
Abstract
This paper seeks to deepen understandings of the relations between health inequalities and migration, with a particular emphasis on health-selective migration. Papers in this journal have urged for a more nuanced consideration of connections between migration and health but these have not seen-through how to combine understandings of health and migration to better theorise their relations. A strong theoretical basis regarding the politics of mobilities can help say more of the structural factors shaping health-selective migration and therefore, changing health gradients in a population.
I Introduction
The terms ‘migration’ and ‘mobility’ are, in many ways, related: a migratory experience is one of mobility, and mobility is the means by which migration occurs (Blunt, 2007). It is unsurprising then, that the terms often appear together in work relating to the movement or relocation of individuals and collectives, domestically (internally) or internationally (externally) across the spectrum of geography (e.g. Bell and Ward, 2000; Hyndman, 2012; Silvey, 2004). Yet despite existing together in common parlance, many scholars of migration (particularly quantitative studies) have yet to engage with mobilities as a paradigm that helps to unpack the drivers, politics and experiences of such movement (although see Halfacree, 2018, Hui, 2016, and Schewel, 2020 for key exceptions). Though the terms ‘mobility’ and ‘mobilities’ might be used in myriad ways, here ‘mobilities’ relates to the study of the politics of movement (Cresswell, 2006). ‘Mobility’ or ‘mobilities’ are not simply descriptors of movement, but also analytic terms that have purchase for how we might come to understand migration, and – as is the focus in this paper – health-selective migration.
There is now a growing acknowledgement that studies of migration may be enhanced through deployment of the ‘new mobilities paradigm’ (Sheller and Urry, 2006). While no longer ‘new’ (Faulconbridge and Hui, 2016), it remains significant for those thinking differently across disciplines which can get stuck in spatial ‘traps’ of analysing geographical phenomena in terms of points of fixity (i.e. in conventional migration studies, the static points at the beginning or end of a migration, see Cresswell, 2006). This critical way of thinking continues to inspire an extensive body of work and bespoke journals all dedicated to exploring our world ‘on the move’ (Sheller and Urry, 2006: 207). Yet it also allows a critical consideration of stasis and immobility. Immobility does not simply describe points of fixity but refers to the power relations enfolded in worlds of movement which make such movements stop, halt, still and slowdown (Cresswell, 2010; and examples including Ryser et al., 2019; Schewel, 2020; Straughan et al., 2020; Zickgraf, 2019).
As a sign of the buoyancy of connecting-up debates between the ‘well-established’ (as opposed to ‘new’) mobilities paradigm and studies of migration, the inaugural International Conference on Migration and Mobilities in 2016 sought to ‘cultivate and share different disciplinary perspectives of migration and mobilities, and to firmly fix the spotlight on the intersections between population and demographic research and the wider social science tradition of work on mobilities’ (2016: n.p., emphasis added). This call is as much a philosophical as methodological call, to bring quantitative approaches that tend to map, measure and describe migration and its patterns, trends and traits, together with qualitative work drawing on the ‘new mobilities paradigm’, which focuses on the subjective experiences, politics and idiographic accounts of migration. While there has certainly been work concerning migration that bridges this gap on subjective/objective knowledge and quantitative/qualitative approaches to the field of study (Boyle et al., 2013 as a key text), we further contribute to efforts to bridge the divide while also addressing wider disciplinary concerns that ‘scholars in population studies have not yet fully exploited the potential advances within the mobilities literature’ (McCollum et al., 2020: 198). We build on Halfacree (2018), whose work demonstrates how mobilities thinking can add depth to analysis of themes such as internal migration, and Hui (2016) who argues the need for building dialogue between migration and mobilities research. Yet rather than consider the breadth of migration and mobilities, we focus on progressing studies of health inequality and migration, an area we argue, demands particular attention in this respect given the power-infused politics that often shape the way people move (or are unable to move).
Research on migration and health has a long and varied history, beginning and expanding from early interests in population movement and the portability of disease. Now, migrant health and well-being, as McCollum et al. (2020: 200) note, is a ‘rapidly expanding’ field covering a breadth of topics including health status and access to healthcare for migrants (Hollander, 2013; Migge and Gilmartin, 2011; Warfa et al., 2006); the migration of medical workers and consequences for the distribution of healthcare (Connell and Walton-Roberts, 2015); or even the implications of climate change in the context of health and migration (Hunter and Simon, 2019). Our focus, however, is research examining how the movement of differently healthy groups and the health selectivity of migration influences health inequalities, and the role an analytic frame of ‘mobilities’ may offer to such work.
This paper contributes to embryonic debates around the role of mobilities thinking in respect of residential mobility and health (Morris et al., 2018), and more established commentary on the relations between migration and the new mobilities paradigm (Coulter et al., 2016). Yet it goes further, setting out how to deepen knowledge in contemporary population and health geographies and, notably, also work under the umbrella of the ‘new mobilities paradigm’. In mobilising mobilities thinking, we seek to unite seemingly disparate bodies of literature, and approaches to research, which are circling tentatively around these issues. Though applied in the context of health inequalities and health-selective migration, our approach may have much greater reach, particularly where social and spatial inequalities are thought to be influenced or shaped by differences in opportunity and uneven patterns of migration. The study of migration should involve a mobilities framework, and not simply in parlance, but in practice. In mobilising mobilities thinking, the questions we ask of the relationships between health and migration change. In turn, such questions would also change should we apply mobilities thinking to the relationships between education and migration, or social mobility and migration. To cite Cresswell, the ‘mobilities framework takes a more holistic view that allows us to make some unlikely connections’ (2011: 550). It is that holistic view, one that is emergent in studies of health-selective migration (see Darlington-Pollock et al., 2018), which will arguably better inform future research and discussion of a politics of health and selective migration.
To develop our argument, we first address some conceptual and definitional ambiguity in discussing residential relocations, mobility as a continuum of movement and the mobilities paradigm. We then review work that has sought to understand migration and health, focusing in particular, on the concept of health-selective migration. Next, we outline how the new mobilities paradigm may offer potential for a deeper theoretical engagement with relations between migration and health and highlight its connection with traditional lifecourse theory (e.g. see Elder, 1998a) and extended lifecourse perspectives (e.g. see Barcus and Halfacree, 2018). The paper finally turns to how we can mobilise the new mobilities paradigm – conceptually, analytically and methodologically – outlining a manifesto for doing more collaborative (health-selective) migration and mobilities research. We conclude with the ramifications this might have beyond migration and health to other dimensions of migration-orientated research.
II Defining Migration, Distinguishing Mobility/ies
Migration is a phenomenon defined by thresholds of distance and time (King, 2012: 136). While international migrations cross national borders, internal migrations reflect subnational residential relocations – both are expected to be of significant or permanent duration (Holdsworth et al., 2016). Internal migrations are further distinguished by scale and context (Castro and Rogers, 1979; Pol and Thomas, 2001; Roseman, 1971). Shorter distance moves, typically framed as residential mobility, tend to occur within the parameters of an individual’s or household’s daily activity spaces and are often assumed to be motivated by housing considerations (Coulter et al., 2016). These are held separate from internal migrations involving longer distances, demarcated by a move to a new community or change in one’s social and economic situation, and more often assumed to be motivated by employment considerations (e.g. see Barcus and Halfacree, 2018).
Mobility, however, as it is typically used by migration scholars, is a descriptor that not only incorporates the more permanent forms of residential relocation outlined above (both migrations and residential mobility) but also the shorter term relocations increasingly evident in households navigating fractured family structures (e.g. children moving between divorced or separated parents) and spatially disparate labour markets (e.g. weekly long-distance commutes) (McCollum et al., 2020). Yet beyond residential relocation, whether temporary or permanent, mobility is also a term employed to capture the more mundane flows and movements in our day-to-day lives. Mobility then refers to a continuum of movement, ranging from every-day movement at home or in the garden, to short-distance daily trips (e.g. school runs or commutes), regular moves between homes (whether for work, climate or family reasons), the varying types of residential relocation, and virtual mobility of information or capital so prolific in contemporary society (see Pooley et al., 2005, cited in Barcus and Halfacree, 2018).
Mobility as a descriptor of both residential relocations and wider forms of everyday movement thus acts as ‘as a template enabling us to see how [migration] is embedded in and links to other forms of mobility’ (King, 2012: 143). Yet the mobilities paradigm pushes this conceptualisation further. The ‘mobilities paradigm’ positions movement at ‘centre stage’ of social science research agendas (Hannam et al., 2006; Sheller and Urry, 2006: 208). It has sought to unpack the intricacies and ‘politics’ of movement, challenging a stable metaphysics where understandings of place, belonging and attachment have been entrenched (quite literally) in notions of sedentarism (see Cresswell, 2006: 27; Sheller and Urry, 2006: 208). As Cresswell (2006) points out, feudal societies were, for many centuries, essentially rooted: fixed to localities, with movement restricted to the privileged or sanctioned as acceptable by relevant authorities. People who moved were branded as tramps (Cresswell, 2001), vagrants and undesirables (Cresswell, 2006) – their very existence as ‘mobile’ was coded as a negative social trait. However, as societies have changed, so have perceptions of mobility. Mobilities research, then, has sought to attend to this world ‘on the move’, and consider that movement is never a given but is historically contingent, and always situated politically (Cresswell, 2010). It is not simply the fact of movement from place ‘A’ to place ‘B’, or that movements happen in a continuum, but it is an attention to the character of the movement, the experience of movement and the political drivers that form and inform it. Mobilities research then moves us away from the ‘push’ or ‘pull’ factors of movement (the beginning or end of a journey) to the very process and experience of moving and of being mobile. It enhances a take on mobility as a continuum that identifies connections, flows and relations in movement, to reveal the power-fused subjectivities encapsulated in those movements (or lack of movements). Mobilities thinking as inspired by Sheller and Urry (2006), Cresswell (2006) and others disrupts the primacy otherwise given in analytical frameworks to the empirical fact of a residential relocation (Halfacree, 2018: 6). More importantly, it provides a different starting point for any student of migration. Rather than only asking ‘who goes where and why’ (Champion and Fielding, 1992: 1), mobilities enables us to ask how while adding nuance and depth to why.
In what follows, we attend to these questions using the term ‘migration’ to reflect any form of residential relocation expected to be relatively ‘permanent’. It is these migrations, or relocations, which are particularly pertinent to shaping health inequalities at the population level. Though we focus on literatures concerned with residential relocations within countries – some interested in residential mobility, some in internal migration, the framework we propose need not be limited to internal moves. In arguing for a mobilities perspective, the continuum of mobility necessarily extends to international migrations.
III Researching Migration, Health Inequalities and Health-Selective Migration
‘Space and place affect people’s health, well-being, and access to and experiences of health care’ (Crookes et al., 2018: 1, cited in Newbold and Wilson, 2019: 2). This quote, as Newbold and Wilson (2019) argue, clearly captures the connections between migration and health, but also inequality. Differential access to healthcare and differential experience of place matter for uneven health outcomes, but migration, both at the individual- and population-level also matters. As such, there is considerable scope for research, both substantively and methodologically, across the nexus of health, migration and inequality. In recent decades, methodological and technological developments have significantly advanced the study of migration and health inequalities, whether through the availability of robust longitudinal datasets such as the ONS Longitudinal Study in the UK (e.g. Norman et al., 2005), the New Zealand Vascular atlas (e.g. Darlington-Pollock et al., 2016; Exeter et al., 2015) or The China Rural Production Survey (e.g. Lu and Qin, 2014); through the application of advanced statistical methods such as multilevel modelling (Owen et al., 2016), a combination of matching methods and logistic regression (e.g. Green et al., 2017), sequence analysis (Shackleton et al., 2018) or cox regression (a form of survival analysis) (Gartner et al., 2018). Broadly speaking, evidence from these types of research suggests that health-selective migration can contribute to socio-spatial inequalities in health at different spatial scales and in different contexts. Migration is an important geographic process, which sorts differently healthy individuals into different life circumstances and contexts. This has implications for existing health inequalities, wider socioeconomic inequalities, spatial segregation, service provision and policy development. While the data and methods used to examine migration and health are increasingly sophisticated with a range of quantitative algorithms and models, qualitative methods can assist in understanding the complexities or dynamics of the relationship and the drivers by which this can contribute to wider (health) inequalities. It is not a question purely of methods (or methodological divisions), however, but of philosophical positioning. Studies of health-selective migration remain under-theorised in how we understand the movements involved in such processes and their politics.
Migration is selective. It differentiates migrants from non-migrants in a number of ways. For health and population geographers, the study of migration and health is substantively shaped by the early observations of Farr (1864) and Welton (1872). Their work highlighted the health-selectivity of migration in that the health of those moving from urban to rural areas was poorer than the health of those moving in the opposite direction. The selectivity of migration is key to the relationship between migration and health, and the role this may play in perpetuating health inequalities. Where differently healthy groups are selectively sorted through migration, we must question: (a) whether this redistribution of the population changes the state of population health between areas, and (b) the extent to which chances of redistribution vary between individuals, conditional on wider contextual factors or demographic and socioeconomic attributes. Though understanding and investigating changing health inequalities are at the heart of extant research into health-selective migration, the analytical framework adopted dictates which of these two broad questions are addressed. Underpinning either approach is a conceptual framework delineating the expected relationship between health and migration, and the directionality of these relationships. This is currently under-theorised in respect of the drivers, politics and experiences that relate to those connections. This is where we believe a more active engagement with mobilities thinking can enhance analysis and understanding.
Since Farr and Welton, research consistently documents the health selectivity of migration, differentiating ‘movers’ and ‘stayers’ by their health status according to the nature of their (im)mobility. However, the selectivity of migration extends beyond health spanning a range of demographic and socioeconomic attributes: age, sex, ethnicity, housing tenure, socioeconomic position, educational attainment all shape propensity for and nature of a migration event (e.g. Darlington-Pollock et al., 2019). These attributes interact, contributing to the complexities of the health–migration nexus. Younger migrants tend to be healthier than their immobile peers whereas the opposite is true for older migrants (Bentham, 1988; Boyle et al., 2002; Findley, 1988; Larson et al., 2004; Maheswaran et al., 2018; Verheij et al., 1998). Young adults in good health are highly mobile, moving for education or employment opportunities (themselves correlates of good health (see Verheij et al., 1998)) or for family formation. With increasing age, reasons for mobility vary as does choice of destination depending on stage in the lifecourse.
Younger healthy adults may first move to a more deprived, less desirable, more central urban area but then move outwards as status, income and aspirations climb to leafier suburbs characterised by lower levels of deprivation (Norman and Boyle, 2014). However, poor health may precipitate migration, particularly in older ages, as people move to be near formal or informal care (Litwak and Longino, 1987). Irrespective of age, poor health may force a move to alternative accommodation, whether for space or location or for economic reasons if poor health results in a loss of earnings (Boyle et al., 2002). Of those who do migrate, whether or not to their (dis)advantage, poor health or illness is also related to distance moved (Boyle et al., 2002; Fox and Goldblatt, 1982; Wilding et al., 2018). Coincident with the selectivity of migration is the selective immobility of those groups either not able to move or choosing to remain. In the context of health-selective migration and wider migration studies, these groups are often neglected from discussion. Sedentarist assumptions underpin much of migration scholarship, whereby ‘staying put’ is the norm (Barcus and Halfacree, 2017; Cresswell, 2010). Analyses then focus on those who ‘deviate’ from the norm, relegating immobility to the footnotes of migration research. Yet the selectivity of immobility is as important to understanding changing health gradients as the selectivity of mobility.
The basis of the work previously described is underpinned by the relations outlined in Figure 1. Research in health-selective migration continually reaffirms this framework documenting the complex relationships between health and migration, particularly in respect of the resulting influence on changing health gradients. The majority of movers are young and relatively healthy although differences emerge when considering later-life migrations, the constraints of declining or poor health, the distance moved, and of course, the conditioning influence of wider individual-level socioeconomic attributes and contextual factors. Therefore, more advantaged individuals tend to move towards or between less deprived areas, reflecting their more advantaged socioeconomic position. Conversely, less advantaged individuals are more likely to drift towards or remain in more deprived areas. This movement, within and between differently deprived areas, often reinforcing wider socioeconomic circumstances, matters for health. The health-deprivation gradient is well-established: more deprived areas are characterised by poorer health, while the inverse is true for less deprived areas.
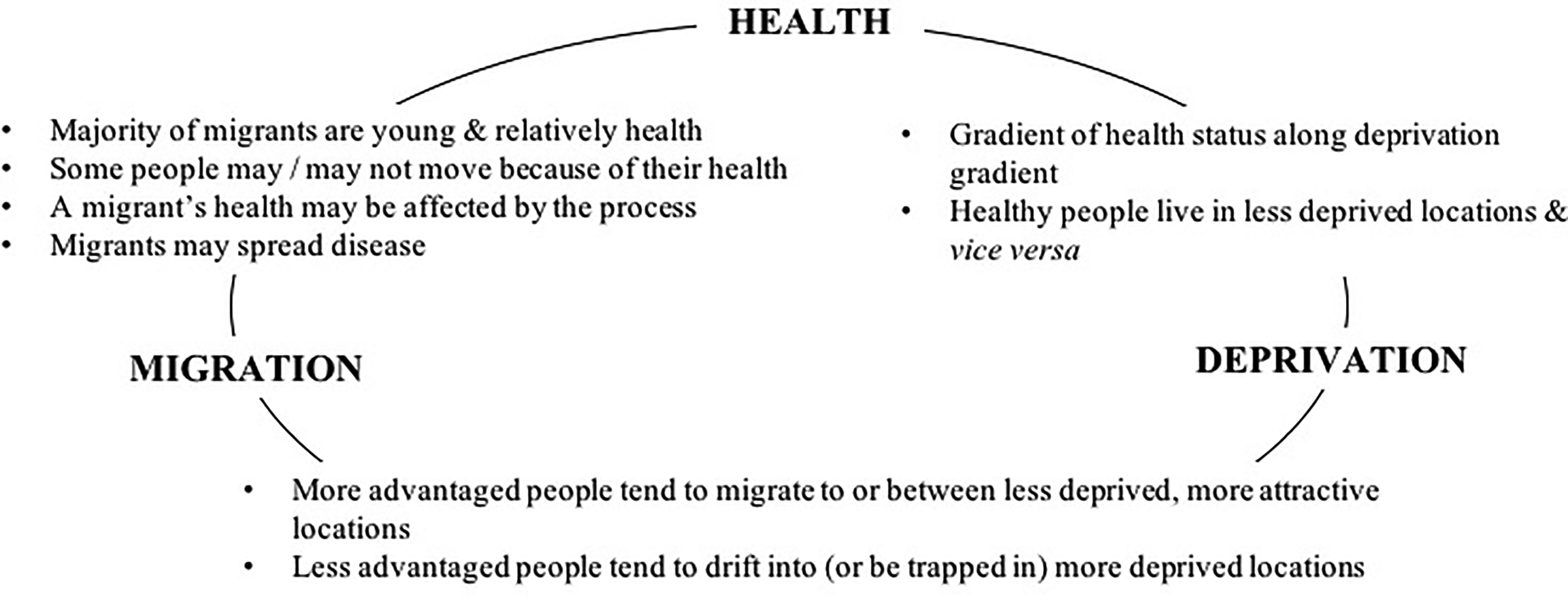
The health–migration–deprivation nexus.
The relationship between health and a change of address can be quantitatively modelled at the individual level. Here, researchers are either interested in what explains the heightened probability of a change of address for people in differing states of health (e.g. Verheij et al., 1998) or what explains the differing health states for different types of (non-)movers (e.g. Tunstall et al., 2014). To explain these differences, individual-level socioeconomic and demographic characteristics and information about geography are variously included within the model. This either reduces the probability of poor health for particular types of movers or reduces the probability of a move for those in good or poor health. The questions asked (and indeed conclusions drawn) within these studies may be directed at understanding changing health gradients, but the modelling approach adopted is better suited to explaining relationships rather than explaining any change in health gradients or inequalities.
To establish whether health-selective migration contributes to changing health gradients (Darlington-Pollock and Norman, 2020; Norman, 2018), analytical frameworks that (re)aggregate individual-level data at the area level to compare health outcomes are more appropriate. The current health profile of a population, stratified by area or area type, is compared to the health profile that would arise if no one in that population had changed address (Boyle et al., 2004, 2009; Brimblecombe et al., 1999, 2000; Kibele and Janssen, 2013; Norman et al., 2005). An alternative is to compare the health of mobile groups joining a particular location (e.g. region) or area type (e.g. according to deprivation quintile) with the health of those leaving that area type. Where there are differences, this is where any change in health gradients between areas and area types will play out. The expanding body of research into health-selective migration, and the health–migration nexus more generally, provides ever more nuanced insights into not only the relations between health status, propensity to move and the nature of a move but also the impact on aggregate population health. In an era of persisting and, in some cases, widening health inequality alongside stagnating life expectancy (Hiam et al., 2018), new insights into the mechanisms perpetuating inequality are continually warranted. However, these insights, and the extent to which the evidence obtained can enable and inform positive policy action, are limited where a more nuanced understanding of relationships remains absent. While Figure 1 offers a useful starting point, the framework leans heavily on (valuable) empirical, quantitative observation with much space available for greater qualitative depth.
Much extant research focuses on residential relocations between two points in time, largely owing to data availability. Analytically then, moves are treated as discrete events: an empirical fact isolated from the wider reasons that condition the act of a move and the direction of it. Yet, individuals do not move in a vacuum. This approach overlooks the complexities of why we move, focusing instead on the fact of the move itself. As geographers, we can attest to the significance of context in shaping propensity for, and nature of, a move. However, micro-contexts – such as social and familial relationships – or macro-contexts – such as education opportunities, labour markets and housing markets, or economic and political climates – are often reduced to readily quantifiable variables such as ‘marital status’, ‘economic activity’ and area-level measures such as population turnover or deprivation. In focusing analyses at the individual- or population-level, critical themes of relationality that are so central to wider research in population and health geography, and the broader social sciences, are often neglected. At the micro-level, for example, research on household and family migrations (e.g. Cooke, 2008) may be pertinent to the relationship between health and migration. At the macro-level, the significance of wider relations with external power structures increase when transitioning from times of economic boom to bust or in times of political instability. Missing, then, from research on health-selective migration are analyses of the plurality of movement and the more subjective experiences that may shape changing health gradients arising through the relational nature of mobility and systematic attempts to better operationalise critical micro- and macro-contextual factors. Though exceptions exist (e.g. see Darlington-Pollock et al., 2018; Shackleton et al., 2018), there is work to be done. As we argue in this article, this can be informed by wider theoretical developments in human geography and the social sciences, including employing the new mobilities paradigm (Shelley and Urry, 2006) and emphasising its connections with traditional lifecourse theory or extended lifecourse perspectives (described below).
IV Health, Migration and the Potential of a ‘Mobilities’ Approach
While there is space for mobilities thinking in health-selective migration research, mobilities perspectives are not all together absent from the work of population geographers. The relationality inherent to mobilities is at the heart of lifecourse approaches which have been central to much of the recent developments in migration from the perspective of population geographers. A lifecourse approach (a biographical mode of analysis) emphasises the interdependence of micro- and macro-level drivers in shaping mobilities over the long term. Lifecourse theory developed out of a need to account for the interdependencies between the social trajectories of individuals and families, and the wider structures that give these trajectories meaning and form (see Elder, 1998b, Elder et al., 2003). In the context of a lifecourse approach, migration is not considered a ‘discrete contemplative act’ (Halfacree and Boyle, 1993: 337) but interpreted through the different constraints and triggers operating across inter-dependent domains of the lifecourse (e.g. see Mulder and Hooimejer, 1999). Recent efforts among human geographers to better theorise residential mobility owe much to this biographical approach. Findlay et al. (2015), Coulter et al. (2016), Barcus and Halfacree (2017) and Halfacree (2018) turn attention away from ‘migration’ towards ‘mobilities’, emphasising lifecourse perspectives and embracing the theme of relationality. Each explicitly urge a use of, or engage with, the ‘new mobilities paradigm’ to make sense of movement. Coulter et al. (2016) contend that migrations are practices embedded within larger structural power relations, the politics or ‘power’ implicit within movement being central to the mobilities approach. Bailey (2009) emphasised the importance of spatial contingencies mediating transitions over the lifespan thus necessitating the relational approach implicit within lifecourse perspective: Coulter et al. (2016) analogously contend the reason for bringing a mobilities approach is ‘context’. Indeed, their arguments resonate with Barcus and Halfacree (2017: 98), urging Population Geographers to more fully embrace the mobilities paradigm and ‘shift from presenting residential migration as an essentially unique or distinctive form of movement to recognizing and emphasizing its location within a broad spectrum of mobilities that both expresses and shapes everyday life’. Their conclusions similarly resonate with calls from Stockdale and Catney (2012) who challenged researchers to pay closer attention to the role of local context and structural factors in shaping patterns of internal migration.
While Coulter et al. (2016) make important acknowledgements towards mobilities, they do not fully demonstrate a ‘mobilities’-enhanced approach nor do they clearly map out how new forms of data may benefit understandings of residential mobility. Morris et al. (2018) explicitly examine progress in health and mobility research, akin to the intention of this article, urging for a broader range of data to enhance studies of migration and mobility. Yet they too focus on various quantitative data rather than seeking to bring together data through a conceptual lens that enables both qualitative and quantitative data and analysis to feature. While Findlay et al. (2015) go further, proposing a framework which gives primacy to the analysis of mobility relative to demographic events, gaps remain. We build on these papers, developing a mode for deepening migration research through the mobilities paradigm, focusing on the question of health-selective migration. A mobilities approach may not just deepen the work of scholars understanding migratory movements (particularly in relation to health) but may also improve research by changing the very questions we seek to ask in the first place. In other words, what happens if you start with a mobilities approach?
Despite the gaps we have identified, there is a sizeable body of qualitative work seeking to make sense of migration, through the lens of the mobilities paradigm. Indeed, mobilities research tends to be informed by qualitative methodologies attentive to idiographic and subjective detail that helps unpack the politics of movement. In a Progress Report published in this journal, Blunt demonstrates the vibrancy that a mobilities lens has provided for understanding migration under a qualitative umbrella unpacking the ‘embodied, material and politicized’ contexts of migration (2007: 2). The extensive work of Burrell has illuminated how a framework of mobilities – taking seriously the drivers, experiences and politics of movement – can frame new understandings of Polish migration (see 2006, 2011, 2012, 2017). Burrell explores how meaning, attachment and materiality shapes processes of migration, with less focus on the large-scale ‘fact’ that movement has happened. This work gets beneath the very experience of what it is to move, and to exist post-moving. Ciobanu and Hunter (2017) have employed the mobilities paradigm to consider migration and older age. Here, the authors attend to the ‘physical, virtual, communicative, or imaginative’ modes by which older people move and the governance regimes that underscore (or limit) movement to attend to the politics of migration for this group (2017: 1). That people move is of less interest here than how and why they move as well as the socio-cultural, political and personal relations that emerge in such movement. This work, however, tends to lack an aggregate or overarching understanding that paints a ‘bigger picture’ insight into movement. Given the uneven opportunities for and the nature of movement, this oversight ignores the ways in which an integrated understanding can enable deeper insights into migration. Nevertheless, it does demonstrate how weaving together the idiographic and qualitative could bolster some aggregate level studies.
Similarly, there is an ever-growing body of work focusing on health, well-being and associated movements (domestic and international) that has demonstrated a keen engagement with the mobilities paradigm. For example, Gatrell (2013) argues that specific mobilities can be conducive to health through the therapeutic act of moving from one place to another (see also Kaspar et al., 2019). In a different vein, Lewis (2015) has explored how migration, health and mobility intersect around those with HIV using a mobilities framing and qualitative data from interviews to ‘depart’ from models of movement that reveal little of the ‘nuance’ of how and why such migration happens. Similarly, Ormond (2013) explores healthcare migrations and how these create a sense of home and belonging for those who travel to gain access to provisions they cannot reach in their countries of origin. Common to these and other works is a tendency towards qualitative methodological approaches, suited to unpacking the ‘politics’ of mobility, central to the spirit of the ‘new mobilities paradigm’ and its determination to get behind and between movement: to tell the stories of movement rather than to take movements related to health/health mobilities as ‘given’.
In spite of this work that engages the ‘new mobilities paradigm’ into understandings of migration, movement and health, research into health-selective migration specifically remain under-theorised and lacking depth and detail. Accordingly, given the omissions in research under the remit of health-selective (and arguably other areas of) migration studies, the remainder of this article sets out a tri-part framework for mobilising the new mobilities paradigm in health-selective migration research and beyond.
V Mobilising the Mobilities Framework: The Politics of Health-Selective Migration
1 Conceptual Mobilisation
Cresswell’s ‘more finely developed politics of mobility’ (2010: 17) unpacks the intricate dimensions that constitute a world on the move. He argues that ‘mobility’ is still largely spoken about as ‘singular’, where movement is conceived in a simple one-dimensional fashion (from point A to B), and as lacking character specific to the type or mode of moving and its experiential qualities (Cresswell, 2010). Accordingly, Cresswell advocates examining mobility not as a ‘singular thing’ but via ‘breaking mobility down into…its constituent parts’ (Cresswell, 2010: 17). Such an effort has enriched mobilities studies by considering the specificity of different typologies of motion and their politics (Cresswell, 2010: 17, see also Peters, 2015). There is a need, therefore, to unpack the specificity of particular ways or methods of being mobile as each of these has its own cultural connotations, affective registers and political purposes. Indeed, we move and are mobile in different ways. These differential mobilities – impacted by force, friction, route, speed and experience – evoke differential politics (Cresswell, 2010). While attention has certainly been paid to the ways in which various means of mobility – walking, flying, commuting, driving, cycling – shape and are shaped by complex compositions of ‘being mobile’, the dynamics of migration and health-selective migration have not been explored in such a way. Cresswell’s ‘politics of mobility’ offers the potential for moving beyond Euclidean conceptualisations of geometric distance to instead, enfolded, multiple, complex, shifting and layered methods, registers and sensations of being on the move, of migrating: here is where we can start to see more space for a mobilities approach within research into health-selective migration.
For example, where a change of address becomes more than a simple relocation between two discrete points in space, whether or not we are interested in the influence on either individual- or population-level health, we must pay more attention to the journey between, before and after. Applying Cresswell’s ‘politics of mobility’ framework we can consider: What is the agency driving a move? Who moves furthest, fastest? What are the barriers preventing or halting a move, the ‘frictions’ that constrain it? What shapes the ‘rhythm’ to a move and how often it is repeated by an individual, a family, a generation or even a population subgroup? What is the socio-spatial direction of a move and what happens to those who do or do not move? These sorts of questions illustrate how residential mobility and immobility are relational practices that, as Coulter et al., argue, link lives together connecting people to structural conditions through time and space (2016: 365). Though arguably apparent in wider literature on internal migration and residential mobility, for example in questioning whether and how migration begets migration (e.g. Coulter and van Ham, 2013), and to a greater extent in literature considering differences in health outcomes and propensity to migrate across different distances (e.g. Wilding et al, 2018), there is scope for more. In particular, using mobilities as a starting point can offer much in unpacking changing health gradients, enabling questions such as: How have the legacies of migrant settlement or gateway towns shaped the socioeconomic, spatial and health experiences of individuals and subsequent generations? How has the legacy of particular industries shaped the life and health chances of individuals and successive generations? Crucially, what are the politics of this, and by extension, what are the politics of selectivity? Who is able to move, who is constrained and who chooses not to are inherently political questions: these decisions and opportunities do not occur in a spatial or political vacuum. Though such questions have informed some wider research on migration and/or health (e.g. Bambra and Garthwaite, 2015; Catney and Simpson, 2010), they are often either missing or rarely made explicit in existing work on health-selective migration. While Bambra et al. (2019) call for a political economy approach to the study of health inequalities, this may be more forthcoming in research on health-selective migration informed by a mobilities perspective. In extant research, these sorts of questions do not underpin the analytical or methodological frameworks adopted nor do they structure the way in which results are interpreted or understood. Conceptually, then, applying Cresswell’s ‘politics of mobility’ framework and breaking mobility down into its constituent parts not only reshapes the sorts of questions we might ask of the relationships between health, migration or mobility and inequalities but also raises some analytical and methodological points.
2 Analytic Mobilisation
At the heart of Coulter et al.’s call for the use of a mobilities framework is the recognition that residential mobility and immobility are ‘relational practices that link lives together to structural conditions through time and space’ (Coulter et al., 2016: 357). This meshes well with the mobilities framework, which places mobility and immobility on a continuum as well as paying substantive attention to the complex plays of power involved in movement. This contrasts with analytic distinctions between ‘movers’ and ‘stayers’ or ‘migration’ and ‘residential mobility’ otherwise inherent to studies of migration, and the treatment as movement as ‘given’. Both Coulter et al. (2016) and Halfacree (2018) urge against such hard distinctions. While quantitative data analysis may necessitate analytic distinctions in types of movement, this need not come at the expense of employing mobilities thinking where movement is a process that cuts across stark definitional boundaries enriching the analytical framework adopted. One notable example ‘widening’ the concept of ‘stayers’ and thereby blurring hard distinctions between mobilities is Clark et al. (2017). Stayers are construed as both those who do not change address and those who only move within their local neighbourhood. Notwithstanding, research into wider lifecourse transitions and residential change is more adept at accounting for the relationality of mobility (e.g. Falkingham et al., 2016; Mikolai and Kulu, 2018). It is critical to heed the insights from such analogous bodies of research.
Some of the early, influential research on health-selective migration and changing health gradients (and analogous work on health-selective social mobility, e.g. Bartley and Plewis (1997, 2007)) concluded, erroneously, that such mobility had little or no impact on changing health gradients. The analytical framework in these studies typically compares health of mobile groups with immobile groups, arguing that for any form of selective mobility to have a significant widening influence on health gradients, the health of those sorted into the most advantaged areas must be substantially better than the health they join. Similarly, the health of those sorted into the most disadvantaged areas must have substantially poorer health than those who they join. While Boyle et al. (2009) persuasively demonstrated that the influence of the sorting process manifests in the differences in health between mobile groups, there remains a tendency to position mobile and immobile groups as diametric opposites in quantitative research. Immobile ‘stayers’ are reduced to a passive reference group within a model, or a point of comparison. Useful inferences can be drawn about the relationship between migration and health when comparing the health of mobile and immobile groups. However, where migration is of interest in terms of its function in the process of selectively sorting and redistributing populations, holding mobility and immobile separate is problematic. In an era of declining migration (Champion and Shuttleworth, 2017) and reported rises in secular rootedness (Cooke, 2011), it is critical to take heed of active non-migrations and not neglect reasons for immobility (Schewel, 2020). A mobilities perspective is as adept at making sense of movement as it is of non-movement. Indeed, the conceptual mobilisation of mobilities in conjunction with analytical mobilisation focuses attention on the politics of selectivity and therefore both migrations and immobility.
Where mobilities ‘works to undermine the predominant significance of the empirical fact of residential relocation from point A to point B’ (Halfacree, 2018: 276), analytical frameworks must, insofar as possible, seek to capture the complexity of the health-migration relationship and the spatial contingency of migration itself. How variables, concepts and ideas are operationalised matters, as does a more critical evaluation of existing approaches. For example, does ‘marital status’ or ‘economic activity’ truly capture the complex micro- and macro-level dynamics that influence propensity to move, the socio-spatial trajectory of a move, and health status? Though choices will be restricted by data limitations, existing analyses may not best capture the sorts of social, economic, political and cultural events that can disrupt and change the relationship between migration and health, particularly given the mediating role local context has been found to exert on patterns of internal migration (Stockdale and Catney, 2012). Finally, though stages in the lifecourse are routinely proxied for by age, the assumed linear progression through stages of the lifecourse with age is problematic in a socially and culturally shifting society, particularly insofar as it masks the underlying interconnectivity and relationality so pertinent to the relationship between migration and health. While non-linearity between age and migration can be accounted for in modelling by including age-squared (where data availability permits), a more critical discussion of the limitations of existing data and variables is needed. Indeed the sorts of critical discussions more routine within gerontology as to the concept of age and it’s relation with health may be useful starting points (Settersten and Mayer, 1997). A mobilities perspective thus offers a platform from which to challenge entrenched approaches to quantitative analyses that though acknowledged are not routinely critically engaged with. Crucially, we need to be more critical of how we operationalise concepts and construct variables, rather than blindly adhering to typical approaches in empirical work.
3 Methodological Mobilisation
To date, much of the research that has sought to make sense of the relations between migration and health and our focus here – health-selective migration – has come from a quantitative perspective. Yet a mobilities perspective is emergent (though not necessarily acknowledged) in more recent quantitative work. For example, with the increasing availability of rich longitudinal data, it is possible to examine trajectories of moves – and therefore some of the power dynamics at play – rather than only exploring the fact of relocation between two points in space and the associations with different health outcomes (e.g. Shackleton et al., 2018). Future work should look to explicitly interpret different socio-spatial trajectories and the influence on health outcomes within the wider socio-historical and political context that shaped them, whether in terms of period effects, or where data availability allows, for particular cohorts (see e.g. Falkingham et al., 2016). A new mobilities approach, conceptually and analytically alert to the politics of movement, is no doubt significant in such work. Moreover, in the advent of big data and significant technological advances, studies of health-selective migration should now prioritise not just analytical frameworks but wider methodological frameworks that embrace examining trajectories of moves (rather than discrete events) and how these are linked to conditions through time and space. Lessons must be learnt from analogous methodological approaches concerned with different types of lifecourse dynamics and the impact on different social, economic or indeed health outcomes (e.g. Hedman et al., 2015). Our methods must make better use of the longitudinal data available to us, and better account for the multi-dimensional nature of health-selectivity: it is not just migration, or deprivation mobility, or social mobility, but a wider set of transitions and relationships that are important.
Yet mobilising a mobilities approach for research on health-selective migration (and beyond) also depends on embracing the coming-together of research modes typical in health-selective research (namely quantitative approaches) with those typical in mobilities-related work (mainly qualitative approaches). Indeed, as Coulter et al. (2016) note there is a need to pay ‘greater attention to the qualitative nature’ of movement that permits ‘sensitivity to power relations’ (Coulter et al., 2016: 362). Yet in spite of this call, the authors acknowledge but do not push forwards a manifesto for more integrative working across quantitative and qualitative techniques, noting it is ‘beyond’ the remit of their paper. Moreover, in recent calls to progress understanding in health and migration, the need for various ‘data’ has featured strongly: indeed, we take much inspiration from Morris et al. who note ‘the health mobility literature appears to ignore many relevant data in research design, even where they are available’ (2018: 121). While Morris and colleagues refer to diverse forms of quantitative data, there is a broader appreciation of data that may enhance understandings of health-selective migration: namely qualitative data that can unlock further nuance, particularly in aggregate level analysis. The mobilisation we thus propose relies on cross-cutting a much longer enshrined epistemological and ontological ‘division’, between the qualitative and quantitative, the largely objective and subjective, the aggregate and the individual.
Our suggestion fits well with a keen shift across human geography to mix or ‘mash-up’ methods (see Peters, 2017) moving beyond triangulation – where various data are used to corroborate findings (Bryman, 2006) – to an integration of methods. This is paramount for progressing understandings in health-selective migration research. Mixed methods research aims, from the start, to meld quantitative and qualitative data collection techniques and analysis (see DeLyser and Sui, 2013, 2014; Sui and DeLyser, 2012). Specific methods are not prioritised over one another but are given equal voice in analysis and understanding. However, such approaches have proven difficult to realise in practice, in part because of ontological and epistemological differences in ways of knowing the world (see Elwood, 2010). Quantitative research that has dominated health migration literature tends to be based on positivist and post-positivist understandings that aim to quantify and model trends in movement – either at individual or population level. Qualitative research that has come to shape most (but not all) of the work under the umbrella of the ‘new mobilities paradigm’ has largely relied on subjective, interpretive techniques that explore the gaps in making sense of ‘power relations’ (to follow Coulter et al. (2016: 363)). These two approaches tend to sit unhappily together because their methods, analysis and eventual knowledge creation are deemed incompatible (see Bryman, 2006; Elwood, 2010; Philip, 1998; Sui and DeLyser, 2012). That said, following a trio of influential papers in this journal, there are a number of reasons for now ‘mixing’ methods.
DeLyser and Sui urge scholars to ‘bury the qualitative-quantitative divide’ (Sui and DeLyser, 2012: 111), arguing that popular topics in geography demand a mixed approach to fully comprehend the complexity of current spatial concerns shaping the discipline. Accordingly, we contend that this methodological ‘mash up’ is key to unlocking greater understanding of health-selective migration (and also as research has already showed, between migration and health more broadly). This chimes firmly with Halfacree’s (2018) embracing of mobilities approaches in recent migration work. Mixed methods could bring several benefits to understanding movements across data divides. First, they provide complementarity. Such approaches can offer consideration of data that complement one another, clarifying ‘the results from one method with the results from another’ (Greene et al., 1989: 259). Mixing methods then provides a clearer picture in relation to a research problem at the outset and how a particular question about health-selective research is framed. It can also yield new insights during analysis, where results from aggregate data may be correlated with coded personalised data to map trends. Such an approach has been successful in GIS work (see Kwan and Ding, 2008, for example) where geo-coded spatial data are mapped with qualitative data to overlay different data types for richer analysis. Such ‘layering’ (even without the use of GIS software and data) is crucial to attending to some of the weaknesses in understanding health-selective migration where the reasons driving particular movements can be better contextualised. Likewise, mobilities research, which can tend towards idiographic analysis, may benefit from framing subjective understandings of movement within larger scale, population wide patterns and/or trends.
Second, and relatedly, as Bryman notes, no form of data collection is without its limitations (2006: 106). Scholars of mobilities appreciate the weaknesses in their data often noting the specific context, power relations and issues of positionality in framing their work in migration mobilities creating situated accounts (e.g. Burrell, 2012). This is likewise for scholars of migration and health (a good example being Morris et al., in their discussion of data limitations and ‘appropriate data use’ (2018: 121)). Mixing methods can ‘offset’ the limits of particular data forms to create deeper understandings of a given phenomenon. Notably then, mixing qualitative and quantitative methods can offer a wide-ranging view on a particular topic – for example, offering up generalisable trends alongside personal reflections (see Kwan (2002), Sporton (1999) and Winchester (1999) for now dated but useful reflections of this kind). Building teams of researchers that cross-cut methodological divides is crucial in achieving this aim and goal. We believe ‘mashing up’ groups of researchers to achieve new research goals is fundamental. Indeed, this article follows this suggestion, embracing DeLyser and Sui’s approach of co-writing across the methodological interface.
Third, we urge a melded approach where qualitative approaches such as in-depth interviewing, focus groups and archival data are used during quantitative analysis to deepen explorations. Such approaches have been used in transport geography. Studies of the spatial organisation of transport systems at local and global scales have often depended firmly on quantitative methods of modelling and mapping to make sense of how such networks function. Qualitative methods are then increasingly used to bring ‘plurality’ to the discussion and to understand how transport systems are experienced (Goetz et al., 2009: 330). Likewise, it would be possible for qualitative data to be combined with quantitative data and analysis. A good example would be to overlay in-depth interview data with mapped routes or aggregate data of migration.
Fourth, to progress research scholars must not just cross the methodological divide but leap over it – mashing together quantitative approaches with the array of innovative and creative ‘mobile methodologies’ now emergent to ‘capture’ mobilities and mobile worlds. It is argued that the ‘new mobilities paradigm’ demands new methods (or at least a reinvigoration of current techniques). Law and Urry (2004: 403–404) noted that ‘classic’ methods, such as interviewing, focus groups, questionnaires and so on, are typically static. They take place in place and, as such, deal ‘poorly’ with capturing the range of movements that are so intrinsic to the contemporary world (Law and Urry, 2004: 403–404). It has been posited, therefore, that mobile methods are required for researching elements of mobile life (although see Merriman, 2014 for a critique). Such a project would be challenging but not impossible. For example, mobile methods might be defined as those where ‘the research subject and the researcher are in motion in the field’ (Ricketts Hein et al., 2008: 1267). These methods seek to grasp what it is to move by ‘being there’ or being ‘in-situ’ with movement (Fincham et al., 2010: 6). In the context of health and migration, this is significant insofar as such methods can enrich insights into whether and how the act of moving is itself related to (changing) health outcomes. This may involve observational research where researchers can trace the journeys of people exploring how travel impacts subjects and objects and the decision-making processes that determine movement. Similarly, time–space diaries whereby participants (and even researchers) can keep a detailed record of ‘what they are doing and where, how they move during those periods and the modes of movement’ would allow the researcher to ‘plot’ movement and its drivers. Technologies such as Global Positioning Systems (GPS) can be embraced to enhance such approaches. These methods may be used together with quantitative data to layer context and deeper knowledge onto broader trends. Indeed, new forms of numerical or mapped data that may be collected ‘on the go’ using app or web-based technologies, when approached from a mobilities perspective, will continue to present exciting opportunities for innovative research.
VI Mobilising a Framework
Before concluding, we draw together the key components of our approach to present a proposed framework for research (Figure 2). The framework is situated within the conditions that shape the research, both in terms of the data landscapes – what data, whether quantitative or qualitative, are available – and the skills and experiences of the research team – for example, interdisciplinary researchers drawing on different methodological approaches, yet both are open and porous (as signified by the dotted line). Within these conditions, a mobilities perspective introduces a number of different ways in which knowledge about mobilities – specifically, residential relocations – and the relationship both with health and health inequalities can be captured or created, and identifies how these are inter-related. These knowledges are defined in terms of different experiences (whether for populations, individuals or researchers), ways of knowing and how we make sense of movement. To interpret this knowledge, a mobilities perspective then emphasises the politics of movement (or indeed of immobilities). Through this, we can make sense of the mobilities (see Barcus and Halfacree, 2018: 99) in relation with the core concepts that connect migration and health (place, space and health (Newbold and Wilson, 2019)), and health inequalities.
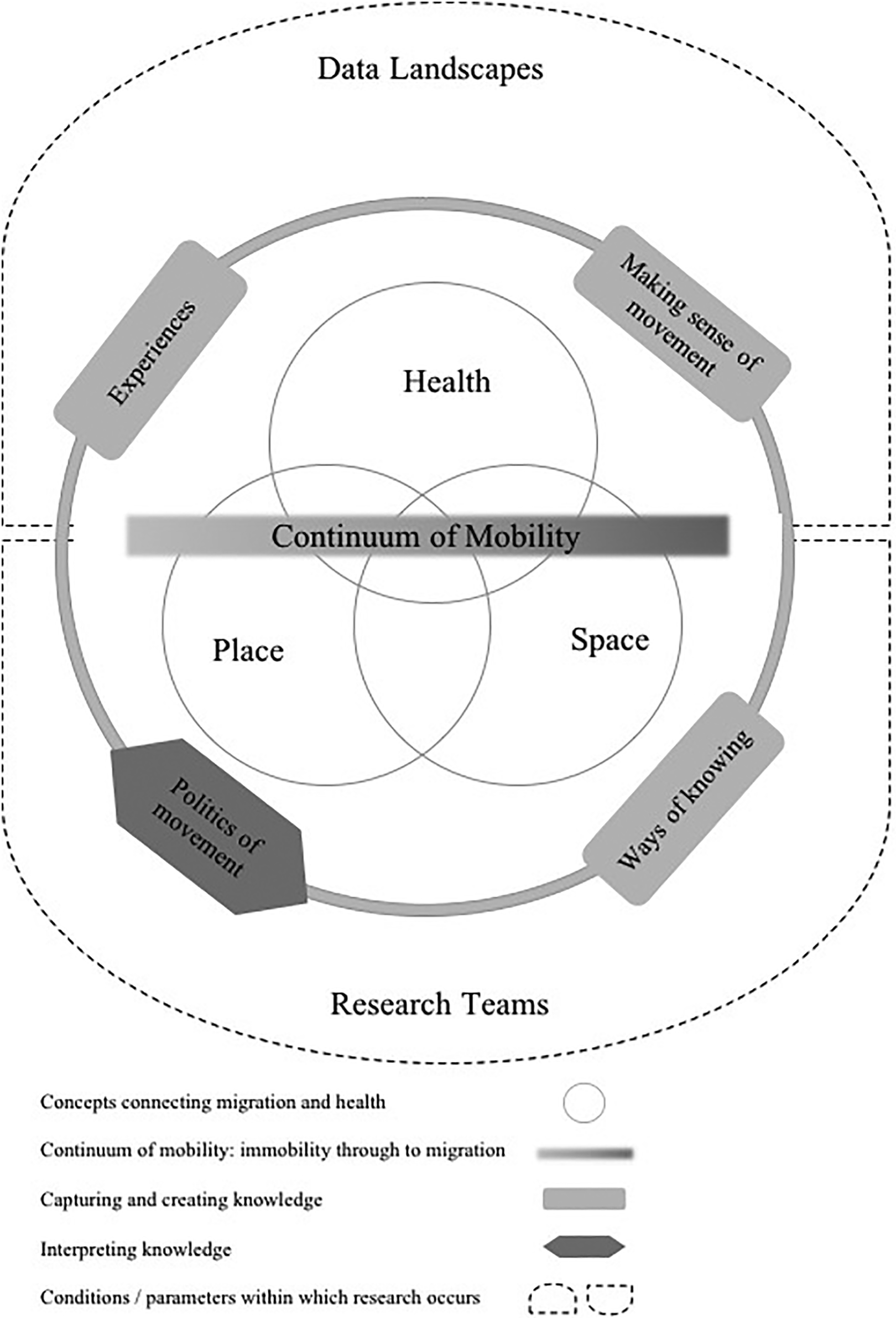
Mobilising mobilities to unpack migration, health and inequalities (developed by the authors).
VII Conclusions
Published in 2012, King’s landmark paper reviewed the past character of and trends in geographic work focused on migration, speculating towards its future. In particular, King noted a shift from ‘population’ approaches to quantifying movement to ‘cultural’ approaches unpicking that movement via the subjective stories that underscore it (see also Thompson’s (2017) paper on a geographical imaginations approach to migration studies). King also contended that population approaches and cultural approaches will remain important but hinted to taking more seriously economic (as well as cultural) factors. Some years since King’s paper, there is still work to be done to deepen understandings of migration, and as we have argued, health-selective studies of migration which remain under-theorised in their predominantly quantitative analytic scope. Although ‘mobility’ and ‘migration’ appear often together in paper titles and academic parlance, a thorough integration of the new mobilities paradigm and what it can offer to understanding topics such as health-selective migration is still absent. Turning to the new mobilities paradigm also forces population and health geographers to look back to traditional lifecourse theory, rather than engaging with more recent empirical work in lieu of a more robust theoretical framing. Similarly, qualitative examinations of migration and health lack an overarching analysis concerning the patterning or trends shaping migration. We advocate that the new mobilities paradigm, and a framework inspired by three approaches – conceptual, analytic and methodological – could enhance research.
Rather than just voice this potential (as other papers have), we establish how such research could be deepened through the deployment of mobilities thinking in our tri-part discussion and in the framework developed in the previous section. If research on health-selective migration lacks an understanding of the drivers, experiences and politics of such migration, mobilities thinking – which has this aim at its heart – is well placed to offer scholars a set of ideas and applications to enhance, layer-over and bolster aggregate analysis. Likewise, in making this connection, quantitative analysis can enrich the specificity of much mobilities work by providing ‘bigger picture’ data on the shape of migration(s). The mobilities paradigm is well placed to bring together research areas because it is an approach fundamentally, above all else, interested in making sense of movement. But more importantly, in its emphasis on relationality, it is as illuminating in understanding non-movement or immobilities. It has the capacity then to act as a bridge in connecting research and also creating new questions for research. Indeed, if quantitative scholars of migration start with a ‘mobilities’ approach attuned to the politics of movement, the questions they ask may change, and shape of their research and the outcomes it produces may be radically different. How these changes unfold remains for future research(ers) to uncover.
In the context of health-selective migration, mobilising a mobilities perspective deepens not only our knowing of the geographies of health, migration and possible mechanisms that may contribute to changing health gradients but also our ways of knowing. This approach then lends itself to more than just research into health and migration. Any inquiry beginning with the premise that a relocation between point A and B may have implications for particular outcomes either at the individual- or population-level may similarly be enriched by mobilising a mobilities framework and ensuring integration, analytically, conceptually and methodologically (in respect of the research tools and data we use). Insofar as migration functions as a sorting process, redistributing populations between areas and area types, understanding the impact of this sorting process on social and spatial inequalities is critical if we are to close long-standing gaps. Where we are attuned to the politics of movement, existing and future research into the impact of migration on employment and labour market outcomes, housing, education systems and even integration will benefit from the sort of approach outlined in this article.
Such an effort is only possible by encouraging inter- and cross-disciplinary working and conversation – such as has emerged through the writing of this article: a collaboration between a scholar of health and migration using mainly quantitative methods and a cultural geographer of mobilities mainly using qualitative approaches in their work. As Hui recently noted, ‘there has…been a significant body of collaboration’ between researchers of migration and mobilities, but ‘boundaries and obstacles have at times limited engagement’ (2016: 79). This article has aimed to engage through not only voicing shared ideas but providing a framework for connecting research areas through theory and mobilising the new mobilities paradigm.
Research into health-selective migration, in particular, may be constrained by the available data, but it need not be constrained by theory or what that theory enables for deepening conclusions (and creating new questions to investigate). A strong theoretical basis regarding the politics of mobilities can help say more of the structural factors shaping health-selective migration and therefore, changing health gradients in a population. And, it need not end here. The framework outlined may also hold potential for other areas of migration studies and add greater nuance to work in mobilities. Indeed, this resonates with Kaufman et al.’s (2004) articulation of the parallels between social and spatial mobility and the concept of motility as a means to understand the inter-relations between different forms of mobility and mobility potential. Yet the framework we propose is only possible, however, through a continued openness, or, as Hui notes ‘finding new questions or problems to engage researchers from fields’ (2016: 80). This article has emerged through this very process; through questions the authors had regarding limitations of each of their research fields. Conference sessions, papers and ultimately research projects that seek to address ‘new questions’ will be essential moving forward and mobilising work in migration studies further.
Footnotes
Acknowledgements
The authors thank Dr Michael Thomas (Statistics Norway) and Dr Jennifer Turner (University of Liverpool) for constructive comments on earlier drafts. The authors are also grateful for the extensive, thought-provoking and helpful feedback received during the peer review process which has greatly enhanced our thinking. Finally, the authors would also like to thank colleagues in the Department of Geography and Planning at the University of Liverpool for nurturing discussion across sub-disciplinary divides. Particular thanks to Professor Andy Plater, for his support in encouraging this cross-collaboration.
Authors’ note
A version of this article was presented at the British Society for Population Studies Conference.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.