
Abstract
Background: A custom moulded ankle orthosis with hinged joints potentially offers a better control over the subtalar joint and the ankle joint during lateral cutting movements, due to total contact design and increase in material strength.
Objectives: To test the above hypothesis by comparing it to three other available orthoses.
Study Design: Repeated measures.
Methods: Eight subjects with a history of ankle sprains (Grade 2), and 11 subjects without such history performed lateral cutting movements in four test conditions: 1) non-orthotic, 2) custom-moulded ankle orthosis with hinges, 3) Sport-Stirrup, and 4) elastic ankle sleeve with plastic support. A VICON motion analysis system was used to study the motions at the ankle and subtalar joints.
Results: The custom-moulded ankle orthosis significantly lowered the inversion angle at initial contact (p = 0.006) and the peak inversion angle (p = 0.000) during lateral cutting movements in comparison to non-orthotic condition, while the other two orthoses did not. The three orthoses did not affect the plantarflexion motions, which had been suggested by previous studies to be important in shock wave attenuation.
Conclusions: The custom-moulded ankle orthosis with hinges could better control inversion and thus expected to better prevent ankle sprain in lateral cutting movements.
Custom-moulded ankle orthoses are not commonly used in preventing ankle sprains. This study raises the awareness of the use of custom-moulded ankle orthoses which are expected to better prevent ankle sprains.
Background
Ankle sprain is a common injury in people involved in sports activities. Previous studies have indicated the high occurrence and recurrence rates of ankle sprain in both recreational and professional athletes.1-4 While most people can fully recovery after appropriate treatments, recurrent ankle sprains may cause significant disability and leave residual symptoms5-6 due to functional instability. 7
Many sports require some rapid changes in moving directions and lateral cutting movements.8-11 Inappropriate positioning of the ankle joint complex during such motions is a major cause of ankle sprain.7,12 This condition occurs more frequently in people with proprioceptive deficits and ligament laxity.13,14 When a foot lands in an inverted position, a high amount of inverted moment is produced at the subtalar joint producing high strain at the lateral ligament and the capsule.15,16
Some studies suggest that an ankle orthosis significantly reduces the number of ankle sprains.17-19 However, some suggested that an ankle orthosis could be ineffective, 20 and that it was not as good as technical training 21 in preventing sprains. A wide variety of ankle orthoses exist on the market. Because there is no consistency about the effectiveness of ankle orthoses in preventing ankle sprains, the decision on which design should be used is usually based on availability and subjective perception.
Some ankle orthoses reduce inversion and eversion motions of the subtalar joint but at the same time restrict dorsiflexion and plantarflexion motions.22,23 The lack of ankle motion reduces the ability to absorb shock during landing, 24 leading to increased stress over the knee joint. 16 Some utilize strapping techniques around the ankle area, and some use foam-padded, gel-padded or inflatable air bladders to provide mild control over the ankle. Previous studies did not reach a consensus about their effectiveness in preventing ankle sprain.17-20 Another approach is to custom make a plastic orthosis to fit to an individual person with a leg section and heel cup connected with a pair of mechanical hinges. The total contact design and the strength of the orthosis might give better control over the subtalar joint, and the hinges allow free plantarflexion and dorsiflexion motions. However, custom-moulded orthosis is not commonly used because of the extent of time and manpower involved.
This study compared three ankle orthoses in subtalar joint motions during lateral cutting movements. It was hypothesized that the custom-moulded ankle orthosis with hinges could have better control of the subtalar joint than the inflatable air bladders and the elastic ankle sleeve with plastic support. This study recruited subjects with and without histories of ankle sprains. It was also hypothesized that people with previous history of ankle sprains would have larger ankle and subtalar joint motions when performing lateral cutting movements.
Methods
Subjects
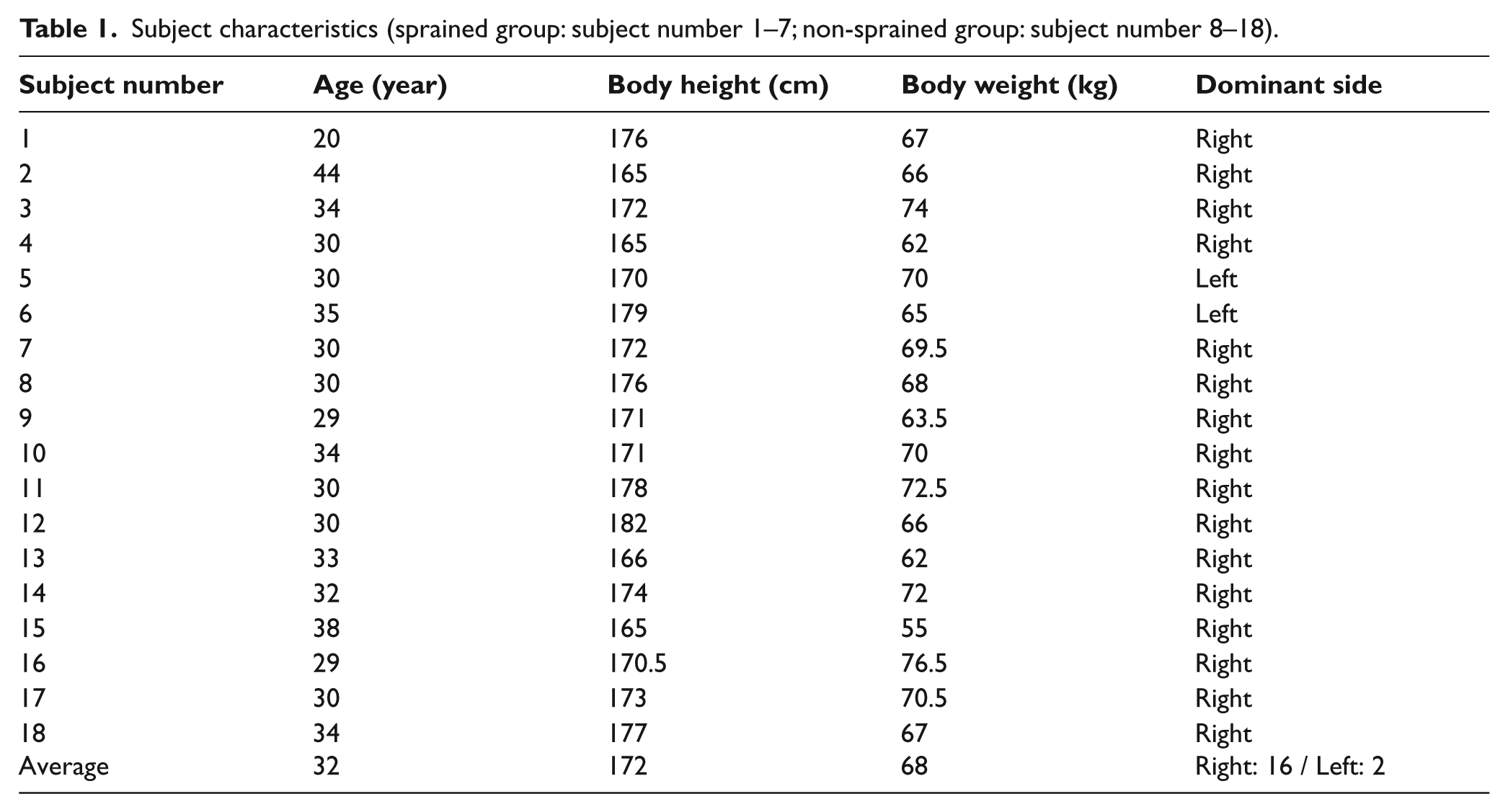
This study was approved by the Human Subjects Ethics Sub-committee of the Hong Kong Polytechnic University, and subjects gave informed consent to this work. Eight subjects (32±3 years old; 173±6 cm in body height; 67±7 kg in body weight) with a history of ankle sprains in the past 18 months (sprained group) were recruited. They had experienced an ankle sprain of Grade 2. 25 Another 11 subjects (32±5 years old; 172±5 cm in body height; 68±4 kg in body weight) without a history of ankle sprains in the past five years (non-sprained group) also participated in this study. Table 1 shows the characteristics of each subject. All 19 subjects were recreational athletes and did not have a history of lower extremity arthritis and fracture or neurological, cardiac and balance problems. They were all male so that gender effect, as reported in a previous study, 26 would not affect the results of this study.
Subject characteristics (sprained group: subject number 1–7; non-sprained group: subject number 8–18).
Orthoses and shoes
Three different ankle orthoses were tested: 1) custom-moulded ankle orthosis with hinges (Figure 1), 2) AircastTM Sport-Stirrups (DJO Incorporated, CA, USA), and 3) A60TM elastic ankle sleeve with plastic support (DJO Incorporated, CA, USA). The leg section and the heel cup of the custom-moulded orthosis were made from low-temperature thermoplastics and were fitted to the subjects by an experienced orthotist. The two sections were connected by a pair of hinge joints. The AircastTM Sport-Stirrup consisted of medial and lateral plastic bands with inner inflatable air cells that could be conformed over the malleoli. The A60TM elastic ankle sleeve with plastics support stabilized the ankle-foot complex by tightening the elastic strap around the foot and ankle over the medial and lateral plastics supports located at both sides of the malleoli. All orthoses were fitted and checked by an orthotist before the experiment. During the experiment, standardized laboratory shoes were provided to all subjects to minimize the mechanical difference that might be caused by different shoe designs. 27 To allow direct attachment of the reflective markers on the foot, openings were created at the toe-box and the posterior heel counter of the shoes.
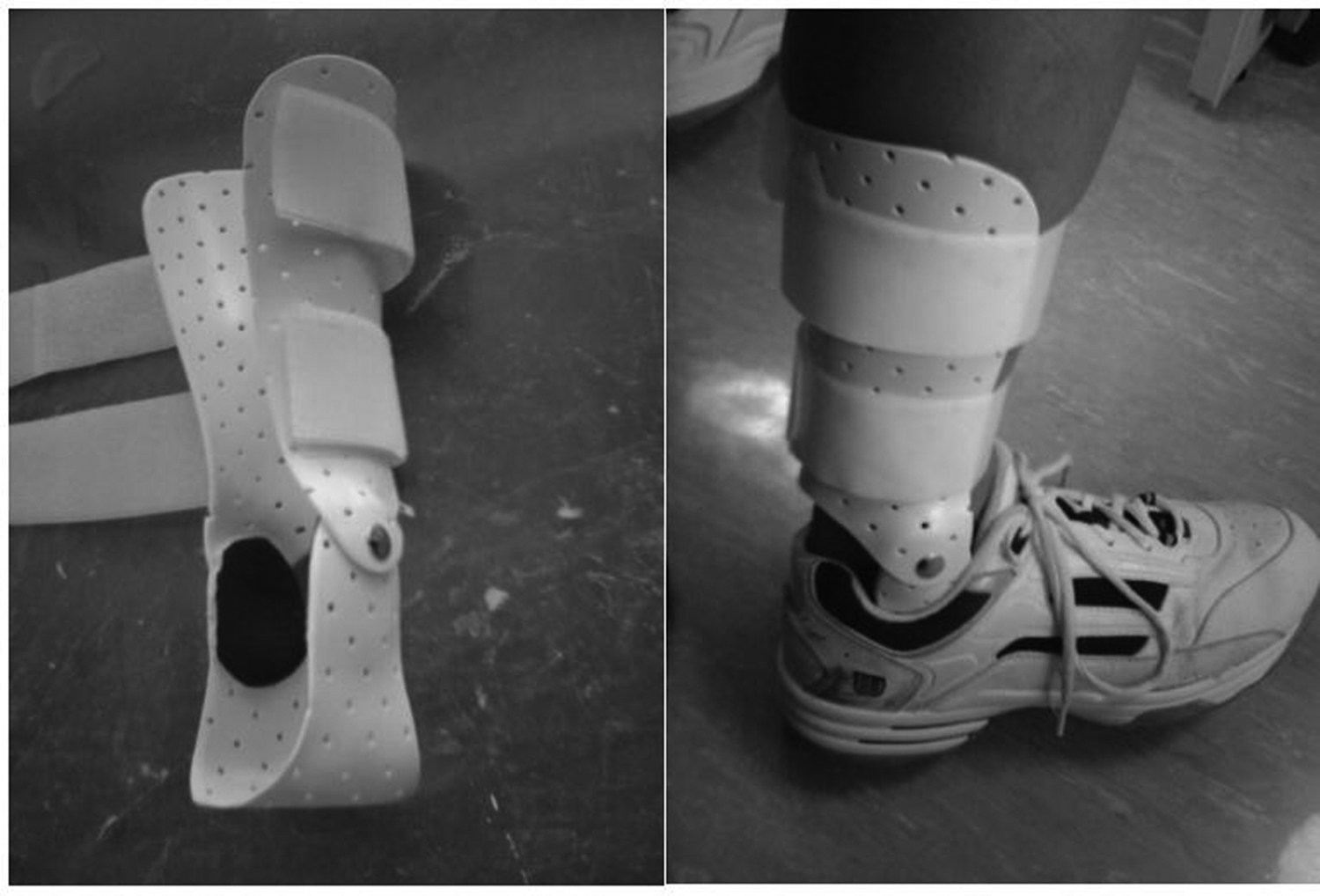
The custom-moulded and hinged ankle orthosis.
Experimental tests
Each subject was asked to perform sideward lateral cutting movements in each of the four test conditions: 1) non-orthotic, 2) custom-moulded ankle orthosis with hinges, 3) AircastTM Sport-Stirrups, and 4) A60TM elastic ankle sleeve with plastic support. The testing order was randomized. The subjects were required to shuffle laterally from a standing position for at least four steps, land onto a square marked on the floor with the dominant foot, and shuffle back to their starting positions. 22 The entire motion was performed as fast as possible. The dominant legs of the subjects were determined by identifying the sides of the leg which kicked a ball placed in front of them. All subjects were given time to familiarize themselves with the movement and each orthotic condition before data collection. The time required to complete the entire movement was measured. A trial was rejected if the time required to was not consistent with others during repeated trials. All subjects completed the movements within 10 seconds. The procedure was repeated until six successful trials were recorded with each subject for each of the three orthotic conditions. The average inversion and plantarflexion angles at initial foot contact and the peak inversion angle at the instance that the subject’s foot stepped on the marked square were evaluated.
A VICON 370 motion analysis system (Oxford Metrics Ltd, Oxford, UK) was used to collect the three-dimensional kinematics data of the dominant leg of each subject. Six infrared-emitting cameras capturing 60 frames per second were used. Reflective markers of 25 mm in diameter were attached to the lateral and medial malleoli, fibular head, tibial tuberosity, heel, as well as the first and the fifth metatarsal heads. 23 Six infrared-emitting cameras, with a sampling frequency of 60 frames per second were used to capture the image. The three-dimensional joint kinematics between each lower limb segment were calculated using Euler’s rotation theory. 28
Statistical analyses
One-way repeated measures ANOVA was performed to study if a significant difference exists among the four testing conditions in both the sprained and the non-sprained groups. Post-hoc Bonferroni tests were subsequently performed to compare each testing condition. To study if there is any significant difference between the sprained group and the non-sprained group, independent t-test was performed in each of the four test conditions. The level of significance was set at α = 0.05. When performing multiple comparisons among the four testing conditions, Bonferroni correction was performed adjusting α to be 0.008.
Results
Figure 2 shows the typical changes in inversion angles when the dominant foot stepped on the marked stance during the lateral cutting movement. As the subjects shuffled laterally, the foot was inverted throughout the entire stance time and the inversion angles had two peaks. The mean and standard deviation values at the initial floor contact and the peak comparing the four test conditions are shown in Table 2. The custom-moulded ankle orthosis significantly lowered the inversion angle at initial contact as compared to the non-orthotic condition in both the sprained (p = 0.004) and non-sprained group (p = 0.006). The custom-moulded ankle orthosis with hinges also significantly lowered the peak inversion angle, when compared to the AircastTM Sport-Stirrups, the A60TM elastic ankle sleeve with plastics support as well as the non-orthotic condition in sprained (p = 0.000) and non-sprained groups (p = 0.000).
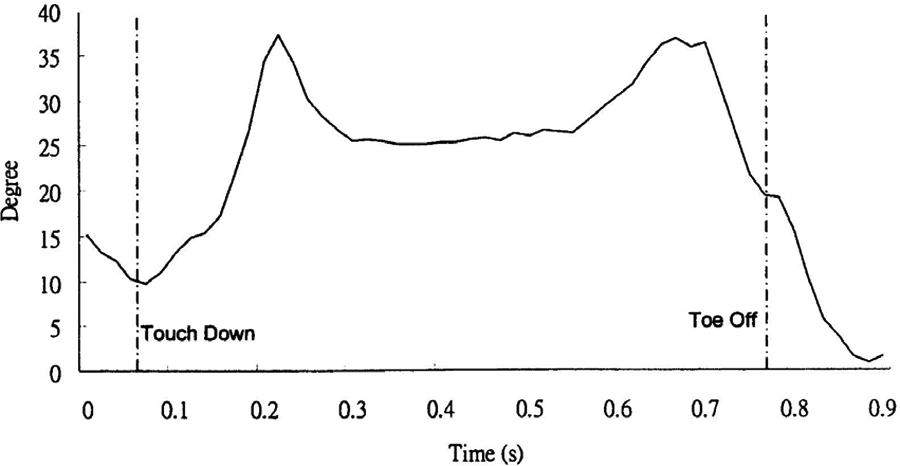
Typical changes in inversion angles in one complete stance during the lateral cutting movement
Comparison of mean plantarflexion/inversion angles and peak inversion in four test conditions and two subject groups performing lateral cutting movements.
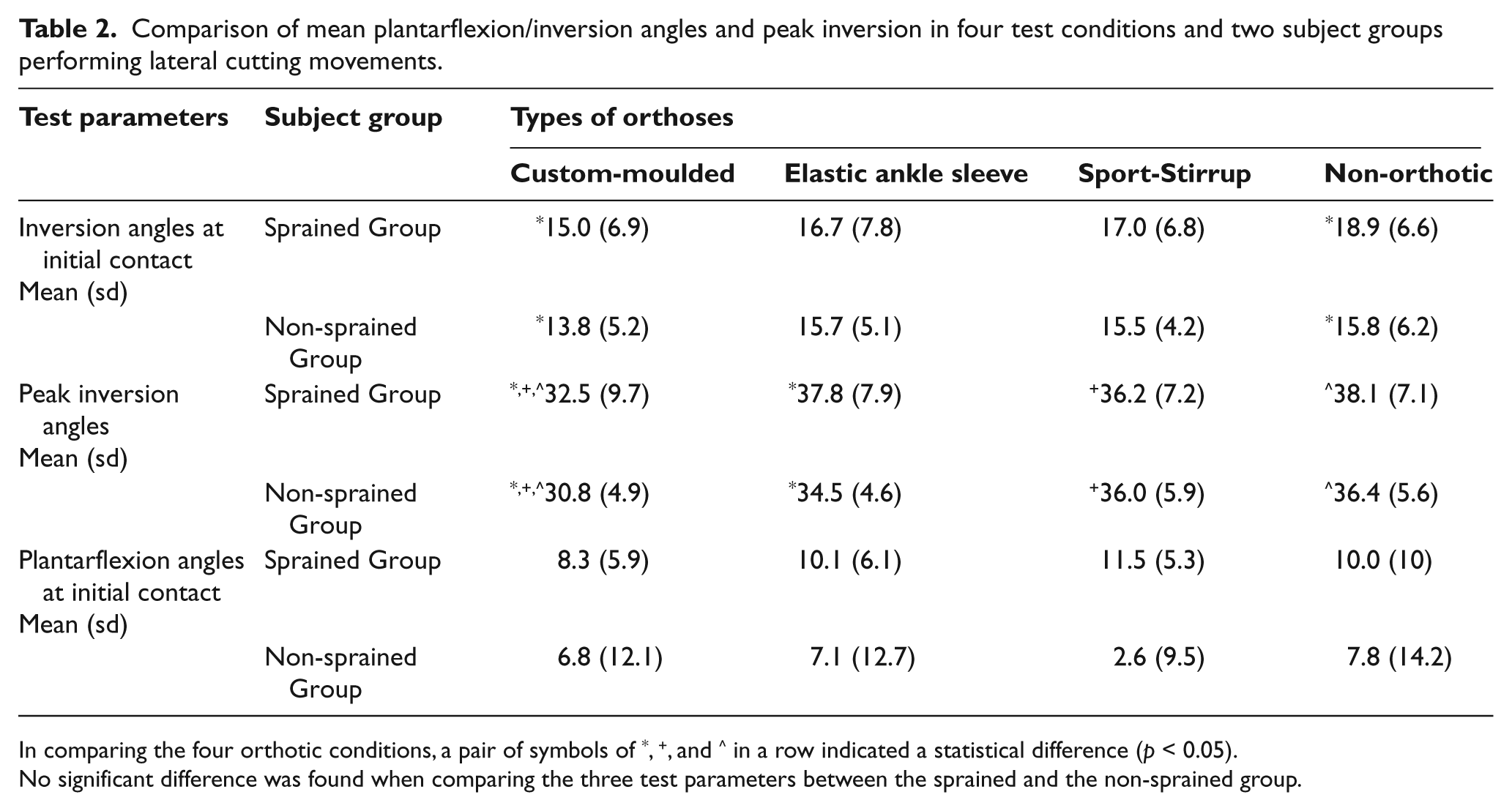
In comparing the four orthotic conditions, a pair of symbols of *, +, and ^ in a row indicated a statistical difference (p < 0.05).
No significant difference was found when comparing the three test parameters between the sprained and the non-sprained group.
The Sport-Stirrup and the elastic ankle sleeve with plastic support did not produce statistical difference in the inversion angle at initial contact and the peak inversion angle, when compared to the non-orthotic condition. Although the plantarflexion angle was on average the lowest in the sprained group when using the custom-moulded ankle orthosis, the differences in plantarflexion angles were not statistically significant among all the four test conditions.
Although the inversion and plantarflexion angles at initial contact as well as the peak inversion angles of the sprained group were on average higher than the non-sprained group in each of the test condition, the difference did not reach a statistical significance. Larger standard deviations were noted in plantarflexion angles. These suggested that various strategies in positioning the plantarflexion/dorsiflexion angles during initial contacts were used among different subjects.
Discussion
Previous studies15,29,30 identified the importance of controlling inversion in preventing ankle sprain. This study looked into the amount of control of three different ankle orthoses over the subtalar and ankle joints. Lateral cutting movements were investigated as uncontrolled inversion during commonly leads to ankle sprains. 15 It was shown that a custom-moulded ankle orthosis with hinges significantly reduced the inversion angle, while the Sport-Stirrup and the elastic ankle sleeve with plastic support did not. It suggests that the hinged ankle orthosis might outperform the two other orthoses in preventing ankle sprains during lateral cutting movements on smooth floor surfaces. More studies, however, are required to compare these orthoses in real sports activities.
Better control of the subtalar joint by custom-moulded ankle orthoses can be explained by the higher stiffness of the material used. The custom moulding of the heel cup and the leg section also enabled well fit and total contact. The orthosis did not restrict plantarflexion motions, thanks to the introduction of the hinge joints, which was suggested to be important in shock absorption. 16 Hinge joints could add prices, fabrication time, and overall weight. To confirm that the hinge joints are necessary, the hinged orthoses can be compared to non-hinged custom-moulded orthoses in future studies. While previous studies were inconsistent in determining the effectiveness of off-the-shelf ankle orthoses,17-19,20-21,31 this study provides objective information to show that the custom moulding and incorporation of a hinged joint would likely improve preventive outcomes.
The custom-moulded approach is not commonly used in treating a sprained ankle because of the time and manpower involved. However, with the objective information provided in this study, this approach should be re-considered. Further investigations are suggested in the choice of materials for the provision of lighter and more comfortable design so that the users need not sacrifice their performances with the intervention. Large contact area between the skin and the orthosis and relief over the bony prominence such as the malleoli could provide better comfort. This study was conducted in a gait laboratory in which the ground condition was different from the actual ground conditions in sports activities. Future studies can also include investigations of different orthotic designs different ground conditions and sports activities.
The specific aim of this study was to study the effectiveness of three kinds of ankle orthoses to control ankle and subtalar joint motions during lateral cutting movements. Ground reaction forces were not investigated. The effects of ankle orthoses on mediolateral forces have been investigated by other researchers,32,33 however, contradictory results were obtained. A direct relationship between ground reaction forces and ankle sprains has not yet been identified.
Conclusion
This study compared the effecitiveness of three different ankle orthoses in controlling ankle and subtalar motions when the subjects were performing lateral cutting movements. It was found that a custom-moulded ankle orthosis with hinges significantly reduced the inversion and plantarflexion angles, while the other two ankle orthoses did not. While previous studies have well documented the importance of controlling inversion, based on better control of the undesired inversion in lateral cutting movements, it is expected that a custom-moulded ankle orthosis with hinges could be more effective in preventing ankle sprain comparing to the using of Sport-Stirrup and the elastic ankle sleeve with plastic support.
Footnotes
None declared
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors