
Abstract
Campaigns for personal health expenses make up the largest and fastest-growing segment of donation-based crowdfunding. Set against the backdrop of retrenchment and disinvestment in public healthcare systems across the global North, health-related crowdfunding is a way to navigate increasingly marketised systems of social reproduction. Despite high profile success stories, campaigns vary significantly in their ability to capture the hearts, and ultimately wallets, of donors. While existing analyses of online campaign pages offer some insight into the marketing of healthcare needs, far less is known about practices and experiences of crowdfunding platform users, including campaigners. Bringing literature on crowdfunding together with accounts of the marketisation of care, our paper asks: how do campaigners work to secure crowdfunded healthcare? Through the accounts of 15 people campaigning on behalf of family or friends in Aotearoa New Zealand, we show how attempts to appeal to donors depend on campaigners’ abilities to ‘market’ illness and need in ways that resonate with the crowd. We have two main foci. First, we examine the responsibility and responsibilisation of campaigners to engage and perform accountability to crowdfunders. Second, we show how campaigners mobilise recipients’ traits of deservingness and other culturally favoured personal qualities to appeal to the crowd's perceived predilections. In sum, the paper demonstrates how the use of crowdfunding is both necessitated by the marketisation of healthcare while simultaneously exerting its own form of market discipline.
Introduction
‘Tough guy faces hardest battle yet’ is the title of Levi Holley's crowdfunding campaign. Following a shock diagnosis with inoperable brain cancer in mid-2019, he has become, according to the campaign web page, a ‘man [whose] sole purpose is to survive’. As a ‘normally healthy, fitness and sports minded 44 year old’, Levi has always ‘given his time and skills away freely’ by being ‘a regular at charity events, fundraising for a number of organizations and more recently sponsoring amateur athletes’. In light of his commitment to the community, Hannah, Levi's best friend, caregiver, and now crowdfunding campaign manager, appeals to readers: ‘it's time for us to come together and help this amazing man out’.
Levi's campaign is but a drop in the ocean of health-related crowdfunding appeals. As a growing practice internationally, personal health-related fundraising makes up the largest and fastest-growing subset of donation-based crowdfunding. On GoFundMe, the world's largest donation-based crowdfunding platform, personal health-related campaigns now comprise the largest category. This global trend is reflected in Givealittle, Aotearoa New Zealand's largest and only dedicated donation-based crowdfunding platform. However, there are wide variations between campaigns’ abilities to capture the hearts, and ultimately wallets, of ‘the crowd’ (a term encompassing an amorphous group of friends, acquaintances and strangers). As emerging literature attests (Berliner and Kenworthy, 2017; Dressler and Kelly, 2018), the growth of health-related crowdfunding stems from structural inequalities and resulting forms of lived precarity. But crowdfunding also appears to amplify conditions of socio-economic inequality and precarity. As we will go on to show, crowdfunding introduces additional axes of inequity which result from the campaigners’ capabilities and advertising savvy, the disposable incomes of those within one's potential donor network, and the ability of particular illnesses and bodies to elicit care from others. As health-related crowdfunding grows, the little-understood practice of crowdfund campaigning is increasingly critical to matters of life and death on an individual level, and to the wider patterning of social reproduction.
Our paper asks: how do campaigners work to secure crowdfunded healthcare? By exploring 15 campaigns on Givealittle, we show how attempts to appeal to donors depend on campaigners’ abilities to ‘market’ illness and need in ways that resonate with the crowd. Semi-structured interviews with the manager of each campaign, and analysis of their campaign web page, provided insights into their perceptions, experiences and practices through the crowdfunding process. We attend, in particular, to the way crowdfunding exerts market discipline through the need for campaigners to frame and promote – or, in other words, market – recipients’ need to potential donors. 1 While donation-based crowdfunding might not immediately appear to resemble ‘the market’, its organisational form (i.e. a decentralised mechanism for exchange and allocation of goods/services) and participant-subjectivities are exceedingly market-like.
After providing an overview of health-related crowdfunding, we turn to the literature on the marketisation of care as one means to grapple with the market-like dimensions of this ostensibly altruistic practice. Then, turning to our empirical material, we focus on the ways that campaigners: (1) compete for the crowd's attention, (2) align the recipient with the crowd's apparent understandings of deservingness and (3) perform accountability to the crowd. In sum, the paper brings to light the effort, skills and traits involved in the use of crowdfunding as a survival strategy amid a more general trend towards the marketisation of care and, by extension, social reproduction. 2 Beyond affirming another frontier for the marketisation of social reproduction, our particular contribution lies in teasing out the marketing practices and marketised subjectivities that animate and enable crowdfunding specifically, and marketised social reproduction in general. In a shift from bureaucratised conditions of healthcare eligibility (which are not without their own inequities), we show how burdens of time, effort and emotion land squarely on crowdfunding recipients, and those campaigning on their behalf, to respond entrepreneurially at times of heightened precarity, offering up their personal challenges to the public in hope of financial benevolence.
Crowdfunding healthcare: Promise and pitfalls
Crowdfunding campaigns involve an open call for funding from the online ‘crowd’ in order to pool the resources necessary for individual or organisational initiatives (Doan and Toledano, 2018; Gonzales et al., 2018; Gray and Zhang, 2017). The umbrella term ‘crowdfunding’ subsumes different types of activities with disparate market sizes. Scholars frequently distinguish between three different models, namely investment-, reward- and donation-based crowdfunding (Galuszka and Brzozowska, 2017; Gray and Zhang, 2017; Kromidha and Robson, 2016; Langley, 2016). The two former provide tangible returns for donors, while donation-based crowdfunding involves the provision of funds without tangible returns. Such campaigns are typically initiated for ‘good causes’, ranging from funding community projects to financing household expenses (Kromidha and Robson, 2016; Stiver et al., 2015).
Across the healthcare sector, crowdfunding campaigns have been mobilised to fund commercial health innovation and research, or to fundraise for health-related organisations (Renwick and Mossialos, 2017; Young and Scheinberg, 2017). At the individual level, however, crowdfunding is increasingly used to cover personal health expenses; this having become ubiquitous on donation-based platforms. Scholars across various social-scientific fields, particularly media studies and health sciences, have begun to explore the nature and implications of this nascent phenomenon (Barcelos, 2020; Berliner and Kenworthy, 2017; Palad and Snyder, 2019; Paulus and Roberts, 2018; van Duynhoven et al., 2019).
Existing research suggests that health-related crowdfunding holds some potential in generating financial and social support for its users, particularly those who are well-networked through social media. For example, drawing on campaigners’ and recipients’ existing (and especially affluent) networks, successful campaigns can provide ‘interim financial relief’ and comradery during times of hardship (Fritz and Gonzales, 2018; Gonzales et al., 2018; Renwick and Mossialos, 2017; Snyder et al., 2016; van Duynhoven et al., 2019). However, regardless of their socially networked base, campaigners must market their illness to attract funding, a process that is inflected with the skills, traits and resources of the campaigner and/or recipient. Those in genuine medical need may be overlooked by the crowd as they have not narrated their illness in a way that is coherent with cultural norms of ‘deservingness’ (Berliner and Kenworthy, 2017; Brabham, 2017). Successful campaigners tend to frame their challenges in a ‘culturally coherent manner’ (Paulus and Roberts, 2018: 65), which requires medical, cultural and social media literacies in addition to the time necessary to establish and maintain the campaign (Gonzales et al., 2018; Snyder et al., 2016).
The need to effectively market one's illness has implications for which kinds of healthcare treatments are successful in a crowdfunding context. As Snyder et al. (2016) explain, the most marketable illnesses are those that are seemingly ‘solvable’, arising from ‘unexpected’ circumstances. The imperative to neatly package and clearly communicate one's predicament disadvantages those with compounding challenges or those with stigmatised health needs (Berliner and Kenworthy, 2017). For example, crowdfunding websites for addiction-related services are largely unsuccessful in financial terms (Palad and Snyder, 2019). Rather, crowdfunding is likely to best serve people deemed to be ‘deserving’ recipients, as well as people with ‘palatable’ health needs. As crowdfunding healthcare becomes normalised, it is likely to further marginalise already-vulnerable groups.
Literature on health-related crowdfunding thus highlights some of the challenges associated with this nascent phenomenon. Despite the salience of these challenges, however, health-related crowdfunding is still relatively under-studied and under-theorised, as many scholars have identified (Berliner and Kenworthy, 2017; Paulus and Roberts, 2018; Renwick and Mossialos, 2017; Snyder et al., 2016; Young and Scheinberg, 2017). As Berliner and Kenworthy (2017) highlight, there is limited research that engages face-to-face with users of these platforms. With the exception of three recent studies (Fritz and Gonzales, 2018; Gonzales et al., 2018; Kneese, 2018), existing scholarly work in this area consists of literature reviews, commentary or content analysis of online campaigns and media coverage. This paper seeks to fill this gap by going beyond the marketing texts to examine, through interviews, the marketing practices of campaigners labouring to secure care on behalf of others. In framing our discussion of health-related crowdfunding, we now engage with accounts of marketised care.
Marketised care
Marketisation processes – privatisation, corporatisation, commodification, competition – have profoundly shaped how relations of care are organised, experienced and understood. In this paper, we examine the emerging use of crowdfunding platforms for health-related costs as a manifestation of marketised care. Once overlooked as a private and ‘pre-political’ concern, there has been increased recognition of the social, political and economic salience of care within social-scientific scholarship of recent decades (Green and Lawson, 2011; Parr and Philo, 2003; Robinson, 2011). Crucial to these developments has been the use of ‘care ethics’ as a theoretical framework. While initially proposed as a moral theory, care ethics has become influential across a range of disciplines as a way of understanding how interdependence and relations of responsibility permeate social and political life (Brown, 2003; Robinson, 2018; Tronto, 1993). The marketisation of care has been a central theme in the care ethics literature, with scholars examining the nature and consequences of care entering the market across a range of contexts. From the rise of commercial childcare (Boyer et al., 2013; Gallagher, 2018; Schwiter, 2013) to home-based elderly care work (Pelzelmayer, 2018; Schwiter et al., 2013; Stolt and Winblad, 2009), accounts have identified the emergence of new marketplaces for care, as well as instances where existing spheres, such as the home, are transformed into marketised spaces (Pelzelmayer, 2018).
Pragmatic critiques have been levelled at the marketisation of care. The atomistic understanding of human nature that market rhetoric promotes may serve to undermine relational approaches to care (Held, 2002; Hoppania and Vaittinen, 2015; Tronto, 2013). Scholars have also raised concerns about the ways in which emphasising the rights and responsibilities of individuals to self-determine their own care may serve to undermine collective models (Boyer et al., 2013; Green and Lawson, 2011; Schwiter, 2013). For instance, Hall (2011) examines the restructuring of care provision for people with learning disabilities through his case study of ‘Personal Budgets’ in the United Kingdom, which shifted the management of care funding from local governments to the individual. Hall argues that emphasising individual autonomy diminished funding for community-based care services; services that, in many cases, provide indispensable support and solidarity for its users (Hall, 2011). In this sense, while a ‘market logic of choice’ can maximise individual autonomy in seeking care (Green and Lawson, 2011; Schwiter, 2013), models informed by this logic may fragment collective structures of care provision.
Furthermore, the marketisation of care has been critiqued for exacerbating inequalities in access to care. The logic of choice conceptualises the market as ‘flat’, with individuals ‘free’ to make their own decisions (Green and Lawson, 2011; Tronto, 2013); however, such an understanding of the market overlooks historical injustices and social inequities that shape individual ‘choice’. By conceptualising individuals as autonomous while simultaneously emphasising personal responsibility, neoliberal discourse permits widening inequalities in access to resources, by individualising what are, in fact, structural challenges (Cox, 2013b; Hall, 2011; Schwiter, 2013). Framing care as a transaction therefore permits situating those who have limited resources ‘outside the social and hence beyond the scope of obligation’ (Green and Lawson, 2011: 651).
Despite the significant critique of market processes, some scholars have challenged the notion that market values necessarily ‘corrupt’ care and lead to undesirable outcomes. Some scholars have argued that the assignment of monetary value to caring services is not, in itself, objectionable. As Cox (2013a: 494) argues, ‘[t]here is much evidence that paid-for care is often deeply caring’. Indeed, the binary framing of marketised care as problematic and non-marketised care as unproblematic overlooks the complexity of lived caring experiences (Boyer et al., 2013; Cox, 2013a; Pelzelmayer, 2018). For instance, this dualism is complicated by evidence of paid caregivers who express ‘heart-felt love’ for their care-recipients (e.g. Pelzelmayer, 2018). Equally, care that is non-commodified is not necessarily ‘uncorrupted’, ‘pure’ or apolitical; as is shown in Muehlabach’s (2012) study in Italy, which draws attention to the alignment of Catholic notions of compassion and charity with neoliberal moral logics, amidst surging trends of volunteerism in Italy, that were in turn necessitated by state welfare retreat. Expectations of volunteer or unwaged socially reproductive labour are also unevenly distributed across gender, race and class categories (Cox, 2013a). Furthermore, some scholars have raised concerns that critiquing the marketisation of care may simply reinforce the devaluation and underpayment of waged caring labour (Held, 2002; Pelzelmayer, 2018). For this reason, Cox (2013a: 494) among others argue that ‘payment itself is not the problem, but the context and organisation of commoditised care can be highly problematic’.
Empirical examinations of marketisation processes within the care literature have largely focused on the shift from unpaid to paid caring labour, with a consequent emphasis on care-giving practices (for exceptions, see discussions on commodification and consumption practices, e.g. Barnett et al., 2005; Goodman and Boyd, 2011; Popke, 2006). In contrast, our paper looks at how campaigners work to meet their recipients’ immediate financial needs, critically evaluating the process of how recipients are deemed (by the crowd) as worthy enough to be taken care of in the first place. We demonstrate how market values influence how justifications are made for being deserving of care. As such, and answering the call of Green and Lawson (2011: 650), we seek to better understand the relationship between marketised care and the marketisation of the care recipient. Crowdfunding provides an apt lens for examining these relations. Crowdfunding practices function through established patterns for socially reproductive care labour (e.g. kin network, friendships, local communities) while also moving beyond them and into the public sphere. As we have described, literature on care has made valuable contributions to mapping out the shift of certain forms of care from one sphere into the other – or shown how they combine in complex and sometimes paradoxical ways. Our research demonstrates how formal and informal, public and private practices are enmeshed in the contemporary phenomena of online health crowdfunding.
Research context
The national health system of Aotearoa New Zealand is widely understood to provide a high standard of care by international standards (Goodyear-Smith and Ashton, 2019). Following the establishment of the Social Security Act of 1938, Aotearoa New Zealand was one of the first in the world to develop a universal, tax-funded health service (Gauld, 2013; Goodyear-Smith and Ashton, 2019). The nation became infamous in the 1980s for its extensive and rapid adoption of neoliberal policy prescriptions – known as the ‘New Zealand experiment’ – mirroring that of structural adjustment programmes implemented in the global South (Kelsey, 2015; Larner, 1997; Prince et al., 2006). In spite of the ubiquity of neoliberalism in the Aotearoa context, healthcare has remained relatively sheltered from, or resistant to, neoliberal reform compared to other domains of social service provision, albeit with a period of healthcare restructuring in the 1990s which was later reversed (Gauld, 2009).
Despite providing a relatively well-regarded standard of care, gaps and under-investment in public healthcare remain widespread in Aotearoa. For instance, stakeholders have criticised the limited and delayed access to new cancer medications compared to nations such as Australia and the United Kingdom (Desmarais, 2019; Wonder and Milne, 2011). Unlike the formal healthcare system, the wider welfare state has been thoroughly eroded and reorganised by waves of neoliberal reform. This has important repercussions for accessing healthcare and recovering from medical procedures, not least because of the welfare system's role in the provision of income support (or lack thereof), which may become necessary in cases where the ill and/or their familial carers are not able to fulfil paid-work and unpaid-care roles simultaneously. In a recent example, highly publicised debates have unfolded over people's right to be paid for their labour in caregiving for disabled family members (Bell, 2019; Johnston, 2018). Insufficient or absent income support for those managing illnesses, or caring for others, has long been a source of contention. Recent empirical research has shown that higher rates of crowdfunding are correlated with weaker formal safety nets, such as minimally state-funded healthcare, high costs of private insurance coverage, or generally reduced welfare provisions (Bassani et al., 2019; Lee and Lehdonvirta, 2020). As we show in later discussion, gaps and inadequacies in both the healthcare and ancillary support systems in Aotearoa New Zealand are key to explaining the demand for crowdfunding.
Methods
In order to examine how crowdfunding campaigners secure care for their loved ones, this paper draws on data collected from interviews with campaigners and analysis of interviewees’ online campaigns. Specifically, we engaged with users of Givealittle, Aotearoa's only dedicated donation-based crowdfunding platform, established in 2008 and, unlike global leader GoFundMe, run on a non-profit model. We recruited interview participants by conducting searches for active health-related campaigns on the Givealittle website (www.givealittle.co.nz). Campaigns were excluded if they were raising funds for either funeral costs, an organisation, or someone based overseas. Furthermore, pages with fewer than 15 donations were excluded on the grounds that the campaigners’ level of engagement with the crowdfunding process was likely to have been limited.
Participants were limited to those campaigning on behalf of another person. Research suggests that the majority of campaigns are created by someone other than the funding recipient themselves (Palad and Snyder, 2019; Paulus and Roberts, 2018; Snyder et al., 2018), and indeed, according to descriptive statistics collected by one of this paper's authors (SW) in June 2020, 83% (a clear majority) of health-related campaigns by private citizens on Givealittle were conducted by a third party on behalf of the stated funding recipient. While the decision to exclude those who managed their own campaigns may have precluded some unique insights from those filling the role of ‘campaign manager’ and ‘funding recipient’ concurrently, we made this decision with the intention of mitigating some of the ethical risks and interpersonal complexities of conducting research with people in life-threatening or terminal health situations (Bergman Blix and Wettergren, 2015; Carroll, 2013).
To recruit participants, we posted tailored advertisements to the ‘Question and Answer’ tab of eligible campaigns in early July 2019 following university ethics approval. We posted to a total of 97 campaigns, received 22 responses, and interviewed 15 campaigners. Interviews were conducted by one of the paper's authors (CN-K) in July 2019, with five face-to-face and 10 over the phone. Preliminary analysis of participants’ online campaigns informed the interviews by providing background information on the context of their particular campaign. Engaging with the online user-generated content alongside interview data was useful, as it enabled us to identify tensions and inconsistencies between interview accounts of participants’ lived experiences and online representations, in essence having ‘a foot in both virtual space and material place’ (Morrow et al., 2015: 532). In this paper, pseudonyms are used and any potentially identifiable details, such as workplaces, are altered.
Campaigning for crowdfunding: Attention, deservingness, accountability
In its use to fill gaps in public funding, health-related crowdfunding reflects the detachment of care from ‘broader, inclusive notions of the social through its commodification’, and instead, the responsibilisation of the funding recipient and their social networks (Green and Lawson, 2011: 639). Where healthcare and welfare needs might once have been understood to be a collective responsibility, the locus of responsibility is increasingly focused on the funding recipient and their loved ones (Lawson, 2007; McDowell, 2004). As care scholars have argued, the term ‘responsibility’ has become appropriated within neoliberal discourse to reflect neoliberal values of individual choice and autonomy (Raghuram et al., 2009; Trnka and Trundle, 2014). Responsibilised citizens are understood to be those that are self-determining and self-managing, engaging in ‘self-care’ (Murray, 2007), with any sense of collective responsibility individualised (Beckmann, 2013). Among our participants, the process of securing marketised, crowdfunded care was discussed in three key ways: attracting and maintaining the crowd's attention; detecting and responding to the crowd's perceived conception of a deserving funding recipient; and demonstrating accountability to the crowd.
Grabbing attention
From the outset, the Givealittle platform hails campaigners as players in a competitive market for the crowd's attention and sympathy. Givealittle's campaign page template encourages campaigners to ‘Get people's attention with a brief title’ and ‘Win donors over with a clear explanation’, alluding to the competition for visibility and, ultimately, donors’ money. While those with an attention-grabbing story may have a competitive advantage, effective communications skills (and time and energy to exert them) are positioned as central to a campaign's success.
In constructing an attractive campaign, users must be able to present a coherent and appealing narrative to capture the attention of the crowd (Berliner and Kenworthy, 2017; Paulus and Roberts, 2018). Indeed, the imperative to produce a well-crafted narrative can place significant demand on the time and energy of those managing campaigns for their loved ones, reflecting the devolved responsibility for securing care that crowdfunding entails. One participant, Michelle, described the time it took to piece together a story that she and her husband were happy to share on Givealittle:
It actually took us about 10 days from the time we decided to structure the Givealittle page to put it out there, because we wanted a very clear message. We didn't want to oversupply information, but we wanted people to have sufficient information to know what it was being used for.
Michelle's account speaks to the perceived imperative to disclose personal details in order to make a story compelling, while also seeking to maintain some degree of privacy (Dressler and Kelly, 2018; Gonzales et al., 2018), a balancing act that can result in a lengthy campaign-crafting process. Her attention to honing ‘a very clear message’ resonates with marketised logics, while also indicating the time and the skilled labour required to produce campaign texts.
Such demands are exacerbated for those who have difficulties with written literacy. Indeed, existing research has flagged how the need to ‘sell’ one's story in an online context to attract attention privileges those with fine-tuned writing skills (Berliner and Kenworthy, 2017; Kenworthy et al., 2020). This heightened burden was evident in the comments of one participant, Nancy, who sought assistance from the funding recipient in writing the campaign due to her dyslexia, as well as her propensity for swearing. She explained:
I had her beside me [while I was writing the campaign], because I have a learning disability and I’m dyslexic so I needed her to help with the format of the paragraph about what's happened, and also in a way where if it was me just speaking there probably would have been a lot of ‘fucks’ and ‘shits’ (laughs). … I thought I was back at uni doing a 3,000-word essay!
Nancy's explanation suggests a hierarchy of communication styles is at play wherein the kind of ‘good’ and persuasive writing thought to be marketable and attractive also indexes cultural and educational hierarchies. As such, Givealittle's apparently free market is suffused with sociocultural privilege. Crowdfunding responsibilises funding recipients and their loved ones, while disadvantaging those lacking the time, skills or capital to craft what they believe would be – or would have the best chances of being – a captivating campaign. While free and democratic in theory, crowdfunding is thus a means of social reproduction that people are variably and inequitably equipped to embrace.
Demonstrating deservingness
Judgements of (un)deservingness are politically and morally charged. As Willen (2012) observes, shared understandings of who is and is not deserving reflect wider social and cultural contexts. A primary means of establishing deservingness is to evidence one's proximity to culturally valued ideals of personhood. It is unsurprising, then, that today's crowdfunding users frequently invoke values associated with neoliberal subjectivity to frame their cause as ‘deserving’ of funding. In order to justify public appeals for money, users frame funding recipients as hard-working and responsibilised, in other words the ‘ideal’ neoliberal subject (Barcelos, 2020; England, 2010).
Such a framing was evident in statements made on participants’ Givealittle pages, including ‘As a striving young Auckland family, Kate and John are both working full time’ and ‘As a young hard working family in a house of their own[,] anything received will be an enormous help’ (Campaign, Bex). This emphasis on worker identities reinforces the idea that caring activities are designed to support the economically engaged, in order to restore autonomy and reproduce the labour force (Green and Lawson, 2011). Many campaigns also foregrounded the dedication and community-mindedness of funding recipients through statements like ‘Sharon has been a passionate teacher for around 20 years’ (Campaign, Tracy) and ‘Sarah is a teacher of 20+ years and loves her job, but is on the verge of not being able to manage that anymore’ (Campaign, Scott). These campaign extracts suggest that the recipients might have earned community investment through teaching, a profession widely understood as a form of service and community development. Recipients who can be categorised as a ‘civil servant’, or otherwise morally reputable, are most readily marketed as care objects.
The notion of choice, or indeed, lack thereof, was emphasised through interviewees’ campaigns. By stressing a lack of control over circumstances, campaigners frame the funding recipient's predicament as a product of ‘bad luck’ (Snyder, 2016; Young and Scheinberg, 2017), thus distancing the recipient from any judgement of personal irresponsibility (Gillespie and Lawson, 2017). For instance, Scott's campaign explicitly emphasised that his wife's circumstances were beyond her control, stating ‘Unfortunately, through no fault of her own, Sarah has developed the debilitating disease, Multiple Sclerosis’. This surprising – and arguably superfluous – rhetorical move indicates the importance of establishing that Sarah is faultless (and therefore worthy of care) in a context where people are otherwise routinely held responsible for their circumstances. Lack of control was also communicated through narration techniques that emphasised a recent, sudden and unanticipated change in the lives of the funding recipients. Describing her nephew's cancer diagnosis, Pat's campaign read ‘The past 8 weeks has seen the Smith family's world flipped upside down’. Similarly, Michelle wrote of her husband's cancer, ‘This diagnosis came as a huge shock to him and his family as well as all who know him well in the community’.
Beyond positioning within online campaigns, the neoliberal tenor of the morally ‘legitimate’ funding recipient was also evident in campaigner's justifications for their decision to crowdfund. Many campaigners emphasised the degree to which they and/or the funding recipient were actively taking steps to address their own hardships, reflecting neoliberal investments in individual responsibility, entrepreneurship and grit, and repudiation of passivity, weakness and inertia. Scholars have discussed how the rhetoric of ‘responsible citizenship’ increasingly informs care provision, for instance in job-seeking requirements for welfare eligibility among the unemployed (England, 2010; Green and Lawson, 2011; Hoppania and Vaittinen, 2015). These values were foregrounded as implied criteria of ‘deservingness’ of care in the comments of participants. Vanessa, for instance, who was fundraising for an overseas procedure for her son, felt that her online appeal for funding was justified because of the extra effort she and her family were putting in on the side to host events and other fundraisers. She explained:
I feel fine about it, knowing that we’re actually putting on all these other events. We’re doing lots of things ourselves as well. Not just ‘oh we’re gonna sit here and do nothing and wait for people to give us some money’, you know? I don't agree with that, but the fact that we are working our arses off as well, I feel okay about it.
In a similar vein, Pat, who was fundraising for her nephew's overseas treatment, felt the need to have a defined time period for her campaign in order to avoid the perception that they were passively taking advantage of the generosity of others. She explained, ‘It's not something that we want to just keep milking, or be perceived as milking. It’ll have a timeline, and then we can start giving back or whatever’.
By juxtaposing their approach to crowdfunding against those who would ‘sit here and do nothing’ or ‘just keep milking’, these interviewees justify their requests for money in assertions of the independence and self-determination of the funding recipient and/or their family; making donations closer to investments, than gifts. In doing so, they distance the funding recipient from those who are seen to be ‘morally illegitimate’ recipients of assistance, such as the homeless or welfare beneficiaries, who are commonly framed as lazy and passive (Gillespie and Lawson, 2017). For instance, Tracy, fundraising for her friend Sharon, explained Sharon's desire to distance herself from the archetype of a ‘beggar’:
She was a bit reluctant [to crowdfund] because she didn't want people to think she had her hand out and was begging for money. … And then I think she was so desperate that she agreed. I can see where she's coming from. You don't want people to think ‘oh gosh, look at poor Sharon, she's struggling’. You don't want people to feel sorry for you.
Here, Tracy suggests that a public declaration of (financial) dependence on others is perceived to trigger responses of pity. In the ‘language’ of neoliberalism, dependency is a trait that has come to be devalued and understood as the antithesis of self-actualisation (McDowell, 2004; Wiles, 2011). Such a devaluing of dependency is at odds with the relational ontology foregrounded within care ethics, which highlights how people are irrevocably interdependent throughout their lives (Brown, 2003; England, 2010; Raghuram et al., 2009). By reiterating their independence and positioning themselves as self-responsible individuals, campaigners therefore play into an understanding of care as a discrete intervention during abnormal circumstances that a market and private investors can solve, rather than a pervasive and necessary feature of social life (Haylett, 2003; Held, 2002).
Neoliberal constructions of the ‘morally deserving’ funding recipient-subject shaped the ability of campaigners to capitalise on donations from strangers. Scholars discussing health-related crowdfunding have previously raised concerns as to what types of health needs are likely to attract funding, and what the implications of this are in contexts where crowdfunding becomes a substitute for public funding (Barcelos, 2020; Berliner and Kenworthy, 2017; Farnel, 2015; Palad and Snyder, 2019). Among the pool of 15 participants, the five campaigns that received the most funding were for individuals with cancer and neurological diseases (see Table 1). Campaigners such as Pat, whose two-year-old nephew Toby had a rare form of cancer, received significant support from strangers, raising about NZ$90,000 in 3 weeks. She explained, ‘Absolute strangers reached out. I think it's people who mostly have kids themselves or whatever and think, “holy shit,” you know, “this could happen”’. Similarly, Bex managed to raise about NZ$20,000 from wider networks and strangers to support her friend Kate, whose daughter had cancer. She stated:
Details of participants and their respective funding recipients and campaigns.
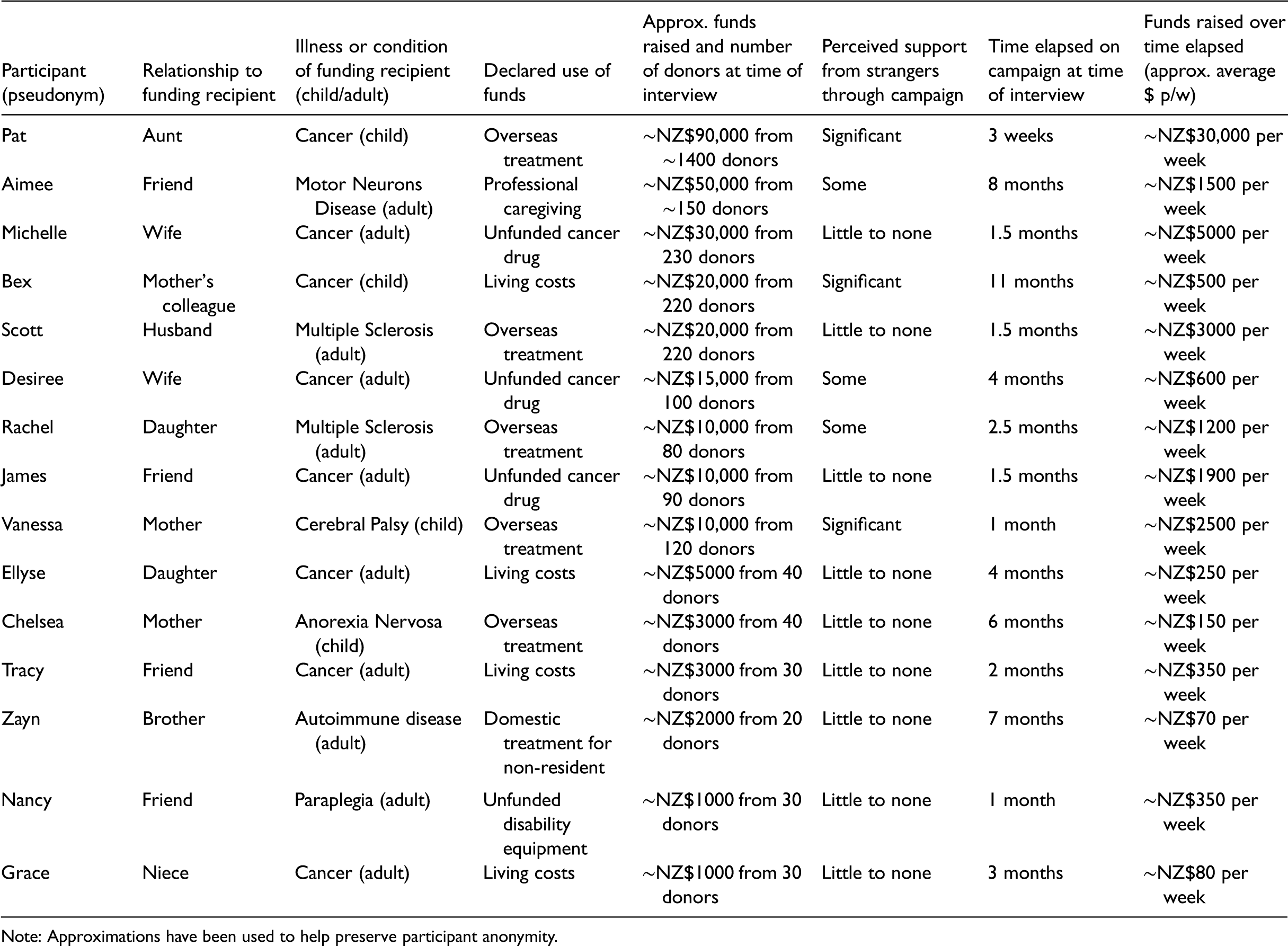
Note: Approximations have been used to help preserve participant anonymity.
I found it was especially elderly ladies [that donated to the campaign]. The kids are all overseas, they don't have grandchildren, and this is the beauty of New Zealand eh. It is for me the fact that there's people out there that just wanna give.
The successes of campaigning for a child relative to that of an adult in the crowdfunding context have been acknowledged (Kenworthy et al., 2020: 17; Snyder et al., 2017) and the contrasting experiences of some participants with others in our study suggest that factors beyond the ‘broad sympathy’ that campaigns for children elicit shape the ability of campaigners to trigger caring responses in a crowdfunding context. Chelsea, who was crowdfunding for treatment for her daughter's Anorexia Nervosa, raised roughly $3000 over 6 months, significantly less than the three other interviewees campaigning around a child's illness. She described in an interview that the money she had managed to raise was a ‘bare minimum’ and came from some very good friends and local community only’. She recounted what she felt was an ‘uphill battle’ in trying to raise funds for a stigmatised cause:
As soon as you mention the Child Cancer Trust, people go ‘oh yeah, I’ll put money into that’, but if you say eating disorders, it doesn't have the same sexy ring to it, does it? People still well-and-truly see it as a personal choice, but it's not. It's no more a choice than anyone having Type One Diabetes thrown in with Bipolar.
Chelsea felt that misunderstanding of eating disorders as a personal ‘choice’, and thus a consequence of personal irresponsibility, impacted her campaign's marketability to strangers. She expressed that as a result of a lack of ‘public awareness and understanding of eating disorders, the page has attracted very little in the way of support’. An inability to convincingly ‘package’ Anorexia Nervosa as the product of ‘bad luck’ and uncontrollable circumstances (Snyder, 2016; Young and Scheinberg, 2017) therefore may hinder the ability of those like Chelsea's daughter to be taken care of in a crowdfunding context, irrespective of medical need.
Crowdfunding campaigners engage with dominant discourses of the responsibilised subject in order to enact the deservingness of their cause, and, ultimately, ensure their loved ones are taken care of. Through their framing both within their online campaigns and in the discussion of these campaigns, campaigners appeal to values of hard work, self-responsibility and economic productivity when describing the funding recipient. In this way, the recipient's behaviours and attitudes become implied criteria of deservingness. Those who cannot easily narrate their circumstances in such a manner, may struggle to pitch and demonstrate the worthiness of their cause in a way that attracts empathy and investments of care.
Burdens and accountabilities
On the whole, interviewees described the labour of setting up and managing a crowdfunding page as burdensome. Beckmann (2013: 171) argues in her discussion of care provision for people with HIV/AIDS that a focus on responsibilisation places ‘an undue burden on people who are barely able to survive.’ In a similar vein, crowdfunding transfers responsibility for taking care of funding recipients from public to private spheres, taxing the time and energy of ailing individuals and their supporters. For participants such as Tracy, who was fundraising for a friend outside her household, awareness of the burdens of crowdfunding was a key motivator in establishing the page on behalf of her friend. Tracy stated:
I set up a Givealittle page just to try and get her some extra money, because I know what it's like when you’re going through health issues and you should really be focusing on that and getting better, not how you’re gonna pay the rent and eat and put petrol in the car.
When campaigners were residing with the funding recipients, the labour of managing a Givealittle page could further compound the challenges of having an ailing loved one. As Michelle explained:
You should just be worrying about having to get this person well and healthy and make the most of every day with one another, not having to try and struggle to raise funds and lead a campaign so to speak. Your time and energy and efforts should be going into really having quality time together as a family, rather than having to spend hours on end emailing, sending texts and that sort of thing to try and encourage them to support you.
The work of managing a crowdfunding campaign does not cease once donors are secured. As well as spending ‘hours on end’ contacting and encouraging potential donors, interviewees described spending considerable thought and effort demonstrating their financial accountability to donor-investors. A sense of accountability, Trnka and Trundle (2014) argue, is a crucial component of becoming a responsiblised individual, involving displays to broader audiences of the extent of one's ability to self-manage. In the crowdfunding context, accountability to donors involves a public demonstration of ‘self-surveillance’ (Trnka and Trundle, 2014), enacted through posting updates to prove legitimate use of funds. Many participants were conscious of these issues of transparency in their dedicated use of funds throughout the crowdfunding process, a concern that was exacerbated by a consciousness of highly publicised cases of fraud in crowdfunding (Snyder et al., 2016; Zenone and Snyder, 2019). As such, many took steps to reassure donors of their legitimate use of funds, for instance through posting regular updates. Several participants felt that providing donors with information was a way of holding up their end of the bargain, as well as advertising continuing need. As Nancy expressed:
There has to be accountability in everything. You’re asking this of people, so I need to be accountable, and giving updates on it is a way of being accountable and going ‘hey’, you know, ‘this is it, her progress is this, we’re getting this much closer’.
Other strategies involved more explicitly marketised means of establishing transparency, including getting an accountant involved to audit the use of funds. As Michelle explained:
I think one of the most important things was to be able to give people reassurance that it was only gonna be used towards his medication. It's not gonna be used for overseas holiday or that sort of thing. That's why we decided to get an accounting firm involved, to use our accountant, who does our business accounts and auditing, so that he will verify that all the money was only used towards the drug and medication.
This perceived need to establish accountability through the crowdfunding process increases the labours of what is, already, a time- and energy-consuming process, but also poses difficulties in the face of evolving caring needs. Scholars have discussed how the commodification of care has led to the expansion of the monitoring and documentation of care practices. Hoppania and Vaittinen (2015: 85) argue in the context of paid care work that this ‘limits the carers’ ability to listen and respond to the actual needs at hand.’ By creating a fixed care ‘product’, care processes are sliced up and fragmented into transactable units, making this commodified care less flexible and responsive to the needs of the care-recipient (Cox, 2013a; Hoppania and Vaittinen, 2015; Mol, 2008).
This reduced flexibility was evident in the narratives of campaigners, who had to negotiate disparities between their ‘advertised’ use of funds and the changing realities of funding recipients’ needs. Partway through raising funds for a targeted cancer drug for her husband, Hone, interviewee Desiree learned that this drug would no longer work for him. She posted an update on the Givealittle page, notifying donors and asking permission for the funds to be diverted to a naturopathic treatment plan; the post read, ‘We would appreciate it if funds could be used towards funding alternative treatments’ (Campaign, Desiree). Of this process, she explained:
[Making that post] was really hard, because we didn't know what was happening over that time. […] I was fine with the possibility that people would take their money back, because it is much easier to donate to something when it's for something specific and you know what's going to happen with it, as opposed to our airy fairy alternative therapies, which we whole heartedly believe in. But yeah, that was really hard. It's just like our world popped again, our whole little bubble. Just keep building it and it keeps getting shredded.
A sense of accountability to donors creates an added layer of uncertainty due to the possibility that people might want their ‘money back’, as they have invested under the assumption of funds being used for a particular purpose that may no longer be suitable in the context of fluctuating care needs. Throughout all of these examples, a care ethics lens highlights the care of donors to crowdfunding campaigns as creating relationships of responsibility, rather than being one-off transactions. Combined with attention to the marketised context of care, however, we can observe the way the ‘incompatibility between care as a corporeal relation and open-ended process on one hand, and the neoliberal logic of choice and commodification that necessitates clearly defined products and services on the other’ (Hoppania and Vaittinen, 2015: 84) can therefore exacerbate the sense of liability to donors among those seeking care through crowdfunding pages.
Conclusion
Crowdfunding invites – and responsibilises – those with unmet healthcare needs to seek funding support from a diverse ‘crowd’ of existing intimate relationships, more distant acquaintances, and strangers. Responsibility for managing crowdfunding efforts is shouldered by a crowdfunding campaigner, usually a family member, partner, or close friend acting on behalf of the person in need. As our analysis demonstrates, the process of pitching for crowdfunding support entails more than stating need. Campaigners work to produce an appealing and captivating representation of the funding recipient's circumstances to convince the ‘crowd’ to invest in care of the funding recipient. The imperative to market medical needs is a form of responsibilisation (Barcelos, 2020; Beckmann, 2013; England, 2010), which can be burdensome for funding recipients and their loved ones. Many campaigners described a sense of duty in remaining accountable to their donors, an accountability that may exacerbate the demands of crowdfunding, but also reduce flexibility in meeting evolving caring demands.
The ability of campaigners to attract funding indexes their ability to position the funding recipient as a ‘deserving’ care-recipient. In verbal justifications of their decision to crowdfund, and in online descriptions of the funding recipient, many campaigners reiterated traits of hard work and self-responsibility; traits that we suggest function as implicit markers of deservingness of care. Those whose lives and circumstances are readily narrated in this way are most easily recognised as worthy recipients of care. Those less readily aligned with dominant understandings of worthiness may not experience the ‘generosity’ of the crowd. This is troubling, given that deservingness, as well as the ability to effectively communicate deservingness, are entangled with sociocultural privilege. While scantly addressed in this paper but worthy of more attention, the imagined ties of nationhood also shape who is ‘read’ as a deserving subject in a crowdfunding context, reinforcing the prevailing importance of social and geographical proximity in spite of the online nature of crowdfunding. These varied experiences therefore highlight how ‘particular bodies in particular encounters can trigger political relations of care, whereas others elsewhere elicit only relations of neglect’ (Robinson, 2018: 327; cf. Bartos, 2018).
In exploring how crowdfunding campaigners face up to the demands of responsibility for healthcare, this paper has made two important contributions to the literature. Existing research on health-related crowdfunding is somewhat abstracted in its claims and, as a nascent body of work, has limited empirical engagement with platform users. Our paper has addressed this shortfall by providing discussion informed by semi-structured interviews with campaigners. Secondly, this research has extended existing literature on the marketisation of care by moving our empirical focus beyond care-giving practices to investigate the criteria that determine deservingness of being taken care of. More broadly, this paper illuminates the various ways in which health-related crowdfunding, as a ‘market device’ (Langley, 2016), is likely to exacerbate inequities in access to care. Our analysis demonstrates one must possess disposable time, resources and culturally-specific knowledge – and, arguably, identities – in order to be taken care of in a crowdfunding context (Gonzales et al., 2018; Snyder et al., 2016). Discourses of deservingness may disproportionately benefit the privileged, who already have greater access to resources and services, and who also, ironically, enjoy better general health, to begin with. Moreover, stigmatised or allegedly ‘self-inflicted’ conditions are unlikely to appeal to donors, and medical need is only able to be evaluated in so far as it is effectively and convincingly narrated. Against a backdrop of limited government support, the emphasis on ‘choice’ within a marketised context of care provision may perversely limit the options of people seeking to secure appropriate care for their loved ones, as care is not guaranteed (Green and Lawson, 2011).
On an abstract level, our account points to the growing importance of crowdfunding as a frontier zone for the marketisation of social reproduction, wherein social relations of care are reshaped. As Cox (2013a) observes, the recasting of care through a marketised mechanism is not uniformly deleterious. Some of our participants, for example, remarked how crowdfunding gave some of their friends and family a way to show they cared, either through monetary donation or as a prompt for them to re-connect with the recipient. And like the story that began this paper, some campaigns are indeed successful and, no doubt, the campaigners and recipients are grateful for the existence of crowdfunding platforms and crowdfunders themselves. At the same time, there are noticeable issues inherent to crowdfunding. Instead of access to care being mediated by citizenship/residency rights or needs assessment, access is deeply contingent on relations to the crowd. Building these relations depends on the skills of the campaigner, the traits of the recipient, and the caprice of the crowd. The relations of care between the recipient and campaigner are also recast: relations of kin or friendship (built on familial responsibility and the like), become overlain and potentially complicated by the roles of ‘recipient’/‘campaigner’ and the entrepreneurial imperative of crowdfunding systems. On a more practical level, while it remains to be seen whether crowdfunded care will erode public systems of care, or solidify as a critical supplement, the findings of this research speak to the need for expanded public cover for healthcare and welfare-related expenses. While some scholars have called for tighter government regulation of crowdfunding (Snyder, 2016; Zhao et al., 2019), prioritising strengthened public healthcare and welfare provision would address the gaps that necessitate the use of these platforms in the first instance. While the subsidised national health system in Aotearoa is undeniably more comprehensive than in some other national contexts, inequities in care and gaps in provision persist. As crowdfunding for health-related purposes continues to grow (van Duynhoven et al., 2019), such concerns will only become more pertinent in years to come.
Footnotes
Acknowledgements
We offer sincere thanks to the participants who gave their time to this research, at a very challenging time in their own and their loved ones’ lives. We also thank audience members at the ‘Bringing life's work to market’ symposium (Auckland, 2019) for helpful feedback.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Marsden Fund (grant number UOA1634).