
Abstract
Previous research has continuously identified a need for a comprehensive model of working with first mothers in adoption. This gap in knowledge has hindered the development of services, to the detriment of the quality of life and well-being of this group. This study seeks to remedy this deficiency by exploring the lived experiences of Irish mothers who have lost a child through closed adoption. It aims to expand understanding of the impact of such loss, in particular exploring how it affects their journey of reconnection and reunion with their child in adulthood. Semi-structured interviews were undertaken with six women from Ireland who had lost a child in this way and their narratives were analysed using Interpretative Phenomenological Analysis (IPA). Two superordinate themes emerged from the data: ‘Motherhood concealed: the loss of autonomy and connection’ and ‘Motherhood revealed: a pathway towards autonomy and reconnection’. Within each superordinate theme, two subordinate ones were identified: ‘Dehumanised, disempowered and dismissed’, ‘Coping through disconnection’, ‘Breaking the silence’ and ‘Reunion and reconnection’. The first two of these encapsulate the loss of personal autonomy and connectedness resulting from the loss of a child and how participants coped with it. The two others describe the participants’ experiences of growth in personal autonomy and agency through the process of breaking the silence of their concealed motherhood and of reconnection and reunification with their now adult children. The findings indicate that engaging in therapeutic services and/or with adoption peer support enables participants to express their feelings of grief and move from coping strategies dominated by disconnection to ones marked by the autonomous processing of emotion and new coping patterns. The process of reunification with their children plays a significant role in this transition.
Introduction
The loss of a child through closed adoption is a profoundly unique experience, often fraught with intense feelings of grief, loss, shame, guilt, remorse and isolation (Madden, et al., 2018). It often brings with it lifelong physical, psychological and social-interpersonal implications for those involved (Henney, et al., 2007). A prolonged and complicated grief reaction, exacerbated by its disenfranchised and ambiguous nature, is one such effect consistently reported in the literature (Coleman and Garratt, 2016; Madden, et al., 2016). While each first mother’s response is personal and individualised, a number of variables have been found to affect post-adoption adjustment. These include coercion (DeSimone, 1996; Madden, et al., 2016), availability of support (Krahn and Sullivan, 2015; Triseliotis, Feast and Kyle, 2005; Wiley and Baden, 2005) and later life events such as intimate relationships and parenting other children (Henney, et al., 2007; Krahn and Sullivan, 2015). The quality and amount of contact between a first mother and her adult adopted child several decades later may also be significant (Ge, et al., 2008; McRoy, et al., 2007).
The language of adoption
The language of adoption has changed over the past decades. In particular, the terminology used to describe the experiences of mothers who have lost a child through adoption has been subject to much debate. While terms such as ‘birth mother’ and ‘natural mother’ have been widely used, others view these as reductionist and stigmatising labels imposed by ignorant and insensitive professionals (Wilson, Lordan and Mullender, 2004). Similarly, terms such as ‘relinquishment’ and ‘placing’ in reference to closed adoption circumstances have been criticised for their failure to accurately represent the experiences of mothers who felt coerced into the decision (Wiley and Baden, 2005). After being consulted about the wording which they felt accurately reflected and respected their self-referencing choices, the women participating in this study suggested the terms ‘first mother’ and ‘mothers who have lost a child through closed adoption’ as most appropriate. Hence, the study will use these terms throughout.
Closed stranger adoption: the Irish context
Closed stranger adoption, sometimes called confidential adoption, is defined as circumstances where a child is adopted by a family unknown to his or her birth relatives, wherein no identifying information about the first parents or the adoptive parents is shared between the two parties and where there is no contact pre or post adoption (Coleman and Garratt, 2016).
Adoption in Ireland has a complex and controversial history. It was first legislated for in the 1952 Adoption Act. The Roman Catholic Church had a strong influence on the Irish state at that time and was able to enforce an almost unquestioned attitude towards and treatment of unmarried mothers (Wilson, Lordan and Mullender, 2004). Giving birth to a child outside of wedlock was viewed in society as unspeakably scandalous and such mothers were condemned as sinners and their children as tainted (Milotte, 1997). Adoption was therefore regarded as the ‘complete’ solution, shielding mothers from the social stigma and shame of pregnancy outside marriage and protecting the children from the stigma of ‘illegitimacy’ while also tending to the needs of couples unable to have children of their own (McCaughren and Lovett, 2014). Adoption practices for several decades were largely closed and characterised by secrecy. This social climate led to a peak of 97% of children born outside marriage being placed for adoption in 1967 (Adoption Authority of Ireland, 2012), and an average of one thousand closed adoptions per annum in the two decades that followed. Since then, a number of factors have contributed to significant change in adoption trends in Ireland, mainly the introduction of an ‘unmarried mothers’ payment in 1973 (Considine and Dukelow, 2009), the abolition of the status of illegitimacy in 1987 (Farren, 1998) and the Church’s waning influence on the state (Wilson, Lordan and Mullender, 2004).
More recently, a number of adoption scandals have emerged, leading to greater scrutiny of adoption practices in Church-run institutions and agencies (Department of Children, Equality, Disability, Integration and Youth, 2021). The discovery in 2018 of a mass grave and infant remains in a septic tank at the Tuam mother and baby home in County Galway highlighted the historical dehumanising nature of the Irish adoption system (BBC News, 2018). In addition, many first mothers who for decades had remained silent about their experiences have begun to express their frustration and distress at their treatment (Kelly, 2005; Redmond, et al., 2012).
While there is some evidence of change, existing tensions between the historical and current legislative bases of domestic adoption threaten the potential for progress (McCaughren and Lovett, 2014). The path to legislative change in respect of search and reunion, in the form of the Adoption Information and Tracing Bill 2016, has been particularly protracted. First introduced in 2001, the proposed Bill would have criminalised adopted people if they made direct contact with their first family members without their prior expressed permission (O’Brien and Mitra, 2018). Shelved in 2003 following successful lobbying by adoption organisations and finally published 14 years later in 2016, the Bill has still not been enacted. Adopted people’s right to their original birth certificates remains a contested issue.
Psychological adjustment and adoption loss
Central to the first mother’s loss of her child through closed adoption is the experience of disenfranchised grief, i.e. grief that is not openly acknowledged, socially validated or publicly mourned (Doka, 2008). The secrecy and stigma surrounding pregnancy outside marriage in Ireland served to intensify the grieving process and deny mothers recognition of their feelings and support from others (Cowie, 2011; Davidson, 2010; DeSimone, 1996). At the same time, their child – although physically absent – remains psychologically present, not only on significant milestones but also in everyday life (Boss, 1999; Fravel, McRoy and Grotevant, 2000). Using the concept of ambiguous loss, Boss (1999; 2007) argues that this is among the most stressful types of loss due to the lack of official confirmation and rituals of support and failed resolution (Boss, 2016). As a result, the individual is often isolated and left to cope alone, caught between states of hope and despair with enduring grief that is at risk of being pathologised (Boss, 1999, 2006, 2007).
The grief reactions of first mothers described in the literature comprise a mixture of physical, psychological and social-interpersonal reactions (Henney, et al., 2007). The psychological responses, which are often suppressed, include feelings of shame, guilt, anger, sadness, remorse and regret (Kelly, 2005; Namerow, Kalmuss and Cushman, 1997; Triseliotis, Feast and Kyle, 2005). These may manifest as symptoms of anxiety and depression, substance dependency, diminished self-esteem, somatic symptoms, secondary infertility and post-traumatic stress disorder (Andrews, 2009; Bouchier, Lambert and Triseliotis, 1991; Brodzinsky, 1990; Christian, et al., 1997; Deykin, Campbell and Patti, 1984; Fessler, 2006; Jones, 1993; Kavanagh, 2015; Sorosky, Baran and Pannor, 1978). Factors associated with psychological distress include feeling coerced into the adoption decision, lack of support from families and professionals, limited opportunities to talk about experiences, suppression of emotion and negative search and reunion outcomes, (Cushman, Kalmuss and Namerow, 1997; De Simone, 1996; Logan, 1996). Social relationships are also affected, including first mothers’ relationships with parents, peers, partners and additional children (Rynearson, 1982). In particular, they report establishing impossibly high standards of parenting and overprotectiveness of additional children with a reluctance to encourage their move to independence (Howe, Sawbridge and Hinings, 1992).
A key question arising from this situation is whether this grief is likely to resolve and if so, under what circumstances. Although the disenfranchised and ambiguous nature of the loss is likely to complicate recovery (Lauderdale and Boyle, 1994; Weinreb and Konstam, 1995), a qualitative study by Kane (2018) suggests that healthy grieving is possible for first mothers if they are given an opportunity to share their experiences in their entirety, and have their experiences acknowledged and their feelings validated. More specifically, the process of reunification and reconnection with the adopted child in adulthood is especially significant. First mothers who have accepted or initiated contact describe a sense of relief from learning about their child’s circumstances (Kelly, 2005; March, 2014) and stress that they would still have initiated and accepted contact regardless of the outcome (Silverman, et al., 1988). Key benefits identified in the study by Triseliotis and colleagues (2005) included diminished feelings of guilt, sadness, grief and confusion as well as increased self-esteem and improved emotional outlook. In addition, the mothers who searched were more likely to have experienced counselling and/or to have been involved in adoption support groups than those who did not (Affleck and Steed, 2001; Triseliotis, Feast and Kyle, 2005). Hence, regardless of the outcome, contact usually helps the first mother by providing emotional healing and a sense of relief in knowing about her child’s life circumstances.
Method
Design and ethical approval
Semi-structured interviews were undertaken with six mothers who had lost a child through the process of closed adoption. An Interpretative Phenomenological Analysis (IPA) framework was used to analyse the information (Pietkiewicz and Smith, 2014; Smith, Flowers and Larkin, 2009). This gives central importance to the individual meaning ascribed to salient experiences (Smith and Rhodes, 2015) and requires the researcher to make sense of the responses of each participant who, in turn, is trying to make sense of him- or herself (Osborn and Smith, 2008). Because of the sensitivity of the evidence, extensive data protection safeguards were applied and ethical approval was given by the Research Ethics Committee, National University of Ireland, Galway.
Selection and characteristics of participants
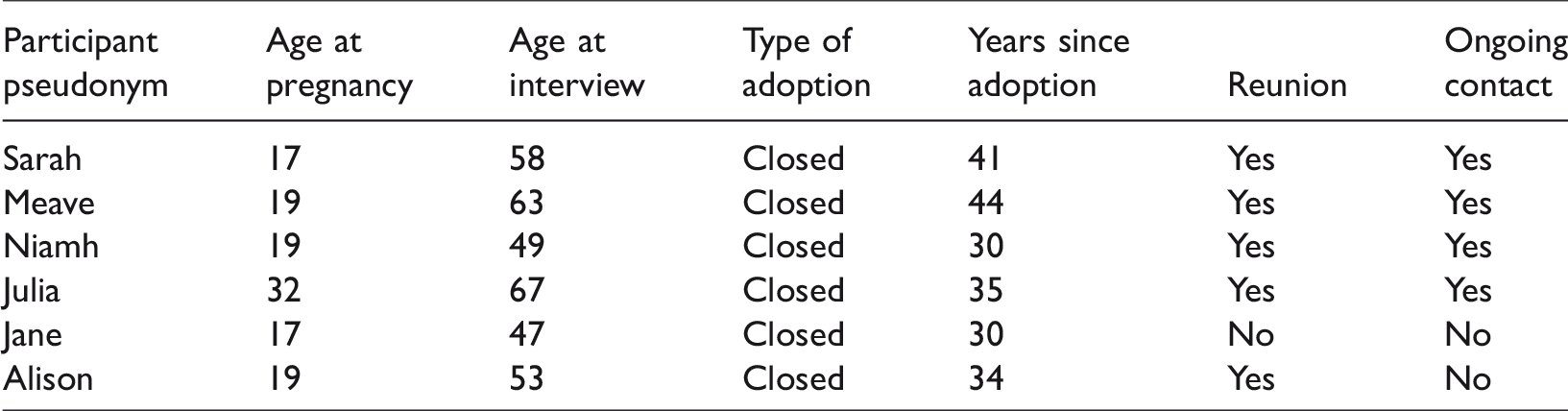
IPA’s commitment to idiographic inquiry encourages the study of small, purposively selected and reasonably homogeneous samples (Charlick, et al., 2016). In keeping with these guidelines, six mothers who had experienced the loss of a child through closed adoption agreed to participate. They were aged between 47 and 67 years (M = 56 years) at the time of interview and the length of time since the adoption ranged from 30 to 44 years. Participants were aged between 17 and 32 (M = 20.5 years) at the time of the adoption. Five women had searched for their child in adulthood and one had been searched for. Five had experienced reunion meetings, four of whom remained in contact with their child. Demographic details are presented in Table 1.
Demographic details of participants.
Results
The IPA analysis identified two superordinate themes ‘Motherhood concealed: the loss of autonomy and connection’ and ‘Motherhood revealed: a pathway towards autonomy and reconnection’. Within each of these, two subordinate themes were developed: ‘Dehumanised, disempowered and dismissed’, ‘Coping through disconnection’, ‘Breaking the silence’ and ‘Reunion and reconnection’. They will now be discussed in detail.
Motherhood concealed: the loss of autonomy and connection
This superordinate theme encapsulates the loss of personal autonomy and connectedness imposed on participants through their experience of losing a child through closed adoption.
Dehumanised, disempowered and dismissed
This sub-theme illustrates the loss of personal autonomy and connection described by all six participants. It occurred against a cultural backdrop of secrecy and shame that surrounded single motherhood at that time; this helps to explain the mothers’ feelings of being ‘dehumanised, disempowered and dismissed’ by their families and the professionals they encountered. Their fate and that of their infants were decided without their involvement, acknowledgment of their wishes or consideration of their emotional needs.
This dehumanising experience is captured in Niamh’s account: You gave birth. You wouldn’t do it to a dog. Pull the child away from their mother within days of the birth and hand it over and expect the mother to hand it over. Say, ‘Have a nice life, go away and don’t talk about that ever again because you’re just a horrible human.’ You know like it was unnatural.
Sarah also chose an animal metaphor to conceptualise her experience of dehumanisation: I became a prime target of examinations with the end result I’m breaking down one day and saying, ‘Ye have to stop. You just have to stop.’ The door to the room never stopped… this trail of doctors. And I know they had to learn but I felt like a guinea pig. That’s something I said, you know, somebody will have to answer for that. I was totally traumatised.
Within the context of their families, five of the six participants spoke of being excluded from the planning and decision-making process about their fate. Their passivity and lack of agency over their own lives are epitomised in their attempts to exert control over the fate of their infant. The theme of disempowerment represents these experiences and is demonstrated in Jane’s account: I rang my mother to tell her I wanted to keep him you know. And she just… she just says, ‘Well, you needn’t expect to be getting any support at home here.’ And I thought ‘Aw.’ And I says, ‘Well, maybe I could keep him over here?’ Oh yeah. And what will all the relatives say over there? You know. And I hung up on her. And she rang back and by Jesus did she tell me don’t under any circumstances hang up on her again. You know it was just… it was so hostile.
This theme of dehumanisation and disempowerment dominated the narratives of five of the mothers and many shocking examples were given: giving birth alone, indifference to physical symptoms, denial of pain relief and general disdain for their situation. The one exception was Jane who described a very different experience of maternity care characterised by compassion and support. She credits the kindness shown to her and feels that memories of precious time spent with her son were integral to coping with the pain of losing him in the years that followed: … the nurses would be encouraging. They’d be saying don’t be afraid to talk to him now and you know. And they were brilliant. Like the nurses in intensive care with the babies are just gorgeous you know, and you and you can tell they love the babies like you know. It was lovely.
Coping through disconnection
In response to the trauma of being faced with losing their babies, the mothers described coping through different forms of disconnection, such as dissociation, thought suppression and repressed memories. Meave describes the unconscious process of coping through dissociation: There was an awful lot I didn’t know about life. I’d like to have died but I didn’t know how. So, I just wasn’t there. I just wasn’t present. It was all happening to somebody else.
The second coping strategy described was suppression – the conscious and deliberate attempt to suppress distressing thoughts and feelings. Jane’s account illustrates this experience: When I signed the final papers. Ummm…. I remember consciously thinking. It was nearly as if I put a gate up. And it was like I just couldn’t cope with it. I just shut… I think… I believe now I shut down, you know. I didn’t know it at the time. But completely shut down.
The conscious process of suppressing unwanted thoughts, memories and feelings is echoed by Julia’s pithy comment: ‘I trained myself. I actually learned not to think, not to remember painful things.’
The third coping strategy, memory suppression, refers to the unconscious forgetting or blocking of distressing memories and is a symptom of dissociation. All of the participants reported occasions where they were unable to recall aspects of their experience. As Sarah explains: That’s all such a blank to me. It’s in and out you know. There’s no solid stuff. It’s like a jigsaw and you’re picking out the pieces and you’re trying to fit it in.
For others, the desire to recall repressed memories conflicts with concerns about the impact of remembering. Alison expresses her reservations about having a complete memory of her experiences: I’d want to be hypnotised sometimes and go back and just remember literally every little thing. But then I think that would put me daft in the head.
Motherhood revealed: a pathway towards autonomy and reconnection
The second superordinate theme relates to a more recent period in the lives of the mothers and explores the journey towards regaining autonomy and connection through the process of search and reunion.
Breaking the silence
This subordinate theme details the participants’ journeys towards regaining a sense of autonomy over their experience through the process of breaking the silence of their concealed motherhood. Five of the women reported attending professional counselling or psychotherapeutic services. Although the catalyst for opting for therapy varied, the opportunity to speak about their experiences facilitated the process of regaining autonomy and reconnecting with their child.
Following years of coping through dissociation, suppression and repression, the mothers identified the life-changing effects of the support they received as it explained their pain as acknowledged grief and gave them space to express it. Sarah describes this as early as in her first session with her therapist: He named it. He says, ‘You’ve been grieving.’ I thought somebody had to die for you to grieve. I didn’t understand it, you know, until he said it. It was like somebody lifted tonnes off me. I remember just crying because I didn’t know. I just didn’t know what it was.
While Sarah used the analogy of lifting a weight, Jane describes the powerful stream of emotion that flowed when she allowed the ‘trapped’ emotions out. The key to this was again reframing the experience as one of grief. The safety of the therapeutic space allowed her to engage with the ‘scary’ place occupied by her concealed motherhood. She became an active participant and regained autonomy over her experience.
In addition to accessing therapeutic support, all participants sought help from adoption networks. This contribution was trusted and useful in the search for and reunification with their adult children. As Jane says: I never, ever tried to look for him because I never felt I had a right to. And then at the birth mothers’ group, you know, they were saying, ‘Well, would you not?’ You know and I was… My mindset began to change and it was like, God, maybe he’ll think I don’t care if I don’t actively look to make contact. In the whole of the adoption network I was contacted by somebody who said, ‘We don’t say this to everybody but we know you’re somebody… you know who would have the intelligence and the patience to not cause any trouble. Okay. So, we’re going to tell you how you locate your daughter.’
The move from passivity to activity also promotes feelings of power to influence the system. Niamh describes how she planned and exerted control to get the information she wanted: I was really manipulative in how I approached it. And I spoke around what do you want and how do you want it and all the rest of it, and I just worked. I teased the whole thing through until I got the date of the adoption order. That’s all I wanted and once I had that I knew I would have my son’s identity within 24 hours.
Reunion and reconnection
This subordinate theme extends mothers’ experiences of growth in personal autonomy and agency by scrutinising the subsequent reunification and reconnection with their now adult children. Their experience was one of catharsis, reintegration and healing. Five participants had reunited with their adopted child and all described it as enormously positive. Julia recalled meeting her adult son for the first time: I was shaking like a leaf and next thing I seen him coming towards me and a big, big smiling face. And that memory will stay with me forever. If everything goes belly up that moment will just stay with me forever. It was just the most fantastic moment of my life. You know what I had to do at the beginning was you have to go back because they are not the child anymore so the adult, and you have to work backwards. You’ve to come back through all the years of you know and work it that way. And when you get from the adult to the baby, then go from the baby up. And it’s amazing what you learn in that whole journey.
Four of the five participants who had a reunion maintained a positive and relatively stable relationship with their adopted child and all spoke about the need for negotiation to maintain the post-reunion relationship. As Niamh explains: I would have said to him, ‘You really need to decide what it is you want and what it is you expect. I can’t do that. And if you need time to do that, that’s okay. I’m going nowhere like. I’m here. It’s okay.’ Do you know that sort of way? So, I do try and give space if it’s needed or whatever. But I’m not going to mollycoddle either. I’m not going to be. I’m not going to be a doormat just for…You know so it’s a matter of trying to get that balance really.
However, not all participants’ experiences of negotiating the relationship were similar to Niamh’s as some highlighted the power dynamic within the relationship as particularly challenging. This was Alison’s experience: To be honest with you, anyone, we’ve always said this, anyone that’s adopted holds the reins. You know they are the boss in the relationship you know. You can’t make them be in your life if they don’t want to be.
Meave was more accepting of the power relationship than the others and explained to her counsellor: He said to me, ‘How do you cope with, you know, her rules and not showing up, and how do you cope with not having as much as you want?’. I said to him, ‘I think what you don’t understand is that every second that she gives me is a gift. I mean it’s a gift. You know years and years of not knowing whether she is dead or alive…’
While the study succeeded in identifying several common themes, it is important to highlight the different journey experienced by Jane. Her son died before she could reconnect with him. This led to a process of disconnection which contrasts with the experience of reintegration described by the other mothers. She reflects on the impact of losing her son for a second time: Everything else is going on as normal and I felt like my whole life had crumbled. As I said, really devastated. I believe I shut down again because I know I’d have been ringing the kids every week, you know, and I couldn’t ring them. I even feel that a bit, even yet. It’s like I can’t fully connect.
Discussion
This study has explored the subjective experiences of six Irish first mothers who lost a child through closed adoption many years ago. To the authors' knowledge, this is the first IPA study of Irish mothers in such circumstances. The two superordinate themes ‘Motherhood concealed: the loss of autonomy and connection’ and ‘Motherhood revealed: a pathway towards autonomy and reconnection’ and four subordinate ones emerged and these will now be organised into a theoretical framework to extend the current understanding of loss and its effects.
Dehumanised, disempowered, and dismissed
The participants’ narratives point to an experience of adoption as disempowering and often dehumanising. Many cited instances of being dismissed as human beings by their families and the professionals whom they encountered. Several earlier qualitative studies of first mothers involved in closed adoptions report similar findings (Jones, 2004; Lauderdale and Boyle, 1994; Lewis, 1983; Logan, 1996; Rynearson, 1982; Weinreb and Konstam, 1995). The powerlessness of the mother’s position was further reinforced by her exclusion from decision-making about her fate and the future of her baby. This was often imposed by family members, particularly mothers, through their denial of the first mother as a primary stakeholder in her child’s life. These findings reflect the punitive attitudes surrounding single motherhood in Ireland at that time, as well as the existence of powerful pressures to accept decisions in favour of adoption (Howe, Sawbridge and Hinings, 1992; Kelly, 2005).
Coping through disconnection
As in earlier qualitative studies (Davis, 1994; Jones, 2004; Lauderdale and Boyle, 1994; Lewis, 1983; Rynearson, 1982), those taking part in this research described to varying degrees coping with the loss of their child through dissociation, suppression and repression. Rooted in a prolonged and complex grief reaction, these coping mechanisms begin in pregnancy and extend in many cases beyond the decision to search. The finding that dissociation is a key coping response to participants’ psychological trauma is of particular significance as it validates findings of raised post-traumatic stress disorder symptoms among first mothers (Kavanagh, 2015; Kenny, et al., 2012).
Breaking the silence
All of the mothers reported experiencing disenfranchised grief. Counselling, psychotherapeutic work and/or involvement with adoption support groups gave them an opportunity to express their grief in a socially acceptable manner, to grieve openly and have it acknowledged and accepted by others in an empathic and caring setting. These findings support earlier research (Brodzinsky and Smith, 2014) indicating that first mothers can begin to recover from their loss if there is support that facilitates the full expression of the experience, validates emotional feelings and acknowledges the loss (Kane, 2018). All participants who had engaged with therapeutic services and/or adoption support networks played an active role in searching for their child, a finding replicating other studies exploring first mother search and reunion contact (Affleck and Steed, 2001; Triseliotis, Feast and Kyle, 2005).
Reunion and reconnection
For all participants, the process of reuniting with their now adult child involved losses as well as gains. For many, there was a significant shift from previous coping strategies marked by suppression and repression to more autonomous processing of emotions, both before and after the reunion. All of those who had met their adult child describe it as a positive experience, regardless of the outcome, echoing findings from earlier research that revealed mothers’ feelings of elation and relief from initiating or accepting contact (Farrar, 2005; Kane, 2018; Silverman, et al., 1988). But things did not always run smoothly. The mothers found that the post-union relationship required considerable negotiation as they sought to determine and meet mutual expectations. Most accepted the boundaries as laid down by the adopted adult to ensure continued contact; however, for some there was an underlying fear that they could lose them again. As March (2014, 2015) has shown, reunification requires a psychological adjustment in facing the reality of meeting an adult unknown to them rather than being reunited with the baby whom they had been forced to leave behind.
Limitations
This exploration of first mother loss through closed adoption within an Irish context is innovative in both its qualitative methodology and in isolating this particular experience from other forms of adoption. However, the sampling strategy limited participants to those engaged with adoption support groups and who wished to reconnect with their child. The analysis also relied on retrospective recall of mothers’ experiences some 30 and 45 years ago.
Implications for practice
As adoption practice changes worldwide, this study offers research findings and practice recommendations to those working with first mothers who have lost their child to closed adoption. It shows that many were deprived of emotional support and experienced secrecy, silence and stigmatisation at a hugely significant time in their lives and how the effects of this can be long lasting, with recovery occurring many years later, usually around the time they contemplate or begin to search for their child. The findings also indicate that to effectively grieve their loss, mothers require understanding, validation and support that is well informed and sensitive to what happened. In particular, practice guidelines need to incorporate the features known to promote the core values of respect, trustworthiness, accountability, fairness, equity, honesty, truthfulness and autonomy, and to recognise that the openness required extends beyond contact and information exchange to include non-judgemental respect, trust and compassion. As mothers are likely to have experienced harsh and often cruel treatment, this might colour their attitudes and responses to services provided.
Finally, the value of therapeutic support where first mothers can meet others in a safe location and receive authentic empathy and validation is testified in all the narratives. All the participants stressed that finding mutuality in their experience helped to normalise their feelings and reduce senses of isolation.
Major gaps continue to exist in many countries in relation to assisting people with search and reunion. This study highlights the complexities of accessing information and searching for adopted children. Information is often closely controlled by adoption agencies and, in some instances, social workers. Legislative change to address this issue should therefore be encouraged. Statutory rights for adopted persons and first parents to have unfettered access to their adoption records and birth certificates has been the case in Scotland and the UK since 1930 and 1975 respectively.
Conclusion
This study extends knowledge and understanding of the lived experiences of first mothers who have lost a child through closed adoption. The findings suggest that recovery from feelings of loss and grief is possible but typically occurs many years later, around the time when the first mother begins to contemplate or starts searching for her child. The findings also indicate that to effectively grieve their loss, the mothers require understanding, validation and formal support networks, together with personal therapy and group interventions that are well informed and sensitive to closed adoption issues.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.