
Abstract
Introduction:
Constraint-induced movement therapy has been shown to be effective in a sub-group of sub-acute stroke survivors but has not been widely implemented in the United Kingdom. This study explored therapist and stroke survivor perceptions and experiences of constraint-induced movement therapy and explored the non-agreement (incongruence) and agreement (congruence) of these perspectives.
Method:
Consenting occupational therapists (n = 3) and physiotherapist (n = 5) participated in a focus group discussion. Four-stroke survivors undertook pre- and post-constraint-induced movement therapy interviews. Stroke survivor participants selected and undertook an evidence-based constraint-induced movement therapy protocol. Focus groups and interview audio recordings were independently analysed thematically. Therapist and stroke survivor views were subsequently synthesised using meta-ethnographic principles.
Findings:
Four over-arching themes were identified: motivation and determination to participate in constraint-induced movement therapy; who benefits; which protocol; making constraint-induced movement therapy feasible. The final over-arching theme comprised five sub-themes: fatigue and sleep; pain; transport; need for support; training, support and mentorship for therapists. Stroke survivors and therapists held contrasting views on three themes.
Conclusion:
Participating stroke survivors successfully undertook a self-selected, evidence-based constraint-induced movement therapy protocol. The identified enablers and barriers should inform future constraint-induced movement therapy protocol development. The contrasting views held by therapists and stroke survivors reinforce the need for collaborative communication and opportunity for choice during constraint-induced movement therapy.
Keywords
Introduction
Approximately 70% of stroke survivors experience arm weakness with an estimated 40% continuing to have a long-term reduction in arm function (Intercollegiate Stroke Working Party, 2023). Constraint-induced movement therapy (CIMT) is a therapeutic intervention to address arm impairment, comprising three components: (1) constraint of the ipsilesional arm; (2) intensive practice of tasks with the contralesional arm; and (3) a behavioural transfer package component (Kwakkel et al., 2015). CIMT literature also describes ‘shaping’ in the practice component to gradually move the person towards achieving new motor goals through meaningful challenge and feedback (Taub et al., 1994). Despite evidence indicating a beneficial effect of CIMT for stroke survivors with some recovery in the arm and hand post-stroke (Kwakkel et al., 2015) and its potential to provide the intensity recommended by clinical guidelines (Intercollegiate Stroke Working Party, 2023; Stroke Foundation, 2023), previous studies (Christie et al., 2019; Stockley et al., 2019; Sweeney et al., 2020) have found that the use of CIMT remains at a low level in practice. A recent national stroke conference identified that evidence-based CIMT protocols have still not been implemented into routine practice by therapists working in stroke services in the UK (Jarvis et al., 2022).
Literature review
Previous systematic reviews indicate that CIMT improves arm motor function and activity outcomes in a sub-group of stroke survivors who have a minimum of 10° extension of at least two metacarpophalangeal and interphalangeal joints and of the wrist (Corbetta et al., 2015; Pollock et al., 2014; Sirtori et al., 2009). Whilst there is evidence from those reviews to support CIMT, a range of different CIMT protocols are described, representing modification of the original, intense CIMT protocol of 6 hours daily practice for 2 weeks with constraint of the ipsilesional arm for 90% of waking hours. These modified CIMT protocols differ from the original protocol and from each other in terms of the number of training and constraint-wearing hours (intensity), the frequency of the CIMT sessions, and the overall length of the protocol (duration). A systematic review of CIMT protocols for the sub-acute phase of stroke (Jarvis, 2015) identified 11 different CIMT protocols, all demonstrating evidence of effectiveness in a sub-group of a sub-acute stroke population with some active movement in the contralesional wrist and metacarpophalangeal joints. It remains unclear which protocols should be selected by therapists, and on what basis different protocols might be preferred by therapists and stroke survivors.
There has been limited exploration of therapist perceptions about when, where, or with whom a CIMT protocol might be used. Stockley et al. (2019) found only 17% of UK therapist respondents would use CIMT to address mild arm impairment (National Institutes of Health (NIH) Stroke Scale – able to lift and hold arm up against gravity for 10 seconds; National Institute of Neurological Disorders and Stroke, 2003), and 15% to address moderate impairment (NIH Stroke Scale – some ability to move against gravity). Christie et al. (2019) explored the implementation and sustainability of CIMT programmes through interviews with 11 therapists from six countries who had used CIMT programmes in their practice. Findings indicated the importance of therapist knowledge and confidence to implement CIMT, support of organisational leaders and the need to be able to tailor programmes to promote feasibility and sustainability. Further studies have identified insufficient staffing (Sweeney et al., 2020), and beliefs about what stroke survivors are able to tolerate (Fleet et al., 2014; Sweeney et al., 2020) also limit therapist use of CIMT in practice.
Stroke survivors’ experiences of participating in a protocolised CIMT programme have also been reported. Three studies (Christie et al., 2022b; Stark et al., 2019; Walker and Moore, 2016) interviewed 45 stroke (n = 41) and brain injury (n = 4) survivors who had completed protocols of between 2 and 4 weeks in duration with a minimum of 2 hours of active training at least three times a week, with daily additional constraint of 2 hours (Stark et al., 2019), 4 hours (Walker and Moore, 2016) and 6 hours (Christie et al., 2022b). The enablers included seeing functional improvements (Christie et al., 2022b), a commitment to the programme (Christie et al., 2022a, 2022b), social support (Christie et al., 2022b; Stark et al., 2019) and structure of the programme, with participants noting that this structure helped them fill their time (Christie et al., 2022b). Therapist support (Walker and Moore, 2016), and the inclusion of meaningful activities in the training (Walker and Moore, 2016) were important in promoting adherence to the protocol. Barriers included physical and mental fatigue (Christie et al., 2022b; Stark et al., 2019), frustration (Christie et al., 2022b; Walker and Moore, 2016) and the repetitive nature of the activities (Christie et al., 2022b).
There is a growing body of evidence to support the use of CIMT following stroke, and a range of potential enablers and barriers are evident as indicated above. Whilst CIMT protocol selection may reduce barriers, protocol preference has not been studied and CIMT remains under-utilised in practice. If CIMT is to be effectively implemented we need to better understand therapist and stroke survivor perspectives of a range of protocols and explore the impact of the interplay of these views, on acceptability and feasibility. The overall aim of this study was to gain an understanding of stroke survivor and therapist perceptions and experiences of evidence-based CIMT protocols and to explore the incongruence (non-agreement) and congruence (agreement) of these perspectives.
Method
Using an exploratory approach, the study was designed in two phases: (1) a focus group with physiotherapists and occupational therapists; and (2) individual semi-structured interviews with stroke survivors before and after engaging in a CIMT protocol.
Research perspectives
This inductive, qualitative study was underpinned by a social constructionist theoretical paradigm which accepts that beliefs and views are made (constructed) in the context of external influence and are shaped by interactions with others (Andrews, 2012) and the context in which it was developed (Creswell, 2009: 8). It was assumed that stroke survivor perceptions of CIMT were shaped by interactions with therapists, family and friends, and therapist perceptions were shaped through contact with other therapists prior to and during the focus group. The lived experiences of the stroke survivor participants after they had experienced CIMT were seen through a phenomenological lens (Willig, 2001).
Research ethics
Ethical approval was gained from the Keele University Faculty of Humanities and Social Sciences Ethics Review Panel for the focus group with therapists, and the National Research Ethics Service, NRES (13/NW/0309) for interviews with stroke survivors. All participants gave informed consent.
Setting
This study setting was an extension to a stroke early supported discharge (ESD) service in the North-West of England. In this service therapists work with stroke survivors in the sub-acute phase of stroke (2 weeks to 9 months post-stroke).
Sampling and recruitment
Focus group with therapists
Consenting qualified occupational therapists and physiotherapists from the participating NHS Hospital Trust were recruited if they were providing interventions to address arm function to stroke survivors who were 2 weeks to 9 months post-stroke. A purposive sampling strategy supported inclusion of participants across both professions with a range of experiences.
Interviews with stroke survivors
Potentially eligible stroke survivors discharged from the ESD service were identified by ESD therapists and invited to volunteer. Stroke survivors were included if they had: been diagnosed with a single first stroke of more than 2 weeks and less than 9 months duration on recruitment to study; been discharged from all occupational therapy and physiotherapy, to ensure that performance was not influenced by co-interventions; reduced arm function due to paresis as a result of stroke, that discharging therapists reported to have ‘plateaued’; at least 10° active extension in the contralesional wrist and metacarpophalangeal joints; ability to balance safely whilst wearing the restraint (assessed through clinical observation). They were excluded if they had been previously diagnosed with another neurological condition, were unable to follow one-step instructions (required to undertake CIMT) due to changes in cognition or communication, or were unable to provide valid consent to participate, assessed using four questions required for assessment of capacity (Department for Constitutional Affairs, 2007).
Procedures
Therapists and stroke survivors meeting the eligibility criteria were provided with verbal and written information about the study. Each participant provided a written consent.
Focus group with therapists
Consenting therapists participated in one focus group lasting no more than 90 minutes, in a Hospital Trust Education Centre. The focus group was facilitated by a researcher (qualified OT) with previous experience in facilitating groups (KJ) and attended by a co-facilitator who observed the group processes, took field notes and identified any additional areas for discussion. The focus group was audio-recorded and subsequently transcribed verbatim.
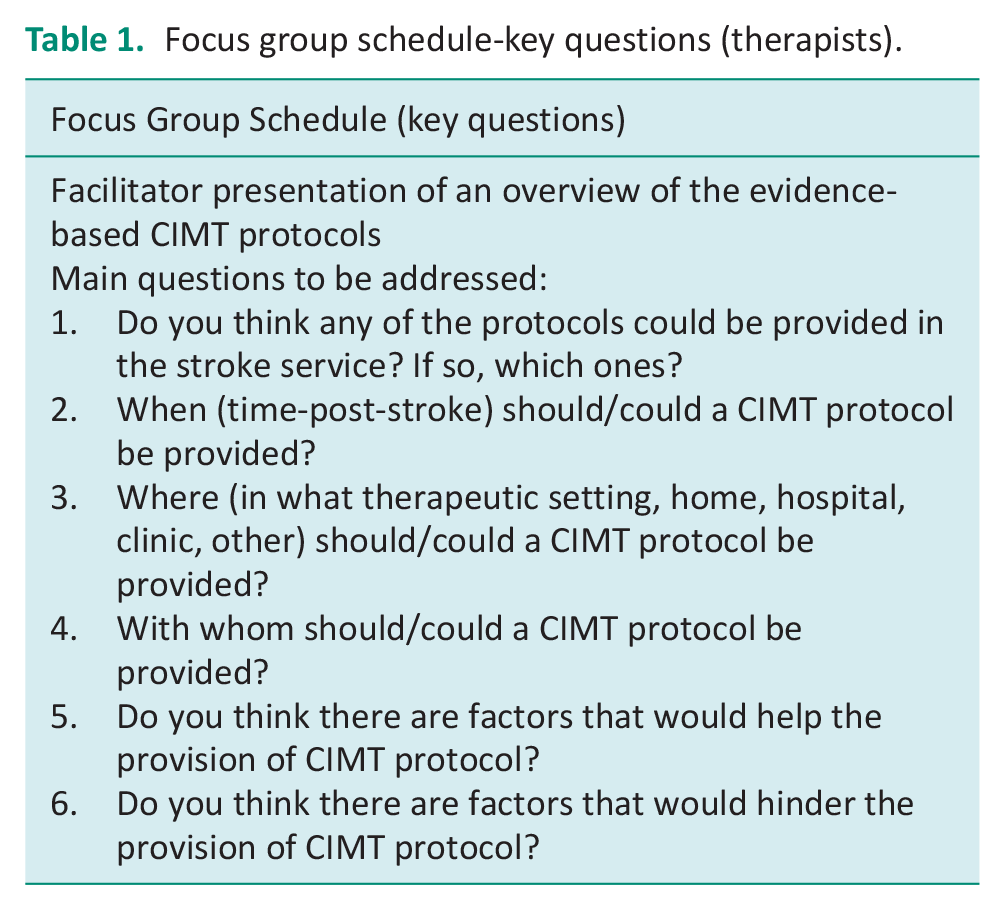
During the focus group, participants were invited to consider and discuss their own needs and those of the organisation in implementing CIMT. The facilitator presented the range of CIMT protocols (Supplemental Appendix 1), which had been identified from a systematic review (Jarvis, 2015). Participants were invited to consider each protocol and respond to questions developed from the study objectives (Table 1).
Focus group schedule-key questions (therapists).
Interviews with stroke survivors
Demographics and stroke history were recorded from the medical notes of consenting stroke survivor participants. Validated measures of anxiety and depression, the Hospital Anxiety and Depression Score (Zigmond and Snaith, 1983), and cognition, the Montreal Cognitive Assessment (Nasreddine et al., 2005) were also completed prior to interview. This information was used to describe the sample and gain a deeper understanding of response to CIMT. Participants were interviewed, by a researcher (KJ), twice: (a) prior to and (b) following participation in an agreed CIMT protocol. The interview schedules (Table 2) were shaped by patient advisors who were formally consulted twice during the planning of the study.
Interview schedules-key questions (stroke survivor interviews).
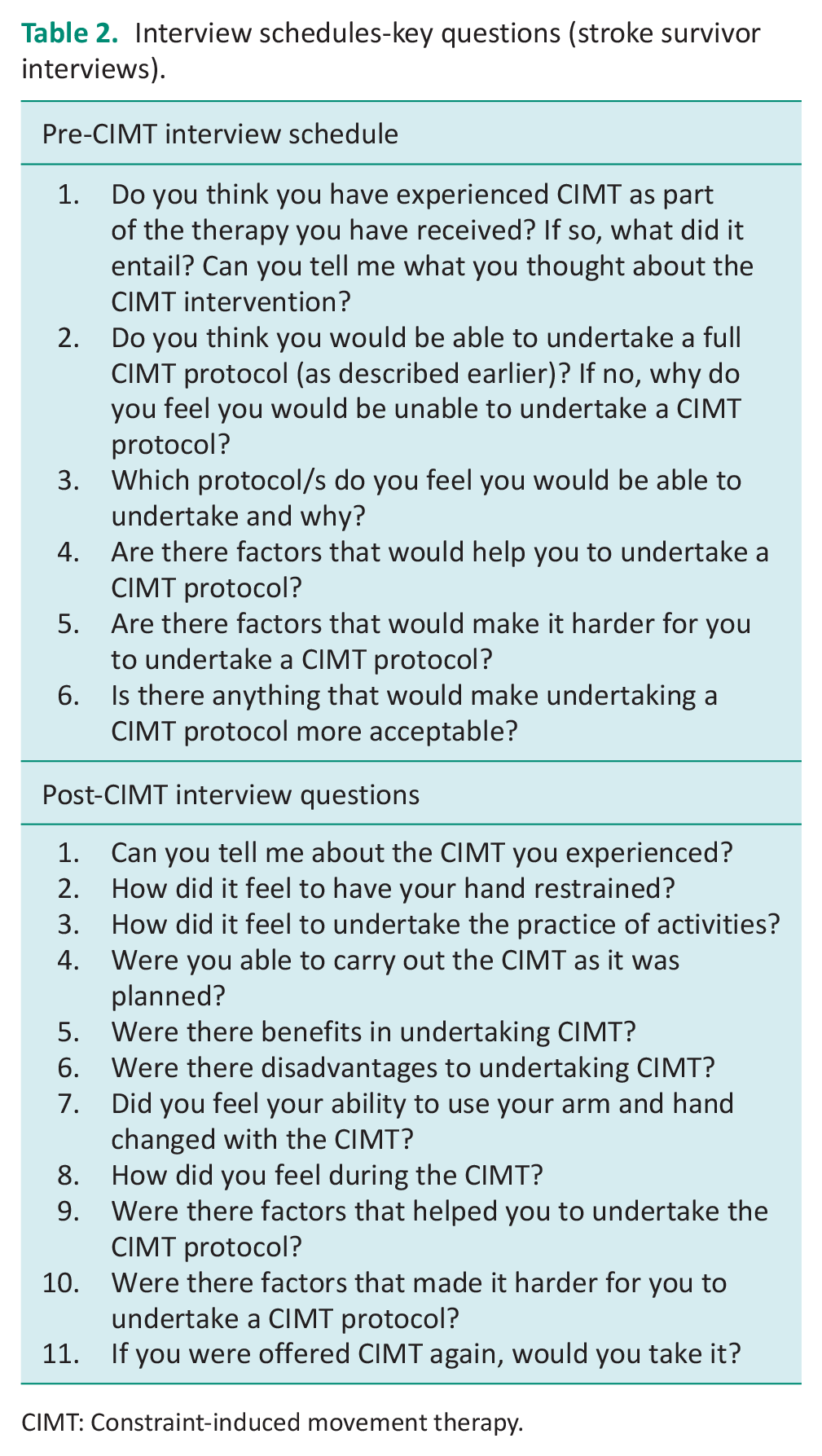
CIMT: Constraint-induced movement therapy.
In the pre-CIMT semi-structured interview (maximum 60 minutes), participants were asked to consider and discuss their perceptions of and attitudes towards CIMT. The range of potential CIMT protocols was presented in written format, supported by a verbal explanation, to enable participants to consider the feasibility and acceptability of each.
Following participation in an individually selected, pre-agreed CIMT protocol, participants were interviewed for a second time (maximum duration 60 minutes), and invited to discuss their experience of CIMT and to describe any barriers and enablers to undertaking the CIMT protocol. This interview was undertaken the day after the CIMT was completed.
Both interviews were audio-recorded and transcribed verbatim unless speech difficulties indicated it more appropriate for the interviewer to document the interview using written notes.
The CIMT protocol
Following the pre-CIMT interview, members of the research team (therapist, lead researcher) met with the participant to discuss and select a CIMT protocol, according to their preference, from a range of protocols published in the literature for which some evidence of effectiveness had been established (Supplemental Appendix 1). The most intensive protocol comprised constraints for 90% of waking hours and practice activities for 6 hours per day, for 10 days over 2 weeks. The least intensive protocol comprised constraint for 5 hours each day, and practice activities in therapy for 1 hour per day for 3 days each week for 10 weeks. Each participant selected their preferred protocol. Training included an approximately equal amount of functional and task-based activities. Each activity was selected by the treating therapist to provide a meaningful challenge to each participant. During the training, feedback was provided by the therapist to ‘shape’ the participant’s response. The activities undertaken were documented using the Occupational Therapy Stroke Arm and Hand Treatment Record (OT-STAR; Jarvis et al., 2014). The ipsilesional arm was constrained with a C-MIT® (Odstock Medical Limited).
Data analysis
The focus group and interview transcripts were analysed separately using Thematic Analysis described by Braun and Clarke (2006). Two members of the research team (KJ and SH) familiarised themselves with the text, developing a feel for the data and the broad concepts encompassed within. Next, they worked through the text line by line and, supported by NVivo 10 (QSR International, 2015) (KJ) and a paper-based system (SH), used open coding to extract data and capture meaning. Strings of text were allocated an initial label or code, which was then analysed for shared reference points. Where there was a perceived sharing of meaning, these codes were clustered to develop themes. The researchers (KJ and SH) worked independently and met to compare, discuss and agree with the initial codes and, subsequently, themes and final interpretation. The pre- and post-CIMT interviews and the focus group were analysed separately.
The relationship between the staff focus group and the pre- and post-CIMT stroke survivor interviews was explored using the principles of meta-ethnography (Atkins et al., 2008). This approach was selected as there was no expectation that the data sets would validate each other disincentivising the use of triangulation. Instead, the aim was to draw together the two data sets to reveal deeper insights. This approach has previously been used successfully in health care to explore qualitative data collected using a variety of study designs (Sattar et al., 2021). The meta-ethnographic synthesis was undertaken by one researcher (KJ) and supported by regular discussions with a second researcher (SH) to ensure a reflexive and rigorous process. The analysis followed established guidance (Noblit and Hare, 1988; Sattar et al., 2021) incorporating ‘translations’ to compare concepts in one data set with the other data set. First, a reciprocal translation was undertaken. Concepts contained within the themes were compared for aspects that were incorporated in both data sets. This was followed by a refutational translation which sought to identify dissimilar or contrasting concepts in the data sets. Finally, a ‘lines of argument’ synthesis was undertaken, bringing together the reciprocal and refutational translation to provide new insights into therapist and stroke survivor perceptions and experiences of evidence-based CIMT protocols. These translations and the lines of argument synthesis resulted in over-arching themes and sub-themes with exemplar quotations. All participants were allocated pseudonyms and these are used in the reporting of the findings to preserve anonymity.
Reflexivity
The lead researcher (KJ) kept a reflective journal throughout the analysis phase, supported by field notes taken during data collection. As an OT experienced in stroke rehabilitation, she recognised that her presence and her role in facilitating the focus group and interviews potentially influenced the data collected. Therefore, as part of the reflexive process, decisions made during data analysis were documented clearly, producing an audit trail. Field notes were made during the focus group discussion by the co-facilitator, and the facilitator reflected post-interview. The reflections made during this process were taken into account in data reporting.
Results
Focus group
Eight therapists (three occupational therapists, five physiotherapists) took part in the focus group. The therapists had a breadth of experience characterised by their time working in stroke rehabilitation (ranging from less than 3 to 20 years) and level of seniority as indicated by Agenda for Change bands (Table 3; The NHS Staff Council, 2013). All eight therapists were aware of CIMT as an intervention post-stroke; four reported encouraging some stroke survivors to use a constraint such as an oven glove or pocket to prevent the use of the ipsilesional hand whilst undertaking tasks. However, none had followed an evidenced-based CIMT protocol. The analysis of the focus group led to six themes: The CIMT Intervention; Personal Characteristics; Setting and Support; Ethical considerations; Education and Training; and Practicalities.
Summary of therapist characteristics.
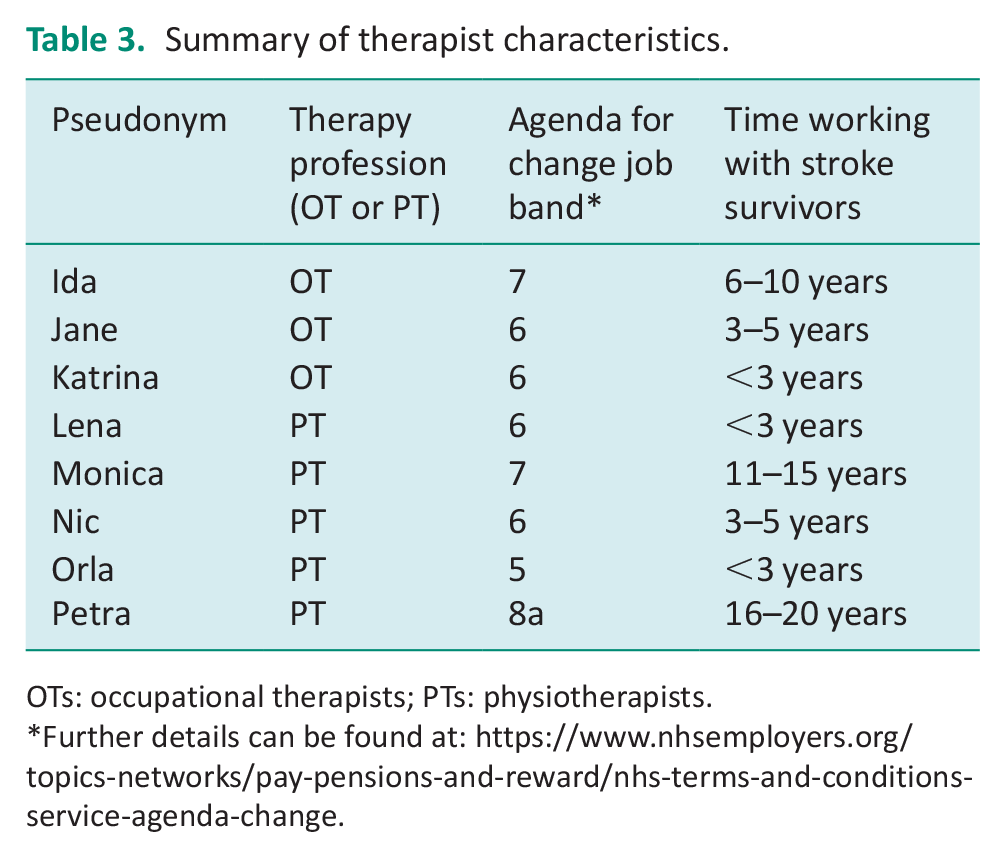
OTs: occupational therapists; PTs: physiotherapists.
Further details can be found at: https://www.nhsemployers.org/topics-networks/pay-pensions-and-reward/nhs-terms-and-conditions-service-agenda-change.
Individual interviews
Four-stroke survivors from the ESD service participated in individual interviews. A summary of these participants is provided in Table 4. The data analysis from the interviews led to four main themes: Undertaking the CIMT; Impact of CIMT; What was important; and Barriers and Facilitators.
Summary of stroke survivor characteristics.
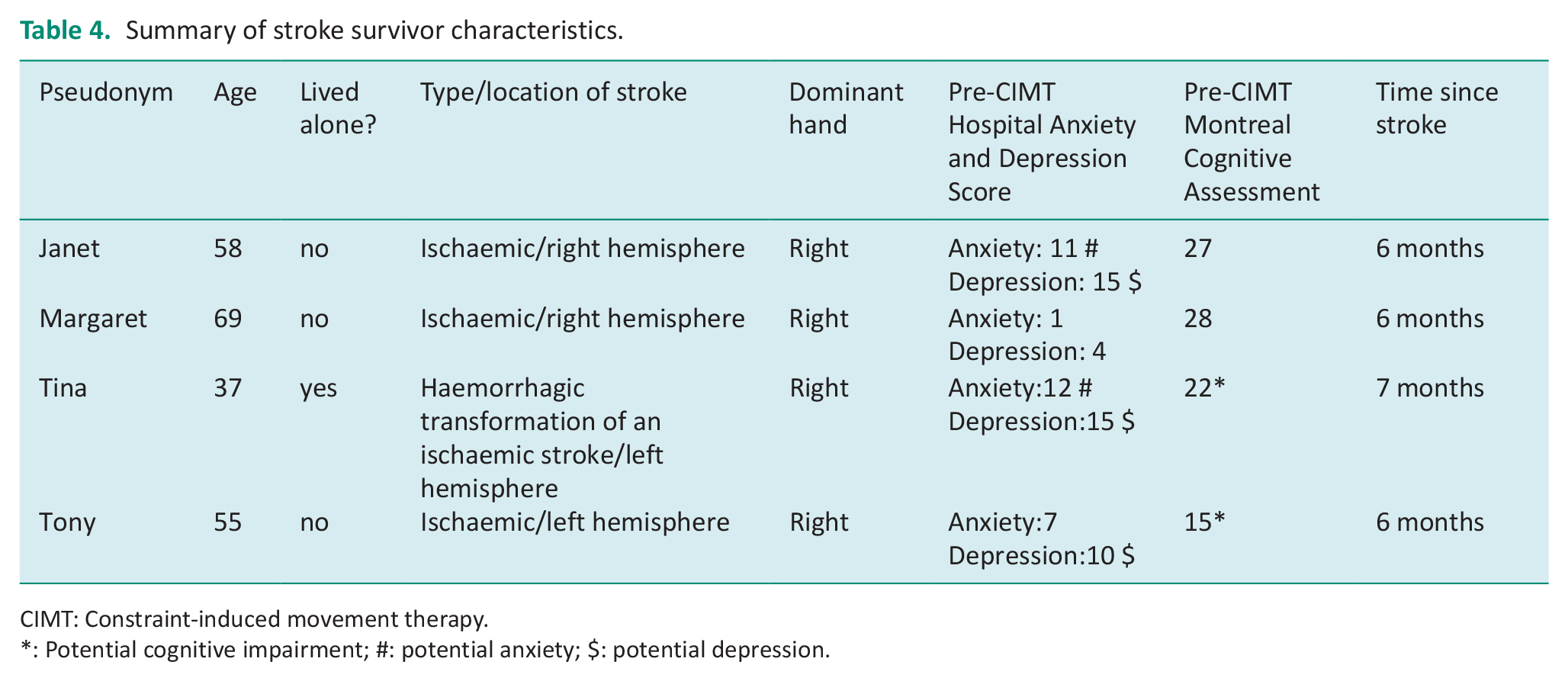
CIMT: Constraint-induced movement therapy.
: Potential cognitive impairment; #: potential anxiety; $: potential depression.
The meta-ethnographic synthesis enabled further analysis of the focus group and interview data and led to the development of four over-arching themes: Motivation and Determination to Participate in CIMT; Who Benefits; Which Protocol? and Making CIMT Feasible. The final over-arching theme contained five sub-themes: fatigue and sleep; pain; transport; need for support; training, support and mentorship for therapists.
Theme: Motivation and determination to participate in CIMT
There was agreement amongst the therapists that motivation was an essential characteristic in undertaking a CIMT protocol:
[service users are] keen to get on and motivated, but as soon as we go, they don’t pick up their home exercise programme, they do very little in between our sessions . . . to get them to follow one of these protocols for four or five hours every single day is a big ask to get them motivated and involved with it. (Monica, focus group)
This was supported by evidence that motivation and determination were enablers to undertaking CIMT, for the stroke survivors who participated in this study. Janet, Margaret and Tony described points during the process where they called upon these personal attributes:
As I say, steam was coming out of my ears a couple of times . . . But I won’t give up. Somebody once said of me, you’re like a tenacious little terrier (Margaret, post-CIMT).
Tina’s motivation was less clear, although she too expressed a level of determination in the post-CIMT interviewer notes:
[I] got on with it because it’s the correct thing to do – want my arm working but felt like hard work (Tina, post-CIMT).
The motivation and determination that the therapists perceived to be important was supported by the stroke survivors who further demonstrated their motivation by completing the protocol and indicating that they would take up the offer of further CIMT if it was offered.
Theme: Who benefits
The therapists indicated that they would only offer CIMT to stroke survivors with some activity in their contralesional hand and seemed to agree that CIMT would be appropriate for only a small proportion of stroke survivors. They indicated that deciding when to use CIMT intervention would be based on the potential benefit for a given person, rather than specifically the time-post-stroke. However, there were suggestions that it might be best utilised in the early stages post-stroke:
It might be best to start as early as possible in terms of compliance and in terms of becoming habitual in their daily routine to build it in (Nic, focus group) The walking wounded that we get in. . . straight from the acute setting to ESD, they’re the type of people who could be using it (Jane, focus group).
The therapists questioned whether a stroke survivor with cognitive impairment or low mood would be able to undertake CIMT.
If you are repeating a task and they’re not really seeing it as meaningful . . . they’ll lose concentration very quickly (Nic, focus group) Our patients are often low in mood and motivation, so getting them to do stuff for that amount of time without a supervising body would be difficult (Ida, focus group)
There appeared to be a mismatch between the therapist’s views and stroke survivor’s experiences. All participants in this study were able to participate in the CIMT and two participants (Tina and Tony) were assessed as having a potential cognitive impairment (Montreal Cognitive Assessment – Table 4) and three (Janet, Tina and Tony) were assessed as having a potential depression (Hospital Anxiety and Depression Score-Table 4). The participants all reported benefits from the CIMT programme, and recognised improved use of their arm:
I am trying to use it [arm] more than I was before (Margaret, post-CMT) I even put the scones in the oven yesterday, which I hadn’t done before because I didn’t have the strength in my wrist to hold the thing. (Janet, post-CIMT) I think when I’m in company. . ., I’m having conversation, I move my hands a little bit more (Tony, post-CIMT).
The four participants appeared to benefit from the CIMT, regardless of whether the stroke survivors met with the therapist’s view of who may benefit.
Theme: Which protocol
All stroke survivor participants selected a protocol that they felt able to undertake, and all four participants independently chose a 2-week protocol ‘to get it over with’ (Margaret). Three participants selected to undertake 3 hours of training per day, and one participant (Margaret) selected 4 hours. The protocol selected by Margaret included constraints-wearing for 90% of waking hours. However, Margaret reported that she did not adhere to this constraint protocol; instead, she wore the constraint for a similar time to the other three participants (approximately 3–4 hours in addition to the training time).
This did not align with the therapist’s views. The therapists felt that the protocols with a smaller training time each week were more feasible. Their preference was for protocols with not more than 4 hours training each week. The feasibility of the CIMT protocol appeared to be based on the time the therapists had available to offer to the training sessions:
The six hours [training] would go over a morning and into an afternoon, taking up most of your day. We’re here seven and a half hours, some of us more, but six hours is a big chunk of your day to sustain over two weeks. (Ida, focus group)
A protocol with 4 hours of arm training per week was discussed at length in the focus group as it was representative of the amount of therapy currently offered by the stroke services:
Most of our patients will get four hours a week if they need that four hours. So they’re do-able (Ida, focus group)
Whilst the therapists could see how they could fit 4 hours per week of training into their current workload, they also agreed that it might be possible to offer slightly more intensive training over a short period:
Two hours [daily training] potentially could be [possible] for like a short-ish period of time, like two weeks, and it might be something that you could have similar level patients doing activities, two supervised by one assistant, and you can keep an eye on both at the same time. (Nic, focus group)
The amount of constraint, additional to that incorporated within the training time, was also discussed. Two therapists felt that constraint of the arm for 90% of the waking hours was not feasible:
But then with 90% of their time restrained per day . . . it just seems a tad unrealistic. (Ida, focus group) That won’t happen in any of our areas. (Petra, focus group)
Stroke survivors reported that they successfully completed between 3 and 4 hours of additional constraint, and this appeared to align with the therapists’ perceptions who felt 4 hours were feasible if this was planned:
The four [hours constraint], you can almost do breakfast, lunch, evening meal, bedtime . . . because at least you can say you’re restrained this amount, you can be free in the afternoon. (Ida, focus group)
Overall, there was therapist and stroke survivor agreement about the amount of additional constraint that was acceptable and feasible. However, this was not the case for the amount of supervised arm training per week.
Theme: Making CIMT feasible
Stroke survivor participants were given choice about where the training element of the CIMT should take place. Three of the participants, Janet, Margaret and Tony, indicated that their homes were not suitable for undertaking therapy and, therefore, attended the rehabilitation unit for their therapy, whilst Tina undertook some training at the rehabilitation unit and some at home. In planning for CIMT, there were indications that each participant needed to make adjustments to fit the protocol into their lives; this included changes to their own occupations (Margaret and Tina), medical appointments (Tony), and carer routines (Margaret and Tina).
Sub-theme: Fatigue and sleep
During the pre-intervention interviews, both Janet and Tina indicated that they had a disrupted sleep pattern, often sleeping during the day.
I can stay up until three or four o’clock in the morning, I can stay up all night and not go to bed because I’m awake, but then other times, like, I’ll fall asleep on the couch. (Janet, pre-CIMT)
The protocol did take effort and caused fatigue, but Janet reported positive effects, resulting in a higher level of activity:
I’m sleeping better, I feel livelier, you know, because I’m not just going home, sitting down and going to sleep, I’m doing things, playing in the garden with the ball with the dogs (Janet, post-CIMT)
Tina accommodated the fatigue with extra sleep and Margaret and Tony managed to continue usual activities on most days, indicating a relatively small impact of fatigue on their occupations. This implied that CIMT did lead to fatigue, but that this may have positive outcomes for some, whilst for others it may require careful management.
Sub-theme: Pain
In the pre-CIMT interviews, Janet and Tina articulated concerns that the CIMT would cause pain. At post-CIMT interviews, it was reported that CIMT did have the potential to increase pain due to the increased levels of functional activity such as baking:
That was the first day we made scones and I said, ‘oh, I can’t do it, it’s absolutely killing me!’ (Janet, post-CIMT)
However, where this had occurred, the pain was assessed as being due to the result of increased activity of the muscles in the contralesional arm. In each case, the pain was monitored and managed with analgesics and by adapting the activities involved in training. Pain may be a feature of CIMT, and where it occurs it needs effective review and action where this is required.
Sub-theme: Transport
All four-stroke survivors used the study transport service and indicated that, without it, getting to the rehabilitation unit would have been difficult or costly and may have been a barrier to CIMT.
By the end of the post-CIMT follow-up, Tony was considering working towards re-gaining his driving licence, and Janet was starting to use public transport, which she attributed to an increase in confidence:
I’m trying more stuff because I feel more confident this week (Janet, post-CIMT)
However, transport remained a potential barrier throughout the CIMT protocol for all four-stroke survivors.
Sub-theme: Need for support
Therapist participants agreed that the majority of CIMT would take place once the stroke survivor was in a community dwelling. There was also agreement that formal carers working in the community would not be able to support CIMT due to a shortage of time, but that informal carers may also be able to offer support:
I think we’d have more chance of getting family carers on board to help their stroke-affected relative than formal carers. Could it be something we could link in with [informal] carers? For example, like the OTs with washing and dressing in the morning, to show how it could still be done in a timeframe, you know. (Nic, focus group)
Therapists indicated this might be particularly important if a stroke survivor had cognitive impairment:
If somebody had . . . cognitive impairments, then it might be okay if we had someone there to prompt them, like a carer (Katrina, focus group)
Whilst therapists identified the importance of carers in supporting the CIMT protocol, for each of the four stroke survivor participants, carer support was not required. Margaret seemed to see therapy as something she did without her spouse and did not report needing any additional support at home from her husband. Moreover, the stroke survivors reported the importance of the therapist during the CIMT intervention, with Janet indicating that it would have been difficult had she not had a good relationship with the therapist, who provided her with motivation to achieve her goals, whilst Tony acknowledged that the therapist’s support was instrumental in him achieving his goals:
She [the therapist] pushed me to where I want to go (Tony, post-CIMT).
Sub-theme: Training, support and mentorship for therapists
Therapists strongly expressed a need to be confident in the evidence base and their knowledge, and discussed the need for training, identifying a variety of training to increase their knowledge and confidence in using CIMT. This included having someone senior to whom they could go for advice and from whom they could learn:
Probably a formal training session and then a double up with a senior therapist (Orla, focus group) Someone we can take any potential problems to, like a trouble-shooter. (Nic, focus group)
There was also agreement in the focus group that a short-term reduction in a therapist’s caseload might help in implementing CIMT to support therapists’ knowledge acquisition.
Discussion
This study has explored and provided a comparison of stroke survivor and therapist perceptions and experiences of CIMT in a UK setting and found both incongruence (non-agreement) and congruence (agreement) of the therapist and stroke survivor views. These have implications for the implementation of CIMT into a sub-acute stroke service.
Previous CIMT implementation studies have utilised the Theoretical Domains Framework and Behaviour Change Wheel to develop a behaviour change intervention for therapists (Christie et al., 2023) and to understand the experiences of stroke and brain injury survivors (Christie et al., 2022b). However, in our study, the findings aligned closely to the five domains (innovation, individual, inner setting, outer setting, and implementation) of the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2022).
The CFIR ‘innovation’ domain (Damschroder et al., 2022), was clearly evident in our findings that addressed the CIMT protocol. Whilst current guidelines recommend a minimum of 3 hours daily therapy for people with motor recovery goals (Intercollegiate Stroke Working Party, 2023), the therapists thought that the most feasible protocols were those that included less intensive training and focussed predominantly on two protocols: the first involved 1 hour of training, 3 days per week over 10 weeks; and the second comprised 4 hours of training on 1 day per week. Therapists indicated that they felt that the stroke survivors with whom they worked would not be able to tolerate the protocols that involved a longer duration of training or mitt-wearing. In contrast, the stroke survivors all chose a protocol, more aligned with current guideline recommendations (Intercollegiate Stroke Working Party, 2023), comprising 3 or 4 hours of training per day over 2 weeks with the constraint being worn for an additional 3–4 hours daily outside of the therapy sessions. There were indications that they perceived the short protocol duration (2 weeks) to be easier to accommodate in their lives. The 3 hours of training could be planned into a half day, giving time in the other part of the day for other activities or rest.
Although the intensity of the protocol has been regarded as a potential barrier by the therapists in this study and in the literature (Viana and Teasell, 2012), this did not appear to be the case for the four participants. Christie et al. (2022b) suggest that a clear explanation of the required intensity is important to prepare stroke survivors’ capability to participate in CIMT. In our study, the process of selecting a protocol necessitated an exploration of the intensity and is likely to have provided this explanation. Data from the interviews indicated that stroke survivors enjoyed the intensive CIMT protocol they selected, although the intensity could be challenging. In this study and others (Christie et al., 2022b), the short intensive protocol appeared to be well received, with each participant in this study completing the protocol; all participants indicated that they would undertake CIMT again if it were offered. Our study is the first to include stroke survivor protocol selection from a range of evidence-based options. A key finding was that a two-week CIMT protocol that comprised 3 or 4 hours of daily training and an additional 3–4 hours constraint was both feasible and acceptable to the stroke survivors in our study.
The characteristics of the stroke survivors undertaking the CIMT (CFIR individuals domain (Damschroder et al., 2022)) provided important insights. In our study, stroke survivor participants did not require support from a carer. It is possible that the participants reduced the need for additional support by choosing a protocol they felt able to undertake independently. Offering a range of protocols may enable participants to choose a feasible protocol and may overcome the challenges identified by Stark et al. (2019) where some non-professional CIMT coaches were unable to offer the support required by the stroke survivor.
The therapists believed that only a small number of stroke survivors accessing their services would be appropriate for CIMT. The recruitment rate for this study supports this, with 302 stroke survivors going through the ESD service during the 11 months of the study, but only four people being identified by the therapists as being appropriate for CIMT. Therapists were the gatekeepers for recruitment to the study: they made decisions about whether a stroke survivor would be appropriate for CIMT based on therapists’ assessment of potential participants’ cognition or perceived ability to undertake the intensive protocol. Therapists may have excluded stroke survivors based on this belief, yet the participants experiencing low mood and/or a potential mild cognitive impairment in this study pre-CIMT participated readily in CIMT. Steps must be taken in future studies to reduce gatekeeping to ensure equal access to all people who meet the inclusion criteria; in this way, potential participants can reclaim autonomy in decisions of beneficence (Sharkey et al., 2010).
Pain featured in the stroke survivor pre- and post-CIMT interviews, with two participants expressing concern about pain, or being unable to use the constrained ipsilesional arm. This perception may be a barrier to CIMT, deterring stroke survivors from agreeing to undertake the intervention. Fatigue has also been identified in previous studies as a possible barrier (Jarvis, 2015), yet neither fatigue nor pain prevented the participants from completing their CIMT protocol, a finding supported by other studies (Christie et al., 2022b).
Whilst therapists thought that the ‘inner setting’ (defined in CFIR as the setting in which the activity is implemented (Damschroder et al., 2022)) for the CIMT should be in the community, three of the four participants selected, in contrast, to receive all their CIMT in the rehabilitation unit. In her reflections, the Research Therapist noted the benefits of undertaking some of the training in the rehabilitation unit as this made available a wider range of equipment and activities. A collaborative approach should be adopted when planning the location of the CIMT training to encourage participation and variety of occupations.
In the ‘Outer Setting’ (defined in CFIR as the setting in which the inner setting exists (Damschroder et al., 2022)) of the CIMT, transport was provided for stroke survivors who participated in the CIMT programme; however, this would not be the case if a CIMT intervention was integrated into the current service. Stroke survivors would have to cover their own travel costs, which may be considerable if the rehabilitation unit continued to be the favoured option as the treatment location; in line with findings from previous studies, transport may become a barrier for some (Christie et al., 2022b; Nicholson et al., 2014). Evidence-based CIMT protocols could not be integrated without changes to the current ESD service. As identified by the focus group therapists, these environmental issues remained a barrier and would need to be considered if a CIMT service was to be commissioned. CIMT via telehealth (Christie et al., 2022a) may provide some solutions to overcome this barrier for some stroke survivors.
Building on previous CIMT studies, the current study provides additional evidence to address the CFIR ‘Implementation’ domain (Damschroder et al., 2022). This study indicates that therapist and stroke survivor pre-CIMT perceptions did not reflect the stroke survivors’ experience of CIMT. CIMT is an evidence-based intervention that has the capacity to improve arm recovery outcomes for stroke survivors. If this opportunity is to be realised occupational therapists need to ensure that their perceived barriers do not erroneously limit access of stroke survivors to evidence-based interventions.
This was the first study to offer stroke survivor protocol selection. With no evidence that one CIMT protocol is more effective in improving arm outcomes (Kwakkel et al., 2015), we recommend that, where possible, a choice of evidence-based protocols is offered to stroke survivors to support acceptability and feasibility of participating in the protocol. This collaborative approach provides opportunity for stroke survivors to consider the intensity of the protocol, their personal circumstances and the ‘Outer Setting’ to establish if the CIMT protocol will be feasible for them. TeleCIMT, CIMT provided remotely (Christie et al., 2022a), may also provide an alternative means to increase accessibility of the CIMT intervention. If the CIMT protocol must be defined, a protocol involving 3 hours of training and 3–4 hours of constraint was considered acceptable and found to be feasible for the stroke survivors in this study. We would therefore recommend a protocol with these features. Therapist perceptions and beliefs about CIMT protocols that do not align with those of stroke survivors need to be addressed through pre-registration and post-registration education. This education should include stroke survivors sharing their experience of undertaking CIMT.
Whilst this was a small study, the findings align and supplement previous CIMT evidence from outside the UK. Further study should aim to develop implementation strategies to increase adoption of CIMT in the UK. These studies should be larger and include quantitative measurements of the impact of the CIMT on arm function outcomes. Reducing gatekeeping in future studies will help establish who gains from this potentially beneficial intervention.
Limitations
This study has gathered meaningful insights into the experiences of the stroke survivors and therapists who participated. The experiences of the stroke survivors in this study are reflected in other studies (Christie et al., 2022b; Sweeney et al., 2020; Walker and Moore, 2016) increasing confidence in our findings; however, transferability of the findings from our study may have been enhanced with additional stroke survivor participants. The findings provide a wealth of information, with probing utilised to achieve data saturation at the level of each interview (Saunders et al., 2018). Nonetheless, it is possible that further interviews would enrich the themes.
This study did not include a specific behavioural transfer package as part of the CIMT intervention. Whilst this probably reflected current practice (Christie et al., 2019), and did not seem to detrimentally influence participation in the protocol, future work should explore the importance of this and the other components of CIMT. Understanding the contribution of each component will support the selection and implementation of CIMT protocols that are effective, and also acceptable, and feasible to therapists and stroke survivors.
Conclusion
There is evidence that although CIMT has been shown to be effective in a small sub-group of stroke survivors, it has not been widely implemented in the UK. This study explored therapist and stroke survivor perceptions and experiences of CIMT and identified a wide range of potential barriers and enablers of CIMT. These should be considered where CIMT is being commissioned or implemented. It is important that therapists do not make assumptions about stroke survivors’ capacity to undertake a CIMT protocol based on their own perceived barriers to this evidence-based intervention. In this study, giving stroke survivors an informed choice over the CIMT protocol they undertake appeared to enable participation. Three to four hours of training and 3–4 hours of additional constraint were found to be acceptable and feasible to all stroke survivor participants in this study. This information may inform the design and protocol selection in practice and future CIMT studies.
Key findings
Three to four hours of training and 3–4 hours of additional constraint over a 2-week duration were found to be acceptable and feasible to stroke survivor participants in this study.
Therapist perceptions and stroke survivor experiences of the implementation of CIMT were not congruent.
Future CIMT protocol development and implementation should incorporate the authentic involvement and engagement of both therapists and stroke survivors.
What the study has added
Therapist perceptions may prevent the successful implementation of CIMT. This study indicates the importance of understanding stroke survivors’ views of their rehabilitation interventions to ensure the potential of evidence-based interventions is appropriately harnessed.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226241261183 – Supplemental material for Implementing constraint-induced movement therapy into practice in sub-acute stroke: Experiences and perceptions of stroke survivors and therapists
Supplemental material, sj-docx-1-bjo-10.1177_03080226241261183 for Implementing constraint-induced movement therapy into practice in sub-acute stroke: Experiences and perceptions of stroke survivors and therapists by Kathryn A Jarvis, Nicola MJ Edelstyn and Susan M Hunter in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors also thank Julie Turner and Rebecca Ashton, for their support throughout the study, the stroke survivor and therapist participants who took part in the study and Gaynor Reid for her work co-facilitating the focus group.
Research ethics
Ethical approval was gained from Keele University Faculty of Humanities and Social Sciences Ethics Review Panel for the focus group with therapists, and the National Research Ethics Service, NRES (13/NW/0309) for interviews with stroke survivors.
This data for this paper were originally collected for and reported in a PhD dissertation that was awarded in 2016. Whilst the original ethical approval was given in 2013, a recent national workshop (UK Stroke Forum 2022) attended by therapists from the four nations indicated the importance of addressing the barriers to CIMT. We, therefore, present the data as a paper to address this gap in the literature and long-standing challenges to the implementation of CIMT into practice.
Consent
All participants gave written informed consent prior to taking part in the study.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in planning and progress of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vreeburg Bursary Fund and the Constance Owens Trust.
Contributorship
KJ, NE and SH conceived the study, were involved in protocol development, and gaining ethical approval. KJ was responsible for patient recruitment and running of the study. KJ and SH analysed the data. KJ wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.