
Abstract
Introduction:
While a small number of occupational therapists have additional training as driver assessors, all occupational therapists have a duty of care to address driving as an occupation. This study aimed to develop a resource to support Australian non-driver trained occupational therapists in daily practice to address driving with clients who may require on-road assessment due to a health concern.
Method:
A literature review and comprehensive process for the development of a driving clinical decision pathway was followed using four phases. A virtual nominal group technique was used to investigate the content validity of the driving clinical decision pathway. Purposive sampling was used to recruit two groups of occupational therapists to participate in a virtual nominal group technique.
Results:
A driving clinical decision pathway was developed with five key sections. The 11 participants attended 1 of 2 virtual nominal group technique for 120 minutes each, where 100% consensus was achieved with both groups relating to the content validity of the clinical decision pathway content, and ease of use.
Conclusion:
Driving is a meaningful goal for all adults who have health-related challenges. A comprehensive driving clinical decision pathway has been developed and made available that supports Australian non-driver trained occupational therapists to address driving as an occupation that maintains individuals’ independence and public safety.
Introduction
With a growing ageing population, there is increasing need and desire for people to drive a motor vehicle. All occupational therapists have a role to play in addressing driving with people who experience a change in health; however, there is a lack of resources to support non-driver trained occupational therapy practice. This article describes the development of a driving clinical decision pathway (CDP) and presents preliminary evidence to support its content validity and clinical utility.
Literature review
Driving is a meaningful occupation that provides adults of all ages with freedom, independence and ease of access to their communities (Liddle et al., 2008). Austroads (2022), the association of the Australian and New Zealand transport agencies describes driving a motor vehicle as a complex skill which requires the interplay of sensory, cognitive and physical functions, with the motor vehicle and the environment for safe driving performance. There are various health conditions that can temporarily and/or permanently impact on driving skills, and therefore appropriate assessment and intervention is needed to ensure that people who have such health conditions can return to driving if safe to do so or explore alternative mobility options if unsafe (Unsworth et al., 2007). This decision-making is important to prevent negative consequences associated with premature driving cessation (Liddle et al., 2008), promote public road safety (Austroads, 2022) and enhance health and well-being.
Occupational therapists are experts in assessing the impact of various health conditions on activities of daily living, including driving (Dickerson et al., 2014). Occupational therapists have long been addressing driving issues in multiple countries such as the United States and Canada (Korner-Bitensky et al., 2006), Australia (Unsworth, 2007), the United Kingdom (Harries and Unsworth, 2013), Ireland (Stapleton et al., 2015) and Sweden (Larsson et al., 2007). In many of these countries, occupational therapists have completed post-graduate training in driver assessment and rehabilitation to become occupational therapy driver assessors (OTDAs) or Certified Driving Rehabilitation Specialists (CDRS). This certification enables completion of comprehensive driver assessment including clinic-based and on-road driving assessments. OTDA practice is well-supported by driving guidelines (Di Stefano and Ross, 2018) and competency standards (Fields and Unsworth, 2017) in Australia where this study was conducted which support best practice and provide equitable and consistent methods of practice. However, all occupational therapists including those without this specialised driver training, also known as non-driver trained occupational therapists or non-OTDAs have a duty of care to address driving as an occupational performance area (Dickerson et al., 2014). Role differentiations between OTDAs and non-OTDAs in the field of driving has been described elsewhere (Dickerson et al., 2014; Scott et al., 2021; Stapleton et al., 2015), but key differences between these roles pertain to the type of driving recommendations provided. For example, while OTDAs predominately provide driving outcome recommendations regarding whether individuals are safe to resume driving or not following on-road assessment, non-OTDAs provide driving process recommendations which focuses on determining the appropriate type and timing of further assessment in order to return to driving. However, research has identified gaps internationally in non-OTDAs’ knowledge of driving processes and process recommendations (Scott et al., 2021) and their confidence in being able to apply assessment findings to driving (Dickerson and Bedard, 2014). This research suggests that further resources are needed to support non-OTDA practice to ensure that driving is consistently addressed by all occupational therapists, as both roles have ethical and legal obligations (Austroads, 2022).
Resources commonly used in healthcare to support clinical decision making include clinical guidelines, clinical care pathways and clinical decision trees or algorithms (Miller et al., 2005). Clinical guidelines and decision trees are developed based on substantial evidence which provides clinicians with guidance on what to do in practice. However, the development of clinical guidelines is not yet possible in non-OTDA practice as research into the role of non-OTDAs in driving is almost non-existent, with only two Australian studies to date (Marnane et al., 2023; Scott et al., 2021). Additionally, clinical guidelines drawn on theories which describe how clinicians select and weigh information to arrive at specific decisions (Miller et al., 2005). Within the area of driving, Social Judgement Theory (SJT) has been used to understand how OTDAs weigh information or cues to make decisions about a whether a person is fit to drive or not (Unsworth et al., 2015). However, this approach does not support non-OTDA practice, which requires theories that focus on driving processes and the appropriate type and timing of driving-related referrals. Clinical pathways are also known as integrated care pathways, critical pathways, CDPs, care plans and care paths. These terms refer to a complex intervention which provides structure and organises care processes that improve the consistency of care, documentation practices and maximise outcomes of specific groups (Rotter et al., 2010). Many theories can underpin the development of clinical pathways, such as the Lean Six Stigma, the Theory of Constraints and the Critical Path Method (Schrijvers et al., 2012). The Critical Path Method includes a two steps: the first, describing key steps for inclusion in the pathway and the second, setting up a flow chart with relevant time points of when to address each step (Schrijvers et al., 2012) which was used to inform the development of the driving flowchart to support the non-OTDA role in the field of driving.
A literature review was undertaken to determine if any occupational therapy driving pathways exist internationally that could be adopted or modified for use by non-OTDAs in Australia. The databases CINHAL, Medline and Web of Science were searched between 2000 and 2021 using the terms clinical decision pathway OR care pathway OR clinical decision pathway OR critical pathway OR integrated care pathway AND driv* AND occupational therapy. Given the large volume of driving research, additional hand searching of retrieved articles was also completed. Two American (Dickerson and Bedard, 2014; Dickerson et al., 2018) and one Irish (Stapleton et al., 2015) pathways were identified. Dickerson and Bedard (2014) developed a framework which includes clinical decision-making questions for activities of daily living tasks based on Michon’s (1985) model for understanding driving behaviour. This model is helpful in providing non-OTDAs with a framework to inform how deficits in everyday functional tasks may impact on driving performance. Dickerson et al. (2018) also developed a flowchart which provided a holistic view of community mobility including driving. This flowchart outlined steps a non-OTDA can take in addressing driving, which differentiated OTDA and non-OTDA roles with colour-codes. This flowchart is helpful in providing a structure to aid non-OTDAs’ clinical reasoning surrounding how to manage driving with clients, while also promoting how health professionals can address driving together. Stapleton et al. (2015) also developed a flowchart which stratified driving outcomes post-stroke including ‘fit to drive’, ‘maybe’ and ‘unfit/not appropriate for driving’. He highlighted high and low threshold factors which guided health professionals’ reasoning on which category clients are stratified into using clinical and functional assessment tools. While these pathways individually provide important elements to guide non-OTDA clinical reasoning, they do not entirely address gaps to guide practice. For example, non-OTDAs require information about the return to driving processes that align with national medical guidelines and state-based licencing jurisdictions processes and legislation. Furthermore, non-OTDAs require details about the appropriate type and timing of referrals or interventions to streamline decision-making, for example knowledge of national driver medical standards, and non-driving time periods, to inform when to refer a client to a medical practitioner for medical clearance to resume driving (Austroads, 2022).
To address the identified gaps in the research, a comprehensive driving CDP that can guide non-OTDA practice for drivers following a change in health is needed in Australia. When developing a new pathway, such as the one described in this article, it is important to ensure that is has strong psychometric properties and that it is practical to use in a clinical setting. Therefore, the purpose of this article was to describe the development and contents of the driving CDP and begin to explore its psychometric properties. The specific aims were to: (1) provide an overview of the development of the driving CDP and (2) evaluate its content validity and clinical utility.
Method
This mixed methods research was guided by a pragmatic approach, where both qualitative and quantitative data were collected simultaneously. Participants’ written and verbal feedback (qualitative data) allowed for interpretation of participants votes on content validity and clinical utility (quantitative data) for each section of the CDP. Ethical approval for the study was sought and granted by Federation University Human Research Ethics Committee (2022-069).
Design statement
To address the first aim, pathway development processes were examined. A review by Harkleroad et al. (2000) summarises the options for pathway development. Gordon’s (1995) delineation of pathway development was identified as the most comprehensive, which included 24 steps within 4 phases; (1) focus and recognition, (2) evaluation and analysis, (3) development and (4) implementation and evaluation. The first three phases are presented in this paper.
To address the second aim to evaluate the content validity and clinical utility of the newly developed CDP, a nominal group technique (NGT) was adopted. The NGT is a highly adaptable consensus methodology (McMillan et al., 2016) for establishing content validity, ensuring that the CDP covers all areas for a non-OTDA to fulfil their role to address driving (Portney and Watkins, 2009). This technique was selected over other consensus methodologies, such as the Delphi technique, due to its ability to gather rich data within a structured and stimulating environment. A virtual nominal group technique (vNGT) was chosen to allow for participants across Australian states to attend face-to-face (virtually) and to reduce participant time burden. While various NGT modifications exist, most versions consist of the following six steps: (1) introduction, (2) silent idea generation, (3) round robin, (4) clarification, (5) scoring and (6) discussion (Thier and Mason, 2019) which were employed in the present research.
Participants
To meet the second aim, purposive sampling was used to recruit two groups of ‘expert’ participants, with written consent obtained (Liamputtong, 2021). Group 1 consisted of Australian non-driver trained occupational therapists who worked in settings connected to a public health service with adults (aged 18 years or older) who were drivers or who had the potential to drive. Clinicians who worked solely with paediatrics were excluded. Occupational therapy managers of large public health services were contacted via email to gather senior clinician contact details. Public health services in Victoria, Australia, were selected as representative of non-OTDA practice across Australia. Group 2 consisted of Australian clinicians who had completed post-graduate training to become OTDAs. Members of the professional peak body, Occupational Therapy Australia’s National Driving Taskforce were (n = 6) invited to participate via email. Participation across Australian states was purposively sampled to allow for holistic feedback, as the CDP is targeted for Australian clinicians.
Instruments
For the first aim, all researchers were identified as experts in the field of driving having worked clinically as OTDAs and through conducting research in this field. The researchers participated in multiple sessions to review the literature, existing OTDA guidelines and resources and, brainstorm key elements that non-OTDAs would require to fulfil their role in addressing driving. While the content of existing OTDA guidelines was not relevant for non-OTDAs (Di Stefano and Ross, 2018), the structure and some sections were identified for content modification to reflect the non-OTDA role such as the introduction of key stakeholder roles, legal and medical standards, assessments and contact/resources. This informed the initial development and sections of the CDP. Existing driving pathways in the literature and further brainstorming of ways to address identified gaps informed the development of the driving flowchart and documentation templates. The researchers reviewed successive versions of the CDP separately and together to finalise the CDP (Scott et al., 2023). Administerial programmes were used to develop various sections of the CDP such as Microsoft Word, Adobe Acrobat Pro and Lucid Chart.
For the second aim, participants were emailed an information package and questionnaire in preparation for the vNGT. The information package contained details of vNGT procedures and background to the study aims, all of which aligned with step 1 (introduction) of vNGT. A questionnaire was developed which asked participants two questions for each section of the CDP: (1) ‘do you agree that this section of the pathway includes all relevant information?’ which addressed content validity and (2) ‘do you agree that this section of the pathway is user friendly?’ which addressed clinical utility. This aligned with step 2 (silent idea generation) of the vNGT which allowed participants to independently generate ideas/comments from the questions posed. The ‘ideaflip.com.au’ programme was utilised within the Microsoft Teams platform to visually present participants’ responses on post-it notes for further discussion.
Procedure
For the first aim, three phases of Gordon’s (1995) pathway development were followed. The focus and recognition phase reviewed the literature which identified the content gaps and the need for the CDP development. The second phase assessed and analysed whether these gaps in the literature were due to performance or process problems to determine how a CDP would address the gaps in the literature. This process identified critical elements for inclusion in the third phase which involved the development of the CDP. A review of existing driving CDPs identified useful elements which were modified for inclusion in the CDP such as the use of a flowchart (Dickerson et al., 2018), development of decision-making questions about how performance in daily occupations may impact on driving skills (Dickerson and Bedard, 2014), and use of both clinical and functional assessment tools (Stapleton et al., 2015). Once a version was established for overview by experts, content and utility testing was then required, as discussed in the second aim of this paper.
For the second aim, the vNGT protocol used was an adaptation of McMillian’s (2016) procedure which involved six steps. Steps 1 and 2 were completed prior to the vNGT session, which is described as pre vNGT data. Participants completed the subsequent 3 to 6 steps virtually for 120 minutes using the Microsoft Teams online platform, which is described as post vNGT data. Data were collected on two separate days approximately 2 weeks apart in October 2022, with both vNGT groups audio recorded. Suggestions from OTDAs participating in the second vNGT were not included in the post-vNGT consensus vote by non-OTDAs who participated in the first vNGT. Please refer to Table 1 for further details of the procedure.
Virtual nominal group procedure and data analysis.
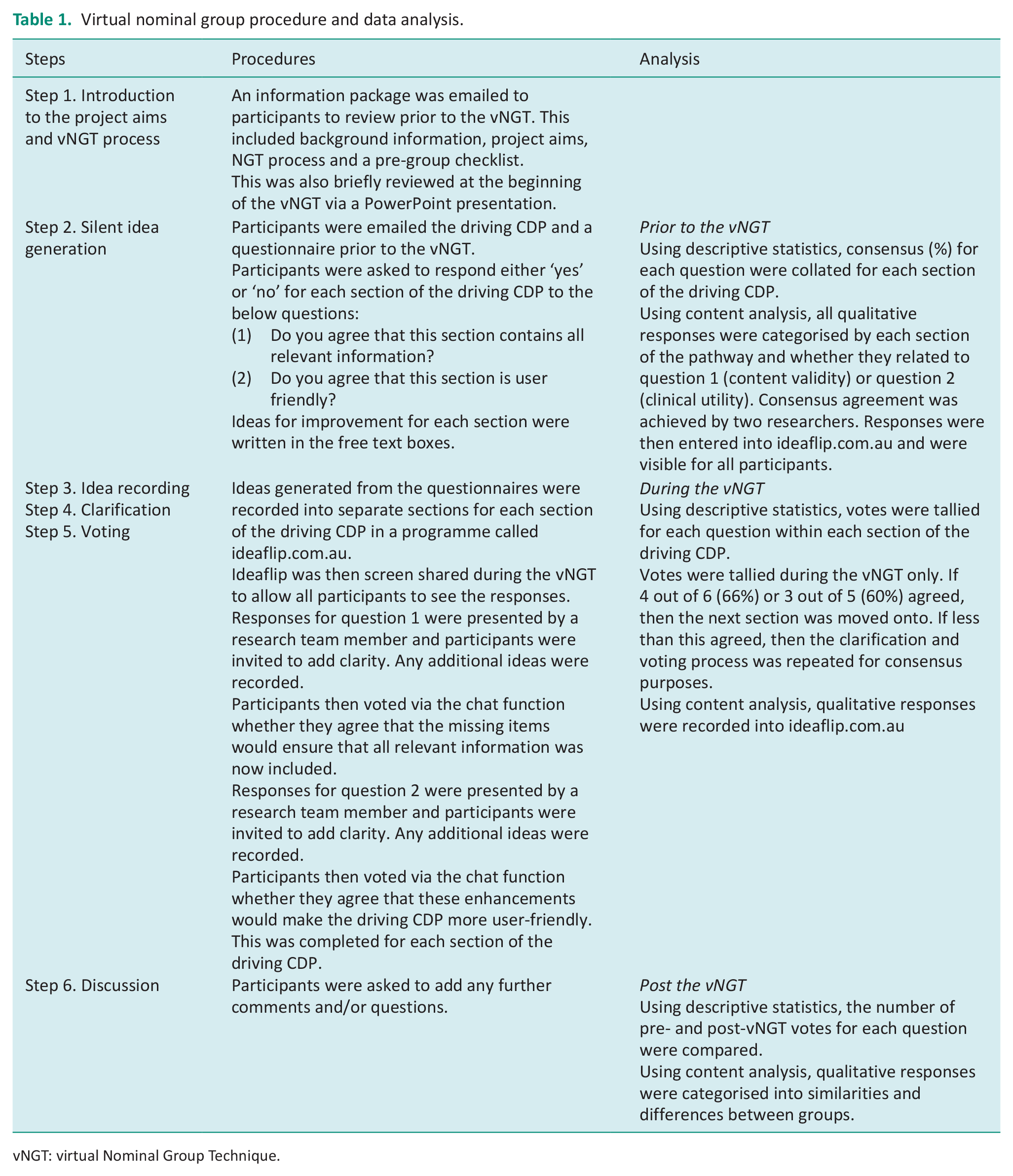
vNGT: virtual Nominal Group Technique.
Data analysis
The data analysis strategy for the vNGT is presented in Table 1. The content analysis as presented in Table 1 followed the generic process of qualitative data analysis which included the following steps: (1) preparation, (2) organising the data into categories and (3) reporting the data (Liamputtong, 2021). Consensus agreement between two researchers was achieved when coding the data to maximise study rigour.
Results
In relation to the first aim, the driving CDP was developed and the content includes an executive summary and flowchart, introduction to driving as an occupation and the roles of key stakeholders, legal and medical standards, evidence-based practice summaries, assessment tools and clinical reasoning prompts for interpretation of assessment results, communication and documentation templates and other various resources. To access the completed driving CDP, please visit otdrivingclinicaldecisionpathway.wordpress.com
In relation to the second aim, a total of 11 participants attended one of the two vNGT; 6 non-OTDAs (54%) and 5 OTDAs (46%) with one OTDA drop out in group two due to a conflicting appointment. All participants were female, either from the state of Victoria (72%) or New South Wales (28%), with 16.6 (4.7 SD) years of experience, range of 7–23 years.
In relation to the second aim, pre- and post-vNGT consensus was similar across both groups. Data from the participants’ pre vNGT presented suggestions for further information to be included in the CDP and for modifications to the layout of the pathway to increase readability. All pre-vNGT data were discussed within the vNGT, where participants achieved 100% consensus that the CDP contains all relevant information and is user-friendly. See Table 2 for details for participant responses within each group. Pseudonyms have been used for anonymity of participant quotes.
Driving clinical decision pathway sections and content validity and clinical utility responses from both virtual nominal group technique groups.
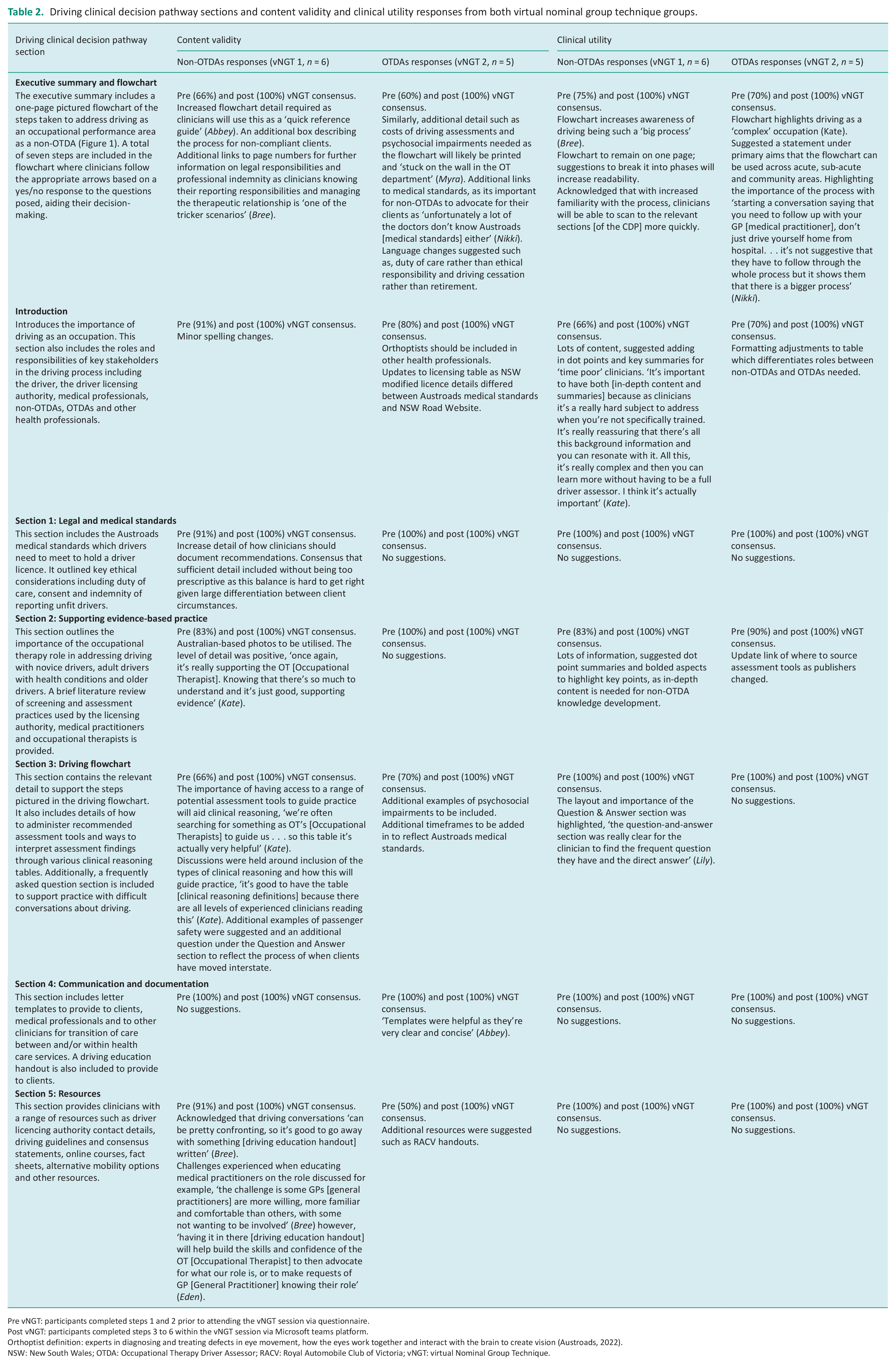
Pre vNGT: participants completed steps 1 and 2 prior to attending the vNGT session via questionnaire.
Post vNGT: participants completed steps 3 to 6 within the vNGT session via Microsoft teams platform.
Orthoptist definition: experts in diagnosing and treating defects in eye movement, how the eyes work together and interact with the brain to create vision (Austroads, 2022).
NSW: New South Wales; OTDA: Occupational Therapy Driver Assessor; RACV: Royal Automobile Club of Victoria; vNGT: virtual Nominal Group Technique.
Both vNGT group responses were categorised and then similarities and differences in these responses were grouped. Both OTDAs and non-OTDAs identified driving as a complex occupation, and noted the pictured driving flowchart is a useful document in guiding non-OTDAs through a process to address driving. Similarly, groups reported that the CDP was very comprehensive with a range of sections to support practice and, that the CDP could be used for multiple purposes such as orientation of staff, within supervision and for educational purposes. Key differences between groups involved OTDAs attending to the content of the CDP such as medical standards and time frames, whereas non-OTDAs responses related more to the practical use of the CDP such as changes to the layout and dot point summaries to support easy use in clinical practice.
Discussion and implications
The role of health professionals including non-OTDAs is crucial in addressing road safety and maximising quality of life for all client groups. However, in Australia, no CDP existed to guide non-OTDA clinical reasoning in this area of practice. A CDP for occupational therapists which included information about the roles of key stakeholders within the driving process, evidence-based assessment tools within the field of driving and tables to support clinical reasoning was needed. Additionally, a flowchart to guide clinicians through the process of addressing driving as an occupational performance issue with key medical standard timeframes was also necessary. This driving CDP appears to be the first to comprehensively assist non-OTDAs to address driving in Australia. Findings from this study have provided feedback to ensure that the CDP contains all of the necessary information and that it is user friendly for non-OTDAs in daily practice, thus representing a resource that has the potential to be valid and clinically useful. Further details of modified key sections of the driving CDP will be discussed below.
Introduction section of driving CDP
While driving is a meaningful occupation, the complexity of this task means that addressing driving as an occupational performance issue can be a detailed and lengthy process that involves various stakeholders at different timepoints. Health professionals report a lack of knowledge of stakeholder roles such as whose responsibility is it to determine whether a person is fit to drive, who to report driving fitness to, when is the appropriate time to do so and what their legal and ethical responsibilities are (Scott et al., 2021). These role confusions are also found among medical practitioners who describe reduced knowledge, confidence and time to adequately address fitness to drive (Jitkritsadakul and Bhidayasiri, 2016; Marshall et al., 2012). Finally, role confusion also exists within the occupational therapy profession, with advanced scope of practice roles in Australia (Scott et al., 2021). In the present research, participants in the vNGT reported that the introduction section of the CDP, which includes key role differentiations within the field of driving, was helpful in determining the scope of practice of non-OTDAs. Participants also reported that a simplified process which included relevant timepoints of what actions to undertake and when, such as screening for unilateral neglect up to 3 months post stroke, will support their practice.
Executive summary and flowchart
Time demands are frequently reported by clinicians as a barrier to efficient and evidence-based practice (Harding et al., 2014). A quick reference guide to address driving as an occupational performance issue was identified through the vNGT as an effective solution to this problem, with a flowchart recommended. Participants reported that this would be used as the ‘go-to’ document within the CDP (see Figure 1); therefore, further key pieces of information were included for increased clinical usefulness. For example, the inclusion of key reporting legislation and indemnity cover to indicate to users what their roles and levels of protection are, were noted as helpful. The inclusion of approximate costs when referring to OTDA for comprehensive assessment was noted as beneficial for clinicians to easily educate their clients. Lastly, the inclusion of key page numbers with hyperlinks so that clinicians can quickly refer to the section for further information was provided. While clinicians reported that the summary points were helpful in supporting time poor clinicians, the inclusion of evidence-based information further described in detail in section 2 of the CDP, supports the flowchart but also provides key knowledge that novice clinicians require to develop their clinical reasoning in this area. Participants also acknowledged that with increased familiarity of the CDP, over time, clinical utility will be further enhanced.
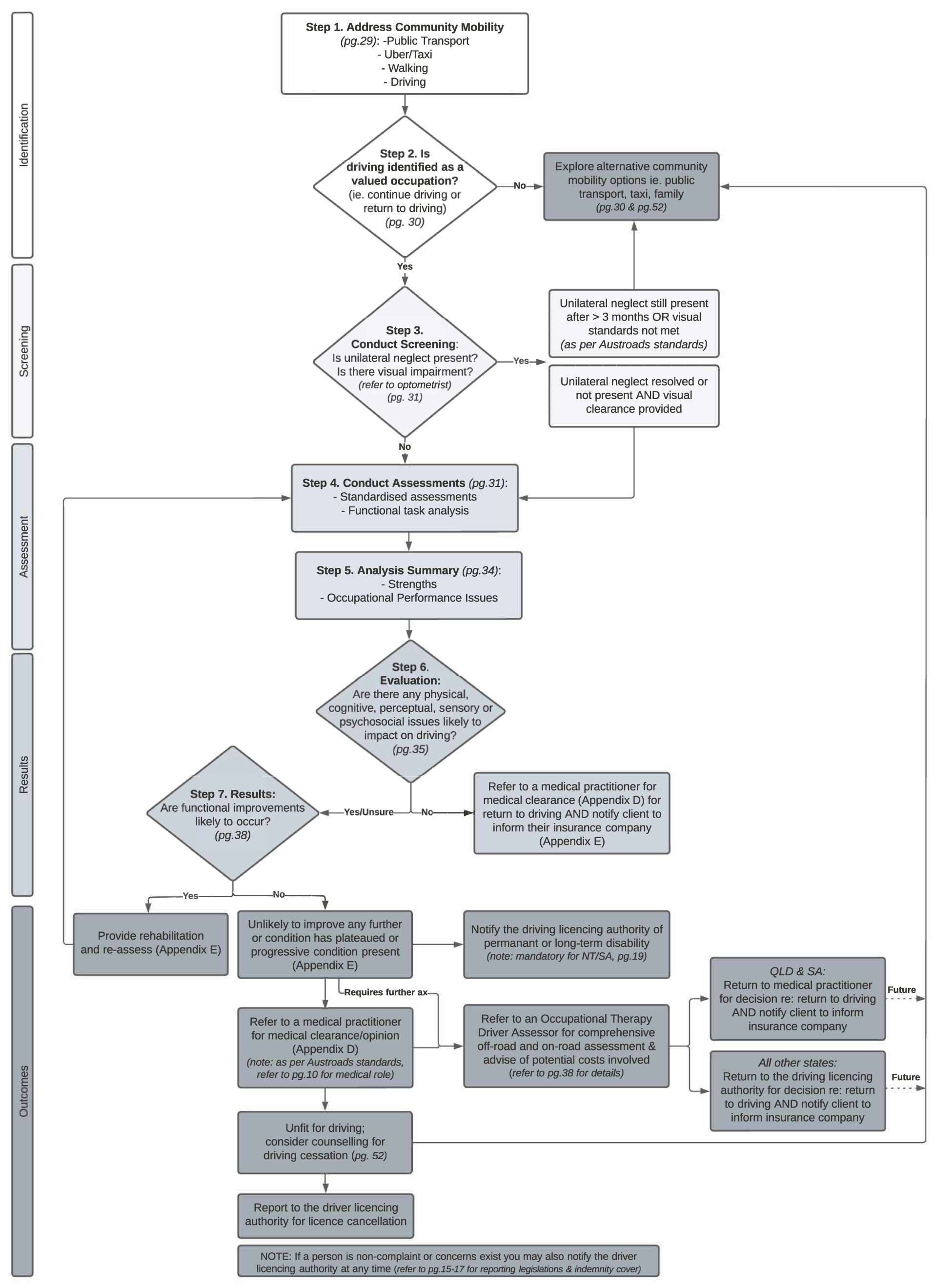
Driving Flowchart.
Information to guide non-OTDAs through using the flowchart
A key component missing from existing driving pathways was the inclusion of recommendations of assessment tools to guide non-OTDA clinical reasoning. Participants in the vNGT acknowledged that behind the wheel or on-road driving assessment is the ‘gold standard’ in assessing fitness to drive, however, noted that confusion occurs in how to assess a client to determine the need and timing for this. Within the area of driving, there is a wide range of clinic-based (or off-road) assessment tools used in predicting whether an individual will pass or fail their on-road driving test (Unsworth et al., 2012). While no one singular tool can predict driving performance, a combination of assessment tools has shown improved predictability in driving outcomes (Dickerson et al., 2014). Further, some of these assessment tools have cut off scores which may guide clinical reasoning when determining the appropriate timing for OTDA referrals. Therefore, in the present CDP, several standardised and functional assessment tools were included to aid decision making, as supported by Stapleton et al. (2015). When clinicians use functional assessments, they often rely on clinical reasoning to help interpret and make sense of this information. Novice clinicians benefit from prompts to assist with their decision-making; therefore, various tables were developed which outline guiding questions linking a variety of occupational performance issues, associated cognitive, psychosocial, physical, perceptual and sensory impairments and potential driving skills impacted. Clinical reasoning definitions developed by Unsworth (2021) were also included for additional support. This will further assist clinicians clinical reasoning when interpreting assessment findings and applying this to driving, which was similarly utilised in Dickerson and Bedard (2014)’s pathway.
Communication and documentation
Consistent documentation practices in assessment and intervention are assumed in healthcare; however, inconsistencies in the field of driving still occur (Scott et al., 2021). Given that we know that time is often a barrier to detailed documentation; key documentation templates were developed and included in the CDP to reduce time for clinicians (Moy et al., 2021). These included letters to key stakeholders, the medical practitioner and the client. As driving occurs across the continuum of care, to align with a client’s journey and to prevent gaps in communication within these stages, a handover template was also developed which clinicians can use within and across healthcare services.
Driving is a sensitive topic for many clients with negative consequences associated with driving cessation for not only the individual but also for their carers (Unsworth et al., 2007). As a result, driving as an occupational performance area is often not consistently discussed by medical professionals which may occur due to knowledge gaps (Jitkritsadakul and Bhidayasiri, 2016), the potential to damage the therapeutic relationship (Jones et al., 2012) and the associated confronting conversations. In the present CDP, the driving education handout was developed to provide to clients during initial conversations about driving. The handout describes driving as a privilege, not a right, and outlines the responsibilities of the driver in reporting their health status to the licencing authority. The handout also outlines who makes decisions about driving ability in this case, in Australia. The participants in the vNGT noted that this was helpful in supporting clinicians to have difficult conversations which clarify the responsiveness of different health professionals and the role of the licencing authority. It was also identified that medical practitioners are often not aware of medical guidelines and their role within the driving decision process (Mardh et al., 2017); therefore, the handout developed could be a useful document to have conversations with medical practitioners to holistically support the client within the driving process; however, further research to investigate the usefulness of the handout is needed.
In summary, the driving CDP is a comprehensive clinical pathway that provides clear descriptions of other health professional roles in driving such as medical practitioners, optometrists, psychologists, physiotherapists, nurses and diabetes educators, a simplified process of the non-OTDA role with a range of resources enabling role fulfilment including assessments, clinical reasoning tools, letter templates and alternative mobility options following driving cessation. It was identified that there could be many purposes for this document including orientation procedures for new staff, learning and as a reflection tool during supervision and, also as an educational tool at universities in preparing students for the workforce.
Limitations and directions for future research
The development of a new resource like the CDP takes time and repeated research to assure its validity and clinical utility. This is the first study to describe the CDP development and initial psychometric properties; however, further studies including piloting of the CDP to evaluate its effectiveness in clinical practice are needed. A modified version of a NGT was used to evaluate the CDPs content validity and clinical utility, which was completed virtually. A potential limitation of this design is that participants voted online with other participants present; therefore, voting bias may have occurred due to the presence of one’s peers and therefore lack of privacy. Additionally, all non-OTDAs were practicing within a public healthcare setting and all OTDAs were practicing in private practice. While this may initially appear to present a bias, this is in fact representative of typical practice in Australia. A further limitation is that the CDP was largely developed and reviewed by clinicians from two states in Australia. However, these clinicians were identified as experts in the field of driving and all OTDAs participated in the National Driving Taskforce membership within the professional peak body, this has given them a national oversight of occupational therapy driving practices in Australia. As a result of this membership, they had knowledge of jurisdictions and practices within other Australian states; however, the inclusion of clinicians from other Australian states and outside of public health settings would be beneficial in the review of subsequent updates to the CDP sections such as legal/regulatory requirements, local resources and contact details of supports. Feedback from novice clinicians is also suggested in this review process, given they are the cohort likely to benefit most from the driving CDP. A final limitation is that the driving CDP was developed for use by Australian non-OTDAs which reflect context-specific roles and licencing jurisdictions. However, this article provides a detailed description of the development of a driving CDP, and this process could be used for making contextual adaptations (i.e., Section 1: Legal and Medical Standards and Section 5: Resources and Contacts) to this CDP for future use in other countries. Additionally, while general mental health guidelines for safe driving were included in the resources section of the CDP (Dun et al., 2023), future adaptations to the CDP could address specific mental health conditions.
Conclusion
This article has described the development of a driving CDP and provided preliminary evidence to supports its use in Australia. Occupational therapists are well placed to address driving as an occupational performance issue, particularly with OTDAs being able to report assessment findings and make recommendations about fitness to drive. However, non-driver trained occupational therapists have been expected to address driving as an occupational performance issue with only limited resources. The driving CDP developed in the present research has been identified as a comprehensive resource to support non-driver trained occupational therapists with addressing driving in clinical practice. While this CDP supports Australian clinicians, with appropriate contextual adaptations, this CDP could also be used to support other health professionals internationally to address driving throughout its entire process, holistically supporting public health risk and safety.
Key findings of this paper
A driving clinical decision pathway (CDP) containing five sections can comprehensively support occupational therapy practice.
The inclusion of a flowchart in the driving CDP promotes timely guidance for busy clinicians.
What this study adds to the field
A detailed process for the development of an evidence-based driving clinical decision pathway has been provided along with preliminary evidence to support its content validity and clinical utility. The driving clinical decision pathway developed is freely available for use by non-driver trained occupational therapists when addressing driving with clients in daily practice.
Footnotes
Acknowledgements
The authors would like to acknowledge the occupational therapists who participated in this study for their knowledge and contributions.
Research ethics
The study was conducted in accordance with protocol number 2022-069 by Federation University Human Research Ethics Committee.
Consent
Written informed consent to participate was obtained from all participants in the study.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research received funding from the Graduate School of Research at Federation University.
Contributorship
All authors meet the criteria for authorship. Individual contributions are specified as follows; conceptualization, H.S., A.B and C.U; methodology, H.S., A.B and C.U; software, H.S and C.U; validation, H.S and C.U.; formal analysis, H.S and C.U; investigation, H.S and C.U.; resources, H.S and C.U.; data curation, H.S.; writing—original draft preparation, H.S.; writing—review and editing, H.S., A.B and C.U.; visualization, H.S and C.U; supervision, C.U; project administration, H.S.; funding acquisition, H.S and C.U. All authors have read and agreed to the published version of the manuscript.