
Abstract
Background:
Post-amputation pain is a multifactorial issue and thus necessitates multiple treatment strategies. Myofascial trigger points-related pain remains under diagnosed and hence not addressed. This study investigates causation and management.
Objectives:
To identify the presence and role of myofascial trigger points in post amputation pain.
Study Design:
Post-amputation pain clinic review and recruitment.
Methods:
Twenty one identified patients in the post-amputation pain clinic with myofascial trigger points were recruited, of which 13 were transtibial and eight transfemoral and all had phantom limb pain and stump pain. The trigger points were identified and injected with long-acting local anaesthetic on a weekly basis and patients were followed up on an ongoing basis.
Results:
There was significant resolution of pain on the Visual Analogue Scale in the majority of these patients within five weeks, though some of the transtibial cohort needed further eight injections on a weekly basis for resolution of the pain.
Conclusion:
Identification of myofascial trigger points in amputation stumps and their role in post-amputation pain, followed by appropriate intervention is an important facet of management of this complex chronic pain.
Clinical relevance
Myofascial trigger points in amputation stumps can lead to ongoing chronic post-amputation pain and our results indicate that identification and intervention of these trigger points does lead to notable resolution of this pain.
Background
The phantom phenomenon following amputations was first reported by the French military surgeon Ambrose Pare in the mid-sixteenth century. Following the American Civil War, Weir Mitchell in 1872 published the first detailed study regarding phantom limb pain. 1 While phantom limb pain is characterized as pain being present in an absent portion of the limb, stump pain is felt in the remaining portion of the residual limb. Several hypotheses have been suggested trying to explain these two types of post-amputation pain, including peripheral nerve involvement, neuronal memory, central pain mechanisms and psychological factors. None of these theories can fully explain, neither the phantom limb pain nor the residual stump pain, and numerous management approaches have limitations as regards long-term success.
The aim of our study was to assess the efficacy of identifying and inactivating the myofascial trigger points in the stump/residual limb of lower limb amputees and do a close follow up to note changes, if any, in their post-amputation pain profile.
Our study of the myofascial trigger points related pain and/or autonomic phenomena referred from active myofascial trigger points in the residual limb, may partly explain the phantom limb pain, the stump pain, the multifarious pain patterns and other peculiarities being observed after a lower limb amputation. However, based on this theory an effective additional treatment modality may be available for alleviation of the troublesome post-amputation pain complex.
The definition of the myofascial pain syndrome is pain and/or autonomic phenomena referred from active myofascial trigger points. 2 Myofascial pain may be acute or chronic, regional or widespread, but in every case it is associated with local tenderness or pain that is localized to a linear or nodular hardening in the muscle that is called a myofascial trigger point. Referred pain, or pain that is felt at a distance from the point of stimulation, is characteristic of myofascial pain. The referred pain does not follow peripheral nerves and the nature of the mechanisms involved is still not known, but the referred pain from each muscle is so constant that trigger point flipcharts are available. 2 In patients suffering from a general myofascial pain syndrome, we know by experience that the active trigger points in an area will organize in groups or bands that run the length of the muscle when the disease has been chronic.
Methods
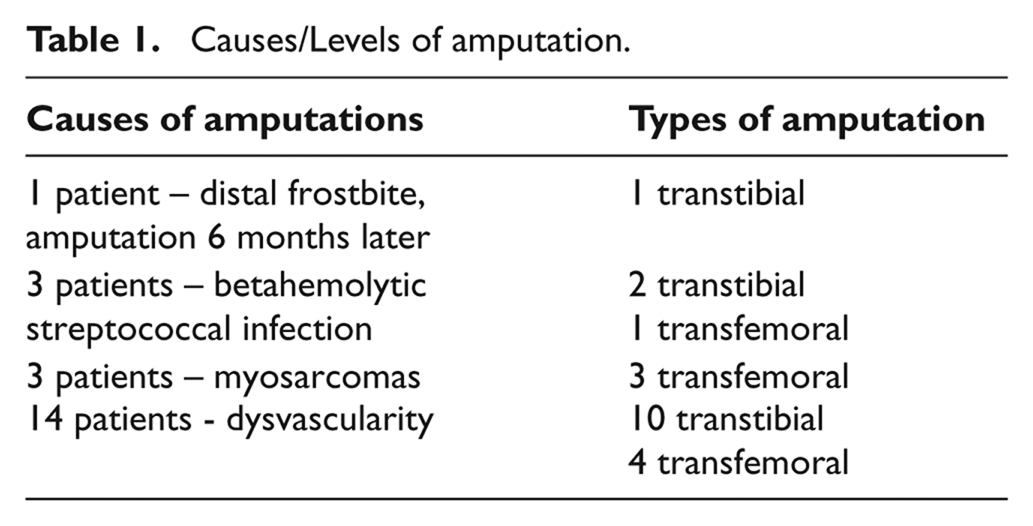
After obtaining ethical approval from the Norwegian Board for Pain Medicine, 21 major unilateral lower limb amputees were included in our study of which 14 patients were male and the mean age in the group was 61.5 years. All amputations were planned and non-trauma related (Table 1). Thirteen patients had transtibial amputations and eight had transfemoral amputations. Post-amputation pain was measured on a Visual Analogue Scale (VAS, where 0 is no pain and 10 is worst imaginable pain).
Causes/Levels of amputation.
The inclusion criteria were that these were healed unilateral lower limb amputees who had their amputations for over two years.
The exclusion criteria were that these patients had no known allergies to local anaesthetic – bupivacaine (without adrenaline). No patients were excluded. Patients were advised not to alter their routine physical activities.
Examination and palpations of the patient’s stump and proximal part of the lower limb was done to identify any longitudinal taut bands containing any active trigger points. In our opinion, the residual stump above the knee can roughly be divided into four quadrants; medial, lateral, anterior and a posterior quadrants. The taut myofascial bands found in each quadrant of the residual limb above the knee joint, co-related to the phantom pain (and in some patients to the distal stump pain) in the corresponding sectors of the distal stump and more importantly for the phantom limb pain in the lost portion of the limb.
Following a detailed clinical examination, the patients were treated on a weekly basis for five weeks, in order to inactivate the trigger points. Using a 5 ml syringe and a 0.60 x 60 mm needle, bupivacaine 5 mg/ml without adrenaline was injected into the trigger points using a special method called ‘walking the needle’ in the myofascial compartment as the longitudinal taut bands gave us the approach model for these injections. Patients were followed up on a fortnightly basis for six more injection procedures using the same technique.
During and after the described procedure, the patients were instructed to stretch the involved muscles/taut myofascial bands to further reduce activity in the remaining trigger points and they were warned not to increase their walking activity too abruptly because of any pain reduction. If the residual post-amputation pain increased, the patients were asked to report for an early follow-up appointment. A review of patients’ analgesics was undertaken.
Results
We detected a constant link between the localization of the taut myofascial bands in the stump and the localization of the phantom limb pain. Typically, a pressure applied to the bands on the posterior aspect of the residual limb would produce a phantom pain localized in the back of the calf spreading to the heel, sole and under and between all the toes. We also found a very distinctive pattern of the pain distribution when applying pressure to the different taut myofascial stump bands.
Pressure to the bands for more than five seconds produced a strong local pain, as well as a centrifugally referred pain to the distal part of the stump and likewise a phantom limb pain in the missing part of the limb that could be of a burning, aching, cramping or pressing nature.
Additionally, tip pressures to the taut myofascial bands – trigger points, when applied to five transtibial amputees in the proximal part of the stump resulted in a burning or aching strong pain localized in the distal stump in the section below the knee joint, as well as a phantom limb pain. When carefully squeezing this distal part of the stump itself, all five patients felt a local uncomfortable pain.
Pre- and post-treatment average phantom limb pain and stump pain are shown in Table 2.
Pain profile: pre and post treatment.
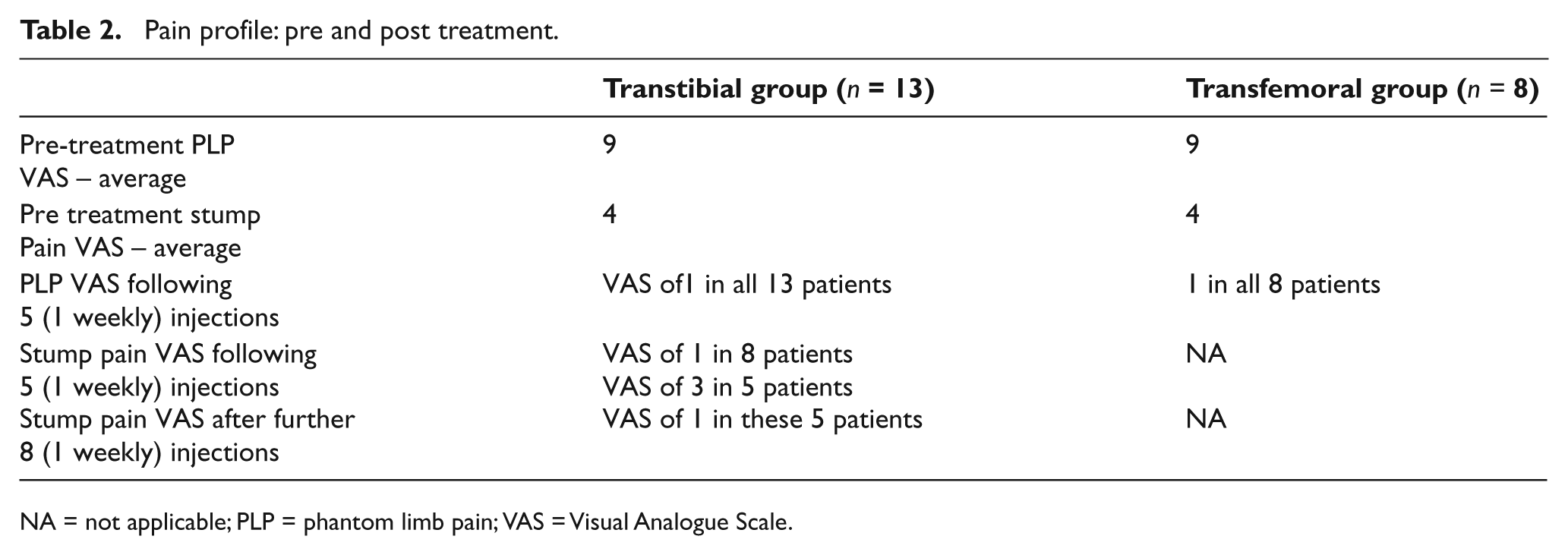
NA = not applicable; PLP = phantom limb pain; VAS = Visual Analogue Scale.
After each injection intervention of the trigger points the patients were completely pain free for six to 12 hours – these periods increased with every treatment procedure, and at the same time the residual phantom limb pain as well as the stump pain grew steadily weaker. After five weekly treatments, the stump pain had disappeared completely in the majority of the patients. The exception being in the transtibial group of five amputees suffering the unique stump pain localized in the distal stump below the knee where pain still remained, but had decreased from a VAS on an average of 7 to 3. It took eight further treatments before it settled to VAS of 1.0 (Table 2).
Interestingly, the patterns of the residual phantom limb pain had changed. The cramping, burning and pressing pain types were a lot weaker while the aching pain type was predominating.
Overall the notable decrease in post-amputation pain following intervention lasted for three to six months, with overall VAS pain scores being 50% less in the ensuing period. We repeated the trigger points injections after six months interval, till there was notable resolution of pain.
All patients in the group declared that a weather change from high pressure to low pressure always increased their post-amputation pain while the opposite happened when changing from low pressure to high pressure and that they had their best pain periods in high pressure weather conditions. Similar changes are reported by non-amputee patients suffering from general myofascial pain. 3
Sitting all evening in a supportive chair looking at the TV may produce the same pressure towards the posterior quadrant trigger points causing increased activity. On the other hand, when the patients are asked to take pauses by walking around, no increased phantom was reported in our group.
We noted that patients used strong opioids in high doses. In our view, strong opiods have no place in the treatment protocol of chronic post-amputation pain. A careful reduction of opioids is recommended.
Carisoprodol, a short-acting muscle relaxant was used regularly by 12 of the patients. In these cases, it was noted to be a risk-prone medication with marked drug dependence and drug abuse characteristics. 4
Pharmacological interventions on their own do have some limitations in managing post-amputation pain. Tramadol in twice-daily dosage reduced stump pain as well as phantom limb pain in about 50% of the patients. Likewise, clonazepam produced better sleep and reduced a post-amputation pain pattern due to the relaxant effect on affected muscles in 15 out of 21 patients, but the use is limited because of the danger of drug dependency and hangover effect. Non-steroidal anti-inflammatory drugs, on the other hand, seemed to have a relative limited temporal effect in the patient group.
Discussion
A universally agreed and accepted mechanism for stump pain and phantom limb pain does not yet exist. 5 In our patient cohort there were no post-trauma cases. We believe that there is an important difference between the post-amputation pain seen after planned amputations, and the acute amputations following an accident. In the latter group, acute nerve damage including destroyed nerve plexuses due to traction/pulling forces play an important role in the post-amputation pain picture and trigger point-induced pain plays a minor role. However, in planned amputations caused by dysvascularity/infection/malignancy; it is likely that trigger points-related pain is pre-existing and of longer duration.
Numerous possible mechanisms have been advocated, but the current main theory is based on the argument that post-amputation pain is a central pain following peripheral nerve involvement. 5 However, this postulate does not fully explain neither the magnitude of pain patterns involved nor the presence of a contemporaneous stump pain, and the fact that the majority of the amputees wake up from the amputation with a picture of a phantom limb. Also, the treatment procedures based on this theory have been problematic. Peripheral stimulation, like transcutaneous electrical nerve stimulation, has no notable documented effect. Spinal cord stimulation has not been very efficacious; and to our knowledge, there are no clinical trials to show any effectiveness of this method in phantom limb pain. However, it has been shown that the method is effective for the overall management of severe neuropathic pain. This appears paradoxical as, if one follows the assumption that neuropathic pain should be an important factor in the mechanism of phantom limb pain.
However, our model of the presence of a myofascial pain syndrome in the stump muscles may explain both the stump pain, related to the trigger points as well as the phantom limb pain. The different post-amputation pain patterns mentioned above may be a function of the activity in the actual trigger points involved. Weaker trigger points produce the local stump pain; more active trigger points may be involved in distal stump pain caused by local referred pain, while the most active trigger points are responsible for the referred pain producing the phantom limb pain. Using this model, an effective treatment protocol could be followed.
The active trigger points in the stump mainly occur as the result of chronic or subacute muscle overload in the actual limb and are likely to appear well before the amputation.
However, also the muscular microtrauma in the stump during the amputation procedure may in a short time develop into active trigger points postoperatively. Studies in patients undergoing amputation because of vascular disease have shown that the onset of phantom pain is usually within a week of the operation. 3 Ninety per cent of the patients even claimed severe phantom limb pain just hours after the amputation. This could be explained by a compression of taut bands in the posterior quadrant of the thigh onto the hard surface of the operation table, activating the trigger points to respond with a referred pain in the removed limb. In the daily life of many lower limb amputees the same mechanism may explain why the phantom limb pain often feels strongest during the night, when they tend to sit on the sofa with pressure on the proximal posterior part of the residual limb.
A good fitting prosthesis which obviates extrinsic pressures, mainly in the posterior quadrant in transfemoral amputees and lateral quadrants in transtibial amputees, often eases both stump and phantom limb pain by relieving direct pressure over the hamstring muscles/sciatic nerve and lateral popliteal nerve respectively.
Pre-amputation pain is also a risk factor for phantom limb pain. Preamputation physiotherapy including stretching of the thigh muscles as well as hydrotherapy could have a role in decreasing post-amputation pain; by partly obviating the taut myofascial bands. Nikolajsen et al reported that phantom pain may mimic pre-amputation pain in both character and localization. 6 Arena et al. reported how phantom pain can be triggered and exacerbated by psychosocial factors. 7
Conclusion
The limitations of our study are the small cohort of patients and that all the amputees were non-trauma causation. Also we were of the opinion that it would be inappropriate to conduct a double-blind study, using isotonic saline, as it could lead to further stump pain. We suggest that in order to obtain optimal and longer lasting effect on post-amputation pain, it is prudent to address the additional issue of myofascial trigger points in the residual limb. Inactivating the trigger points using the above described method as soon as feasible after the amputation, would decrease one element of the conurbation of factors that leads to post-amputation pain. We postulate that on balance, better results may be obtained by starting the treatment before the amputation. The procedure should be repeated if pain recurs. Lastly, we recommend a larger prospective trial in this group of patients to further confirm our findings.
Footnotes
Acknowledgements
We would like to thank all our patients who took part in our study, and Dr Johansen, Dr Grady and Dr Richardson for their constructive comments.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.