
Abstract
Introduction:
Using models of occupation in occupational therapy can promote professional identity and self-efficacy. This study evaluated implementing the Person-Environment-Occupation-Performance Model (PEOP) in a neurosciences occupational therapy service in the United Kingdom.
Methodology:
A mixed-methods approach with four stages. 1: survey of conceptual models in practice; 2: conceptual model teaching followed by focus groups; 3: PEOP training followed by implementation and Community of Practice; 4: individual semi-structured interviews. Participants were occupational therapists working in a neurosciences service.
Findings:
The survey identified limited use of conceptual models in practice. Participants chose the PEOP model due to congruence with practice, model semantics and potential to reinforce professional identity. Following training, therapists reported increased knowledge and confidence in using the model. During implementation, data from the community of practice created three themes: feasibility of application, documentation is key to change, keeping it meaningful. Follow-up interviews after 3-months generated three themes: PEOP legitimises the occupational therapist’s role, communities of practice spark change, the model supports occupational adaptation.
Conclusion:
Implementing the PEOP model was feasible and impactful. Training improved knowledge and confidence, and the community of practice and modified documentation supported application. Implementation realised continuity of occupation-centred practice across patient pathways and enhanced professional identity.
Introduction
The occupational therapy workforce has a mission to demonstrate the unique contribution of the profession, which is to facilitate participation in occupations that people need to do, want to do or are expected to do (World Federation of Occupational Therapists (WFOT), 2025). As such, occupational therapists can use occupations as a means and as an outcome using research evidence, theories, conceptual models and practice frameworks to inform what they do. Conceptual models of practice can provide a language to dialogue with others about the unique perspective of occupational therapy (Turpin et al., 2019). Although there are demonstrable benefits of the unique occupational therapy contribution, it has been and remains a challenge for occupational therapists to engage in practice that is truly occupational (Bennetts et al., 2025; Di Tommaso et al., 2016; Jewell et al., 2016; Jones et al., 2022). For instance, Fortune (2000) referred to the term ‘filling gaps’ (p. 225) to describe the influence of the occupational therapist’s role within practices that are not rooted in occupational therapy philosophy. The implementation of occupation-centred practice can be one of the strategies to facilitate a contemporary role that fosters professional identity and shows the benefits of the unique occupational therapy contributions. This article presents the findings of a mixed-methods study of the implementation of the PEOP model (Baum et al., 2015) in an occupational therapy neurosciences service in the National Health Service (NHS) in the UK.
Literature review
A focus on occupation in occupational therapy practice has been debated and established in the literature (Fisher and Marterella, 2019; Fisher, 2013; Mangalindan and Bulan, 2025; Molineux, 2025). According to Fisher and Marterella (2019), an occupation-centred practice refers to ‘our professional perspective – our way of thinking about our clients, their occupations, and our services; one where we maintain our profession-specific perspective and ensure that we place occupation in the centre of our professional reasoning and link everything we do to the core paradigm of occupational therapy’ (p. 75). Supporting this approach, occupational therapy practice is informed by conceptual models of occupation that explain the complexities of how occupations are patterned and experienced (Turpin et al., 2024; Reid et al., 2020). There is a range of models, including the Model of Human Occupation (MOHO; Taylor, 2017), the Canadian Model of Occupational Participation (CanMOP; Egan and Restall, 2022) and the PEOP (Baum et al., 2015). Although the use of models and theories of occupation as an organising framework for practice is becoming more common, application has been inconsistent and proved challenging for therapists in some settings (Leclair et al., 2013; Lee, 2010; Ikiugu, 2012; Phillips et al., 2023).
There are a limited number of theory-to-practice studies that have reported on the implementation of models of occupation. A recent scoping review (Bass et al., 2024) found that the PEOP model was used to guide occupational therapy processes across a range of services globally, including those addressing sleep and self-management, as well as in primary care. Boniface et al. (2008) facilitated the use of the Canadian Model of Occupational Performance and Engagement (CMOP-E) (Townsend and Polatajko, 2013) in a participatory action research (PAR) study across health and social care in the UK. Their findings suggested that using a model promoted person-centred approaches and demonstrated professional reasoning. Wimpenny et al. (2010) also used PAR to implement the MOHO in a mental health setting where it was found to foster professional identity through shared understanding, mutual language and self-efficacy. The effectiveness of instruction in models of occupation on student competence at an occupational therapy programme in the USA was examined by Ikiugu and Smallfield (2015), who found that, following instruction, students demonstrated significant improvements in their perceived understanding of theory, leading to greater confidence in assessments and intervention skills. To support theory to practice implementation, Boniface et al. (2008), Wimpenny et al. (2010) and Phillips et al. (2023) pointed out the importance of critical learning spaces, effective instruction, identifying barriers, taking time to embed, ensuring a flexible application to the specific setting, and continuous supervision were powerful strategies to encourage occupation-centred practice. Several barriers to theory-practice integration have been identified, including constraints of the practice setting, therapists’ attitudes and knowledge and potential confusion about combining models (Lee et al., 2008; Ikiugu, 2012).
Recent empirical research on the use of models in practice is lacking, and there do not appear to be any studies that consider theory to practice implementation of PEOP in a hospital neurosciences therapy setting in the United Kingdom. Therefore, the aim of this study was to evaluate the implementation of the PEOP model in a neurosciences occupational therapy service through the following objectives:
To evaluate the attitudes, knowledge and skills of occupational therapists using models in practice before, during and after training and implementation of an occupation-centred model of practice.
To deliver training in the use of an occupation-centred model and then explore the experience of occupational therapists implementing this in a neuroscience service.
Methodology
The research was conducted in a large National Health Service (NHS) Teaching Hospital in a UK city that treats 1.5 million patients annually and employs 22,000 staff. The neurosciences department includes neurology, neurosurgery, neuro-oncology and stroke services spread over three hospital sites. Occupational therapy is provided at all sites as part of multidisciplinary teams (including social workers, physiotherapists, speech and language therapists, psychologists, dieticians, medics and nurses) across acute inpatient, inpatient rehabilitation and outpatient rehabilitation services. This occupational therapy department was chosen due to an ongoing collaboration between clinical and academic researchers, and occupational therapy pre-registration students and hospital staff, bringing attention to a lack of professional identity and ability to focus on occupation in their work. The participant inclusion criteria were occupational therapists working in the neurosciences therapy department. This research used a mixed methods approach (Corcoran, 2017). The project had four stages informed by change management theory and Learning-Transfer Evaluation (Thalheimer, 2018). The study took place over a 16-month period.
Research ethics
This research had ethical approval from the University of Bradford (approval E1056) and was recorded as a service improvement project by the NHS Trust. The NHS service managers acted as gatekeepers and emailed participant information to all occupational therapists in the neurosciences team. Participants responded to the research team to limit feelings of coercion or a requirement to take part. Potential participants had as long as they needed to consider taking part in the project. Participants were asked, but not required, to take part in all stages of the project, with separate participant information and informed consent gained at each stage. Participants had the right to withdraw their consent at any time, but previously collected data was included in the project.
Reflexivity
Reflexivity was embedded throughout the research as a continuous process involving participants examining and sharing their experiences and critically analysing how their subjectivity and context influenced the study (Olmos-Vega et al., 2022). The first four authors are academic researchers with clinical and teaching experience in conceptual models of practice, while the remaining three are researcher-practitioners directly involved in the services studied. Reflexivity was fostered through horizontal relationships, MS Teams discussions and debriefings to reflect on successes and plan improvements. All authors contributed written reflections that were shared with the first author of this article. In the final meeting, they met in person to discuss the analysis, highlight key discussion points and explore future research directions. Finally, to support best practice in reporting our research, we followed the Reflexive Thematic Analysis Reporting Guidelines (RTARG), which included, but was not limited to, reflections on themes being generated rather than emerging and on analysis being more appropriate than findings (Braun and Clarke, 2024).
Analysis
Stage 1: Pre and post survey
Thirteen occupational therapists participated in the first survey, which aimed to characterise participants and their prior knowledge of conceptual models of practice. The mean time working in the neurosciences service was 25 months, and the mean years qualified was 12.8. Since our research had a small number of participants and the places where they work could be easily identified if detailed information is provided, we opted to present participants generally instead of describing them using a table. Participants worked in a variety of settings, such as complex neurorehabilitation, neurosurgery, stroke, neuro-oncology, rotational and managerial work. In order of responses, the conceptual models of practice participants most used in their practices were: MOHO (n = 8), CMOP-E (n = 7) and PEOP (n = 4). Five participants reported using a conceptual model in their current work (PEO, PEOP and MOHO). Table 1 shows how participants believed the conceptual model of practice would help effectively in the occupational therapy process, with a higher rate of ‘effective’ responses for contribution to: occupation-centred practice, interventions, outcomes, service user satisfaction and professional identity.
Perceived contribution of a model in the effectiveness of occupational therapy process (n = 13).
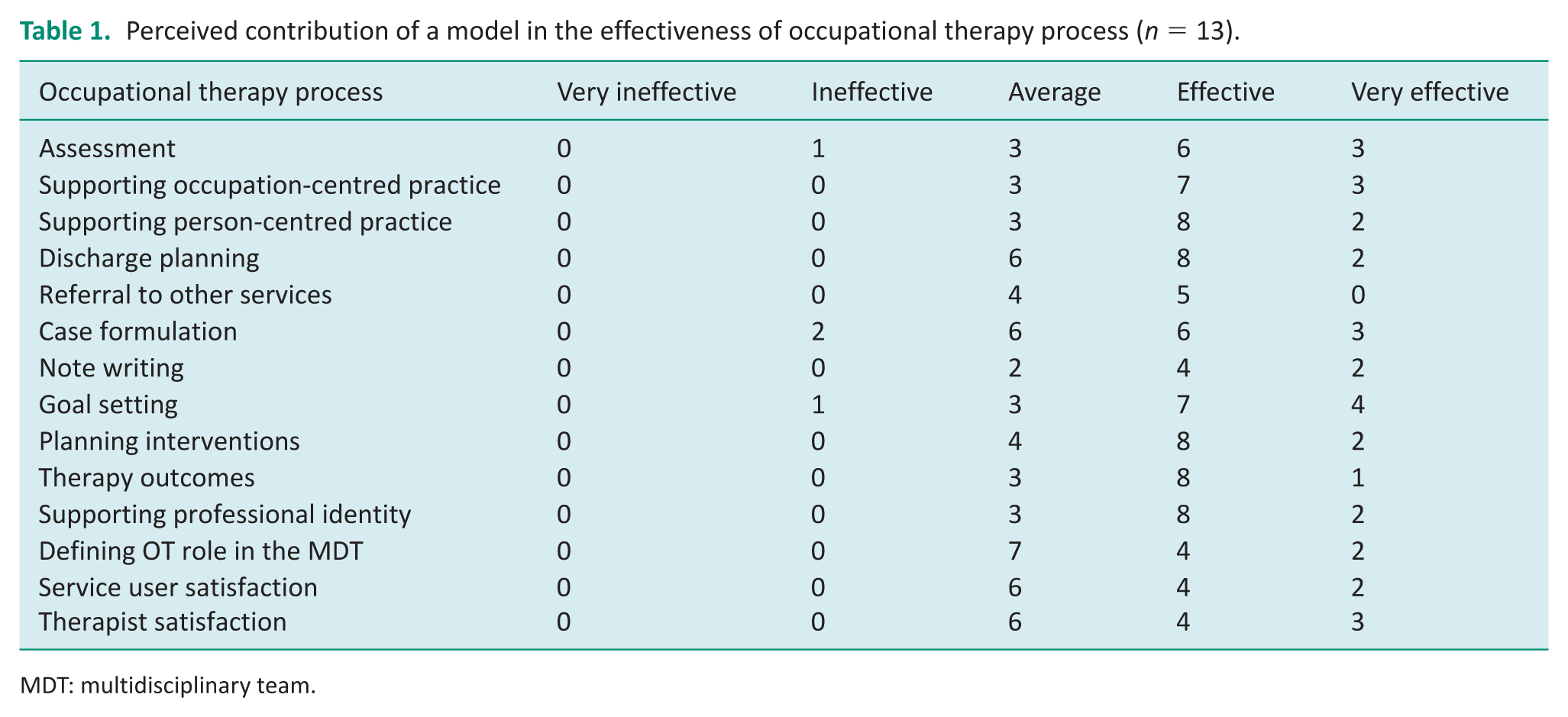
MDT: multidisciplinary team.
Twenty-two participants took part in the second survey, which was delivered following the conceptual models teaching and focus groups in Stage 2 of the study. This survey identified participants’ perceptions of using a conceptual model in their practice. Table 2 presents the results, where it shows that there was participant agreement that using a conceptual model could enhance documentation and be very helpful with occupation-centred practice.
Perceived contribution of PEOP for the occupational therapy process.
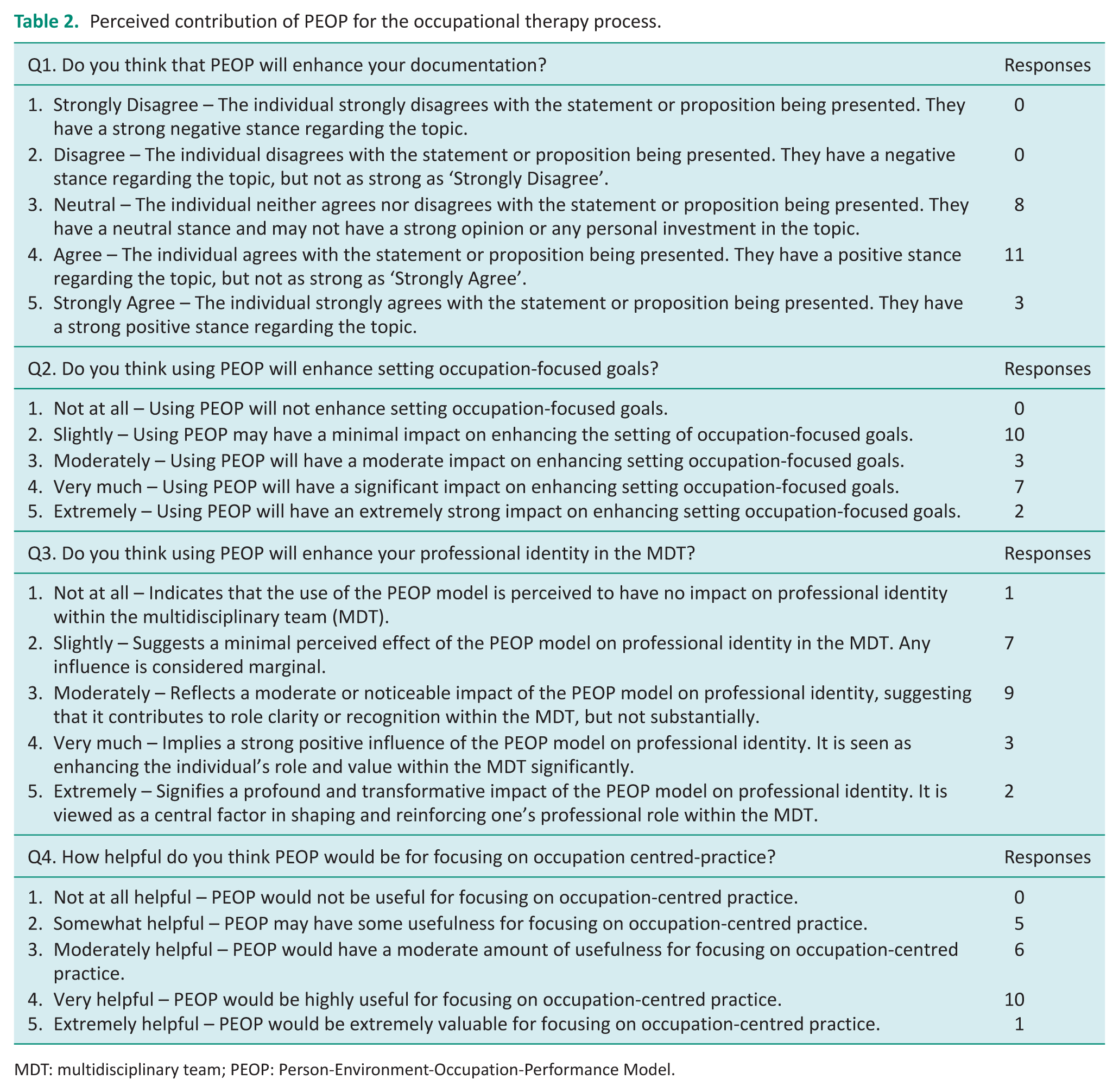
MDT: multidisciplinary team; PEOP: Person-Environment-Occupation-Performance Model.
For the third survey, 21 participants completed the pre-PEOP training survey and 22 the post-PEOP training survey. The survey asked two questions regarding knowledge and confidence in using the PEOP model. Table 3 presents the results, where it demonstrates that the PEOP training increased their knowledge and confidence in using the model.
Training results – pre and post participants’ knowledge and confidence.
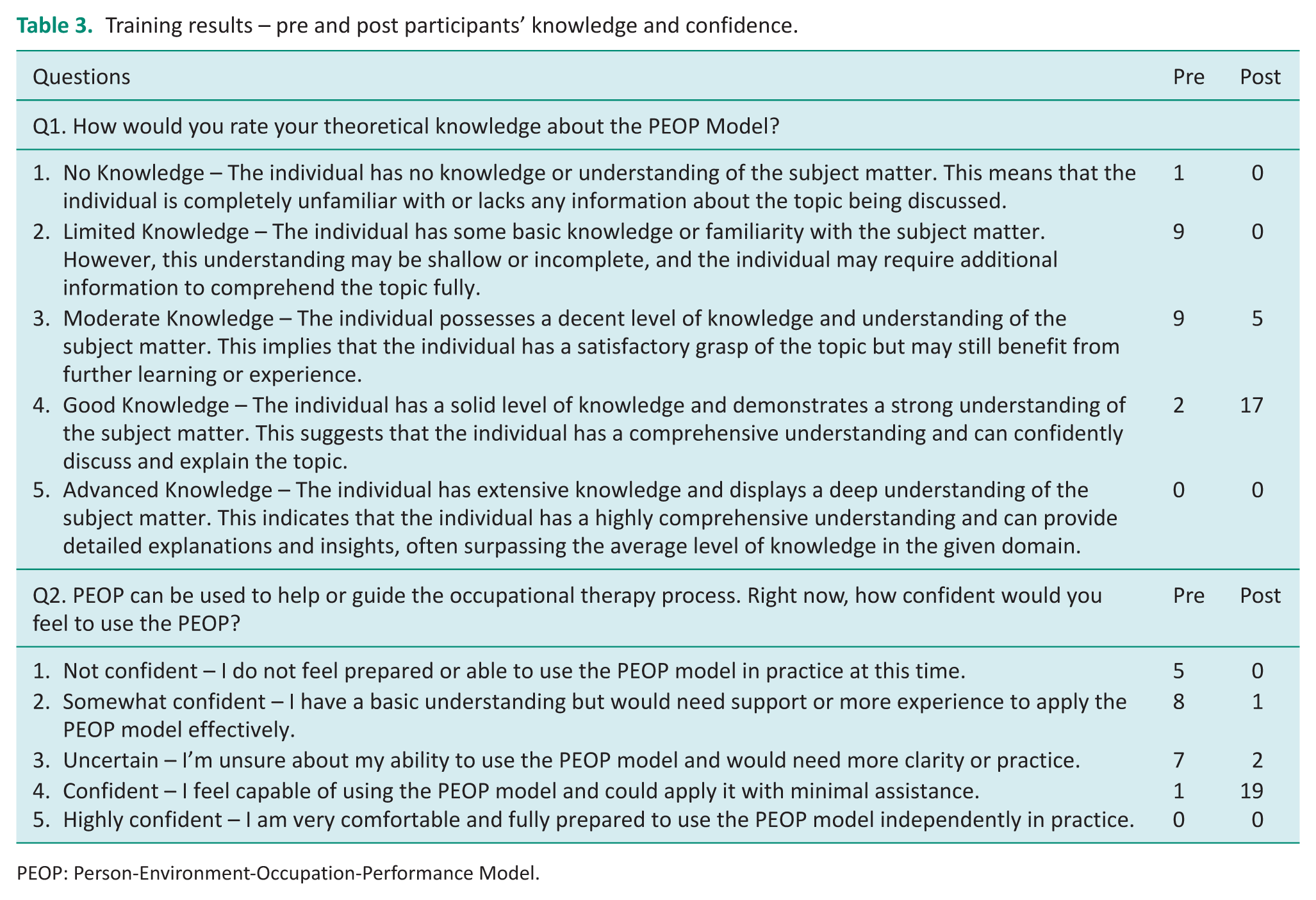
PEOP: Person-Environment-Occupation-Performance Model.
Stage 2: Teaching of conceptual models and focus groups
The model selection stage involved a lecture presenting four occupation-centred models of practice, followed by three concurrent focus group discussions. Thirty participants took part across two lectures and six focus groups. Focus group discussions were recorded with participants’ permission and lasted approximately 30 minutes. The focus group facilitators guided the discussion structure through questions on initial thoughts on the models, the language, the occupational therapy process, implementation barriers and professional identity. Following the discussion, each focus group ranked the four models in order of preference for implementation. Following transcription, a six-stage reflexive thematic analysis was employed to create initial codes and generate themes (Braun and Clarke, 2021).
The PEOP was selected by participants for implementation because it was ranked first or second choice in each of the six groups. Discussion associated with the model selection is presented in three themes with Illustrative quotes from the focus groups.
Theme 1: Congruence with the practice setting
The first theme reflects how participants felt the model fits with their occupational therapy practice setting. Discussion included considering the attributes of each model and weighing up the pros and cons against use in a medical service context.
I think with PEOP. . .it does break down for the person like. . .the motor component, your cognition so I think from that element that fits how you would probably assess a patient sometimes in a service. (Focus Group 1)
The applicability, integration and translation of the models into practice were considered. This congruence concerned pragmatic and realistic considerations of implementation, such as time pressure and perceived gaps between the models and practice.
. . .if you had the luxury of time, it would be brilliant to go through it all, but you don’t. (Focus Group 2)
This theme also incorporated ideas about the person/patient in the neurosciences service pathway. The application of the holistic, person-centred and personalised elements of the models was thought to support a patient’s pathway through acute services to rehabilitation and to out-patient services, but it was recognised that a person’s needs change during this journey. Discussions centred on the merits of the models for the varied practice contexts.
I like the PEOP but that’s because . . . the acute nature of where we work whereas perhaps you could go more into the COPM . . . in the rehab setting cause I think it’s the speed of it and what we are looking at . . . so we are at the assessment kind of phase more and moving towards the goals phase, so I think unfortunately the institution guides us. . . (Focus Group 2)
Theme 2: Model semantics
The model semantics constituted a theme involving the meaning of terms and language employed in the models. There was much discussion of the attributes of the professional language used as a facilitator or barrier to the adoption of a model, and the participants related this to their professional background, education and practice knowledge. Participants discussed how occupational therapy theories, concepts and models form the basis of professional language, and that they needed to contend with how to explain the complexity of these so that they have resonance within and beyond the occupational therapy profession.
I think some of them use quite a lot of jargon that they wouldn’t necessarily be able to understand, and it might be quite difficult for us to explain in simple terms (Focus Group 1) . . .if you look at PEOP, a lot of the terminology is what we do use and we break it down and we look at cognition we are looking at you know motor skills. . .it brings in all the terminology we already use (Focus Group 2)
Theme 3: Reinforcing the profession’s identity
The third theme related the models to the professional identity and status of occupational therapy. This included the professional standing and influence of occupational therapy within the multidisciplinary team (MDT) and wider organisation. This theme was linked to the perceptions and understandings of the profession by other disciplines, with the professional image portrayed through the models being considered important to professional esteem. In the MDT setting, there was discussion of the tensions, challenges and conflicts encountered in a sometimes-combative environment. Use of an occupation-centred model had the potential to change practice and positively influence the MDT, which was seen as empowering for the profession.
. . .we are always fighting for kind of validation and just understanding and appreciation of just what we do from patient and professionals depending on the setting. (Focus Group 2)
Stage 3: Training and communities of practice
Twenty-two participants received training and resources to support implementation of the PEOP, similar to the recent Australian study of Bennetts et al. (2025), which applied PEOP in an acute hospital. During a three-month implementation period, two CoP were facilitated; mean attendance at the CoP’s comprised 10 participants. The CoPs were audio recorded, transcribed and analysed using reflexive thematic analysis (Braun and Clarke, 2021). Three themes are presented with anonymised participant quotes.
Theme 1: Feasibility of application
The participants referred to the PEOP applying in all settings but demonstrated a careful consideration of the feasibility of application relating to the timing within the patient journey, as well as which patients to apply it to initially. The therapists were positive, open minded, problem solving and explored their implementation in acute and rehabilitation settings.
It’s not impossible (CoP 2) There’s only two of us in our team, so it’s quite easy for us to make a decision to roll with something and trial it for a period of time (CoP 3) So we’ve only tried it with a couple people so far, . . . it is still quite new, but we’ve used some headings from the model (CoP 2)
Theme 2: Documentation is key to change
Participants discussed the practicalities of applying the PEOP by exploring ideas and sharing experiences, particularly regarding adjusting documentation to facilitate easier implementation of the changes. Interestingly, the documentation was key to the implementation of the change.
Initially, my thoughts were ‘this is a bit more extra work’ in comparison to what we’re doing at the moment anyway, with the documentation that we already do, [BUT] I think, if you think of the bigger picture (CoP 1) I can see there’s a massive value . . . it (current documentation) doesn’t show the detail and the quality or the richness of what they (OTs) do, you know, it’s (current documentation) not really giving the right information (CoP 1)
Theme 3: Keeping it Meaningful
In this theme, it was apparent that therapists were able to identify how the investment in time added to a more person-centred, occupation-centred and meaningful occupational therapy process. This yielded more meaningful results and was better suited to the therapists’ professional identities. Furthermore, this offered above and beyond the medical model by reclaiming the ‘occupational’ therapy identity amid fast-paced medical environments.
For me, it’s a prompt to keep things more meaningful. A reminder to write down what is important to this person. . . .what’s relevant to the occupations they need to do, because I think a lot of the time we go in with the focus of what’s essential to get them out of hospital, or you know, what are the risks. It just brings your thinking back a little bit more to the person. . .it’s another way we can be prompted to bring it back to towards meaningful (CoP 1) It just brings it back to, . . . meaningful occupation. Sometimes you can get carried away with certain goals about getting somebody out of hospital or whatever (CoP 3) It reminds me to keep occupation focused – putting our focus on where it should be (CoP 3)
Stage 4: Interviews
Following the CoP and a three-month period of implementation, all participants from Stage 3 were invited to take part in follow-up interviews. Five individual semi-structured interviews were conducted, lasting 20–30 minutes each. They were audio-recorded, transcribed verbatim and analysed using the six stages of Braun and Clarke’s Reflexive Thematic Analysis (Braun and Clarke, 2021). Three themes were created, which are explored and illustrated with anonymised quotes. For these individual interviews, participants at this stage were assigned pseudonyms: Alex, Charlie, Jay, Nat and Pat.
Theme 1: PEOP legitimises the occupational therapists’ role
Participants consistently highlighted that the PEOP model offered a structured yet flexible approach that aligned with their professional values, particularly in promoting a person and occupation-centred focus within the acute medical setting.
I think one thing I’m really pleased about is actually it’s just giving people time to pause and think . . . actually . . . what’s important to the patient, you know, rather than, I think, there’s a tendency when you’re working in such an acute and fast environment to just be like . . . get the patient home and be very sort of medical model focused’ (Pat)
The PEOP model was viewed not only as a guide for professional reasoning but also to foreground occupational therapy’s distinct contribution. Participants described the model as ‘allowing’ them to maintain focus on occupation rather than defaulting to isolated impairments or symptoms – reinforcing their identity as occupation-centred professionals.
However, there was concern voiced across the interviews that occupational therapists are sometimes perceived within the MDT as the ‘gap fillers’ for non-medical tasks, for example, conducting cognitive assessments, managing discharge planning, or addressing functional limitations, and there were perceived clashes in the priorities for patient care.
. . .the model makes us keep going back to the relationship between person, environment and occupation . . . and not allow the focus. . . or priority to be a cognitive assessment, or you know, I . . . question myself. ‘Am I just filling gaps’? (Alex) because their (acute surgery/medicine) priorities are different, different to perhaps rehabilitation. They’re looking at discharge planning and things like that. So being able to concentrate on the occupations can be really difficult. (Charlie)
Participants also reflected on how the language of the PEOP model, with its emphasis on participation and person-centred practice, was more readily accepted and understood by other MDT members, ‘So like, I’ve definitely seen some of the physios. . . having a good read and seeing it, which is nice.’ (Nat) However, one participant acknowledged, ‘The fear of if I start using language in my notes that people don’t understand, they won’t read them.’ (Jay) Nonetheless, participants acknowledged ongoing tensions between traditional medical expectations and their occupation-centred philosophy.
Traditional ways of working can still raise its ugly head . . . sometimes there’s still the expectation of you’re there to fix their cognition . . . their vision . . . their physical arm. And it’s like—no, I’m here to fix occupation. (Alex)
Theme 2: Communities of practice spark change but need sustained change
Participants articulated that while the introduction of the PEOP model through communities of practice served as a valuable starting point, the process of embedding this as a new occupational therapy practice demanded structured support, leadership and continuous reinforcement.
We’ve got the tools, we’ve got the education, we’ve got people who are passionate . . . We just almost need those opportunities to continue to discuss it and use it . . . That’s the key. . . that’s what will sustain the change. (Pat) It’s the change management thing of changing practice. It takes a lot of doing from lots of different directions. (Charlie)
Initially, some participants found the model’s implementation burdensome in the context of existing workloads ‘When you’re first starting to do something, it kind of felt like it took quite a lot of time. . . if we’re having a particularly busy week, we won’t always do that’. (Nat). However, over time, attitudes shifted ‘I don’t really feel like it has taken that much more time. . . it’s just slightly adapting how we do it’. (Nat).
Several participants described practical strategies that supported the model’s integration, such as visual prompts (e.g., PEOP posters) and having designated champions or team leads ‘Perhaps have champions. . . thinking of new ways. . . a journal club. . . just to keep that conversation going and embedding it’. (Jay). Participants also discussed the importance of managerial support, noting that both managerial engagement and institutional structures are essential. ‘It felt easier to adopt the model, as my manager has made me engage in this project. . . it’s not just me thinking, ‘oh, no one else is using it’ (Pat), ‘It needs a kind of organised oversight. . . someone as a head of it, you know, head of clinical practice, three or four tiers above us.’ (Alex).
Theme 3: The PEOP model supports long-term occupational adaptation
Participants strongly conveyed that the PEOP model provides a more comprehensive framework for addressing the enduring impacts of life-changing health events. This theme reflects a shared feeling that the PEOP enabled occupational therapists to consider the long-term consequences of illness or injury on participation, and therefore, enabling more meaningful and person-centred goal setting that extends beyond the hospital or acute setting.
Often in the medical acute services it’s a case of. . . . you’re going to recover from that temporary interruption. . . but a lot of what we see for our neuro-patients is life changing. It’s forever then . . . It’s much more about how are we going to keep adapting, changing, finding the new normal? (Jay)
The ability of the PEOP model to support continuity of care across settings was highlighted ‘It’s important that it follows the patient path right the way through’. (Charlie). Participants reflected the increasing emphasis on ensuring seamless transitions from hospital to community services and underscored how a shared theoretical model can support interdisciplinary collaboration and consistent goal progression.
It (PEOP) kind of leads to more conducive goals in terms of, like, right, we’ve written down what they, the person.….exactly what they’re able to do at the minute….but what is the environment that they’re going back to, what support have they got available and. . .what are the occupations that are important to them? . . .Any goals going forward for [the community team] is then like, well, we’ve already identified kind of what they want to work on. (Nat)
Discussion
This research is the first to evaluate and explore the experience of implementing the PEOP model within a neuroscience occupational therapy service in the United Kingdom. Overall, the study found that occupational therapy practitioners considered the introduction of the model to be potentially effective at various stages of the occupational therapy process, with particular emphasis on gathering information and goal setting. Notably, participants initially selected the PEOP model over other conceptual frameworks. This preference may be attributed to the specific characteristics of neuroscience services, such as acute care and rehabilitation, where early intervention priorities often centre, for example, on cognitive assessments or the analysis of motor components. These, among other elements, are encompassed within the PEOP model, which maintains its outcome focus across three domains: participation, performance and well-being (Baum et al., 2015).
Participants reported that their knowledge of and confidence to use the PEOP model increased following training. Participants also reported that the conceptual model’s specific terminology for occupation reinforced their professional identity. Interestingly, the research resonates with that of Ikiugu and Smallfield (2015) that knowing the model and its concepts increased participants’ knowledge and confidence, demonstrating that a single session of discussions can start a process of change, as evidenced in the Mentimeter poll pre- and post-training. These promising analyses reinforce the need for a continuous professional development focused on occupation-centred practice. A review conducted by Turner and Knight (2015) revealed that the lack of knowledge in depth about the profession’s values and beliefs can be one possible reason for inconsistent messages about our identity. Therefore, an investment in terminology appears to be crucial to implement conceptual models so practitioners can relate to those concepts to communicate their professional reasoning and inform others what they do. Furthermore, discussions within the CoP centred on the vital role of documentation as a guide, a facilitator and as a method for developing and maintaining continuity of occupation-centred practice across service pathways. Importantly, it was felt that the time invested early in the patients’ pathways saved time in the latter rehabilitation stages and despite challenging environments dominated by a sense of urgency and the medical model, the role, value and identity of the occupational therapists were perceived to be enhanced. This insight resonates with the literature on occupational disruption and the need for models that support identity reconstruction, co-construction and adaptation over time (Brooks and Parkinson, 2021; Hammell, 2009).
In the interview analysis, terms such as ‘fear’ or ‘Am I just filling gaps’ indicated a need to strengthen occupational therapists’ confidence to apply conceptual models and their language. This supports the findings from Lee et al. (2008) and Ikiugu (2012) that therapists’ attitudes and knowledge can be a barrier to implementation. Whether conceptual models are viewed as organised frameworks that integrate concepts to guide systematic thinking and provide a shared language for discussing practice (Turpin et al., 2024) or as tools that give structure to professional practice (Polatajko and Davis, 2021), there is no rigid formula for their application. Rather, their use is shaped by the interpretations occupational therapists make in response to the realities of their practice contexts. Findings from the focus groups suggest that therapists engage with the PEOP model to some extent, particularly when they can relate to and articulate its components in support of their professional reasoning. Interestingly, even in neuroscience settings such as acute care, where applying occupation-centred practice can be challenging due to the nature of patients’ conditions, participants demonstrated that an occupation-focused approach is still possible; indeed, they acknowledged the long-term occupational adaptation needed for some neurological conditions that go beyond the acute setting. The findings are consistent with the literature asserting that occupationally grounded models facilitate continuity and coherence across care pathways (Durocher and Kinsella, 2021) and support the co-construction of goals that reflect clients’ lived experiences and aspirations (Brooks and Parkinson, 2020). The PEOP model was viewed not only as a guide for professional reasoning but also to foreground occupational therapy’s distinct contribution within an MDT often oriented toward biomedical outcomes.
Furthermore, the use of the PEOP model provided an opportunity to enhance therapists’ communication skills, including active listening, clear and open verbal communication and effective written expression (Bossers et al., 2008). Occupational therapists are encouraged to reflect on how well they adapt their communication for service users, families, carers, the multidisciplinary team, and other stakeholders, particularly in conveying the key concepts of occupation. Using an occupation-focused tool, early in the patients’ recovery journey, particularly by focusing on the person’s narrative, allows for their strengths and personal assets to be built into future and longer-term goals of therapy, which naturally reflect their occupational sought-after lives (Dunn, 2017). This includes considering how professional terminology can be tailored to describe an individual’s situation within clinical documentation and records. Therapists might also reflect on whether the MDT can fully grasp nuanced concepts such as occupational engagement. Suppose occupational therapists are expected to understand the medical and technical language used by other health and social care professionals. There should be reciprocity, respect and recognition for the terminology that underpins the profession identity (Cezar Da Cruz, 2025). A recent study reinforces the key role of language for occupational therapists to keep the occupational focus in their practices (Bennetts et al., 2025). In addition, Wilcock (1999) emphasised the need to ‘market the profession better’ (p. 7), while Polatajko (1992) highlighted the importance of naming and framing what we do. Although these observations were made decades ago, the challenge remains unresolved. Establishing and consistently using our professional language is essential not only for fostering a strong professional identity but also for clearly communicating our mission and vision to diverse stakeholders. This has significant political implications, as it enables therapists to strategically advocate for service improvements – an issue also discussed by Turner and Knight (2015).
This study echoes findings by Wenger et al. (2002), Boniface et al. (2008), Wimpenny et al. (2010) and Phillips et al. (2023), who all described critical reflective and learning spaces, such as communities of practice, as powerful tools for generating situational learning and social engagement alongside professional development. Indeed, the initial phases of implementing the PEOP model reflect the ‘engagement’ stage of change, where professionals are exposed to new ideas and begin considering how they fit into current practice (Kinney et al., 2023). This transition from resistance to routine practice reflects Prochaska and DiClemente’s (1983) stages of change model, where early hesitation may give way to internalised practice as professionals develop confidence and perceive value. The reflexivity on the experience of conducting research in healthcare settings revealed that implementing an occupation-centred practice is a continuous process, and that there are different ways for occupational therapists to interpret how it should be implemented. The study has shown that this implementation has different layers that inform an occupation-centred practice is being practised. In line with the recent study of Bennetts et al. (2025) and Ford et al. (2022), our study fostered the use of theory (model), the use of specific language (e.g., to discuss caseloads), and strategies to include the model in documentation and assessment by offering a non-standardised tool to apply PEOP in the occupational therapy process. This supports the literature that stresses the importance of ongoing dialogue, infrastructure and leadership to move from episodic change to sustained professional transformation in occupational therapy settings (Tynan et al., 2023).
Finally, this study arose from concerns raised by occupational therapists and students about a lack of professional identity and challenges to a focus on occupation in an acute hospital setting. This reality is reflected in a recent study conducted by Mangalindan and Bulan (2025) in the Philippines, which identified that the hegemony of biomedical and referral systems that were hierarchical limited the autonomy of occupational therapists, leading them to an impairment-based approach rather than an occupation-centred practice. Acknowledging this challenge, higher education plays a crucial role in educating occupational therapy students to question biomedical ways of thinking in the services in which they will work, by implementing occupation-centred practices. However, for this to be achieved, curriculum design should put occupation in the foreground of teaching, learning and assessments, which, according to Hooper et al. (2024) and Roberts et al. (2025), characterises an occupation-centred education. This initiative potentially can change the landscape of occupational therapy practice. Newly qualified occupational therapists can also be educated to implement an occupation-centred practice (Bennetts et al., 2025) and mentoring and interprofessional collaboration could be potential strategies in the advocacy for an occupation-centred practice (Mangalindan and Bulan, 2025).
Strengths and limitations
The research identified barriers to the implementation of the PEOP model in practice. Time constraints experienced by therapists, exacerbated by staff shortages, led to the cancellation of meetings and a smaller than anticipated number of participants in stage 4 of the study. These findings likely reflect the broader context of the NHS, for example, Sarre et al. (2018) noted that while both staff and their managers valued training, a significant barrier was the limited time available to participate. Another study limitation was that occupational therapists engaged with only one conceptual model. Nevertheless, the use of multiple data collection methods represents a key strength of the research, and this methodological diversity enhances the trustworthiness of the findings through both researcher and methodological triangulation. As participation was voluntary, there could be a bias towards more motivated therapists, and the findings should be interpreted with caution, as the sample may not be representative of the entire service. In addition, the small sample size, lack of detailed demographic data and single study site could present limitations to the transferability of the findings to settings beyond the NHS and beyond the UK, however, similar findings with the study conducted in Australia by Bennetts et al. (2025), where participants increased in occupational language, theoretical awareness and professional identity enhancement support the potential transferability of our findings.
Implications for occupational therapy and occupational science
Future research could explore the implementation of a more dynamic and flexible use of combined conceptual models (a multimodel approach). As noted by Wong and Fisher (2015), integrating multiple models may enhance occupation-centred assessment and intervention. Further studies could also examine how occupational therapists incorporate evidence from occupational science to inform their practice. For example, the Participatory Occupational Justice Framework (Whiteford and Townsend, 2011) or the Framework of Occupational Engagement (Morris and Cox, 2017) could provide valuable theoretical grounding for addressing broader social and occupational issues in practice. An additional valuable study would also be to evaluate the impact of the use of the PEOP on service users.
Conclusion
This study demonstrates that implementing the PEOP model in a neurosciences occupational therapy service in the UK is both feasible and impactful. When learning about and selecting a model of practice, therapists sought a practice framework that aligned with their practice setting and enhanced their professional identity. Receiving training and using communities of practice to support implementation of the PEOP improved knowledge, confidence, application, a focus on occupation, and fostered reflection and shared learning. The need for leadership to reinforce and sustain practice change was identified. The implementation of the PEOP realised the participants’ expectations; this study shows that using the PEOP enhances the professional identity, role and language of occupational therapy in an MDT setting and brings a greater focus on person-centred and occupation-centred therapy and goal setting that extends beyond the hospital or acute setting.
Key findings
Training on the PEOP model improved occupational therapists’ knowledge and confidence in its application.
Communities of practice were a useful tool for reflection and shared learning.
Implementation of the PEOP model strengthened person-centred occupation-centred practice, particularly enabling goal setting that extends beyond the acute setting.
What the study has added
Training and application of the PEOP practice model enhances professional identity and person-centred occupation-centred occupational therapy.
Footnotes
Acknowledgements
To all occupational therapists who contribute to this study.
Research ethics
This research had ethical approval from the University of Bradford and was carried out as described in the approved protocol.
Consent
All participants signed a consent form to participate in the study.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was not included at all stages of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an innovation grant from the Elizabeth Casson Trust.
Contributorship
RB led the project. RB, MT, DC and AM researched the literature and conceived the study. DC was involved in designing the surveys with input from RB, MT, AM, CW, LM and SR. DC, BR, CW conducted the data collection. CW, LM and SH organised the meetings and led the small discussion groups with RB, MT, DC and AM. All authors revised the data analysis and the final draft. All authors approved the final version of the article.