
Abstract
Introduction:
Occupational therapists in acute practice are increasingly likely to work routinely with people in later life who drink alcohol. Therefore, this knowledge translation study aimed to evaluate the development of a continuing professional development Learn@Lunch programme, designed to enhance awareness and understanding of occupational therapists who work in an acute hospital setting, of drinking alcohol as an occupation in later life.
Method:
Guided by the Promoting Action of Research Implementation in Health Sciences framework, the continuing professional development programme was developed, and a qualitative evaluation undertaken. This included pre- and post-focus groups with occupational therapists (n = 8) in an acute setting, where the programme was delivered, pre- and post-programme delivery interviews with the research champion recruited from the site, and one interview with the Allied Health Professions Service Lead.
Findings:
Findings indicate the Learn@Lunch continuing professional development programme enhanced therapist knowledge and understanding of the changing patterns of drinking alcohol in later life. However, practical barriers exist impacting how participants perceived the value and delivery of the programme.
Conclusion:
Learn@Lunch was an effective continuing professional development programme and supported enhanced knowledge and awareness of drinking alcohol as an occupation in later life, leading to changes in local acute occupational therapy practice.
Introduction
One mechanism through which to grow therapist knowledge in practice is via translational research, moving the findings of appropriate studies into practice, for the benefit of people, as quickly and as efficiently as possible (Translational Research Institute, 2023). Knowledge translation approaches have been recognised as an important vehicle in occupational therapy through which to transfer the underpinning evidence of the profession with practice (Perkins et al., 2020). Professional education has been adopted as a method of transfer in the allied health professions, including occupational therapy, although a need to explore further the effectiveness of this approach has been indicated (Jones et al., 2015). This is set within wider recognition that knowledge translation is a complex activity due to the diverse scope of practice in which therapists are situated, including the systems in which they work (Jones et al., 2015). Consequently, this article sets out a knowledge translation study which outlines a novel approach to continuing professional development (CPD), set within an acute occupational therapy service. This educational approach to knowledge translation was designed to grow and enhance occupational therapists’ knowledge and awareness of drinking alcohol in later life.
Literature review
CPD is considered an important educational conduit through which occupational therapy practitioners can grow knowledge, including the underpinning evidence-base of practice, to enhance outcomes for people (AOTA, 2017). It has been defined as a ‘learning activity undertaken throughout life, with the aim of improving knowledge, skills and competencies within a personal, civic, social and/or employment-related perspective’ (Commission of the European Communities, 2001, p. 9). Recognition therefore exists of the need to develop innovative approaches to CPD to prepare practitioners with new skills, as practice evolves (Alsop, 2013).
One example of the need to enhance therapist knowledge connects with the changing patterns of drinking alcohol in later life, where older people are drinking at higher levels than previous generations (Barry and Blow, 2016). Drinking alcohol is now recognised as a complex and important area of concern for health practitioners when working with older adults (Karlsson and Gunnarsson, 2018), with a range of factors influencing how, when, and why people drink, including it being an integral part of social life for many, as well as a coping mechanism for others (Kelly et al., 2018). Professional research recognises addictions, including alcohol misuse, can be understood as an occupation (Wasmuth et al., 2014). Yet in practice occupational therapists are hesitant to ask older people about drinking when admitted to acute hospital settings due to the complex range of factors that influence alcohol consumption in later life (Maclean et al., 2015, 2020). This is particularly important in Scotland, one nation of the United Kingdom (UK), where approximately 93% of alcohol-related stays are to general acute hospitals and are highest in the 55–64-year age group (Richardson and Giles, 2021). The rates of alcohol-related hospital stays are now four times higher than they were in the 1980s (Richardson and Giles, 2021). Consequently, this article presents an evaluation of the development of a CPD programme in Scotland, designed to enhance awareness and understanding of occupational therapists who work in an acute hospital setting, of drinking alcohol as an occupation in later life.
Method
This knowledge translation study designed, implemented and evaluated a CPD workshop programme for occupational therapists working in acute settings called, ‘Learn@Lunch: Drinking alcohol as an occupation in later life’. The overall aim of this CPD programme was to help move theory and empirical evidence about older people (65+ years) and alcohol into practice through an educational intervention. The first step was to select an appropriate theoretical framework to enable the development of the programme.
Supporting implementation framework
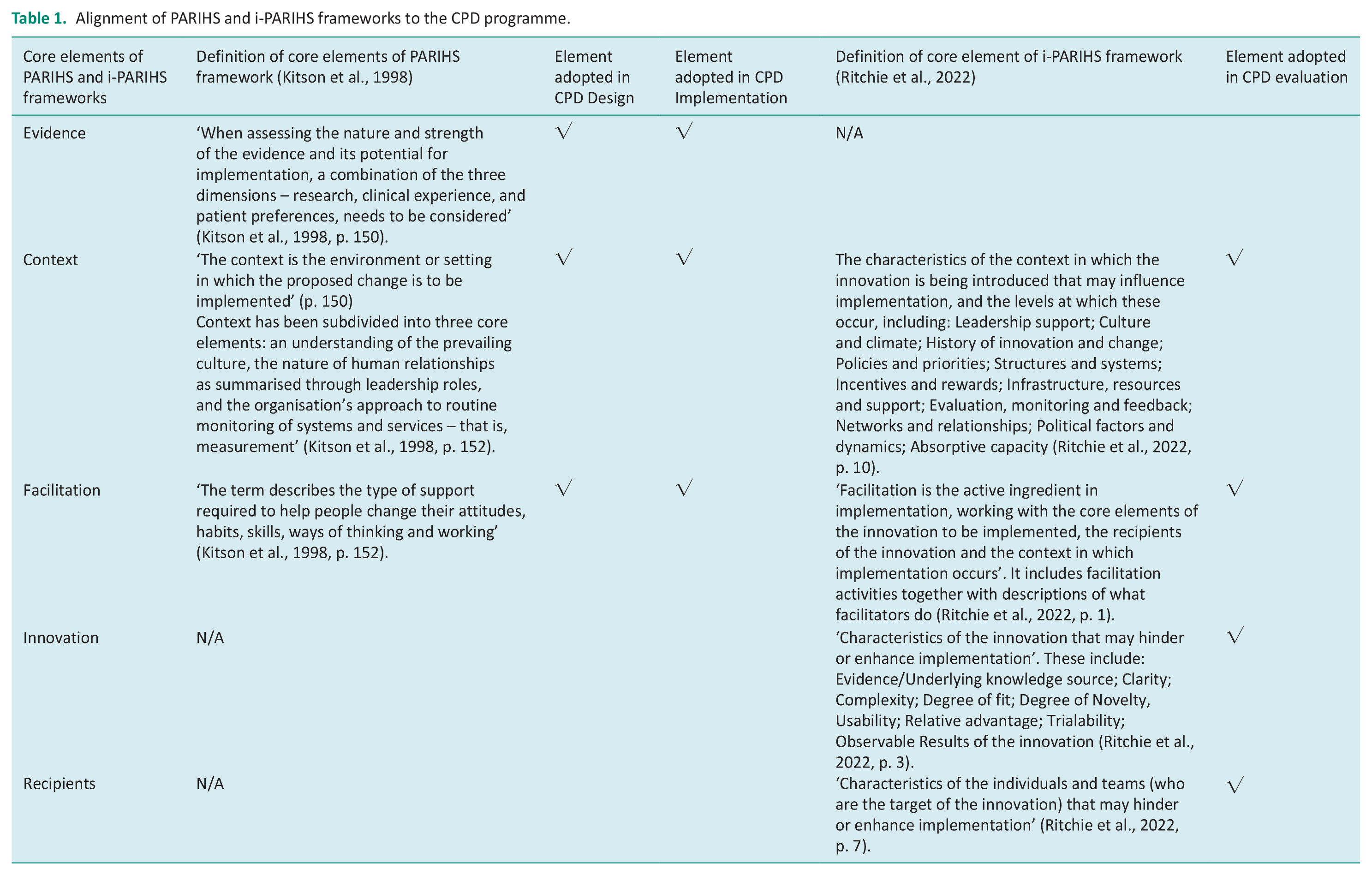
Using a theoretical framework to support knowledge translation studies helps to guide researchers in both the implementation and evaluation of new initiatives to maximise their transferability, usefulness and effectiveness (Damschroder, 2020). There are multiple implementation theories, frameworks and models within the implementation science field (Nilsen, 2020). This project has been guided by the Promoting Action of Research Implementation in Health Sciences (PARIHS) framework (Kitson et al.,1998), which is one of the leading and most widely cited models in the field (Bergstrom et al., 2020). As a model, it has been shown to help guide and predict how evidence can be translated into healthcare practice (Harvey and Kitson 2015). In comparison to other implementation models, the PARHIS framework has a significant focus on the role of context in determining whether evidence can be translated successfully into healthcare settings. As such, it was well suited to this study because existing research shows that the combination of societal views on ageing and the medicalised nature of acute healthcare presents complex contextual barriers to occupational therapists asking about and addressing alcohol use in practice (Maclean et al., 2020). As originally published, the PARHIS framework outlined that successful implementation of evidence into practice was a function of evidence, context, and facilitation (Kitson et al., 1998). Therefore, researchers should pay heed to the nature of the available evidence, the environment in which the evidence is to be assimilated, and who and how implementation will be supported. Since its original publication, the framework has evolved (i-PAHRIS) (Duan et al., 2022). First, the important role of recipients within the knowledge translation process has been recognised. Second, evidence has been reconceptualised as innovation, to capture the various characteristics of the proposed innovation, moving beyond a narrow understanding of ‘evidence’ to include awareness, for example, of underlying knowledge and degree of fit to the local context (see Table 1) (Ritchie et al., 2022). The four inter-related and dynamic elements of innovation, context, recipients and facilitation are seen to combine in processes of knowledge translation in practice (Duan et al., 2022). In this methods section, we outline how a combination of PAHRIS and i-PAHRIS informed the design, implementation and evaluation of a new CPD programme in the form of the Learn@Lunch programme (see Table 1).
Alignment of PARIHS and i-PARIHS frameworks to the CPD programme.
CPD programme development
The Learn@Lunch programme, consisting of three workshops were created and designed by the research team, led by the first author (FM). Given our focus on implementing an existing body of evidence into practice, our approach was aligned with the original PAHRIS framework, designing the workshops with consideration of evidence, context and facilitation as outlined next.
Evidence
The workshop content was rooted in a body of literature built over the past 10 years which has highlighted occupational therapists’ gaps in knowledge and learning needs around older people and alcohol (Maclean et al., 2015, 2019, 2020). The workshops sought to address these gaps by providing therapists with contemporary information about the changing patterns of drinking alcohol in later life (The Royal College of Psychiatrists, 2018), recent evidence underpinning understanding of drinking behaviours and reasons for this in the lives of older people living in the UK (Holley-Moore and Beach, 2016), including the need to build health professionals’ knowledge and awareness of drinking in later life (Wadd et al., 2011), in particular to build therapists’ confidence in asking about alcohol use in acute practice (Maclean et al., 2015, 2020).
Specifically, the workshops were designed around the findings of earlier research that had developed a typology of reasoning that informs occupational therapists’ decision-making in practice (Maclean et al., 2020). This typology – the ‘Four I’s’ – sets out the circumstances in which therapists may or may not open a conversation with older people about their alcohol consumption. These are based on whether issues around drinking have been previously Identified, are Implied, such knowledge is Incidental, or Invisible. The typology and its development are set out in detail in Maclean et al. (2020).
The workshop content was also underpinned by the theoretical concepts of person-centredness (McCormack and McCance, 2017), specifically healthfulness (McCormack, 2012), including the purpose and role of collective occupation (Kantartzis and Molineux 2017), as outlined in Maclean et al. (2020). These overarching perspectives framed delivery of the professional understanding of the complexities of occupation which can unfold in older people’s lives. This has potential to offer therapists an enriched understanding of how they might respond with older people who drink alcohol in later life.
Context
The workshops were designed to be delivered in an acute occupational therapy service in a large general hospital. An occupational therapy team lead from the service was recruited as the ‘Learn@Lunch’ research champion to co-create workshop content and support active participation of the recipients to help maximise the fit of the workshops with the needs of the local context. The champion worked with the research team to review the planned programme content and mode of delivery. The champion brought their own knowledge of the setting, as well as acting as a conduit for requesting and feeding back potential participants’ preferences for CPD course attendance. For instance, the champion guided us towards delivering the workshops in person (within appropriate COVID 19 guidelines) rather than online, as therapists said they had missed this aspect of learning during the pandemic. The workshops were also purposefully designed to be delivered during lunch with the intent of making access to CPD learning as easy as possible with prior research showing that lunch times provide social spaces that enable knowledge sharing between professionals (Mawhinney, 2010) and providing a free lunch can encourage attendance (Rey, 2018). The workshops were held in the education suite of the hospital, facilitating easy access for participants.
Facilitation
In advance of workshop delivery, the programme was piloted with a group of occupational therapists working in a Higher Education Institute (HEI) in Scotland. As a result, changes were made to some aspects of content, course materials and delivery. The final programme comprised three workshops, each lasting 1 h. The workshop schedule was designed to give therapists 1 week in between each to allow sufficient time for them to apply and reflect on their new knowledge, whilst being short enough to build a sense of momentum throughout the course. Table 2 outlines the learning goals and summary of each workshop content.
Workshop learning goals and content.
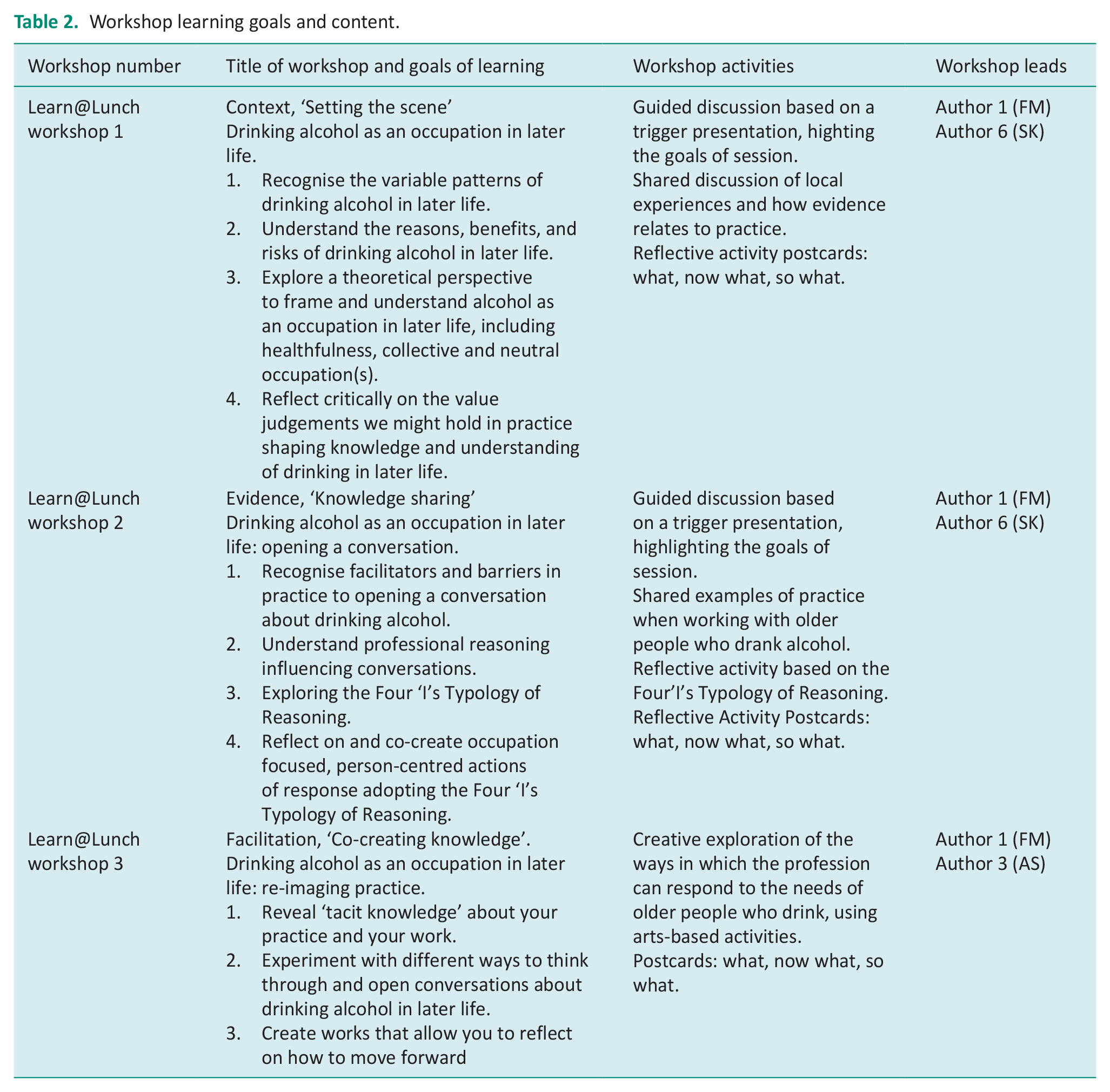
The progression of the workshop schedule was directly informed by the key PAHRIS concepts of context, evidence and facilitation. This was intended to help guide therapists logically and progressively through their learning. They were first asked to reflect on their own context, to explore their existing assumptions regarding drinking alcohol in later life, and their perceived fears and barriers to exploring this with patients. In the second workshop, evidence was shared, and the Four I’s introduced (Maclean et al., 2020), relating this to their own settings. Finally, in the third workshop, therapists were asked to think about their role in facilitating the assimilation of this knowledge in practice, as they identified strategies for making changes to current practice. The workshops were led by the first author (FM) in collaboration with (SK) and (AS) who combined expertise, respectively, in alcohol and older people, occupational approaches and change design. Materials for each workshop were circulated to all potential participants (n = 8) in advance of the workshops, including PowerPoint presentations and activities based on Rolfe et al.’s (2001) model of reflection.
Learn@Lunch recruitment and attendance
Information about the workshops was cascaded to all occupational therapists working in the service (n = 35, Agenda for Change (AfC) bands 5–8) by the Learn@Lunch champion. Eight occupational therapists volunteered to take part, all of whom worked in acute practice which included neurology, medical, orthopaedics, care of the elderly, surgical and vascular specialties. The AfC bands of course participants ranged from 5 to 7, representing diversity of years in practice.
Evaluation of the Learn@Lunch programme
The PARHIS framework can be best used when combined to prospectively inform the design of a knowledge translation programme, and to concurrently and/or retrospectively evaluate how effectively the evidence/innovation was implemented (Hill et al., 2017). The Learn@Lunch programme followed this, using a multi-method evaluation embedded throughout. The aim of this evaluation was to generate transferrable lessons about the effectiveness of the Learn@Lunch programme as a knowledge translation approach. The evaluation was led by the second author (JB), who was not involved in the design and delivery of the programme content to maintain a level of objectivity and to enable participants to be open and honest in their feedback. The multi-method approach included pre- and post-focus groups with workshop participants; pre- and post-interviews with the Learn@Lunch champion; and a post-programme interview with the occupational therapy service lead. Figure 1 shows the timing of each evaluation method relative to the workshop schedule. All groups and interviews were facilitated by (JB), audio recorded and transcribed in full by a professional transcription company.
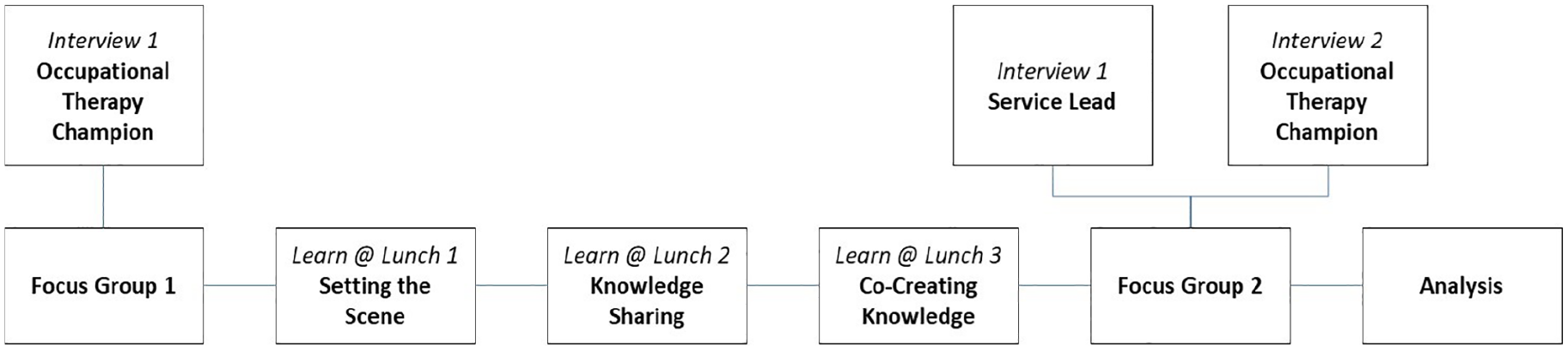
Summary structure of the embedded Learn@Lunch evaluation.
Pre- and post-focus groups
Eight participants took part in focus group 1, which took place 1 week prior to the first Learn@Lunch workshop and lasted 1 h. Six participants took part in focus group 2, 1 week after the final Learn@Lunch workshop, lasting 1 h. Both focus groups took place in the education suite of the hospital at lunch time, with lunch provided as per the workshop format. Topic guides for the focus groups were developed in accordance with the PARHIS framework. In the first focus group, participants were asked to describe their work setting and current approach when asking older people about alcohol (context), their current level of knowledge and awareness of the evidence base around drinking in later life (evidence) and their hopes and expectations for the programme (facilitation). In the second focus group, participants were asked to reflect on what they had learned (evidence), including how their new knowledge, if any, had been assimilated into their work (context) and their opinions about how acceptable, feasible and useful the CPD programme had been (facilitation).
Service lead interview
One interview was undertaken with the Service Lead, following completion of the Learn@Lunch programme. The interview took place online and lasted 1 h. In the interview, the service manager was invited to reflect on how they perceived the Learn@Lunch programme had impacted, if at all, on therapists’ knowledge and confidence in asking older people about alcohol use (evidence), how well they felt that the programme fitted the work environment (context) and how the facilitation and champion role influenced the success, or not, of the programme (facilitation).
Learn@Lunch champion pre- and post-interviews
Two interviews were undertaken with the Learn@Lunch Champion, 1 week prior and 1 week following completion of the programme. The first interview took place in person, and the follow-up interview took place online. Both lasted approximately 1 h. The interview involved asking the Learn@Lunch champion to reflect on the evidence, context and facilitation of the programme. The interview also invited the champion to share their experiences of the champion role, reflecting on the barriers and facilitators to this role.
Data analysis
The design of the Learn@Lunch programme and the embedded evaluation methods were primarily informed by the original PAHRIS concepts of evidence, context, and facilitation. Throughout data generation however, it became clear that the more complex definition of evidence as innovation within the i-PAHRIS framework (see Table 1) was potentially better suited to consider the complexity of the evidence/innovation that was being introduced in the programme and the way in which therapists were interacting with content. Similarly, the way in which participants (recipients) received, understood and interpreted the innovation was a critical factor shaping the implementation of the programme. Moreover, the timely publication of the i-PAHRIS qualitative codebook (Ritchie et al., 2022) offered a robust approach to enhancing the evaluation of the Learn@Lunch programme. Therefore, we evolved our analytical approach to include i-PAHRIS, which enabled us to analyse more effectively the data we had generated.
Data were analysed by three researchers (FM, JB, SK). Analysis began with all three researchers reviewing the first focus group transcript independently. Each undertook an initial inductive analysis, followed by a second reading of the transcript against the i-PARHIS codebook. The researchers compared their inductive findings and assessed the fit of the codebook. Having agreed that the codebook allowed sufficient capture of all the relevant data, we divided up the remaining data sources and independently, using the codebook as a guide, coded the data into the four categories: facilitation, innovation, recipients, and context. We used the codes flexibly to allow for inductive insights simultaneously. Where there was doubt or cross-over, data were coded into all applicable categories. The final stage of analysis was to code the data within each of the four categories, again using a combination of inductive insight alongside the codebook subcodes. The innovation and facilitation categories were sub-coded by two researchers independently to allow for further rigour in the process. Discussion of each category was then prepared, bringing the findings together with quotes of participants.
Ethical approval
Ethical approval for the study was obtained from The Nursing, Paramedic Science, Occupational Therapy and Arts Therapies Divisional Ethics Panel, Queen Margaret University, Edinburgh. The project was also registered with Clinical Governance from the participating NHS health board.
Findings
Findings are presented according to the four constructs of the i-PARIHS framework (Ritchie et al., 2022): innovation, recipients, context and facilitation.
Innovation
Compatibility of values and norms in acute practice
Evidence underpinning the CPD programme was seen to be relevant to acute practice by participants to the extent that ‘we know they’re going to go home and drink’ (FG1). However, this understanding did not necessarily mean that therapists saw drinking alcohol as an area of priority to which they should respond, ‘we can’t address every single lifestyle choice, and is drinking more important than smoking?’ (FG1). In part this was influenced by a perception that people ‘were going to continue drinking anyway’ (FG1) on discharge, and therefore input could have little or no impact.
Nevertheless, the wider purpose and meaning of drinking for some older adults was valued by participants. This included understanding the importance of where drinking took place and the reasons attached to this. For example, an older person who wanted to go to the pub every day ‘for a pint, just to meet friends and have a chat. . . . that’s all he wanted to do when he got home’, (FG1) resulting in recognition of the complex inter-relationship between drinking as a benefit to the person, versus the potential for harm, as a delicate ‘balance’ (FG1).
However, navigating this balance was complicated, in part due to the values of other colleagues:
someone thought I was wrong by putting that as a goal [going to the pub], but if that’s his main leisure, occupation and hobby, then why shouldn’t that be part of our goal? (FG1).
Therefore, therapists in acute practice were likely to work with people who made ‘choices that maybe weren’t the best for their health’ (AHP Lead). As such, a service aim via the programme was to grow knowledge to shift priorities towards facilitating conversations whereby people could make ‘informed choices’ (AHP Lead) about their drinking, valuing the potential of making ‘healthier choices’ (AHP Lead) in future. In tandem, to counter a perceived ‘acute mindset’ (AHP Lead), where there was concern,
we don’t have time for these conversations, and we do. They don’t take any longer, they just need to be the right conversations with people (AHP Lead).
Relative advantage to practice
The potential advantage of the programme to participants was initially centred on the extent to which it could be considered useful in terms of enhancing practice, influenced by the pressures of time in an acute setting. This included the need for practical responses to ‘talk about our tools for practice’ (FG1), to respond directly to the needs of older adults who drink.
Following the Learn@Lunch programme an adjustment was made to the occupational therapy initial assessment to include a question about drinking alcohol, to prompt conversations, ‘we’ve put in an option to say, if there were any concerns raised [about drinking] we could onward refer to services as needed’ (RC2).
Such changes to paperwork were reflected by the research champion to have led to a shift in perspective(s), and therefore action in practice
. . . . there was a patient who had come in and there were some alcohol issues. They perhaps wouldn’t have asked about it before, but they did. From attending [Learn@Lunch], she did think to ask about it a bit more (RC2).
Recipients
Knowledge of recipients
The participants were all situated in an acute hospital context. They possessed varying degrees of practice experience in terms of years post-qualification; however, all agreed that as a profession ‘none of us are confident discussing it [alcohol]’ (FG2). Hesitancy in asking older adults about their drinking was evident in so far as ‘I don’t think I want to start asking every older patient, unless the patient identifies this as an issue’ (FG2), ‘it is well documented in notes’ (FG2), or it arises ‘through conversations with next of kin’ (FG2) because ‘where does it stop?’ (FG2)
Additional reasons for hesitancy in asking about older adults drinking patterns also reflected therapists’ uncertainty connected to knowledge of what to do next: ‘If I’ve asked the question, I wouldn’t know what to do with that information or how to take it further’ (FG2).
However, the occupational therapy champion highlighted ‘we’re not always talking about alcohol excess, it could be the day-to-day, what’s the normal limits, and that it is [drinking] part of people’s occupations’ (RC2).
As such the programme appeared to alter how therapists’ thought about the place of alcohol in the lives of older people who drink, ‘age shouldn’t really matter, it’s important to you, as long as it’s safe’ (FG2).
General attitude of recipients to research and practice
Programme implementation offered an opportunity to involve therapists and discuss the evidence base to practice, because ‘when you mention the word research everyone’s like “nope, not doing that” (RC1), because there’s sort of a stigma towards research. A lot of people tease’ (RC2).
This was underlined further by the AHP service lead who found ‘occupational therapists less likely to engage with research opportunities’ (AHP Lead) with a tendency ‘to get their heads down and treat patients’ (AHP Lead). The programme was viewed as offering ‘small steps’ (AHP Lead) to support change in how CPD could be delivered and to help therapists ‘achieve all four pillars of practice, especially research’ (AHP Lead). Participants highlighted the value of the opportunity to access CPD: ‘This is a nice opportunity to do something for our profession, research based rather than people constantly wondering what we do’ (FG1).
Context
Culture and climate
There was strong support for the Learn@Lunch programme from the service manager and team leads, and the impact of this support was noted by all participating therapists, influencing a positive workplace culture. This included the importance of giving participants permission to take time for learning and development even in the context of busy clinical responsibilities: ‘Our manager is really supportive of all of us attending, she encouraged us to do it’ (FG1).
All participants reflected too on the compounding effect of persistent staffing issues caused by the Covid-19 pandemic, winter pressures and staff leave. As a result, whilst all participants felt more confident asking about alcohol after attending the Learn@Lunch programme, they continued to feel overwhelmed by the context related to ‘time and bed pressures’ (FG2).
The research champion, reflecting on the time commitment for their role, felt that it did not have a ‘massive impact’ (RC2) overall. However, it did involve periods of intense activity, particularly recruiting participants and taking on additional clinical workload to free up staff time. It was not initially anticipated that this would fall into the research champion role but used their discretion during the project to maximise attendance.
The structure of the Learn@Lunch programme with three, 1-h workshops, spread over a number of weeks was seen by all (participants and manager) as an effective means of embedding learning into clinical practice, giving space for reflection and sharing their learning between workshops:
I work really close with the vascular physios, and they ask what have you taken away from it, and last week being in that creative mindset, I’m like, actually, this is what I’ve learned (FG2).
The ability of band 5 therapists to articulate new knowledge and to open conversations about drinking was noticed by the research champion, ‘before they perhaps wouldn’t have asked about it, but they did’ (RC2).
Incentives that encourage innovation implementation
Providing a good quality lunch helped to incentivise sign-ups and attendance, as well as advertise the Learn@Lunch programme:
They [other OT staff not attending] are very jealous of lunch. When we come back with our bags and like, where can we sign up? We want to do that next time (FG2).
However, delivering the workshops over lunchtime did elicit mixed views from different participants depending on their position. The service manager, for instance, perceived that holding the workshops during lunchtime was a strength of the programme because practitioners ‘don’t feel that they’re missing out on their clinical time so much’ (AHP Lead). In contrast, practitioners taking part in the programme disliked the expectation to undertake education during lunch:
for most of us because we’re on the go all day, we’d like to have our downtime. And we like to just be able to sit and, maybe not have noise, just kind of have time to myself? (FG2).
However, on reflection, it was difficult to identify an ideal time, especially within the busy routine of the setting:
It’s really difficult to get a time because mornings can be difficult, you’re busier and afternoons can be difficult because you might get caught up with a patient. (RC2).
Facilitation
Adapting the programme to local context
Findings demonstrated the importance of adapting the programme, during planning and implementation, to the local context, particularly in relation to staffing and culture. Whilst staffing levels were a pragmatic issue, and absences due to Covid were noted, a pervasive culture seemed to favour clinical work over CPD, ‘why are you not giving up your CPD? I’m covering your ward for you’ (FG1).
The perception that ‘clinical practice always comes first, and then learning and development comes second, if there’s time’ (FG1), required attention to the number of workshops and the timing. Participants felt that three workshops were manageable, whereas a longer programme would ‘absolutely not’ (FG2) be possible.
Despite pressures from clinical work, face-to-face workshops were preferred as they were more interactive, supporting discussions and engagement. Participants felt that online delivery might lead them to ‘zone out’, ‘switch off’ (FG1), and perhaps use the time to write clinical notes or answer emails. However, when some participants contracted Covid, it was appreciated that participation via TEAMS was facilitated.
The local research champion was identified as key to successful planning and organisation of the programme, ‘that person can encourage people and organise because every hospital has different ways of working’ (RC2).
The research champion provided valuable insights into the local context, influencing development of course content and delivery, crucially also to lead and develop future projects,
will be that legacy after the project finished, whereas if it was someone external coming in, they would go and they would move on and not think about that continuing development (AHP Lead).
Discussion and implications
This knowledge translation study aimed to mobilise existing knowledge findings from a published body of work exploring the occupation of drinking alcohol in later life. It created a Learn@Lunch programme, aimed at transforming existing occupational therapy practitioner knowledge and awareness related to the changing patterns of drinking alcohol in older age. It also sought to conduct a thorough evaluation of the method, content, and mode of delivery of the programme. Consequently, the findings offer an important contribution to how and in what way CPD can evolve in acute professional practice.
The findings suggest that participant knowledge and understanding of professional reasoning directing when to open a conversation about drinking with an older person, reflected previous research findings informing the Four ‘I’s Typology (Maclean et al., 2020). Specifically, there remained a reticence to ask older people about their drinking, unless documented in notes. However, there was evidence of shifting perspectives, which influenced changes of actions in practice. For example, the research champion subsequently noticed therapist willingness to discuss alcohol with a particular person, which may not previously have occurred.
Participants reflected on their altered approach to practice, which appeared to be linked to expanded understanding of the complexity of the occupation of drinking alcohol in people’s everyday lives as they age. This enabled a deeper appreciation of the nuances of the enactment of activities [occupations] associated with drinking that were identified as important by an older person. However, despite the support of the wider community of leadership (Research Champion and AHP Lead), practical concerns such as pressure of time, a focus towards discharge and ongoing reticence to discuss alcohol remained.
Nevertheless, depth of understanding connected to why this reticence existed was highlighted, caused by the inherent tension to sustain an occupation-focus to treatment goals, for example, when working with an older person whose identified goal on discharge was to be able to return to the pub to drink alcohol. For occupational therapy, responding to, and noting this, as a goal of therapy as part of the wider multidisciplinary team was viewed as problematic. This was in part because of the values held by other health professional colleagues regarding older people drinking alcohol, potentially influenced by the bio-medical context, where drinking alcohol can be viewed as contrary to supporting ‘good’ health.
Despite this, enhanced therapist knowledge led to revisions in the occupational therapy initial assessment paperwork to include questions about and prompt discussion of the place of alcohol in older people’s lives when admitted to hospital. Consequently, rather than rely on competence-based tools, therapists subsequently embraced the opportunity to consider wider contextual experiences and reasons why older people might drink.
More broadly, evaluation of the programme revealed the importance of the context in which the workshops were delivered, set within a large occupational therapy acute service. Striking was the value and importance attached to the role of the research champion, embedded throughout the study design. This included involvement in the initial development of the research proposal, supporting the practical arrangements of evaluation and covering for those participants who attended the workshops.
The research champion was nominated by the AHP Service Lead due to their interest in research and was a senior member of the team. In addition, the champion was valued and respected by occupational therapy colleagues, helping to enable and advance positive participant engagement with the study. The champion also acted as a bridge between the research team based within the HEI’s leading this study, and the practice environment where the delivery of the workshops and evaluation were to take place. As a result, the champion was seen to provide local insight and knowledge which positively influenced the design, delivery and evaluation of the Learn@Lunch programme, enhancing its relevance. Findings indicate this role can leave a legacy of experience to enable wider engagement with evidence-based practice in future.
This is clearly of importance as a culture of initial wariness and hesitancy to participate in and with research was evident, in part due to pressures to ensure rapid patient discharge. Participants tended to prioritise clinical time over CPD, to the extent that guilt was felt at leaving the ward for the purpose of learning. Wider barriers to growing a culture of research and knowledge translation activities were identified, including anxiety and even stigma associated with participation in the study.
Reasons for this are difficult to ascertain. Often, the role of senior leadership has been identified as an important influencer of the extent to which research and knowledge exchange can translate to practice (McCance and McCormack, 2021). However, in this study both the research champion and the AHP Service Lead were fully supportive of the CPD programme, noted by participants.
Of interest is the reflection of the AHP Service Lead that hesitancy around research was, in their experience, unique to occupational therapy in comparison to other disciplines for whom they had responsibility. Whilst it is beyond the scope of this study to consider this in detail, the relevance of this finding is crucial to the profession to enable translation of research with practice. Particularly in relation to efforts that will, ‘build the capability, capacity and enthusiasm for research in our profession, to ensure that the evidence base underpinning occupational therapy practice continues to expand’ (RCOT, 2019, p. 4).
Limitations
The COVID-19 pandemic significantly influenced aspects of the study, leading to delays in implementation and evaluation. Extensive discussion took place as to whether the workshops should be delivered online or in person, subject to current local pandemic guidelines. Whilst the workshops were eventually delivered in person, because of feedback provided by the Learn@Lunch champion, social distancing was still in place which did limit elements of workshop activities. We also acknowledge the challenging nature of practice in general at this time.
Conclusion
This knowledge translation study is one of the first to consider the importance of how and in what way knowledge and research connected to drinking alcohol as an occupation in later life can be mobilised with practice. It extends understanding of how CPD in the profession of occupational therapy can be delivered, and applied, specifically in a busy and often hard to reach group of therapists who work in acute practice.
This evaluation highlights that through the Learn@Lunch programme, therapists can grow knowledge and confidence connected to asking older people about their drinking, leading to changes in practice. This work signals a need to further understand how an occupation-focus in acute practice can support person-centred actions of response to ensure the rights of older people to make informed choices about their drinking. Further, this study has identified key elements of good practice in how CPD learning can be designed and delivered in acute practice, to enhance and enable the translation of current evidence with professional practice.
Key findings
The Learn@Lunch CPD programme led to changes in occupational therapy practice to support therapist conversations about drinking alcohol as an occupation in later life.
Occupation-focused practice requires targeted CPD support in the acute practice setting
Contextual relevant CPD programmes can support changes in occupational therapy practice
What the study has added
This study illustrates the value and importance of a novel programme of CPD to grow knowledge and awareness of drinking alcohol as an occupation in later life, as part of acute occupational therapy practice.
Footnotes
Acknowledgements
The research team would like to thank all those who participated in the study, including colleagues who generously gave of their time to support the pilot evaluation of the workshops.
The original grant proposal and application for funding would not have been possible without the support and contribution of Prof. Jan Dewing, who passed away during the implementation of this work. She is remembered as a valued and much respected member of our team.
Research ethics
Ethical Approval was gained from, The Nursing, Paramedic Science, Occupational Therapy and Arts Therapies Divisional Ethics Panel, Queen Margaret University, Edinburgh (Approval No.: 2020/3).
Consent
Written and verbal informed consent was sought from all participants in this study and included a statement confirming consent for publication.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was included in planning and progress of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by an Elizabeth Casson Trust Implementation Study Grant.
Contributorship
FM, SK and JPB researched literature and conceived the study, including protocol development. BMcC and JG supported protocol development and JG led participant recruitment and advised on elements of design and delivery of knowledge translation. AS supported the development of materials and delivery of knowledge translation activities, as did FM and SK. JPB led the data collection and FM, SK and JPB undertook data analysis and co-authored the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.