
Abstract
Care-experienced youth are more likely than their peers to present with earlier, more severe and more chronic mental health difficulties. This case study presents the development of a Compassion-Focused Therapy (CFT) group for young people who do not live with their birth families due to an early history of abuse and neglect, delivered by psychologists in a social care service. Eight adolescent girls (aged 12–16), who lived in foster, adoptive or kinship care, attended eight face-to-face weekly sessions of a ‘Building Your Self-Confidence’ group. Most of them attended all sessions, found the group ‘enjoyable’ and ‘interesting’, and reported finding it helpful to improve their self-confidence at least to some extent (‘a little’ or ‘yes’). On standardised measures, half of the caregivers reported improvements in their child’s mental health but none of the adolescents did themselves. These initial data pave the way to further optimise the application of group CFT for care-experienced youth and inform psychological treatment innovation in youth more generally.
Plain Language Summary
Young people who grow up with significant trauma such as abuse and neglect, are often taken into the care of the local authority at some point in their lives when they cannot remain at home. These young people tend to experience high levels of mental health difficulties such as depression, anxiety and post-traumatic stress. Innovative approaches to improve mental health in this population are therefore crucial. In this paper, we describe a therapy group called ‘Building Your Self-Confidence’, based on a therapy model called Compassion-Focused Therapy (CFT). This group was attended by eight adolescent girls aged between 12 and 16 who lived in foster, adoptive or kinship care. There were eight weekly face-to-face sessions in total, delivered by psychologists within a social care service in the UK. We found that most of the adolescents attended all the sessions and commented that they found the group ‘enjoyable’ and ‘interesting’, and that their self-confidence was somehow improved. On questionnaires measuring mental health difficulties, half of the caregivers reported that their adolescents’ mental health improved. However, adolescents themselves did not report improvements in mental health in these questionnaires. Overall, this therapeutic group is promising but needs to be refined so that its benefits can be maximised.
Keywords
Introduction
Children and young people who have gone through the care system have usually experienced considerable trauma in their lives, with abuse and neglect being the main reasons for an alternative care placement to their birth family (Chambers et al., 2010). Recent statistics by the UK’s Department for Education (2021) showed that over 80,000 children were in the care system, of which fewer than 3,000 were adopted and fewer than 4,000 were in kinship care with relatives or friends (under a court order known as a Special Guardianship Order). Compared to their peers, care-experienced youth are more likely to have psychiatric disorders (Ford et al., 2007), with up to 45% meeting diagnostic criteria (Meltzer et al., 2003). Maltreatment is an established risk factor for mental health problems that develop earlier, and are more severe (Hovens et al., 2010), more frequently co-occurring (e.g., anxiety and depression) (Harkness and Wildes, 2002), more persistent and recurrent (Hovens et al., 2012; Nanni, Uher and Danese, 2012), and less responsive to standard treatments (Nanni, Uher and Danese, 2012). Many care-experienced children also display emotional, behavioural and social difficulties that significantly impact on functioning despite not meeting diagnostic criteria (Dejong, 2010). These difficulties are likely to be exacerbated during adolescence, as this represents a time window of heightened vulnerability for emotional disorders (Kessler et al., 2005; Patel et al., 2007). Beyond mental health, maltreatment is also associated with additional needs including loneliness (Arslan and Yildirim, 2021), deficits in social competence (Raby et al., 2019), cognitive difficulties (Masson et al., 2015) and neurodevelopmental conditions such as autism and attention deficit hyperactivity disorder (ADHD) (Dinkler et al., 2017).
Available guidelines stipulate that care-experienced children should access evidence-based treatments for mental health disorders (NICE, 2021), but it remains unclear how direct interventions can be used to address the subthreshold symptoms (often of multiple disorders) common in this population which detrimentally impact on wellbeing (Dejong, 2010). A promising avenue for addressing youth mental health is Compassion-Focused Therapy or CFT (Carona et al., 2017). CFT is an integrative psychotherapeutic approach that aims to alleviate mental distress by counteracting shame and self-criticism – both thought to underlie emotional problems transdiagnostically (Tangney, Wagner and Gramzow, 1992; Werner et al., 2019) – through self-compassion of one’s own struggles (Gilbert, 2014). A key focus within CFT is on the three-circle model of emotion which captures three evolved functions of emotions. These include: i) a threat system which activates defensive strategies; ii) a drive system which activates reward-seeking activities; and iii) a soothing system which activates feelings of contentment, safeness and affiliation. This model provides a pragmatic tool to guide individuals to recognise the need to achieve a balance of the three systems and the critical value of developing the soothing system via self-compassion (Gilbert, 2014).
There is a growing body of evidence supporting CFT’s effectiveness for a range of clinical presentations, including anxiety, depression, disordered eating, and post-traumatic stress disorder (PTSD), although more robust study designs are sorely needed (Craig, Hiskey and Spector, 2020; Kirby, Tellegen and Steindl, 2017). CFT is promising for care-experienced youth given that lower self-compassion is associated with psychological distress and experiences of early maltreatment (Marsh, Chan and MacBeth, 2018; Zhang et al., 2021). For PTSD following complex trauma, which refers to long-standing, interpersonal traumas often associated with experiences prior to care, CFT has been proposed to improve readiness to engage with evidence-based psychological treatments (Ashfield, Chan and Lee, 2021; Bowyer, Wallis and Lee, 2014). Specifically, CFT helps an individual to acquire adaptive regulation skills (for a range of emotions including high levels of shame) which in turn increase their willingness and ability to engage more optimally with the processing of traumatic memories that is an essential mechanism for treatment effectiveness (Brewin, 2014).
Explorations of CFT for adolescents remain limited. Individually-delivered CFT interventions have been published through case studies but these either lacked outcome measures (Lander, 2019) or did not use/assess CFT as stand-alone (Bowyer, Wallis and Lee, 2014). A group-based CFT was explored in a recent non-randomised control trial compared to treatment-as-usual (TAU) in a Swedish outpatient psychiatric setting (Bratt, Svensson and Rusner, 2020). In this study the CFT intervention involved groups for adolescents and separate groups for their parents run in parallel; TAU included alternative evidence-based interventions (e.g., cognitive-behavioural therapy or CBT, family therapy, etc.) and strict criteria were applied (e.g., excluding autism). While there were no statistically significant differences in self-compassion and perceived stress in adolescents between both intervention arms, they nevertheless described having gained ‘the courage to see and accept oneself through meeting with peers who are experiencing similar difficulties’ (Bratt, Svensson and Rusner, 2020). Building on this small evidence base, this case study presents the initial development of a novel CFT group for adolescents with experiences of abuse and neglect and who are no longer living with their birth parents, to inform further protocol standardisation and future efficacy studies.
Method
Participants
Eight young people (aged 12–16) living in adoptive, foster or kinship care took part in the group. They were referred to a specialist psychology team within social services in southern England to help increase their ‘self-confidence’ and support their emotional wellbeing. They were all in mainstream schools. See Table 1 for additional description of the eight attendees.
Young people’s basic demographics and circumstances.
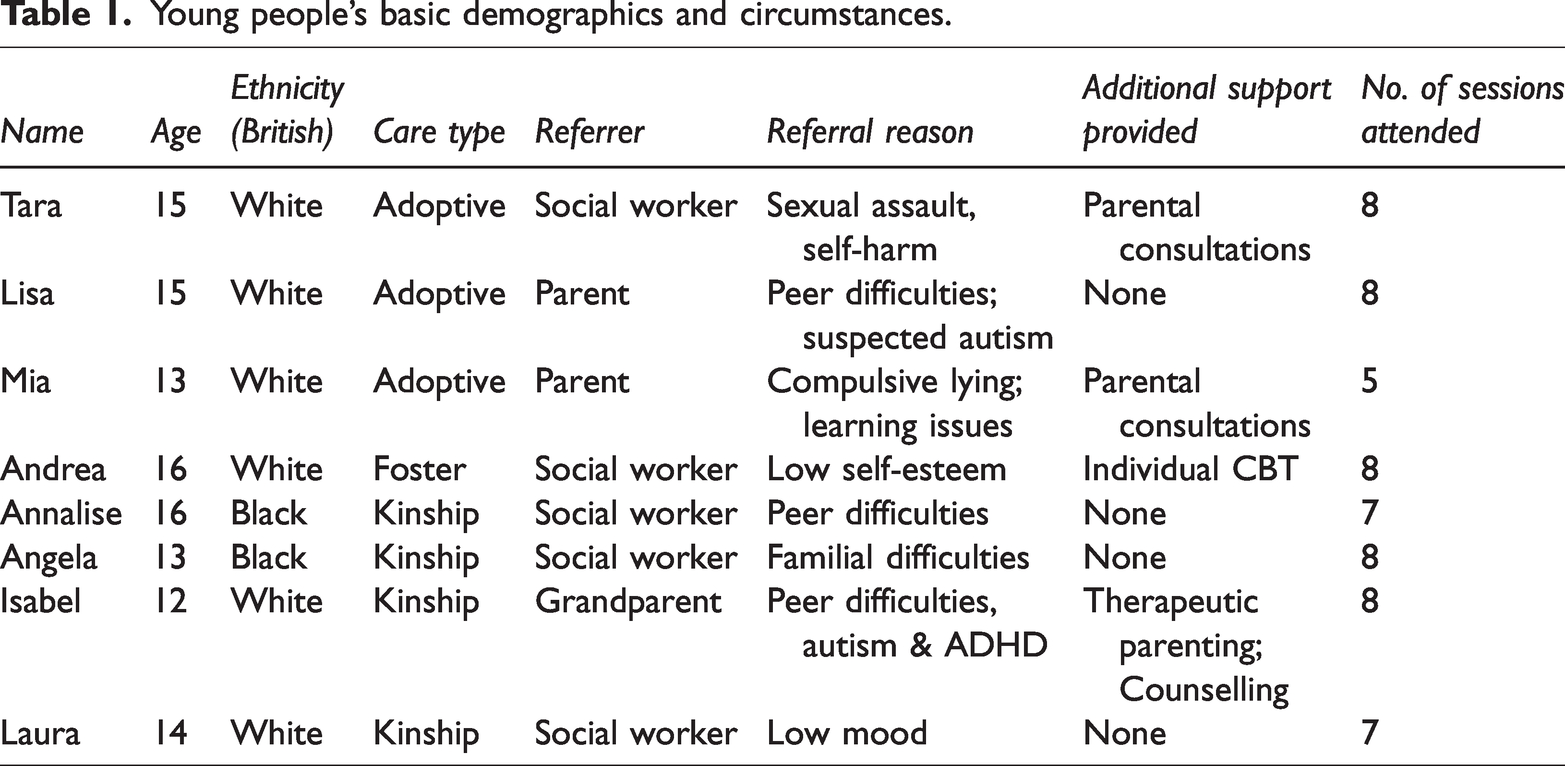
Strict eligibility criteria were not applied given the inherent complexity of the referrals into the service (e.g., neurodiversity, mild learning issues, self-harm) unless they had significant learning difficulties (e.g., attending specialist provisions) or were experiencing acute risks or crisis. Although only girls attended the group, it was not intended for girls only.
Ethical approval was not required as the work presented was part of routine practice in a therapeutic service within children’s social care in the UK. We followed the Ethical Principles of Psychologists and Code of Conduct as set out by the British Psychological Society and British Association of Behavioural and Cognitive Therapies. Consent for both intervention and publication was obtained for young people and their caregivers as part of routine therapeutic work. All names/ages and some background information were changed to preserve confidentiality and anonymity.
Case Illustration: Tara
One young person, Tara, will be presented in more detail to illustrate the process of assessment and formulation that informed their suitability for a CFT approach. Tara was referred by her social worker following a sexual assault by an older male cousin who had a learning disability. Since the incident, Tara’s family has been supported by social care and her cousin has gone to prison. The social worker asked the psychology team to provide therapeutic support for Tara and her family.
Initial Assessment
The initial assessment was conducted online with her mother, Olga, only. She explained that since the incident, Tara had started self-harming by cutting her arms, although the resulting injuries had not required medical attention. Olga understood that Tara wanted to ‘feel something’ as she often felt numb. Tara reported experiencing unwanted memories of the event. She needed to have the lights on to sleep and was often argumentative with family members. She was often on edge when someone walked past behind her. Olga explained that Tara calls herself ‘a survivor’, but also has expressed thinking she could have done something different to avoid the assault, especially given that she and her cousin had a positive relationship growing up. Two people that Tara thought were her ‘friends’ started spreading ‘rumours’ after she confided in them about the incident, thus a change of school was being considered. Prior to the incident, Tara was involved in her school theatre club, enjoyed horseriding and was performing academically well in school.
Olga explained that Tara was adopted into the family when she was six years old. She was taken into care due to severe physical and emotional neglect from her birth mother, who had long-standing mental health difficulties and experienced domestic violence. Tara has three younger birth siblings but she was adopted separately from them as it was thought that she would be overprotective after having played the role of the ‘parent’ for all of them at such a young age. Tara also had lived in two different foster placements prior to the adoption.
This sexual assault had caused enormous pain to the whole family. Olga said that they ‘all’ wanted to stop dwelling in the past and ‘move on’. Olga’s priority was for Tara to stop self-harming. Olga was not sure how to talk to Tara about it as it may ‘bring it all up again’. She also explained that Tara would not agree to therapy that would require her to talk about the incident.
Case Conceptualisation
A working formulation was drawn based on information at assessment and then expanded based on Tara’s contribution to the discussions (see Group sessions and content). A three-system model (Figure 1) based on CFT hypothesised an imbalance in emotional regulation strategies. Her ‘threat’ system was likely overactive, in line with the difficulties reported by Olga which were consistent with a diagnosis of PTSD, including symptoms of re-experiencing, avoidance and hyperarousal (American Psychiatric Association, 2013). This was further exacerbated by internal threats (e.g., self-blaming for the assault) and external threats (e.g., ‘gossip’ in school). She relied on a ‘drive’ system for regulation, working hard to be recognised as a ‘survivor’ and keeping going with her life, which her family supported to avoid ‘dwelling’. However, her ‘soothing’ system was likely underdeveloped due to her history of early neglect and parentification.
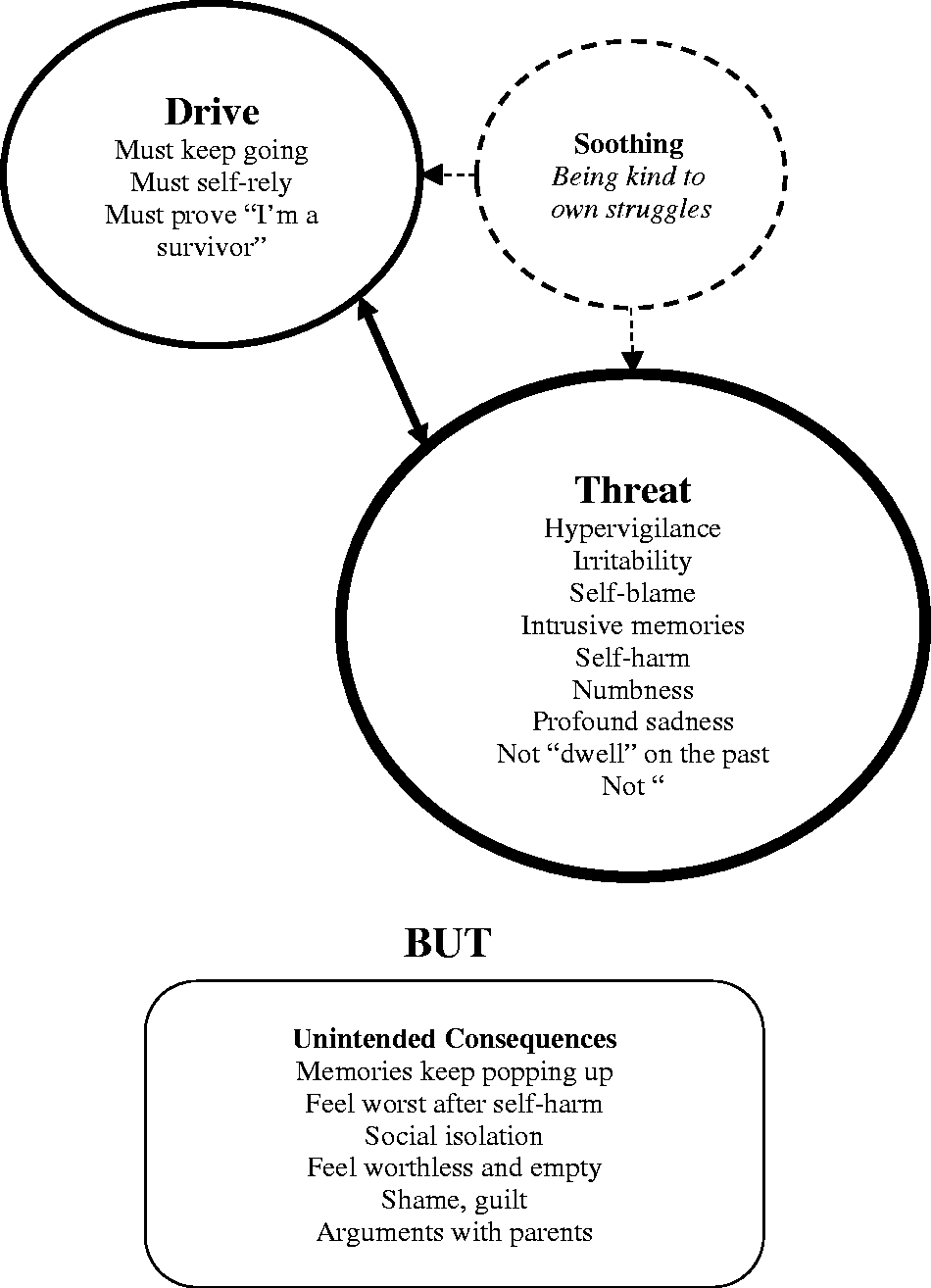
Three-systems formulation for Tara based on CFT.
This imbalance between the three systems may have origins in Tara’s early caregiving relationships, especially the severity of her neglect coupled with parentification. These maltreatment experiences have likely contributed to a shame-based sense of self and core fears such as ‘fear of expressing needs’ or ‘fear of being left alone’ (Carona et al., 2017). Her current safety strategies since the incident represent possible means of addressing these fears, for example: avoiding reminders and talking about the incident to block painful memories; relying on herself, including self-harming, to regulate her own feelings and avoid asking for help; and blaming herself for the incident, as a way to make sense of it and avoid assault in the future. However, these well-meaning strategies lead to unintended consequences, including more persistent memories, numbness and social isolation, and further exacerbate feelings of shame and self-criticism.
This formulation indicated that Tara was likely to benefit from a CFT approach to increase more adaptive regulation skills and reduce self-harm, as well as to augment readiness for possible trauma-focused CBT, which would involve talking about the incident. Olga spoke with Tara who agreed to join a therapeutic group with other young people which would not require her to talk about anything she was not comfortable with.
Group Sessions And Content
The group was called ‘Building Your Self-Confidence’ in line with self-confidence issues being a common concern for referral as described by young people, their families and social workers. Group content was initially developed to make it youth-friendly (Beaumont and Welford, 2020; Welford, 2012), with ongoing modifications (e.g., spending longer on some content and moving some content to a different session) as the sessions went along to consider emerging needs of the group (e.g., learning difficulties and arousal regulation).
Weekly sessions were face-to-face and 90 minutes each (with a 15-minute break). All began with a warm-up exercise (e.g., reporting your emotional weather) and finished with a game (e.g., ‘Would you rather …’). Sessions were run after school and were facilitated by three psychologists (qualified, trainee and assistant) with experience of delivering CFT.
Session 1
The introduction included an icebreaker and discussing ground rules to feel safe. The term ‘self-confidence’ was discussed including celebrities who embody it. Emphasis was made on self-confidence as something that can be built. A small group exercise involved creating a movie character and identifying the signs of their struggles in this area.
Session 2
The role of evolution in brain development was discussed, emphasising it was ‘not designed by you’. The three brain systems underlying one’s own emotions (threat, drive and soothing) were explained alongside the need for a balance between them to increase self-confidence, particularly developing the soothing system. As a self-reflection activity each person drew the size of their three systems.
Session 3
Soothing rhythm breathing was practised to slow down the body and activate the soothing system. The concept of compassion was introduced, emphasising two key parts: ‘noticing the suffering of yourself and others’ and ‘choosing to try to reduce the suffering’. The three flows of compassion (to others, from others, to oneself) were presented with examples. A group exercise involved three groups, each role-playing one emotion system in response to a vignette (i.e., a young person struggling with a new group of friends).
Session 4
Common fears and blocks to compassion (e.g., self-compassion means … ‘I’m weak’, or ‘selfish’, or ‘I’m letting myself off the hook’) were introduced and discussed. An adapted youth-friendly version of the Fears of Compassion Scale (Gilbert et al., 2011) was used as a reflection exercise. The link between imagination and emotions was explained, including imagery as a powerful tool to develop the soothing system. A detailed description of a ‘perfect nurturer’ image was prepared linking multi-sensory details with feelings of safety and inner warmth (Lee, 2005).
Session 5
An overall framework of ‘food for the soothing system’ (Figure 2) was introduced as a menu of options to develop this system over time, linking back to previous exercises (e.g., breathing). The perfect nurturer imagery exercise was performed as a group. The notion of ‘inner bully’ was introduced, followed by a self-reflection exercise to identify it. Emphasis was made on understanding ‘What is it trying to protect you from?’.
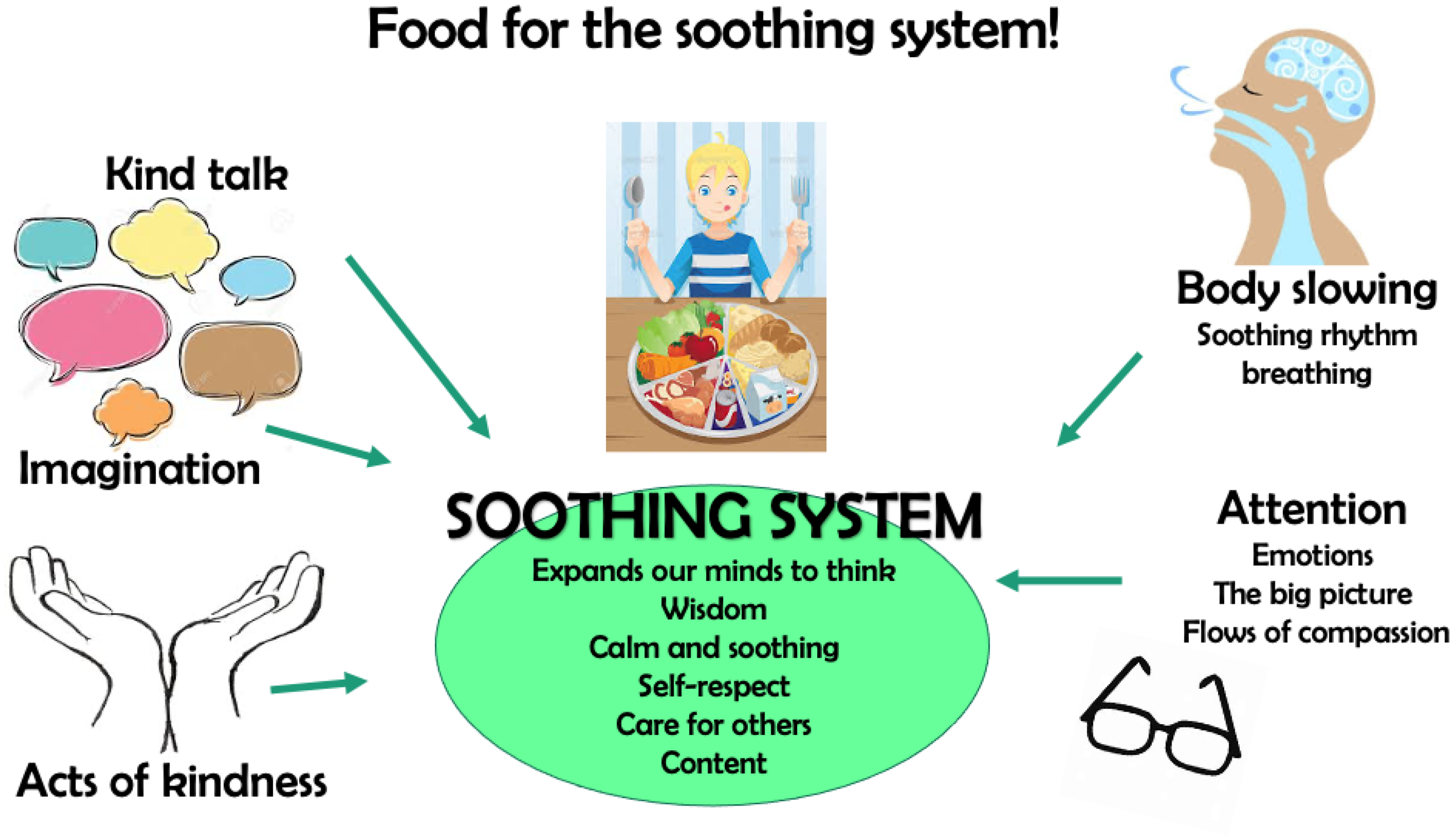
Food for the soothing system.
Session 6
The idea of ‘speaking to ourselves differently’ was introduced to counteract the ‘inner bully’. Emphasis was made on tone of voice as well as the words said. An exercise in pairs involved showing compassion to someone going through something mildly upsetting. A whole-group exercise involved helping a character to talk to herself differently about her struggles of starting a new school. Acts of kindness were introduced as an invitation to practise compassion to others.
Session 7
Fears and coping strategies were discussed, alongside their unintended consequences (‘what I want to happen’ vs. ‘what happens but I don’t mean it to’). An initial example was used to illustrate these concepts (i.e., avoiding eye contact as a coping strategy for the fear of being judged), followed by three examples that were directly relevant to the group (i.e., always putting on a brave face and wearing a ‘mask’; avoiding stressful situations such as school; being critical of myself). The concept of ‘wisdom’ was introduced as the ability to choose to do something different in response to one’s struggles.
Session 8
Loving-kindness meditation was introduced as another self-soothing strategy. A recipe for ‘self-talk’ was presented, bringing previous concepts under the acronym KUWS: knowledge (e.g., ‘How am I feeling?’; ‘Which system is active?’); understanding (e.g., ‘Why does it make sense that I feel this way?’); wisdom (e.g., ‘What is good and not good for me?’); and strength (e.g., ‘What will help me to have the courage needed?’). An example of a compassionate letter to the self was presented with an invitation for participants to do this in their own time. Final reflections were shared and everyone received an ending certificate.
Outcomes
Measures were collected at the start and at the end of the group. For mental health difficulties, the primary outcome was overall symptoms of anxiety and depression (given this approach was not diagnosis-driven). Caregivers completed the Revised Child Anxiety and Depression Scale (RCADS) – 47 Items with a clinical cut-off of t-scores ≥70 (Chorpita et al., 2000). Analyses also explored the number of disorder-specific subscales in the RCADS-47 (i.e., separation anxiety, generalised anxiety, panic, social phobia, obsessive-compulsive disorder and depression) with scores that were above the clinical cut-off. Young people completed the child version of the RCADS-11, with a score range of 0–33 and a clinical cut-off of ≥14 (Radez et al., 2021). For both RCADS measures, higher scores reflected greater severity.
General functioning was assessed by the child version of the Outcome Rating Scale (ORS) which has four visual analogue scales (VAS) capturing wellbeing in ‘me’, ‘family’, ‘school’ and ‘everything’ (Duncan et al., 2006). Higher scores reflected better wellbeing and the score range was 0–40 (with each subscale ranging 0–10). Clinical cut-offs are <28 (for aged 13–17) or <32 (for ages 12 or below).
Change in self-compassion was explored with a single VAS stating, ‘I am kind to myself about my struggles’ and anchored by ‘completely disagree’ and ‘completely agree’.
Anonymous feedback from young people was collected at the end through a bespoke questionnaire with six questions and each with four response options (i.e., ‘Yes’, ‘A little’, ‘Not really’, and ‘Don’t know’): 1) Has coming to the group helped you to feel more self-confidence?; 2) Was the information clear and 3) interesting?; 4) Did you find the group helpful; and 5) enjoyable?; 6) If a friend wanted to build confidence, would you recommend they come to these groups?. Additional qualitative feedback was also collected.
Results
Six out of eight young people attended all sessions and there were no drop-outs for everyone who attended the initial session. Subsequent non-attendance was due to extenuating circumstances (e.g., medical reasons).
Scores on the RCADS-47 (Table 2) revealed that, according to caregivers, five (out of eight) adolescents showed overall mental health symptoms that were in the clinical range at the start, but only two of them showed symptom levels within the clinical range at the end. Furthermore, across all adolescents, five showed a decrease in the number of disorder-specific symptom subscales within the clinical range from start to end, while three had the same number at both timepoints.
Outcome data at the start and at the end of the group.
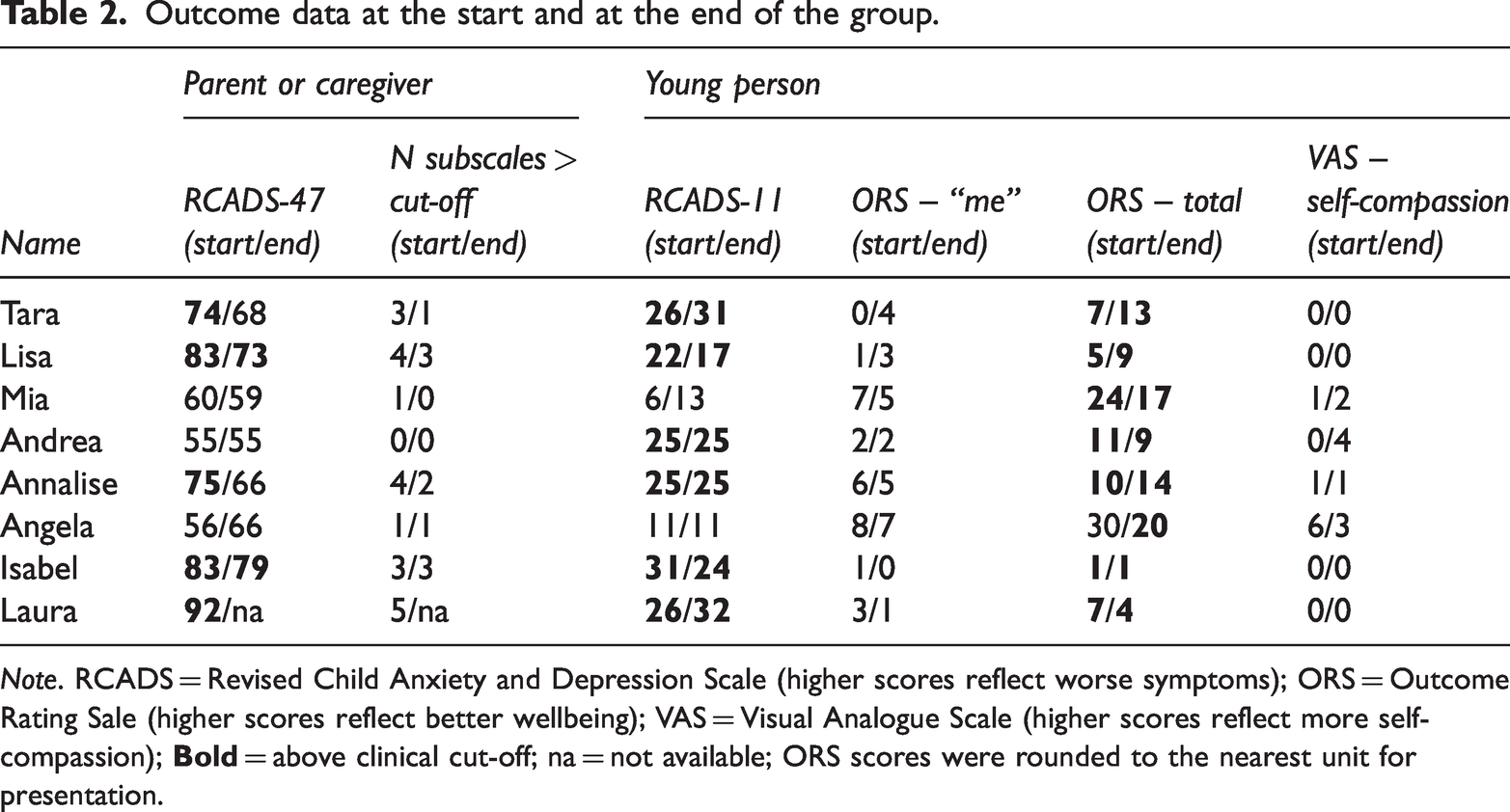
Note. RCADS = Revised Child Anxiety and Depression Scale (higher scores reflect worse symptoms); ORS = Outcome Rating Sale (higher scores reflect better wellbeing); VAS = Visual Analogue Scale (higher scores reflect more self-compassion);
Scores on the RCADS-11 (Table 2) revealed that, according to the adolescents themselves, six (out of eight) showed overall mental health symptoms that were within the clinical range at the start and at the end. Scores on the ORS (Table 2) revealed that for ratings of overall wellbeing, seven (out of eight) adolescents were within the clinical range at the start, while everybody was at the end. On the self-compassion (exploratory) item (Table 2), three showed an increase, one a decrease and three no change.
On feedback about the group, three of the eight adolescents said, ‘yes’ to finding the group ‘helpful’ while five said ‘a little’. Two said ‘yes’ to the group helping them to feel more self-confident and again five said ‘a little’. Six said they would recommend the group for a friend who wanted to build their self-confidence. Seven found the information ‘clear’ and ‘easy’ to understand and five found it ‘interesting’. Six found the group ‘enjoyable’. They said they appreciated ‘the compassion tasks and meditation’, ‘the discussions’, and importantly ‘meeting new people’. Informal conversations with caregivers after each group session also suggested that young people were ‘buzzing’ after the group and talked positively about it at home.
Discussion
This case study presented the initial development of a ‘Building Your Self-Confidence’ group based on CFT for young people with early history of abuse and neglect and who live in foster, adoptive or kinship care. All eight adolescents attended the group until the end; everyone reported that it improved their self-confidence to some extent (‘a little’ or ‘yes’), and six found the group overall ‘enjoyable’ and one said ‘a little’. On standardised measures, half the caregivers reported improvements in their child’s mental health but none of the young people did themselves. We use these initial data as a springboard to share key reflections on the process of adapting and evaluating this group intervention and to discuss ways forward to further adapting it for care-experienced youth.
Why did young people and their caregivers report different outcomes on standardised measures? It is possible that caregivers were more able to notice ‘external’ changes in behaviours but underestimated more ‘internal’ symptoms in young people (De Los Reyes et al., 2015), such as their thoughts and feelings. However, caregivers rated the more established 47-items version of the RCADS which has been shown to be sensitive to change (Chorpita et al., 2000), whereas young people rated a recently developed 11-items version which has been validated for screening purposes only (Radez et al., 2021). This shorter version was chosen to reduce demands on children with maltreatment histories who often experience cognitive difficulties (Masson et al., 2015) but it may not have been sensitive to the benefits of CFT on mental health. The ORS may also be less sensitive to changes in everyday functioning given the frequent psychosocial stressors in care-experienced children. The discrepancies between informants underscore the importance of a multi-method approach to measuring outcomes.
A core skill taught in CFT is to notice one’s own struggles to enable further compassionate understanding (Carona et al., 2017; Gilbert, 2014), so improved recognising and reporting of distress in some young people could have masked improvement in other symptoms within the same questionnaire. In other words, young people may have learnt to acknowledge their own sadness while experiencing less self-accusation, but not necessarily ‘feel better’ yet in the short-term. Indeed, everyone reported at least to some extent that their ‘self-confidence’ was helped by the group. Our single-item, non-validated question on self-compassion was insensitive to change, thus there is scope for improved ways of tracking changes in self-compassion skills to better understand the mechanisms of change. The fact that changes were more apparent to caregivers may reflect young people’s newly acquired ability to open up and talk more about how they feel (Bratt, Svensson and Rusner, 2019). Further developments may consider upskilling caregivers in parallel so that they become more receptive to the young people’s possible increased need for closeness (Bratt, Svensson and Rusner, 2019).
While the promise of CFT for adolescents has been highlighted before (Beaumont and Welford, 2020; Bowyer, Wallis and Lee, 2014; Bratt, et al., 2020; Carona et al., 2017; Lander, 2019), it remains unclear whether and which adaptations in content are necessary to better scaffold adolescent learning. The established approach – developed in adults – emphasises the importance of developing self-compassion through activating physiology underlying the soothing system early on, such as through breathing and imagery (Carona et al., 2017; Gilbert, 2014). The young people found these exercises challenging despite several attempts, possibly because feelings of grief were triggered when the self-soothing system was first activated (Gilbert, 2014). This process may be heightened in care-experienced children who have often had multiple losses in their care history (Chambers et al., 2010). At least for this population, future CFT adaptations could consider first emphasising cognitive components (e.g., safety strategies and unintended consequences; fears and blocks), allowing greater trust to be built in preparation for physiological techniques later.
The delivery context may also be important in optimising the benefits of this approach. Psychosocial complexity is inherent to the lives of many care-experienced children. In our group, some ongoing stressors included bullying, sibling violence, school exclusions and health complications. Some may argue that eight 90-minute sessions did not constitute a sufficient ‘dose’ of CFT for this group and that after-school hours are less optimal for additional learning. To be most inclusive, strict eligibility criteria were not applied (including neurodiversity), but this meant there was a broad range of learning needs. Some alternatives or additional components could include individual booster sessions and incorporating caregivers (e.g., to promote practice) but these have resource implications. While individually delivered CFT may be the best approach for some, many valued “meeting new people” in a group setting, echoing previous work with adolescents where connecting with others was described as a key benefit (Bratt et al., 2020) as well as the current stronger evidence base for CFT delivered in groups (Craig, Hiskey and Spector, 2020). Moving forward, more in-depth views should be sought from young people, parents, and professionals about the most optimal context for delivering CFT.
We also did ongoing modifications primarily in relation to spending more time on some content (e.g., recognising and helping the inner bully) over others (e.g., writing a self-compassion letter) as we realised the group needed more time and support to identify and address particularly emotive issues. However, it remains unclear if the usefulness of these modifications was specific to this group or will also apply to other compositions. This issue merits further exploration given the important need for protocol standardisation for future dissemination.
Limitations
While this case study represents an early-stage adaptation of a CFT group for care-experienced young people showing some promising data, important limitations remain. Awaiting further refinement of its content and format, more robust designs would be needed to confirm its effectiveness in promoting mental health. These include: a comparison to an appropriate control group; bigger samples with sufficient power facilitating formal statistics (including moderation analyses by care type); use of improved outcome measures across all stakeholders (e.g., including repeated baseline assessment of outcome variables); and follow-up assessments to ascertain long-term impact. It is difficult to isolate the contributions of CFT from other ongoing support that young people and their families are receiving (Table 1), but within social care a multi-professional and multi-agency involvement is the norm rather than the exception. It also remains to be tested whether this approach can be applicable to care-experienced boys and in a non-UK context. Low recruitment of boys has also been shown in a recent application of group CFT in Sweden (Bratt, Rusner and Svensson, 2020), an issue that needs further unpacking.
Conclusions
Our early-stage adaptation of a CFT group showed promise to alleviate psychological distress and improve mental wellbeing in care-experienced young people. Future developments that we are hoping to explore include further adaptations for (blended) digital delivery, mixed gender groups, older versus younger teen groups, a parallel group for parents, and specific adaptions that consider neurodiversity. Further, delivering this group as a one-week summer programme is underway and evaluation is pending within our service. A better understanding of how best to improve its delivery and evaluation will pave the way to further optimise the application of group CFT for this population, which could also inform psychological treatment innovation in youth more generally.
Footnotes
Acknowledgements
We are grateful to Dr Carmen Chan (and the Oxfordshire Compassion Focused Therapy Special Interest Group) for sharing materials and providing consultation to develop the group’s content; and to Chloe Reed for co-facilitating the group.
Declaration of conflicts of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Oxford Health NHS Foundation Trust as part of clinical psychology doctorate training for ALZ.