
Abstract
Introduction:
Around 3000 occupational therapists graduate annually in the United Kingdom, but evidence shows variability in their readiness for practice. This study explored multi-stakeholder perspectives on the practice readiness of newly qualified occupational therapists in the United Kingdom.
Method:
A qualitative research design with an interpretive description approach was employed. Four focus groups were conducted separately with newly qualified occupational therapists (n = 8), occupational therapy practitioners (n = 9), practice educators (n = 8) and university lecturers (n = 4). Discussions were transcribed, thematically analysed and integrated through constant comparative analysis and the researchers’ disciplinary knowledge. Revision of findings with participants enhanced credibility.
Results:
Three themes emerged: graduation marked professional rather than full practice readiness; preparedness was influenced by variability in curriculum design, placement and workplace induction, with placements being the most influential yet inequitable factor; and individual characteristics further influenced the evolution of readiness.
Conclusion:
Findings highlight the need for intentional educational design and regulation of placement quality to reduce variability and ensure equitable practice readiness across the profession. Development of a co-produced ‘Day-one OT’ competency profile provides educational programmes with clearer educational targets and offers workplaces a consistent benchmark for induction and support.
Introduction
Practice readiness is a multidimensional construct extending beyond disciplinary knowledge encompassing confidence, applied clinical skills, capacity for lifelong learning, communication, teamwork, interpersonal effectiveness, knowledge integration, person-centred care and basic management competence (Le Huray et al., 2023). Occupational therapy is a regulated health profession in the United Kingdom (UK) and around 3000 occupational therapists (OTs) graduate every year and join the workforce (Royal College of Occupational Therapists (RCOT), 2022). Graduates must meet programme, professional and statutory requirements before entering practice (World Federation of Occupational Therapists, 2016). However, newly qualified occupational therapists (NQOTs) often feel underprepared (Gray et al., 2012; Moir et al., 2021; Opoku et al., 2022; Sjoberg and Lexen, 2024). Practice readiness is a shared concern for NQOTs entering autonomous practice for the first time, clinical practitioners who receive and support them in the workplace and educators who design programmes intended to produce practice-ready graduates at the point of qualification. Research on practice readiness among OTs in the UK is limited (Brennan et al., 2024), and empirical accounts that synthesise the collective perspectives of stakeholders are even more limited. This research aimed to explore the perceptions of NQOTs, occupational therapy practitioners, placement educators and lecturers on the current state, meanings and expectations of NQOT practice readiness, educational strategies, workplace support and individualistic factors influencing practice readiness among NQOTs.
Literature review
In occupational therapy, much research on practice readiness has been carried out to understand the experiences and challenges faced by NQOTs. Studies among NQOTs from Australia, New Zealand and Sweden have reported that NQOTs do not feel fully prepared (Gray et al., 2012; Sjoberg and Lexen, 2024) and experience transition to practice overwhelming and stressful (Turpin et al., 2021). Based on a matrix review of studies about NQOT practice readiness from countries including Australia, Canada, New Zealand, South Africa, UK and United States, Moir et al (2021) found that NQOTs report challenges associated with client-related reasoning and decision-making, applying knowledge and skills to actual practice situations and managing caseload and contextual pressures. NQOTs in Australia were also found to face challenges in managing ethical dilemmas related to management focus on financial gains over quality care, client choice over therapist judgement, managing emotions (resulting from client aggression and client death), balancing legislative demands and relationship with the client and dealing with counter-productive team culture (Hazelwood et al., 2019).
Lack of a clinically oriented curriculum and preparation for certain settings were also reported in studies conducted in Australia and Ghana (Adam et al., 2014; Opoku et al., 2022; Spaseska et al., 2022). This aligns with Morley’s (2009) proposal for a university–health service partnership in the UK to bridge the education–practice gap. Practice readiness is not only shaped by university preparation, but the supports provided at the workplace, and self-strategies employed by NQOTs also play a role. Evidence-based workplace supports that are found to assist with practice readiness of NQOTs are formal supervision, informal collegial support and professional development strategies (Moores and Fitzgerald, 2017). Learning-to-practice strategies for NQOTs have also been identified and recommended based on research reported from Australia (Moores and Fitzgerald, 2017; Murray et al., 2020).
In health professions, readiness spans the education–practice continuum as an evolving trajectory rather than a fixed expectation at graduation (Swan et al., 2024). Yet, the collective perspectives of those in education and practice regarding practice readiness of NQOTs are less explored in research. This research builds on the existing knowledge of practice readiness of NQOTs from other countries and explores contemporary insights within the UK. This research integrates perspectives of diverse stakeholders involved in preparing NQOTs for successful practice. Including multiple stakeholder perspectives provides a holistic understanding of the process and ways of integrating their efforts to better achieve practice readiness among NQOTs.
Method
Research design
An interpretive description (ID) approach within an interpretivist orientation was used. ID is a flexible qualitative methodology that enables the integration of multiple strategies and triangulation of perspectives within a disciplinary framework, thereby moving beyond description towards practice-informed interpretations (Thompson Burdine et al., 2021; Thorne, 2000). In ID, disciplinary experience is used to see patterns and help generate practice-relevant interpretations (Thorne, 2025). ID methodology was particularly suited to this study, as we want to propose actionable insights to inform curricula, placements and early-career support for NQOTs, rather than construct a formal theory.
Participants
Participants were from four stakeholder sub-groups in the UK; (1) NQOTs between 6 and 12 months of post-qualification experience, (2) occupational therapy practitioners in supervisory roles, (3) lecturers from occupational therapy programmes, and (4) occupational therapy practice placement educators including apprenticeship mentors, who had supervised occupational therapy students during practice placements. All participants were qualified OTs, and if some held more than one role (e.g. lecturer and clinician, or practitioner and practice educator), they were asked to select the focus group that best represented the perspective they wished to contribute and to respond primarily from that standpoint during data collection. No minimum years of experience were required for practice educators, lecturers or occupational therapy practitioners. NQOTs who had graduated from pre-registration occupational therapy programmes (BSc or MSc) were eligible to participate.
Recruitment
Theoretical sampling (Liamputtong, 2016) was used to recruit participants from each stakeholder subgroup. This sampling strategy ensured multiple perspectives on the concept of practice readiness across educational, workplace and practice-placement contexts. An electronic advertisement with study purpose and eligibility criteria was distributed through professional mailing lists, with an invitation for eligible individuals to contact the research team. Recipients were encouraged to share the advertisement with colleagues and networks; consequently, the full extent of circulation could not be determined. Additional targeted emails were sent to university occupational therapy programmes, practice placement sites and organisations employing NQOTs. Recruitment generated a strong response with participants enrolled on a first-to-respond basis while ensuring diversity within each subgroup. Snowball sampling was used to supplement recruitment of occupational therapy lecturers. Researchers took care to recruit participants from different geographical locations and institutions, avoiding recruitment from the same workplace and sought variation in experience, clinical settings and occupational therapy training programmes. Recruitment was between October 2024 and February 2025. One NQOT participant was previously known to the lead researcher as a student at the same university, and one lecturer was known to the second author. These pre-existing relationships were disclosed at the start of the relevant focus groups and were not considered to have influenced data collection or analysis.
Data collection
Ethical approval was granted by the University of Northampton Faculty Research Ethics Committee in 2024. All participants provided written informed consent to take part in the study and to the video and audio recording of the focus groups. Four focus groups were conducted, one per stakeholder group. Focus groups could be used to facilitate complimentary and argumentative interactions so that both shared experiences of participants and individual variations could be captured (Bryman et al., 2022). The groups were planned as homogenous with respect to job roles to promote openness and free-flowing conversations (Liamputtong, 2016).
Each focus group aimed to recruit around 10 participants, providing scope for a small number of dropouts while ensuring a balance between diversity of perspectives and opportunities for individual contributions. This target was met except for university lecturers, where only six participants could be recruited. Nevertheless, this number was considered sufficient to proceed. Each focus group lasted approximately 90 minutes and was conducted via Microsoft Teams to enable participation from across the UK.
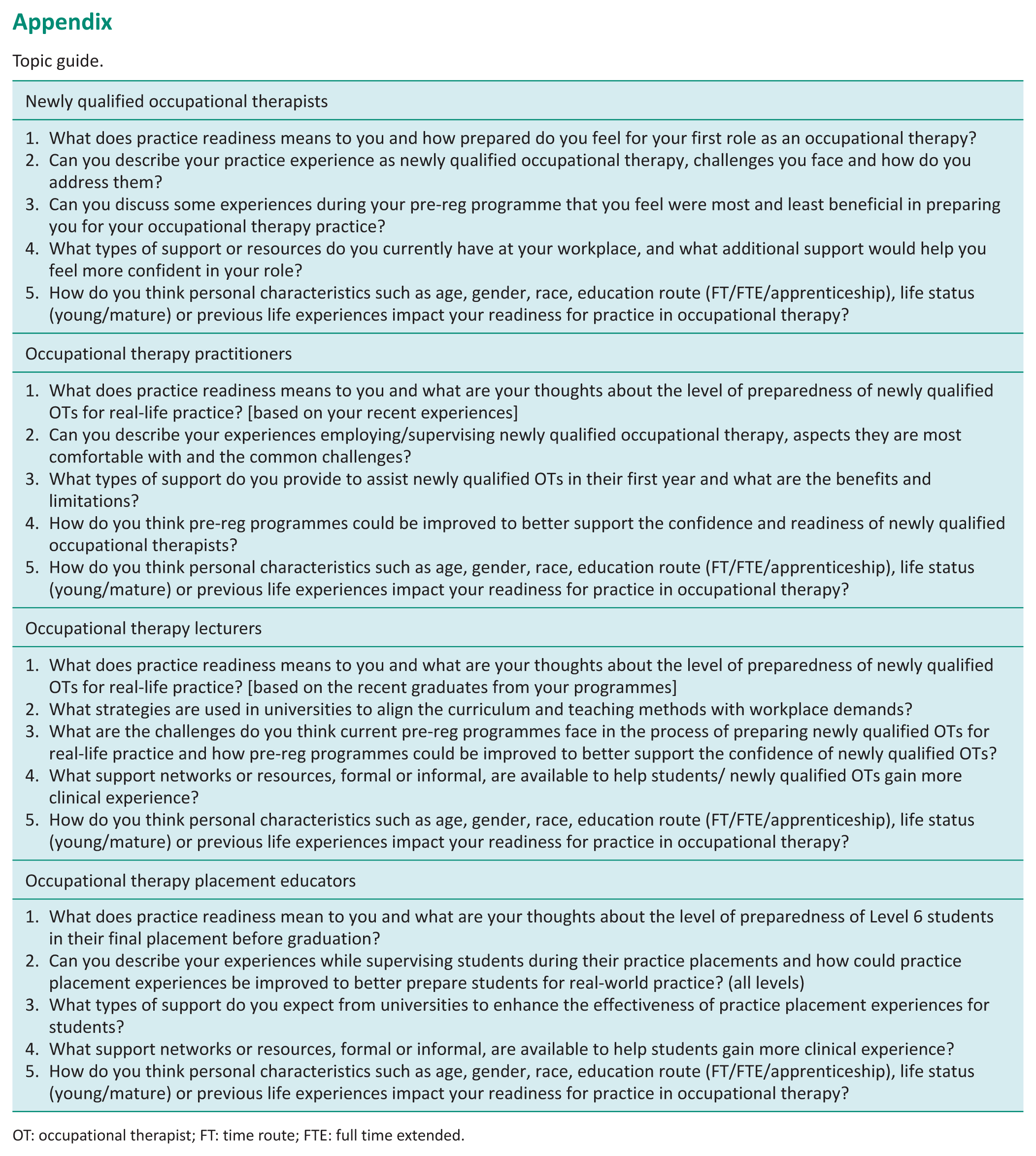
Focus groups were led by one co-author and co-facilitated by the lead author. All members of the research team were occupational therapy lecturers (three male and two female) and received training in facilitating focus group discussions with an experienced qualitative researcher. Discussions were guided by a topic guide (see Appendix) developed through a review of the available literature on the study topic and iterative discussion within the research team. The guide was then piloted with an advisory panel comprising an NQOT, an occupational therapy practitioner and a lecturer and refined accordingly to improve clarity and relevance. During the sessions, the facilitator guided the dialogue, while the lead author maintained observational notes to supplement the transcripts. Sessions were audio/video recorded, transcribed verbatim with pseudonyms and recordings deleted post-analysis.
Data analysis
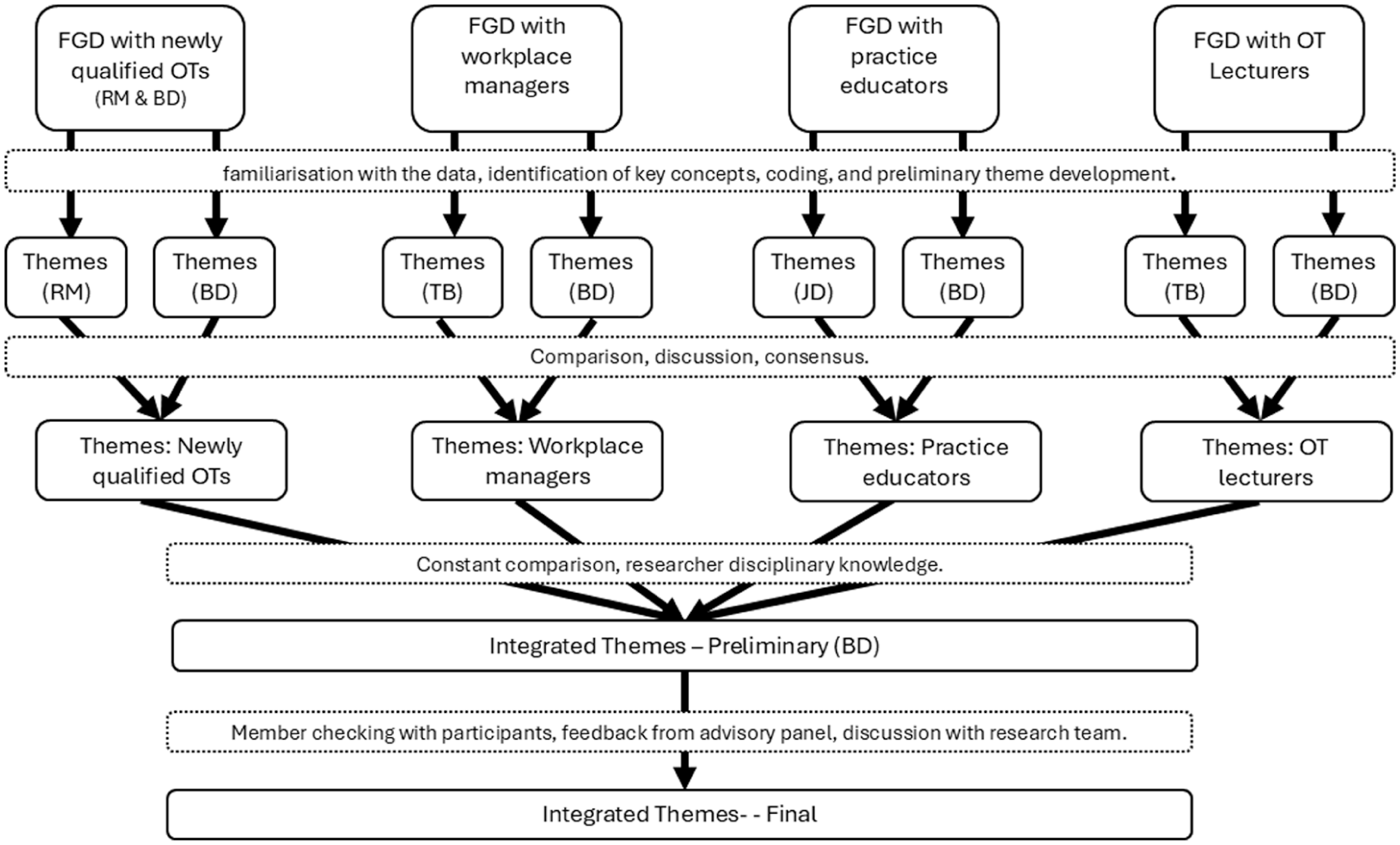
Each focus group transcript was thematically coded independently by the two researchers who facilitated the respective focus group. The analysis followed the steps outlined by Naeem et al. (2023) namely familiarisation with the data, identification of key concepts, coding and preliminary theme development. Themes were derived from the data. NVivo-14 (Lumivero) was used to code the data and support with subsequent analysis.
Subsequently, constant comparative analysis, congruent with ID was applied to refine and extend these themes (Thompson Burdine et al., 2021; Thorne, 2000). The two coders compared and discussed their coding, reaching consensus on a set of themes for each focus group. This was then synthesised through constant comparison, comparing and linking the themes from the different focus groups (Boeije, 2002) to generate a set of integrated themes.
These integrated themes were further refined through collaborative discussion with all co-authors and validated through participant feedback by sending them a draft of the findings for their feedback. This process of member checking, allowed emerging conceptualisations to be clarified, refined or challenged by research participants, ensuring both credibility and resonance with practice (Thompson Burdine et al., 2021). The overall analytic process is summarised in Figure 1.
Data analysis process.
Results
Focus group characteristics
The characteristics of the focus groups are shown in Table 1.
Focus group participant characteristics.
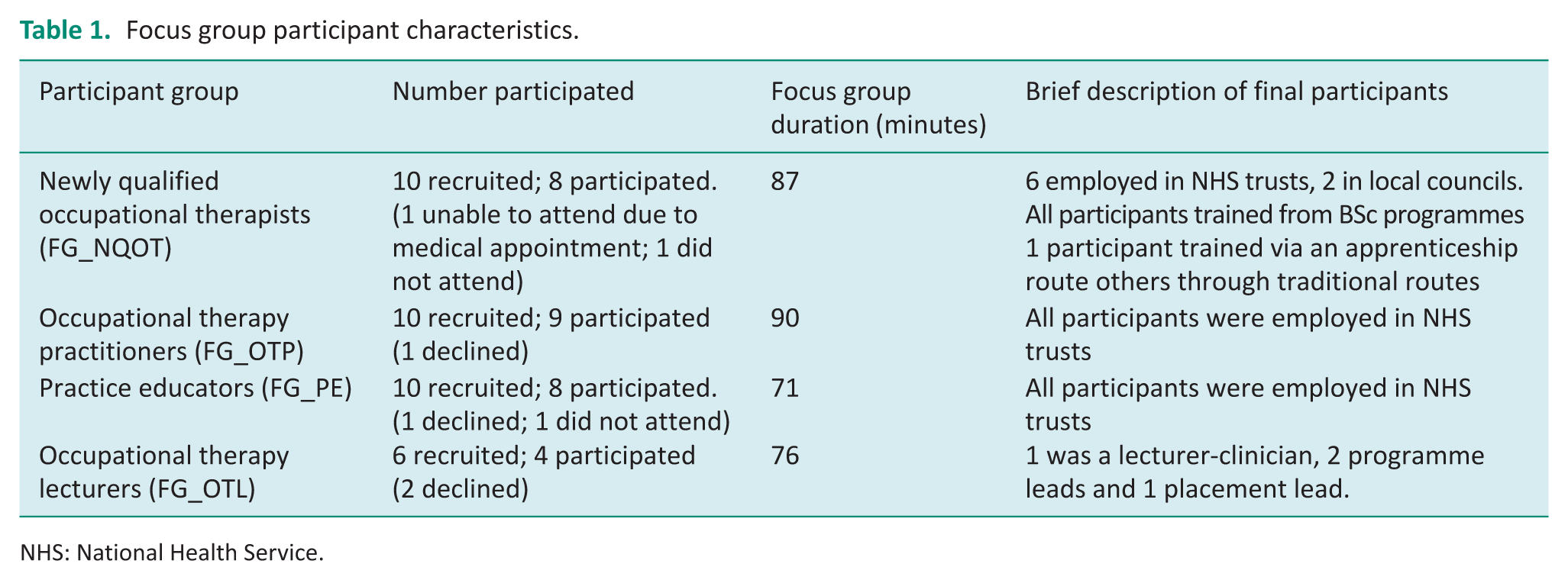
NHS: National Health Service.
Reflexivity
The lead author (BD), responsible for the study’s design, implementation, analysis and interpretation, is an internationally trained OT with practice experience in international settings. Over the past 2 years, he has been working as a lecturer in the UK. This diverse experience has shaped his understanding of practice readiness and may have influenced the interpretation of findings. Co-authors, TB, JD and RM trained and practised within the UK, and VS, trained in India, has lived, studied and worked in the UK for over two decades. CD is an educational researcher who acted as the mentor.
Several strategies were used to mitigate potential personal bias in the interpretation of data. Authors engaged in sustained data immersion and reflexive practice throughout the research process. For each focus group, coding was independently undertaken by two researchers. Draft manuscripts underwent critical review and iterative revision with contributions from study participants, advisory panel, and co-authors. These contributions provided contextual grounding and ensured that the analysis and interpretation reflected all perspectives.
Integrated themes
Themes from the individual focus groups are presented in Supplemental Material. Three integrated themes were identified, with theme two comprising two sub-themes.
Theme 1: Practice-ready or profession-ready?
This theme highlights how stakeholders debated what it means to be ‘practice ready’ and generally felt that practice readiness is unrealistic at the point of graduation due to the breadth of occupational therapy practice settings.
Consider the following reflections from an NQOT: ‘You can’t understand all the different areas, they are so, so broad. . . even with all the placements there is no way you can get your head around and be competent in all the different areas’. (FG_NQOT_P5)
NQOTs indicated that confidence emerges over time through practice experience rather than being fully established at graduation. Lecturers agreed that practice readiness evolves through lifelong learning, practical experience and reflection and emphasised that normalising the reality among NQOTs that no one is fully ready on graduation is essential. They pointed out that OTs work in varied contexts, each with unique demands and required competencies and practice stakeholders may prioritise different skills. Additionally, they described ongoing tensions between occupational therapy’s conceptual foundations on occupations prioritised in educational settings and practical demands, often resulting in a mismatch. The following quote from a lecturer summarises the point.
‘. . .from my perspective there’s this huge tension between from an educational perspective returning to our roots of occupation and promoting occupation focussed practice and really philosophical thinking and thinking skills that allow application across society more broadly; and practice partners who want the OT that is ready for that band 5 position, wherever that is, whether that’s in acute mental health or community rehab or physical acute. Your description, (quoting another participant), of a rock and a hard place, from my perspective every practice partner thinks that they are it, that all settings are like them. So they are like, ‘You are not preparing the students’. Well no, because there’s another 500 different settings and it’s impossible’. (FG_OTL_P1)
The four stakeholder groups attached slightly different meanings to practice readiness. According to NQOTs, practice readiness entails confidence in managing caseloads, understanding the occupational therapy’s role, clinical-reasoning and problem-solving. Lecturers described readiness as an openness to continuous learning and supporting clients with humility. Practice educators highlighted embedding professional identity and values, demonstrating initiative and problem-solving abilities, engaging in independent reflective learning, confidently communicating within multidisciplinary teams, advocating for occupational therapy and progressing towards professional autonomy as indicators of practice readiness. In addition to clinical reasoning, reflective practice, autonomy, accountability, people-focused and managerial skills and confidence, occupational therapy practitioners emphasised foundational knowledge and skills in the occupational therapy process and clear awareness of professional boundaries as entry-to-practice expectations. One practitioner described this as follows: ‘What I would expect to see with practice readiness is a good foundation with a good grounding and knowledge and skills within the basic OT process, being able to apply it within different settings. have those clinical reasoning skills that they are starting to build from the experience that they’ve had already and be a reflective practitioner’. (FG_OTP_P4)
There was a notable absence of discussion among lecturers, NQOTs and practice educators about mastery of occupational therapy interventions as a defining component of practice readiness. However, this issue was evident in practitioners’ focus group discussions, where they reflected on the implications of being unready for practice upon graduation. They described NQOTs as frequently unprepared for the realities and demands of professional practice, highlighting insufficient practical experience, deficits in applied practice and gaps in non-technical skills (e.g. communication, leadership, reflection and self-directed learning). Practitioners linked these gaps to feelings of inadequacy and distress among NQOTs, high attrition and sickness rates, additional pressure on senior staff expected to provide support, unfavourable comparisons with other professions and additional time spent on training. One practitioner expressed this as follows: ‘I think my experience is probably quite similar to everybody else’s. . .. because a lot of the time they are not [ready for practice] and they are really struggling. There are more and more with lots of anxiety over it, becoming unwell. They don’t know how to cope; they don’t know what to do. It just turns into an absolute panic and our sickness is increasing with that as well’. (FG_OTP_P2)
These experiences were corroborated by NQOTs, who reported feelings of being undervalued, overwhelmed, embarrassed, inadequate, intimidated, lonely, unready, lacking confidence, out of their depth, worried and experiencing imposter syndrome. Consider the following statement by an NQOT: ‘And I was just like, Oh my god. . .. it was really, really overwhelming and I found that really difficult. I did not feel ready to – that was real, I’m so out of my depth here; I don’t know what I’m doing here’. (FG_NQOT_P3)
Together, our participant narratives implied that practice readiness at the point of graduation is an unrealistic expectation and is not currently evident among many new occupational therapy graduates. Instead, stakeholders’ discussions revealed a more attainable expectation at graduation: an emerging professional identity and reasoning, embedded occupational therapy values and transferable management skills, which we term ‘profession readiness’.
Theme 2: Practice readiness – Shaped by chance or intentional design?
The themes from the individual focus groups highlighted the variations in the developmental journey of practice readiness beginning even before university enrolment, with the individuality of each candidate including their life experiences, maturity, personality and background shaping their capacity for readiness. After entering university, further variation arises through differences in academic curricula, the depth and focus of theoretical versus practical content and, notably, the diversity of placement experiences and skills training opportunities. In the workplace, NQOTs are faced with further variability, in the form of differing expectations, induction processes and the level and nature of support available. These inconsistencies can have a profound impact on early professional experiences, often resulting in feelings of inadequacy, heightened stress and at times increased sickness, absence or attrition. These challenges also place significant demands on workplace resources and support systems.
The variability in educational experiences was summarised by a practice educator: ‘I feel like every university’s curriculum is so different, or programme is so different, and where the students are at. So every time a student comes it’s about actually trying to figure out on what level they are, to then be able to provide the right level of support for that placement to get out where we were’. (FG_PE_P2)
Practice educators in our research described numerous learning opportunities available to students during placements that are designed to expose them to the realities of occupational therapy practice, support their transition into employment and foster professional identity and multidisciplinary collaboration. These opportunities extend beyond routine clinical tasks, encouraging broader skill development and professional networking. Compare these rich experiences with the following account from an NQOT that offers a stark contrast highlighting the variability that can characterise placement experiences: ‘I didn’t get an awful lot of placements; I didn’t get a mental health placement. My first placement was purely remote – I saw an occupational therapist who worked in forensic, but I only saw him for an hour once a week, that was all we got. The rest, it was 240-odd hours of us just essentially filling our time with whatever’. (FG_NQOT_P8)
These findings show that practice readiness is shaped as much by circumstances (emphasis in curricula, available placements) as it is by deliberate educational design. We argue that this variability is neither inevitable nor desirable. Instead, curricula and placements should be purposefully orchestrated to provide a coherent, progressively layered preparation for practice. The following sub-themes provide insights from our participants on how such intentional design could be realised based on stakeholder-informed curriculum enhancements.
Sub-theme: Practice-ready education
NQOTs identified educational strategies they found highly beneficial such as simulated learning scenarios, case-based learning and meaningful involvement of service users and recent graduates in teaching sessions which could be utilised more in the curriculum.
Gaps in foundational knowledge, particularly anatomy and physiology, were a major concern ‘. . .But you need to have a basic idea of anatomy and physiology. And it’s so unfair when – as I’ve said, when you are newly qualified you do compare yourselves to newly qualified physio[therapist]s, and they know so much and you feel like an absolute idiot. You are going to MDT with doctors and you’ve got no idea what they are talking about, “What condition? What does that mean?” You just feel so out of depth and you feel so angry about the institution that you’ve just come from, like, “How have they allowed this to happen?”’ (FGD_OTP_P7)
Manual handling training was another area where NQOTs expressed feeling significantly underprepared, a sentiment that resonated strongly with workplace managers. Participants also noted a pronounced imbalance between physical and mental health training and an excessive focus on theory at the expense of practical skills.
NQOTs also critiqued pedagogical approaches such as independent group work, which they felt lacked adequate tutor guidance; overly generic modules (e.g. professional development) and activities (e.g. crafts or play) that they perceived as disconnected from contemporary occupational therapy practice; and the limited authenticity of multidisciplinary education. The heavy emphasis on theoretical models, with little opportunity to translate these into practice, was a recurring point of frustration ‘We also learned an awful lot on models, which I don’t use and a lot of the qualified OTs I speak to don’t very often use models. It’s very heavily focussed on at [university name] and all the different lecturers have their favourite models so you ended up doing a lot on their [lecturers’] favourite ones’. (FG_NQOT_P7)
Practice educators voiced concerns about the timing and impact of academic pressures, such as incomplete dissertations or assignments carried into placement settings, disrupting students’ capacity to fully engage in practical learning. They also called attention to the unique support needs of international students, advocating for more robust mental health and academic support mechanisms from universities.
Occupational therapy practitioners offered suggestions for curricular improvements, including enhanced training in manual handling, equipment proficiency and greater familiarity with standardised assessments. They emphasised the need for development of organisational skills, such as diary management, scheduling and multitasking, alongside practical preparation for job applications and professional interviews.
Lecturers described a range of strategies in use to bridge the theory-practice gap. These included incorporating experiential methods such as simulations, case studies and real-world scenarios; strengthening reflective practice; integrating placement experiences with coursework; structured pre- and post-placement feedback to reinforce practical application of theoretical learning; and involvement of service users, alumni and practising clinicians in curriculum design.
In addition, lecturers highlighted preparing students for future practice by enhancing digital literacy and introducing emerging healthcare technologies such as virtual reality and artificial intelligence. Initiatives such as CV and interview workshops, employability days with external organisations and opportunities for paid work (e.g. temporary staff roles) were seen as critical for easing the transition into practice. There was agreement on the value of generalist skills training to foster adaptability, resilience, flexibility, social skills and well-being as a foundation for professional growth.
Intentional curriculum design, directly informed by such stakeholder experiences and insights, could narrow the existing gaps between academic preparation and the realities of professional practice, ultimately leading to better prepared NQOT graduates.
Sub-theme: Placement-based learning
NQOTs underscored the critical role placements play in their preparedness for practice, with some participants strongly advocating for an increased emphasis on practical placements over theoretical modules.
‘But just echoing what some of the others have said about placements, that was where [clinical placement] I learned the most and it was definitely the most beneficial. I think, should be more placements and less theory’. (FG_NQOT_P7)
NQOTs viewed placements as pivotal experiences where theory is translated into actionable skills, professional identities are consolidated and clinical confidence develops.
Occupational therapy practitioners expressed concerns about limited placement opportunities, which restrict vital clinical exposure before graduation.
‘And then in terms of professional practice, because the placements are so limited for such a practical profession that we are in, it doesn’t help with that clinical understanding’. (FG_OTP_P8)
Participants frequently described the quality and variety of their placement experiences as a matter of ‘luck’, highlighting inconsistencies in preparation and skill acquisition among graduates.
‘So I [NQOT] was really lucky with the ones that I got, so I was able to go into community inpatient as well as a neuro one as well. So I was quite lucky in that aspect of things, which I think definitely prepared me initially to going into full time [job]’. (FG_NQOT_P6)
Role-emerging placements, where students practice independently without direct on-site occupational therapy supervision, drew mixed reviews. While valued by some NQOTs for fostering autonomy, initiative and service development skills, practice educators and workplace managers raised concerns regarding limited exposure to critical occupational therapy processes and inadequate role-modelling opportunities. A practice educator captured this tension: ‘. . .that there’s a huge gap between learning from OTs in the context where OTs work and seeing the actual work being done in front of you, and then the opposite of that’. (FG_PE_P6)
Lecturers discussed ongoing collaborative efforts with regional universities to standardise placement assessments and outcomes, guided by the Royal College of Occupational Therapists (RCOT) career development framework, to ensure comparable learning experiences. An example collaborative initiative was described as: ‘we’re working very closely with [four university names] to develop a single placement assessment paperwork so that we can better prepare those students. So wherever they train actually doesn’t matter because they are all going to be based on that [RCOT] career development framework. So then when they go into practice, hopefully irrelevant of where they trained within (a region), they’ll all be trained in a very similar way and they’ll all be assessed in a very similar way’. (FG_OTL_P4)
Practice educators highlighted their role in supporting reflective practice, promoting autonomous decision-making and offering structured supervision to maximise learning. Additionally, educators emphasised exposing students to authentic practice scenarios encompassing patient management, prioritisation and manual handling skills: ‘I think from our perspective, as well as especially the last couple of weeks for the final placement, is to give them the opportunity to experience that autonomous working, so maybe taking a slight step back from that intense direct supervision’. (FG_PE_P2)
They also recommended enhanced pre-placement preparation by universities. Specific suggestions included clearer communication of placement expectations, improved support for international students and tailored screening processes to ensure appropriate placements for students requiring accommodations.
Theme 3: Path to practice readiness – Is it the same for every student?
Themes concerning individuality arose prominently across all four focus groups. The discussions highlighted the significant impact of individual characteristics on practice readiness, particularly the role of maturity (not same as chronological age) and apprenticeship routes.
NQOTs who possessed substantial prior work and life experience exhibited enhanced interpersonal skills and were perceived as more prepared for practice compared to peers entering directly from college. Practice educators and occupational therapy practitioners explicitly commended the performance of NQOTs trained via apprenticeship pathways. Conversely, lecturers identified challenges associated with the apprenticeship route, notably the necessity for apprentices to engage in processes of ‘un-learning’.
Additional factors included international backgrounds, familial connections to healthcare professions, specific personal capabilities such as driving skills and neurodiversity.
Lecturers proposed the adoption of tailored or triaged educational approaches to meet the distinct needs of various cohorts, such as apprentices, full-time undergraduate students and pre-registration master’s students. The following example underscores the limitations of uniform learning activities for cohorts with heterogeneous prior experience, highlighting the need for more differentiated training ‘we’re involved in this brilliant project called [project name], where our first- and second-year students are allocated a family with [a condition] and they do three visits a year. It’s linked to the curriculum and they have to write a reflection and that then forms the basis of their personal tutor meetings, discussing the reflection. . .. And the students, the diversity of experience of the students is insane isn’t it? So you get somebody that can’t speak to somebody, to somebody that’s been working in crisis services for 30 years and decided to train. And you can never get positive feedback from either/or can you, because you are doing a generic set of training’. (FG_OTL_P1)
Discussion
This study examined multi-stakeholder perspectives on the practice readiness of NQOTs. Our findings concerning entry-to-practice experiences, workplace support and individual determinants resonate with prior research in other disciplines (Masso et al., 2022; Mirza et al., 2019; Wynne et al., 2024). Further, our study identified the need for minimum expectations for readiness at graduation and reducing variability in educational and placement experiences through more intentional, regulated design.
The framing of graduation as the beginning of a supported transition into practice, alongside the recognition that practice readiness is unrealistic at graduation, is echoed in prior literature (Swan et al., 2024). However, they raise an important question: should the notion that practice readiness at the point of graduation is inherently unrealistic be passively accepted or should regulatory and educational bodies collaborate with practice settings to establish a clearly defined set of minimum competencies for entry to practice. Brennan et al. (2024) note the paucity of occupational therapy-specific research on practice readiness in the UK while emphasising the need for allied health professionals to deliver safe and effective care from day 1 for better patient outcomes, practitioner well-being and workforce retention. Consistent with this, workplace managers in our study described consequential gaps in applied skills and non-technical capabilities that burden teams and distress NQOTs.
In the UK, occupational therapy education is delivered primarily by universities, with clinical learning undertaken through placements. Although programmes are approved against RCOT and Health and Care Professions Council standards (Health and CareProfessions Council, 2022; RCOT, 2019), substantial variation persists across universities. Considering the variability present at each stage (admission, educational experiences and workplace transition), the question arises: To what extent is practice readiness a product of chance rather than intentional design? The substantial variation in placement experiences expressed by participants in our study raises concerns about equity in professional preparation and suggests that some graduates may enter the workforce with advantages over others. A content analysis of 108 healthcare studies found readiness to practise strongly associated with clinical and social experiences and competencies typically consolidated through placements rather than classroom learning alone (Le Huray et al., 2023). Consistent, high-quality placement experiences integrated thoughtfully within occupational therapy education are vital for ensuring graduates are adequately prepared for professional practice.
A further challenge in occupational therapy education is aligning occupation-centred curricula with the realities of medical settings where most of our participants were based. Participants described a tension between the theory taught in universities and what is immediately required on hospital wards. This divergence may, in part, reflect the broader epistemological transition within the profession from impairment-focused biomedical models towards holistic, occupation-centred practice (Dove et al., 2022). However, biomedical knowledge and scientific credibility are often seen as a prerequisite for professional recognition and integration in medical settings (Wynne et al., 2024), and under-preparation of NQOTs in these domains could make them feel less confident than peers from other health professions as reflected in our participant narratives. While an occupation-focused curriculum is fundamental and of critical importance (Yerxa, 1998), an overemphasis on occupational models in pre-registration programmes at the expense of biomedical knowledge may leave graduates less prepared for medical settings, potentially contributing to a reduced occupational therapy presence in these contexts. Therefore, it is imperative for universities and professional bodies to strengthen curriculum alignment with clinical realities, supporting practice educators and advocating for the distinctive value of occupational therapy within multidisciplinary teams. Recent research suggests that universities need to evaluate and adapt curricula to better prepare NQOTs for clinical practice (Sjoberg and Lexen, 2024). Finally, the pathway to practice readiness is influenced significantly by individual factors while current undergraduate occupational therapy programmes typically offer limited differentiation. Targeted learning experiences could help to bridge this gap by supporting less experienced students while ensuring that the expertise of more experienced students is used effectively.
Researchers in the nursing profession caution against placing responsibility for attaining practice readiness solely on universities and new practitioners and argue for ‘system readiness’ in which health services are more equipped with onboarding and continuously supporting novices (Swan et al., 2024). Extending this perspective to occupational therapy, our findings suggest that without a clear articulation of graduates’ baseline capabilities, workplaces struggle to calibrate support effectively. We therefore propose a co-produced ‘day-one occupational therapy’ profile that specifies minimum competencies at graduation, enabling universities and employers to align curricula, induction, supervision and preceptorship around a shared standard.
Strengths and limitations
Conducting only one focus group for each subgroup (NQOTs, occupational therapy practitioners, practice educators and lecturers) restricted the depth and breadth of the findings. Additional groups might have uncovered further nuances. While purposive sampling achieved the minimum number for a viable discussion, the lecturer group fell below the target. Participants volunteered after seeing email adverts, favouring individuals who were motivated or had strong opinions about practice readiness. Voices of less engaged stakeholders may, therefore, be under-represented. Moreover, detailed participant characteristics such as age, gender, ethnicity, prior work experience, neurodiversity or training institution were not collected, and these factors may have influenced participants’ accounts in ways that could not be examined. Online groups increased geographical reach but may have constrained natural interaction and excluded those with limited digital access. Another limitation is that researcher bias, including pre-existing assumptions about practice readiness, may have influenced data generation and interpretation. Although reflexive procedures and member checking were used, this potential bias may have shaped the emphasis of the findings and, consequently, the conclusions drawn.
Recommendations
Based on our findings, we would recommend active discussion and additional research on
Co-development of a minimum competency framework, such as a ‘Day-one occupational therapy’ profile, may provide a consistent benchmark for induction and support of NQOTs.
Rebalancing curricula by expanding practical skills training, reducing excessive theory and greater involvement of NQOTs and clinicians in design and delivery could support practice readiness.
Structuring placements intentionally, exposure to core practice settings, regulated role-emerging sites and extra clinical opportunities for school-leavers might improve the quality of practice preparation.
Tailoring education and placement pathways to learner profiles through differentiated tracks and/or modules for apprentices, international students and less experienced entrants might improve responsiveness in meeting diverse learning needs.
Formalising stakeholder collaboration will lead to improvements and keep the education system responsive to evolving needs.
Final considerations and future directions
Our findings add new insights into practice readiness of NQOTs. Equitable access to quality placements, adequate stakeholder involvement and practical skills training to rebalance occupational therapy curriculum and innovative differentiated training based on prior experiences could contribute to a consistent standard of practice readiness.
Key findings
Graduation signifies professional, not practice readiness for occupational therapy graduates.
Placements most influence perceived preparedness. However, access and quality remain highly variable.
Differences in curriculum, workplace induction and individual learner attributes influence practice readiness.
What the study has added
Triangulating multi-stakeholder perspectives, the study evidences the expectations on practice readiness for NQOTs and reveals the variability across curricula, placements and workplace induction influencing preparedness to practice.
Supplemental Material
sj-jpg-1-bjo-10.1177_03080226261427207 – Supplemental material for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study
Supplemental material, sj-jpg-1-bjo-10.1177_03080226261427207 for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study by Brightlin Nithis Dhas, Terence Brown, Jennifer Devers, Rachel Murrill, Cristina Devecchi and Vimal Sriram in British Journal of Occupational Therapy
Supplemental Material
sj-jpg-2-bjo-10.1177_03080226261427207 – Supplemental material for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study
Supplemental material, sj-jpg-2-bjo-10.1177_03080226261427207 for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study by Brightlin Nithis Dhas, Terence Brown, Jennifer Devers, Rachel Murrill, Cristina Devecchi and Vimal Sriram in British Journal of Occupational Therapy
Supplemental Material
sj-jpg-3-bjo-10.1177_03080226261427207 – Supplemental material for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study
Supplemental material, sj-jpg-3-bjo-10.1177_03080226261427207 for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study by Brightlin Nithis Dhas, Terence Brown, Jennifer Devers, Rachel Murrill, Cristina Devecchi and Vimal Sriram in British Journal of Occupational Therapy
Supplemental Material
sj-jpg-4-bjo-10.1177_03080226261427207 – Supplemental material for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study
Supplemental material, sj-jpg-4-bjo-10.1177_03080226261427207 for Practice readiness of newly qualified occupational therapists in the United Kingdom: A multi-stakeholder qualitative study by Brightlin Nithis Dhas, Terence Brown, Jennifer Devers, Rachel Murrill, Cristina Devecchi and Vimal Sriram in British Journal of Occupational Therapy
Footnotes
Appendix
Topic guide.
| Newly qualified occupational therapists |
|---|
| 1. What does practice readiness means to you and how prepared do you feel for your first role as an occupational therapy? 2. Can you describe your practice experience as newly qualified occupational therapy, challenges you face and how do you address them? 3. Can you discuss some experiences during your pre-reg programme that you feel were most and least beneficial in preparing you for your occupational therapy practice? 4. What types of support or resources do you currently have at your workplace, and what additional support would help you feel more confident in your role? 5. How do you think personal characteristics such as age, gender, race, education route (FT/FTE/apprenticeship), life status (young/mature) or previous life experiences impact your readiness for practice in occupational therapy? |
| Occupational therapy practitioners |
| 1. What does practice readiness means to you and what are your thoughts about the level of preparedness of newly qualified OTs for real-life practice? [based on your recent experiences] 2. Can you describe your experiences employing/supervising newly qualified occupational therapy, aspects they are most comfortable with and the common challenges? 3. What types of support do you provide to assist newly qualified OTs in their first year and what are the benefits and limitations? 4. How do you think pre-reg programmes could be improved to better support the confidence and readiness of newly qualified occupational therapists? 5. How do you think personal characteristics such as age, gender, race, education route (FT/FTE/apprenticeship), life status (young/mature) or previous life experiences impact your readiness for practice in occupational therapy? |
| Occupational therapy lecturers |
| 1. What does practice readiness means to you and what are your thoughts about the level of preparedness of newly qualified OTs for real-life practice? [based on the recent graduates from your programmes] 2. What strategies are used in universities to align the curriculum and teaching methods with workplace demands? 3. What are the challenges do you think current pre-reg programmes face in the process of preparing newly qualified OTs for real-life practice and how pre-reg programmes could be improved to better support the confidence of newly qualified OTs? 4. What support networks or resources, formal or informal, are available to help students/ newly qualified OTs gain more clinical experience? 5. How do you think personal characteristics such as age, gender, race, education route (FT/FTE/apprenticeship), life status (young/mature) or previous life experiences impact your readiness for practice in occupational therapy? |
| Occupational therapy placement educators |
| 1. What does practice readiness mean to you and what are your thoughts about the level of preparedness of Level 6 students in their final placement before graduation? 2. Can you describe your experiences while supervising students during their practice placements and how could practice placement experiences be improved to better prepare students for real-world practice? (all levels) 3. What types of support do you expect from universities to enhance the effectiveness of practice placement experiences for students? 4. What support networks or resources, formal or informal, are available to help students gain more clinical experience? 5. How do you think personal characteristics such as age, gender, race, education route (FT/FTE/apprenticeship), life status (young/mature) or previous life experiences impact your readiness for practice in occupational therapy? |
OT: occupational therapist; FT: time route; FTE: full time extended.
Acknowledgements
The authors wish to express their sincere gratitude to all participants for generously sharing their time and insights. We would also like to thank the advisory panel members for their valuable guidance throughout the project and support with recruitment. Special thanks are extended to the Royal College of Occupational Therapists for their funding towards this research and University of Northampton for supporting the study’s delivery. This study is supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration Northwest London. The views expressed are those of the author and not necessarily those of the NIHR or the Department of Health and Social Care. The funding body played no part in the design of the study and collection, analysis and interpretation of data and in the writing of the manuscript.
Research ethics
Faculty of Health and Society Research Ethics Committee, University of Northampton. Reference No: FHSHEA000419. Approval year: 2024
Consent
All participants provided electronic written informed consent prior to data collection.
Patient and public involvement of data
An advisory panel comprising a newly qualified occupational therapist, a university lecturer and an occupational therapy manager was convened at the outset of the study. The panel contributed to development of the topic guide and participant recruitment and, on a voluntary basis, provided feedback on the findings.
Data availability
Due to ethical issues, data underpinning this publication cannot be made openly available. Due to the nature of the focus group discussion data, there is a remote chance that participants could potentially be identified from the transcripts. However, data could be provided upon request. Further information about the data and conditions for access is available from the University of Northampton Research Explorer at ![]() .
.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was undertaken with the support of a Research Career Development Grant from the Royal College of Occupational Therapists Research Foundation awarded in 2024.
Contributorship
BD conceptualised and administered the study. Methodology was selected by BD with inputs from VS and CD. BD, TB, JD and RM were involved with investigation and formal analysis. BD wrote the original draft that was revised with inputs from TB, JD, RM, CD and VS; BD and TB were involved in funding acquisition.
Supplemental material
Supplemental material for this article is available online.