
Abstract
Background:
High rates of osteoarthritis of the knee joint of the intact limb in persons with amputation have raised concern about the long-term consequence of running. The purpose of this intervention was to determine if loading of the knee on the intact limb of a person with transtibial amputation during running could be decreased by changing the intact limb initial ground contact from rear foot to forefoot strike.
Case Description and Methods:
This study compared kinematic, kinetic and temporal-spatial data collected while a 27-year-old male, who sustained a traumatic unilateral transtibial amputation of the left lower extremity, ran using a forefoot ground contact and again while using a heel first ground contact.
Findings and Outcomes:
Changing initial ground contact from rear foot strike to forefoot strike resulted in decreases in vertical ground reaction forces at impact, peak knee moments in stance, peak knee powers, and improved symmetry in step length.
Conclusion:
This case suggests forefoot initial contact of the intact limb may minimize loading of the knee on the intact limb in individuals with transtibial amputation.
Clinical relevance
Individuals with transtibial amputation may decrease their already elevated risk for osteoarthritis by decreasing the loading forces on the knee of the intact limb when running with a forefoot ground contact.
Background
A growing number of young adults, who have had lower extremity (LE) amputation due to trauma, tumor or congenital anomalies 1 return to physically active lives. Running is a key element in their active lifestyles. Although running is beneficial for cardiovascular health, there is concern for the health of the intact limb. Increased velocity seen with running is associated with increased vertical ground reaction forces (vGRF)2,3 and increased rotational torque or moment at the knee at impact. 4 These impact forces, often measured as magnitude and rate of loading, and moments are associated with osteoarthritis (OA). 5 Osteoarthritis is typically the result of impact trauma to the articular cartilage and resulting chrondrocyte death. 6 Chondrocytes are the cells embedded within the cartilage matrix, which help to control both the synthesis and degeneration of cartilage matrix. 7 Chrondrocyte death is affected by the magnitude of the load, the rate of loading, and the number of loading cycles. 5 Individuals with amputation who compensate for limb loss by increasing the loading of the intact leg may increase their risk of OA of the knee on the intact limb.8,9 Knee OA rates as high as 65% per cent, nearly double that of the non-amputee, have been observed in individuals with amputation. 10 Therefore, efforts to minimize the amount and rate of loading in persons with amputation may be beneficial to long-term knee health.
One method of altering limb loading is to modify the manner in which the intact foot contacts the ground. The foot can contact the ground in one of three ways: rear foot strike (RFS) where the heel makes initial contact (IC) while the ankle is in dorsiflexion; mid-foot strike (MFS) where the mid- and forefoot contact the ground but the heel does not; and forefoot strike (FFS) where the metatarsal heads make IC with the ankle in plantarflexion. Lieberman et al. 11 compared impact forces of able-bodied runners using RFS and FFS while shod and barefoot. They noted an abrupt initial peak in loading, referred to as an impact transient, with RFS. The impact transient is a vertical ground reaction force (vGRF) that is 1.5 to 3 times body weight generally occurring during the first 50 ms of stance. 11 A more gradual loading rate was seen with FFS, with no impact transient. The peak magnitude of vGRF generated during the impact period was three times lower in FFS than in RFS. 11 Rate of loading was seven times slower in FFS. 11 To date, no studies have determined if these effects are also seen in individuals with amputation. The asymmetrical loading and increased risk of OA that exist in the amputee population translate to a greater need to protect the knee of the intact lower extremity while running.
The purpose of this intervention was to determine if demand on the knee of the intact limb of an individual with transtibial amputation is decreased by changing the pattern of IC of the intact limb from RFS to FFS during running. We predicted that vertical loading patterns and rotational force moments at the knee of the intact limb would be different in RFS and FFS. No significant between technique differences were expected in the kinematic or kinetic data of the amputated lower extremity because the loading pattern of the involved lower extremity remained essentially unchanged.
Case Description and Methods
The patient was a 27 year-old male who sustained a traumatic unilateral transtibial amputation. Anthropometric measurements include: height of 1.72 m; body mass of 76 kg; and residual limb length of 19 cm. The patient initiated a running program six months after amputation as part of his physical therapy program. This assessment of running gait was completed seven months post-amputation following four weeks of training with FFS. Prior to amputation this patient ran with RFS. Other injuries sustained at the time of amputation include L2 vertebral wedge fracture and mild traumatic brain injury. These conditions were fully resolved prior to data acquisition and did not impact data collection. Additional past medical history includes bilateral pars fracture at L5 as an adolescent with no evidence of spondylolisthesis that resolved with conservative, non-surgical treatment. Prior to amputation, his career required long distance runs and jumps from airplanes carrying equipment often weighing greater than 100 pounds. The patient reported use of over-the-counter non-steroidal anti-inflammatory medications to control discomfort in the low back and knees from these activities.
Prior to participation, the patient provided informed consent for clinical assessment and use of video and acknowledgement of HIPPA policies and procedures. The patient was informed and approved use of the data in this case report. A comprehensive biomechanical analysis was performed to assess kinematic, kinetic and temporal spatial parameters during running with RFS and FFS on a level 16 meter runway at a self-selected velocity. The laboratory is configured with eight embedded force plates in the center of the runway. The patient was instructed to look straight ahead in an effort to prevent targeting the force plates. Video recordings were used to verify that targeting did not occur. The subject wore a dedicated running prosthesis consisting of a carbon fiber total surface weight bearing socket with LimbLogic vacuum pump system (Ohio Willow Wood (OWW), Mount Sterling, OH); an ALS-53K suspension sleeve; an OWW medium plus 6mm contour spirit non locking liner and a junior Flex Run foot (Ossur, Reykjavik, Iceland).
Full body kinematic data were collected using 57 reflective markers and a 26 camera optoelectronic motion capture system (Motion Analysis Corporation, Santa Rosa, CA) operating at 120 Hz. The locations of 20 bony landmarks in relation to marker clusters were found by manual palpation and recorded using a digitizing pointer (C-Motion, Inc., Germantown, MD). Kinetic data were collected at 1200 Hz (AMTI, Inc., Watertown, MA). Segmental markers and landmarks were used to create an eight segment model in Visual3D (C-Motion, Inc., Germantown, MD). Local coordinate systems for each segment and angular motions of ankle, knee, and hip were defined using International Society of Biomechanics recommendations. 12 Five trials were collected for each condition, RFS and FFS. Kinetic measures, including moments, powers and loading rates, were normalized to body weight and 100% of the gait cycle. Three methods were used to verify foot strike pattern at IC for each trial. First, we visually inspected the subject while running. Next, we examined the video of each running trial to verify foot strike pattern. Finally, we compared the ankle angle at IC for each of the five trials in RFS and FFS using the kinematic data provided by the Visual 3D software.
Findings and Outcomes
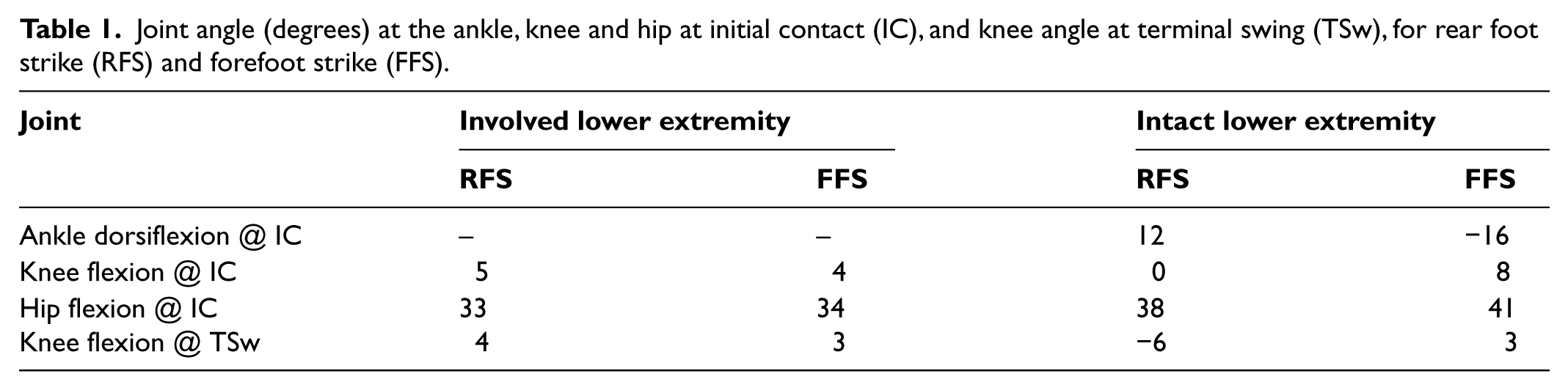
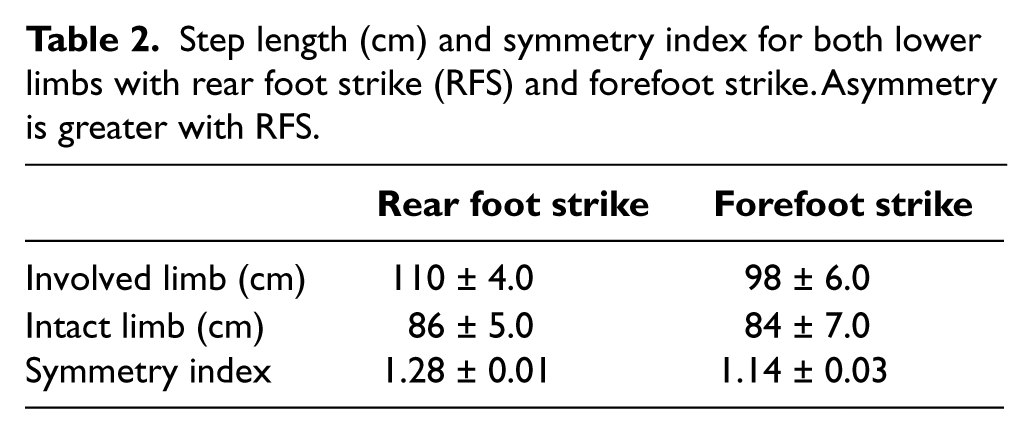
Changing initial ground contact of the intact limb from RFS to FFS resulted in changes in lower extremity kinematics and kinetics during running over level ground. As the patient modified the joint angle at the ankle to adopt a FFS running style the joint angle at the knee remained in a more flexed posture throughout the cycle (Table 1). The position of the knees at IC and terminal swing (TSw) is more symmetric with FFS. In addition, hyperextension of the knee of the intact limb noted at TSw while running with RFS is eliminated during FFS. Altering the position of the foot-ankle complex at IC from a RFS technique to a FFS technique reduced the asymmetry in step length (Table 2). This table displays the mean step length of the involved and intact lower extremities and the symmetry index (SI) for RFS and FFS. SI is a ratio of the involved limb to the uninvolved (intact) limb, denoted by the fraction i/u. A SI of one signifies perfect symmetry while deviations away from one (either greater or lower) signify increased asymmetry. The 95% confidence intervals for the means of the five trials for RFS and FFS do not overlap (the range for FFS is 1.09 to 1.20, while the range for RFS is 1.25 to 1.31); implying that there is a difference in step length symmetry between the two running techniques. Self-selected velocity was 2.8 m/s with FFS and 3.0 m/s with RFS.
Joint angle (degrees) at the ankle, knee and hip at initial contact (IC), and knee angle at terminal swing (TSw), for rear foot strike (RFS) and forefoot strike (FFS).
Step length (cm) and symmetry index for both lower limbs with rear foot strike (RFS) and forefoot strike. Asymmetry is greater with RFS.
The rate of vertical loading of the intact limb at impact was 47% lower with the FFS technique compared to the RFS technique (Figure 1A). The initial loading rate of the intact limb with RFS was 73.74 ± 8.06 N/kg/s, but only 39.31 ± 3.06 N/kg/s with FFS. An impact transient was noted only with RFS on the intact limb, whereas the rate of loading was gradual with FFS (Figure 1B). The impact transient associated with RFS occurred at 32 ms after IC, with a peak magnitude of 134 N or 1.8 times body weight. At the same point in the gait cycle, 32 ms after IC, the magnitude of vertical loading with FFS was only 81 N or 1.1 times body weight.
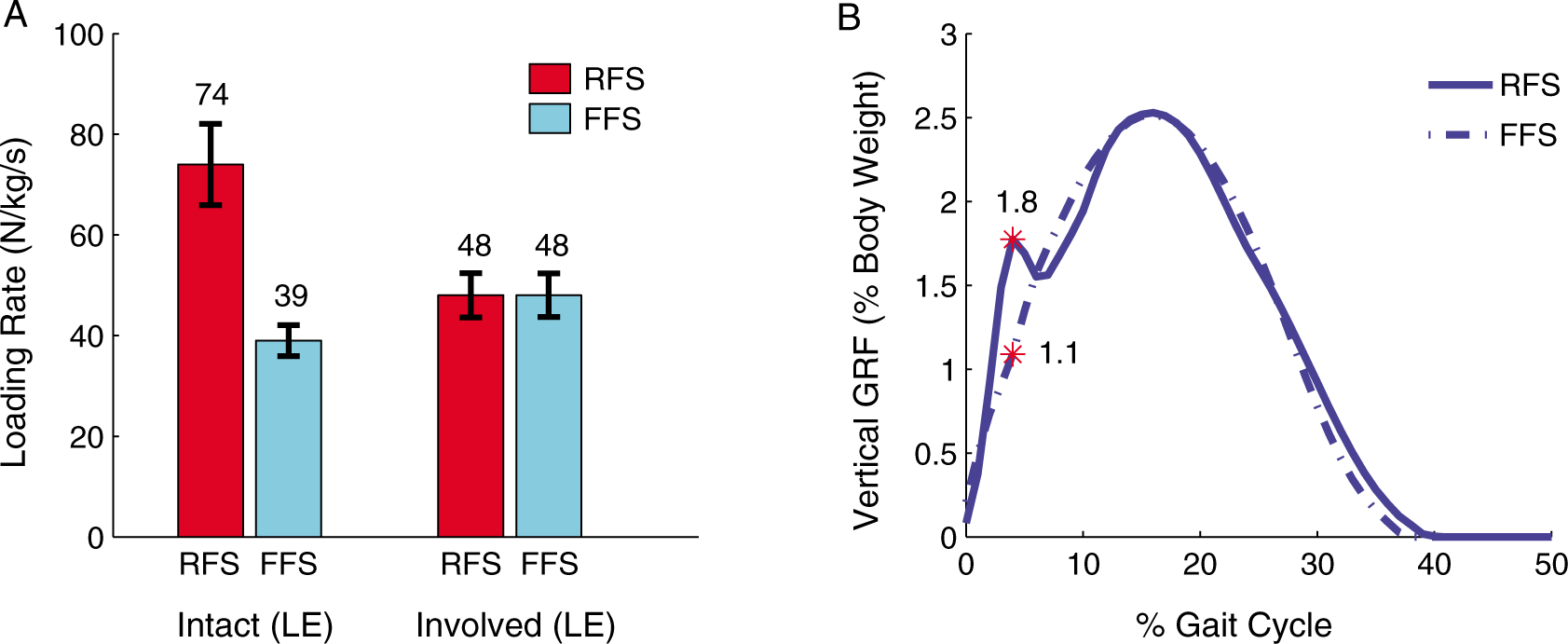
(A) Initial peak loading rate for the intact and involved extremities and (B) mean vertical ground reaction force, demonstrating the impact transient observed with RFS for the intact lower extremity.
Peak knee extensor moment decreased by 19.4% when using the FFS (Figure 2). The peak knee extensor moment of the intact lower extremity using a RFS is 2.42 ± 0.2 N·m/kg, and diminishes to 1.95 ± 0.13 N·m/kg using FFS. Peak sagittal plane negative knee power of the intact limb was nearly 50% lower while using the FFS technique (Figure 3). The peak negative power observed during early stance represents the extent to which eccentric quadriceps torque is used to control flexion of the knee. The peak negative power in early stance of the intact limb was -10.8 ± 1.3 W/kg with RFS and -5.5 ± 0.5 W/kg for FFS.
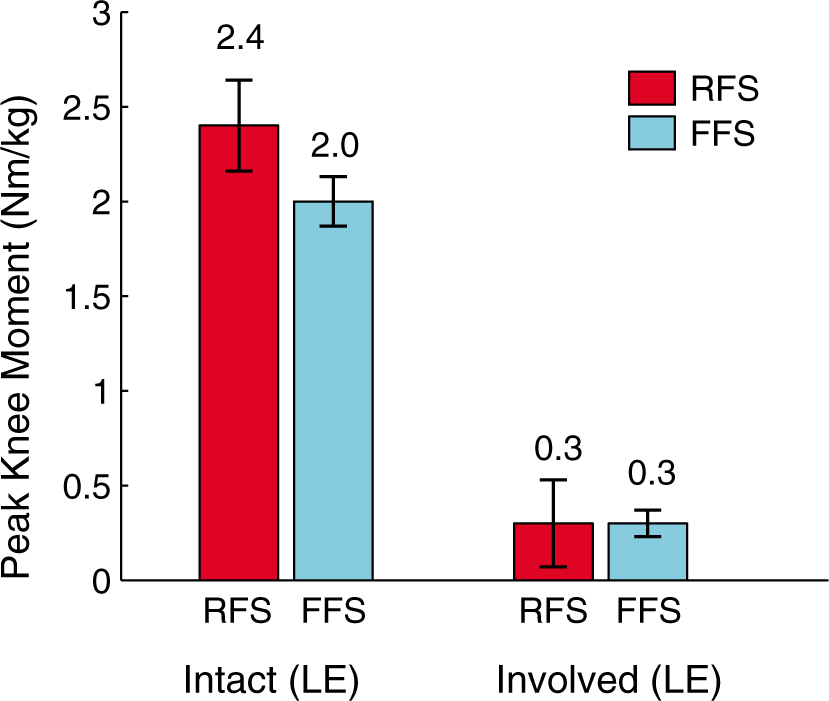
Peak knee extension moment for RFS and FFS.
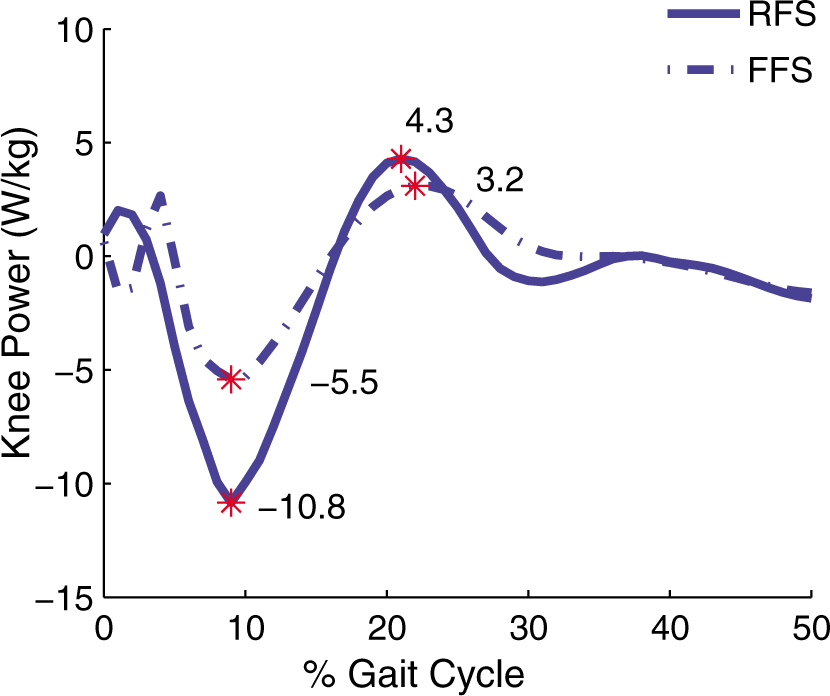
Knee joint power of the intact limb for RFS and FFS.
The patient was seen for follow-up at two weeks and at six months, and interviewed by phone at 16-months post-data collection for feedback. He continues to run three to four times per week with a weekly mileage of 16 km using the FFS technique. Although subjective and anecdotal in nature, this patient reports several observations: 1) He lands softer with less ‘stress’ on his foot-ankle complex, knee and low back of his intact limb when using the FFS; 2) FFS is more natural, more comfortable and easier to maintain than RFS. He states that running with the prosthetic leg forces him to run in a way that is similar to the FFS on the intact side; 3) He experiences less low back, knee and foot-ankle pain when using FFS.
Discussion
This is one of the first reports to show that altering initial contact while running decreases the forces on the knee of the intact limb of an individual with transtibial amputation. Both the rate of vertical loading of the intact limb during early stance phase and peak knee extensor moment were markedly lower with the FFS running technique. These results agree with previous findings in healthy, uninjured individuals during barefoot running. 11 Higher knee extension moments in early mid-stance phase have been associated with higher forces on the patellofemoral joint and increased presence of anterior knee pain. 13 The decrease in the knee moment on the intact side with FFS potentially reduces the long-term risk of developing anterior knee pain. 13 The decreased loading rate associated with FFS may be protective for the articular cartilage of the knee as the rate of loading articular cartilage has been shown to affect the severity of cartilage damage.5,6 Applying force slowly allows the forces to be dampened and distributed throughout the cartilage; whereas with rapid loading the cartilage matrix sustains greater force with little dampening, subjecting the cartilage matrix to damaging levels of stress. 5 The elimination of the impact transient, along with the lower magnitude and loading rate seen in FFS may result in less mechanical stress to the cartilage matrix with the potential benefit of improved long-term knee health. Additionally, eliminating hyperextension of the knee on the intact side during TSw may protect the posterior structures of the knee.
Greater joint angular motion, especially increased knee flexion is associated with less vGRF at impact.11,14 This is consistent with finding a lower peak magnitude of vGRF with FFS with this patient. Multiple loading parameters interact in a complex manner to determine risk of injury. These would include the magnitude, rate and frequency of loading cycles, the duration of loading cycles and rest time between loading cycles, 14 and the magnitude of rotational force moments at the knee. 4 Therefore, decreasing both the magnitude and rate of loading and/or rotational forces of the intact knee by using a FFS running technique, may decrease injury to that joint.
The sprinting gait of individuals using a dedicated running prosthesis has previously been described as an ‘up on the toes’ gait. 15 These carbon fiber prosthetic feet are designed and aligned to simulate a FFS. These feet are designed without a heel component with only a small, anterior, distal area of the prosthesis in contact with the ground during stance. The overall height of the prosthetic leg is increased to accommodate a decrease in vertical height of the prosthetic foot due to compression when loaded. The increased length and limited area of the prosthesis in contact with the ground simulate a FFS position on the involved side. Therefore, running with a FFS on the intact side creates more apparent symmetry between involved and intact limbs.
The running specific carbon fiber prosthesis acts as a simple spring, deflecting when loaded and returning to its original position when unloaded, to store and release energy. Initial contact on the involved limb remains essentially unchanged; therefore the change in foot strike on the intact limb had essentially no influence on the kinematics or kinetics of the amputated limb (Table 1).
Risk of injury is a concern to all runners. Although injury associated with a RFS technique has been well documented, there is presently no data available to indicate that the risk of injury is increased with FFS initial contact as compared to RFS initial contact. As with any intervention, it must be tailored to the needs of the individual. If the individual has any comorbidity that includes instability in the joints of the intact lower extremity, especially ligamentous damage to the ankle resulting in chronic ankle sprains, this may not be a suitable running technique.
Conclusion
The results of this case indicate between technique differences in loading rate and knee moments in the intact leg of an individual with transtibial amputation while running. Based on these results, this individual with transtibial amputation who ran with a forefoot IC decreased the forces on the knee of the intact lower extremity and may be at reduced risk for OA of that joint. Although promising, the results from one patient cannot be extrapolated to the larger population of individuals with amputation. Further study is necessary to fully understand the extent to which running technique influences loading rate and knee moments following transtibial amputation.
Footnotes
Acknowledgements
The authors would like to thank Kelly Rodriguez, MS and Emily Sinitski, BS for their assistance with data collection and data processing; Marie Black, MPT for her role in treating the patient and reviewing the manuscript; and Deanna Gates, PhD for her assistance in reviewing and editing the manuscript.
Funding
Support provided by the Military Amputee Research Program.
Conflict of interest
The authors declare that there is no conflict of interest.