
Abstract
Background: Postural asymmetries are thought to lead to impairment of body structure and function such as muscle imbalance, gait asymmetry and possible chronic conditions, which result in limitation of mobility and restriction of daily activity for transfemoral amputees (TFAs). Despite the potential clinical impact, postural asymmetries have not been confirmed or quantified in TFAs.
Objectives: To identify the presence of postural asymmetries in TFAs utilizing clinical evaluation measures.
Study design: An observational cross-sectional study in which participants were evaluated at a single time point without intervention or follow-up.
Methods: Forty-seven unilateral TFAs were measured for standing limb length, pelvic innominate inclination (PII), lateral trunk flexion and hip extension.
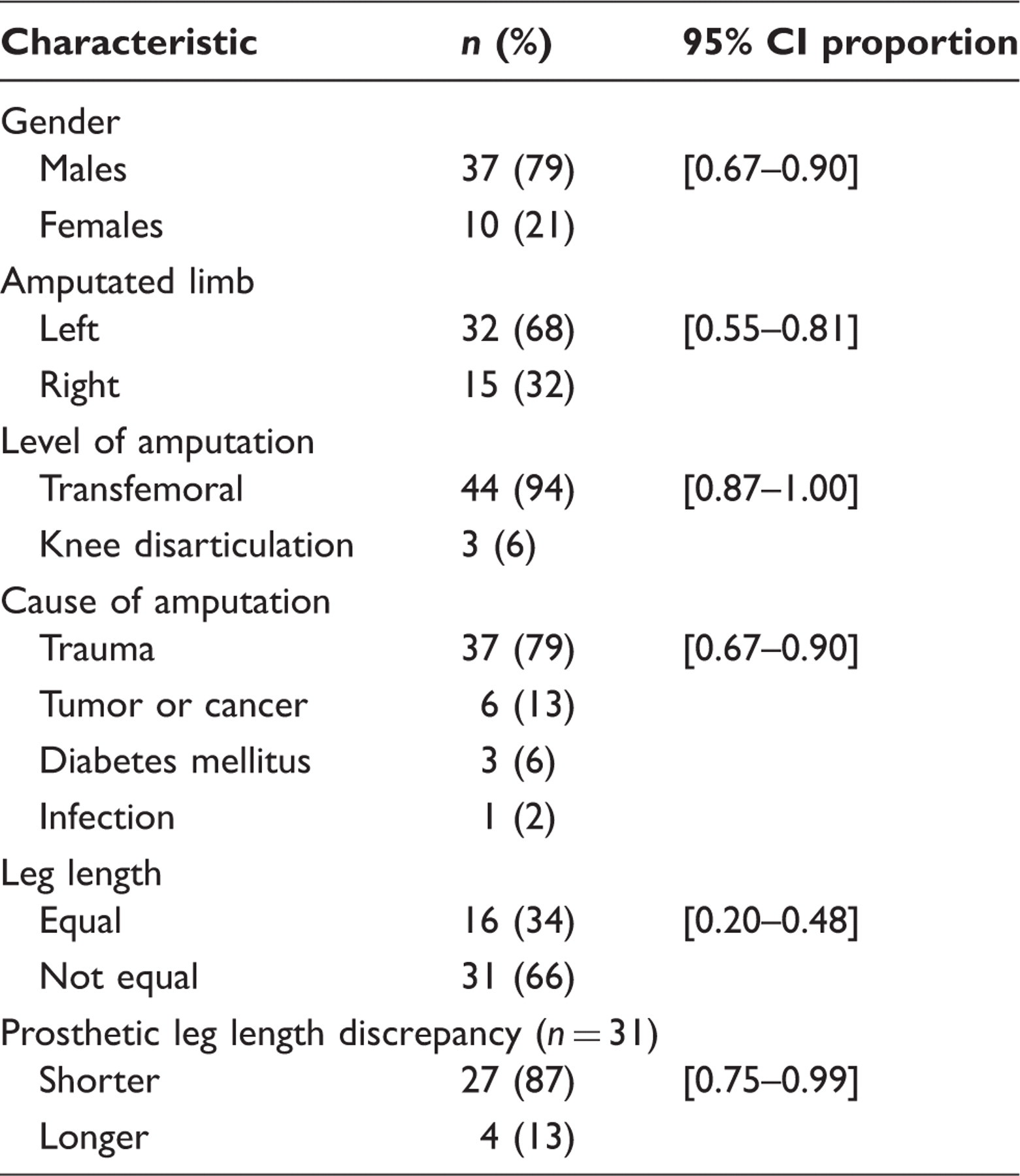
Results: Limb length discrepancy was present in 66% of participants and 57% had a short prosthetic limb. PII was greater than has been reported in the literature, and the shorter the prosthetic lower limb, the greater the PII on the amputated side (r = −0.422, p = 0.004). Limb length discrepancy and decreased lateral trunk flexion accounted for 26% of the variance in amputated side PII.
Conclusion: Three postural measurements, namely leg length, pelvic innominate inclination and hip extension, were found to differ between the intact and amputated limb in this study sample.
Clinicians should include postural assessment as part of their routine evaluation of TFAs in an effort to achieve postural symmetry and reduce the risk of chronic conditions associated with impairment of body structure and function.
Introduction
Clinicians have assumed that, over time, transfemoral amputees (TFAs) will experience musculoskeletal adaptations at the trunk and pelvis. Musculoskeletal adaptations may be defined as alterations in muscle, connective tissue and bone in relation to posture or repetitive movements of daily activity. Musculoskeletal imbalances at the trunk and pelvis resulting in differences in muscle length, connective tissue extensibility and skeletal alignment may be defined as postural asymmetries. 1,2 Postural asymmetries that have been associated with TFAs include limb length discrepancy, pelvic innominate inclination, limitations in lateral trunk flexion and hip extension (tight hip flexor muscles). To date there has been inadequate description and quantification of postural asymmetries in TFAs in the literature.
Limb length discrepancy (LLD) in unilateral TFAs can be treated by clinicians by adjusting the height of the prosthesis. In some cases the prosthesis may be intentionally shortened with the expectation of improving toe clearance during ambulation. 3 While the benefits for ambulation of a shorter prosthetic limb are unclear, the resultant leg length discrepancy during standing has been associated with impairment of body structure and function. 4,5 Although contentious, the non-amputee literature associates LLD (0.5–3.0 cm) with greater incidence of low back pain; 6 – 8 increase lumbar lordosis; 9 emergence of functional scoliosis; 7,10 compensatory spinal actions; 7,11 – 13 lateral pelvic tilt 13,14 and greater oxygen consumption during walking, 15 as well as increased limb loading 16 – 18 and stance time through the longer lower limb. 17 – 20 Many issues associated with LLD have also been described in people with limb loss. 21 Friberg, the first to report LLD in lower limb amputees, found that 85% of lower limb amputees presented with a short prosthetic lower limb, 66% having LLD greater than 1.0 cm and 34% greater than 2.0 cm. 3
Pelvic innominate inclination (PII), also referred to as rotation, is defined as the angle in the sagittal plane between the horizontal line and the line passing through both the anterior superior iliac spine and the posterior superior iliac spine. 13 Sanders postulated that TFAs undergo musculoskeletal adaptation at the pelvis because of their inability to flex their prosthetic knee during the terminal stance phase of gait. 22 The inability to flex the prosthetic knee during late stance phase results in an increase in PII from 3° to 10° in order to achieve 15° of lower limb extension and therefore an equal stride length. 22 The increased PII necessary during ambulation may contribute to the increased lordosis frequently observed in TFAs. 22 Although the increased PII is frequently noted, no literature has been found that quantifies the altered rotation.
The relationship between LLD and PII has been examined in the non-amputee population but not in the amputee population. In non-amputees, LLD causes anterior PII on the shorter limb and posterior PII on the longer limb. 13,23 An inclination difference between the two innominates in the sagittal plane is called pelvic innominate asymmetry (PIA). 13 Pelvic innominate asymmetry could lead to asymmetrical loading of the lumbosacral ligaments and predispose an individual to chronic strain. 23 The relationship between LLD and PII in TFAs merits investigation to determine if it is similar to that seen in non-amputees.
Leg length discrepancy may also have an effect on LTF during standing and gait. Lateral trunk lean has often been described as an observable postural and gait deviation in TFAs. 24,25 While differential diagnoses for the anatomical structures at fault for the limitation of lateral trunk flexion are complicated and not well defined, gross assessment of lateral motion of the trunk can assist in determining if a limitation exists.
Likewise, hip flexor muscle tightness or limitation in hip extension have been frequently described as a postural restriction, associated with short residual limbs in TFAs who sit for long periods of time or have other postural issues. 26,27 Hip flexion contractures require alignment accommodation such as additional socket flexion to allow for hip extension. Although hip extension limitation has been associated with increased lumbar lordosis, 28,29 its relationship with other postural asymmetries such as LLD and PII has not been investigated in TFAs.
The purpose of this study was to offer clinicians and investigators baseline values for clinical assessment, treatment, and future research regarding TFA posture, by quantifying four variables associated with postural asymmetries, namely LLD, PII, lateral trunk flexion and hip extension, and determining whether a relationship exists between these variables. We hypothesized that TFAs would present with short prosthetic limbs, increased pelvic innominate inclination and decreased lateral trunk flexion toward the intact side, and that those with increased PII would have a decrease in hip extension.
Methods
Study design
This investigation was an observational cross-sectional study in which participants were evaluated at a single point in time without intervention or follow-up. Participants were recruited as a convenience sample at the Functional Outcomes Research and Evaluation (FORE) Center at the Miami Veterans Affairs Healthcare System (VAHS) and at an amputee organizations annual meeting. The study protocol was reviewed and approved by Human Studies Subcommitte and the Institutional Review Board (IRB) at the Miami VAHS. Informed written consent was obtained from each participant prior to enrollment. A licensed physical therapist acted as the examiner and performed all evaluation and testing procedures.
Inclusion and exclusion criteria
Of the 52 individuals screened, 47 met the inclusion criteria and were enrolled. Participants were healthy men and women aged 28 to 75 years who had undergone a unilateral transfemoral or knee disarticulation amputation at least 12 months prior to enrolment. The inclusion criteria required participants to ambulate independently of an assistive device.
Study procedures
Study procedures were explained to the participants and those who met the inclusion criteria and were interested in participating underwent the informed consent process. Standard demographic information was collected.
Limb length discrepancy (LLD) was determined using the indirect method with the pelvic leveling device and block method (Figure 1a).
30
The indirect method has been reported to have good intrarater and interrater reliability and is considered a good measure of LLD.
30
Participants stood comfortably in their prosthetic limb with a base of support of 10 cm. If needed, manual corrections were performed to the head, trunk and pelvis in order to achieve a symmetrical standing posture. The iliac crests were identified by palpation and a pelvic level was used to assess limb length equality. If unequal limb length was present, the examiner corrected the discrepancy by placing a combination of 0.64 cm (0.25 inch) step boards under the foot of the shorter limb. The participant was measured again with the pelvic level to ensure limb length equality.
Clinical evaluation measures for transfemoral amputees. (a) Indirect method via pelvic leveling device and block method; (b) Laser-Line™ standing pelvic innominate inclination measurement; (c) lateral trunk flexion finger-tip movement technique; (d) the modified Thomas Test.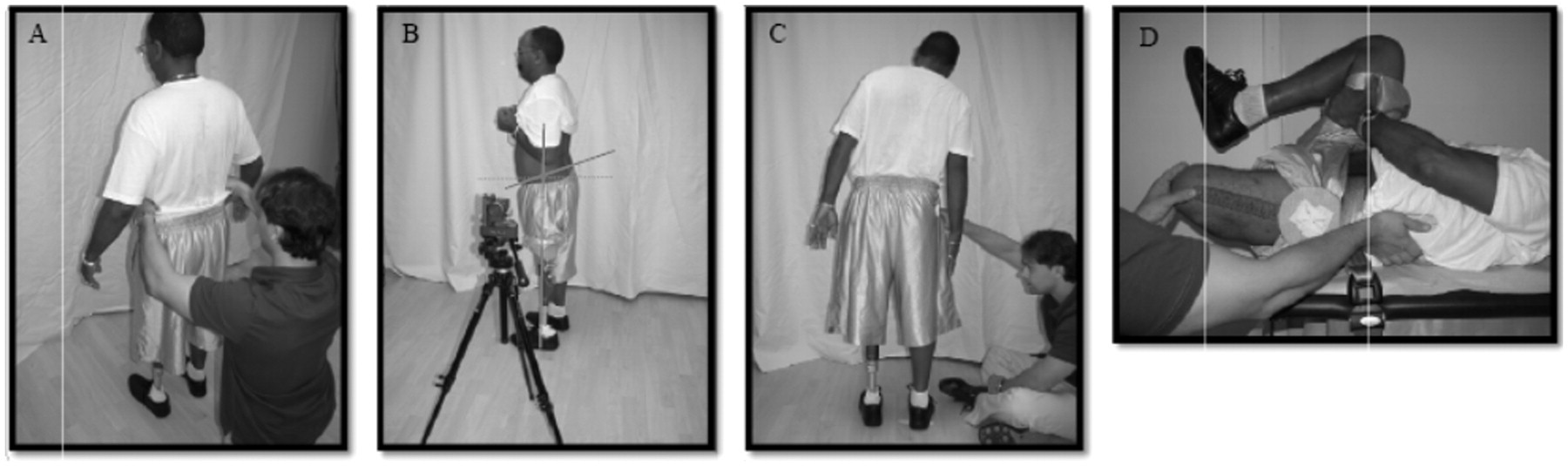
To measure PII during standing, the participant’s greater trochanter (GT), anterior superior iliac spine (ASIS) and posterior superior iliac spine (PSIS) were identified bilaterally using standard anatomical palpation techniques and marking them with adhesive tape. These landmarks have been found to have reasonable accuracy when compared to X-ray measurement in determining PII in the sagittal plane. 30 Della Croce et al. reported that intra-examiner precision was superior to inter-examiner precision and a minor degree of error was associated with identifying pelvic and femoral anatomical landmarks using standard palpation techniques. 31 For these reasons, a single examiner was used to identify anatomical landmarks throughout the study. The examiner measured PII in the sagittal plane using the Laser-Line™ (Otto Bock®, Duderstadt, Germany) (Figure 1b). The Laser-Line™ projects two bisecting lasers and records the relative angle between them to within 1 degree. The vertical line was aligned with the GT. The horizontal line began at the neutral position (perpendicular to the vertical line) and was rotated until it bisected the ASIS and PSIS markers. The angle between the neutral position and the rotated horizontal line was measured bilaterally.
The fingertip movement technique was used to measure LTF limitations in the frontal plane (Figure 1c). 32 – 33 Frost et al. reported good interrater and intrarater reliability when using the fingertip movement technique to measure lateral trunk flexion (LTF). 34 From standing, participants flexed laterally to one side as far as they comfortably could, while their upper limb remained relaxed on the side of the torso. At the end of the movement, the vertical distance from the participant’s third finger to the floor was measured. Measurements were taken bilaterally to the nearest 0.5 cm using a standard tape measure.
Residual limb length was measured while lying supine on an examination table with the prosthesis removed. Length was measured to the nearest 0.5 cm in the sagittal plane from the GT to the distal end of the lateral femur.
The hip flexors were evaluated using the modified Thomas Test (Figure 1d), which determines hip flexion tightness by measuring hip extension range of motion (ROM) with a universal goniometer. 35,36 The interrater and intrarater reliability of the modified Thomas Test has been found to be excellent with a universal goniometer. 37 Participants lay supine on an examination table with their prosthesis removed and their intact foot on a step stool on the floor. To prevent anterior pelvic tilt and maintain a flat lumbar spine, a participant’s pelvis was secured against the table with a pelvic stabilizing belt across the ASISs. Prior to taking measurements, the examiner confirmed that participants were able to bring the residual or intact limb into a neutral position without soft tissue resistance, to rule out the presence of abductor contractures. Participants flexed and held the intact lower limb to their chest. Two measurements were taken: resting hip extension, which is the angle of hip extension in a gravity-dependent position, and end-range hip extension, which included manually-applied over-pressure on the residual limb. 35 These measurements were taken bilaterally. The examiner was blinded to the results of the measurement by using a universal goniometer with single-sided numerals.
A non-amputee control group was not recruited because internal control with respect to comparison between the prosthetic and intact limbs was used for all variables including limb length, PII, LTF and hip extension.
Data analysis
The statistical software used for data management and analysis was SPSS for Windows version 17 (SPSS Inc., Chicago, IL). Statistical techniques used included one sample t-tests, paired samples t-tests, Spearman and Pearson correlation analysis, and multiple linear regression analyses. One sample t-test was used to assess the statistical significance of the mean of the LLD measurements obtained via the indirect method. Paired samples t-tests were used to assess the difference between the intact and amputated side with respect to measurements of PII, LTF, resting hip extension and end-range hip extension. Positive values for these differences indicate greater values for the side of the intact limb. To reduce error related to LLD, the LTF measurement on the amputated side was corrected for participants who presented with a longer or shorter prosthetic lower limb. The correction consisted of adding the LLD to the amputated side LTF measurement. The corrected value was utilized for statistical analysis.
The block method used to determine LLD resulted in a variable with multiples of 0.64 cm (0.25 inch). Spearman correlation analysis was used to assess the association between LLD and PII. Pearson correlation analysis was used to determine the degree of association between amputated side PII and amputated side end-range hip extension and amputated side PII and intact side LTF, respectively.
Multiple regression analysis was performed to determine if amputated side PII was predicted by prosthetic limb length, restrictions in LTF, hip extension and residual limb length. One participant was removed from the regression analysis because the presence of a unilateral elbow flexion contracture altered the standardized method of measurement for LTF.
Results
Characteristics of study participants (n = 47).
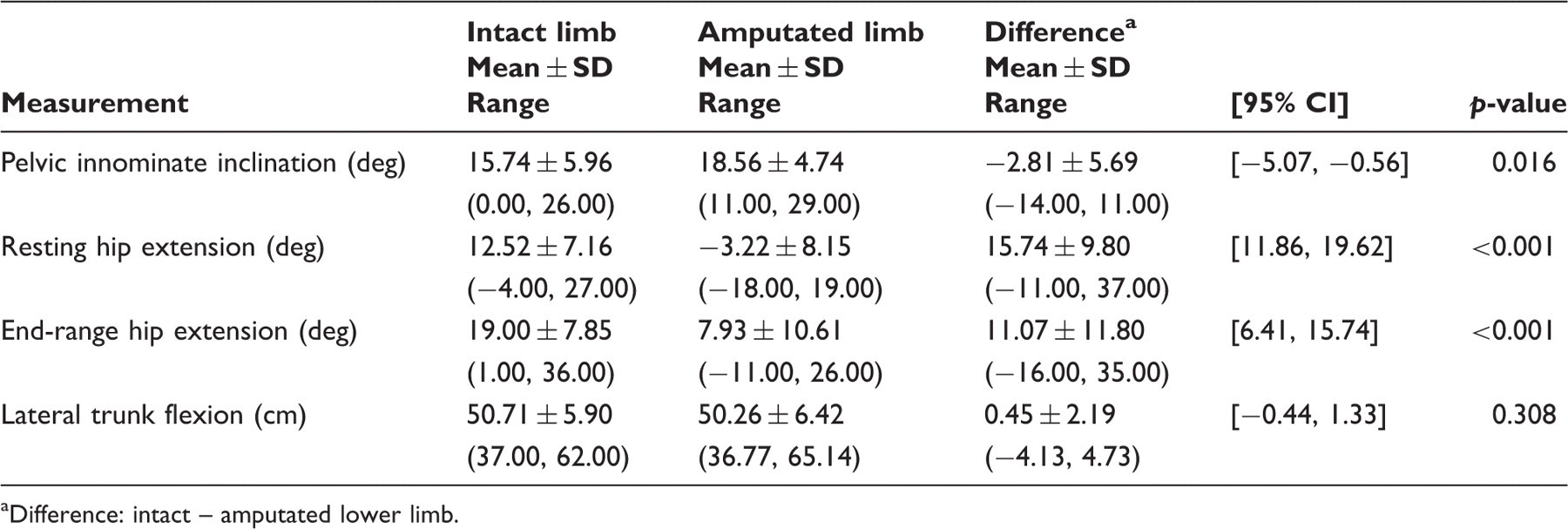
Posture measurements for all participants (n = 47).
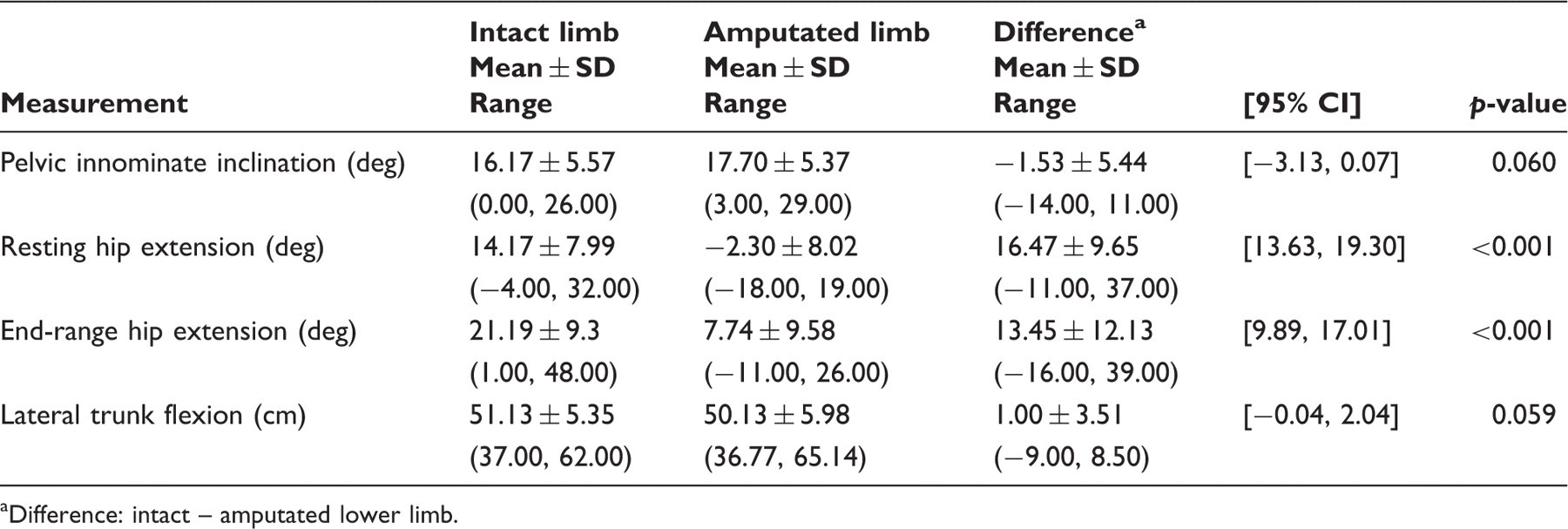
Difference: intact – amputated lower limb.
Posture measurements for participants with equal lower limb length (n = 16).
Difference: intact – amputated lower limb.
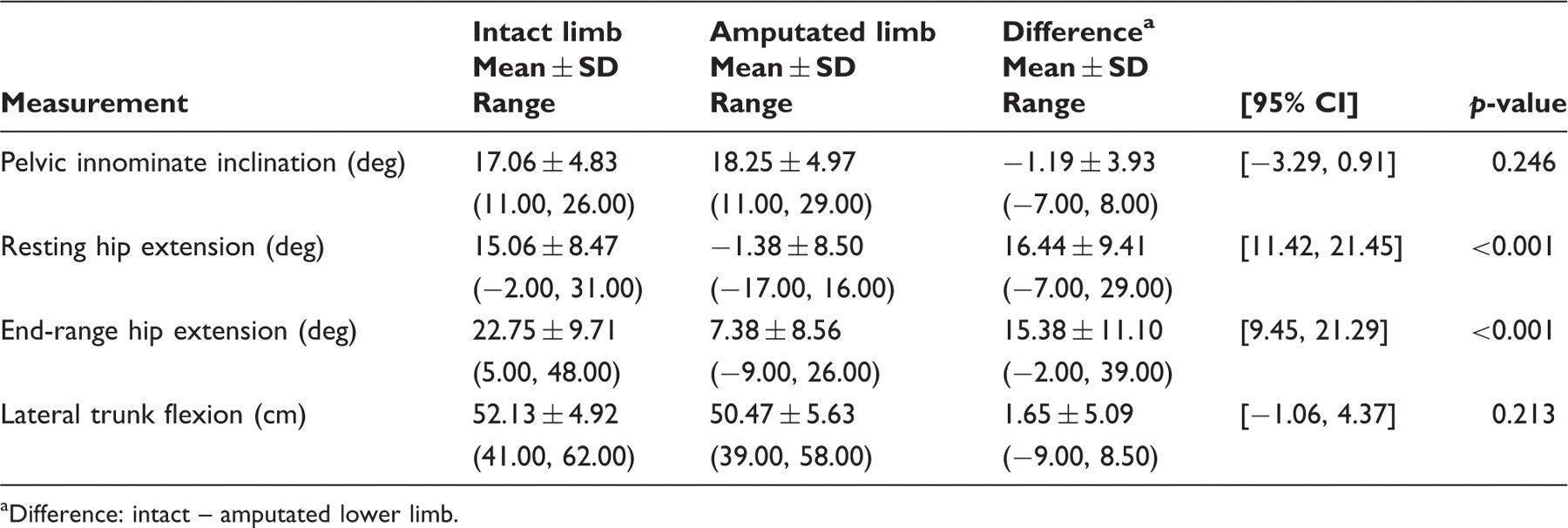
Posture measurements for participants with a short prosthetic limb (n = 27).
Difference: intact – amputated lower limb.
Spearman rank correlation analysis suggests that the shorter the prosthetic lower limb, the greater the amputated side PII (n = 47, r = −0.422, p = 0.004). Pearson correlation analyses suggests that the greater the amputated side PII, the less intact side LTF (n = 46, r = 0.31, p = 0.038). No correlation was found between amputated side PII and end-range hip extension (n = 47, r = −0.18, p = 0.23) indicating that increased PII was not related to decreased hip extension.
Linear regression analyses were performed to assess if LLD (X1), intact side LTF (X2), amputated side end-range hip extension (X3) and residual limb length (X4) were predictors of amputated side PII (Y). Analyses of separate models for the linear regression of Y on each of the independent variables indicated that LLD and LTF were statistically significant predictors of amputated side PII (p = 0.006 and 0.038, respectively, but that amputated side end-range hip extension (X3) (p = 0.225) and residual limb length (X4) (p = 0.093) were not statistically significant predictors of Y. Only X1 and X2 were entered in the final multivariate regression model, and they accounted for 26% of the variability in amputated side PII (R 2 = 0.263, F(2, 43) = 7.66, p = 0.001). X1 accounted for 16% and X2 for 10% of the variance, respectively.
Discussion
The purpose of the study was to identify and quantify the presence of postural asymmetry in TFAs with regard to LLD, PII and restriction in LTF and hip extension. The study results were consistent with earlier findings by Friberg regarding the percentage of participants who presented with prosthetic LLD. 3 The mean prosthetic LLD in the short prosthetic limb group was 1.13 cm (SD = 0.54) which is comparable to that reported for TFAs measured during static standing using instrumented gait analysis. 38 The clinical implications of this amount of LLD in TFAs has not been determined. In the non-amputee population, LLD of 1.13 cm is associated with postural asymmetries that lead to impairment of body structure and function, such as low back pain, 6 – 8 impaired balance 4 and gait asymmetry. 17 – 20
Comparisons of PII between intact and amputated limbs in TFAs have never been reported in the literature. A range of 8.4 to 11.3 degrees PII has been reported in the non-amputee population. 39 – 41 For transtibial amputees, PII has been found to be 12 degrees, without reporting whether differences exist between intact and amputated limbs. 42 The PII results for the TFAs are greater than for non-amputees and transtibial amputees, with a mean range of 16.17 to 17.70 degrees on the intact and amputated limb, respectively.
The TFAs were divided into two groups; those with equal lower limb length and those with a short prosthetic limb. TFAs with equal limb length did not present with differences in PII between intact and amputated limbs. TFAs with a short prosthetic limb presented with significant differences in PII between intact and amputated limb, with less PII on the intact limb side. The difference in PII is consistent with prior reports from non-amputees, suggesting that a longer lower limb length promotes posterior PII. 13,23 Moreover, a fair correlation was found between a shorter prosthetic limb and PII, suggesting that the clinical practice of shortening the prosthetic limb may have an effect on TFA posture. Although this study did not examine the clinical implications, arguably an asymmetrical loading of the anatomical structures has been associated with the potential for low back pain. 23
It was found that increased amputated side PII was correlated with restriction of LTF. The cause of restricted LTF is difficult to determine because no clinically friendly tests exist to differentiate the tissues at fault. Spinal column restrictions and muscle shortening may limit LTF motion. Because of the complexity of the trunk and pelvis, however, it is difficult to determine the specific musculoskeletal tissues restricting motion.
Surprisingly, limitations in hip extension and PII were not related. Several muscles are involved in hip flexion or restriction of hip extension, yet the iliopsoas is the only primary hip flexor that remains intact following transfemoral amputation.
43
The results demonstrated that hip extension ROM was significantly less on the amputated side than on the intact side
The study found that 57% of TFAs in the sample population presented with a shortened prosthetic limb, increased PII and tighter amputated side hip flexors. These results support the relationship between hip flexors, back extensors and abdominal muscles. These muscle groups, which help to prevent postural asymmetries at the pelvis,
46
may contribute to postural imbalances in TFAs. Figure 2 illustrates the potential contribution to imbalance on the amputated and intact sides. If the iliopsoas, acting as the primary hip flexor, becomes shortened, a muscle imbalance could occur between the back extensors, abdominals and hamstrings (Figure 2a). As an increase in anterior PII occurs, the back extensors are placed in a shortened position resulting in increased lumbar lordosis (Figure 2a). The abdominal muscles, which are now in a lengthened position, have reduced force potential (Figure 2b). The hamstring muscles, which have been cleaved, reattached either by myodesis or myoplasty and atrophied,
29,47
are unable to counteract the taut back extensors to keep the pelvis in a neutral position (Figure 2b). The intact side of the TFA presents with muscle length change that is similar but less dramatic due to the intact hamstrings (Figure 2c).
The relationship between the hip flexors, back extensors, and abdominal muscle (shaded in grey) at the pelvis of transfemoral amputees: (a) Shortened hip flexors and taut back extensors promote pelvic innominate inclination. (b) The lengthened abdominal muscles and atrophied hamstring muscles are unable to counteract the shortened hip flexors and back extensors to keep the pelvis in a neutral position. (c) The intact side presents with similar yet less dramatic muscle length change due to the intact hamstrings (reproduced with permission from Advanced Rehabilitation Therapy, Inc. Miami, Florida, illustration by Frank Angulo).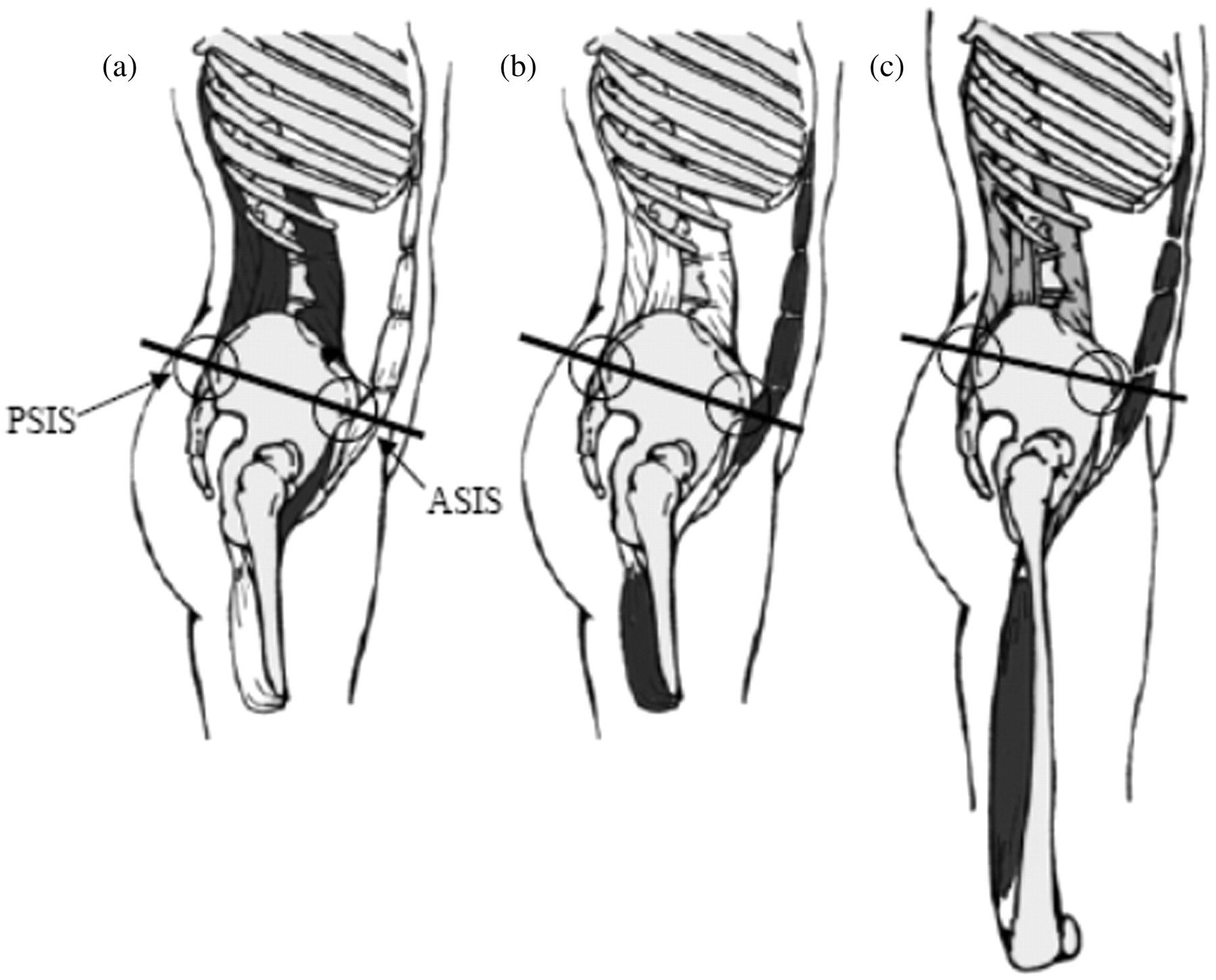
Regression analysis suggests that LLD and restrictions in LTF are moderate predictors of amputated side PII, accounting for 26% of its variability. Even though other musculoskeletal factors not investigated in this study also contribute to PII, clinicians should assess for LLD and restrictions in LTF in the transfemoral amputee population.
The long-term consequences of LLD, PII, LTF and decreased hip extension in TFAs have not been determined and are beyond the scope of this study. Future research should examine the long-term effects and associated chronic conditions that may be related to postural asymmetries. Moreover, standardized assessment methods and treatment interventions, if required, should also be investigated with the goal of reducing limitations of mobility and restrictions of daily activity for TFAs.
There were several limitations to this study. The reliability and validity of the indirect method have been examined in the literature and deemed both acceptable and unacceptable by different authors. 30,48,49 The indirect method was determined to be the most clinically feasible means for measuring LLD in TFAs because (1) it measures the participant during standing, (2) it avoids testing error associated with the direct method, which requires identifying standard lower limb landmarks absent in this population, and (3) it avoids supine measurement which involves the distraction and subsequent false lengthening of the prosthetic lower limb. Unfortunately, the indirect method is unable to determine which prosthetic components proximal or distal to the prosthetic knee unit are at fault for the LLD.
PII was measured in the sagittal plane using the Laser-Line™ (Figure 1B). Interrater and test–retest reliability of the Laser-Line™ as a clinical tool warrant future research in non-amputee and amputee populations. Future research should address concurrent validity of the Laser-Line™as compared to Saunders’ technique for measuring PII. 50 The fingertip movement technique has been found to be a reliable measure of LTF. 32 However, two additional components should be added to the test: (1) if LLD is found and corrected via the block method, the participant should be measured with the corrected limb length, and (2) measurement points should be taken at the starting position and at the end of the perpendicular movement in order to determine the excursion.
Conclusion
Clinical evaluation measures were utilized to determine baseline values and the presence of postural asymmetries in TFAs. In this study, 66% of participants were found to have LLD with 57% having a short prosthetic limb. PII was found to be greater in TFAs than in the general population, as reported in the literature. PIA was found in participants with a shorter prosthetic limb. No differences were found in LTF, despite a significant reduction in hip extension ROM found at the amputated limb. Shortness of the prosthetic limb and restriction in LTF accounted for 26% of variability in prosthetic-side PII. Interestingly, limitations in hip extension and amputated side PII were not correlated. Clinically, postural asymmetry in TFAs should be more closely examined, with future efforts focused on choosing the appropriate treatment solution.
The authors suggest the following measures to examine for postural asymmetry in TFAs: (1) LLD measured by the pelvic leveling device and block method; (2) PII measured by the Laser-Line™ or Sanders’ technique using a depth calliper and ruler; 41,50 (3) LTF measured by the fingertip movement technique; and (4) hip extension measured by the modified Thomas Test with a pelvic stabilizing belt.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. The authors declare that no competing interest exists.
Acknowledgements
We wish to acknowledge Otto Bock® for their support and donation of research equipment. We would like to thank the Amputee Coalition of America for supporting necessary research in the field of amputee rehabilitation and prosthetics. We would like to thank Prosthetic Research Study for their joint effort in this study. Lastly, we would to extend our gratitude to Mr Frank M Angulo for his time and work on the pelvis illustrations.
Oral presentations of these results were given at The 12th World Congress of the International Society of Prosthetics and Orthotics on July 31st, 2007, in Vancouver, Canada.