
Abstract
Introduction:
The COVID-19 pandemic has significantly impacted the home healthcare industry, with increased rates of burnout and stress among homecare rehabilitation professionals (hcRPs). This study aimed to (1) examine the nature of burnout and occupational stress among homecare rehabilitation professionals at a large home care organization in Ontario, Canada, transitioning out of the pandemic, and (2) assess its impact on work participation and engagement.
Methods:
We conducted a cross-sectional survey using the National Institute for Occupational Safety and Health Generic Job Stress Questionnaire and Copenhagen Burnout Inventory to examine burnout and job stress.
Results:
One hundred thirty-nine participants identified that work stress and burnout are more likely to occur when one struggles to cope, experiences unexpected circumstances, and feels a lack of control, which can lead to anger and emotional exhaustion. The adjusted odds ratio for emotional exhaustion was 5.46, indicating that the probability of experiencing work stress among homecare rehabilitation professionals increases as emotional exhaustion increases. Significant associations were found between coping with daily tasks and levels of burnout.
Conclusion:
Work stress and burnout influence coping, unexpected circumstances in homecare rehabilitation professionals work–life. Furthermore, highlighting the need to provide organizational support and policies that specifically address these issues in the home care sector.
Keywords
Introduction
Over the past ten years, there has been a significant rise in the frequency of debilitating illnesses, reaching about 183 million in comparison to the year 2005 (World Health Organization, 2017). By 2030, it is expected that 20% of the general population will be over the age of 65 (Kern et al., 2019). As this population increases, there is also an increase in chronic health conditions which require the care of home care rehabilitation professionals (hcRPs), (Maresova et al., 2019) such as occupational therapists, physical therapists, speech-language pathologists, social workers, and dietitians. However, there is a significant shortage of hcRPs to meet this large demand (World Health organization, 2017). Therefore, it is imperative to address the sources of their burnout and stressors to help recruit and retain this working population.
The coronavirus disease in 2019 significantly impacted the delivery of home care services by hcRPs. Among the health professions studied in the stress and burnout literature, hcRPs have received little attention as most of the research has focused on nurses and physicians (Bruschini et al., 2018; Wilkins, 2007). According to a 2020 study conducted in Cadiz, Spain, 65% of physiotherapists surveyed experienced an intermediate to high level of work-related stress (Carmona-Barrientos et al., 2020). Furthermore, in a 2020 study investigating work-related mental health problems and risk factors in Sweden, 40% of occupational therapists indicated having experienced stress-related symptoms (Lexén et al., 2020).
Research specific to the impacts of the pandemic on Canadian hcRPs is limited, particularly in home and community care settings. Prepandemic, a 2012 study conducted in Ontario aimed to investigate the burnout level among occupational therapists (Gupta et al., 2012). The results of the mixed-methods study indicated that the participants only scored highly for the depersonalization (cynicism) dimension, reporting average levels of emotional exhaustion and personal accomplishment (Gupta et al., 2012). Postpandemic, there is a need to expand upon the existing research regarding stress and burnout in hcRPs in Canada and the impact this may have on their participation and engagement within their practice. This is especially relevant given the changing healthcare needs of the general public and the increasing recognition that hcRPs, including occupational and physical therapists, can and will play an important role in meeting these demands (Rogers et al., 2017).
Literature review
Occupational stress is inevitable and can serve as a necessary motivator to improve job performance (e.g., meeting deadlines). However, chronic exposure to stress can have a variety of negative physical and emotional consequences including occupational burnout with limited ability to cope successfully. This can result in decreased job performance and negatively impact the quality of client care (Devebakan, 2018; Lloyd and King, 2001; Pustułka-Piwnik et al., 2014).
Occupational burnout has been defined as a psychological syndrome that involves a prolonged negative response to chronic interpersonal stressors on the job (Maslach and Leiter, 2017; Rogers and Dodson, 1988). It can result in emotional exhaustion, depersonalization, and negative assessment of personal accomplishments (Devebakan, 2018; Lloyd and King, 2001; Pustułka-Piwnik et al., 2014). The important predisposing factors to provider burnout include extended work hours, lofty and unachievable production targets, and an increased struggle in striking a work–life balance (Shanafelt et al., 2016; Sinsky et al., 2016). A 2021 meta-analysis for burnout in OTs concluded that a high level of burnout is associated with multiple factors including turnover intention, job challenges, as well as certain factors related to the organization (Gupta et al., 2012). However, it is important to note that when categorized simply as experiencing low, average, or high levels of burnout more broadly, the majority of respondents were categorized as experiencing high levels of burnout. Among physical therapists in Canada, the limited data suggest they are at risk of demonstrating burnout, but conclusions are hampered by poor response rates (Bainbridge et al., 2017). A recent randomized control trial reported that participation, involving employees in decision-making processes that influence their work and working conditions, predicted improvements in work engagement and reductions in burnout (Nielsen et al., 2021).
Recent qualitative research has illustrated that the pandemic has led to inadequate mental health outcomes among hcRPs, such as increased work stress and burnout (Brown et al., 2017; Chatzittofis et al., 2021; Gohar and Nowrouzi-Kia, 2022; Hoel et al., 2021; Howe et al., 2024; Rodríguez-Nogueira et al., 2022; Śliwiński et al., 2014; van Oorsouw, 2022). This is due to HcRPs facing higher workloads, staffing deficits due to the pandemic, encompassing a higher risk of spreading COVID-19, and having less resources readily available to tackle these issues (Howe et al., 2024). A systematic review by Lluch et al. (2022) found increased rates of burnout postpandemic compared to prepandemic levels among healthcare personnel in general. However, there are a lack of studies that have quantitatively measured the impact of the pandemic on work stress and burnout on hcRPs working in home care settings. Occupational stress and burnout are factors present in all sections of healthcare. RP’s however experience unique challenges when working in intimate spaces other than clinical settings which can add onto their burden of existing stress (Dyck et al., 2005; Ruotsalainen et al., 2015). We hypothesize that this workforce may experience occupational stress related to post-COVID clinical practice changes, increased work demands, and professional isolation. To effectively manage the mental health needs of these workers and support occupational engagement, organizations must develop policies, programs, services, and practices designed specifically for public health crises such as the COVID-19 pandemic. Understanding how burnout and occupational stress have impacted hcRPs participation and engagement at work are vital to improving quality care for the clients and communities they serve. Moreover, existing literature has highlighted the role personal and work-related factors have in influencing burnout and occupational stress among healthcare workers during the pandemic (Jalili et al., 2021). Identifying whether these factors persist among rehabilitation professionals transitioning out of the pandemic is crucial in devising tailored interventions that can alleviate their concerns and improve their well-being.
Workplace mental health is a significant concern for hcRPs working in Ontario. The objective of this research study was to examine the nature of burnout and occupational stress among home care hcRPs transitioning out of the COVID-19 pandemic and to identify types of experiences which predict burnout and occupational stress within this occupational group.
Methods
Design
The potential participants were individuals working at a large nonprofit home care provider organization in Ontario, Canada. Potential participants were invited to complete self-administered questionnaires online. This article focuses on the findings and analysis from Phase I. Ethical approval for the study was obtained from the University of Toronto Research Ethics Board (protocol number 42041).
Sample
The population from which the sample was drawn included approximately 420 hcRPs, of whom approximately 64% were occupational therapists, 24% were physiotherapists, and the remaining 12% were a mix of speech-language therapists, social workers, and registered dieticians. All hcRPs at the organization were able to communicate in written and spoken English as a condition of employment. Written informed consent was obtained from all participants.
Given a power level of 0.80 and a significance level of .05 and assuming a moderate effect size d = 0.4 for the relationship between factors associated with participation and engagement, a sample size of 140 is required when seven independent variables including (1) workload, (2) patient-related difficulties, (3) organizational structure and processes, (4) relationships and conflicts with other professionals, (5) lack of resources, (6) professional self-doubt and (7) home–work conflict are included in the analysis (Faul et al., 2009).
Data collection
A self-administered questionnaire was distributed to all hcRPs working at the organization. The data collection period occurred in fall 2021, following the peak of the pandemic. All data were collected using an online database and stored on REDCap (Harris et al., 2009) servers at the University of Toronto.
The questionnaire collected demographic data such as gender, sex, age, ethnicity, marital status, education attainment, years of experience working as an occupational therapist, the total number of years working, area of clinical practice, hours of work per day and in a week, overtime hours worked, income, and travel time required for work. The questionnaire also included an inventory of factors experienced as occupational stressors and burnout based on the Copenhagen burnout Inventory, a widely used instrument used to measure burnout (Kristensen et al., 2005), the Perceived Stress Scale (Cohen et al., 2014), and the National Institute for Occupational Safety and Health (NIOSH) Generic Job Stress Questionnaire (Hurrell and McLaney, 1988).
Measures
The Copenhagen Burnout Inventory
Burnout was measured using the Copenhagen Burnout Inventory (CBI). The CBI has been used extensively, and a growing body of evidence demonstrates robust psychometric properties for measuring occupational burnout (Andrew Chin et al., 2018; Borritz et al., 2006; Thrush et al., 2021). The CBI is a 19-item survey created to measure the degree of psychological and physical fatigue and exhaustion attributed to personal-burnout (six items), work-related burnout (seven items), and client-related burnout (six items) (Kristensen et al., 2005). For example, one item states, “how often do you feel tired.” Twelve items use a 5-point scale from 0 (never), 25 (seldom), 50 (sometimes), 75 (often) to 100 (always). Seven items use response categories varying in intensity, including “a very low degree,” to “a low degree,” “somewhat,” “a high degree,” and “a very high degree.” A total score is computed as the sum of the item scores. Scores from 50 to 74 are considered “moderate,” and those from 75 to 99 are high, and an individual with a score of 100 is considered to experience severe burnout. Previous studies have reported high Cronbach alpha reliability coefficients (personal α = 0.90; work-related α = 0.88; and client-related α = 0.89; Creedy et al., 2017) of the CBI subscales and internal reliability (Kristensen et al., 2005).
NIOSH Generic Job Stress Questionnaire
The NIOSH generic job stress questionnaire provides a measure of job satisfaction among workers, the presence of depressive symptoms, and the common job stressors in the work environment. The following sections were included job satisfaction (four items), mental demands (five items), physical environment (ten items), work hazards (six items), and social supports (nine items). Responses were measured on a scale of 1–5, 1 denoting “very much” and 5 indicating a sense of “don’t have any such person.” It is widely used and considered a valid questionnaire in occupational settings (Wiegand et al., 2012).
Perceived Stress Scale
The Perceived Stress Scale (PSS) is used to measure the perception of stress and items capture the capricious nature of stress in one’s daily life. It is the most extensively used tool to assess stress (Hurrell and McLaney, 1988). The PSS is a 14-item questionnaire revolving around an individual’s “thoughts and feelings” in the past month. Four of these items contain positive statements. For instance, a positive item is “In the last month, how often have you felt confident about your ability to handle your personal problems?” Other items include “In the last month, how often have you been upset because of something that happened unexpectedly?” or “In the last month, how often have you felt nervous and stressed?” Responses are made using a 5-point scale: 0 (never), 1 (almost never), 2 (sometimes), 3 (fairly often), and 4 (very often) according to how frequently an individual has experienced a certain feeling or thought. To calculate the final PSS score, first the scores for only the positive statements are “reversed.” For example, for the item “In the last month, how often have you felt that things were going your way?” a response of 0 is given a score of 4, while a response of 4 is given a score of 0 (Cohen et al., 2014). Then, the scores of all questions are summed to receive a total PSS Score. Total PSS Scores between 0 and 13 indicate low stress levels, scores between 14 and 26 indicate moderate stress levels, and scores ranging from 27 to 40 suggest that the individual is experiencing high stress levels (Cohen et al., 2014).
Data analysis
Data were analyzed in R version 4.0.5 (R Core Team, 2021) to determine the demographic and work-related predictors of stress using descriptive and inferential statistics through logistic regression analysis. The predictor variables were based on previous studies that assess burnout and job stress among healthcare professionals (Ab Aziz et al., 2023; Godifay et al., 2018; Kim et al., 2020; Nantsupawat et al., 2024; Park, 2021; Peter et al., 2024; Sklar et al., 2021), as well as based on discussions among the research team. In preparation for the regression analysis, relevant variables were recoded according to the CBI and PSS to calculate burnout and stress scores. All variables used in the regression analysis were then dichotomized, where a value greater than or equal to the median was assigned a value of 1, while those less than the median were assigned a value of 0. Following the development of the two regression models, with burnout and job stress as the response variable for each, we calculated the adjusted and unadjusted odds ratios, and corresponding 95% confidence intervals, for each independent variable, allowing us to compare the odds of burnout and job stress based on exposure to each variable. Preliminary checks were also performed to ensure that there is no violation of the assumptions of normality. Furthermore, 25% of the sample was randomly selected and re-entered by the principal investigator (BNK) and another author (AY) for quality assurance purposes. Weighted Cohen’s kappa was used to measure agreement and bias on each reason for match failures (discrepancies between the two raters), revealing an excellent agreement (kappa = 0.9) between the two raters.
Results
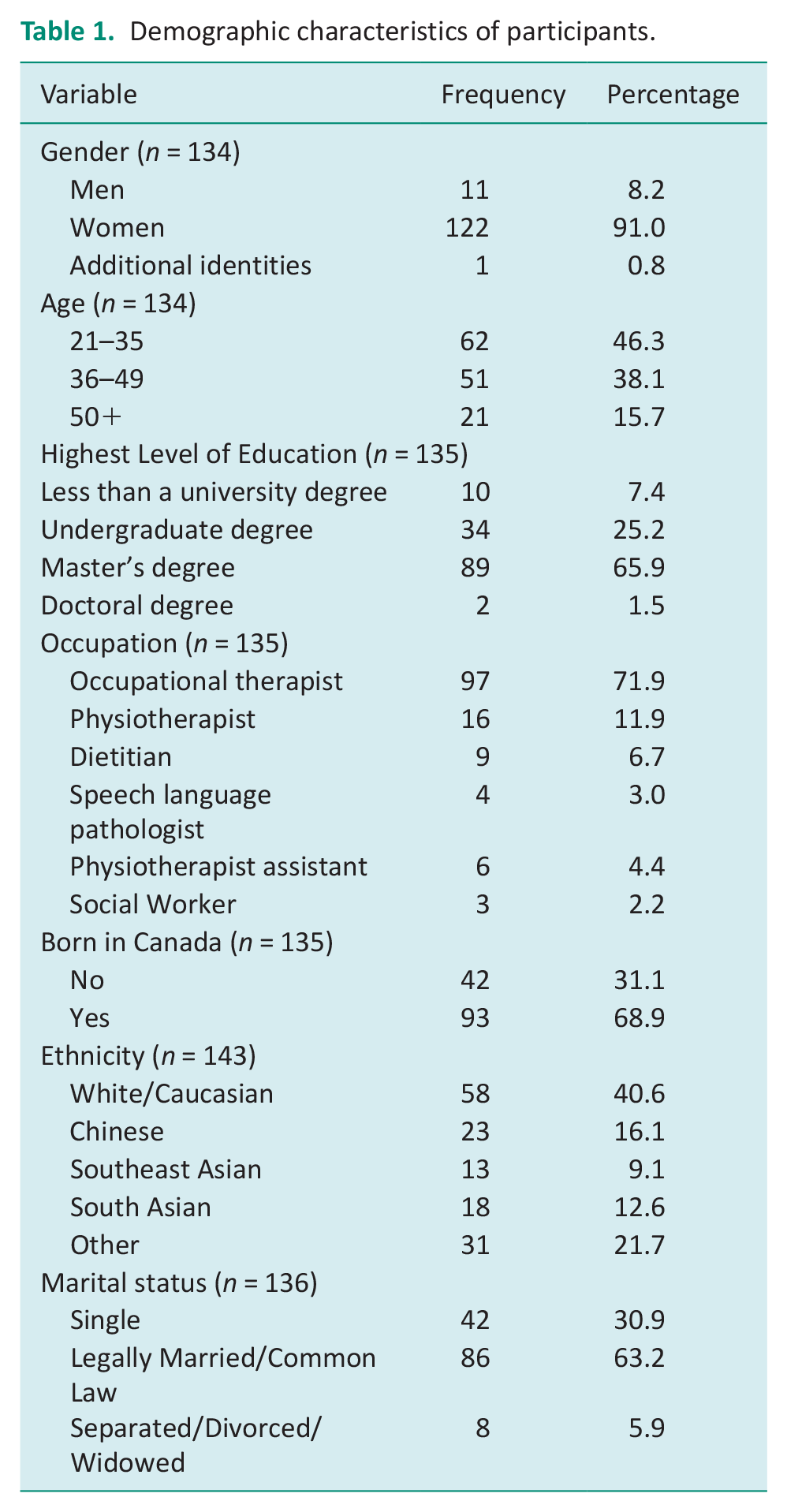
A total of 139 participants completed the questionnaire, resulting in a response rate of approximately 33.1% (139/420). The personal and occupational characteristics of the study participants are presented in Tables 1 and 2. Notably, over 91% of respondents identified as female. The majority of participants fell within the age range of 21–35, with a mean age of 38.5 and a standard deviation of 10.4. The highest level of education for more than 65% of respondents was a master’s degree, and only 7.41% did not hold a university degree. Respondents were predominantly born in Canada (68.9%), under half were White/Caucasian (40.6%), and 63.2% were married. Moreover, most of the participants were Occupational Therapists (71.9%).
Demographic characteristics of participants.
Occupational characteristics of rehabilitation professionals working in home care.
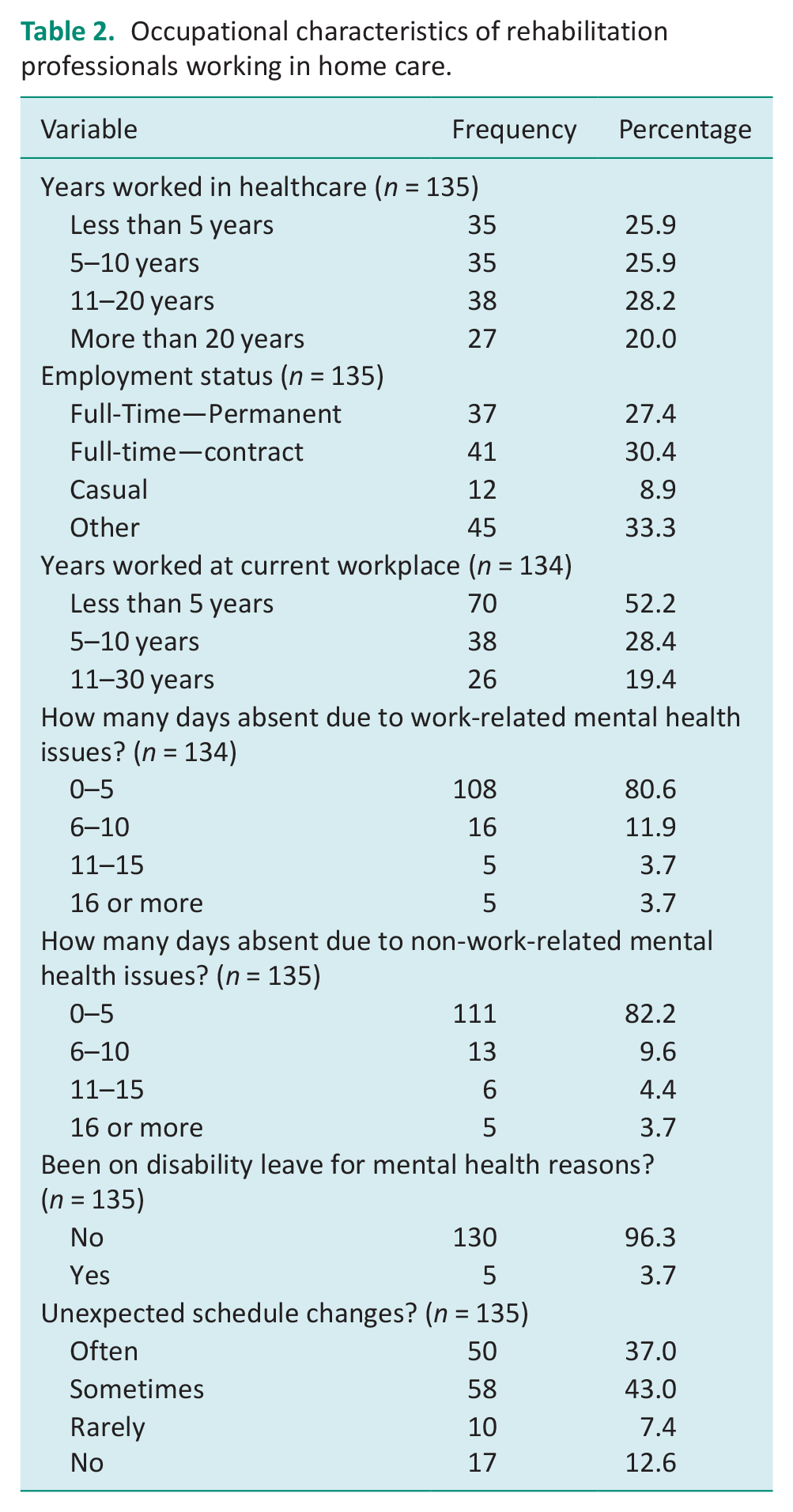
There are also demographics of this data related to the workplace of the participants. Most participants were experienced healthcare providers (average ~12 years), with 74% having over 5 years of experience, and nearly half (48.2%) having 11 or more years of experience. Approximately half of the respondents reported that they had worked less than 5 years at their current workplace. The majority of homecare workers are compensated based on the services they provide rather than receiving a salary. Many of these workers encounter challenges in meeting financial obligations, such as struggling to pay bills. Additionally, 91% of participants work as direct care providers without subordinates reporting to them. Notably, 43% of respondents reported occasional experiences of unexpected schedule changes, and 34.1% have a daily commute lasting between 30 minutes to an hour.
When asked directly about the impact of mental health on their work participation, mental health issues were reported to have caused 19.4% of participants to miss six or more days or work, 17.8% missed six or more days of work due to nonwork-related mental health issues, and 3.7% of respondents had been on disability leave due to mental health.
The mean scores for personal burnout had a value of 42.0, with a standard deviation of 20.5 and an IQR of 26.7. In contrast, the mean scores for work-related burnout had a value of 48.6, with a standard deviation of 21.4 and an IQR of 28.5. The mean scores for coworker burnout had a value of 13.2, with a standard deviation of 14.1 and an IQR of 21.4. Three of the potential predictors of burnout were significantly associated with experiencing high levels of burnout in the burnout regression model (Table 3), as indicated by significant adjusted odds ratios (AORs). An increase in the inability to cope with daily tasks for hcRPs increased the odds of experiencing a high level of burnout threefold (AOR = 3.06, 95% CI: 1.17–8.45). Participants reporting higher levels of unexpected occurrences also had a greater than fourfold increase in the odds of experiencing high levels of burnout (AOR 4.43, 95% CI: 1.22–21.23). Finally, a lack of control causing anger correlated with a nearly threefold increase in the odds of experiencing a high level of burnout (AOR = 2.80, 95% CI: 0.90–9.40). The remaining predictors included in the burnout model (age, employment status, schedule changes, lack of control and ability to handle problems) were not significantly associated with the degree of burnout reported (Table 4).
Job Stress among rehabilitation professionals working in home care.
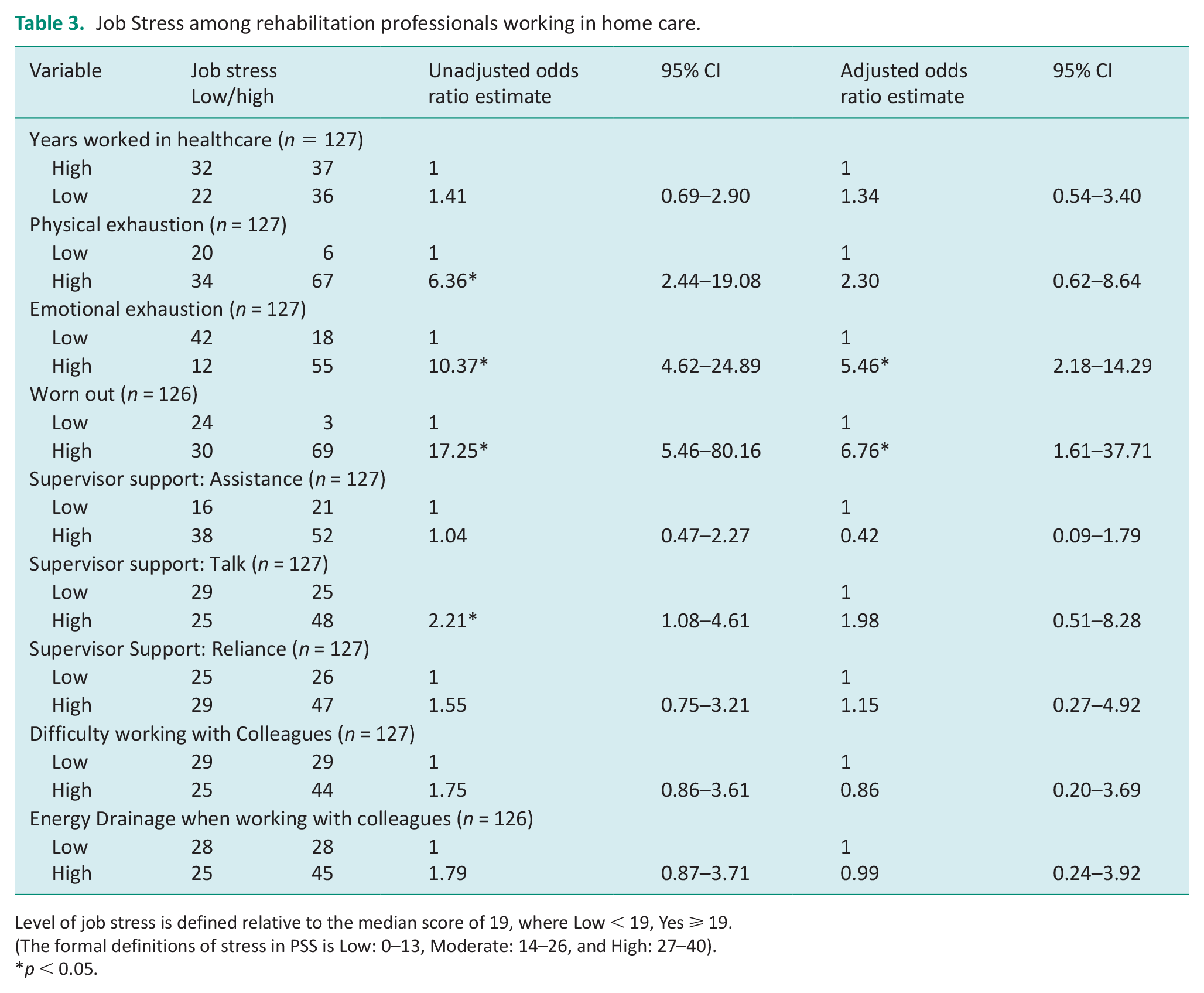
Level of job stress is defined relative to the median score of 19, where Low < 19, Yes ⩾ 19.
(The formal definitions of stress in PSS is Low: 0–13, Moderate: 14–26, and High: 27–40).
p < 0.05.
Burnout among rehabilitation professionals working in home care.
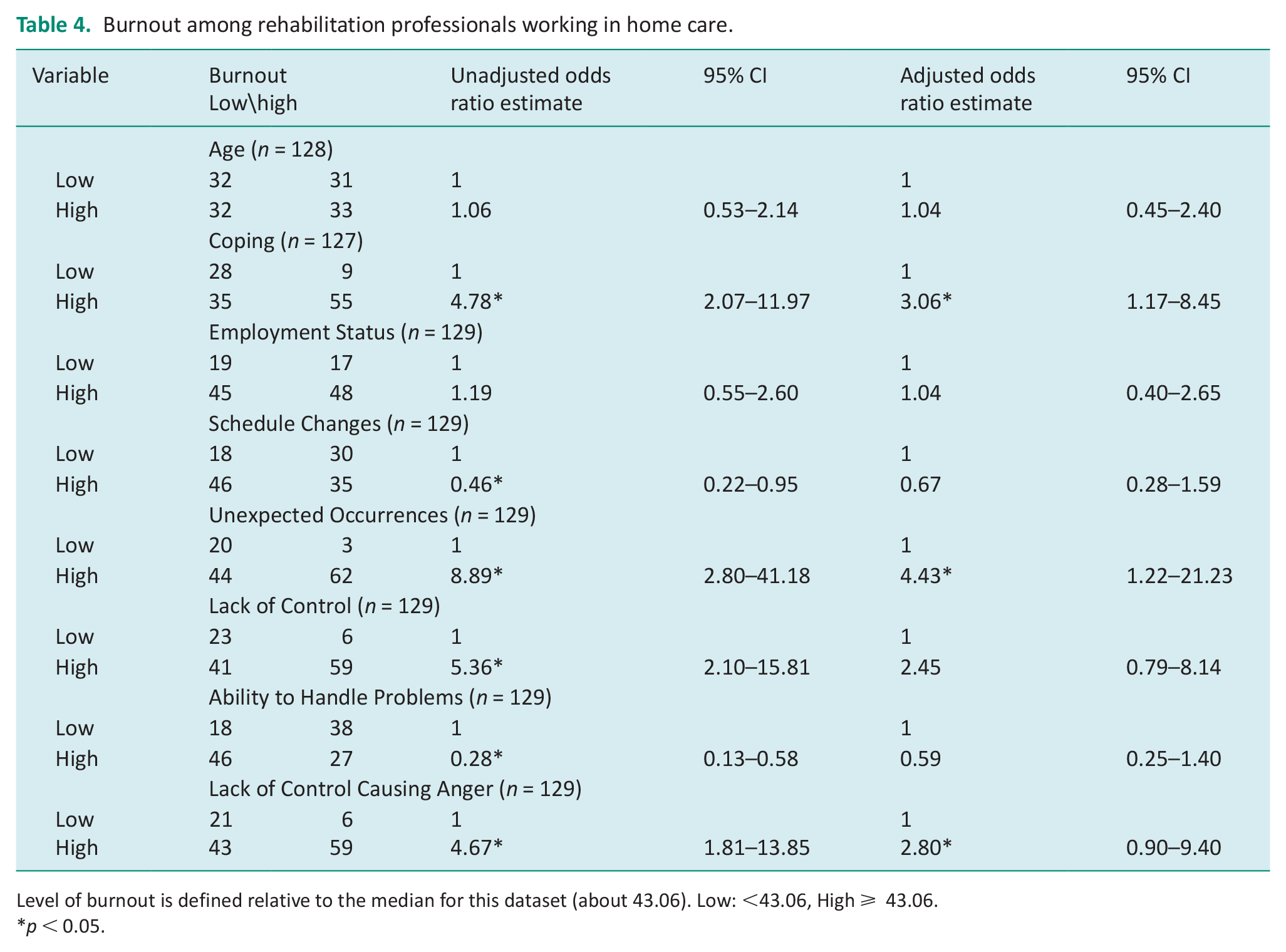
Level of burnout is defined relative to the median for this dataset (about 43.06). Low: <43.06, High ⩾ 43.06.
p < 0.05.
The scores for the PSS had an average of 38.0 across all participants, with a standard deviation of 12.3 and an IQR of 11. Additionally, 82 respondents reported that they were experiencing high levels of stress, whereas low and moderate levels of stress had 53 respondents (10 and 43, respectively). Only two of the eleven potential predictors significantly affected the level of job stress experienced by hcRPs: feeling “worn out” and “emotional exhaustion” (Table 3). Emotional exhaustion was associated with more than five times higher odds of experiencing a high level of job stress (AOR = 5.46, 95% CI: 2.18–14.29). Furthermore, hcRPs were nearly seven times more likely to experience a high-level job stress when they felt “worn out” within the workplace (AOR = 6.76, 95% CI: 1.61–37.71). The remaining predictors such as years worked in healthcare; difficulty coping; physical exhaustion; available support from supervisors in the forms of assistance, talk (level of comfort/ease talking to one’s supervisor) and reliance on supervisors; difficulty working with colleagues, and energy drainage when working with colleagues were not significantly associated with participants’ levels of job stress.
Discussion and implications
Our study aimed to examine the experience of burnout and occupational stress among hcRPs at a large home care organization transitioning out of the COVID-19 pandemic. The study identified predictors of burnout such as the inability to cope, unexpected occurrences, and lack of control leading to anger. Additionally, feeling “worn out” and emotional exhaustion were found to be significant predictors for job stress. In our study with 139 participants, a majority were women and 63% of them were married. No data were collected on the number of children one has; however, prior research has suggested that among occupational therapists, greater levels of burnout have been found in professionals with children in comparison with those without (Balogun et al., 2002; Poulsen et al., 2014). Pustulka-Piwnik et al. (2014) found that physical therapists working with adults in hospitals experienced higher rates of emotional exhaustion and depersonalization among men. This suggests that burnout among physical therapists may be associated with selected demographic and organizational variables contrary to findings of other studies. A Spanish study by Escudero-Escudero et al. have assessed the prevalence and risk factors of burnout syndrome among 758 occupational therapists using Maslach Burnout Inventory—General Survey (MBI-GS) and found that 69.4% of the occupational therapists presented burnout syndrome and especially emotional fatigue (63.5%; Escudero-Escudero et al., 2020). The study highlighted that occupational therapists’ health is clearly at risk from burnout syndrome, which could have an immediate impact on the working environment and how patient interventions are carried out. The challenges of the pandemic resulted in decreased well-being, which in turn made hcRPs with no previous intentions of retiring have desires to leave their career or change their occupation entirely. Specifically, 63.2% of healthcare workers state that occupational stress and burnout are their top reasons for changing their careers. We found that coping (level of difficulty coping with various tasks at hand), unexpected occurrences, and lack of control causing anger as some predictors of burnout. Escudero-Escudero et al. found that burnout had no significant relationships with gender, age, or tenure (Escudero-Escudero et al., 2020). Other studies have also reported that there are no significant relationships of burnout with gender or age (Bruschini et al., 2018; Lloyd and King, 2004).
Difficulty coping with daily tasks was significantly associated with the level of burnout in our study. This is namely due to excessive work responsibilities and constant pressures to be a high achiever, putting a strain on the mental health of hcRPs in the pandemic (Cotel et al., 2021). A Canadian study by Gupta et al on the burnout and the coping strategies of occupational therapists using MBI-GS found that 34.8% of individuals indicated significant levels of emotional weariness, 43.5% reported high levels of cynicism, and 24.6% reported low levels of professional efficacy. The study further added that spending time with family, keeping professional/personal balance, control of job responsibilities, retaining a sense of humor, and self-awareness/self-monitoring were coping techniques. A Danish prospective study by Borritz et al. involving 824 participants using CBI investigated whether burnout predicts sickness absence days and sickness absence spells in human service workers. They found that burnout was prospectively associated with both sickness absence days and sickness absence spells per year. Changes in burnout level from baseline to follow-up were positively associated with changes in sickness absence days. The study concluded that burnout predicts sickness absence and reducing burnout is likely to reduce sickness absence (Borritz et al., 2006). A Portuguese study by Reis has highlighted that burnout among occupational therapists is emerging in an accumulative way and increasing progressively the severity of the symptoms (Reis et al., 2018).
Our results also showed that anger caused due to a lack of control was significantly related to burnout (AOR = 2.80). Thus, hcRPs may be more likely to be angered and experience burnout when things are out of their control. In line with our findings, an Italian burnout study by Bruschini et al. among the hcRPs using Health and Safety Executive Management Standards Indicator tool found control (p < 0.01) as a significant predictor of burnout (Bruschini et al., 2018). Additionally, many staff were burdened with work overload during the COVID-19 pandemic (Hassaine et al., 2022), which contributed to a lack of control over work–life and heightened burnout levels.
Besides, the study also called for implementation of measures (individual, labor, and political) for both the avoidance of burnout in occupational therapists and the reduction of those who suffer from it (Escudero-Escudero et al., 2020). In alignment with our study’s findings on job stress, a Turkish study conducted by Devebakan (2018) using the MBI investigated the relationship between burnout and perceived stress among a sample of 156 healthcare workers and found that stress was positively correlated with both emotional exhaustion and depersonalization. However, they also found that stress and burnout scores were not significantly correlated with sociodemographic variables such as gender, marital status, education level, and working unit (Devebakan, 2018).
Regarding the job stress experienced by the sample, we have analyzed eleven predictor variables in our study. Among the analyzed factors, feeling “worn out” and “emotional exhaustion” had a statistically significant impact on the level of job stress experienced by HcRPs. In this context, Bruschini et al. in their burnout study among 390 Italian hcRPs using the MBI tool found that 14% of the participants were at the risk of burn-out, and there were no significant differences seen among physical therapists, speech therapists, and occupational therapists. However, the study found that there are common mechanisms underlying burnout in the three different professional groups (physiotherapist, speech therapists, and occupational therapists) investigated (Bruschini et al., 2018).
In our study, the AOR for emotional exhaustion was 5.46 indicating that the probability of experiencing job stress increases as emotional exhaustion increases among hcRPs. Furthermore, hcRPs are significantly more likely to experience job stress when they feel “worn out” within the workplace. Another Polish study on burnout syndrome using MBI by Pustułka-Piwnik et al. (2014) among 151 physical therapists found that burnout among physical therapists was characterized by increasing emotional weariness and a diminished sense of personal accomplishment. Another Canadian survey by Spilg et al. (2022) among the 962 healthcare workers including the occupational therapists and PTs concluded that there are elevated moral distress and mental health symptoms in healthcare workers and called for the development of interventions promoting moral resilience as a protective measure against moral adversities (Spilg et al., 2022). Suicidal ideations and mental distress were more prevalent in hcRPs working during the pandemic (Sica et al., 2023). Lloyd et al. have emphasized that repeated exposure to distress and difficult behavior, extended treatments, and an uncertain outcome are all risk factors for occupational stress and burnout among healthcare workers, similar to the findings of our study. However, they have further added that professional status, staffing concerns, and the nature of the practice have been identified as additional risk factors for occupational therapists (Lloyd and King, 2004).
We wanted to examine the nature of burnout and occupational stress among hcRPs transitioning out of the pandemic. According to the postpandemic literature, researchers such as Bassett et al suggest that absenteeism, increased staff rotations, and decreased quality of service are some of the suggested organizational effects of burnout (Bassett and Lloyd, 2001). Another Systematic review by Nowrouzi-Kia et al. on the factors associated with work performance and mental health of healthcare workers during pandemics have identified nine factors associated with work performance and mental health. These are including experiencing feelings of depression, anxiety, having inadequate support, experiencing occupational stress, decreased productivity, lack of workplace preparedness, financial concerns associated with changes in income and daily living, fear of transmission, and burnout/fatigue. The study emphasized that regular and sustained interventions, including the use of information and communication technologies, such as telehealth, are warranted (Nowrouzi-Kia et al., 2022). It was also recommended that it is necessary to address burnout among occupational therapists by creating a healthy and safe environment by identifying the needs and the approach to problems with professional practices (Brown and Pashniak, 2018). Another Spanish qualitative study by Palacios et al. on the physical therapists’ experience in Madrid during described that COVID-19 as an apocalyptic and unexpected war which recommends comprehensive support for the therapists and all frontline workers (Palacios-Ceña et al., 2021).
Our study analyzed various job stress factors namely years worked in healthcare, difficulty coping, physical exhaustion, emotional exhaustion, feeling worn out, available support from supervisors in the forms of assistance, reliance on supervisors and talk (level of comfort/ease talking to one’s supervisor). However, many studies have pointed that fear of making a mistake, a lack of gratitude and feedback from supervisors, an overflow of work, a lack of professional identity and visibility, patient behavior, professional performance in chronic-care situations, a lack of resources, and a lack of time are some sources of exhaustion among occupational therapy professionals (Brice, 2001; Edwards and Dirette, 2010; Scanlan and Still, 2013; Wressle and Samuelsson, 2014). Future studies should consider incorporating these factors in examining burnout among hcRPs.
This study was conducted with home care rehabilitation professionals recruited through a single service provider organization. Although many also worked with other employers, this may limit the generalizability of findings. The cross-sectional design and its timing relative to the pandemic also limit the external validity of the study. Thus, our findings should be interpreted with caution when generalizing them to rehabilitation professionals working in other homecare settings. In addition, future research should consider applying a gender-based analysis lens in women-dominated healthcare settings such as in rehabilitation professionals. Our study was not able to make conclusions based on gender due to limited sample sizes.
Conclusion
This study, which focused on burnout and job stress among home care rehabilitation providers as they emerged from the pandemic crisis, identified that rehabilitation providers’ levels of burnout were significantly more likely to be high if they reported difficulty coping with the tasks at hand, experienced unexpected occurrences, or experienced a lack of control causing anger. hcRPs were significantly more likely to experience a high level of job stress when they felt “worn out” within the workplace or reported emotional exhaustion. These findings indicate a need for support for hcRPs to handle this crisis situation. The high prevalence of burnout and high levels of job stress should raise significant concerns for employers of rehabilitation providers, since job dissatisfaction, low organizational commitment, absenteeism, and high turnover have all been linked to work-related stress and burnout. These challenges highlight an opportunity for occupation-based support for rehabilitation providers. Opportunities for interventions to address the identified risk factors for burnout and job stress could include policies such as encouraging and supporting staff to maintain a healthy work–life balance (e.g., through limiting over-time requests), ensuring adequate staffing (to the extent possible given the current health human resource crisis), and by encouraging staff to access their employer-supported counseling services.
Key findings
hcRPs commonly identified predictors for burnout (e.g., inability to cope).
The probability of experiencing job stress in hcRPs increases as emotional exhaustion increases.
Significant associations were found between coping with daily tasks and burnout levels, due to lack of control and experiencing unanticipated incidents.
What has this study added to the literature
Our study found work stress and burnout influence coping, unexpected circumstances in hcRPs work–life. Furthermore, highlighting the need to provide organizational support and policies that specifically address these issues in the home care sector.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226241269251 – Supplemental material for Burnout and occupational stress of home care rehabilitation professionals transitioning out of the COVID-19 pandemic in Ontario, Canada
Supplemental material, sj-docx-1-bjo-10.1177_03080226241269251 for Burnout and occupational stress of home care rehabilitation professionals transitioning out of the COVID-19 pandemic in Ontario, Canada by Behdin Nowrouzi-Kia, Emily King, Brydne Edwards, Sonia Nizzer, Amin Yazdani, Basem Gohar, Ali Bani-Fatemi, Aaron Howe, Yusra Fayyaz, Bushra Alam, Raabia Khan and Vijay Kumar Chattu in British Journal of Occupational Therapy
Footnotes
Acknowledgements
We thank and acknowledge all participants for their time and contribution to this work.
Research ethics
The University of Toronto Research Ethics Board approved of this project (Approval number: 00042041).
Consent
All participants provided informed written consent.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was: Not included at any stage of the research.
Data availability
Available upon request of the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Social Sciences Humanities Research Council partnership engagement provided funding to produce this project. (Award number: 892-2021-1085).
Contributorship
BNK conceptualized the study and wrote the initial draft. YF, BA, and RK assisted with the data analyses. EK, BE, SN, AB, AH, YF, BA, RK, VKC, BG, ABF, RK, and VKC reviewed and provided feedback for the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.