
Abstract
Practising self-care is vital for foster carers to cope with the stresses of the caring role, provide the best care possible and continue in their task. This current study contributes to emerging research on the self-care practices of foster carers in Australia and worldwide. It used an exploratory design, surveying 148 foster carers about their self-care and conducting individual, semi-structured interviews enabling nine of them to elaborate on their self-care experiences. The results indicate that while the participants sometimes engage in self-care and value it as a way of maintaining their wellbeing and increasing their caregiving capacity, they face several barriers to doing this. These include the multiple responsibilities of the foster carer role, children’s commitments, employment and finances. Facilitators of self-care include social and family support, contact with other carers and carer respite. Foster care agencies and the out-of-home care system should aim to meet the self-care needs of carers by providing increased support, resources and education.
Plain language summary
Self-care is important for all individuals and vital for those providing care to children in out-of-home care who often have complex and challenging needs. This study asked 148 foster carers in Australia what they did to practise self-care. Foster carers demonstrated an understanding that self-care is important and a desire to practise regular self-care. However, they identified many barriers to engaging in self-care. This article explains why and how foster carers practise self-care, what prevents self-care from occurring and how to improve foster carers’ self-care practices.
Introduction
As of 30 June 2021, there were 46,200 children and young people in out-of-home care (OOHC) in Australia, of whom 36% (n = 16,600) were living in foster care and 54% (n = 25,000) in kinship care (Australian Institute of Health and Welfare [AIHW], 2022). Foster/kinship care (hereafter referred to as foster care) is the everyday care of a child or young person who is unable to live safely with their biological parents, provided by an authorised caregiver in the carer’s own home on a short- or long-term basis (AIHW, 2022). In 2021, there were approximately 9,000 foster care and 15,600 kinship care households in Australia (AIHW, 2022).
Children and young people in OOHC have increased caregiving needs compared to the general population. Many have had traumatic experiences that can result in challenging behaviours (Bridger, Binder and Kellezi, 2019). As a result, some foster carers are exposed to regular or ongoing stressful and potentially traumatic experiences themselves (Blythe et al., 2013), which place them at risk of vicarious trauma or secondary traumatic stress (Bridger, Binder and Kellezi, 2019; Jenkins and Baird, 2002). Unfortunately, many recommended strategies to combat vicarious trauma are unrealistic for foster carers (Bell, Kulkarni and Dalton, 2003; Trippany, Kress and Wilcoxon, 2004). For example, it is impractical for them to reduce exposure to their foster child’s trauma while providing continual care and support.
There is also a relatively high prevalence of physical, intellectual and learning disabilities as well as mental health issues among children and young people in OOHC (Murray, Tarren-Sweeney and France, 2011). These issues necessitate increased engagement with educational facilities and specialist services, placing additional demands on foster carers (Meetoo et al., 2020; Murray, Tarren-Sweeney and France, 2011).
As part of their caregiving role, foster carers are supported by and accountable to foster care agencies (Randle, Miller and Dolnicar, 2017). These are responsible for providing training and facilitating access to professional services, respite and financial support. However, extant literature reveals that many carers in Australia (Octoman, McLean and Sleep, 2014; Riggs, Augoustinos and Delfabbro, 2007) and internationally (MacGregor et al., 2006; Murray, Tarren-Sweeney and France, 2011) feel unsupported in the role.
There are also persistent issues related to foster carer recruitment and retention in the US (Hanlon et al., 2021; Melz, Killian and Graham, 2019; Wulczyn et al., 2018), the UK (Blackburn, 2016; Ofsted, 2021) and Australia (Harding et al., 2018; Randle et al., 2017; Sammut, 2017; Thomson, McArthur and Watt, 2016), resulting in insufficient numbers of carers. Finances and family circumstances are common factors precluding recruitment (Randle et al., 2017; Thomson, McArthur and Watt, 2016), with some carers discontinuing due to age or unrelated family issues (Osborn et al., 2007). However, others leave for reasons associated with the task, for example, due to burnout, lack of support, challenging demands, the responsibilities of the role, the impact of foster care on the family and a lack of training (Gilbertson and Barber, 2003; Osborn et al., 2007; Randle et al., 2017). Attrition of carers results in a detrimental loss of valuable experience, fewer homes available for children (Bromfield and Osborn, 2007a) and increased risks of placement breakdowns, with some children subsequently experiencing multiple placements during their time in care (Bromfield and Osborn, 2007b). Such placement instability leads to an increased risk of behavioural issues (Rubin et al., 2007; Stott, 2012) and psychopathology (Fawley-King and Snowden, 2012) among the children and young people.
Self-care
Self-care is an intentional process or action to enhance functioning and overall wellbeing (Dorociak et al., 2017). It comprises many domains, including physical, psychological, social/relational, spiritual and mindful (Cook-Cottone and Guyker, 2018; Richards, Campenni and Muse-Burke, 2010). It can vary significantly between individuals due to cultural background, values, age, physical and emotional needs and personal preferences (Dorociak et al., 2017). Individuals who engage in regular self-care experience better health and wellbeing compared to those who do not (Moses, Bradley and O’Callaghan, 2016; Rupert and Dorociak, 2019), suggesting that proactively engaging in such activities is an important preventative measure for stress and burnout (Cook-Cottone and Guyker, 2018; Dorociak et al., 2017).
Regularly incorporating self-care into one’s daily routine also increases resilience and life satisfaction and improves stress management (Dorociak et al., 2017; Richards, Campenni and Muse-Burke, 2010). The activities that fall into the category of ‘mindful self-care’, which involves an awareness of one’s feelings and responses, have been shown to be especially effective in enabling people to care for others resiliently and sustainably (Li, Yuan and Zhang, 2016; Sanchez-Reilly et al., 2013). This approach enhances the positive effects of traditional self-care by incorporating awareness and active, mindful practices into one’s regular self-care routine (Cook-Cottone and Guyker, 2018). However, while it is clear that self-care benefits people who care for others both formally and informally (Merluzzi et al., 2011), its benefits for foster carers have not yet been thoroughly examined in the context of Australian OOHC.
Foster carer self-care
There is limited research on foster carers’ self-care needs and practices. Several studies have examined the experiences, challenges, needs and satisfaction of foster carers in Australia and internationally (Blythe et al., 2013; Cooley, Thompson and Wojciak, 2017; MacGregor et al., 2006; Murray, Tarren-Sweeney and France, 2011; Randle, Miller and Dolnicar, 2017; Samrai, Beinart and Harper, 2011), but few have specifically explored how foster carers engage in self-care to mitigate the challenges associated with their role.
An exploratory study by Miller and colleagues (2019) used an online survey based on the Self-Care Practices Scale (SCPS) to examine the self-care practices of foster carers in the US. They found that factors such as gender, race, health and employment status affected self-care, with women, non-white/-Caucasian people, those with poor health and the unemployed reporting less self-care engagement than their peers. Miller and Grise-Owens (2021) also used the SCPS to explore the self-care practices of 1,229 foster carers in the US during the Covid-19 pandemic. Results showed that participants’ engagement with self-care was generally low and further decreased during the pandemic.
A recent qualitative study by Miko, Berger and Krishnamoorthy (2022) explored the self-care practices of foster carers in Australia. Analysis of individual interviews with eight carers showed self-care to be a multidimensional process that required the support of foster care agencies and the OOHC system. The carers revealed that they often put others’ needs above their own but articulated the importance of regular self-care for stress management and longevity in their caregiving role.
While these studies provide some insight into foster carers’ engagement with self-care, there is minimal literature exploring their understanding of it or the facilitators of and barriers to their engagement with it in the Australian context.
Study aims
The purpose of this research was to gain an understanding of the self-care practices of foster carers in the Australian context. The following questions guided the study:
What do foster carers understand about the concept of self-care? How often and in what ways do foster carers engage in self-care? What do foster carers perceive to be barriers to and facilitators of self-care?
Methodology
Research design
The study employed an exploratory, concurrent design that consisted of a quantitative online survey and qualitative semi-structured interviews. This design was selected to gain an in-depth understanding of foster carers’ perceptions of and engagement in self-care practices.
Sample
To be eligible for the study, participants needed to be 18 years or older, be an authorised foster carer in Australia, have provided foster care in their own home in the last five years and speak good English. The survey was posted on seven randomly selected, closed Australian foster carer Facebook groups and the authors’ Twitter and LinkedIn pages. Participants were encouraged to share the survey link with other potential participants.
Measures
Information about the study was provided at the beginning of the survey. All participants gave informed consent.
The survey collected demographic information on participants’ gender, age, employment, number of children they looked after and how long they had been providing care. Two additional questions asked participants to rate on a 0–10 Likert scale how stressful their life had been and how stressed they had felt in the previous two weeks. The remainder of the survey used self-care questions from the Mindful Self-Care Scale (MSCS). This validated tool (Cook-Cottone and Guyker, 2018; Hotchkiss and Cook-Cottone, 2019) measures the self-reported frequency of self-care behaviours across the self-care domains of mindful relaxation, physical care, self-compassion and purpose, supportive relationships, supportive structure and mindful awareness. The 36 questions asked the respondent to rate the frequency of that self-care behaviour in the past seven days across a five-point Likert scale from ‘Never’ to ‘Regularly’. One question was reverse scored. The final survey question invited participants to leave their contact details if they were willing to be interviewed. The survey was administered via Qualtrics and took approximately ten minutes to complete.
Statistical analysis
Survey data were analysed using SPSS version 27.0.1.0. Descriptive statistics were used to summarise the demographics of survey respondents, such as age, employment status, number of children in care, self-care behaviours and perceived stress levels. Average subscale scores were generated for each respondent by summing the scores for each question within the self-care domain and then dividing by the number of questions within the domain. These scores were then used to generate the mean subscale scores across the sample. Mean scores for the physical domain were calculated after reverse-scoring the sedentary question. Pearson’s correlation was used to assess the relationship between participants’ perceived stress levels and their engagement in self-care.
Interview process
A total of 43 survey participants indicated a willingness to be interviewed. Information regarding the interview and consent processes was sent by email, and interviews were scheduled at a mutually convenient time. Both written and verbal consent was obtained from all nine interview participants. The semi-structured interviews were conducted, recorded and transcribed using Zoom. A list of questions was used as a guide, allowing the researcher to prompt participants to share their stories freely (Adams, 2015). Examples of questions included, ‘What is your understanding of self-care?’ and ‘What are any barriers you may experience that prevent you from practising self-care?’
Qualitative analysis
Transcripts were anonymised and checked for accuracy then thematically analysed using Braun and Clarke’s (2012) framework. This analytic process included examining and becoming familiarised with the data, generating initial codes, collating potential themes and gathering data related to them, revising the themes and, finally, naming the themes to best represent the shared stories of the carers (Braun and Clarke, 2012). The first author (MG) undertook the initial analysis of the transcripts, while two of the other authors (SB and NP) read a small sample of transcripts to confirm the analytical method. Regular discussions were held throughout the analytical process to ensure consensus between authors.
Survey and interview data were initially analysed separately. Subsequent data integration allowed for a more comprehensive understanding of foster carers’ self-care practices and perceptions of self-care.
Ethical considerations
The Human Research Ethics Committee at Western Sydney University granted ethical approval.
Results
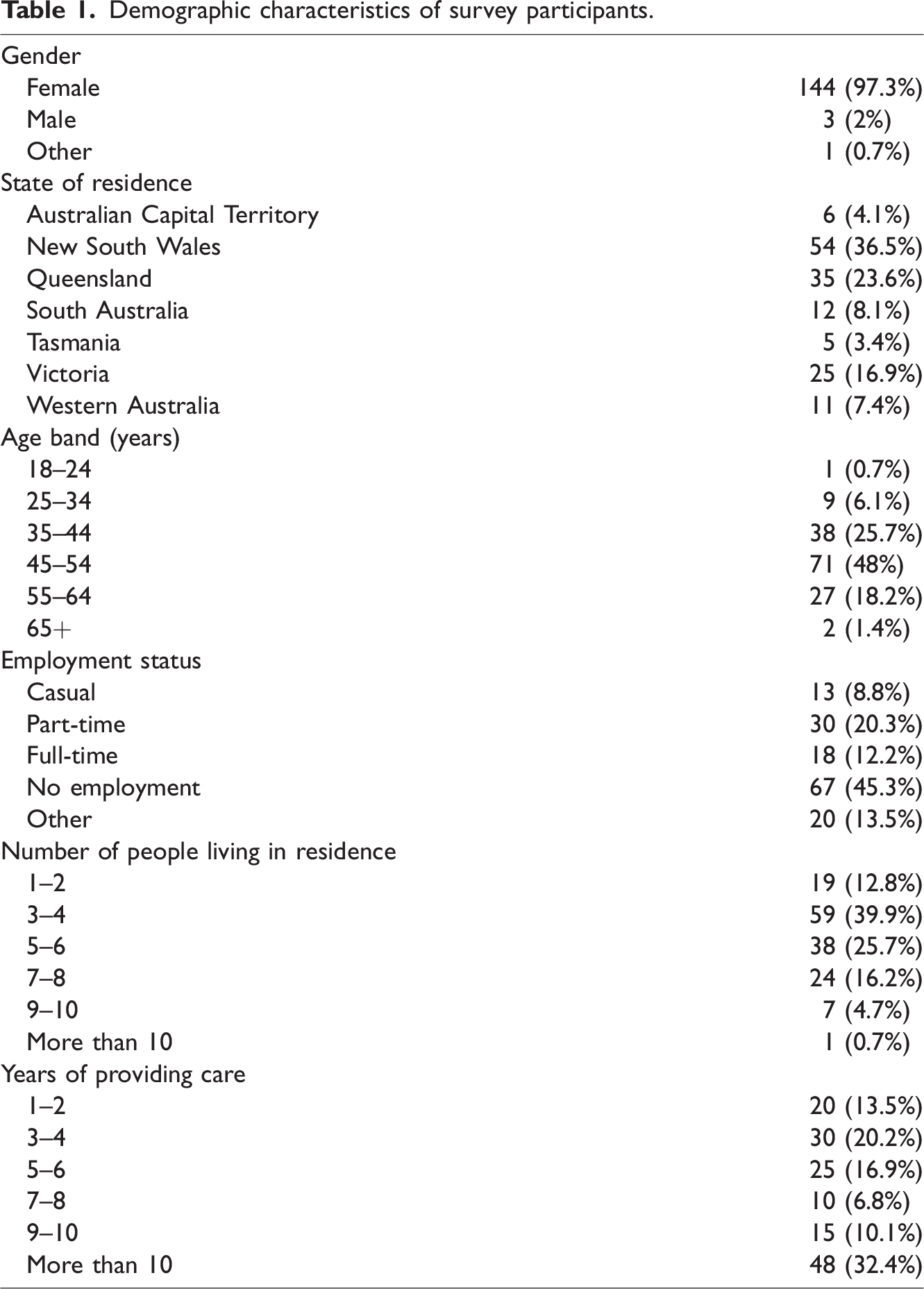
The survey was available online from December 2020 to May 2021. A total of 180 foster carers started the survey, 148 of whom submitted complete or mostly complete survey responses and were thus included in the analysis. See Table 1 for the demographic characteristics of survey respondents.
Demographic characteristics of survey participants.
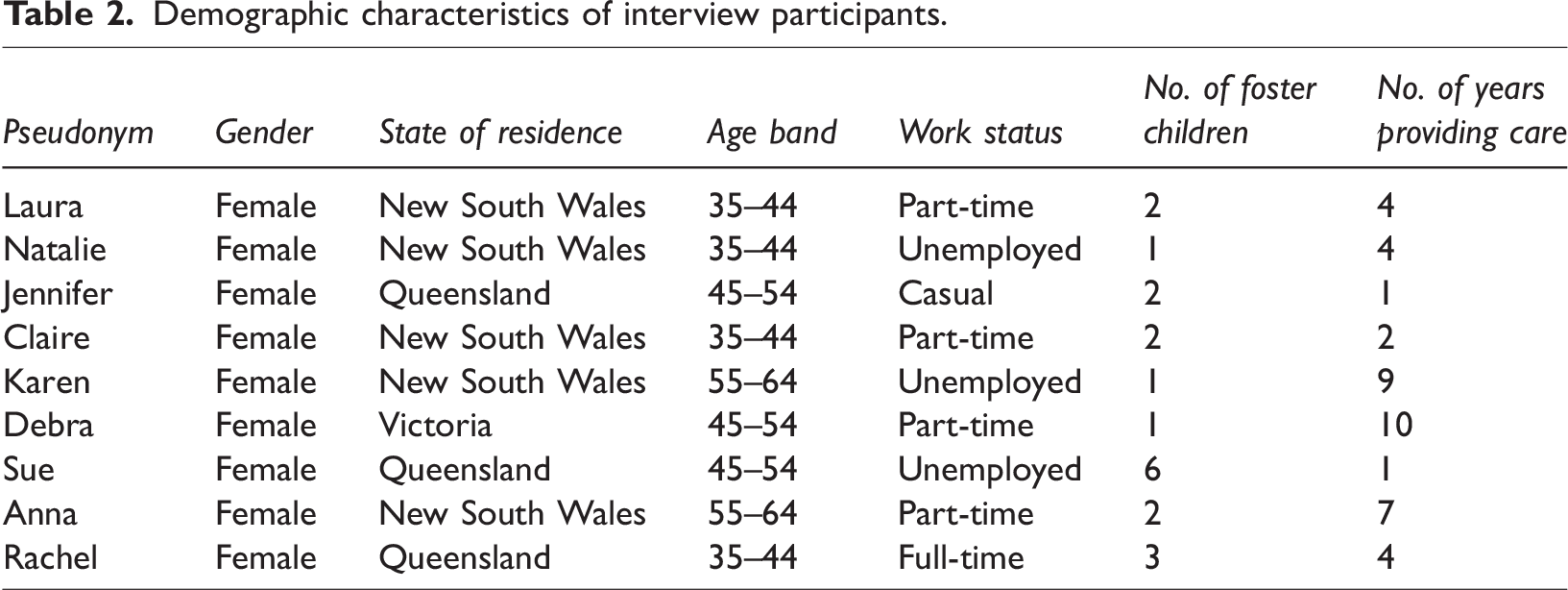
Although 43 survey respondents indicated their willingness to be interviewed, only nine responded to follow-up emails/phone calls and participated in the study. Their demographic characteristics are shown in Table 2. The interviews occurred between January and March 2021, and the average interview duration was 30 minutes, ranging from 20 to 39 minutes. Pseudonyms have been used to present the findings and to ensure participant confidentiality.
Demographic characteristics of interview participants.
Foster carer’s self-care experiences
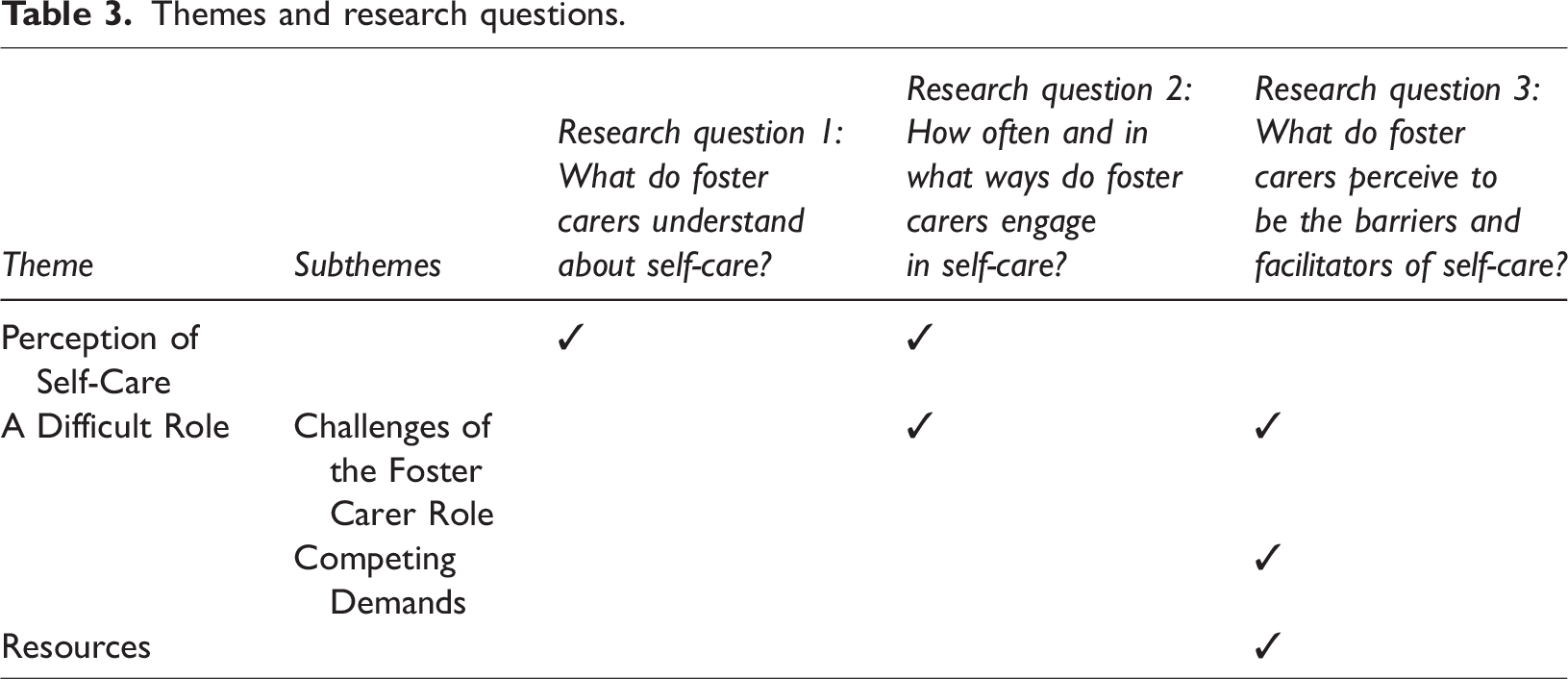
Three salient themes arose from the interview data. These were: (1) Perception of self-care; (2) A difficult role; and (3) Self-care resources. These themes along with correlated survey data are presented in Table 3.
Themes and research questions.
Perception of self-care
Foster carers shared different perceptions and understandings of self-care and practised it in various ways. Scores for four out of five of the self-care domains in the survey ranged from nought days (never) to six to seven days (regularly) (see Figure 1).
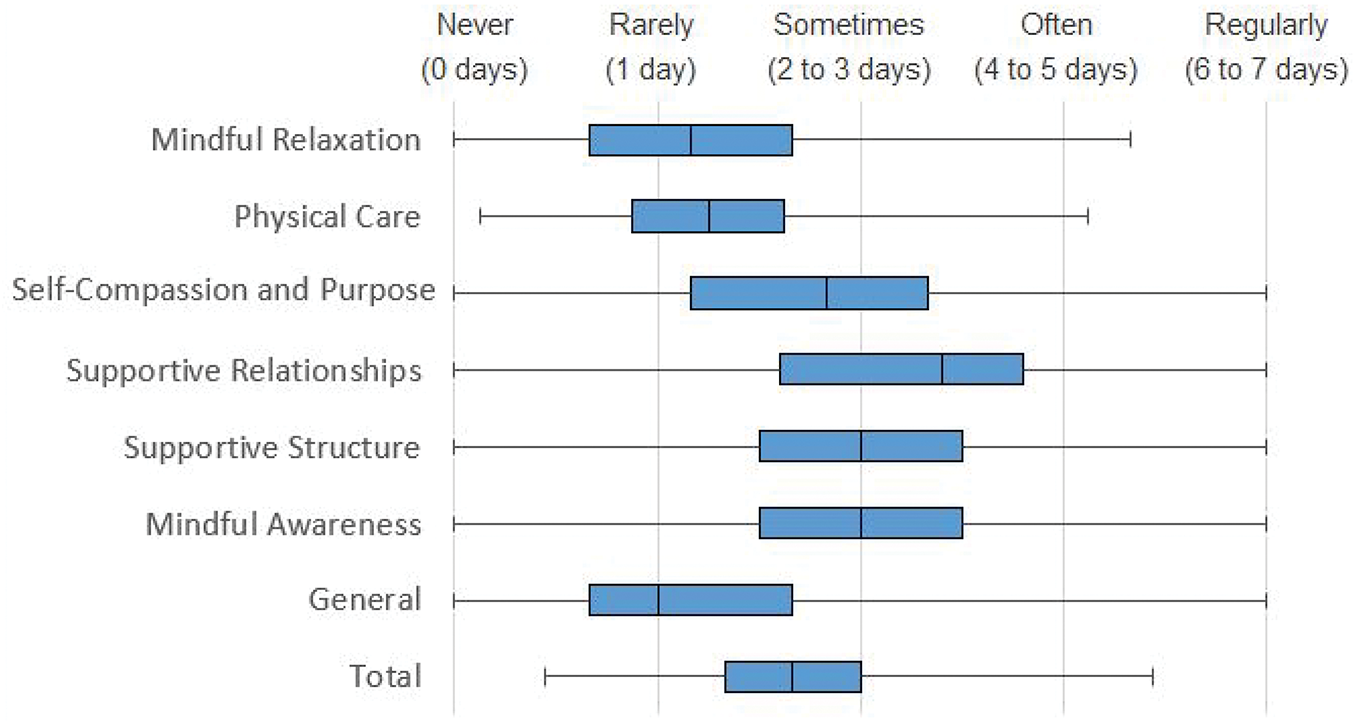
Box and whisker plot of scores for self-care domains.
Just under half of the carers interviewed described self-care as comprising physical behaviours; the survey showed that most respondents engaged in it two to three days per week (Figure 1). Physical exercise was undertaken on an average of one day per week while nutritious foods were consumed more frequently (three to four days per week). Two-thirds of those interviewed also described social interaction, such as spending time with their partner or a good friend, as a vital part of their self-care, with the survey results emphasising the value they accorded to this and their regular engagement in supportive relationships (three to four days per week).
Mindful self-care, in contrast, was practised less frequently, at one to two days per week (Figure 1). In the interviews, carers rarely described their self-care as consisting of mindful activities, but those who did valued them highly. The activities mentioned included gardening, reading and crafts. When discussing mindfulness, carer Natalie stated: ‘For me it’s staying home alone with a book … quiet and alone. That’s self-care.’
Overall, the data showed that most carers reported engaging in some kind of self-care, either occasionally or at least two days per week.
A significant perceptual difference among carers was whether their self-care was intentional (planned) or incidental (unplanned). Just under half of the interviewees reported self-care planning to be necessary. Such activities included gym classes, meeting a friend and spending time with their partner. Carers valued them as they enabled a scheduled break from caring duties. However, the survey also showed that they rarely planned self-care, with some respondents describing it as ‘incidental’. This involved finding personal time between caring responsibilities or at the end of the day, such as watching Netflix while the children were asleep. Carers who perceived their self-care in this way expressed dissatisfaction with their planned activities and a desire to increase them. For example, when discussing future self-care, Debra stated: ‘I plan on sort of implementing more of a routine for myself …’
More than half of the interviewees identified self-care as a strategy to prevent burnout in their caring role. When asked about the impact insufficient time for self-care would have had on her work as a carer, Jennifer stated: ‘I would have quit. I couldn’t do it.’ Many interviewees also recognised the effect of poor self-care on the children they looked after. When they were unable to engage in regular self-care, they described having difficulty meeting the children’s needs and feeling less patient or tolerant. For example, Jennifer explained: ‘… if the carer’s not okay, they’re not going to be providing the kids with what they need.’ Conversely, interviewees also recognised the positive impact of self-care on their caring capacity. Many described feeling that they were better carers when they had time to themselves as they had more patience and empathy. As Laura said: ‘If I’m looking after myself and I’m feeling really good then I can give, I can fill their cup …’
A difficult role
Challenges of the foster carer role
The foster carer role was described as ‘difficult’ and ‘stressful’ by several interviewees. Survey respondents scored, on average, seven out of 10 for how stressful their life had been and seven out of 10 for how stressed they had felt in the past two weeks. There was a strong negative correlation (r = 0.40, p < 0.001) between perceived stress levels and self-care scores from the survey, indicating that those who reported higher perceived stress levels also reported engaging in less self-care.
A key source of stress identified by all but one of the interviewees was the OOHC system. Several aspects of it were perceived as contributing to stress, including restrictive OOHC policies, a lack of foster carer rights and poor distribution of services. As Natalie recalled: ‘… I felt, from the very beginning, I was kind of fighting a system.’ Alongside this, most interviewees described the constant need to prioritise the demands of others, especially the children, over themselves. For example, when asked about the barriers to self-care, Jennifer replied: ‘… it feels a bit like constantly trying to, you know, like, keep everyone happy.’
Some carers expressed feeling an overarching pressure within the OOHC system to avoid asking for support, thus creating a barrier to freely engaging in self-care. For example, when discussing respite, Rachel described feeling as though using respite needed to be normalised: ‘… it’s a cultural thing in my area that, it’s … it’s not okay to ask for that kind of support.’
Many of the carers interviewed discussed the emotional toll of providing care, including feelings of frustration when struggling to manage children’s behavioural issues and guilt when utilising childcare or respite services. Almost half of them described feelings of exhaustion, both physical and emotional, and how this reduced their motivation and desire to practise self-care. As Karen stated: ‘… sometimes when you’re really tired, you just don’t have the energy to go and do anything.’
The interviewees identified strategies they used to combat these challenges, such as setting boundaries, reducing commitments and saying ‘No’ to increasing the number of children for whom they provided care. Some also identified specific self-care tasks to combat stress, such as reading or doing something creative.
Competing demands
Interviewees stated they did not have the time to engage in self-care due to competing demands and responsibilities. All but one of them prioritised the responsibilities set by the OOHC system or their foster care agency over their self-care. These systemic barriers included extra meetings, visits from caseworkers and documentation, such as applying for permission for activities, travel or visitors. For example, Jennifer pointed out that despite foster care being a voluntary role, it demands a considerable amount of time and effort: ‘The workload is huge.’
Similarly, just over half of the interviewees said that the requirement to maintain contact with foster children’s biological families diminished opportunities for self-care. Contact occurred via supervised phone calls and personal visits, which carers described as time-consuming and emotionally draining.
Two-thirds of interviewees identified foster children’s extracurricular and social commitments or having a child with high needs, such as a disability or a history of trauma, as further barriers to prioritising their self-care. These competing responsibilities included medical appointments and extra meetings or visits with the caseworker or agency. When describing these, Jennifer said she felt overwhelmed: ‘… we have appointments every single day of the week.’
Nearly half of the interviewees also identified being in paid employment as a major demand on their time. The need to support the household financially as well as to look after a child made it difficult to fit self-care activities into their schedule. This was especially the case for sole carers in single-income households. As Rachel observed: ‘Apparently, we need to relax and have time to ourselves … I don’t get a lot of that time between [shifts at] work …’
Lastly, some interviewees experienced limited time for self-care as they needed to prioritise their unallocated time for housework and errands, such as laundry or grocery shopping. Nevertheless, despite all these competing demands, survey respondents indicated engaging in an environment where they felt supported and undertook their regular routine of self-care activities two to three days per week (Figure 1).
Self-care resources
All nine foster carers interviewed discussed the impact of resources on their self-care engagement. Most identified the support of foster care agencies as an essential resource, and those that did not receive it felt less motivated to engage in self-care. The perceived lack of support led to increased stress causing their self-care to suffer. The agency supports mentioned as the most helpful were promoting and supporting carers’ wellbeing, listening to them and offering practical help when needed. Many carers reported feeling a lack of agency support to look after themselves, leading Claire to suggest that: ‘… if the agencies advocated for self-care more, if they encouraged it more, it’d be a lot easier to do.’
As well as the perceived lack of support, some participants identified feeling unappreciated by their agencies for their role, although others described the positive impact of caseworker support on their wellbeing. Anna stated: ‘… my caseworker is really nice … I feel okay in saying that I’m not okay.’
All but one interviewee expressed the value of contact with other foster carers as a self-care resource. This was often online, such as through Facebook groups, but could also be in person, with carers meeting up or seeing one another at foster carer events. As Sue remarked: ‘… I think self-care is, you know, having a community, really, in foster caring.’
Similarly, other forms of social support were mentioned as essential for self-care, with most interviewees stating that social relationships with friends, partners and family members were particularly important. This was echoed in the findings from the survey where respondents indicated that they felt supported by those already involved in their lives and who would listen to them when upset. Some also recognised the positive impact of having a partner on their ability to schedule self-care, as highlighted by Karen when discussing help from her husband: ‘… he knows when I’m wearing out of energy and he will tell me, “You need to go and take a break”.’
However, despite the value of social support as a resource, just over half of the interviewees identified a lack of wider social understanding about the foster carer role as a barrier to receiving it in sufficient amounts. They discussed feeling judged and misunderstood about the challenges of fostering, particularly from friends and family members who were unfamiliar with this work. Karen complained: ‘… some people can be very judgemental about the problems you’re having …’
All participants identified respite as a critical resource that influenced their self-care as they had more time to themselves and fewer demands to meet. As would be expected, those who did not regularly receive respite reported more difficulty in making time for such activities. As Jennifer stated: ‘I do get that one day a fortnight where I don’t really do anything and that actually makes me a better carer.’
Lastly, financial resources were mentioned by just under half of the carers interviewed. Those with a disposable income felt they had more freedom and choice of self-care activities, such as paying to attend a gym or being able to go out for meals. However, those with limited finances found that their self-care activities were also limited. For example, when discussing things she would like to do, such as getting a massage or going out for dinner, Natalie stated: ‘… they’re just not things that fit in with my budget.’
Discussion
This study sought to explore foster carers’ perceptions and practices of self-care in the Australian context. The use of parallel quantitative and qualitative methods enabled the collection of rich data, which provides new insights into their self-care behaviours.
Perception of self-care
The findings indicate that foster carers have varying perceptions of self-care, but three aspects were consistently expressed by participants, namely, that self-care is essential, beneficial for reducing burnout and attrition, and conducive to providing better care. This finding is consistent with Miko, Berger and Krishnamoorthy’s (2022) study, in which carers identified self-care as contributing to better care provision.
Many of the participants in Miko and colleagues’ research valued intentional and planned self-care. However, carers in this present study reported that this was rarely possible. This is an important finding as previous research has concluded that the planning of breaks and personal time is a vital aspect of self-care (Cook-Cottone and Guyker, 2018) and that planned self-care can be a preventative measure for vicarious trauma in those caring for others (Salloum et al., 2015). This disconnect between the desire and ability to plan for self-care suggests that carers may need specific support to help them develop appropriate routines. This could be provided by professionals such as occupational therapists (Haugen and McNelly, 2020), while recreational therapists could enhance leisure activities and leisure literacy to improve carers’ health and wellbeing (Peel and Robinson, 2019).
The results of the current study also indicate that, overall, foster carers’ engagement in self-care practices is minimal. This finding is consistent with Miller and colleagues’ (2019) research, which found poor self-care engagement among foster carers in the US. These findings are concerning as regular engagement in self-care has been found to be essential for those in caring roles to provide care in a sustainable way (Richards, Campenni and Muse-Burke, 2010). Foster carers would clearly benefit from the incorporation of small amounts of regular self-care into their role as this would help guarantee their overall personal wellbeing and caring capacity.
In the current study, foster carers reported engaging in various self-care domains. Physical self-care behaviours, such as regularly drinking water and eating nutritious foods, were frequently mentioned, whereas regular exercise was much less common. This may be because drinking water and eating nutritious foods are heavily promoted to parents and are perceived as components of caring for a child. But this finding has been found for the general population where parents report similar barriers to exercise, such as family responsibilities, scheduling difficulties and paid employment (Mailey et al., 2014). Moving beyond the basic needs of food and water requires more encouragement from the community and institutional structures within carers’ lives to enable them to survive and flourish.
Carers in this study valued social self-care, with participants indicating they often engaged in intentional and meaningful social activities, such as connecting with friends and family. In these relationships, carers could communicate openly and find affirmation in their caring role when seeking the support they may not have been getting from elsewhere. These relationships demonstrate that carers find ways to cope within their support structures. This is unsurprising in view of previous studies of foster carers finding that social support is highly valued for promoting family resilience, individual coping skills and personal wellbeing (Adams, Hassett and Lumsden, 2018; Fuentes-Peláez et al., 2014).
Despite reporting high stress levels, carers indicated rarely engaging in mindful self-care practices that might reduce their perceived stress and benefit their overall wellbeing. Mindfulness is an aspect of self-care that has been found to help manage stress through improving emotional regulation, resilience and productivity (Cook-Cottone and Guyker, 2018; Keng, Smoski and Robins, 2011). Carers may benefit from more education highlighting the value and importance of mindful self-care for stress management. This could be provided in workshops, training sessions, online or via written resources.
Barriers
This study identified several barriers to carers engaging with self-care. There appeared to be a strong theme in which foster carers felt overwhelmed by the administrative and practical responsibilities of the role set by their care agencies. This finding is consistent with that of Miko, Berger and Krishnamoorthy (2022), where demands set by the foster carer agency were found to be time-consuming and thereby limiting for carers’ ability to practise self-care. This barrier warrants further investigation to ensure the administrative responsibilities of providing foster care to children are not unevenly distributed or overly burdensome on carers.
A key barrier discussed by foster carers was a lack of time availability, indicating that self-care is somewhat incompatible with the numerous responsibilities of their role. The results indicate that the needs and commitments of the foster children are a significant contributor to this. This finding again echoes Miko, Berger and Krishnamoorthy’s (2022) finding that the significant needs of the children in care were a barrier to carers’ self-care, particularly for those with placements involving disability or behavioural challenges. This finding is not surprising, with literature showing that many children in foster care have a history of complex trauma (Bridger, Binder and Kellezi, 2019), intellectual, learning or developmental disabilities (Murray, Tarren-Sweeney and France, 2011; NSW Ombudsman, 2004) and mental health issues (Murray, Tarren-Sweeney and France, 2011).
Carers in both the current study and Miko and colleagues’ research described having minimal time for their personal self-care as they prioritised the demands of other people. This commonly discussed phenomenon is present in the literature on mothering and parenting more broadly. It acknowledges selflessness as an expectation of parents, particularly mothers, and the pressure to prioritise their children over their own needs (Damaske, 2013; Malacrida and Boulton, 2012). This perception may be a deep-rooted societal expectation surrounding parents which negatively impacts their ability to practise self-care. The finding that foster carers also experience this supports the assertion that they perform the role of a parent rather than a paid carer (Blythe et al., 2013; Riggs, Augoustinos and Delfabbro, 2007). Through education, carers need to be empowered to take the time to engage in self-care as a priority in their caring role.
Notably, carers in both the current and Miko and colleagues’ studies felt unappreciated and thought that their self-care would be enhanced if the foster care agency provided more support. These findings echo those repeatedly presented in the foster care literature, where carers have described system-related challenges such as ongoing scrutiny of their care, intrusion into family matters, not being heard and a general sense of powerlessness in the parenting role (Blythe et al., 2013). The desired supports are tangible (e.g., access to formal respite services) and intangible (e.g., verbal affirmation that self-care is necessary and not an indulgence). This suggests that carers feel less able to practise self-care without these systemic supports and that there is a disconnect between carers’ needs and the resources and support provided to them.
Indeed, a lack of financial resources also contributed to time availability and opportunities for self-care and leisure among foster carers in the current study. This supports the findings of Miller and colleagues (2019), where carers with higher financial security were found to engage in more self-care than those who were just making ends meet. Researchers have established the negative impact that financial strain can have on the family unit’s health, wellbeing and functioning (Stack and Meredith, 2018; Taylor et al., 2017), and on the children themselves (Davis, Mantler and Doyle, 2004). Its impact on self-care was amplified in this study for sole carers in single-income households. This is congruent with research by Stack and Meredith (2018) who found that single parents have more significant stress and concern about their finances and therefore make greater sacrifices for their children, again an issue that agencies need to recognise.
Facilitators
Foster carers in the current study also discussed the facilitators of their self-care. It is clear from this study that social support from friends and family contributes significantly, expanding on the previous research that demonstrates that support from friends and family helps to alleviate the emotional strain intrinsic to the foster carer role (Murray, Tarren-Sweeney and France, 2011). Of concern, however, is the finding that some foster carers experience a loss of social support from friends and family who do not understand what fostering is about (Blythe et al., 2012). Whether this lack of support and subsequent difficulty engaging in self-care impacts foster carers’ wellbeing or attrition should be further investigated.
Previous research has demonstrated that foster carers value interaction with others as it reduces isolation and promotes a sense of belonging in their unique caregiving role (Blythe et al., 2012; Blythe, Wilkes and Halcomb, 2014; Murray, Tarren-Sweeney and France, 2011). This study builds on this finding by identifying that interaction within the foster care community enables individual carers to engage in self-care. Ways to create support circles and community among foster carers could, therefore, be fruitfully explored.
Foster carers’ partners were also identified as facilitators of self-care as they shared the responsibilities and challenges of the caring role. This is congruent with Miller and colleagues (2019) who found partnered carers engaged in higher self-care levels than sole ones. However, statistics indicate that an increasing number of foster carer households consist of sole carers (Qu, Lahausse and Carson, 2018; Siminski, Chalmers and McHugh, 2005), and ways to best support sole and partnered carers to engage in self-care need to be further explored.
Finally, formal respite was identified as an invaluable resource and facilitator of self-care. This has long been recognised as an important but under-resourced avenue to rejuvenate carers, thereby increasing their role satisfaction and ability to perform their task (Hudson and Levasseur, 2002; MacGregor et al., 2006; Murray, Tarren-Sweeney and France, 2011; Qu, Lahausse and Carson, 2018; Samrai, Beinart and Harper, 2011). However, it should be noted that some foster carers are not comfortable accessing respite services, even when available. This has been found in several studies where carers articulate concern that placing the children in respite services may cause them to feel unwanted or burdensome to carers (Hudson and Levasseur, 2002; Murray, Tarren-Sweeney and France, 2011). Most recently, Miko, Berger and Krishnamoorthy (2022) found that foster carers experienced guilt and selfishness if they took time to practise self-care. This reinforces the societal pressure for parents to prioritise their children’s needs over their own. However, what children need most are sensitive and responsive caregivers, something that is less likely to be consistently provided if the caregiver does not engage in regular self-care. Perhaps incorporating regular, planned respite care from the beginning of the foster care journey would help to shift this unhealthy societal norm.
Strengths and limitations
It is worth noting that this study was conducted within the context of the Covid-19 pandemic. Among the foster carer population specifically, the pandemic has created increased childcare issues, carer distress, fear and financial issues (Whitt-Woosley, Sprang and Eslinger, 2022), all of which create a greater need for regular self-care to maintain wellbeing (Miller and Grise-Owens, 2021). This should be considered when interpreting the findings.
This study is based on a small, self-selecting sample, and so the participants’ experiences may not wholly reflect those of the wider foster carer population. The sample also comprised 97% female participants; the experiences of male carers are therefore underrepresented. However, the findings reported are supported by literature from both the US (Miller et al., 2019) and Australia (Miko, Berger and Krishnamoorthy, 2022). Finally, the current study did not collect cultural/ethnic data from participants which prevents the exploration of any correlation between culture/ethnicity and self-care practices.
Implications for practice, policy and research
Foster carers would benefit from training that explicitly addresses self-care, emphasising its importance and offering ways to engage in it and creating effective individualised self-care routines. This would provide an opportunity to empower carers to prioritise their own health and wellbeing while setting a positive example for the children and young people they look after.
Foster carers would also gain from increased support and resources to engage in regular self-care. These should include the provision of respite. This is particularly important for sole carers and those with limited informal support. Similarly, carers should be given access to the broader foster carer community, in-person and virtually.
Due to the limited scope of the current study, future research topics could include the impact of stress on self-care, the impact of self-care on vicarious trauma and vice versa, wider social pressures surrounding parenting and mothering within the foster carer role and how this impacts self-care, and the self-care practices of male foster carers.
Conclusion
The current study explored the self-care practices of a small sample of foster carers in Australia. Foster carers are an essential part of the OOHC system, and their regular self-care engagement will help maintain their wellbeing and caregiving capacity. The results indicate that foster carers sometimes engage in self-care in various ways, and most consider self-care an essential preventative measure for burnout and carer attrition. Barriers to self-care include administrative and practical responsibilities of the foster carer role, a lack of agency support, the complex needs of the children and limited finances. However, self-care would be facilitated by social support, contact with other carers and respite. This study contributes to the emerging research on Australian and international foster carers’ self-care practices and suggests changes that can be made to educate and support carers to better engage in them in order to maintain both their own wellbeing and the quality of the care provided to the children.
Supplemental Material
sj-pdf-1-aaf-10.1177_03085759231178034 - Supplemental material for An exploration of the self-care practices of foster carers in Australia
Supplemental material, sj-pdf-1-aaf-10.1177_03085759231178034 for An exploration of the self-care practices of foster carers in Australia by Mia Gowan, Nicole Peel, Emma Elcombe and Stacy Blythe in Adoption & Fostering
Footnotes
Acknowledgements
The authors would like to extend their gratitude to the foster carers who gave their time to participate in this study and share their experiences.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.