
Abstract
Background:
While the positive effect of sports and exercise on physical and psychological well being is well documented within the general population, the effects of sports on the functional ability of a child with mental retardation are limited.
Objectives:
To determine if sports activities have been detrimental in improving functional ability in sample of children with mental retardation based in Kolkata, a metropolis in India.
Study Design:
Field level study.
Methods:
Six sports associations registered under the Sports Authority of India for training children with mental retardation were shortlisted on the basis of four criteria. From the register, every third name (gender irrespective) belonging to the second (12–15 years) and third (15–21 years) subclasses (out of the four categories laid down in the Special Olympics participation rules) against a constraint of at least two years active attendance in the sports facility for the child was selected. A sample of 31 children was drawn and the WHO Disability Assessment Schedule 2.0 (WHODAS 2.0) 12-item version was administered to the caregiver-teacher-coach team of the sample. Relative changes in scores between the point when the survey was conducted and the point when the child joined the sports facility was used as the dependent variable for regression analysis. The number of years in active sports, in school age of the respondent and base score of the children when they joined school were the independent variables.
Results:
For seven of the WHODAS 2.0 12-item attributes, the number of years in sports activities was found to have a statistically significant effect (p < 0.01) on the functional well being of children with mild to moderate mental retardation. The number of years in school was also another statistically significant factor (p < 0.01) responsible for this improvement. The children, however, perceived of being not welcome in community activities, but participated in activities meant exclusively for them.
Conclusions:
This small study showed that the proposition that number of years in sports activities was a significant factor responsible for improving the functioning of children with mild to moderate mental retardation.
Clinical relevance
WHODAS 2.0 12-item version has been a useful tool to monitor the effect of intervention (sports activity in this case) on the functional abilities of children with mild to moderate mental retardation. From a developing nation perspective with people with disabilities having very limited access to rehabilitation, this study would find its clinical relevance in the use of sports as an inexpensive and indigenous rehabilitative measure to promote the health and well being of people with disabilities as proposed in community-based rehabilitation guidelines (2010).
Keywords
Background
Modern education scholars are propagating inclusive education when students with disabilities learn, participate and interact together with normal children in the same classroom. It is a healthy scenario towards ‘equality in opportunity, full and effective participation and inclusion in society’. 1 Society however, is indecisive on the concept of inclusive education. For example, a study 2 found parents ‘supportive of or resistive to’ inclusive education. While some appeared to be in favour of an inclusive education, and this was based on the fact that the special child would learn more in a general education classroom. In contrast, parents who opposed considered their child’s disability was too severe to gain any benefit from inclusive education. 3
The history of education suggests that Western authors such as Rousseau and Socrates and Indian educationalists, Swami Vivekananda and Tagore, consider the importance of co-curricular activities towards complete education and upbringing of a child. While there is an expectation that children with disabilities are to participate in co-curricular activities as well to enhance their quality of living, some communities continue to have a tendency to exclude children with disability both from inclusive education and from extra-curricular tasks. Furthermore, a child with disability has a tendency to present with ‘poor coordination’, which in turn presents challenges for them to be physically active and compete with non-disabled counterparts in life. Current research suggests that most children with mental retardation ‘are taught in special class settings with minimal integration’ both in curricular and co-curricular activities. 4
The Paralympics and Special Olympics stand as an elite sports competition for people with physical and intellectual retardation to prove their determination and talent in the fields of co-curricular activities. Like other international sports meetings for the disabled, the London 2012 Paralympics is prepared to act as a platform to emphasize participant’s athletic achievements despite their disability. Intellectually, it provides a forum to discuss multidisciplinary approaches towards creating a Paralympian. Analysis of motion and force patterns within sport aimed at improving functional ability and performance of a participant is an important feature within prosthetics and orthotics research. However, the symbiotic relationship between sport and functional ability from a different causal effect perspective can provide a foundational understanding by identifying which sports have been influential or detrimental in improving functional ability of a child with mental retardation. By establishing information based on personal improvement and mapping of functional abilities provides a platform for ancillary intellectual benefits and help in designing policy prescriptions.
The overall Indian disability scenario
The Indian Census (2001) reports disability to be 2.13% on a total population of 1.08 billion and is in contrast to the World Health Organization’s (WHO’s) 2000 study that states, even by modest estimates, 10% of the population of developing nations suffer from one form of disability or other. A further and more recent report 5 estimates people with disability to comprise around 4 to 8 per cent of the Indian population. By the 2001 Census, 10.33% of the disabled population in India had mental retardation and 49.53% of this population were in the 0–18 age group. The gross under-enumeration in the disability statistics has been due to a variety of factors:
The use of the traditional ‘diagnostic’ identification method by non-medical investigators
Activities of daily living indicators (ADL) are not used
From a social choice point of view, a typical respondent from a less developed country has actually learnt to strive for only what seem attainable to avoid disappointment. Thus there is an inherent reservation of the population to share information on disability with the enumerator
These, coupled with the fact that a disability is due to past sins, Karma, has alienated the disabled from the social mainstream.
Mental retardation vis-à-vis intellectual disability
Mental disorder 6 is characterized by significantly sub-average intellectual functioning (an Intelligence Quotient of approximately 70 or below) (Criterion 1) and concurrent deficits or impairments in adaptive functioning in at least two of the following skill areas such as communication, self-care, home-living, social inter-personal skills, use of community resources (Criterion 2) with onset before age 18 year (Criterion 3). However, a decade-long movement by activists with disability and advocates made the American Association on Intellectual and Developmental Disabilities (AAIDD) Committee on Terminology and Classification to rethink that intellectual disability better ‘reflects the changed construct of disability proposed by AAIDD and the WHO’ 7 than mental retardation. AAIDD, 2010 8 defined ‘intellectual disability’ to be characterized by significant limitations both in intellectual functioning and adaptive behaviour as expressed in conceptual, social and practical adaptive skills. This disability originates before age 18. Therefore, intellectual disability ‘covers the same population of individuals who were diagnosed previously with mental retardation in number, kind, level, type and duration of the disability and the need of people with this disability for individualized services and supports’ 7 As the term mental retardation is still in use in India, and has been used in its Census 2011 questionnaire, for consistency this study describes their sample as children with ‘mental retardation.’
Overview of related studies
Over the last five decades there has been a multi-pronged improvement in educational techniques for teaching children with mental retardation. In particular, teaching within an extra-traditional learning environment is one technique commonly used today. Though the label extra-traditional may have many connotations in educational terminology, it usually means providing additional therapy and training in music, sports, painting,9-11 supplementing class-room teaching. Participation in culture, arts and sports have also been identified in the community-based rehabilitation (CBR) 12 report as measures towards personal growth and development of people with disabilities. The impact of any of these additional therapies could be studied at length as an intervention towards rehabilitation of the special children. The theme of sports activity is identified here in order to determine how it has been beneficial towards better functioning of a child with disability.
Physical activity is vital for all children as exercise helps reduce the risk of developing high blood pressure, diabetes and obesity. Disabled children who are physically active have increased motor control and are more socially active. 13 They are less likely to suffer from depression as physical activity triggers a release of endorphins in the brain.14-15 However, a different group of scientists have questioned the efficacy of the hypothesis and stated that ‘the whole endorphin-runner’s-high hypothesis is the scientific version of an urban legend’ and is without a universally proven scientific evidence. 16 Other studies17-22 cite sport as an effective means of training that affect the reaction time positively for children with mild to moderate retardation. In addition, a study 23 reveals the existence of some correlation between developmental level and persistence, attention span and emotional control.
While obesity in general is an epidemic problem worldwide, it is considered a critical issue in children with disability than it is for the general population.24-25 Devising sports programs and recreational activities is an important and crucial way in assisting children who are less sedentary by controlling their weight.26-27 Achieving better physical health also helps to build up an individual’s immunities and resistance to disease. Sports activities have been proved to build stamina and strength, coordination and flexibility, which allow children with disability a greater use of joints and limbs that have been compromised by disability.28-31
Group sports have been instrumental in promoting social support, networking and developing friendship.32-33 The understanding of how teamwork contributes to the outcome of a game has fostered a feeling of mutual self-respect among peers. It will provide a foundation for social maturity and generate confidence with both cooperative and competitive styles of interaction.34-35 Leadership skills also have a chance to emerge through involvement in sports.36-37 In addition to the immediate emotional, physical and social benefits for children with disability, it deepens their sense of belonging to a community.38-40 and contributing to the vitality of a region. Previously unknown career options in physical education open up for children with disability as well as team management, sports event announcing, teaching and equipment repair 41 . CBR guidelines 12 propose to provide ‘appropriate training and resources to support people with disabilities who want to set up their own recreation and sports groups/clubs’. In summation, the guidelines enumerate the benefits of participation as follows: (a) health promotion and disease prevention, (b) skills development, (c) awareness raising, reduction of stigma and social inclusion and (d) international peace and development.
WHODAS 2.0 as a test tool for mental retardation and sports activity
The WHO Disability Assessment Schedule 2.0 (WHODAS 2.0) which is based on the theoretical structure of the International Classification of Functioning, explores the level of functioning of an individual in six life domains (provided below). To date, a number of studies have employed the WHODAS 2.0 on various populations. 42 For example, a study 43 analyzes the functional health status in adults with acquired hearing loss with hearing aid as given intervention using WHODAS 2.0. A three community diagnostic group comparative study 44 uses WHODAS 2.0, while another article 45 analyzes the impact of prosthetics and orthotics on a major limb amputated population. While the WHODAS 2.0 appears to be an important and commonly employed tool, there is no evidence that demonstrates the use of the WHODAS 2.0 to understand the impact of intervention (sports activity) on a child with mental retardation. In essence, the authors note that if sports activities are considered to have the ability to reduce the reaction time, increase and improve coordination and motor activities, it would be reflected in the functioning of the individual.
By definition, mental retardation is characterized by sub-average intellectual functioning (Criterion 1), concurrent deficits or impairments in adaptive functioning in at least two of the following skill areas like communication, self-care, home-living, social inter-personal skills, use of community resources (Criterion 2) with onset before age 18 year (Criterion 3). (Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition, Text Revision). 6 The effect of a given intervention on a child with mental retardation is expected to be reflected in (i) an improvement in his IQ score, (ii) an improvement in the basic skill areas of the child. A study 46 has indicated that physical exercise does not significantly affect the academic performance of a child with mental retardation. This current study proposes to monitor the gains in the functional abilities of children with mental retardation from intervention (sports activity in this case). The authors propose to use WHODAS 2.0 47 which rates the nature of disability directly from a patient’s response. In particular, it provides an internal (subjective) perspective of the individual and assesses the limitations in activities and restrictions in participating experienced by an individual, independent from a medical diagnosis. The six psychometric domains included in the instrument are as follows: a) understanding and communicating (concentrating for 10 minutes, learning a new task), b) getting around (standing for 10 minutes, walking a long distance), c) self-care (washing your whole body, getting dressed, d) getting along with people (interaction with unknown people, maintaining friendship), e) life activities (household chores, day-to-day activities at work/school) and f) participation in society (joining community activities, emotional effect of disability). 48
Aim of the study
The aim of this study was to determine if sports activities have been detrimental in improving functional ability on the basis of a case study administered in a sample of children with mental retardation based in Kolkata, a metropolis in India. The following hypothesis was set: the independent variable of number of years in sport does significantly influence the functional ability of children with mild to moderate mental retardation.
Methods
Source of data and sample design
It was proposed that the WHODAS 2.0 12-item version would be administered on the caregiver-teacher-coach team of a subject to grade the child’s improvement in functioning. The World Mental Health Survey had previously used the WHODAS 2.0 12 item version (Table 4.1, p. 35) (Manual for WHODAS 2.0, 2010) and for consistency it was decided that the same version of the WHODAS 2.0 was to be used for this study. The authors analyzed the impact of factors responsible for the improvement. All association registered with the Sports Authority of India with a Kolkata postal address for training children with mental retardation were approached. Six were shortlisted which fulfilled the following criteria:
The sports association needed to have facilities to practice the five stages of mounting complexity as fundamental skills, basic game skills, relay games of low organization, team games and specialized sports events.
Sports instructor/coach should have at least 10 years’ experience and the co-instructor(s) to have a minimum of five years’ experience in training children with mental retardation.
The sports facility should have produced at least five national level participants and at least two medal-holders in Special Olympics within the last three years.
Training should be provided three times a week for two hours a day. Routine homework should also indicate that children should follow the stretching exercise pattern two hours a day for any other three days of the week.
The first stage sampling was undertaken in order to homogenize and control the data set for inter-temporal and inter-spatial homogeneity of coaching and exercise time. For second stage sampling we reviewed the Special Olympics manual which categorized participants on the basis of their biological age into four sub-classes of 8–11 years, 12–15 years, 15–21 years and 22–29 years. We chose the two mean classes so that our sample represented the population. From the six sports association registers we chose every third name (gender irrespective) belonging to the second (12–15 years) and third (15–21 subclasses) against a constraint of at least two years active attendance in the sports facility.
At the end of the second stage sampling a total number of 31 participant databases were identified. As one should have at least 25 observations to run a meaningful regression, the authors merged the second and third subclasses into one homogeneous category. As 23 observations out of the sample of 31 belonged to the 14–17 age group (the last two years from the second and the first two years from the third category) (mean = 15.09 years, SD = 2.3 years, range = 6 (12–18 years)) it was expected that the data set would follow the normal distribution pattern with more observations cluttered around the central tendency rendering homogeneity to the sample.
The authors did not try to control the homogeneity of classroom teaching both in terms of number of active teaching hours in school and quality of teachers as both of these attributes were uniformalized by the monitoring authority. The special education schools which the sample children attended were accredited and monitored by the Disability Commissionaire of West Bengal (an Indian state with Kolkata as its capital). It was a positive coincidence to find that 26 out of 31 children belonged to the Montessori special education level, with mild to moderate disability (tested IQ of 24/31 falls in the 45–58 band) after having passed through the ladders of therapeutic level, small group level and the activity level. Five of the 31 children belonged to the traditional classroom level, the highest class that a child can attain in a special education school.
As any class in any of these schools is taught by the heterogeneous set of degree-holders, diploma-holders in special education, Montessori trained teachers and trained psychologists, a more or less homogeneous quality of classroom teaching prevails in the city. Only three out of 31 children from our sample took assistance from professional caregivers, in all other cases the mother provided this support. This was deemed too sensitive an issue to adjudge the quality of the mother caregiver, and the authors declined to homogenize this attribute.
The data were generated on a personal investigation method, where the coach, the caregiver and the class-teacher (the person taking care of the administrative paper work for that class) helped the surveyor to fill in the data sheet on the condition of extreme anonymity. The child consistently sat through and participated in the interview process. When a question was asked, the coach, the teacher and the parent provided a score in the 10-point scale. The child contributed to the answer of the question from a qualitative point of view and shared experiences.
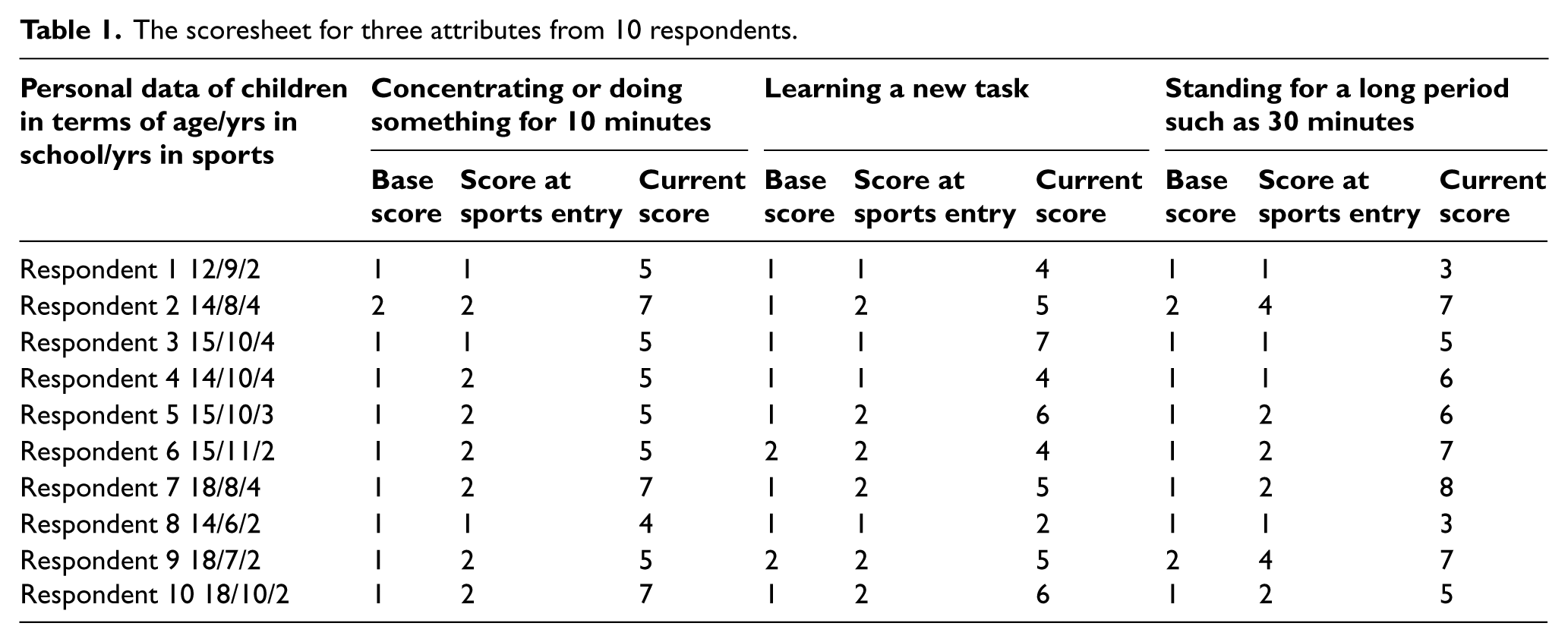
Scoresheets were filled for three points of time. Stage I was when the respondent joined school. In case the student changed school, or the teacher changed, the first score was recalled from school records. The second score was recalled from the time when the child actively joined the sports group and the third score was the current one. The respondents were asked to provide scores on a 10-point cardinal scale, with one depicting negligible response and higher scale values reflecting improved functioning. An assistive device in the form of ordinal values (1 = negligible, 2 = very poor, 3 = poor 4 = below average, 5 = average, 6 = just above average, 7 = fair, 8 = good, 9 = very good, 10 = perfect) was also provided. Table 1 gives an overview on how the scorecard appeared for three attributes and 10 respondents. Ethical approval for this study was sought and approved by the author’s institution and informed consent was obtained from the parents.
The scoresheet for three attributes from 10 respondents.
Data analysis
The authors wanted to determine and analyze the impact of intervention, sports activities in our context. Firstly, the gain in scores were calculated between the second and third points of time to find the absolute difference. The difference was expressed as a ratio to the second score ((S3-S2)/S2) to provide a relative improvement for each attribute for every respondent.
Multivariate regression was used with relative improvement in scores as the dependent variable. Number of years of active participation in sports activity (intervention I), number of years in integrated school (Intervention II) and the age of the child are incorporated in the model as dependent variables. The score of the child generated during their school enrolment has also been incorporated an independent variable to quantify the proxy clinical condition. As the children participating in sports activity have been clinically diagnosed to have mild to moderate retardation, the initial functioning score should serve as a proxy to his clinical condition.

Where Yi is the dependent variable: improvement in the relative score for the ith individual, X2i is the first independent variable: number of years in sport, X3i is the second independent variable: the number of years in school, X4i is the third independent variable: the age of the respondent and X5i is the fourth independent variable: the first score of the respondent.
This is a classical linear regression model that is linear in the parameters, and is applicable to the data here which is also linear in the explanatory variables. In a technical sense, ui is known as the stochastic error or the stochastic disturbance term, that stands as the surrogate or proxy for all the omitted or neglected variables that may affect Y but that the model has not been able to incorporate. The overall significance of the three-variable regression is checked by making use of the F-test. The F-value in this case is 36.850, and is therefore statistically significant at the lowest level of significance.
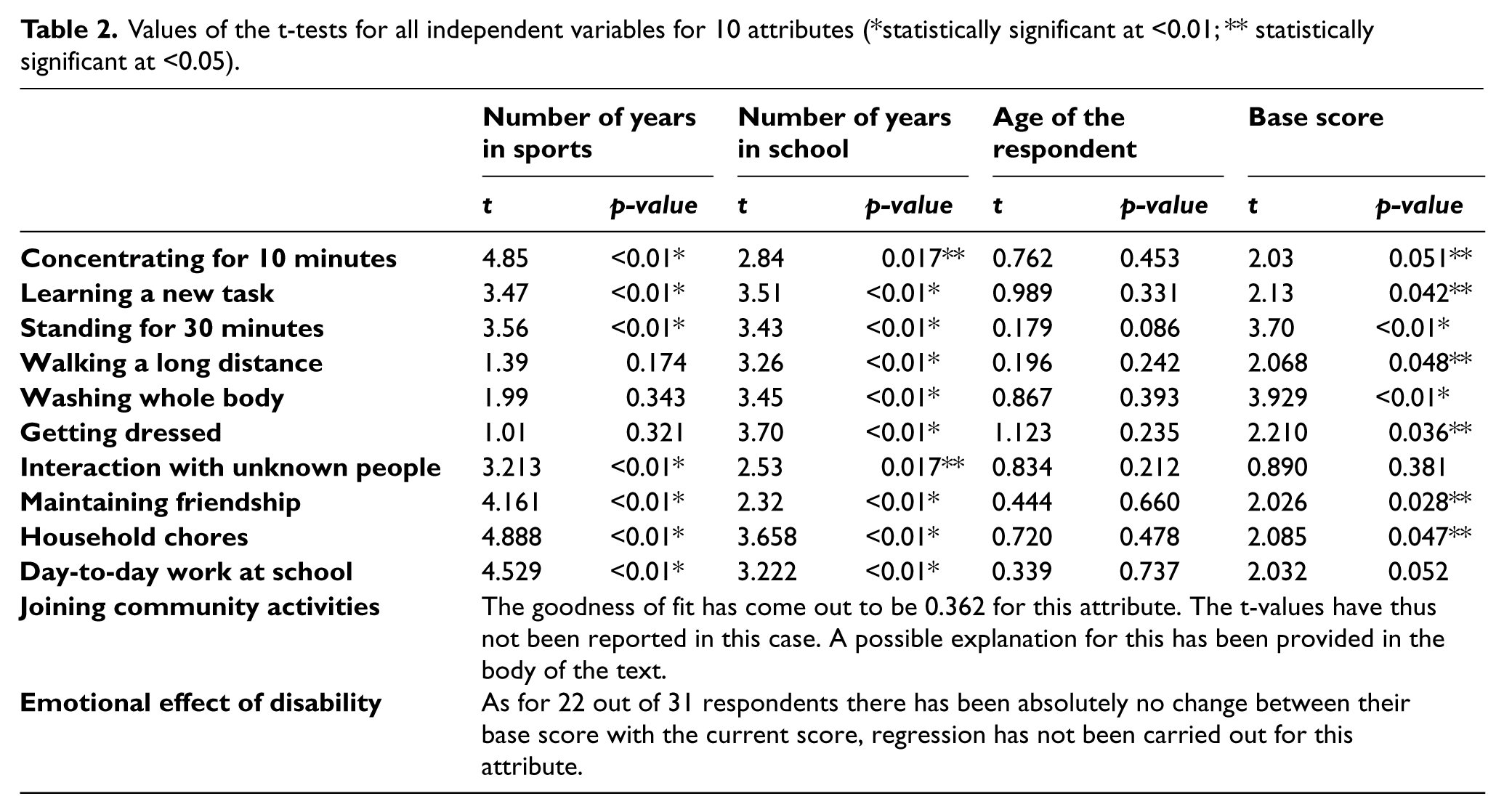
The regression analysis was carried out in 11 out of 12 attributes by using the standard SPSS 10 software. The F-test that adjudge the overall significance of the model by postulating the null hypothesis H0: ß2= ß3 = ß4 = ß5 = 0 (that is all slope coefficients are simultaneously zero against H1. Not all slope coefficients are simultaneously zero (if the observed F > the critical value of F at α level of significance then we reject the null hypothesis) was conducted. Results clearly indicated statistical significance of the model (F = 36.850) at the lowest level of significance. The Durbin-Watson test was run to check the presence of any serial correlation within the independent variables. The D-statistics were reported to be 1.444, less than the rule of thumb value of ‘d’ that is specified to be 2, indicating absence of serial correlation among independent variables. The Student’s t-tests for all independent variables with corresponding levels of significance are presented in Table 2. An alpha level of 0.01 was used for all statistical analysis performed.
Values of the t-tests for all independent variables for 10 attributes (*statistically significant at <0.01; ** statistically significant at <0.05).
Results
The descriptives of the sample are as follows: n = 31 years, mean = 15.09 years, SD = 2.3 years, range = 2–18 years. For 10 out of 11 attributes the values of R2 are greater than 0.70. This indicates that over and above 70% in the variation in the dependent variable are explained by the independent variables, which in turn proves that the relationship proposed between the regress and the regressors assumed in the model is correct. However, the scattergram and regression line could not be drawn as the multivariate regression gives a multidimensional plot (5D in this case).
Discussion
In this study the authors set out to analyze the positive effects of sports activities on the functional ability of children with mild to moderate mental retardation on the basis of a case study administered on 31 respondents from Kolkata, a metropolis in India. For all 10 attributes of the WHODAS 2.0 12-item version that showed meaningful regression results the coefficients of the independent variables like years in sports, years in school, age of the respondent and the base score have come up with expected signs. The t-test for the number of years in special schools have been found to be statistically significant at the lowest confidence level (t statistic is statistically significant at 0.000 (p < 0.01) for number of years in school) for all the 10 attributes (Table 2).
The hypothesis that sport activity has a positive impact on the functioning of an intellectually retarded child has been found to hold for seven out of 10 attributes for which meaningful regression result was obtained. It has been found to be statistically significant at the lowest confidence level (t statistic is statistically significant at 0.000 for number of years in sport) (p < 0.01). As the test statistic lies in the critical region, it is said to be statistically significant with 99% confidence (p < 0.01). In this case, the null hypothesis is rejected. The t statistic for the base score has been found out to be statistically significant but for higher confidence intervals. That is, for these attributes t-tests for the base value score falls in the narrower critical region.
The number of years in sports activities was found to not have a statistically significant impact on functioning in three of the attributes. In these cases the base score of the child has very strong effects on the dependent variable along with the obvious parameter of number of years in school. The result can be analyzed as follows. As none of the respondents had any locomotor disability or motor coordination retardation, they enjoyed walking. They joined school with quite high base value for this attribute. They had high base scores for dressing and washing attributes as compared to other WHODAS 2.0 parameters, which were tasks years in school and parenting prepared them for. All 31 respondents were at least four years ahead in terms of school-going than sports participation. The authors checked the curriculum of all schools the respondents attended and found that special children were trained extensively on getting dressed and washing oneself from the therapeutic level itself.
However, for the age of the child as the independent variable t-statistic could be accepted with a lower confidence (p>0.05). In most cases either we have not been able to authenticate or been able to authenticate the impact of the child’s age with a lower confidence. As for 22 out of 31 respondents the 12th attribute (recording the emotional effect of disability) did not show any change, regression analysis for this attribute was not run at all. For the 11th attribute (joining in community activities) the value of R2 has been recorded as 0.342. This indicates dropping out of some very crucial independent variable/s from the model. We felt that joining in community activities has quite a lot to do with the receptive ability of community along with the participating ability of the respondent. A repeat visit to the respondents to cross-check it, revealed severe barriers from the society in the form of people’s attitude, asymmetric information and transport bottlenecks. The presence of these qualitative attributes could have influenced the dependent variable, albeit in a negative manner. A 2005 study 49 has commented on the ‘lack of social support, limited opportunities for education, employment or participation in the community further isolates disabled children and their families, leading to increased levels of stress and hardship’.
A similar concern was voiced in the report 50 which observed that children with disabilities ‘experience stigma from birth and are more prone to exclusion, concealment, abandonment, institutionalization and abuse’. Social exclusion of people with disabilities from the mainstream has been acknowledged and the need to create a special environment for them has been reflected both in the mission of Paralympics and Special Olympics events. However, the respondents participated and enjoyed sports and school activities for special children, 12 out of 31 respondents participated in state, national and international levels of Special Olympics and were medal holders in basketball, table tennis, floor hockey, shot put, walking and athletic events. They were comfortable in the special child environment, but shied away from general community activities, a trend so very much in line with the existing literature in this regard.51-52 The Braille Chess Club in Bangladesh, the Afghan Amputee Bicyclists for Rehabilitation and Recreation and the Blind Cricket World Cup are cited in the CBR guidelines as success stories highlighting this trend.
Limitations
In any study, biases are certain to creep in through attributes that cannot be controlled by a quantitative design. Though extreme efforts were taken to homogenize the data set, inter-personal relationship between the teacher, instructor, caregiver and the child, learning ability of the child and training ability of the teacher (in that order) have been responsible for the stochastic error term in this particular experiment. As the purpose of this endeavor was to understand the impact of sports on children with MR, the authors devised criteria to screen all registered sports association for inclusion/exclusion in the sample. However, no screening norms were imposed on schools attended by our sample. We just checked the mandatory accreditation by the Disability Commissionaire. As these children have come from different schools spread all across the city, despite all efforts quality biases might have crept in, which the model has not been able to control. However, an effort to screen both the sports association and the school in the same sample design in a metropolis of a developing nation with limited facilities for the disabled would have resulted in a paucity of data to carry out any meaningful statistical exercise.
Though the standard deviation for our sample was small, merging two subclasses rendered the sample to a slightly high range, especially towards the lower-end of the age spectrum. This is another limiting factor of the study. The authors propose to investigate the data set further and conduct this exercise in other A-1 cities of India to find out whether the proposition tested in this case study holds uniformly across the population. If it does, the use of sports activities as an intervention towards improving the functional abilities of children with mental retardation should have to be strongly considered.
Conclusion
This study was carried out to determine if active participation in sports improved functioning abilities of a child with mental retardation. For seven out of 12 WHODAS 2.0 attributes, the null hypothesis that proposed ‘the independent variable of number of years in sport does not significantly influence the dependent variable of improvement of functional abilities’ could be rejected. In contrast, it could be accepted that the proposition that active participation in sports, beside other factors, did improve the functioning abilities of children with mental retardation who, as sample, were respondents in our study.
The sample of children appeared to have a biological advantage in the ‘walking for a long distance’ attribute. Schooling and parenting prepared them more for the two self-care-related domains of getting dressed and washing up. They participated in community activities (sports events) held exclusively for the disabled population. The society, in their perception, did not come up with a reciprocative role to welcome them in community activities. There was little or no change for the emotional aspects of disability attributes for almost all of the respondents. This study has attempted to highlight the positive impact of sports in developing the functional abilities of children with mild to moderate mental retardation. Moreover, it has the potential to disseminate its use as an indigenous rehabilitative tool in a developing country.
Footnotes
Acknowledgements
The authors would like to express our sincerest gratitude to the sports authorities, sports-instructors, parents, caregivers, respondents for giving us their precious time in filling up the questionnaire.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.