K-Level-2 and five K-Level-3 subjects were tested in their existing prosthesis during Session 1 and again in Session 2, following 2 weeks of standardized gait training. In Sessions 3–6, subjects were tested using a study socket and one of four randomized test feet. There was an accommodation period of 10–14 days with each foot. Symmetry in External Work for positive and negative work was calculated at each session to determine symmetry of gait dynamics between limbs at self-selected walking speeds.
Results:
K-Level-2 subjects had significantly higher negative work symmetry with the K3 foot, compared to K1/K2 feet. For both subject groups, gait training had a greater impact on positive work symmetry than test feet.
Conclusion:
Higher work symmetry is possible for K-Level-2 amputees who are trained to take advantage of K3 prosthetic feet designs. There exists a need for an objective determinant for categorizing and prescribing prosthetic feet.
Clinical relevance
Findings that gait training can influence symmetry of gait dynamics and that K-Level-2 amputees can achieve greater work symmetry with a K3 foot having a “J-shaped” ankle and heel-to-toe footplate could potentially impact prosthetic care and foot prescription by clinicians and reimbursement guidelines by third-party health-care payers.
Introduction
In the United States, the Medicare Functional Classification Level (MFCL) classifies unilateral lower limb amputees into one of five functional levels (K-Level-0 through K-Level-4) based on their potential to ambulate with a prosthesis (Table 1). 1 Subsequent to recommendations by manufacturer representatives and invited advisors, the Centers for Medicare and Medicaid Services committee assigned prosthetic feet to a specific MFCL K-Level (categories K1–K4 feet) primarily based on their mechanical properties (Table 1). 2 Prescription and reimbursement of a prosthetic foot are concurrent with an amputee’s functional level and the prosthetic foot’s K-Level categorization. While mechanical properties of prosthetic feet have been quantified by independent organizations, 3 functional differences between the various categories of prosthetic feet, in amputees with dissimilar K-Levels, have not been evaluated.
DMERC prosthetic policy definition of foot/ankle assemblies by MFCL.
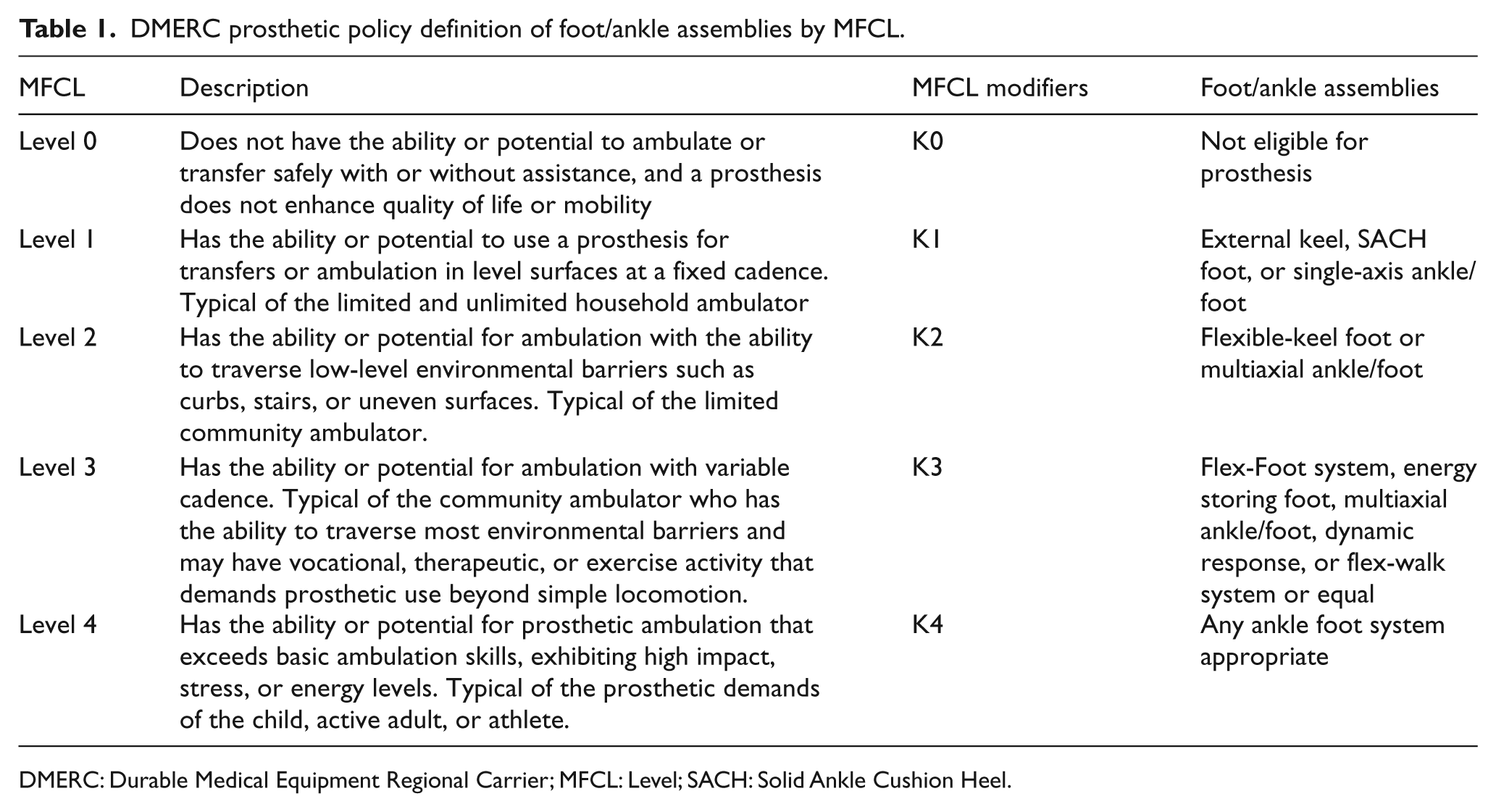
DMERC: Durable Medical Equipment Regional Carrier; MFCL: Level; SACH: Solid Ankle Cushion Heel.
Numerous comparative effectiveness research studies on prosthetic feet have failed to consistently demonstrate functional differences between prosthetic feet.4,5 These results have been attributed to confounding variables, such as socket fit, differences in functional levels among subjects, and selection of the appropriate measurement tool. 6 Traditional methods of gait analysis typically assess temporal, spatial, kinetic, and kinematic variables at discreet points during a gait cycle. 7 On the contrary, the Symmetry in External Work (SEW) measure incorporates the property of integration, which allows force, time, and center of mass (CoM) displacement over a step to be combined into a single value. 8 By definition, changes in the potential or kinetic energy of the body result in work, with positive and negative work resulting from an increase and decrease in CoM energy, respectively. While internal work is primarily done by the muscles, external work is the result of ground reaction forces (GRFs) and the subsequent displacement of the CoM during the stance period. The SEW measure thus calculates the changes in energy of CoM with the intact limb and the prosthetic limb, and determines the index of symmetry. This measure has been proposed as a clinical tool to detect symmetry in gait dynamics unilateral transtibial amputees (TTAs) and has the ability to differentiate between prosthetic feet. 8 Even though the use of symmetry for assessing unilateral TTA gait has been debated, 9 increased forces resulting from asymmetrical movement have been theorized to contribute to degenerative joint diseases in the intact limb. 10 Application of interlimb symmetry measures (e.g. SEW) for comparing prosthetic feet has the advantage of providing a common measurable outcome for each amputee subject, which eliminates the task of comparing numerous gait deviations that may arise between amputee subjects.
Clinical studies comparing prosthetic feet have not classified test subjects using the MFCL scale, and a crossover study between various categories of prosthetic feet and subjects with different K-Levels has not been reported. Furthermore, since the majority of published studies did not provide standardized gait training to participants, gait deviations resulting from habit or lack of training may have influenced measured parameters. The purpose of this study was to determine the functional contribution of four prosthetic feet in promoting external work symmetry in MFCL K-Level-2 and K-Level-3 unilateral TTAs, while minimizing confounding variables that influence gait. The “functional contribution” of prosthetic feet, for the purposes of this study, is defined as the restoration of symmetry between lower limbs during level walking. This study has implications for prosthetic feet prescription and reimbursement, as it has not been objectively determined whether K-Level-2 amputees would benefit from a category K3 foot.
Methods
Fifty-five unilateral TTAs were screened using the following inclusion criteria:
Males and/or females, 40–65 years old;
Amputations resulting from diabetes mellitus, peripheral vascular disease (PVD), traumatic events, or cancer;
Ability to use a prosthesis for ambulation on level surfaces, with a consistent cadence, for a minimum distance of 200 m;
Comfortable fit of current prosthesis for a minimum period of 6 months;
Ability to tolerate the study protocol without fatigue during testing.
The exclusion criteria were as follows:
Body weight more than 115 kg (255 lb);
Wound or partial foot amputation on the intact limb;
Poor control of diabetes and/or neuropathy of the intact foot;
Neurological disorders, for example, paralysis, or orthopedic conditions, for example, joint contractures that would affect gait;
Moderate to severe lower limb arthritis;
Cardiac or pulmonary disease limiting their ability to exercise;
Problems with prosthetic fit or the residual limb, such as open wounds and blisters, which would cause pain during the testing procedure.
This study protocol was reviewed and approved by the Miami VA Medical Center’s Institutional Review Board and informed written consent was obtained from all subjects prior to study enrollment. Each subject was evaluated by a physician for his or her current and past medical conditions, which included a foot examination, neuropathic assessment, vascular assessment, foot ulceration history, and a neuropathy symptom score. The subjects’ residual limb and prosthesis were inspected by a prosthetist for any limitations that would cause pain, prohibit prosthetic wear, or put them at risk throughout the course of this study. Upon physician and prosthetist clearance, subjects started the experimental procedure. This study was conducted in two phases—reliability study and intervention study.
Reliability study
Test–retest reliability of F-scan sensors (Tekscan Inc., Boston, USA) was determined for the anatomical and prosthetic feet in five unilateral TTAs, as sensor reliability has not been established for this population. Data collection and calibration of F-scan sensors were performed by the same team of researchers using previously validated procedures.11,12 During each session, a new sensor was trimmed to match the subject’s shoe size, such that it was not wrinkled when placed inside the shoe. Before the calibration process, sensor warm-up was performed for about 10 min. 11 In addition to the manufacturer-recommended calibration, a force plate calibration was also performed using two Kistler force plates embedded in a 10-m-long level walkway. Vertical GRFs from force plates and F-scan sensors were collected at 50 Hz and were compared to calculate a calibration factor for F-scan sensors, as described by Mueller and Strube. 12 Subjects were tested twice within a period of 48–72 h using standardized shoes (Aetrex Ambulator, type T1220, Aetrex Worldwide Inc., Teaneck, NJ, USA) and socks. Intraclass correlation coefficient (ICC) was used to determine the correlation between test–retest SEW values. 13
Intervention study
A convenience sample of 10 TTA subjects was equally divided into K-Level-2 and K-Level-3 subjects according to their Amputee Mobility Predictor (AMP) score. 14 All K-Level-2 subjects coincidently lost their limb from dysvascular disease, whereas all K-Level-3 subjects required amputation for nondysvascular reasons. A three-dimensional (3D) image of the subject’s residual limb was obtained using the BioSculptor software (Maramed Inc., Miramar, FL, USA), which was modified by the study prosthetist and used to fabricate a total-surface bearing prosthetic socket. All subjects had a suction suspension mechanism with a Seal-In® Liner. Because of fitting issues in one subject, a standard silicone cushion liner and an external sleeve were used. The study socket was used to test four prosthetic feet, that is, Solid Ankle Cushion Heel (SACH; Kingsley Manufacturing Co., Costa Mesa, CA, USA), Stationary Attachment Flexible Endoskeleton (SAFE; Campbell-Childs Inc., White City, OR, USA), Talux (Ossur hf, Reykjavik, Iceland), and Proprio Foot (Ossur hf, Reykjavik, Iceland). The four prosthetic feet chosen were selected to represent each category; 2 K1—the SACH foot identified by name in the Durable Medical Equipment Regional Carrier (DMERC) prosthetic policy definition of foot/ankle assemblies, K2—the SAFE Foot—a truly flexible keel foot, and the Talux as the K3 foot because it is a Flex-Foot with J-shaped dynamic response design (also named by DMERC) combined with multiaxial capabilities because of the elastomer block ankle. The Proprio Foot, a K3 device, was included as a microprocessor-controlled ankle (MPA) that operates similar to traditional prosthetic foot during stance but provides active dorsiflexion during swing for greater toe clearance. All socket fittings and prosthetic alignment were performed by the same study prosthetist.
Each subject underwent six different testing sessions. At each session, GRF data were collected with the force plates and F-scan sensors using the above-mentioned procedure. During Session 1 (baseline session), subjects were tested in their existing prosthetic socket and foot. They then received up to 4 h of standardized prosthetic gait training over a period of 14 days. Session 2 (training session) thus measured the effects of training on subject gait in his or her existing socket and foot. Subjects were then fit with the study socket and randomly assigned to one of the test feet. They had an accommodation period of 10–14 days with the prosthetic foot and were given 1–4 h of gait training. To date, no evidence exists in the literature with respect to the duration of time required for an amputee to accommodate to a prosthesis. Best clinical judgment estimates that a period of about 2 weeks is sufficient time for a lower limb amputee who is at least 6 months post amputation, is medically stable and has received prosthetic gait training. At testing session 3, effects of the first test foot on subjects gait were measured. Following testing, subjects were fit with the randomly selected second test foot and were given 1–4 h of gait training and an accommodation period of 10–14 days. Session 4 thus measured the effects of the second test foot on subjects’ gait. The same testing and training procedure was repeated during Sessions 5 and 6 for the third and fourth test feet, respectively.
Each subject received standardized prosthetic gait training with their existing socket and foot as well as with the study socket and test feet. The prosthetic gait training program included single-limb balance, resisted gait training for maximizing prosthetic toe load and restoring pelvic and trunk rotation, and specific exercises to promote speed of muscular contraction at the knee and hip.15,16 The objective of standardized training was to minimize gait deviations resulting from habit or lack of training and to maximize the appropriate use of each foot based on its mechanical design. At the end of a training session, subject’s gait proficiency was assessed on predefined criteria. Each subject was trained only in areas in which training was needed. Gait proficiency with the assigned test foot had to be clinically observed prior to the physical therapist concluding the subject’s training sessions. No subject required additional training beyond four sessions. All sessions were standardized and administered by the same physical therapist. Any issues with socket fit or alignment were addressed within 48 h of notification, and all prosthetic- or training-related issues were resolved during one return visit.
Data analysis
Four consecutive steps with the intact limb and the prosthetic limb were utilized for work calculations. External work due to vertical GRFs and the resultant CoM displacement was calculated using a line integral as described by Agrawal et al. 8

where W is the external work, F is the GRF, and s is the CoM displacement.
Positive and negative work—resulting from a positive and negative integrand—implied upward and downward CoM displacement, respectively. SEW between limbs was calculated for each stride using the following equation, and a mean SEW value was obtained by averaging the four strides

where WI is the work done by the intact limb (J) and WP is the work done by the prosthetic limb (J).
An SEW value of 100% indicates equal work by each limb, whereas values greater than 100% and less than 100% indicate more work by the prosthetic limb and intact limb, respectively. Baseline and Training sessions were compared using the paired t-test. A repeated-measures analysis of variance (ANOVA) was used to determine differences between the four test feet used during Sessions 3–6. For post hoc analysis, pairwise comparisons using related paired t-tests were used, and p values that were less than a critical alpha of 0.05 were considered statistically significant.
Results
Subject characteristics for the reliability and intervention studies are described in Tables 2 and 3, respectively. Table 4 shows the differences in demographics between K-Level-2 and K-Level-3 subjects.
Demographic characteristics of five test subjects used to determine test–retest reliability of the SEW measure.
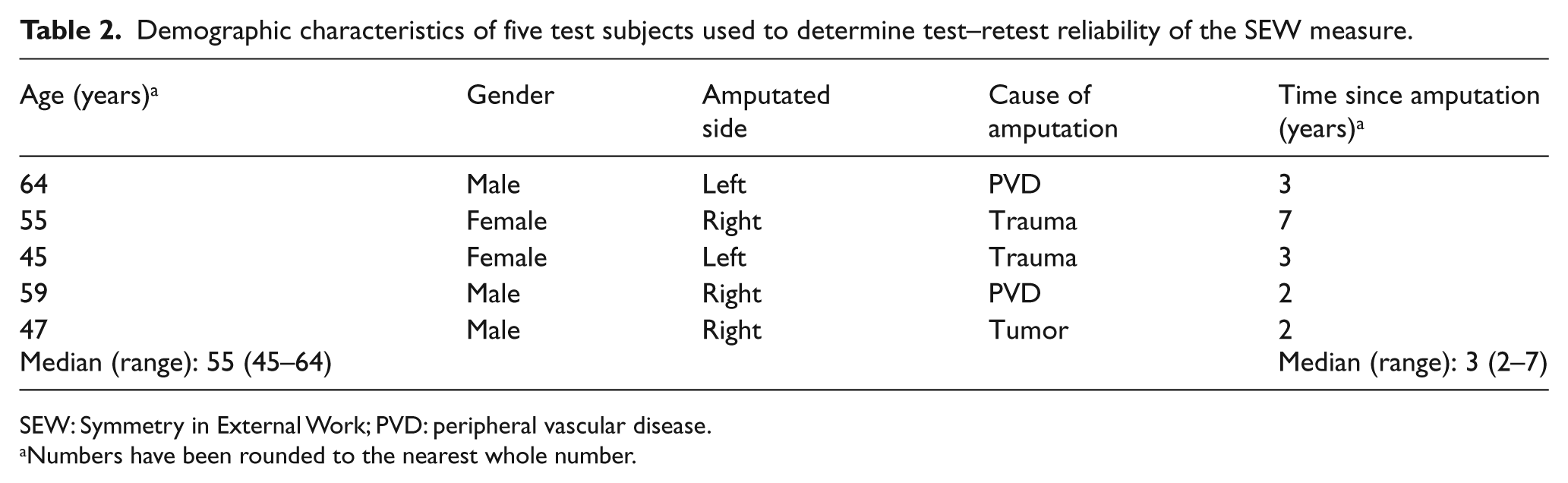
SEW: Symmetry in External Work; PVD: peripheral vascular disease.
Numbers have been rounded to the nearest whole number.
Demographic characteristics of study subjects.
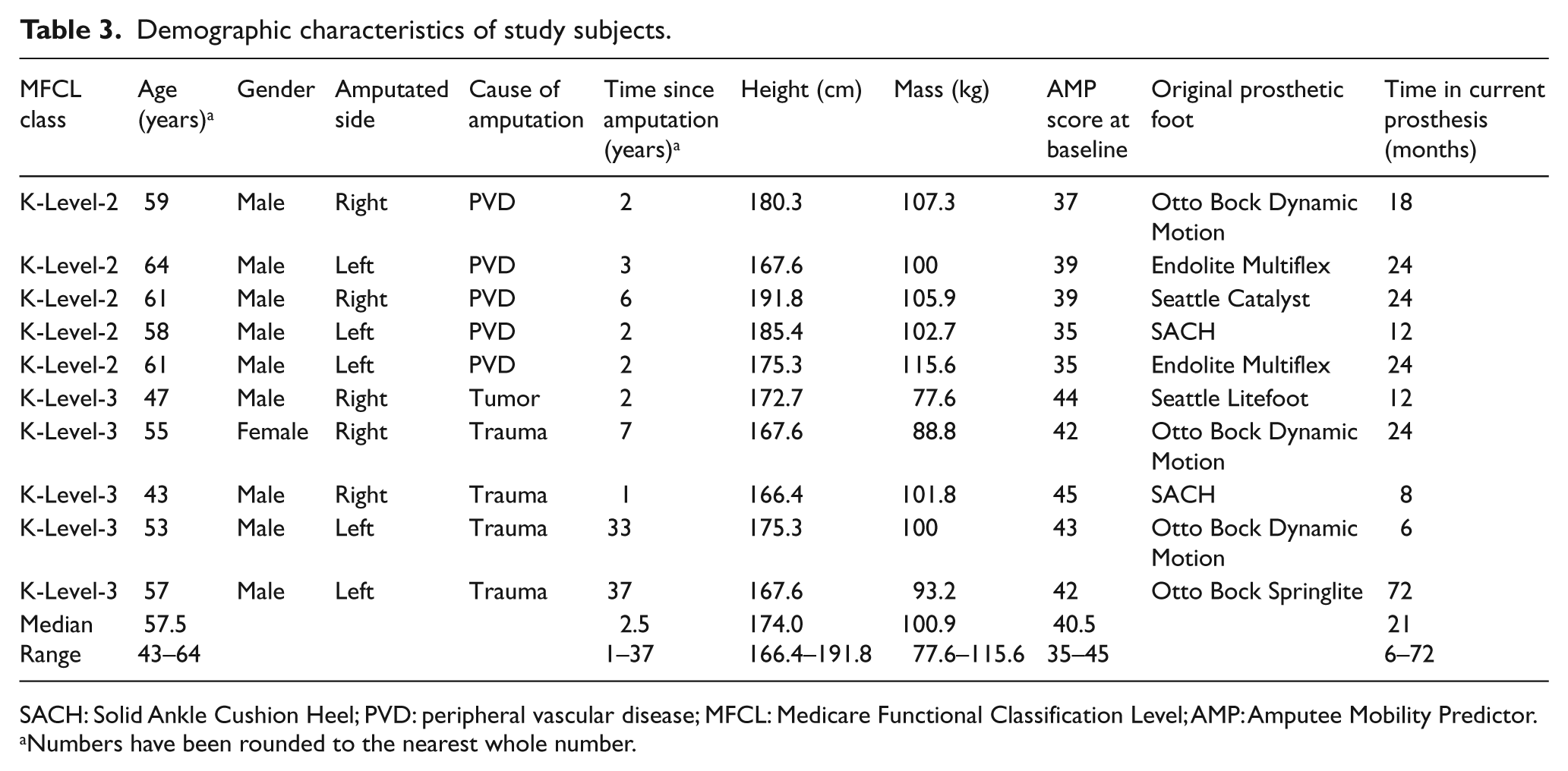
SACH: Solid Ankle Cushion Heel; PVD: peripheral vascular disease; MFCL: Medicare Functional Classification Level; AMP: Amputee Mobility Predictor.
Numbers have been rounded to the nearest whole number.
Mean ± SD of subject demographics for K-Level-2 and K-Level-3 amputees, and the differences between groups.
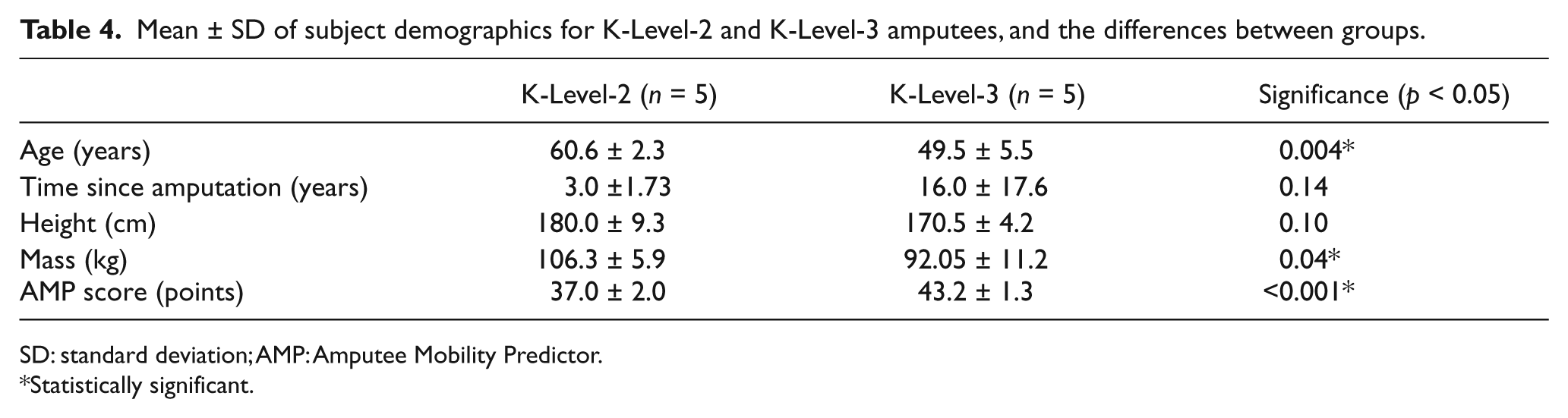
SD: standard deviation; AMP: Amputee Mobility Predictor.
Statistically significant.
Reliability study
The ICC for test and retest was found to be 0.89, which is similar to the reliability of F-scan sensors published for nonamputee walking. 12 The high ICC indicated excellent reliability of F-scan sensors with TTAs and corroborated the stability of subjects’ gait.
Intervention study
The mean (standard deviation (SD)) SEW values for positive and negative work in both subject groups are presented in Table 5. After receiving standardized gait training, positive work symmetry significantly increased over Baseline in K-Level-3 subjects (p = 0.02) and approached statistical significance in K-Level-2 subjects (p = 0.07). In K-Level-2 subjects, positive work symmetry was not significantly different between feet, while the negative work symmetry of the K3 foot was significantly better than the K1 and K2 feet. In K-Level-3 subjects, neither positive nor negative work SEW values were significantly different between feet; however, the difference between K3 and K1 foot approached statistical significance (p = 0.08).
Mean (SD) SEW value, in percentage, for positive and negative work of K-Level-2 and K-Level-3 amputee subjects.
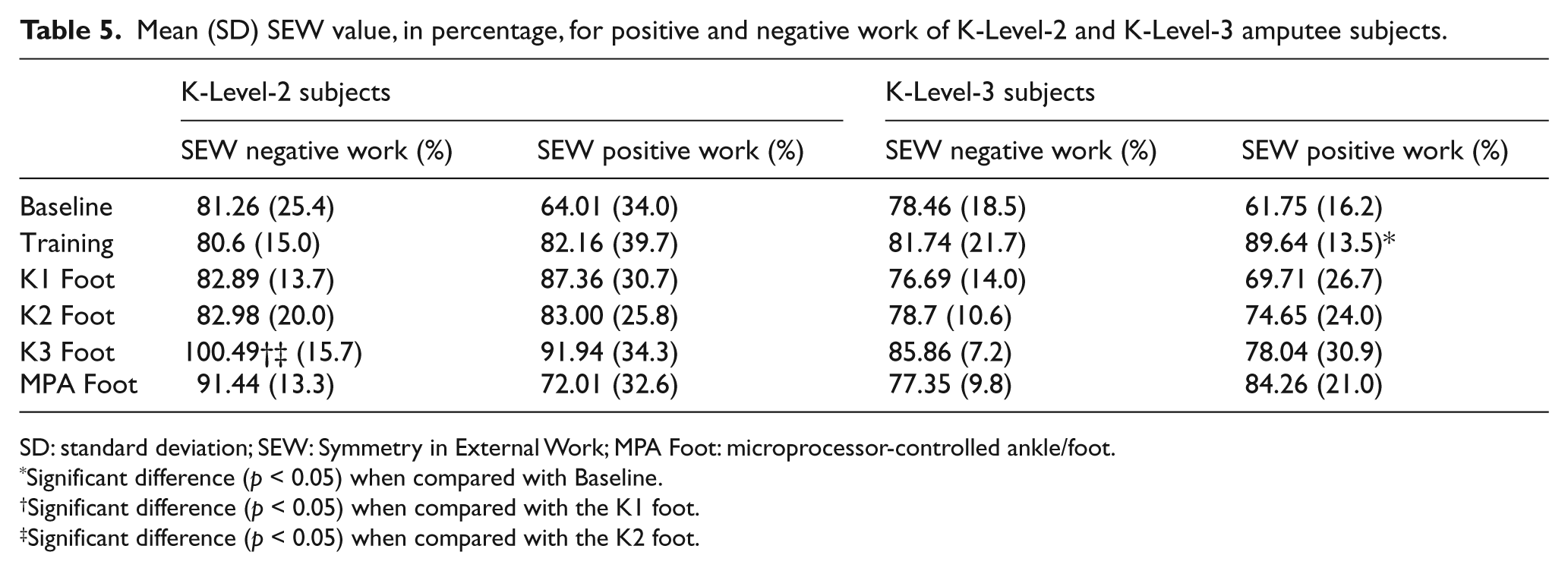
SD: standard deviation; SEW: Symmetry in External Work; MPA Foot: microprocessor-controlled ankle/foot.
Significant difference (p < 0.05) when compared with Baseline.
Significant difference (p < 0.05) when compared with the K1 foot.
Significant difference (p < 0.05) when compared with the K2 foot.
Discussion
The gait deviations typically associated with unilateral TTA gait can be attributed to either prosthesis-related variables or amputee-specific factors. The research methodology of this study was designed to limit the influence of confounding variables on outcome measures. The gait variability arising from demographic characteristics, such as age and comorbidities, was addressed by identifying strict inclusion criteria. Prosthesis-related confounding variables were controlled for by providing a new standardized socket with one of the two similar suspension mechanisms, fabricated by the same board-certified prosthetist. Standardized prosthetic gait training was employed to reduce gait deviations related to habit or lack of training and the accommodation period served to familiarize subjects with the properties of the foot. Every effort was thus made to ensure that any observable gait variations would be attributable to differences in design of test feet and not to other controllable variables.
During gait, negative work is the result of downward CoM displacement, which occurs during weight acceptance and late stance phases of gait. In both subject groups, negative work symmetry index with the K3 foot was higher than the K1/K2 feet. The high SEW values for negative work observed with the K3 foot can be attributed to its “J”-shaped ankle spring and its heel-to-toe footplate design. Deflection of the “J”-shaped ankle spring during mid-stance to late stance phases of gait simulated ankle dorsiflexion by facilitating forward tibial progression.17,18 The heel-to-toe footplate allowed subjects to balance on the prosthetic forefoot during terminal stance.19,20 As a result, subjects were able to lower the CoM in a controlled manner and systematically transfer weight to the intact limb. Higher negative work by the prosthetic limb during late stance and lower work by the intact limb during weight acceptance thus resulted in high negative work symmetry.
K1 and K2 feet have relatively shorter keels, a flexible forefoot, and rigid ankles because of a direct attachment between the pylon and foot. These design features limited the forward tibial progression during the stance phase, resulting in early “drop-off” as amputees progressed over the prosthetic foot and a sudden transfer of weight to the intact limb. Lower negative work by the prosthetic limb during late stance and higher work by the intact limb during weight acceptance thus resulted in low negative work SEW values for both K-Level-2 and K-Level-3 subject groups. In a recent study, Morgenroth et al. 21 reported similar results, in which conventional prosthetic feet resulted in higher loading impulses and external knee adduction moments at the intact limb. The MPA foot did not perform significantly better than any of the test feet in either the K-Level-2 or K-Level-3 subject groups. This result can be attributed to its ankle design that has active dorsiflexion during the swing phase but supports limited dorsiflexion during the stance phase, thus constraining the forward tibial progression. The heel-to-toe footplate of the MPA foot appeared to promote greater negative work symmetry in K-Level-2 amputees compared to the shorter keels of K1 and K2 feet.
Upward CoM displacement during gait results in positive work. There were no significant differences in positive work symmetry between prosthetic feet, and gait training was the most important contributor in increasing symmetry. The high SDs in K-Level-2 subjects may have resulted from variability in walking strategies despite gait training, sample size, and differences between prosthetic feet. Tesio et al. 22 reported that in TTAs, the power generated by the prosthetic limb during the prosthetic-to-sound transition was much lower than that generated by the sound limb during the sound-to-prosthetic transition. Results of this study corroborate their findings and demonstrate that the positive work is not influenced by the type of prosthetic foot used. In the absence of active power generation at the ankle and because of the interchange between hip and ankle kinetics,23,24 the residual limb musculature appears to be instrumental in promoting positive work symmetry. The standardized gait training program used in this study may have facilitated increased use of residual limb musculature resulting in a significant increase in symmetry for K-Level-3 subjects. Although no significant differences were detected after training in the K-Level-2 group, observed trends suggest that in the absence of obtaining a new prosthetic foot, standardized prosthetic training may be of benefit to some unilateral TTA populations.
Our findings conclude that the “J”-shaped ankle and heel-to-toe footplate design characteristics of the K3 foot (Talux) result in the greatest symmetry of work for K-Level-2 amputees followed by K-Level-3 amputees. There were significant differences in age and function between the K-Level-2 and K-Level-3 subject groups in this study (Table 4). As prescription of a prosthetic foot is concurrent with an amputees’ functional level and the prosthetic foot’s K-Level categorization, these results question the relevance of the current categorization of prosthetic feet and their subsequent prescription to the amputee. The descriptors for each MFCL appear to be appropriate since multiple functional outcome instruments have established significant differences between the five K-Levels. 4 To date, the appropriateness of the categorization of prosthetic foot assignment has not been established. If symmetry of work between lower limbs is one of the clinical goals with regard to the prescription of the prosthetic foot, this study suggests that there exists a need for an objective determinant for prescribing prosthetic feet and categorizing feet with respect to their functional contribution to amputees within each K-Level.
The number of participants in each K-Level (n = 5) can be considered a limitation of this study. The costs for prosthetic feet, socket fitting, gait training, the total time commitment by subjects, and the strict inclusion criteria were limiting factors for subject recruitment. Ideally, in addition to increased number of subjects, a greater demographic representation, including vascular and nonvascular, different levels of amputation, and gender and age, would be warranted. As calculation of SEW values utilizes only vertical GRFs, future work may include measuring the effects of shear forces on the intact foot and resulting work values. Although the magnitude of anterior–posterior and medial–lateral GRFs is lower than vertical GRFs, 25 altered shear stresses and the resulting work asymmetry during gait may increase the risk of plantar ulceration in unilateral K-Level-2 TTAs with diabetic neuropathy in the anatomical foot.26,27 The absence of motion capture data restricted our ability to determine the relationship between joint kinematics, which limited the discussion to clinical observation and findings published in the literature.
Conclusion
A combination of standardized gait training and appropriate prosthetic foot can promote higher external work symmetry in K-Level-2 and K-Level-3 unilateral TTAs. K-Level-2 amputees can achieve greater work symmetry using K3 feet with J-shaped ankle and heel-to-toe footplate designs. In the absence of advanced prosthetic componentry, gait training could improve interlimb symmetry in some unilateral TTAs. Because of the disparity between assigned amputee K-Levels and prosthetic foot categorization, there exists a need for an objective determinant for prescribing prosthetic feet and categorizing feet with respect to their functional contribution to amputees.
Footnotes
Conflict of interest
None declared.
Funding
This material was based on work supported in part by Ossur Americas. The research project was administered through the Miami VA Healthcare System and the South Florida VA Foundation for Research and Education.