
Abstract
Introduction:
Although occupational therapists work within mental health settings, there is limited research regarding their role in seclusion. This study aims to explore occupational therapists’ experiences of delivering occupational therapy in seclusion whilst working as part of a multi-disciplinary team.
Method:
An exploratory qualitative approach using a semi-structured virtual interview approach was adopted. A convenience sample of six participants with experience of working in inpatient mental health seclusions settings were recruited at a national level. Interviews were recorded, transcribed verbatim and analysed using reflexive thematic analysis.
Findings:
Four key themes were identified: (1) the perception of seclusion as a punitive approach, (2) the role of occupational therapy in improving the patient’s journey through seclusion, (3) grading and adapting occupations to manage risk and increase engagement, and (4) promoting the role of occupational therapy in seclusion.
Conclusion:
Occupational therapists can play an important role in improving the experience of patients in seclusion. They have unique skills that enable them to work in this challenging environment. It has also highlighted the lack of understanding about occupational therapy within the multi-disciplinary team and how important it is for occupational therapists to promote their role.
Keywords
Introduction
Seclusion is defined in the Mental Health Act Code of Practice as ‘the supervised confinement and isolation of a patient, away from other patients, in an area from which the patient is prevented from leaving’ (Department of Health, 2015: 300). Seclusion should only be used ‘where it is of immediate necessity for the purpose of the containment of severe behavioural disturbance’ and should only be used for as short a time as possible (Department of Health, 2015: 300). There is a lack of research that demonstrates the effectiveness of seclusion (Nelstrop et al., 2006), and in recent years, seclusion has been highlighted as traumatic and potentially causing harm to patients (Askew et al., 2020). For example, previous studies exploring the impact of seclusion have reported negative physical and psychological effects (Brophy et al., 2016; Kontio et al., 2012), sensory deprivation (Mellow et al., 2017) and occupational deprivation (Allikmets et al., 2020). Occupational deprivation is defined as ‘A state of preclusion from engagement in occupations of necessity and/or meaning due to factors that stand outside the immediate control of the individual’ (Whiteford, 2000: 201). Occupational deprivation can have long-term effects such as difficulty structuring time, social exclusion and difficulty reintegrating into the community (Whiteford et al., 2019). The Care Quality Commission (CQC) has recognised that seclusion can be detrimental with seclusion rooms often not fit for purpose (CQC, 2020) and a lack of suitably trained staff to provide specialist care (CQC, 2019). Additionally, studies have revealed that most patients who spent time in seclusion reported it to be a negative experience, sharing feelings of humiliation, fear and abandonment (Haw et al., 2011). Keski-Valkama et al. (2010) found that over half of patients believed seclusion is used as a punishment for their behaviour. In light of this, researchers and practitioners have advocated for the reduction of restrictive practice and the promotion of recovery orientated approaches (CQC, 2020) which can reduce the use of seclusion in mental health services (Ashcraft and Anthony, 2008). The Mental Health Act (1983) Code of Practice (Department of Health, 2015) also states that during periods of seclusion patients should be encouraged to engage in activities that are meaningful to them.
Occupational therapists are in a good position to work with patients in seclusion as they use a person-centred recovery approach to assess patient’s functional skills by promoting engagement in meaningful activity (RCOT, 2017); thus, reducing the potential for occupational deprivation (Whiteford et al., 2019). Occupational therapists are encouraged to take positive risks to support patients to make choices and to overcome barriers that prevent them from engaging in meaningful activities and not to see risk as another barrier (RCOT, 2018). Supporting patients to engage in meaningful activities can also help to maintain and develop skills and facilitates reintegration into the ward (Whiteford et al., 2019). Occupational therapy can also provide relief from the ward environment, opportunities for self-expression, a sense of purpose and reduce stress (Bryant et al., 2016). Furthermore, patients have expressed a desire for continued therapeutic relationships whilst in seclusion (Knight et al., 2023), which has been shown to reduce the need for seclusion in the future (Chieze et al., 2019).
As occupational therapists do not work in isolation, their specialist skills in meeting patients’ occupational needs make them a valuable part of the multi-disciplinary team (MDT) working with patients in seclusion (Evatt et al., 2016). One factor which is poorly understood is the role of the MDT in influencing the provision of occupational therapy to patients in seclusion. Evidence in general mental health settings suggests that the MDT is crucial to being able to perform occupational therapy roles effectively (Simpson et al., 2005). Research into the extent that the MDT is involved in decisions around seclusion suggests that the ‘full healthcare team’ is only present for half of all seclusions (Larue et al., 2010). However, the introduction of a ‘collaborative problem-solving approach’ has been shown to reduce seclusion by 98% and ‘continued active support by senior medical, nursing and allied staff’ was identified as important in the delivery of the approach (Black et al., 2020: 578–584).
Despite the growing recognition of the potential detrimental impact of seclusion and the potential role for continued therapy for patients in seclusion, there is currently a lack of national guidance in the United Kingdom on the role of occupational therapy with patients in seclusion and little research to demonstrate its effectiveness. The need for further research into the role of occupational therapy in seclusion has been recognised by the Royal College of Occupational Therapists (RCOT, 2017). This study aims to explore occupational therapists’ experiences of delivering occupational therapy to patients in seclusion whilst working as part of an MDT. It will also consider their views on positive risk taking and the barriers and facilitators to delivering occupational therapy in seclusion.
Methods
Research design
As existing research in this area is limited and due to the exploratory nature of this work, a qualitative approach independent of any specific theoretical and epistemological approach was taken. The use of semi-structured interviews allowed specific topics to be explored, but also gave researchers flexibility to follow-up or further clarify statements and allow participants to raise additional points (Braun and Clarke, 2013, 2022). This allowed for in-depth data to be gathered regarding personal experiences, beliefs and values that may be otherwise obscured by using a focus group approach (Stokes and Bergin, 2006). A reflexive and critical approach was necessary to enhance quality and credibility of the outcomes of the study (Holloway and Wheeler, 2009), which involved writing reflexivity diaries, reflective supervision, peer debriefings and verification of final themes across the multi-disciplinary research group.
Patient and public involvement and engagement (PPIE) and pilot work
PPIE is important to ensure that key stakeholder’s views and experiences are represented in the research, and that the research is focusing on the issues and potential outcomes deemed to explore the question and improve knowledge of the specific phenomenon (UK Public Involvement Standards Development Partnership, 2019). The draft interview schedule was reviewed by an advisory occupational therapist working in seclusion to help establish the validity of the interview schedule in relation to the research aims. The feedback was incorporated into the final interview schedule. Prior to formal data collection a series of face-to-face practice and pilot interviews were carried out within the project team to practice interview skills and review the semi-structured interview schedule (Holloway and Galvin, 2017).
Ethical review
As the study does not involve patients in the NHS, ethical approval was sought from the university of Southampton ethics committee via the ERGO2 online process (approval number 70887).
Sampling and participants
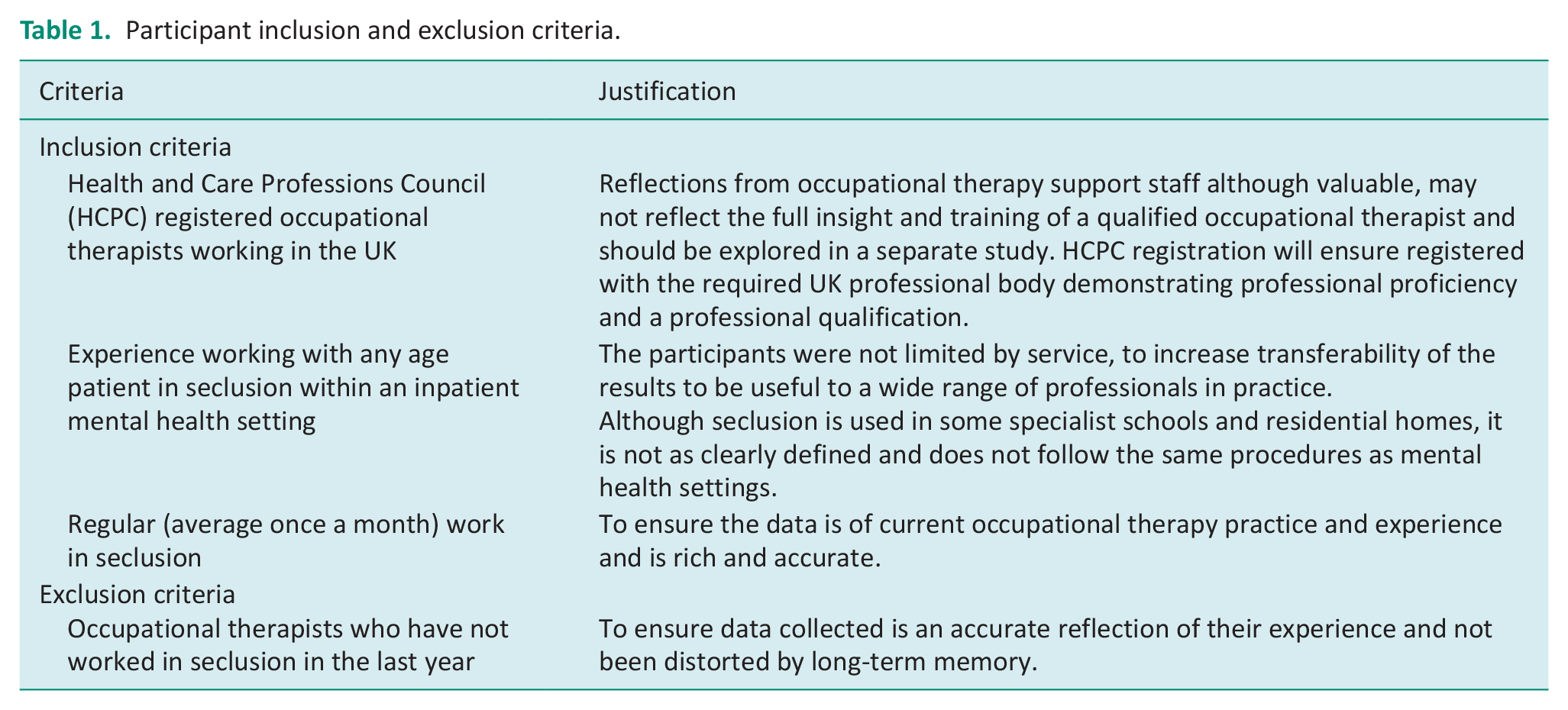
The target sample was occupational therapists working in inpatient mental health services in the UK who had worked with patients in seclusion within the last 12 months. Due to the exploratory nature of the qualitative approach and time constraints of the study, the use of convenience sampling was initially used to recruit the target sample of 6–8 participants (Hinton and Ryan, 2020). Following initial recruitment, an ethics amendment was submitted to integrate snowballing where participants were asked to share the study information with any colleagues who may be interested in taking part in the study (Etikan et al., 2016). The participant inclusion and exclusion criteria are outlined in Table 1.
Participant inclusion and exclusion criteria.
Recruitment
A study recruitment poster was advertised on specialist occupational therapy groups social media platforms including MH4OT, OT4OT and occupational therapy students: Get connected Facebook groups, as well as posting on Twitter. Key peers and supervisors were tagged into social media post to share the study details. Anyone interested in the study contacted the researchers via a study specific email address and were sent a reply slip and Participant Information Sheet (PIS) containing a full outline of the aims of the study. The PIS included the information that participants have the right to withdraw their data up to when it is anonymised, and participants were reminded of this throughout the research process. Those interested in taking part in the study were asked to provide informed written consent and their HCPC registration details. Participants were then contacted to arrange a suitable time and date for data collection. Confidentiality was maintained by ensuring that only the research team had access to the research data, which was stored securely.
Data collection
Semi structured interviews were conducted online via Microsoft Teams to enable a wide geographical range of participants and convenience for both participants and researchers. The interviews were carried out by two researchers, one asking the interview questions whilst the other remained present as support in the background (Roberts et al, 2021). The semi-structured nature of the interviews allowed the conversation to flow and for the interviewer to build up rapport with the participant by showing interest whilst remaining non-judgemental (Braun and Clarke, 2013). Interviews lasted a maximum of 90 minutes. Data were recorded on video and transcribed via Microsoft Teams and manually checked by the researcher to ensure accuracy. Data were anonymised and pseudonyms used to ensure a sense of cohesion in the data whilst upholding participant confidentiality when discussing their work, to enable an honest and true reflection of experience. Transcripts were cleaned to remove any personal identifiable data, such as place names or names of individuals, and replaced with equivalent generic terms such as ‘the ward’ or ‘a nurse’. Following transcription, the video recordings were permanently deleted, leaving only the anonymised transcripts.
Data analysis
Data was analysed using reflexive thematic analysis following the approach outlined by Braun and Clarke (2006, 2013), which provides a flexible approach to grouping and identifying meaning across the dataset (Braun and Clarke, 2013). To ensure that the participants voice was at the centre of the analysis, an inductive approach was taken, and no pre-existing theory was being used to frame the study (Braun and Clarke, 2013). All four researchers were involved in the data analysis at different stages to ensure verification of the themes and provide a rich variety of perspectives. The process involved, first, reading each transcript extensively, noting points of interest relevant to the research questions and aims. Next, each transcript was coded using NIVO software (QSR International, Melbourne, Australia) as this is a useful way to manage the dataset. Codes were then copied into Microsoft Word documents to begin the process of theming. To identify themes, codes were read and read again, reflected on and considered in relation to the research questions and aims. Identified themes were discussed, negotiated and re-worked with the research team using a series of diagrams. Finally, the whole dataset was re-read, looking for data missed or negative cases to ensure that the themes clearly reflected the data and participants voices.
Findings
Participant characteristics
Six participants took part in this exploratory qualitative study. To de-identify participants, all participants were provided with a pseudonym. Demographic data are reported in Table 2.
Demographics of participants in the study.
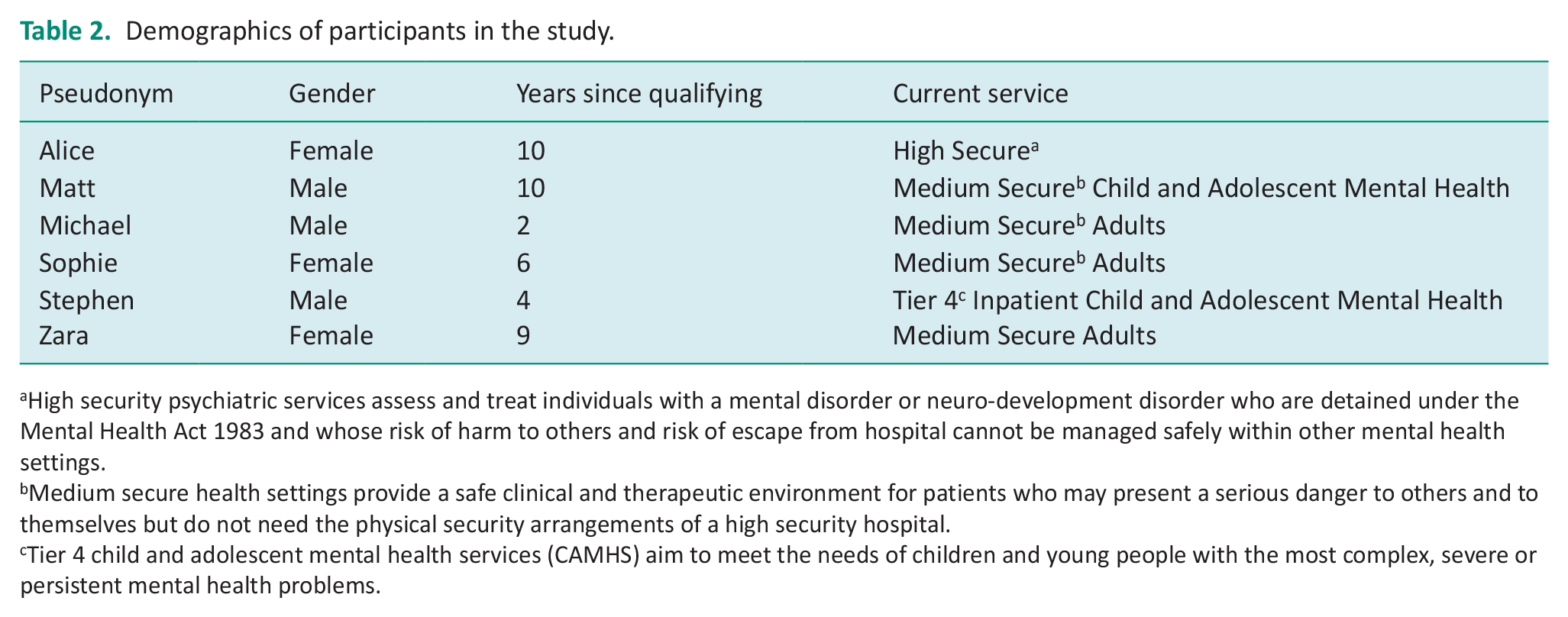
High security psychiatric services assess and treat individuals with a mental disorder or neuro-development disorder who are detained under the Mental Health Act 1983 and whose risk of harm to others and risk of escape from hospital cannot be managed safely within other mental health settings.
Medium secure health settings provide a safe clinical and therapeutic environment for patients who may present a serious danger to others and to themselves but do not need the physical security arrangements of a high security hospital.
Tier 4 child and adolescent mental health services (CAMHS) aim to meet the needs of children and young people with the most complex, severe or persistent mental health problems.
Themes
Four key themes were identified that captured the participants’ experiences of delivering occupational therapy in seclusion whilst working as part of an MDT. Table 3 provides a summary of the four themes, and then each theme is presented using a range of direct quotes from the participants.
Summary of the themes.

Theme 1: The perception of seclusion as a punitive approach
Some participants sometimes viewed seclusion as a punishment for bad behaviour or a means of behavioural control over the patient. Therefore, it was felt that it was the occupational therapist’s role to address this misconception or attitude, and explain the need for occupational therapy whilst in seclusion, as outlined by Matt.
[the MDT can] take a more punitive thought process [. . .], you know: ‘[they] have misbehaved, they need to think about what they’ve done and apologize’, [. . .] we’re [saying] the patient is clearly really struggling right now and, if anything, what they need is more input. (Matt)
Participants described how this ‘punitive view’ led to the assumption by some members of the wider team that patients should not be allowed to engage in activities whilst in seclusion. This view appeared to lead to a need for participants to clinically reason with members of the wider team to help them recognise the benefits of continuing therapeutic sessions with patients in seclusion:
[in MDT perspective] ‘[the patient is] in seclusion, so they shouldn’t really be engaging in activity’ [. . .they’re] not necessarily seeing the benefits of [therapeutic activity. . .] you’re sort of having to [. . .] argue your case a bit more for why you should be going in there and working with them still. (Zara)
Participants reflected on conversations where multidisciplinary colleagues had reacted negatively about their planned OT interventions for recently secluded patients. For example, a stressful incident or experience may have been the catalyst to the patient being in seclusion which led to a reluctance to support occupational therapy interventions. This is explained by Matt:
they’ve just seen one of their colleagues, possibly friends get hurt. And then I’m showing up with, like, some cookie dough mix and or a pack of cards going, can I go in and spend some time with someone? They’re like what? No! (Matt)
However, participants did acknowledge that other professions within the wider team had different priorities to consider in their roles such as staffing ratios, current patient needs and the safety of staff and patients on the ward. Some participants also felt that a punitive view was not held by all staff and that in some areas, this view was beginning to shift as, described by Stephen:
they’re in there for a reason. You can see them once they back out on the ward. Yeah, that has definitely shifted, because I think we’ve kind of got the message across that. . .the more interventions they have whilst they’re in there, the shorter the stay will be, the better is going to be for everyone. So that’s definitely improved. (Stephen)
Theme 2: The role of OT in improving the patient’s journey through seclusion
Whilst recognising the inevitability of some patients occasionally requiring seclusion, participants were empathic to the patient’s experience and acknowledged the possible negative side effects of restrictive environments for patients. For example, Michael felt that patients in seclusion had their
negative self-thoughts validated [. . .] by the whole situation. (Michael)
Therefore, providing adapted occupational therapy interventions was seen as a possible way of mitigating the impact and improving the experiences on several different levels. Matt discussed how therapeutic engagement illustrated to the patient that the therapist was willing and dedicated to support them
if you’ve got someone [a patient] in that situation [seclusion] and you’re willing to open that door and come in and do something with them, that says a lot in terms of your intentions and your relationship with them. (Matt)
Participants also discussed how the provision of occupational therapy in seclusion could provide a sense of consistency and routine. This was viewed as making a significant difference to patients and could help minimise the patient’s time in seclusion and support a quicker transition back to the ward or less restrictive environment, as explained by Zara.
I think it really makes a difference [. . .] to maintain some sense of normality and orientation [. . .and] thinking about how we would be [feeling] if we were stuck in a room, [. . .] you know, they’re just in that one room they haven’t got a window, so they [. . .] haven’t got like any cues as to what time of day it is or um, what the date is or what’s going on. [. . .] [we can] adapt that [therapeutic activity] and do that whilst they’re in seclusion so they’ve got that sense of normality and that routine [. . .] I think that it makes a huge difference in, in getting them out quicker. (Zara)
Participants felt that patients in seclusion environments, regardless of the risk, should continue to receive occupational therapy as they benefit from consistency of an occupational therapy presence:
I’m not trying to say I turn up with my jazz hands on [. . .] quite the opposite, but [. . .] being alone for 24 hours, having brief, minimal interaction [. . .] through a hatch and not having any stimulation [. . .] at the right sort of level is actually quite torturous if you’re completely psychotic [. . .] it doesn’t make sense to not have any. . . any kind of input. (Sophie)
Participants also felt that occupational therapy could shorten the time spent in seclusion:
we know the positive impact that can have on the young person and their time in there. [. . .] we know it does shorten the time. It does help re-integration back to the ward. (Stephen)
Some participants talked about how their therapy sessions enabled them to assess the patient’s level of functioning and feed this back to the team.
it’s also a really good way to be able to help assess somebody and how they’re doing. Because, yes, in the moment, of course, it’s really nice to be able to provide nicer things that are more purposeful for somebody and fits with them. But actually, if I can see that, that person’s managing to engage with me for so many minutes, and that’s a much better improvement than yesterday, then actually, that can be really great feedback in terms of assessment of how somebody’s improving. (Sophie)
Theme 3: Grading and adapting occupations to manage risk and increase engagement
All participants felt that patients in seclusion should have continued or increased access to occupational therapy. This contrasted with the view often held by the wider multidisciplinary team, who tended to be averse to this due to potential risks. Matt reported that nursing staff would sometimes tell the occupational therapists that they could not run their sessions stating:
they’re really risky at the moment’ [and Matt would reply] “well, let’s think about the context [. . .because] I’m talking to them right now and they seem fairly settled”. (Matt)
Some participants recognised that their views on positive risk taking were unique within the multidisciplinary team:
we’re [. . .] well placed to take positive risks because we are engaging [in things] that aren’t kind of standard for other people’s practice. (Michael)
All participants discussed the importance of positive risk taking and grading and adapting therapeutic activity to control levels of risk and support patient experiences. Alice reported that the use of clinically justified graded activity to suit individuals would lower their risk and facilitate therapeutic engagement:
I think it comes down to effective grading. [. . .] it’s about using your knowledge as a profession, your knowledge of your patient and their interests [. . .] by engaging somebody in something that is meaningful for them. You’re automatically gonna reduce their risk level anyway because it’s something that they want to engage in [. . .] so you’re able to kind of take those positive risks, but in an evidence based, structured, managed way. (Alice)
Participants also felt that using their core skills in activity analysis and grading enabled them to identify appropriate levels of task complexity in sessions and facilitated progress over time. This was explained by Sophie:
And I think occupational therapists are quite good at being able to pick out those elements and do that task analysis and all those things to try and help with finding what makes it slightly more challenging, what makes it slightly riskier. And so, it does pull on all those core skills that we have. (Sophie)
Sophie and Alice explained how they graded activities to keep them meaningful for their patients whilst eliminating the need for tools to maintain safety:
. . .he liked yoga, so we would try and do our sun salutations. . . me one side of the hatch, him the other, and we do them together. And then I do music appreciation, so I’d play the music that he wants to listen to, and then we can talk about the lyrics and things through the hatch. I read [to him] from his short stories book and then do that, “oh, what do you think is gonna happen next? (Sophie) They don’t have to have any tools or equipment to do them. So, we do a lot of kind of like collage-y type stuff, . . . playing games, playing cards. A few [patients] like baking activities as well, so a lot of them have . . . made bread, so they can use their kind of hands and . . . . we’ve done pizza making with the patients through the Hatch. (Alice)
Michael discussed how interventions could be graded to be more challenging and complex as patients transitioned out of seclusion:
looking at your more complex um, activities and engagement, so things that required kind of mild tools or non-sharp tools so your craft activities. . . that’s stuff like cooking or anything that kind of involves sharp tools and we also put group social activity into the high risk category for most people, just because it can be quite overwhelming if someone’s been in, in isolation or seclusion for a long time and to bring them out to interact in a group is quite complex. (Michael)
However, participants reported that when they graded activities the wider MDT sometimes misunderstood what they were doing as some received criticism for their sessions being overly simplistic.
Initially doing some of the lower-level sessions [. . .] there was a bit of criticism in terms of the tasks being too simple. [. . .] but then when you see over time how you can then grade that to support somebody, to engage in a more complex tasks [. . .] that helps to kind of reduce some of those criticisms. (Alice)
The majority of participants discussed the challenges of working in seclusion and the need to be creative and share the session ideas with their colleagues.
You have to be quite creative of. . . you’re doing sessions without any equipment or. . . or very limited kind of equipment. But again, [. . .] We have like, certain sessions that we’ve shared. [. . .] ‘you can try this’. (Stephen)
Some of the participants talked about adapting the length and frequency of their sessions, that they tended to be more frequent and shorter to meet the patients’ therapy needs:
. . . So every day, I’d go and see him and do one of these sessions not for very long. I see him usually around about 15 minutes-ish as a maximum. (Sophie)
Participants described minimising the risk of occupational therapy interventions by grading and adapting activities, this may begin with something as simple as talking to the person through the door.
. . .if someone is in high care or seclusion [. . .] we have some kind of interaction, whether it’s a session or an interaction with them every day. Whether that’s for short periods or for a longer period of time. [. . .] if it’s a genuine concern that it’s too risky to go in, then we’ll do something through the door. (Matt)
Theme 4: Promoting the role of Occupational therapy in seclusion
A frequent idea throughout the interviews was that there was a lack of understanding in the MDT of the role of occupational therapy in seclusion. Some participants mentioned that occupational therapists were seen as activity co-ordinators and did ‘fun stuff’ or were an ‘extra pair of hands’ (Michael). There was also a view that the occupational therapists could be used in other ways such as helping nursing staff to give medication.
You can often be seen as, well, you’re a trained member of staff. You can come in and help us . . . but I’m not gonna drop everything I’m doing because you want to go in and give them medication. (Matt)
Participants were keen to develop their professional identity, particularly in their reputation for challenging restrictive practice. Some felt that it is the responsibility of practitioners to share information about their profession. Zara felt that there was potential to improve understanding of roles and foster positive relationships between occupational therapists and wider professions through multidisciplinary collaboration as an educational experience.
Maybe [it’s] partly our fault we don’t include them enough. We don’t explain enough about what we’re doing [. . .] there’s that lack of education, that lack of understanding the benefits of OT whilst someone’s in seclusion. (Zara)
Strong clinical justification was considered important by the participants in order to successfully take positive risks and feel confident in their professional identity. Participants mentioned clear patient advocacy, session plans, risk assessments and goals when discussing their professional reasoning with the multidisciplinary team:
a lot of other disciplines, certainly from a security perspective, don’t necessarily understand the rigorous process that the OT staff have gone through in order to do [. . .] assessments with the patient [. . .] it does constantly feel like [. . .] a battle. (Alice)
Furthermore, participants discussed using accurate clinical language to underpin and evidence their practice and knowledge. They believed that their practice and interventions had reasoning and complexity that should be shared with the wider team to build understanding of the role of occupational therapy.
It’s about having our sessions recognized as key treatment, [. . .] as valuable as the medication in terms of [. . .] developing their skill set [. . .] it comes down to [. . .] clear communication and how we articulate the aims and purpose of our sessions and using [. . .] treatment language. (Alice)
Alice also talked about the importance of promoting the role of occupational therapy within MDT meetings:
We . . . promote it at the MDT meetings, we need to think quite strategically in terms of how that information is presented at your CPA meetings, your review meetings, those kinds of things. (Alice). And doing this by making sure that they use clear communication.
Matt felt that by encouraging members of the MDT to work alongside occupational therapists and seeing the effectiveness first hand they developed a better understanding.
The majority of staff really take to it. And I think the ones that don’t, when they see it work, it kind of shifts their opinion a little bit. (Matt)
Some participants spoke about the other ways in which they could promote their role and develop a better understanding in the MDT. Alice spoke positively about educating new staff as part of their induction. Stephen raised the importance of ensuring that the involvement of occupational therapy is included in seclusion protocols:
. . . the protocols [. . .] we made sure that there’s like, the OT element was included in that policy. So, in theory if a young person gets does get put in there, . . . the named OT should be notified, like, within like 24 hours. (Stephen)
Discussion
The aim of this study was to explore occupational therapists’ experiences and views of delivering occupational therapy to patients in seclusion as part of an MDT, reflecting on key barriers and facilitators. As far as we are aware, this is the first study to specifically explore occupational therapist’s views using a qualitative approach and providing a unique perspective from a sample of therapists working in mental health services in the UK.
Traditionally, occupational therapy was paused when a patient was in seclusion, but there has been a recent shift in this practice which has seen occupational therapists in the UK increasingly continuing their work during periods of seclusion (Sherwood, 2021). This shift may have been facilitated by several factors raised by participants in this research. First, participants talked about the importance of taking positive risks to support engagement in meaningful occupations which is also encouraged by the RCOT (2018). Second, participants discussed the national push for least restrictive practice in mental health settings, now a key principle of The Mental Health Act 1983: Code of Practice (Department of Health, 2015). This advises that patients in seclusion should have access to occupations to increase independence and aid recovery. Third, the participants spoke at length about their unique skill in activity analysis and grading occupations which enabled them to creatively adapt and grade activities to reduce risk whilst maintaining their meaning. This was also identified in research by Knight et al. (2023: 19) who argued that occupational therapists ‘combine their unique skills in activity analysis and grading occupations with positive risk taking which enables them to adapt occupations so that they can be safely carried out in seclusion’. Lastly, the participants in this study reported the positive impact that their input has on patients whilst in seclusion, particularly maintaining a therapeutic relationship and trust. This is supported by a study by Knight et al. (2023) that found that patients expressed the need for human connection and reported distress if this did not happen. Furthermore, participants felt that their interventions reduced length of stay in seclusion and facilitated a smoother transition back to the ward.
However, participants described a range of barriers which prevented them fully utilising the potential of occupational therapy in seclusion. Despite the acknowledgement that seclusion should be used in circumstances of severe behavioural disturbance and the advocacy for least restrictive practice (Department of Health, 2015), the participants in this study shared their views that seclusion was sometimes viewed in a punitive way by members of the wider MDT. This echoes previous work with patients who felt that seclusion was a form of punishment for their behaviour (Keski-Valkama et al., 2010). Some participants felt that this punitive undertone may have led to the restriction of activities by the wider team, which contradicts the philosophy of occupational therapy in supporting people to engage in meaningful occupations regardless of the environment and therefore made it a challenging environment to carry out their role. Given relatively recent Care Quality Commission (CQC) policy (2020) in promoting recovery-orientated approaches within mental health settings, this perhaps illustrates the need for further MDT training and the promotion of occupational therapy interventions as a vital part of this goal throughout the entire patient pathway, which will include seclusion.
Participants acknowledged that they needed to take more responsibility for promoting the role of occupational therapy. They made a range of suggestions which included clearly articulating their professional reasoning using appropriate language and referring to occupational therapy as a treatment. They also felt that encouraging members of the MDT to work alongside them helped to develop an understanding of the role. Furthermore, in order to facilitate participants recognised the need for occupational therapy to be identified as an essential intervention in national and local policy guidance.
This research has identified the important role that occupational therapists can play in improving the patient’s journey through seclusion by maintaining therapeutic relationships and facilitating their engagement in meaningful occupations. It is evident that there is good practice taking place in some areas; however, this does appear to be ad hoc in nature and is dependent on the skills of the staff and culture of the MDT. Occupational therapy practice in this field is not driven by national guidance although there do appear to be some local protocols.
There is a need for further research to evidence the therapeutic impact of occupational therapy interventions on patients in seclusion and whether there is a direct link to patients’ length of stay in seclusion. As seclusion is extremely costly due to the high levels of staffing, reducing length of seclusion would significantly reduce costs. Moreover, being in seclusion for a shorter period of time would be better for the patient themselves. Further research could also act as a driver for change and national guidance to ensure that there is access to occupational therapy for all patients in seclusion.
Strengths and limitations of the study
Due to the exploratory nature of the study and limited time constraints during the study recruitment stage, a convenience sampling approach was used. Although the use of a social media recruitment and a virtual interview approach enabled national level involvement that led to good geographical representation, the use of this self-selecting approach may have led to potential bias in terms of views on the topic area and lack of diversity of the sample. Furthermore, although the aim of qualitative research is not to generalise to the wider population, a sample size of six participants may be considered small as the target sample was HCPC registered occupational therapists working in the UK. Another limitation of the study is the absence of routine information on how frequently the participants worked in seclusion. This information would have indicated the participant’s level of experience working in this specialised setting. Due to the time constraints of the study, we were also unable to go back to the participants to offer them the opportunity to reflect and feedback on the themes. However, the data were analysed by all members of the team through an interactive verification process. As a result, the findings are considered to have a high degree of credibility and trustworthiness.
Despite the sampling approach and small sample size, the use of a rigorous and approach analytical approach has provided an in depth understanding of this under researched topic area. The themes identified could be used as a basis for thinking about potential Quality-Improvement projects, including introducing education about occupational therapy in staff inductions to improve knowledge of the role and decrease misunderstandings. However, this study needs to be considered as a starting point and further research is needed to explore the extent to which these views are held with the occupational therapy community working in this sector. Since occupational therapists do not work in isolation within seclusion, future research could explore the perspectives of the broader multidisciplinary team on the delivery of occupational therapy to patients in seclusion.
Conclusions
There is a paucity of research to demonstrates the effectiveness of occupational therapy in seclusion; furthermore, there are not any national guidelines for its provision. This research has explored occupational therapist’s views of working in seclusion with similar findings to previous studies, demonstrating the important role that they play in improving the patient’s experience. However, the role of occupational therapy remains misunderstood by the MDT, and there is a need for occupational therapists to promote their unique skills in activity analysis, grading and adapting occupations and positive risk taking which enable them to work in seclusion. There is a need for further research to evidence the outcomes of occupational therapy interventions in this challenging area which could then act as a driver for national guidance in the field.
Key findings
Grading and adapting occupations can facilitate engagement, reduce risk and improve patient’s experiences of seclusion.
Occupational therapists need to promote their unique skills as their role remains misunderstood by the MDT.
What the study has added
Occupational therapy facilitates occupational participation of people in seclusion, reducing occupational deprivation and improving their experience; however, there is a lack of national guidance and limited research on its effectiveness.
Footnotes
Acknowledgements
Thank you to all the occupational therapists who participated in the interviews. For the purpose of open access, the author has applied a Creative Commons attribution license (CC BY) to any Author Accepted Manuscript version arising from this submission.
Research ethics
As the study does not involve patients in the NHS, ethical approval was sought from the university of Southampton ethics committee via the ERGO2 online process (approval number 70887).
Consent
All participants gave written consent for their anonymised information to be shared.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship and/or publication of this article.
Contributorship
BH, RW, AB and MDH researched literature, conceived the study and developed a protocol. BH and RW gathered data. All authors conducted data analysis and wrote and edited the manuscript, approving the final version for submission.