
Abstract
Background:
Subtalar joint hyperpronation plays a fundamental role in the development of hallux valgus (HV). Foot orthotics have used to treat this condition and are aimed at preventing progression of the deformity.
Objectives:
The aim of this study was to determine if the use of custom-made foot orthotics for 12 months prevented the advancement of HV in women.
Study Design:
Prospective trial, using a repeated-measures design.
Methods:
Fifty-four women with mild to moderate HV were divided into two groups: the experimental group used custom-made foot orthoses, and the control group used no treatment. First intermetatarsal (IMA) and hallux abductus (HAA) angles were measured at the beginning of the study and after 12-months follow up. Inter-group comparisons were made of these angles at both times of measurement, and intra-group comparisons between the two times of measurement.
Results:
The initial HAA was similar in both groups (19.92 ± 4.25 degrees for the control group, 20.55 ± 5.10 degrees for the experimental group; p = 0.392), and also the IMA (10.56 ± 2.45 degrees for the control group, 10.86 ± 2.33 for the experimental group; p = 0.618) There were no significant differences in the follow-up values of these angles (p = 0.395 and p = 0.288, respectively). There were no significant intra-group differences in the comparisons of the initial and follow-up angles.
Conclusions:
HV did not have a significantly slower evolution in participants of the experimental group compared with controls. Custom-made orthoses appear to have no effect in the evolution of mild and moderate HV during a 12 month period.
Clinical relevance
Subtalar joint hyperpronation plays a fundamental role in the development of hallux valgus. Conservative management typically involves the use of foot orthotics which is aimed at preventing the progress of the condition. The use of foot orthotics however should be used as a long term management strategy (beyond 12 months).
Background
In hallux valgus (HV) the great toe is deviated laterally and the first metatarsal medially, resulting in a medial bony prominence at the first metatarsophalangeal joint (MPJ).1,2 The exact ætiology of the development of HV is not entirely clear. According to many authors, the development of HV is multifactorial, including both intrinsic and extrinsic factors.3-11 The most common cause of adult HV is a combination of environmental factors (e.g. mechanical abnormalities caused by badly fitting footwear) and a genetic predisposition to constitutional anatomical factors, with some authors describing the latter to be involved in 70% of cases.4,12 However, in most cases there is a clear biomechanical base ætiology. Excessive pronation of the subtalar joint during the stance phase of gait is responsible for instability of the foot, causing dysfunction of the first ray and the first metatarsophalangeal joint (MPJ), leading to deformities such as HV.1,6,8,13-15
If subtalar joint hyperpronation plays a fundamental role in the development of HV, then controlling the abnormal mobility of this joint by means of foot orthotics should prevent or control progress of the condition. But even though there have been various studies of the effectiveness of such conservative treatments, they have led to a situation of some controversy. Some longitudinal studies have reported that foot orthoses are effective in preventing HV while others have refuted this claim. The present work was aimed at responding to the question of whether treatment with custom-made foot orthotics can reduce or slow down the progress of HV in women with mild to moderate HV (according to the classification of Kelikian 16 ), after a 12-month follow-up period. The null hypothesis is that foot orthoses have no effect in controlling the advance of HV, i.e. that the study participants using foot orthoses for 12 months would have the same increase in HV as participants who did not use them.
Methods
Subjects
A prospective trial, using a repeated-measures study was carried out with 54 women of mean age 30.63 ± 11.87 years with mild to moderate HV (97 affected feet). Each foot was counted as a separate case, since for a given participant only one foot may be affected. The participants were volunteers from three sources: students of podiatry at University of Seville (30 women); patients attending the Podiatry Clinic Area at the University of Seville who met the inclusion criteria and agreed to participate voluntarily in the study (11 women); and staff of this centre who, when they heard of the study, decided to volunteer (13 women). Patients were divided into two groups – an experimental group corresponding to participants to whom the use of foot orthotics was applied, and a control group corresponding to participants to whom no treatment was applied. Data for the study were collected between January 2008 and November 2011, at the Podiatry Clinic Area of University of Seville. The study was approved by the Experimentation Ethics Committee of the University of Seville.
Allocation to either the control or the experimental group was as follows (Figure 1). All the women who met the inclusion criteria and had attended the Podiatry Clinic Area at the University of Seville seeking treatment with orthotics and had agreed to participate in the study were assigned to the experimental group (11 participants). For ethical reasons, and to maintain the quality of care provided by this centre, the authors believed that when patients had presented seeking treatment they could not be assigned to the control group because this would have meant 12 months without treatment. To prevent this producing heterogeneity between the groups, the technique of matching on grounds of age and severity of the HV was used to choose the first 11 participants to include in the control group. The remaining participants (32 people) who voluntarily asked to participate in the study were randomly assigned (by coin toss) to the groups. Originally, the control group consisted of 48 feet of 26 women, mean age 30.31 ± 9.27 years, and the experimental group of 49 feet of 28 women, mean age 30.94 ± 14.05 years.
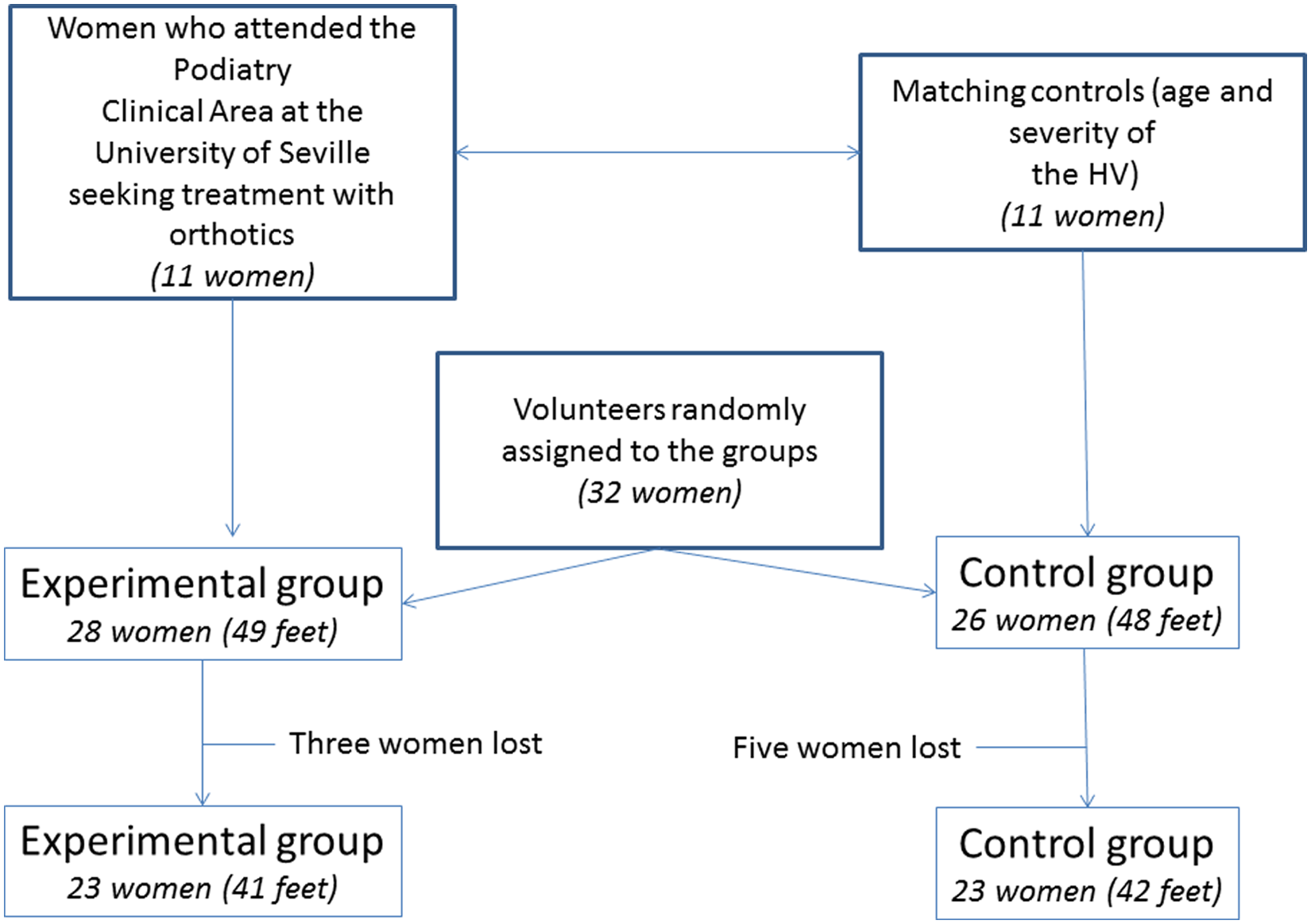
Flow diagram explaining the inclusion process.
In the control group, three women did not attend the 12-month follow-up study for the following reasons: one of them because of change of residence and two did not attend on the day set for the follow-up (unknown reasons). In the experimental group, five women did not attend the 12-month follow-up study for the following reasons: one of them for pregnancy, another one because she had lost the foot orthoses, and three did not attend on the day set for the follow-up (unknown reasons). The final sample consisted of 46 women (83 feet), aged 30.63 ± 11.87 years. Control group consisted of 23 women (42 feet) aged 30.94 ± 14.06 years, and experimental group consisted of 23 women (41 feet) aged 30.31 ± 9.27 years.
Inclusion criteria
One selection criterion was that the growth physes of the participant’s bones should be closed for there to be no possibility of variation in any of the parameters measured due to growth. Other inclusion criteria were: having an inclination angle of the calcaneus to the ground greater than five degrees, and presenting an HV angle greater than 15 degrees and lower than 40 degrees. Exclusion criteria were: having undergone osteoarticular surgery on the foot; having suffered serious injury to the foot that could have altered its bone morphology; having received orthopædic treatment; suffering from degenerative bone and joint diseases or neuromuscular imbalances; obvious deformities other than HV in the forefoot that might affect the results of the study; pregnancy; women who experienced poor acceptance of the treatment, or who refused the X-ray of the feet.
Variables
The independent variable was the use of foot orthoses. The dependent variables were the intermetatarsal angle between the first and second metatarsals (first IMA) and the hallux abductus angle (HAA) (Figure 2). These variables were measured at the beginning of the study (initial) and after one year (follow-up) so that comparisons could be made. The HAA is a measure of the deviation of the proximal phalanx of the hallux with respect to the longitudinal axis of the first metatarsal. It is considered to be the principal parameter with which to quantify the HV deformity. 15 The first IMA is considered to be the best measure of the medial deviation of the first metatarsal in the transverse plane – one of the components of the HV deformity. 17
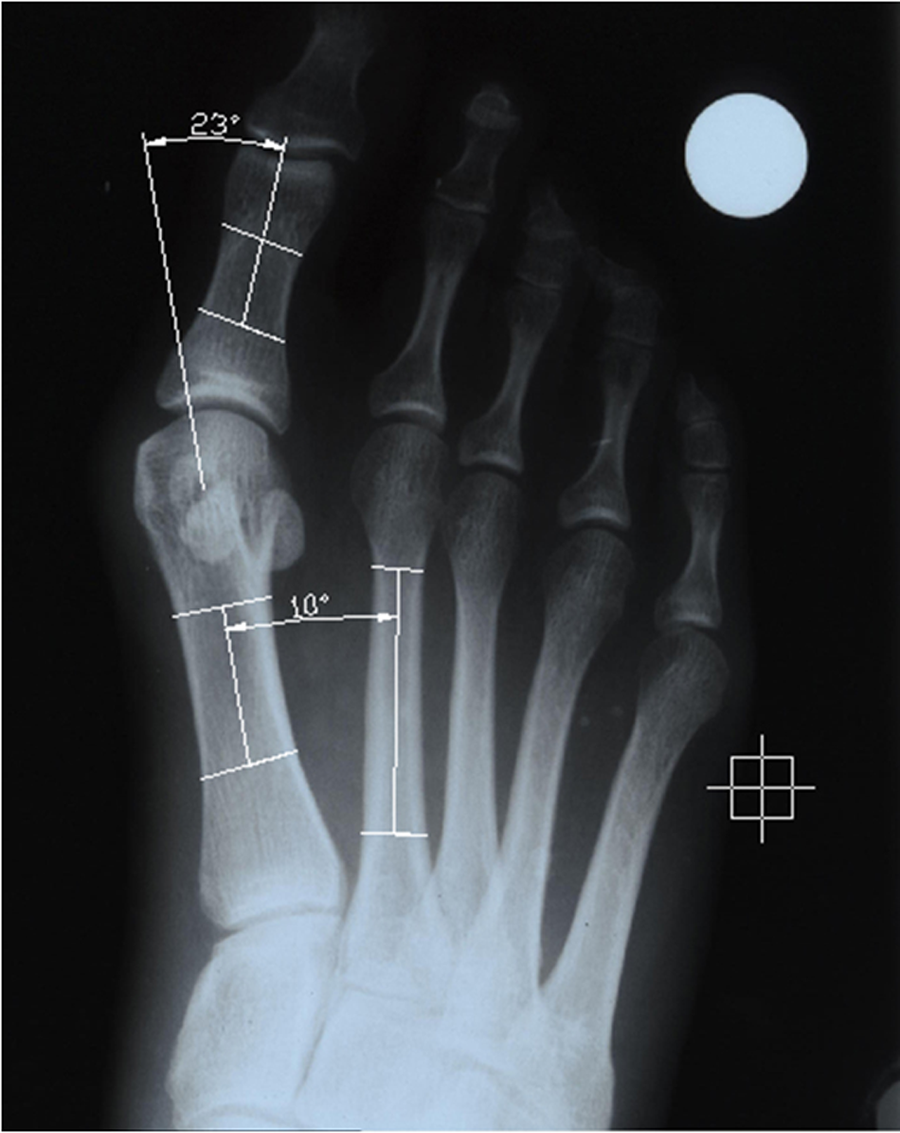
Radiographic measurements: hallux abductus angle (HAA) (top) and the first intermetatarsal angle (between the first and second metatarsals, first IMA) (bottom).
Procedure
Each participant was given an informative document which explained the nature of the research, its objectives and its potential risks. If, after reading it and having any doubts clarified, she agreed to participate, she was asked to provide her written consent. For each participant, a data sheet was prepared with her parentage data and an anamnesis. Articular explorations were made with the participant on the examination table, standing and walking, following the protocol used in the Podiatry Clinic Area of the University of Seville. The data from this exploration were used to establish that there existed rearfoot hyperpronation and mild to moderate HV according to the classification of Kelikian. 16
For all the participants, a weightbearing dorsoplantar X-ray was taken of both feet together, with the X-ray tube at one metre from the feet and inclined at 15 degrees from the vertical.18,19 The apparatus used was a Sedecal SPS HF-4.0® portable X-ray unit with a collimator. Kodak® Point of Care CR Cassette® chassis were used, equipped with a flexible GP phosphor screen of 24 × 30 cm. The operating parameters were 45 kV and four mA/sec, as recommended by the manufacturer. Each subject wore a lead apron to shield the rest of the body from radiation. A Kodak Point of Care 140® digital radiology device with Kodak Acquisition Software® was used for the acquisition and transmission of DICOM data, elements and images. With this set-up, a digital radiographic image is obtained which can subsequently be exported to the AutoCAD® computer program (AutoCAD 2006; Autodesk Inc, San Rafael, California) to perform the measurements. X-ray measurements using this procedure have been described in previous works.18,20 Measurements were made by a single observer (MR) in order to reduce the error due to variability in the measurements. 21
Fabrication of the foot orthoses
For each participant in the experimental group, a mold of the foot was obtained with phenolic foam with the subtalar joint placed in neutral position. The patient’s foot was manipulated before being introduced into the phenolic foam to place the subtalar joint in the neutral position and the forefoot plantar plane parallel to the floor. The negative molds of phenolic foam were filled with liquid plaster to obtain a positive mold of the foot on which to make the foot orthosis. Foot orthoses were made with polypropylene of three-mm thickness from the heel to just behind the metatarsal heads, and three-mm thick polyethylene foam posting of 45 shore A hardness on the distal part (Figure 3).
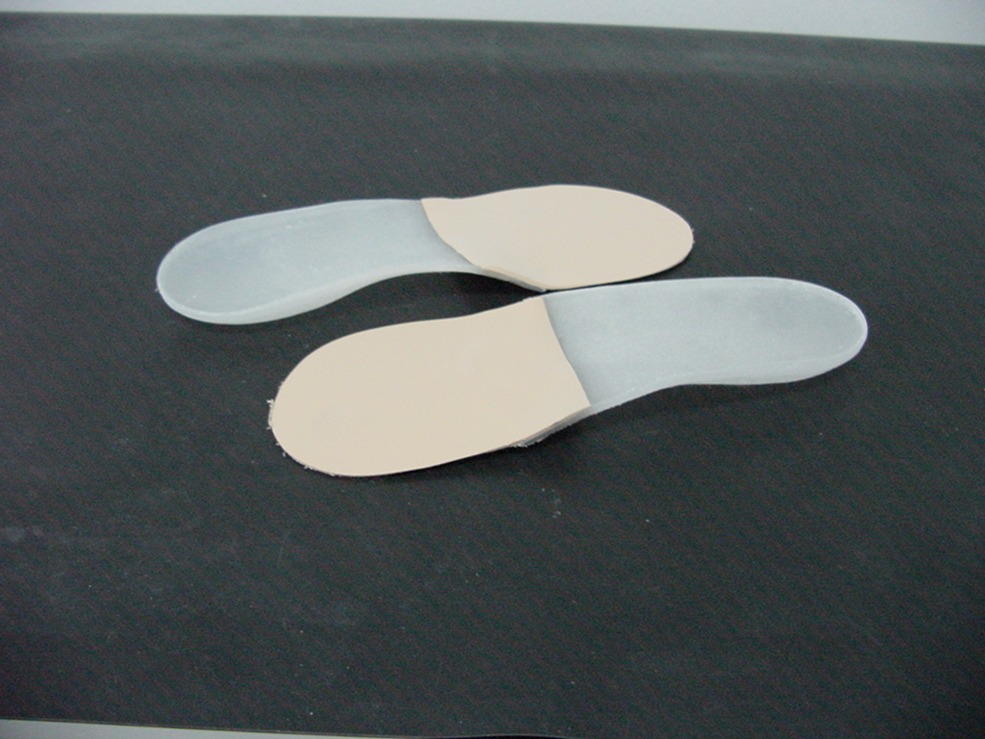
The custom-made foot orthoses used in the study.
The positive plaster cast was placed into a vacuum with the plantar surface upwards. A 3-mm thick polypropylene sheet was heated up to 180 degrees, until it became transparent (3 to 4 minutes), for vacuum press forming the orthosis. The 3-mm thick polyethylene foam sheet was heated and placed to the upper surface of the positive cast just before the polypropylene, so that both materials were adhered by heat and pressure. Some marks were painted on the orthosis in order to remove the spare material: a calcaneal line parallel to the dorsal surface of the positive cast and 10–15 mm above the support surface level; one point just below the navicular tuberosity, representing the maximum height of the orthosis on the medial side; and a distal line joining the points just proximal to the metatarsal heads and ending at the proximal edges of the first and fifth metatarsal heads. The spare material was removed by means of a polishing machine.
When the orthoses were finally handed over to the patient, their definitive adjustment to the foot was made, and the participant then tried out the treatment in the footwear, being asked to walk for five minutes so as to report any discomfort or incidence. Only when the patient stated that they felt comfortable was the orthosis taken as being completed. The patient was recommended to use the foot orthoses for at least seven hours a day, five days a week.
Telephone follow-up was conducted every two months to check the correct use of the treatment. After 12 months of follow-up, a new radiological control was performed for the participants in both groups following the same protocol as at the beginning of the study.
Data analysis
The study was designed to detect changes with an effect size greater than 0.8 (large effect size) for a contrast of difference between two independent means, assuming type I and type II errors of 0.05 and 0.1, respectively. With these design values, the GPower 3.1.0 software package (Franz Faul, Universität Kiel, Germany) was used to calculate the minimum sample size, which was found to be 36 cases per group. We assumed 15% loss during follow-up, so it required a minimum of 48 cases per group.
The data were analyzed with the SPSS (SPSS Science, Chicago, Illinois). The Shapiro-Wilk test was used to check for normality of the variables. The initial and follow-up first IMA and the age were found to be normally distributed, but the corresponding sets of HAA were not.
A preliminary exploratory analysis was made to check for homogeneity between the groups in age and side (right or left foot), using Mann Whitney’s U-test for independent samples in the former case, and the chi-squared test in the latter.
Then an inter-group comparison was made of the initial and follow-up HAA using Mann-Whitney’s U-test, and of the initial and follow-up first IMA using Student’s t-test for independent samples.
For the evolution of the condition over 12 months, an intra-group comparison was made for each group between the initial and follow-up HAA using the non-parametric Wilcoxon test, and between the initial and follow-up first IMA using Student’s t-test for paired samples.
Differences were considered to be statistically significant if p < 0.05.
Cohen’s d was calculated to estimate the effect size in the dependent variables, using the formula: (Mean 1 – Mean 2)/([SD1 + SD2]/2), where the value of d is positive if the difference between the means is in the predicted sense. This parameter classifies the effect size into small if d = 0.20, medium if d = 0.50, and large if d is greater than or equal to 0.80.
Results
The groups were homogeneous (no significant difference) with respect both to age (p = 0.530; Mann Whitney’s U-test for independent samples) and side (i.e. left or right foot: p = 0.920; chi-squared test), with the total sample comprising 49.5% left feet and 50.5% right feet, the control group 50% and 50%, respectively, and the experimental group 49% and 51%, respectively.
The initial values of the dependent variables did not present statistically significant differences between the two groups. The initial HAA was homogeneus (19.92 ± 4.25 degrees for the control group, 20.55 ± 5.10 degrees for the experimental group; p = 0.392). The same was the case for the initial values of the first IMA (10.56 ± 2.45 degrees for the control group, 10.86 ± 2.33 for the experimental group; p = 0.618). The groups were therefore homogeneous with respect to the values of the dependent variables.
The inter-group comparison of the follow-up values of these dependent variables revealed that there was no significant difference after the follow-up period (HAA: 20.36 ± 4.54 degrees for the control group, 21.02 ± 5.14 degrees for the experimental group, p = 0.395; and IMA: 10.52 ± 1.85 degrees for the control group, for the experimental group, p = 0.288).
The intra-group comparisons showed there to be no significant changes for either group in the values of the dependent variables from the beginning of the study to the follow up at 12 months. In addition, size effect was small for both comparisons. Table 1 summarizes the initial and follow-up values of the HV and first IMA for the two groups, and p-values and size effect for comparisons.
Mean and standard deviation of the hallux abductus (HAA) and first intermetatarsal (IMA) angle, at the beginning of the study and at the 12-month follow up for the control and the experimental groups. P-values and effect size (Cohen’s d) for the intra-group comparisons of the initial versus follow-up values of the HAA and the first IMA angles, and p-values for comparisons between the control and the experimental groups.

Discussion
The main objective of the present study was to test whether the type of custom-made foot orthoses employed controlled the advance of the HV deformity. According to the results observed, the null hypothesis cannot be rejected. The progression of the HV deformity was similar in both, the control group and the experimental group, after a 12-month follow-up period.
This study has certain limitations. Firstly, the follow-up period was relatively short; if the progress of this deformity had been observed over a longer time period, the results might have been more conclusive. Nevertheless, many studies on this subject have used similar, or even shorter follow-up periods, obtaining significant results in three or four month.8,22-26 Another limitation may be that the sample consisted entirely of women. The main reason is that HV is far more common in women than in men,27-29 and various studies of this type have been conducted with samples entirely, or in a large proportion, consisting of women.25,26,30,31 Finally, although in most cases the origin of HV is biomechanical due to excessive pronation of subtalar joint during gait,1,6,13,14 the progress of HV is multifactorial,3,7,10,11 and those remaining factors were not controlled.
Several studies have been carried out in order to test the effectiveness of different conservative treatments to reduce or control HV. Although many have concluded that foot orthoses at least prevent advance of the deformity, others have reported unfavourable results. Kilmartin et al. 30 studied the effectiveness of foot orthoses in adolescents with HV. After three years of treatment, the deformity was assessed by means of the HAA and the first IMA. The difference in the degree of advance of the deformity between the two groups was not significant. Tehraninasr et al. 25 studied the effect of semi-rigid foot orthoses incorporating a toe-separator compared with night splints in female patients with painful HV. A follow-up conducted at three months showed both treatments to have reduced the HAA, but not significantly. The authors concluded that these treatments could not serve to correct HV, but did prevent its progress. Also in 2008, Ferrari et al. 32 published a Cochrane review on interventions in the treatment of HV. This review included three trials that evaluated conservative treatments versus no treatment,23,30,31 finding no evidence for differences in outcome between treatment and no treatment. The evidence from these trials suggests that neither foot orthoses nor night splints appear to be more beneficial than no treatment at all.
On the other hand, a positive effect of foot orthotics in reducing or preventing the HV deformity has also been reported. Budiman-Mak et al. 33 studied the prevention of HV by means of foot orthoses in patients with active rheumatoid arthritis. After three years, the HV had advanced more in the control group than in the group using the orthotics. Tang et al. 8 studied the application of a new plantar orthosis to control foot pronation, with an incorporated toe-separator. They found that, after three months of use, the HV angle had decreased significantly. In 2009, Landsman et al. 24 published a study designed to determine the effect on foot position of medial longitudinal arch support with over-the-counter foot orthoses. After the use of these orthotics for a period of two to four weeks, X-ray evaluations showed a significant decline in the first IMA and a non-significant decline in the HAA. According to those authors, their results indicated that there was a reduction of the HV deformity, and hence that this type of treatment is effective.
As it can be observed, the results of studies on the effectiveness of foot orthoses in preventing or reducing HV have been varied. Excessive pronation of the subtalar joint favours the first metatarsal acquiring a position of dorsiflexion in the push-off phase of gait. 34 In this position of the first ray, the hallux is destabilized instead of lying flat along the ground to favour propulsion. Treatment to prevent excessive pronation of the subtalar joint in the stance phase of gait would, in theory, prevent this abnormal position of the first metatarsal, and would favour a normal push-off phase. 34 Although in clinical practice foot orthoses are often recommended to reduce the progress of HV, further studies are clearly required before one can rigorously assert that this treatment reduces the HV deformity or halts its advance.
Conclusion
At the beginning of the study there were no significant differences in the dependent variables, the HAA and the first IMA, between the control group and the experimental group, nor differences were significant after 12 months of follow up. Comparison of the values at the beginning of the study with those at the 12-month follow up within each group showed no significant differences at a significance level of p < 0.05. According to these results, there was no difference between having used the foot orthoses applied in this study, and not having used them. It therefore appears that custom-made foot orthotics had no effect in the evolution of mild and moderate HV in the women over a 12 month period.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors