
Abstract
This article addresses what could contribute to sustainable care in a child welfare context, drawing on a qualitative case study of a Norwegian long-term care arrangement that combines residential care and specialised foster care. The analysis illuminates how a variety of activities contribute to flexible and reliable shared care systems that enable carers to cope with demanding care in daily life and over time. The concept of a ‘community of care’ is suggested to comprehend the various features that interconnect and contribute to sustainable care. This concept aims to transcend individualised and decontextualised conceptions of care and dichotomised categorisations, like residential care and foster care. A ‘community of care’ is relevant for research addressing how to ensure sustainability in child welfare and as a thinking tool for practitioners.
Plain language summary
Children in need of alternative care have experienced various insufficient care conditions, and the care they receive is of significant importance. While safe and stable care environments are a primary objective for child welfare authorities, many children undergo multiple moves while in care, leaving them with stressful childhoods. Drawing on a qualitative case study of a Norwegian long-term care arrangement that combines residential care and specialised foster care, this article examines what could contribute to sustainable care. Although residential and foster care have been extensively studied, less is known about what opportunities a combination of these two care strategies may hold.
Sustainability refers to the process and qualities by which a care arrangement can endure and be maintained over time. This article explores the perspectives of foster carers, professionals and parents. While shedding light on the range of challenges in providing care, their stories also provide insight into how various activities within this care arrangement foster the sharing of care tasks and emotional burdens, facilitate peer support and collective learning, and promote unified responsibility for the organising of care and the child's wellbeing. This study can inspire reflection and the development of various combined care strategies to endorse sustainability, also encouraged by the suggested concept of a ‘community of care’.
Introduction
When children need alternative care, foster care and residential care constitute the primary public care strategies. Internationally, foster care is preferred, with residential coming in second (Holmes et al., 2018; Konijn et al., 2019). In Norway, the preference for foster care was reinforced by a child welfare reform in 2004, leading to the closure of nearly all residential facilities for children under 13 years old. Specialised foster care – where the foster carer is temporarily compensated and serves as a full-time carer, receiving training, supervision and respite care – has widely replaced residential care (Backe-Hansen and Bakketeig, 2011). Similar trends, particularly for younger children, can be seen in several Western countries (Holmes et al., 2018; Thoburn, 2016).
Many children experience multiple moves, whether in foster care or residential care (Egelund, 2006; Leathers et al., 2019; Oosterman et al., 2007; Sallnäs et al., 2004). Longitudinal studies in Scandinavia indicate that 20–50% of foster care placements end prematurely (Christiansen et al., 2010; Vinnerljung et al., 2017), aligning with the findings of meta-analyses (Konijn et al., 2019; Oosterman et al., 2007). Repeated moves undermine quality care and the child welfare system’s objective, leaving many children with stressful childhoods, potentially increasing their marginalised position in society (Backe-Hansen et al., 2014; McGuire et al., 2018). Pursuing greater stability in children’s care environments is an international concern.
Numerous studies have addressed what contributes to stability and disruption in care (Ahn et al., 2017; Geiger et al., 2013; Gouveia et al., 2021; Hanlon et al., 2021; Harkin and Houston, 2016; Konijn et al., 2019; Leathers et al., 2019; Schofield et al., 2012; Thoburn, 2016). Although several challenges have been emphasised, including a lack of support, relief, training, stress and more, children’s emotional and behavioural problems are highlighted as a main factor in causing instability (Holmes et al., 2018; Konijn et al., 2019; Oosterman et al., 2007). However, focusing primarily on the child could lead to individualising problems, limiting the understanding of complex phenomena, such as care, stability and disruptions (Colton and Roberts 2007; Jakobsen 2013; McGuire et al., 2018; Olsson et al., 2012). Considerations should also be given to the organisation and quality of care.
Over the years, various placement options, including residential facilities and holistic care models, have been proposed to enhance placement stability (Barber et al., 2001; Christiansen et al., 2010; Norges offentlige utredninger [NOU], 2023: 24). However, the literature remains limited. Research here has typically focused on either foster care or residential care. The present article explores a Norwegian long-term care arrangement combining residential and specialised foster care for children, and the opportunities this organisation of care may have for meeting some of the sustainability challenges in organising care for children with complex backgrounds. To the best of our knowledge, only a few studies have examined a combination of these two care arrangements (Arieli and Feuerstein, 1987). We ask the following question: Which traits of a care arrangement combining residential and foster care may contribute to sustainable care?
Here, sustainability refers to the process, qualities and characteristics by which a care arrangement can endure and be maintained over time. This concept is chosen for its emphasis on dynamic and processual aspects, which differ from the more static notions, such as stability and permanence, which are widely used in literature. What makes caring endurable is a complex matter (Geiger et al., 2013; Hanlon et al., 2021). Nevertheless, several studies either take a descriptive approach or draw on developmental psychologies focusing on individual children’s needs and their primary carers (Lassemo et al., 2022; Neagu, 2021; Ulvik, 2009). In line with Ulvik (2009), we argue that there is a need for wider theoretical analysis and concepts grasping the complexities of care to prevent the individualisation of problems and enhance professional understanding and existing practices. Our aim is to contribute both empirical and theoretical insights to broaden the understanding of sustainability within public care.
By drawing on sociocultural theory (Rogoff, 2003), we explore the perspectives of several groups of carers, including foster carers, residential carers, parents, foster care consultants and managers. The concepts of shared care (Singer, 1993) and community of practice (Lave and Wenger, 1991; Wenger, 1998) are applied, and we suggest the concept of a ‘community of care’, inspired by Lave and Wenger, to elucidate the various interconnected features contributing to sustainable care.
Concepts of care and theoretical outline
According to sociocultural theory, care is a social and cultural practice aimed at ensuring children’s survival and acquisition of mature ways of living (Rogoff, 2003); the organisation of care should be seen as a continuous interaction and understood in light of the conditions caregivers and children face in their everyday lives and the cultural practices, regulations and structures they engage in and negotiate meaning through within a given society (Kousholt, 2011; Rogoff, 2003). Because of diverse sociocultural contexts, there is variability in how care is arranged and understood (Rogoff, 2003: 116). Public care arrangements, which represent exceptional institutionalised care organisations (Ulvik, 2018), evolve within the broader societal context, encompassing cultural ideals, norms and structures related to childhood and care. Understanding sustainable care traits in child welfare arrangements requires considering this comprehensive context and the interplay between the exceptional and the ordinary.
The concepts of ‘shared care’ and a ‘chain of care’ – core concepts for analysing the empirical variation of care arrangements for children today (Andenæs and Haavind, 2018: 1483) – are rarely utilised in child welfare research (Kesselring et al., 2016) but are relevant in our analysis. The idea of ‘shared care’ (Singer, 1993) emerged in the 1990s in opposition to universal developmental theories positioning one maternal caregiver as the standard of quality care. Shared care emphasises that children grow up within several contexts (kindergarten, school, etc.) and that several caregivers share an engagement with the child, supplement each other and contribute to the child’s developmental wellbeing (Andenæs and Haavind, 2018; Singer, 1993). The concept of a ‘chain of care’ (Andenæs, 2011; Gullestad, 1979) emphasises how, through various shared care practices, caregivers construct links or interconnected environments of care (Andenæs, 2011). Linking care to care chains entails coordinating and enabling adults to combine their care efforts. The family serves as the primary care context in our society, and parental responsibility, as outlined by Andenæs and Haavind (2018), involves maintaining an overview and ensuring the adequacy of each link and the entire care chain. The term ‘caring from a distance’ emphasises the continuous aspects of care, even when the child is in different locations and under the care of someone else (Andenæs, 2011).
Some authors further develop these concepts, pointing to how contradictions, conflicts and problems are part of care arrangements, despite shared overarching goals (Højholt, 2015; Kousholt, 2011). Emphasising the contradictory nature of care organisations helps explore challenges beyond individualised explanations, examining how they are addressed and interconnected across contexts, organisational structures and broader systems of meaning (Højholt and Kousholt, 2020).
We used the concepts outlined above to facilitate contextual analysis of the organisation of care within a complex care arrangement combining residential and foster care and to elucidate how various sharing care practices shape conditions and become significant for carers. To explore the collective and organisational aspects of care, we have adapted the concept of a ‘community of practice’ (Lave and Wenger, 1991; Wenger, 1998), which provides insights into how people who collaboratively engage in shared practices within a common domain foster collective learning and bonds among participants – a community. Through sustained mutual engagement, participants can expand their knowledge and skills, develop a shared repertoire of ways of doing things, acquire vocabulary to articulate their experiences and contribute to a collective knowledge base, fostering cohesiveness and intentionality beyond the interpersonal dynamics of informal networks (Wenger, 1998; Wenger et al., 2002). The term ‘community’ does not imply either harmony or discord but rather serves as a focal point for analysis, enabling exploration of the opportunities, challenges and significance a community of practice brings to its members and the circumstances that sustain or erode them (Wenger, 1998).
Research on public care
The literature highlights various factors influencing retention and disruption in foster care. While some studies indicate the individual characteristics of foster carers, such as demographic factors, child-rearing skills, unrealistic expectations and more (Ahn et al., 2017; Crum, 2010), others note the significance of the quality of relationships with parents and child welfare professionals, training, supervision and so on (Beek and Schofield, 2017; Chateauneuf et al., 2018; Konijn et al., 2019; Taylor and McQuillan, 2014; Vinnerljung et al., 2017). Overall, support for foster carers is crucial for their satisfaction as foster carers and decision to continue fostering (Ahn et al., 2017; Geiger et al., 2013), emphasising the importance of foster carers’ networks, teamwork, respect, emotional support and shared commitment with social workers (Ahn et al., 2017; Gowan et al., 2023; Hanlon et al., 2021; Luke and Sebba, 2013; Schofield et al., 2012). Respite care is vital for the welfare and retention of foster carers (Geiger et al., 2013; Gowan et al., 2023). Yet ongoing debates in Norway question the impact of respite care on children’s attachment to foster parents and their sense of belonging to the foster home, calling for research on its effects (NOU, 2018: 18).
Within residential care, the potential of short-term residential care to strengthen retention, by providing children with relational support and aiding in transitions to foster care, is emphasised (MacDonald and Gillespie, 2023). However, turnover among residential care staff undermines children’s stability (Grünfeld et al., 2020; Pinheiro et al., 2022), highlighting the critical role of carers in shaping children’s conditions. Turnover is attributed to emotional exhaustion, heavy workloads, low salaries and low status (Colton and Roberts, 2007), with overload, stress, burnout and compassion fatigue being increasingly recognised as issues (Audin et al., 2018; Seti, 2008).
Although sparse, the literature on combined care strategies provides valuable insights into how organisational features impact carers’ conditions and retention. Arieli and Feuerstein (1987) examined a combination of residential and foster care in Israel, revealing that this reduced foster carers’ feelings of inadequacy and loneliness in managing children’s difficulties and prevented burnout and high turnover among residential staff. The children lived with their foster carers but spent significant daytime hours in the residential facility, which was responsible for education, leisure activities, family visits and counselling.
Another notable example is the Mockingbird Care Model, originally developed in the USA and adopted in the UK, Australia and other countries (Grossman and McKenna, 2007; McDermid et al., 2016; McLaren et al., 2023). Designed to emulate an extended family network, the model organises foster households into clusters of six to 10, supported by a hub home providing various services, including respite care, training and peer support. Evaluation reports have emphasised the significance of non-judgemental peer support, easy access to well-acquainted respite carers and immediate support (Grossman and McKenna, 2007; McDermid et al., 2016; Ott et al., 2020), while a recent study by McLaren and colleagues (2023) also highlights the significance of shared responsibility among carers. Further research is needed to enhance our understanding of the interconnectedness of features that make care sustainable.
The research setting
The ‘Bluehill’ care arrangement is a multifaceted long-term care arrangement combining residential care and specialised foster care for children aged two to 18 in Norway. Bluehill encompasses two residential homes for children aged two to 12, individual residential units, specialised foster homes, a unit of foster care consultants and various group activities for children and carers and former residents. Most children in Bluehill have undergone multiple moves and were initially placed in care because of various insufficient care conditions. They need specialised residential care (for one to two years) before moving to a Bluehill foster home or another care arrangement. Foster care consultants recruit foster families, organise transitions into foster care, group activities and respite care. These activities take place at Bluehill residential facilities, which remain integral to the children and carers after the child moves into foster care. The residential facility offers 24-hour support in case of challenges or crises in the foster homes, and the children can temporarily return to the residential facility, if needed. Bluehill is a non-profit care organisation undertaking assignments from child welfare authorities.
Method
This is an exploratory qualitative case study of a care arrangement combining residential and foster care. Bluehill was chosen because of its unique combination of residential care for children under 13 years old and specialised foster care. To explore this care arrangement and address the research question, a multi-method approach (Mik-Meyer, 2021; Silverman, 2020) was employed, encompassing individual, paired and group interviews with carers of different positions, participatory observation and reading institutional documents. The larger project also included interviews with children and young people. Their perspectives are presented elsewhere (Negård et al., 2020). Data collection was conducted by the first author from 2017 to 2018.
Participant recruitment
Participants occupying various positions, including residential staff, foster care consultants, managers, foster carers and parents, were selected to ensure a broad range of perspectives. The interviews included 42 carers, as specified in Table 1.
Participant information.
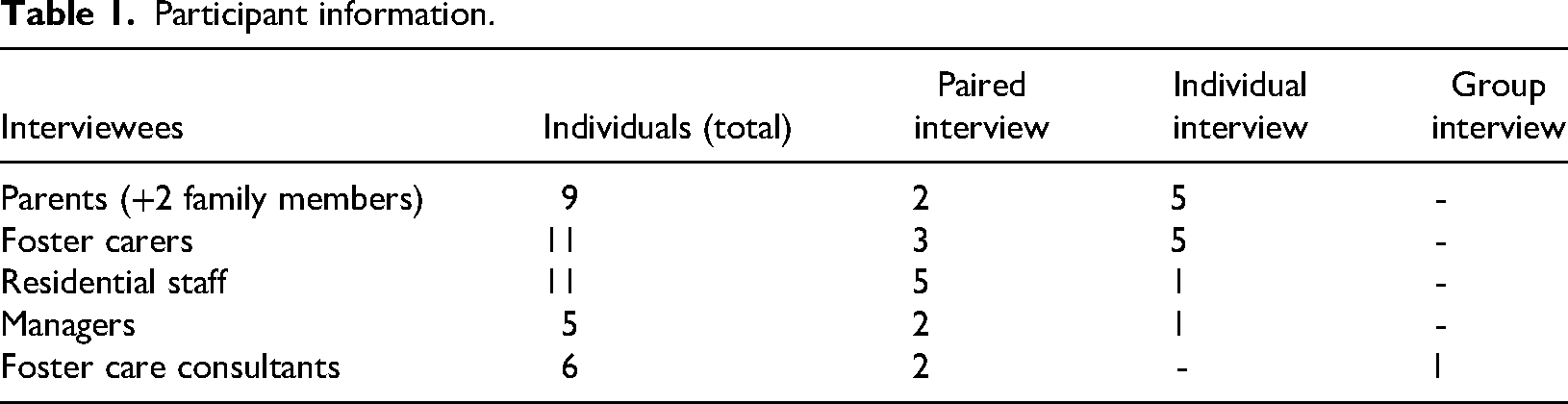
The broad use of the term ‘carers’ underscores that all participants contribute to the organisation of care, despite variations in tasks and closeness to the child.
Interviews and observations
The interviews explored carers’ perspectives on organising care in daily life and over time using a combination of a life-mode-inspired approach (Haavind, 1987) and a semi-structured thematic interview approach (Kvale and Brinkmann, 2015). Life-mode interviews are flexible and structured around the temporal, spatial and cyclic aspects of everyday life. The interviewees’ descriptions of situations and sequences of events are the focus (Haavind, 2020), allowing for exploration of a variety of activities, relationships, interactions, dilemmas, reasoning and areas/themes of interest adjusted to the carers’ positions. Paired and group interviews involved interviewing two or more participants together, facilitating interactions and joint reflection (Greenbaum, 1998; Wilson et al., 2016). Carers from the same category and household were paired. The interviews were conducted in various settings based on the interviewees’ preferences, including their homes, Bluehill facilities and designated public venues. The interviews lasted from one to two-and-a-half hours. All interviews were audio-recorded, transcribed verbatim and anonymised. The quotes were translated into English.
Observations aimed at gaining insights into the care arrangement served as a supplementary source of information alongside enterprise documents. Observations were conducted where access was feasible, including training sessions and social gatherings for residential and foster carers and regular meetings for training planning. The topics and questions arising from observations were further explored in the interviews. The observation sessions lasted between one to six hours, depending on the events. Keywords were noted during the observations and elaborated on afterwards.
Ethical considerations
Ethical approval was obtained from the Norwegian Centre for Research Data (now SIKT) (Project ID: 323437). Various forms of written consent were obtained. Some parents consented to interviews with their child’s substitute carers, while some youths aged 16 and over consented to interviews with their foster and residential carers. Some carers, including managers, foster care consultants, residential carers and foster carers, were interviewed with their consent only, in accordance with confidentiality regulations. Bluehill’s directors consented to the study. Formal conditions, including voluntariness, the right to withdraw at any time and the guarantee of confidentiality, were restated multiple times to all participants. Most carers looked forward to the interviews, and all reported that they found the interview to be a positive experience afterwards. To maintain anonymity, the participants are referred to by their positions or pseudonyms.
Analyses
During the observations and interviews, an understanding of a community-oriented care organisation emerged. Despite challenges, carers across various positions seemed content with being part of Bluehill. These initial impressions informed the analysis of the interview transcripts, which followed an interpretative analytical approach, inspired by Haavind (2000) and Kousholt and colleagues (2018). The analysis began with a broad search within each interview, seeking patterns, internal coherence, contradictions and meaningful themes in carers’ descriptions of organising care. These vertical readings were followed by a horizontal analysis across interviews within each participant group, looking for commonalities, differences and nuances in the emerging themes of interest. As the analysis progressed, it provided a deeper understanding of the range of complexities and dilemmas involved. By exploring these challenging aspects further, the significance of the activities emerged. Expanding the analysis across different groups of carers added further understanding to activities and interconnectedness. The observations provided details about the activities. The theoretical concepts proved fruitful for exploring how care became endurable and how the care arrangement led to not being alone in dealing with demanding care. To elucidate the multiple and interconnected features contributing to sustainable care, the concept of a ‘community of care’ was constructed, pointing to the collective responsibility for providing care.
Results
Many residential carers, consultants and managers had been with Bluehill for years, and some foster carers had provided care for several children within Bluehill. They all emphasised the necessity of reliable support systems to deal with the complexities and unpredictability inherent in providing care within a child welfare context, driven partially by previous experiences of a scarcity of support elsewhere. For some parents, Bluehill represented a turning point in their children’s lives, following previous experiences of recurrent moves. Below, we delineate what was characterised as significant by the carers to cope with and remain part of the care arrangement and which traits may contribute to sustainable care. The analytical results are presented in three widely interconnected themes to which different carers across positions contributed: (1) Sharing care experiences – mutual recognition and togetherness; (2) Legitimacy of shared care; and (3) Care chains – ‘double fuses’.
Sharing care experiences – mutual recognition and togetherness
Conducting daily care was described by almost all residential and foster carers as ‘very demanding’ and by several as beyond what they could have anticipated. Many found it difficult to articulate their experiences, often resorting to expressions such as ‘you have to feel it in your body’. Although phrases such as ‘to be in their [the children’s] nervous system’ and ‘to regulate the children with ourselves’ pointed to the relational intensity involved, the difficulties in verbalising their experiences led many to grapple with validating their care efforts and emotions, as illustrated by two residential carers in the following interview quote: Residential carer 1: How should I explain what it’s like to work here? We sort of have three others, who understand, no one else, not even Suzan, our manager, understands. RC 2: Yes, that is true. It is a bit lonely. Suzan knows a lot but not in her body. RC 1: And then you don’t attain that understanding of what it is truly about, right. That is perhaps, I think, which we quite agree upon, is the most demanding in the job – to explain what you are doing. It is difficult to explain attendance as a way to become exhausted.
Having someone who understood the ‘embodied’ and ‘invisible’ aspects of care, as some described it, was regarded as crucial by all residential and foster carers, fostering mutual recognition and a sense of togetherness, which was difficult to achieve elsewhere because of confidentiality constraints and the lack of understanding of ‘outsiders’. Foster carers described engaging in joint monthly training sessions and group supervisions, bi-weekly individual supervisions from foster care consultants (hereafter ‘consultants’) and further supervisions as needed. They also attended annual two-day seminars alongside their partners and participated in joint training sessions with Bluehill carers and other foster carers. Similarly, residential carers described engaging in joint weekly meetings, planned group supervisions and training. These opportunities to share experiences within organisational structures seemed to reinforce a sense of recognition. A residential carer said the following: What becomes more visible to me the longer I work here are all the ‘valves’ put in place for us, the adults. The numerous resources Bluehill spend taking care of us, such as conversations with the team leader, time allocated during working hours, and debriefing at our Wednesday meetings. We engage in discussions about our emotions, talk with our team partners and analyse situations and processes. I think this makes you able to stay longer and stand safely in it.
Viewed through a lens of shared care (Singer, 1993), these practices, or ‘valves’, can be seen to facilitate the sharing of emotional care burdens and dilemmas through joint interpretation, mitigating the individualisation of care and overload for the carer. Consultants and managers referred to these practices as ‘safety valves’, elaborating on how they prevented the likelihood of unprocessed feelings from manifesting in interactions with children, within foster families, among staff and across contexts. They also emphasised the valuable insights gained from participating, enabling them to provide adequate support for both children and carers and organise training adapted to their situations and needs.
All residential and foster carers described encountering situations and phenomena requiring ‘professionalism’ and collective training arrangements, often involving ‘external professionals’, ensuring a ‘shared professional platform’ and ‘common language’. But foster carers in particular stressed the importance of regularly engaging with peers in similar positions. One foster carer shared the following: I think the group guidance is very good, so I can meet the others [foster carers]. I listen to them a lot when they talk, and those who may have had foster children for many years. How some [children] have been and changed a lot from the time they arrived through puberty. I think it is very useful.
The peer activities seemed to provide valuable learning opportunities and from a peripheral participatory position as beginners. According to Wenger and colleagues (2002: 9), ‘know-how’ knowledge implies a profound understanding of complex, interdependent systems, enabling dynamic responses to context-specific problems requiring interactions and informal learning processes, such as storytelling and conversation. The foster carers emphasised that peer activities helped to enhance their understanding and approaches, identify challenging periods, recognise development and maintain future hopes, which several described as difficult ‘amid struggles’. These aspects align with Wenger’s description of communities of practice, where sharing experiences and knowledge, identifying and addressing shared challenges and exploring new possibilities help both individual members and the larger group (Wenger, 1998). The joint activities fostered relationships among carers within their groups and across positions and contexts, fortified by social activities, such as joint meals, celebrations of holidays, summer parties and so on, which we term ‘community-promoting activities’, to facilitate informal interactions. All foster carers referred to each other as ‘colleagues’, with some forming friendships. These community-promoting features also extended to the parents who described participating in social gatherings at Bluehill and parent support groups.
According to Wenger and colleagues (2002: 37), an environment conducive to learning requires openness and a safe space to speak the truth and ask difficult questions. Both residential and foster carers described how dealing with demanding care situations evoked feelings of inadequacy, leading to frustration and internal struggles. Some recounted instances where their credibility was compromised, such as when children ‘made up stories’ about them. Although sharing such experiences associated with being a ‘poor carer’ could be difficult, all emphasised the supportive climate among their peers, including managers and consultants. One foster carer made the following comments: You can share things and talk about how you feel and what concerns you, without being afraid that someone will use what you share against you. You are being understood. It becomes a community giving strength and that I feel a very strong bond with and that you are not alone.
This trust, which several foster carers also related to the consultant’s long-term involvement and knowledge about the child and foster family, unified their engagement in addressing challenges and making the care situation work, also accommodating differences in opinions and disagreements. Residential carers shared instances of dissent, attributing this to their commitment to the child’s wellbeing and valuing diverse perspectives to improve their practices and professionalism. Strong bonds, as noted by Wenger and colleagues (2002: 37), can withstand disagreement and enable community members to deepen their relationships and learning.
Legitimacy of shared care
Bluehill carers across positions deemed rest a necessity to endure the demandingness involved in providing care in this context. Residential carers had designated ‘time off’ following their rotational work schedule, while foster carers had planned ‘relief’ every third weekend and for two weeks during the summer, with additional flexibility as needed. Weekends at Bluehill were organised into age-based groups, where children spent time together, while summer respite included a summer camp for children of all ages. The consultants orchestrated these arrangements.
All foster carers valued the respite conditions and appreciated that these were planned, continuous and flexible, ensuring predictability for them, their children and the foster child(ren). Many described these arrangements as providing ‘real relief’, as illustrated by a foster carer: … what Bluehill does fantastically is that the weekends are real relief, and I call it real relief because I know that my foster child (NN) is taken care of, and Bluehill has a plan that NN is incredibly happy about every time. The residential carers are so skilled that, when there are things, they deal with them and take care of NN. They’re on all the time, so I indeed trust them to take care of NN. And then it becomes real relief for me.
This sense of ‘real relief’ was not taken for granted by either foster carers or residential carers who described themselves as being ‘available’ and on ‘standby’ in daily life as issues frequently arose in other contexts where the children participated. Some described being constantly in ‘emergency response’ mode, anticipating calls from school or others requiring their immediate attention. Several residential carers referred to these aspects of care as ‘invisible’ and noted that they seldom experienced ‘true breaks’ during the day but rather ‘breathing spaces’. Through the lens of the concept of ‘caring from a distance’ (Andenæs and Haavind, 2018) these ‘invisible’ but demanding distant aspects of care become apparent. In this context, ‘real relief’ could mean a pause from demanding daily distance caring and responsibility. As illustrated by the quotation above, ‘true breaks’ and ‘real relief’ rely on confidence that the child’s wellbeing is being maintained and that any issues are adequately addressed when the child is somewhere else and with someone else.
According to the foster carers interviewed, respite provided time to rest, pursue hobbies and nurture relationships with partners, family and friends and, most importantly, time to spend with their own children. Despite conveying an unwavering commitment to the foster child, foster carers with their own children living at home expressed concerns about how it impacted them. Several noted that the ‘extensive attention and efforts’ required to care for the foster child generated dilemmas and doubts. Although coordination of daily life, as emphasised by Kousholt (2011), entails contradictions and problem-solving in all families, the intensity involved led several foster carers to question: ‘What have I done to my family?’ Having dedicated time alone with their own children was described by some as ‘absolutely necessary’ to continue as a foster family. This underscores how respite affects the entire family system in handling relational tensions and easing foster carers’ doubts.
However, several challenges also emerged. A significant concern shared by all foster carers and many Bluehill carers reflected the professional discourse on how respite affects the foster child’s sense of belonging in the foster family. To address this, all foster carers described refraining from any extraordinary activities during respite that could make the child feel ‘outside of the family’. This illuminates how foster carers assumed responsibility for the child’s belonging and engaged in distance caring to legitimise respite care, causing their own situation to recede into the background. Additionally, several foster carers expressed challenges in legitimising respite to the child. While all foster carers described it as helpful that Bluehill decided on respite conditions and that these conditions were equal for all, the children’s appreciation of participating in the respite arrangements seemed to alleviate their concerns the most.
From a sociocultural perspective, children can experience attachment and belonging to several people and care contexts (Rogoff, 2003). This understanding was also echoed by foster carers, who emphasised the importance of the community of children and Bluehill residential carers. Some foster carers described the Bluehill community as their child’s ‘extended family’ and ‘trusted safety net’. For others, this community also represented a ‘pause’ from concerns about their foster child’s social wellbeing by giving the child an opportunity to socialise with peers and friends (see Negård et al., 2020). The children’s attachment to Bluehill made some consultants question its potential impact on their attachment to foster parents, illuminating how the prevailing discourse on attachment influences carers’ perceptions.
Bluehill carers across positions recognised that the children often needed ‘breaks’ from ‘tight family life’ too. The residential carers described themselves as being in a unique position in this regard, being ‘not too close and not too distant’, akin to a supportive relative with whom it could be easier to share and process experiences. Moreover, they emphasised the importance of continuity in relationships fostered by these practices, as portrayed by a residential carer: … the children also become part of our lives, like an extended family in a way. That feeling is there for us, too, not just for the children. There is something beautiful about that sharing. It feels like part of life to be there [respite weekends].
In the position of Bluehill carers, these long-term aspects aligned with their professional beliefs regarding quality care, emphasising enduring relationships and providing a secure and consistent environment for the children, serving a compelling reason to remain with Bluehill. They also described instances where children sought out Bluehill during difficult times in foster care, creating a sense of security for all involved.
From the consultants’ perspectives, these practices provided insights into the child’s situations and development, aiding them in providing ‘hands-on’ supervision and adjustment in support. The consultants and managers emphasised the significance of maintaining continuous respite support and predictable care conditions, and they negotiated foster carers’ terms with child welfare services. Consultants noted that this process sometimes required accentuating challenges rather than progress to justify ongoing support because discussions of reducing support often arise when ‘things go well’. Viewed through the lens of shared care, and the preceding analysis, the perception that ‘things are going well’ may indicate that the sharing care practices were well organised and accurately met the needs of several parties, underscoring the interconnected nature of caring (Kousholt, 2011).
Care chains – ‘double fuses’
The children’s care systems encompassed several people, parties, and professional support systems, including Mental Health Care for Children and Adolescents (BUP) and Educational Psychological Service (PPT) among others. The consultants played a pivotal role in linking and coordinating carers, assuming an overarching responsibility for the child’s care system, as portrayed by a consultant: We have this picture where the consultants are in the centre, surrounded by various participants and parties. The consultant then tries to coordinate everyone to pull in the same direction in the child’s best interest. This includes foster parents, biological parents, respite arrangements and families and support contacts, as well as BUP, the school, the supervisory officer and more. Moreover, consultants must report to child welfare services and hold evaluation meetings.
To make all parties ‘pull in the same direction’, the consultants described how they engaged in various ways. The carers emphasised that many children encountered difficulties in school, socially and/or academically, necessitating meetings and discussions with peers, parents and professionals. One foster carer succinctly summarised this complexity by stating: ‘Elementary school has been horrendous in that manner.’ To support both foster carers and children, the consultants described participating alongside foster carers in school meetings, conducting trauma lectures for teachers to enhance their understanding of the child’s struggles and needs, and more. These joint efforts were universally valued by the foster carers, with some describing them as necessary ‘to get their message through’ and ensuring adequate support. One foster carer expressed how: ‘Theresa’s [consultant] contribution has been amazing. She has worked hard and intensely to secure the pedagogical situation for our boy.’
During challenging periods, the consultants described having daily contact with foster families. This consistent presence, accessibility and engagement of the consultants, along with the continuity of the relationship, were underscored by all foster carers. Several noted that they felt cared for and had a sense of shared responsibility for the child’s developmental conditions and the overall wellbeing of the family system. One foster carer expressed this as follows: ‘I don’t think I could have managed this assignment without Karen [consultant]. I have used her a lot. She meant so much to us. She has been genuinely concerned for our wellbeing that we are fine at all times.’ The consultant’s involvement in linking, shaping and buffering the child’s care system – or care chains (Andenæs, 2011) – appeared to form multiple ‘double fuses’, addressing challenges, precarious relationships and difficult periods that could impede foster carer retention. This also included contact with the child’s parents and family members.
Involving parents in the care for the child was a priority for Bluehill from when the child moved into residential care, and maintaining contact with parents and family was considered vital for children to reconcile their situation. However, Bluehill carers also emphasised challenges, potentially adding to the burden on foster carers. A consultant shared the following: ‘We act as a buffer, and foster carers say they appreciate that Bluehill does so. Several express that this is one of the most important things we do as contact with parents is very challenging for many.’ This buffering involved transmitting information among carers, including parents and foster carers, supporting them around visits, organising support groups for parents and more. The consultants emphasised the importance of children knowing that their parents are okay and being taken care of to reduce stress on the child and foster family, respectively. This underscores how relationships are interconnected and mutually constituent and how parents are recognised as integral members of children’s care chains.
These sentiments were echoed by foster carers and parents alike. Some foster carers described a collaborative atmosphere, finding that the child’s interactions with parents or other family members were supportive and beneficial to the child’s wellbeing, while others expressed concerns, particularly regarding the child’s reactions and anxiety before and after visits. The importance of the consultants' support in managing these reactions was emphasised, as was ensuring that the child’s interests were addressed.
All parents expressed confidence in how Bluehill cared for their child and a desire to support their work. One parent rejected the legal and commonly used term ‘deprived care’: ‘I am concerned for my daughter every day, all year round’. This sheds light on the continuous nature of care, as described by Andenæs and Haavind (2018). However, not being part of their child’s everyday life appeared to be a challenging and peripheral care position. This could lead to insecurity during visits – as if ‘I don’t know my child anymore’, as one parent noted. While some found communication with foster carers, such as talks, letters and photos, to be helpful, several described consultants being supportive in navigating dilemmas. Parents also emphasised the opportunities to share experiences and discuss their care position during parent support groups, yet revisiting challenges could also be ‘burdensome’. All parents appreciated the occasional lectures during these meetings and the joint meals as well as social gatherings that provided a shift in focus, and they felt included and cared for. This illuminates how care remains a context-dependent social practice for parents.
From the consultants’ perspectives, fulfilling these multiple tasks and responsibilities and ‘tailoring’ support could be demanding and intense, requiring additional working hours. While they emphasised recognition from leaders and colleagues, as well as flexibility in their working hours in return, the ‘double fused’ approach apparently extended to them. They described working together in pairs and sharing tasks and responsibilities for the families – practices they described as supportive but also crucial for maintaining continuity and quality care.
Alongside the broader web of the support system, this organisation contributed to a sense of ‘robustness’, as noted by several Bluehill carers, enabling them to navigate inherent complexities and withstand difficult times, including crises. This sentiment was also echoed by foster carers: The system means that they are so close to you that they can keep up and take your pulse without feeling that they are trying to follow you at the seams. The whole system is so close, that you don’t get any surprises, one way or the other.
These features, which some consultants also described as ‘layers of care’ encompassing the child and the carers, seemed to unify their engagement in making the care situation last.
Discussion: ‘Community of care’
Given the challenges faced by children and carers because of disruption in care relationships, efforts to understand what contributes to sustainable care are crucial. We examined the traits of a care arrangement combining residential and foster care that may do so. Below, we discuss what could be learned from this case study empirically, methodologically and conceptually, and what knowledge about sustainable care can be inferred.
The present study illuminates how a range of shared care practices encounter and buffer a variety of challenging situations and dilemmas that could compromise sustainability. These practices fostered a collaborative approach, joint responsibility and community among carers, seemingly mitigating individualised conceptions of problems and care. Moreover, these shared practices facilitated opportunities for carers to develop insights and mutual support across positions and contexts, which might otherwise be constrained by institutional boundaries. These features, some of which can also be found in other combined care strategies (Arieli and Feuerstein, 1987; McLaren et al., 2023; Ott et al., 2020), formed what could be conceptualised as a ‘community of care’ embodying qualities of continuity and flexibility, combined with the elasticity to adapt to carers’ various situations. Timely and appropriate support is vital for the retention of foster carers, yet it often falls short (Konijn et al., 2019; McDermid et al., 2016). In this case, the web of support systems seemed to reach out to carers and even anticipate possible challenges preventing them from having to seek support in times of difficulty. These traits are reminiscent of the community of practice (Wenger et al., 2002), which can aid its members in obtaining help with immediate problems, saving time in searching for information and devising better solutions by incorporating the perspectives of peers, coordinating efforts and finding synergies across organisational boundaries.
Wenger (1998) argues that dealing with complex problem-solving necessitates multiple perspectives and learning together. Caring within a child welfare context expands ordinary care experiences and informal communities among parents, necessitating the facilitation of learning opportunities. The current study illuminates how providing carers with opportunities to regularly interact on situational and long-standing issues created a ‘living repository’ for insights and knowledge, creating learning loops and bonding among carers. These features nurture carers’ endurance and long-term relationships, which is a well-known challenge in public care because of staff turnover (Colton and Roberts, 2007; Geiger et al., 2013; Grünfeld et al., 2020). Certain dynamics sustain a community of practice, including participants finding meaning in what they do, developing relationships and experiencing a sense of identity and belonging (Wenger, 1998). Here, these dynamics were reinforced by what we call ‘community-promoting activities’, underscoring the vital aspects of people’s shared lives together and reinforcing that care is a fundamental social practice (Rogoff, 2003; Wenger et al., 2002).
Højholt and Kousholt (2020) emphasise that dilemmas in practice are embedded in societal systems of meaning. Our study illuminates how prevailing professional notions may constrain professionals’ and foster carers’ agency, as exemplified by respite care. Although involving other adults in shared care practices is a common cultural norm among parents and in other contexts of demanding care (Andenæs and Haavind, 2018), similar practices in child welfare appear to be associated with risk. Our study illustrates how sociocultural theory, and the concepts of shared care and communities of practice, can enrich our understanding of care practices in child welfare, allowing insights into how care organisations, such as respite care, can address multiple challenges and have synergies significant to several parties involved, including children. A previous article (Negård et al., 2020) emphasises the significance of these respite arrangements for children in terms of social support, belonging and continuity.
The conceptualisation of care has implications for research, practice and policy. The concepts informing this study have inspired a multi-method approach, enabling a broad exploration and comprehensive analysis of how dimensions resonate across the entire care system, holding multiple meanings and synergies that offer more possibilities than the sum of its parts. This approach has facilitated understanding of the multiplicity and interconnectedness of issues/problems and significance of coordinated sustained support systems capable of adjusting to changes over time.
Based on our analysis, we suggest the concept of a ‘community of care’, which is an analogy to ‘community of practice’, building on its conceptual apparatus while adapting it to the domain of care. ‘Community of care’ provides a position to all involved in the organisation of care, not as suppliers, but as interdependent participants who are acting within given conditions. Moreover, it underlines that the concept of sustainability addresses developmental-conducive processes for all parties involved, in contrast to concepts such as permanency and stability. Applying the concept of sustainability could inspire various care organisations, emphasising the support of all parties involved. Organising care as a combination of residential and foster care seems to be one feasible pathway to holistic care, which is requested in Norwegian public inquiries (NOU, 2018: 18; NOU, 2023: 24). Notably, sustainable qualities cannot be easily transposed from one context to another. The qualities exemplified by Bluehill are not readily adaptable or transferrable at the model-level but can serve as a valuable case for inspiring research, policy and practice in efforts to design for sustainable care.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the article was provided by VID vitenskapelige høgskole/VID Specialized University, Oslo, Norway.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.