
Abstract
The UK’s foster care system supports over two thirds of children in care, with the majority being in care due to maltreatment, neglect or family-related adversities. While evidence shows that children in care face greater risks of emotional, behavioural and mental health challenges than the general population, foster care uniquely offers children the opportunity to build attachment relationships that can be protective in the face of adversity and support their overall wellbeing. However, differences in outcomes and operation between independent fostering agencies (IFAs) and in-house local authority (IHLA) foster placements remain largely underexplored. This study investigates the characteristics, psychological needs and stability of children/young people in IFAs and IHLAs using data from the online BERRI assessment. Findings reveal that children in IFAs are typically older and experience greater psychological needs than children in IHLA fostering. Despite these differences, children in both placement types were found to be similarly susceptible to risk, and demonstrated comparable stability and trends in mental health outcomes over an approximate four-month period. These findings suggest that IFAs perform an alternative function to IHLAs, where they appear capable of providing support that better accommodates children with more complex needs, though this distinction requires further investigation.
Plain language summary
In the UK, the vast majority of children in care are supported within the foster care system, often due to experiences of maltreatment, neglect or family difficulties. These early adversities can have a knock-on effect on a child or young person’s mental health and behaviour, where children in care often face greater challenges with their overall wellbeing than the general population. However, foster care can help by offering children the opportunity to build positive, nurturing relationships with carers that can be protective in the face of adversity and support their overall wellbeing. In the UK, foster placements can be provided either directly by a local authority (public sector) fostering service or through an independent fostering agency in the private or voluntary sector. Differences in outcomes and operation between independent fostering agencies (IFAs) and in-house local authority (IHLA) foster placements remain largely unexplored. This study investigates the characteristics, mental health needs and the variation in these needs over time amongst children/young people in IFAs and IHLAs using data from the online BERRI assessment tool. Findings reveal that children placed in IFAs are typically older and experience greater psychological needs compared to children in IHLA foster placements. Despite these differences, children in both placement types appeared equally at risk of harm from themselves/others, and both groups of children demonstrated similar stability and changes in their mental health outcomes over approximately four months of follow-up. These findings suggest that IFAs perform an alternative function to IHLA foster placements and may be better equipped to support children who experience more complex mental health needs, though this distinction requires further investigation.
Keywords
Introduction
In 2023, there were 83,840 children in care in England (Office for National Statistics [ONS], 2023) and 107,000 in the UK (National Society for the Prevention of Cruelty to Children [NSPCC], 2024). Foster care is the most common placement type across the UK, accounting for 66–83% of children in care in 2023 (NSPCC, 2024). The remainder live in residential care (staffed provision that provides full-time care for one or more children), supported accommodation (accommodation with some staff visits that is defined not to provide ‘care’ and is only legal for young people aged 16 or above) or with connected people, such as non-parent relatives. Smaller numbers live in secure units, residential schools, independently or at home with their parents with social work supervision. Research has consistently shown that children in care face significant challenges and have higher rates of behavioural and mental health problems than the general population (Hiller et al., 2020; National Institute for Health and Care Excellence [NICE], 2021; Sanders, 2020).
The most common reasons for children arriving in foster care are maltreatment and neglect (Department for Education [DfE], 2024; Jackson et al., 2014). Seventy percent of former foster children report over five adverse childhood experiences (Bruskas and Tessin, 2013). These experiences can negatively affect a child’s emotional, behavioural and academic development, consequently putting children growing up in care at elevated risks of experiencing mental health problems and subsequent difficulties with social integration in adulthood (Engler et al., 2022; Owusu-Bempah, 2010; Viner and Taylor, 2005). Given the high level of association between adversity and trauma for children in care, it is therefore unsurprising that research has consistently documented that psychological difficulties and diagnosable mental health conditions are disproportionately common within this population (Ford et al., 2007; Forsman, 2025; Luke et al., 2014; Sawyer et al., 2007). Furthermore, children in care are 50 times more likely than their peers to experience poorer educational and employment outcomes, as well as greater rates of sexualised behaviour, criminal convictions, attention difficulties and homelessness, which may be contributed to by emotional and behavioural challenges (Forsman and Brännström, 2024; Hiller et al., 2020; Knight et al., 2006; NICE, 2021; Roberts et al., 2017; Svoboda et al., 2012; UK government, 2023).
Efficacy of foster care intervention
Attachment is a pivotal factor in outcomes for children in foster care. Children removed from their birth parents after infancy intrinsically lack the opportunity to develop secure attachments from a consistent caregiver – a well-evidenced protective factor in the face of childhood trauma (Lieberman et al., 2005; von Cheong et al., 2017). Foster care offers dyadic attachment relationships that may not be possible within residential and other forms of placement which involve a staff team providing care and/or support for a child or group of children. These relationships can offer reparative or even therapeutic reparenting (Balbernie, 1989; Dalgaard et al., 2022). It is through healthy and stable relationships that children can return to a healthier developmental trajectory and more trusting positive relations with others who can support their development (Herman, 2002).
Whilst recent longitudinal research has found that children placed in foster care were at a higher risk of experiencing poor labour market status later in life compared to the general population (Forsman and Brännström, 2025), other research suggests that children in care have better life outcomes than children who were at a similar level of risk but were not removed from their family of origin (Luke and O’Higgins, 2018). Similarly, children in foster care have been found to have better educational outcomes than children in need who remain within their birth family (Sebba et al., 2015). However, a meta-analysis by Dubois-Comtois and colleagues (2021) found that young people in foster care had more mental health difficulties than both community and matched/at-risk samples but similar levels of difficulties to children living with their biological parents who are involved with child-protective services. The researchers suggested that children in foster care likely faced greater risks and maltreatment prior to entering care than those who remained with their biological parents, so the lack of difference in mental health outcomes may indicate that foster care prevents further deterioration but does not reduce difficulties below the level experienced by maltreated children who stay with their parents.
Fostering agency- versus local authority-delivered foster placements
In the UK, foster carers are self-employed but must be approved by and registered with a fostering service provider inspected by Ofsted (England) or the Care Inspectorate of Scotland or Wales (Northern Ireland currently has no inspections or standards for foster care). Fostering services in the UK can be either a local authority (public sector) fostering service or an independent fostering agency (IFA) in the private or voluntary sector. The balance between the use of public and private foster care services varies across different countries and cultures. The UK’s structure tends to share similarities with that of Sweden and Norway, where local authority and IFA foster care coexist (Fridell Lif, 2023), whereas within the US, privatisation is generally more prevalent, with some states fully privatising their foster care system (e.g., Florida; Steen, 2013). In England, local authority-run services (which are known as ‘in-house’ provision and abbreviated here as ‘IHLA’) directly deliver the majority (46%) of foster care households. This is closely followed by IFAs, which make up 43% of fostering households, with the remainder in friends and family households (Ofsted, 2023). IFAs are more likely to offer solo placements, which partly explains why the number of children cared for in them is slightly lower than the proportion of fostering households. However, the proportion of fostering places offered by IFAs within England has risen from accounting for 42% of filled fostering places in 2019 to 47% in 2023 (Ofsted, 2023).
Despite the rising use of IFAs, it has been highlighted that the relationship between local authorities and IFAs is complex, and there are reports of mistrust between organisations (Baginsky et al., 2017). This has led to conflicting perspectives and policy challenges about costs and benefits, overlaid on existing issues of supply and demand within foster care.
Since their introduction in the UK, IFAs have helped to address foster carer recruitment difficulties faced by local authorities (Sellick, 1999) and to accommodate children’s diverse needs (DfE, 2018), where local authorities have limited capacity to care for the number of children entering care, especially those with more complex needs who require more specialist foster placements (Baginsky et al., 2017). Local authorities tend to follow an ‘in-house first’ policy, where a suitable foster placement is first sought within IHLA foster carers (Narey and Owers, 2018) and IFAs are only used as a last resort when an appropriate in-house foster carer cannot be found (Sellick, 2011). IFAs are often associated with greater costs for the local authority than in-house foster placements, though not to a degree that should influence the decision about the right placement (Narey and Owers, 2018; Sellick, 2007). However, some have suggested that this differential cost may be influenced by IFAs being structured to care for greater numbers of children with more complex needs, including older children, children with higher scores on the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997), those with special educational needs and those with substance misuse difficulties (Narey and Owers, 2018). Compared to IHLA foster placements, Narey and Owers (2018) also noted that IFAs invest more into support and training for foster carers, and social workers within IFAs typically manage smaller caseloads than those in local authorities. As a result, views of IFAs tend to be divided, with some viewing them as profit-driven (as the majority are profit-making companies, although some IFAs are charities, social enterprises or have other not-primarily-for-profit structures), whilst others believe that they are innovative in developing a holistic approach to fostering children (Sellick, 2011).
Whilst some comparisons between public and private foster care have been evidenced within Western nations, there is a paucity of conclusive research within this area (and no studies from the Global South have been identified). Academics within the US have examined public versus private foster care with mixed results. Griffiths and colleagues (2021) found private foster carers more satisfied, better prepared and more open to fostering a more diverse pool of children, and Kessler and colleagues (2008) reported better outcomes overall for care leavers in private foster care. Conversely, US research has also suggested that private foster care is associated with a higher incidence of multiple placements (Steen and Duran, 2013). Given these mixed findings, it is unsurprising that other US studies have concluded that both types of foster care have distinct advantages, without one being superior to the other (Huggins-Hoyt et al., 2019; Steen and Smith, 2012).
UK research involving private foster care agencies show generally positive views on IFAs (although much of the research on this topic within the UK is dated): children and young people within IFAs expressed high levels of satisfaction with the care they received, their IFA social worker, and the activities and support provided (Selwyn et al., 2008). This was further supported by reports from local authority social workers, where it was concluded that 97% of IFA cases were going well or quite well (Selwyn et al., 2008). Compared to IHLA foster carers, staff working within IFAs also have generally higher levels of satisfaction, particularly due to the support, educational and therapeutic services provided by the agencies (Sellick, 2011). Finally, where the quality of care provided by IFAs has been brought into question, Narey and Owers (2018) found no clear differences between IHLA foster placements and IFA placements and highlighted that in 2017, 91% of IFAs were deemed by Ofsted to be good or outstanding.
Despite this, much remains unknown about the differences in outcomes, health, education and stability for those within IFA placements compared to those within IHLA foster placements in the UK.
Research aims
Due to limited research directly comparing children in IFAs and IHLA foster placements, this study set out to examine differences in the BERRI scores (a measure of psychological needs) between professional/caregiver ratings of children and young people in both IHLAs and IFAs, as well as differences in age, gender and experiences of life events. A secondary question explored whether scores on the BERRI remained stable over time. This was analysed in both types of foster placement. Though the overall BERRI total score was reported, five subscales covering ‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships and attachments (Relationships)’, ‘Risk to self and others (Risk)’, and ‘Indicators of atypical neuropsychological and psychiatric development (Indicators)’ were also examined. Further information on the BERRI assessment measure is detailed below (see Measures section) or can be accessed at berri.org.uk/.
The research hypotheses are as follows:
Children in IFAs demonstrate significantly different psychological needs (measured by BERRI scores) compared to those in IHLA foster placements. The level of stability over time (measured by changes in psychological needs/BERRI scores) will differ depending on foster placement type (IFA or IHLA foster placement).
Methods
Data collection
The data used were anonymised naturalistic data extracted from the BERRI Limited database between 2021 and 2024, where the online BERRI tool was used by 14 local authorities and four private care providers regarding children in foster care. Of the four private care providers, all provide therapeutic foster care but do not specify whether they cater to children with specific needs/complexity and are thus considered ‘standard’ fostering agencies. Within the local authority data, information regarding the type of IFAs was unknown.
Whilst BERRI has often been used with children where there are particular concerns or with a high level of complexity (Competition and Markets Authority, 2022), the majority of local authorities included in this study aimed to use BERRI with a representative sample of children in their care, accounting for 61.8% of all BERRI records in the study’s larger sample. The remaining local authorities used BERRI with children about whom they had particular concerns in terms of placement stability or a move from residential to foster care, accounting for 7.6% of all BERRI records in the sample. The majority of BERRI records directly from IFAs were also from providers who aimed to use BERRI with all the children in their care, accounting for 26.7% of all BERRI records in the sample. The remaining BERRI records directly from IFAs were from providers who used BERRI with a particular subset of children, weighted towards children about whom they had particular concerns in terms of psychological needs, which accounted for 3.9% of all BERRI records in the sample.
This data contained the birth year, gender, placement type, BERRI assessment date, BERRI total and subscale scores and recent life event information. All BERRI user information was anonymised before being securely sent to the research team. No personal information, such as names, ethnicity, exact age or address, is collected during BERRI completion, thus the data are anonymised at point of entry. BERRI collects only birth year, not exact date of birth, to preserve this anonymity, and therefore the ages of participants used in this study are approximations calculated by subtracting birth year from the year the BERRI assessment was completed.
Ethical approval was obtained through University College London (Project ID: 0389 051). The data collection and storage adhered to data protection legislation including the GDPR (Data Protection Act, 2018), ensuring data remained anonymous, stored securely, with no individuals able to be identified.
Sample
The overall sample included in the analysis consisted of all BERRI assessments (720 BERRI records) completed for 436 children/young people in foster care. Just over half (55.3%) of the overall sample were male (n = 241) and 44.7% were female (n = 195). Five children recorded as non-binary were excluded from the overall sample and analyses due to implications for statistical validity; including such a small group could lead to unreliable results, and meaningful comparisons between this small group and other genders would not be possible. One child within the IFA sample had incorrectly recorded date fields. This child remained in the overall sample, but their age was imputed to the average age of their group. The approximate age of the sample ranged from less than one year old to 19 years old (M = 11.18, SD = 4.25).
Within this sample, 56.2% (n = 245) of children were in IFA placements and 43.8% (n = 191) were in IHLA foster placements. Some children within the BERRI data had multiple assessment records within different placement types (for example, due to a child moving from residential care to foster care). In these instances, only the assessments completed whilst the child was in foster care were included in this sample. All children in IHLA placements were rated by staff from the child’s local authority. Children in IFAs were rated by either IFA staff or local authority staff.
In conducting the analyses, subsamples of the overall dataset were formed and utilised to address specific research questions appropriately (see Figure 1):
Sample A: This sample included only the first BERRI assessment for each child within an IFA placement or IHLA foster placement (n = 436). Sample B: This subgroup of Sample A included only the 245 children placed in IFAs. The first BERRI assessment completed by either staff within an IFA or local authority was utilised. One hundred and ninety children were rated by local authority staff and 55 children were rated by staff from their IFA. Ratings within the local authority were completed by the child’s social worker with various levels of input from the foster carer, while ratings by IFA staff were completed by the foster carer jointly with the linked social worker; ratings by IFA staff may be skewed as they are more likely to provide some direct care for the child’s day-to-day needs, whereas local authority social workers may only hear about more significant issues. The children rated by local authority staff were aged between one to 17 years old (M = 11.9, SD = 3.45), and the children rated by IFA staff were aged between one to 18 years old (M = 11.1, SD = 3.75). Sample C: This subgroup of the overall sample included only children in IFA or IHLA foster placements who had at least two BERRI assessments where there were at least three months between the first and successive assessment(s). This resulted in an assessed sample of 107 children, consisting of 69 children in IFA placements and 38 children in IHLA foster placements. To ensure a fair time interval between the first and successive BERRI questionnaires for comparison, average intervals (M = 4.8 months, median = 4.0 months) were calculated for children within this sample who had only two BERRI records (n = 66), and this mean interval was used as a basis to select an appropriate successive BERRI with a similar interval for those with more than two BERRI records (n = 41). For children in IFA placements, the time between the first and second BERRI assessment ranged from 3.0 to 9.5 months (M = 5.3 months, median = 4.1 months). For children within IHLA foster placements, the time between the first and second BERRI assessment ranged from 3.1 to 9.4 months (M = 4.9 months, median = 4.7 months). Within the IFA group, 30 of these children were rated by staff within an IFA, and the remaining 39 children were rated by local authority staff.
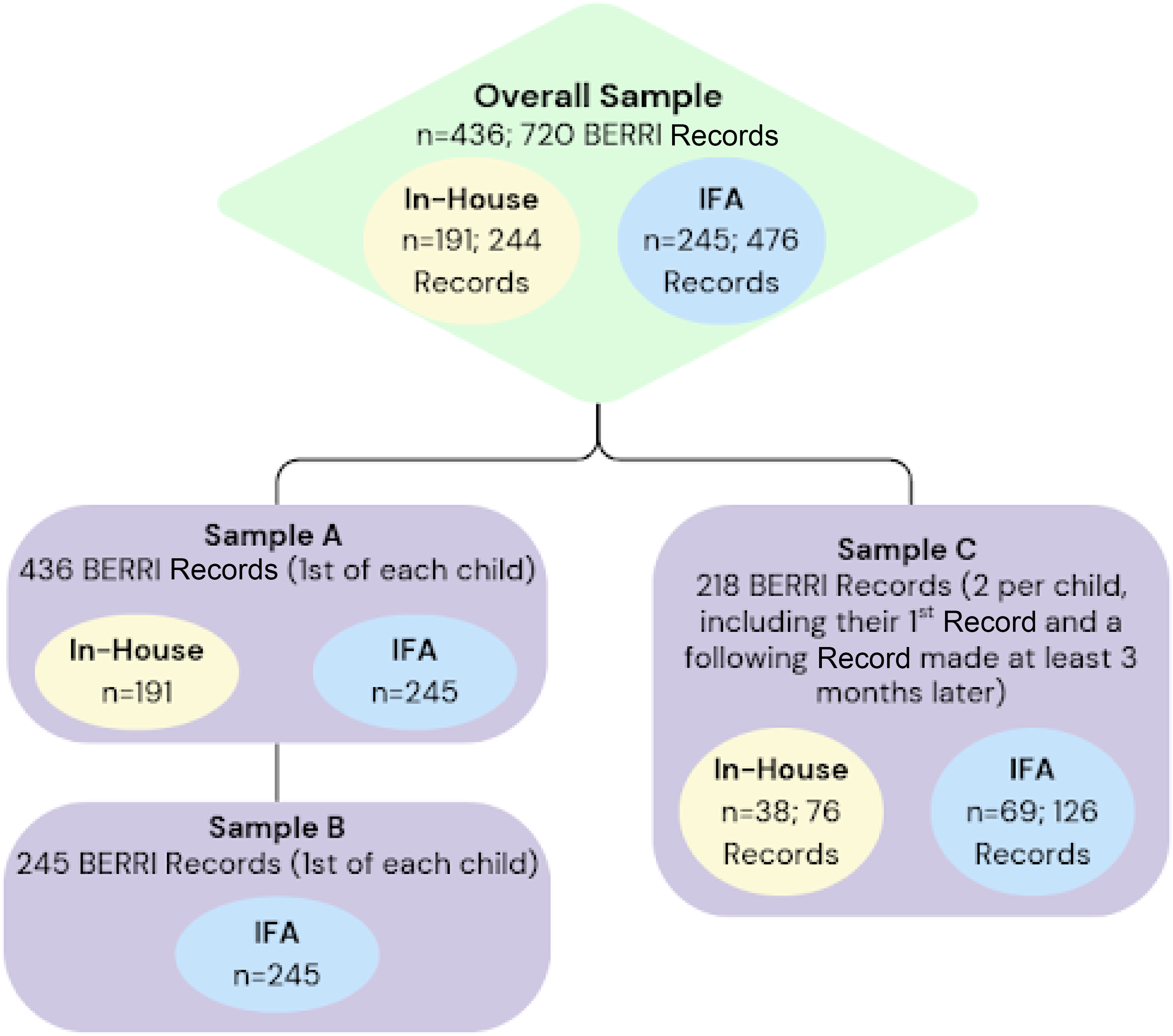
Visualisation of study samples and comparison groups.
Measures
BERRI is an online assessment tool consisting of 87 items, which measures the psychological needs of children in care on five subscales: ‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships’, ‘Risk’ and ‘Indicators’. BERRI has been widely used to map the psychological needs of children in care within the UK (BERRI, 2015).
The ‘Behaviour’ scale (19 items) includes items around externalising behaviours, such as aggression. The ‘Emotional wellbeing’ scale (18 items) contains difficulties associated with affect and self-concept, such as low mood. The ‘Relationships’ scale (15 items) measures difficulties in creating and maintaining relationships with peers and carers, such as lacking empathy. The ‘Risk’ scale (14 items) consists of items relating to a young person’s level of risk towards themselves and others, such as self-harm. Finally, the ‘Indicators’ scale (21 items) includes items indicative of neurodevelopmental conditions and other psychiatric symptoms, such as lacking concentration.
The BERRI assessment also collects information relating to demographics (birth year, gender, placement type) and has a measure of recent life events. The life events measure consists of 17 items representing various recent circumstances that may have occurred within the past three months and can provide context to changes in the child’s psychological needs. For example, ‘change in contact/family time’, ‘court proceedings’ and ‘death of a significant relationship figure’. The rater selects which life events, if any, have occurred for the child within the past three months. The number of life events recorded are totalled to give a life event count for the child (e.g., if four life events are recorded for the child, they will have a life event count of 4; if none are recorded, they will have a count of 0). BERRI is used within care organisations and local authorities, and the data are routinely collected from carers and professionals (such as foster carers, social workers, teachers, therapists and other members of the care team) who fill out an assessment about a child within their care. The BERRI takes around 11 to 15 minutes to complete by an individual, or 20–30 minutes to discuss and complete as a team around the child.
For this paper, psychological needs were measured using the five BERRI subscales and a total BERRI score. For each of the subscales, carers rate a number of items based on two scales that measure their frequency and difficulty to manage using a 0–4 Likert scale (where 0 indicates never/does not occur, and 4 indicates that the item occurs at a high frequency/is extreme and requires substantial support). These scores are then multiplied together to give a challenge score from 0–16 for each item (with 0 indicating the least challenge, and 16 indicating the most challenge). Challenge scores are totalled for each subscale to give separate ‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships’, ‘Risk’ and ‘Indicators’ scores. All subscale scores are also totalled to give an overall total BERRI score. Higher subscale and total BERRI scores indicate a higher level of psychological need.
The BERRI measure has demonstrated good internal consistency and construct validity for all subscales in previous studies (Harris, 2019; Viziteu et al., 2024). Total BERRI score, along with both ‘Behaviour’ and ‘Risk’ scales, had moderate to good inter-rater reliability (Harris, 2019). More recently, the BERRI has been shown to be reliable, valid and sensitive to change, with a factor structure that is clinically meaningful (Viziteu et al., 2024). In the current sample, internal consistency for challenge scores of each BERRI subscale was assessed using Cronbach’s alpha, as follows: Behaviour (α = .83); Emotional wellbeing (α = .89); Relationships (α = .91); Risk (α = .81); Indicators (α = .91). Altogether, this indicates good internal consistency across subscales.
Data analysis
Various analyses were conducted to explore the demographics and psychological wellbeing of children in each sample. All statistical analyses were carried out using R statistical software (v4.4.2; R Core Team, 2024).
Normality testing using the Shapiro-Wilk test indicated significant deviations from normality in the wider sample and all subsamples used within this study. Brown-Forsythe tests were also used to investigate homogeneity of variance between comparison groups throughout this analysis. Therefore, with consideration of normality, variances and uneven group sizes, non-parametric methods were used to investigate the hypotheses of this study. To control for multiple comparisons and analyses, a Bonferroni correction was applied separately for each of the preliminary tests and hypotheses tested in this study, adjusting a p < .05 level of significance to prevent false positive results.
Preliminary tests: Demographics, life events and rater effects – Sample characteristics and correlations
Before evaluating the aforementioned hypotheses, an investigation into sample and scoring characteristics was conducted, as well as an exploration into the effect of age, gender, number of life event experiences and questionnaire rater on BERRI psychological need scores. This helped to inform analytical plans in testing Hypotheses 1 and 2, as well as aid in understanding the implications of results from hypothesis evaluation.
Statistical tests were utilised to better understand demographic differences between the placement types. For age, a Mann-Whitney U test was performed to compare the ages of children within IFAs and IHLA foster placements. As variance differed between these groups, results were interpreted as a comparison of overall age distributions (mean ranks) rather than group medians. A Chi-squared test examined the association between gender and placement type. Additional Mann-Whitney U tests were used to investigate differences in the number of life events reported for children in IFAs and IHLA placements; in this case, group distributions were similar in shape, so results were interpreted as median differences. The significance level for this section was adjusted to p < .0125 after Bonferroni corrections.
Additionally, using Sample B, six Mann-Whitney U tests explored whether a child/young person’s BERRI score differed based on ratings by IFA or local authority staff. Results were interpreted in terms of medians, as similar distributions were found between comparison groups for each test. Bonferroni corrections adjusted the significance level for these analyses to p < .0083.
A correlation matrix was generated using Sample A to compare the relationships between age, gender, life events, rater and psychological needs according to the child’s total BERRI score and BERRI subscale scores. Medians, means and standard deviations of each variable were calculated, and 45 Spearman's Rank Correlation Coefficient tests were used to investigate the relationships between these variables. Gender was coded as 0 (females) and 1 (males), and BERRI rater was coded as 0 (local authority staff) and 1 (IFA staff). Although Spearman’s Rank correlations were used, in these cases the independent variable (gender or rater) was dichotomous. Therefore, this approach assesses the monotonic relationship between the ranked continuous outcome and binary grouping. All children within IHLAs were rated by local authority staff. After Bonferroni corrections, the significance level for this matrix was adjusted to p < .0011.
The results from this prior investigation informed covariate selection to enrich hypothesis testing, with analyses for each hypothesis structured as follows:
Hypothesis 1: Comparing psychological needs (BERRI scores) between foster placement types
Descriptive statistics were obtained for the five BERRI subscales and total BERRI score using Sample A. Given the violation of normality assumptions and potential for heteroscedasticity, the ranked ANCOVA (analysis of covariance) was chosen as a more robust alternative to the parametric ANCOVA. Six one-way rank-based ANCOVAs were carried out to test for differences between mean ranked total BERRI score and five BERRI subscale (‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships’, ‘Risk’ and ‘Indicators’) scores across each foster placement, factoring in the potential influence of age, life-event experiences and the rater of the BERRI questionnaire. The significance level for this analysis was adjusted to p < .0083 after Bonferroni corrections.
Hypothesis 2: Comparing stability of psychological needs (BERRI scores) over time between foster placement types
To explore the differences in stability over time between the first and second BERRI assessments for children in IFA and IHLA placements, descriptive statistics from Sample C (regarding the first BERRI, second BERRI and the calculated difference in scores between the two BERRIs) were analysed, as well as the average change in score. Six one-way rank-based ANCOVAs were then used to compare the change in total BERRI score and BERRI subscale scores between IFA and IHLA foster placement types, while accounting for the child’s age, life event experiences and the BERRI questionnaire rater. As with Hypothesis 1, this ANCOVA variant was selected with consideration of violations in normality assumptions and potential for heteroscedasticity. The significance level for this section was adjusted to p < .0083 after Bonferroni corrections. In addition, a further six ranked ANCOVAs were performed using the overall Sample C (children in IFA and IHLA placements combined) to compare total BERRI and subscale scores between the two BERRI assessment time points, irrespective of placement type. Significance level of this analysis was also set at p < .0083 after Bonferroni correction.
Results
This section presents the findings from analyses of IFA and IHLA foster placements. A variety of statistical tests were conducted to investigate the differences between the placement types, specifically differences in characteristics, psychological needs (BERRI scores) and changes in psychological needs (BERRI scores). P values were adjusted using Bonferroni corrections for each hypothesis. The results are detailed below.
Preliminary tests: Demographics, life events and rater effects – Sample characteristics and correlations
Age group
As demonstrated in Figure 2, IFAs appear to have a smaller percentage of children below eight years old than IHLA foster placements, with this difference being particularly evident in children aged below four. IFAs also have a greater percentage of children aged between nine and 16 years old; however, those aged 13–16 make up the majority of both IFA and IHLA foster placements. Both types of foster placement care for a similar percentage of adolescents aged above 16.
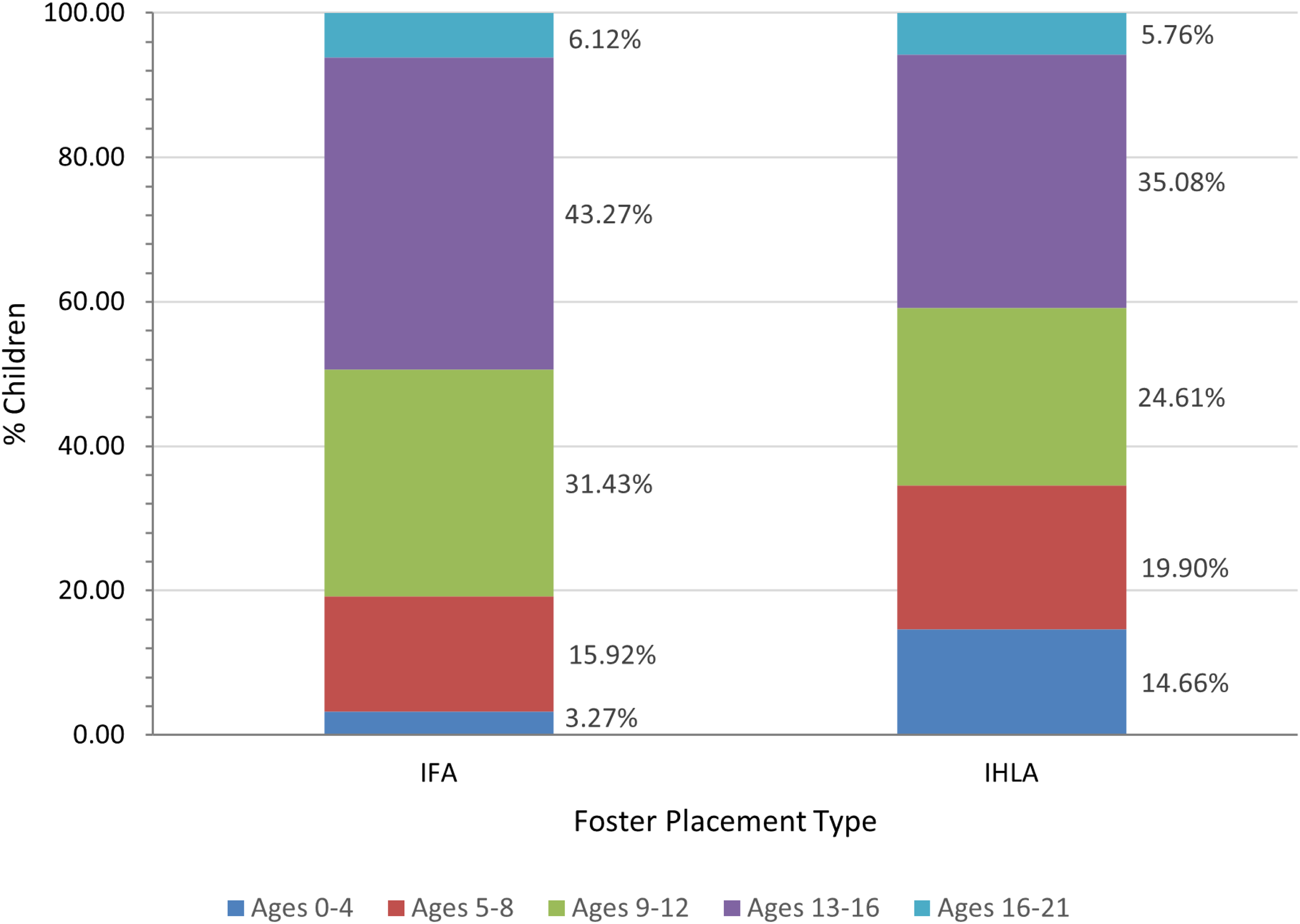
Age distribution among children in IFA and IHLA foster placements. Note. IFA: n = 245; IHLA: n = 191.
In examining children’s ages within the foster placement types, it was found that the mean age for IFA placements was 11.76 years (SD = 3.54) with a median age of 12 years, while the mean age for IHLA placements was 10.45 years (SD = 4.93) with a median age of 11 years. A Mann-Whitney U test revealed that the distribution of ages varied significantly between the two groups (U = 20584, Z = -2.16, p = .031), indicating that children placed in IFAs are significantly older than those in IHLA foster placements.
Gender
Figure 3 displays the percentage of children in each gender category within each foster placement type. There is a higher percentage of male children than female children in IFA and IHLA foster care. However, the proportions of male and female children appear to be more equal in IHLA foster care; this was investigated using a Chi-squared analysis (Table 1).
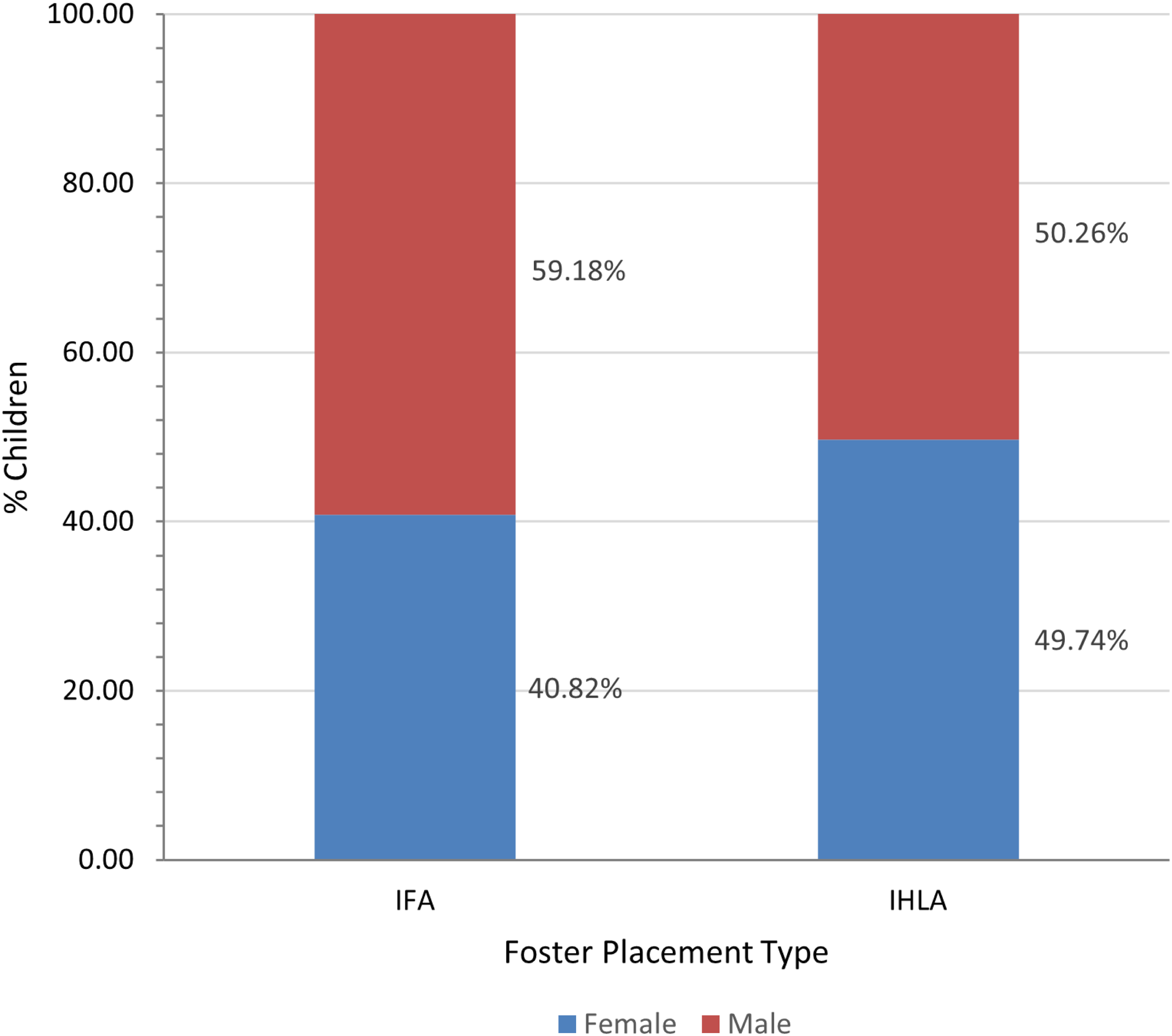
Gender distribution among children in IFA and IHLA foster placements. Note. IFA: n = 245; IHLA: n = 191.
Chi-squared analysis comparing gender differences in IFA and IHLA fostering.
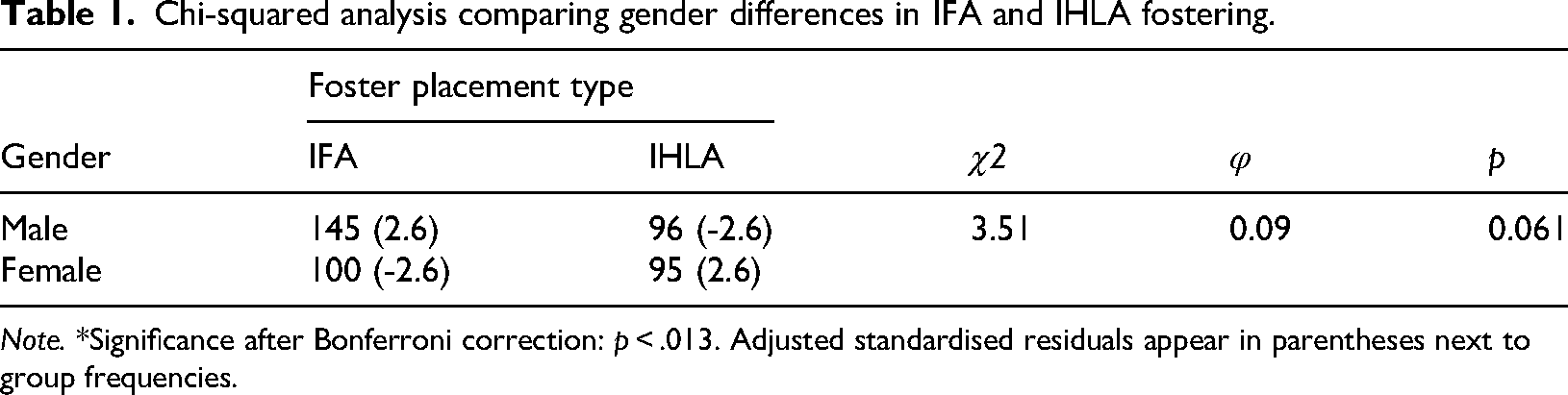
Note. *Significance after Bonferroni correction: p < .013. Adjusted standardised residuals appear in parentheses next to group frequencies.
A Chi-squared analysis (Table 1) reported that the difference in the percentage of males and females between IFAs and IHLA fostering did not reach statistical significance, χ2(1, N = 436) = 3.51, p = 0.061.
Life events
Figure 4 demonstrates the percentage of children who experienced a particular number of life events within the three months prior to their BERRI assessment in each type of foster placement. Over 80% of both groups experienced at least one life event within the past three months. Over one third of children in each group experienced at least three life events, and there were no clear differences between IFA and IHLA groups.
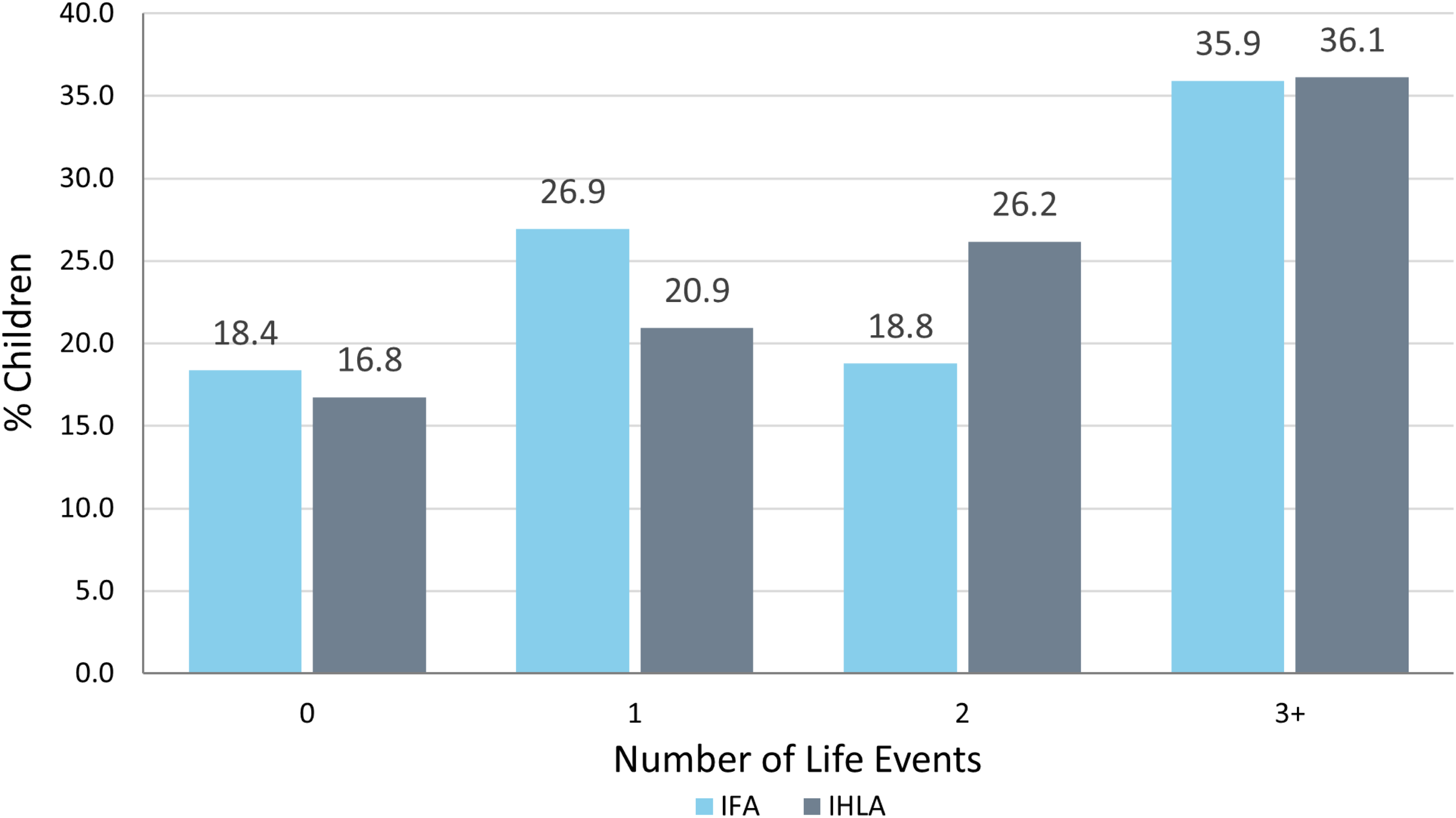
Number of recent life events experienced by children in IFA and IHLA foster care. Note. IFA: n = 245; IHLA: n = 191.
The mean number of life events faced by children within the three months prior to their BERRI assessment in IFAs was 2.23 (SD = 1.96) with a median of 2, while the mean for IHLA foster placements was 2.24 (SD = 1.85), also with a median of 2. The Mann-Whitney U test indicated no statistically significant difference (U = 24011.50, Z = 0.47, p = 0.63) in the median number of life events between the two groups, suggesting that there are no clear differences in number of life events experienced by children from IFA and IHLA foster placements.
Relationships between BERRI rater (IFA or local authority staff) and BERRI scoring
In addition to sample characteristics, the effect of rater on BERRI score was investigated. Differences in the psychological needs of children in IFA placements, measured by BERRI scores, when rated by staff from local authorities and IFAs were analysed using six Mann-Whitney U tests. Figure 5 shows the median total BERRI scores and subscale scores for both of these groups.
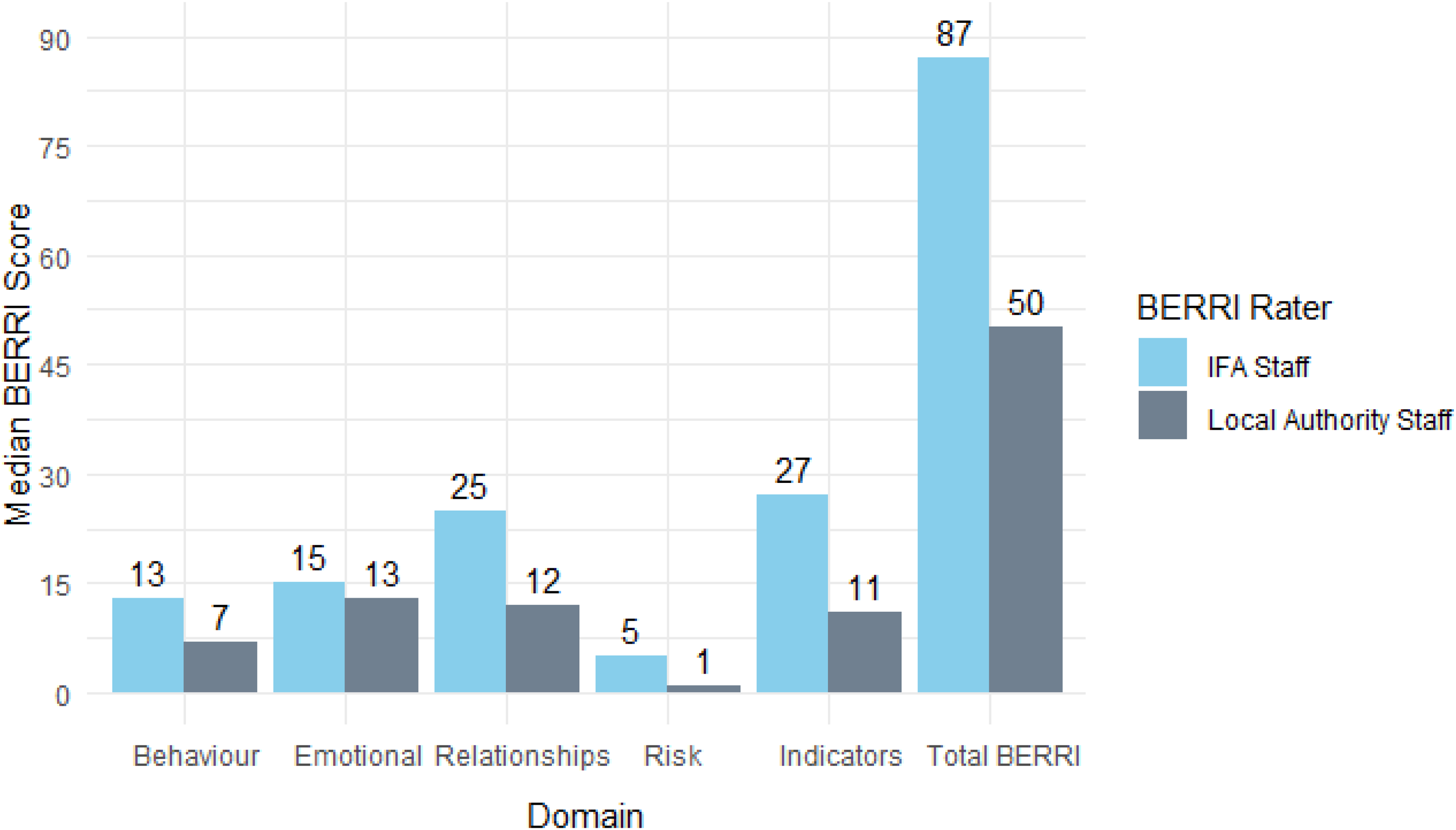
Median BERRI scores of children in IFAs, rated by local authority and IFA staff. Note. Local authority staff ratings: n = 191; IFA staff ratings n = 55.
Mann-Whitney U analyses revealed that children in IFAs who were rated by IFA staff have significantly greater BERRI scores for total BERRI and all BERRI subscales except ‘Emotional wellbeing’ when compared to children in IFAs rated by staff from local authorities. Results are provided in Table 2.
Mann-Whitney U results of test of difference in BERRI scores depending on BERRI rater (IFA children only).
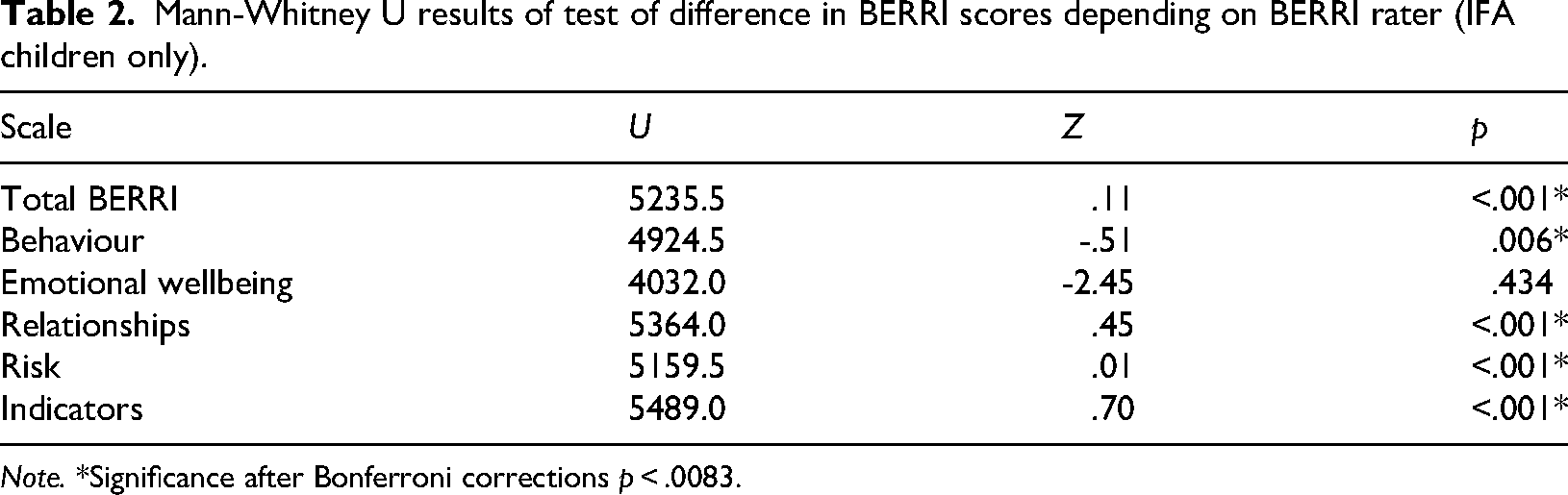
Note. *Significance after Bonferroni corrections p < .0083.
Correlations between sample characteristics and BERRI scoring
A series of Spearman’s Rank correlations were conducted to evaluate the relationships between the study variables (BERRI total and subscale scores, age, gender, life events and rater). This found significant relationships (p < . 001) between all BERRI subscales and total BERRI, indicating intercorrelation between all factors of psychological wellbeing as assessed by BERRI. Additionally, significant relationships were revealed between age and ‘Emotional wellbeing’, ‘Relationships’ and ‘Risk’ subscales, as well as with total BERRI score. A significant positive relationship was also found between life events and all BERRI subscale scores. This indicates that older age and experiencing a larger number of life events are both associated with higher BERRI scores. The rater of the BERRI assessment also appeared to have a significant positive relationship with total BERRI score and all BERRI subscales, excluding ‘Emotional wellbeing’. No significant relationship was found between gender and scores for any BERRI scale. Results are shown in Table 3.
Descriptive statistics and Spearman’s Rank correlations for study variables.
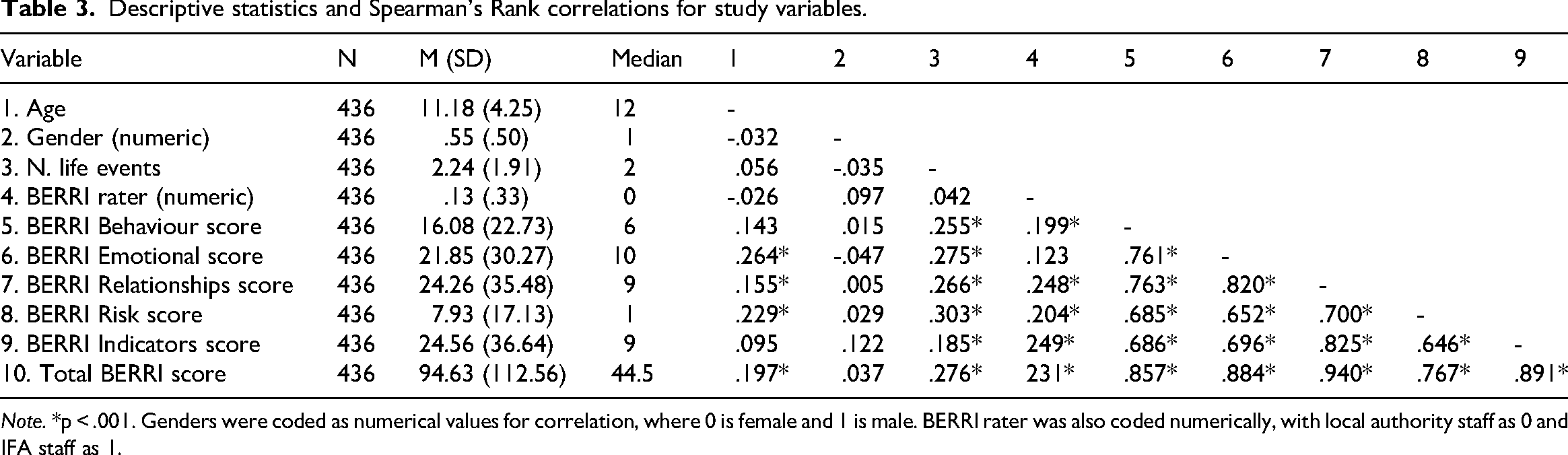
Note. *p < .001. Genders were coded as numerical values for correlation, where 0 is female and 1 is male. BERRI rater was also coded numerically, with local authority staff as 0 and IFA staff as 1.
Hypothesis 1: Comparing psychological needs (BERRI scores) between foster placement types
The differences in psychological needs, measured by BERRI scores, between children in IFA placements and IHLA foster placements were analysed. Figure 6 shows the median total BERRI scores and subscale scores for both of these groups.
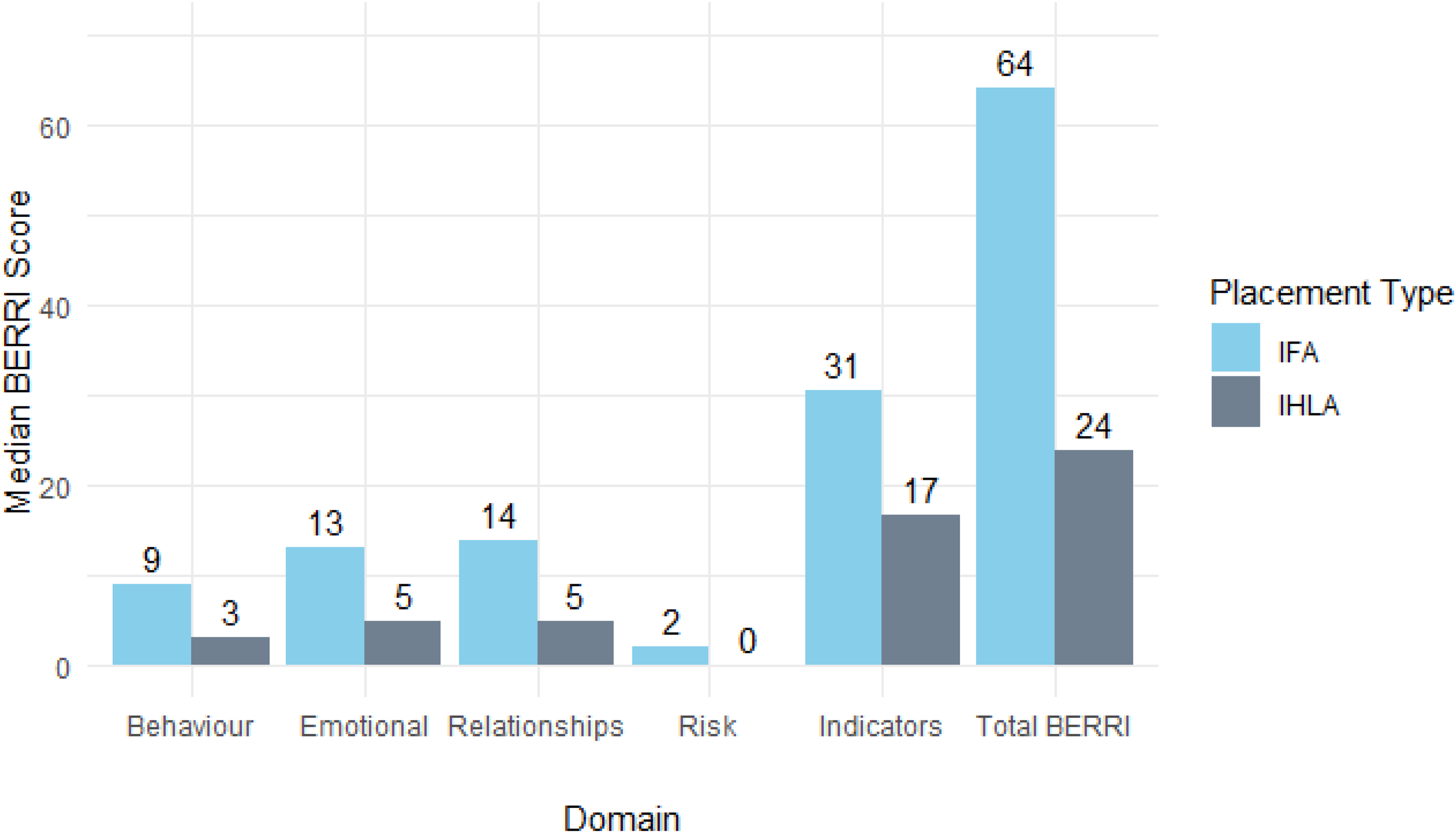
Median total and subscale BERRI scores of children in IFA and IHLA foster placements. Note. IFA: n = 245; IHLA: n = 191.
To investigate the effect of placement type (IFA or IHLA) on BERRI scores, several ranked ANCOVA analyses were conducted using age, number of life events experienced and rater as covariates. These were selected based on findings from the prior correlation matrix (Table 3), which indicated their relationship with BERRI scores. Gender did not show a significant effect on scoring, thus was not accounted for. P values indicating a notable result were compared to a Bonferroni-adjusted significance level of p < .0083. Results are in Table 4.
Results from six one-way ranked ANCOVAs investigating differences in BERRI scores between IFA and IHLA foster placements, controlling for age, number of life events and the rater of the BERRI assessment.
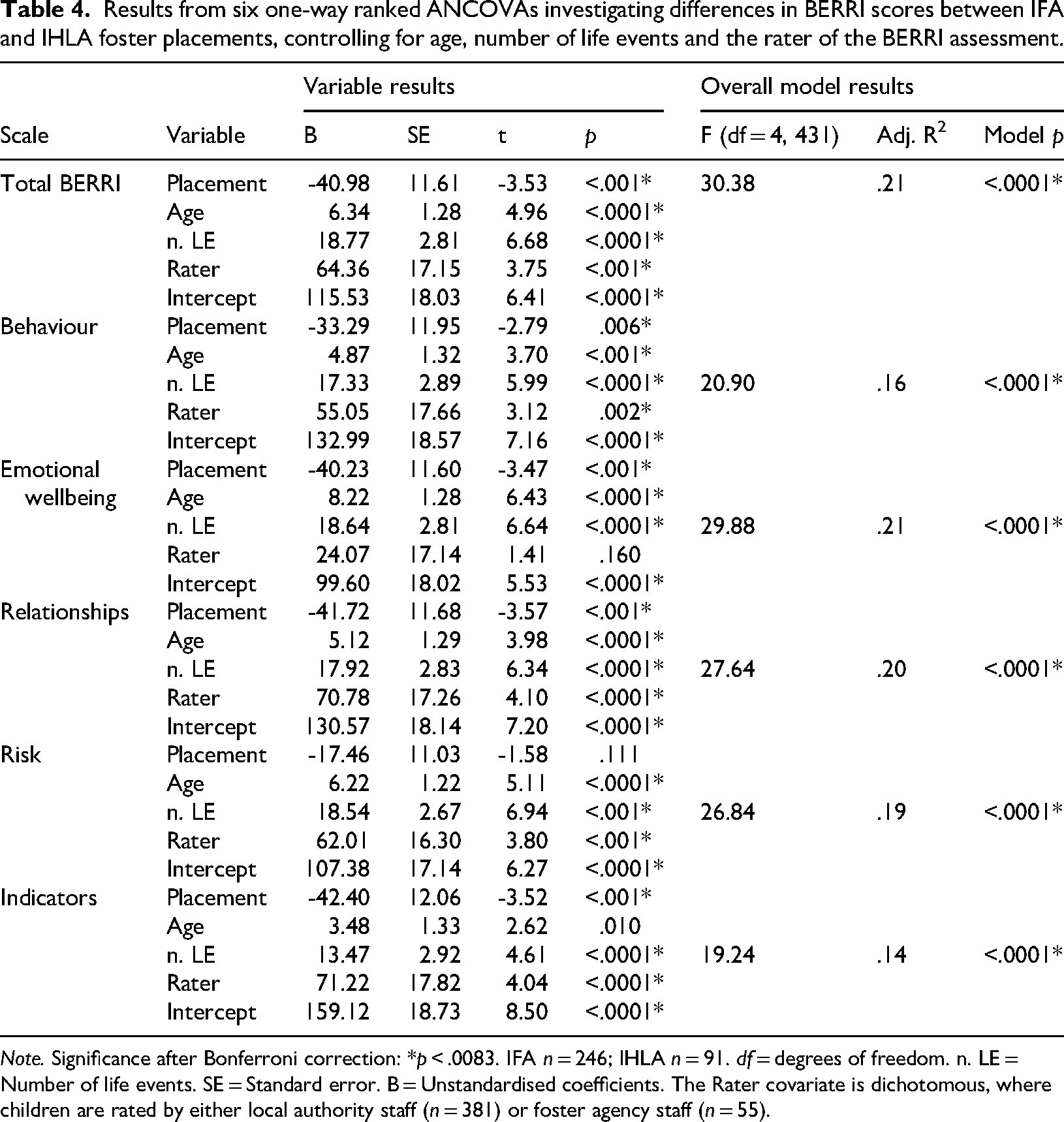
Note. Significance after Bonferroni correction: *p < .0083. IFA n = 246; IHLA n = 91. df = degrees of freedom. n. LE = Number of life events. SE = Standard error. B = Unstandardised coefficients. The Rater covariate is dichotomous, where children are rated by either local authority staff (n = 381) or foster agency staff (n = 55).
The analyses revealed that across total BERRI and all five BERRI subscales, the overall ANCOVA models were statistically significant (p < .0083), with F-statistics ranging from 19.24 to 30.38 and adjusted R2 values ranging from .14 to .21. This indicates that the models explained between 14–21% of the variance in ranked BERRI scores.
For total BERRI score, children in IFAs had significantly higher total ranked BERRI scores than those in IHLA placements (p < .0083), after controlling for the effects of age, number of life events and rater. Additionally, placement type showed a statistically significant effect (p < .0083) in four of the five BERRI subscales (‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships’ and ‘Indicators’), with children in IHLA care consistently showing lower ranked BERRI scores at their initial assessment and thus less complex psychological needs generally and less challenge within these areas compared to IFA children.
Furthermore, the covariates (age, rater and number of life events) were significant predictors of BERRI score in most models (p < .0083). The number of life events experienced significantly influenced scores for all BERRI subscales and total BERRI score, indicating that more life events were associated with a greater level of psychological need. Age was also positively associated with higher ranked scores in total BERRI, ‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships’ and ‘Risk’ subscales, suggesting that older children tend to have higher scores in these areas, regardless of placement type. Moreover, whether the BERRI rater was staff from an IFA or local authority appeared to affect the total BERRI, ‘Behaviour’, ‘Relationships’, ‘Risk’ and ‘Indicators’ scores (but not ‘Emotional wellbeing’), where staff from foster agencies rated children higher compared to local authority staff. Nevertheless, after accounting for covariates, significant differences between placement types persisted for total BERRI score and the ‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships’ and ‘Indicators’ subscales.
The only BERRI subscale that showed no statistically significant effect of placement type on scoring was ‘Risk’ (p = .114), although direction of effect remained consistent with those of the other BERRI subscales and total BERRI results. As all covariates were found to be significant predictors of scoring for this subscale, it can be suggested that the score variations for ‘Risk’ are more strongly influenced by the age of the children, rater of the BERRI and number of life events experienced, rather than type of foster placement.
Hypothesis 2: Comparing stability of psychological needs (BERRI scores) over time between foster placement types
Differences between first (T1) and successive (T2) total and subscale BERRI scores were analysed for children in IHLA foster placements and IFA placements. Descriptive statistics for change in score over time are detailed in Table 5. Average BERRI scores for both IFAs and IHLAs showed modest reductions from T1 to T2 across most BERRI subscales and total BERRI score, indicating slight improvements in children’s general psychological wellbeing during the period assessed. The only exception was the ‘Risk’ subscale within the IFA group, which showed a marginal increase in average score. The difference in scoring between the two placement types was then further analysed using ranked ANCOVAs (Table 6), with age, change in number of life events experienced between T1 and T2 and rater as covariates in reflection of the prior correlation matrix (Table 3).
Descriptives for first BERRI (T1), successive BERRI (T2) and the difference between first and successive BERRI scores (T2–T1) for IFAs and IHLA placements.
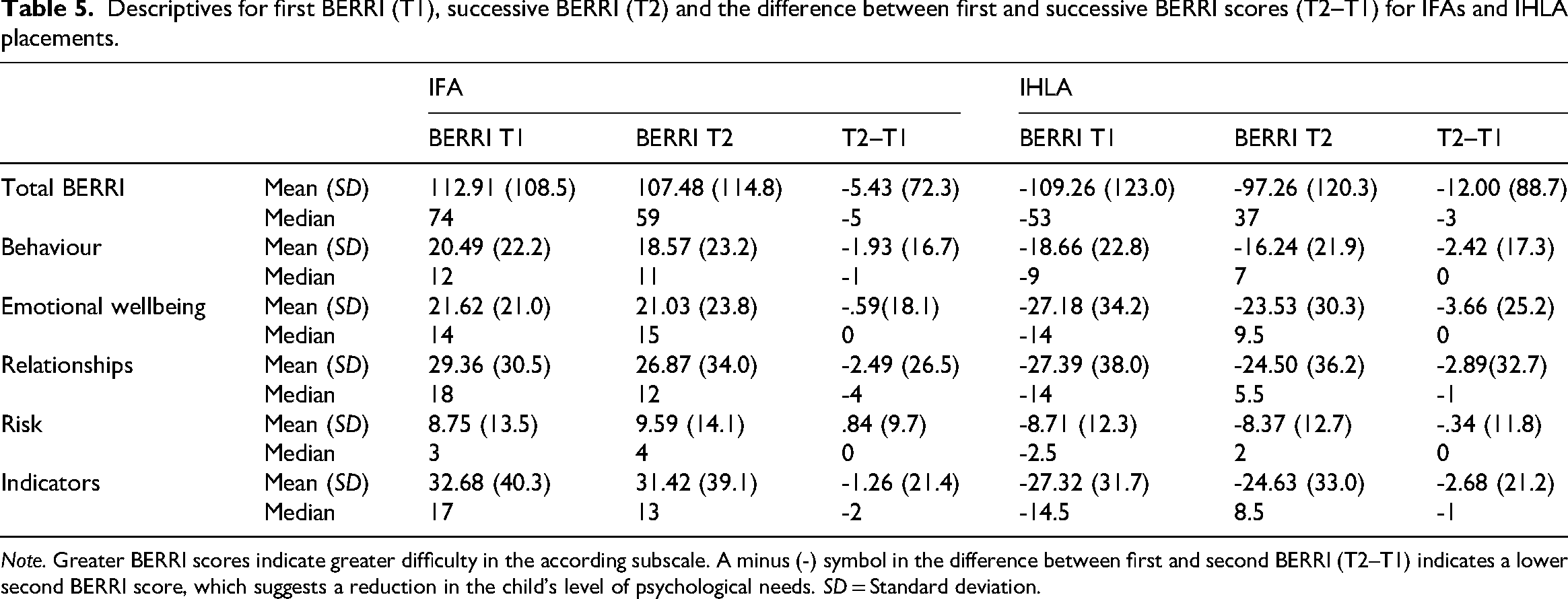
Note. Greater BERRI scores indicate greater difficulty in the according subscale. A minus (-) symbol in the difference between first and second BERRI (T2–T1) indicates a lower second BERRI score, which suggests a reduction in the child’s level of psychological needs. SD = Standard deviation.
Six one-way ranked ANCOVAs investigating the effect of foster placement type on change in scores between first and successive BERRI, controlling for age, change in number of life events and rater.
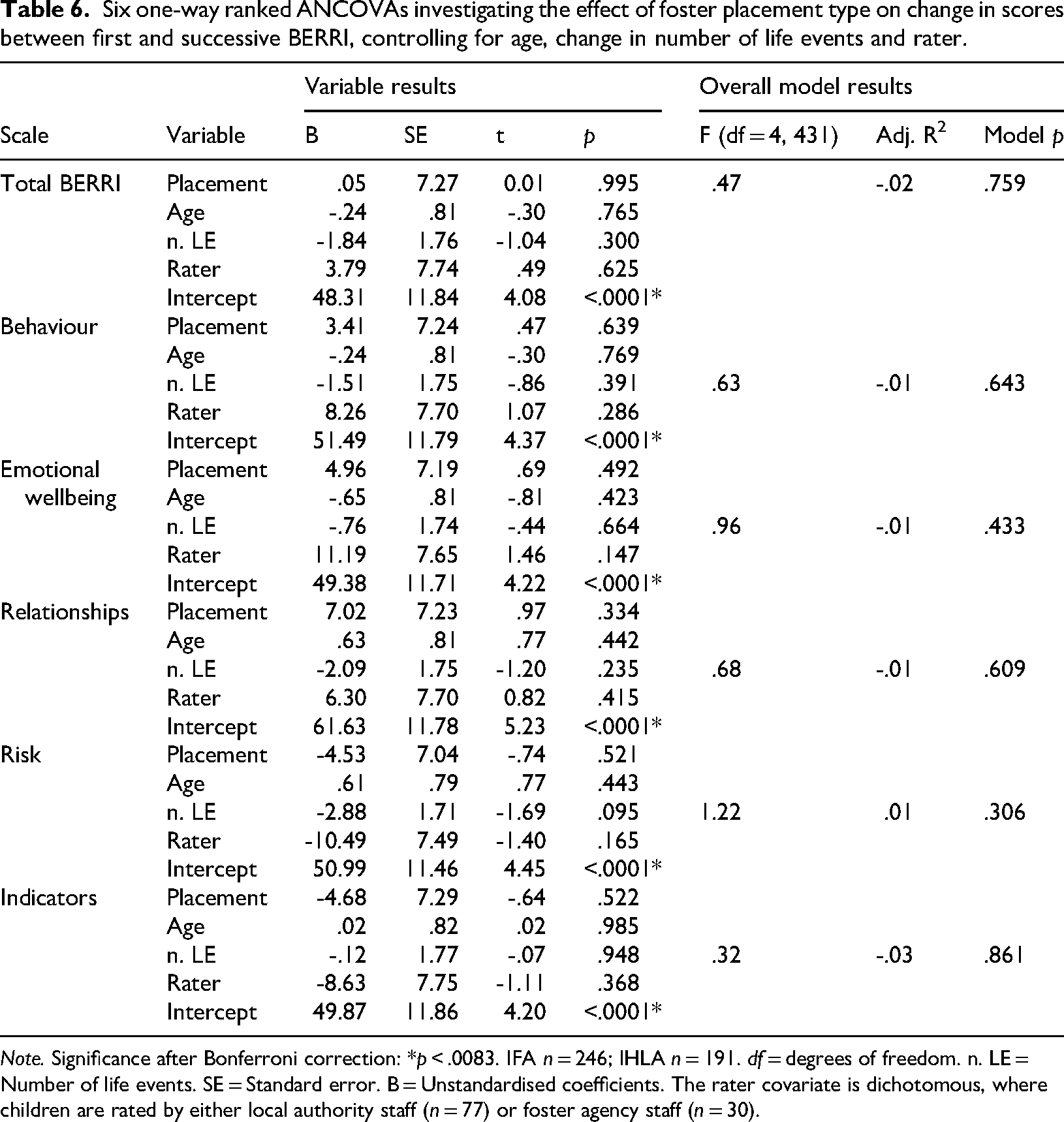
Note. Significance after Bonferroni correction: *p < .0083. IFA n = 246; IHLA n = 191. df = degrees of freedom. n. LE = Number of life events. SE = Standard error. B = Unstandardised coefficients. The rater covariate is dichotomous, where children are rated by either local authority staff (n = 77) or foster agency staff (n = 30).
The series of six one-way ranked ANCOVA analyses (Table 6) revealed that no ANCOVA model showed significance overall (p > .0083). Model fit across all ANCOVAs was poor, where adjusted R-squared values for each test were near or below zero, ranging from -.03 to .01. This indicates that the variables included in the models (i.e., placement type, age, rater and number of life events) explained very little about the variability in the ranked scores assessed. The F statistics for each assessment were also non-significant, confirming that the models were not able to significantly predict changes in BERRI score.
Accordingly, no statistically significant differences (p > .0083) were found between children in IFA placements and those in IHLA fostering in terms of their change in total BERRI scores or in the subscale scores (‘Behaviour’, ‘Emotional wellbeing’, ‘Relationships’, ‘Risk’ and ‘Indicators’), after accounting for the effects of age, life event experiences and rater on scoring. Similarly, none of the covariates showed significant associations with change in score values for each subscale. These results suggest that neither placement type nor the selected covariates significantly affect how children’s wellbeing may change across the BERRI scales over the measured time period.
These results were complemented by findings from ranked ANCOVAs comparing T1 and T2 scores across the whole sample, regardless of placement type, with age, rater and life events as covariates. The models within these analyses explained a modest proportion of scoring variance (adjusted R² = 0.12-0.17). As with the placement-specific analyses (Table 6), no significant differences were found between time points for total BERRI score or any subscale scores (p > 0.0083). However, age, rater and life event count were found to be significant predictors of scores at individual time points. Together, this indicates that individual characteristics and experiences only contribute to score variability at the distinct assessment time point, but not to the amount of change in score observed.
Discussion
This research investigated the differences in characteristics and presenting psychological needs of children and young people in IFA and IHLA foster placements. Data were drawn from the online BERRI questionnaire, completed by carers/professionals about children in their care. Cross-sectional data were collected for both placement types, with IFA data including two types of raters (BERRIs completed by IFA staff or local authority staff). Additionally, use of some longitudinal data facilitated the analysis of psychological stability and change in psychological needs within and between placement types.
Preliminary analyses revealed that IFAs tended to care for a significantly older group of children, with a greater proportion aged nine to 16 years old compared to IHLAs. This characteristic may reflect policies or referral pathways that lead to older, and thus generally young people with more complex needs, being placed in IFAs when IHLA placements are unavailable (Baginsky et al., 2017). There were no notable differences in gender distributions and number of recent life events by children in the two placement types. To better investigate the effect of these characteristics within foster care populations, the study explored the consequences of age, gender and recent life events on psychological needs, as measured by the BERRI questionnaire. While gender showed no effect, older children consistently scored higher on total BERRI and ‘Emotional wellbeing’, ‘Relationships’ and ‘Risk’ subscales, aligning with research suggesting that cumulative/age-related exposure to adversity increases psychological and attachment challenges amongst children in care (Bazalgette et al., 2015; Hillman et al., 2020; Liming et al., 2021). This current study thus reinforces the rather mixed picture of the relationship between age, children’s mental health difficulties and the complexity of their care needs. Conversely, no age-related variations were found in the ‘Behaviour’ and ‘Indicators’ subscales in the preliminary analysis, which could suggest these factors are less weighted by age. It is relatively unsurprising that age shows no relationship with scores on the ‘Indicators’ subscale, which assesses neuropsychological and psychiatric traits (e.g., autism and other neurodivergences), where prior findings show that these traits tend to remain stable over time, particularly when they are severe (Gotham et al., 2012; Szatmari et al., 2015; Venker et al., 2014). The lack of relationship between age and behavioural difficulties shown in the preliminary analysis is also in line with existing research (e.g., West et al., 2023). One possible explanation is that different types of behavioural difficulties may emerge at different developmental stages (Lahey et al., 2000), although West and colleagues (2023) also highlight that all children in care, regardless of age, have faced a kind of adversity which is likely to affect behaviour in some form. Additionally, experiencing more adverse life events in the three months preceding the child’s assessment was associated with greater psychological difficulty overall, across all BERRI subscales. As would be expected, stressful life events can destabilise young people’s mental health, though different theoretical explanations might be applicable in understanding this relationship; the diathesis-stress model of psychopathology suggests that stressors make individuals inherently vulnerable to developing psychopathology (Broerman, 2017).
Rater variability within the IFA sample further influenced BERRI outcomes, where children placed in IFAs who were rated by IFA staff scored higher in ‘Behaviour’, ‘Relationships’, ‘Risk’, ‘Indicators’ and total BERRI than children placed in IFAs who were rated by local authority staff. This discrepancy may reflect the agency staff’s closer proximity and familiarity with the children (Seifer et al., 2004), which may be influenced by reportedly lower caseloads of IFA social workers (Narey and Owers, 2018).
The study’s first hypothesis examined the effect of foster placement type on psychological wellbeing (as rated in the child’s initial BERRI) while controlling for the effects of age, number of life events and rater variability. Children in IFA placements scored significantly higher on total BERRI and four of the five subscales (‘Behaviour', ‘Emotional wellbeing', ‘Relationships' and ‘Indicators') compared to those in IHLA placements. Elevated ‘Behaviour’ subscale scores suggest IFA children display more externalising behaviours, such as impulsivity and opposition, than IHLA children, which may also reflect unmet psychological needs (Nikstat and Riemann, 2020). The ‘Emotional wellbeing’ subscale implies that IFA children likely struggle more with internalising behaviours, such as low mood, self-criticism and extreme emotional responses. Additionally, higher ‘Relationships’ scores reflect greater challenges with attachments and interpersonal connections, and elevated ‘Indicators’ scores reflect potential neurodivergence, developmental delay or more organic/genetic risk factors (Sonnet Advisory and Impact, 2022). These results support existing literature indicating that children entering IFAs present with generally more complex needs than those in IHLA placements (Narey and Owers, 2018), with our findings suggesting that the older age group supported by IFAs may explain some of this difference. Interestingly, the ‘Risk’ subscale showed no significant differences between the IFA and IHLA samples. With respect to the prior findings, this could suggest that IFAs implement measures amongst children with more complex needs that can manage risky behaviours to a level comparable to the IHLA group, reinforcing the importance of having well-supported and skilful staff within the foster placement. These findings are supported by research suggesting a link between age, adversity, mental health and risk (Bazalgette et al., 2015; Engler et al., 2022) and this study’s evidence of interconnection between all subscale scorings, where each BERRI subscale plays a complementary role in mental health. However, the results may alternatively raise questions about the limits of behaviour and risk management within foster placements overall. It is possible that foster care often accommodates these characteristics up to a certain level, where alternative placement types, such as residential care settings that typically offer higher staff-to-child ratios and more specialised resources, may be better equipped to support more complex behaviours (Hart et al., 2015; Li et al., 2017). This underscores the importance of matching placement type to the child’s individual needs.
Elaborating on this, the second hypothesis sought to examine how change in psychological needs (measured by change in BERRI scores) appeared between foster placement types over a short-term period. In line with this, a minimum three-month window was selected as a meaningful minimum timeframe to capture indications of psychological stability within a placement, resulting in an average four-month window where change was observed. This period allowed focus on the steadiness and functional quality of each placement type in supporting a child’s mental health, without being conflated with longer-term effects. A three-month interval has been considered an appropriate and evidence-based timeframe for assessing trends in change and stability in psychological wellbeing, empirically supported by numerous studies (e.g., Cole and Maxwell, 2003). Further studies on similar measures of emotional and behavioural functioning have also adopted this time period on the Child Behaviour Checklist (CBCL; Achenbach, 1999) (e.g., Piper et al., 2014) and the SDQ (Stone et al., 2010). No statistically significant differences in change of BERRI total and subscale scores were observed between IFA and IHLA placements, although both placement types saw a slight reduction in BERRI score across the majority of BERRI subscales during this period, suggesting stability with a trend towards a steady or improved psychological wellbeing. As children with a more severe profile of psychological needs are more vulnerable to stressors that could worsen their mental wellbeing (Bazalgette et al., 2015), similar levels of stability across placement types could suggest that IFAs provide more robust support models that buffer against these influences, but this claim warrants further investigation. On the other hand, the short period addressed in this study means that long-term changes are not fully represented. Bowlby (1969) proposed that children develop an internal working model (IWM) at a young age which acts as a framework for how they interpret the world and those around them. This IWM framework is heavily shaped by a child’s early attachment relationships. For children in care, IWMs are often disrupted, negative or inconsistent due to early trauma, neglect or instability (Bowlby, 1969), resulting in progress and change being quite slow for this population.
The current study highlights the discrete characteristics of children in IFAs, which may be partially influenced by the foster placement pipeline (Baginsky et al., 2017). Despite this, it seems that IFA placements are capable of providing support and stability to children with higher levels of psychological needs. Although higher BERRI scores could alternatively indicate that IFAs are less successful in supporting the needs of their children, especially with local authorities considering IFAs as a fall-back (Competition and Markets Authority, 2022), the results indicated that IHLA placements and IFAs were similar in terms of stability, suggesting that the higher scores in IFAs reflect a higher level of need at placement rather than the absence of progress over time. This is supported by a 2018 UK government review of foster care systems, which affirmed that most IFA placements support larger proportions of children with greater/more complex needs at an Ofsted good or outstanding standard, with few differences in the quality of care provided by IFA and IHLA placements (Narey and Owers, 2018). Furthermore, this quality is likely not due to the number of carers present in the home, as a similar proportion of households containing two carers was found amongst IFAs (71%) and IHLAs (69%) (Ofsted, 2022). Our findings partly echo previous research showing that SDQ scores were greater (indicating more psychological difficulty) amongst children in IFAs compared to those in IHLAs (Narey and Owers, 2018), reinforcing ideas that IFA carers require greater skill and more robust support systems to manage the needs of children in their care.
Implications
Placement decisions are currently informed more by supply and demand than by the specific needs of the child (Baginsky et al., 2017). The current research highlights that IFA placements serve a distinct function, with the ability to achieve similar levels of psychological stability to IHLA placements despite caring for children with higher levels of psychological needs. These findings advocate for IFAs to be considered equally alongside IHLA care based on the child’s specific needs, rather than as a fallback option when IHLA placements are unavailable, given the consistent evidence associating multiple placement breakdowns with negative outcomes for children in care (e.g., Eltink et al., 2025). Despite this, it should be acknowledged that differences in foster placement costs raise considerations for policy and commissioning. The Competition and Markets Authority (2022) reported a 40% cost variation between IFA and IHLA placements, with IHLA being 26% cheaper in operating costs between 2016 and 2020. However, Rome (2016) has highlighted that such comparisons are ‘often materially flawed’. Local authority cost calculations frequently exclude overhead expenses, such as for infrastructure and corporate services. As shown by this study, IFAs also support an older cohort of children with more complex needs, making cost averages misleading as these children might require a greater level of specialised care and have needs that are more costly to support (Children’s Commissioner, 2019; Rome, 2016). Thus, if IFAs are better placed to accommodate children with more complex needs, higher costs may reflect necessary investment to achieve stability and effective care. Resource allocation should therefore be guided primarily by the quality and suitability of different placement types, aligning with the best interests of the child.
The BERRI assessment has been an effective tool utilised by local authorities in placement planning decisions to help assess a child’s suitability for various placement types – as stated by the Competition and Markets Authority report (2022): BERRI has been used to review local authorities’ most complex children and identify changes that improved the outcomes for children and save money that could be used to meet children’s needs more effectively. More systematic assessment of needs would in turn support a more granular understanding of what care needs are being met by different care settings.
The current findings have their own important implications for children’s social care with insights into the differences in the populations of those in IFAs and IHLAs in terms of characteristics, needs and complexity of mental health. Firstly, the study suggests the value of context and understanding past and recent stressors which can contribute to children’s mental health presentations. Support and interventions offered by social workers and foster carers to children should be considered with these events in mind. Moreover, social care professionals must offer early intervention tailored to the specific needs of each child in their care. As previous research has demonstrated, older children and those with more complex mental health problems appear to be in IFAs as opposed to local authority settings. This challenges the tendency to group different fostering systems together in research and policy as if they are equivalent (e.g., Hiller et al., 2020; NICE, 2021), rather than treating them as distinct systems addressing different ages, experiences and needs. The present study highlights that it might be beneficial to examine how these different models of providing foster care may serve populations that are both overlapping and different.
Limitations
Despite incorporating some key covariates within the analysis, these were somewhat limited due to the type of data collected by the BERRI. This affected the present study’s ability to examine scoring differences, changes and influences in further detail. The BERRI life events measure is a useful way of capturing recent stressors in a child’s life but remains an unvalidated element of the tool. Currently, the schedule records the number of potentially stressful experiences, but there is no published evidence or research substantiating the implications of these events in relation to BERRI scores. Moreover, the present study had insufficient data on relative costs of each placement type to be able to examine the relationship between placement type, cost of placement and differences in psychological needs, which would help to address conflicting claims on this matter. The present study also lacked long-term data that would better address progress, as well as sufficient data on factors like the age that the child was placed and their number of prior placements. These factors may offer a clearer window into a child’s mental health than current age alone, as earlier entry into care and greater placement stability have been associated with better psychological wellbeing and outcomes (Maguire et al., 2024; Wade, 2024).
Through the BERRI assessments, an understanding could be developed of not only the issues children face, but also those that carers may find most distressing. Despite the advantages to obtaining the carers’ perspectives, this can also lead to study limitations as BERRI scores may face some influence from bias in those who completed the assessment. While inter-rater reliability for BERRI is not known in foster care, it has been found to vary in residential care (Harris, 2019). The present study attempted to control for these biases by including rater as a control variable; however as the rater analysis could not be applied to children in IHLA care, where all data was provided by local authority staff, this puts into question its strength as a covariate during placement comparisons. Additionally, the variability in scores may have been influenced by differences in carers’ proximity and exposure to the child compared to social workers, aligning with literature suggesting that closeness, understanding of context and professional roles influence assessments, with closer relationships often amplifying perceived difficulties (Seifer et al., 2004). This study also lacks data directly from the child regarding their own psychological wellbeing and care experiences, which would have been particularly beneficial to gain a more rounded view of their needs and experiences of their placement type.
Despite the reasonable sample size used, the use of many analyses within the present study can increase the potential for statistical error, although Bonferroni corrections were applied to manage this risk. Additionally, the sample analysed excluded the small number of children recorded as a non-binary gender due to the impact this would have on statistical validity and the ability to make meaningful comparisons between genders. However, this decision means that the sample was not representative of children across all gender identities.
Recommendations for future research
A multi-informant study, including children’s self-report, foster carer, social worker and potentially clinician reports, could help in understanding and developing the present findings and provide a more comprehensive view of the differences between IFA and IHLA foster care. There is evidence that children’s own self-reports can provide a more reliable window into their mental health (e.g., Goodman et al., 2003). For this reason, BERRI developed a ‘Voice of the Young Person’ tool which directly captures the thoughts and feelings the young person has about their needs and care, which could be valuable in future comparisons. Investigation into other factors, such as age when placed in care and the number and type of prior placements experienced by the child, would also enhance the findings of this study. Moreover, expanding comparisons to include BERRI data from supported accommodation and residential populations would further clarify differences in characteristics and psychological needs across placement types, particularly with the increase in private sector, for-profit residential care within the UK and the noted controversies around this (Sen et al., 2024). Altogether, this could support more informed placement decisions and enable care to be better shaped to meet the individual needs of each child, rather than encouraging children to adapt to existing placement models, thereby reducing the likelihood of multiple placement breakdowns.
A larger replication of the present study and further validation of BERRI using an equivalent measure of psychopathology, such as the SDQ (Goodman, 1997) or CBCL (Achenbach, 1999), would help address the reliability and validity of the findings, given the number of analyses increase the potential for statistical error. Additionally, a recent paper (Viziteu et al., 2024) has identified a new eight-factor solution for BERRI, which is possibly more statistically robust and might provide more nuanced and meaningful findings than using the five subscales. The second hypothesis, albeit on a reduced sample, explored the stability of psychological needs between two time points over a period of approximately four months. However, a larger sample with more than two time points over a longer time period would offer a deeper understanding into longer-term outcomes for children in different foster placement types.
Attention should be paid to the key finding that older children and those with more complex mental health needs are more likely to be in IFAs as opposed to IHLAs. Research should explore if these children have had more prior placement changes or prolonged exposure to maltreatment and whether this reflects the positioning of IFA care as a fallback option when IHLA placements are unavailable or cannot meet the child’s needs. It is important to explore the reasons for this apparent difference, which go beyond the scope of the current study. Further qualitative and experiential research is needed to understand why disparities might have been observed between IFAs and IHLAs, and the possibility of this relating in part to caregiver characteristics.
Conclusion
This study is the first to provide evidence using the BERRI questionnaire to investigate children’s mental health difficulties across both IFA and IHLA foster placements. The differences reported amongst the BERRI scales demonstrate the importance of assessing the different facets of psychological needs that are commonly known to be experienced by those in care.
To facilitate recovery from trauma and optimise long-term outcomes, it is crucial to provide children with higher levels of needs with enough wrap-around support to thrive in family-based placements. This study shows that IFAs appear to offer placements where foster carers are better supported to care for more complex children, compared to those within the direct provision of local authorities. Despite their higher levels of need, children in IFA placements showed levels of stability and early indications of progress comparable to the younger and less complex children in IHLA foster care. This suggests that IFAs allow a broader range of children to benefit from reparative attachment relationships; however, this needs to be investigated in greater detail.
Further research needs to be undertaken regarding the differences in outcomes for those within IFAs compared to IHLA foster placements in the UK, particularly with regard to the level and quality of support offered to the child in each placement model. To improve outcomes for children in care, it is essential to improve the basis of knowledge surrounding how these distinct systems operate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nationwide Association of Fostering Providers (NAFP). The NAFP provided funding for the initial analysis but had no input into the methodological/analytical approach, interpretation of results or writing of the article.