
Abstract
Introduction:
Professional identity is a multifaceted conceptual term combining behaviours, knowledge, skills, values, beliefs, contextual and socio-cultural factors with personal and group identity. The historical underpinning of occupational therapy is partly attributed to the difficulties occupational therapists face articulating their unique identity and the profession being misunderstood by others. Little is known about how occupational therapists working in community physical health settings experience their professional identity.
Method:
Interpretative phenomenological analysis was used to understand how five occupational therapists interpreted and made sense of their experiences of professional identity working in community UK physical health settings. Interviews were carried out following social media recruitment and analysed using interpretative phenomenological analysis guidance.
Findings:
Participants identified that their professional identity was forged through experiences over time developing skills, confidence and their inner understanding of who they were as an occupational therapists. Maintaining a secure professional identity was attributed to building their community of practice and creating a sense of belonging.
Conclusion:
Professional identity was forged through time and experience of ‘doing’, ‘being’ and ‘becoming’ occupational therapists. Building a community of practice and creating a sense of ‘belonging’ were key components of how these occupational therapists working in community physical health roles sustained their professional identity.
Keywords
Introduction
Occupational therapy is underpinned by ‘occupation’, the activities, roles and routines that an individual needs, is expected or wants to undertake that are central to their everyday life (RCOT, 2021a). However, the historical discord with the medical model has meant that the profession has been poorly understood, described as a ‘jack of all trades’ by Drummond (2010: 283) and not valued as equal by other healthcare professionals. This is attributed to the difficulties in defining the occupational therapy role and how occupational therapists articulate their ‘unique’ skills, values and professional identity (Molineux, 2011; Turner, 2011; Turner and Knight, 2015). Whilst Turner (2011) suggested that poor identity may be due to occupational therapy being a profession in adolescence, Preston (2021), 10 years later, still held the opinion that occupational therapists needed to reaffirm their own fundamental belief in the value of occupational therapy and articulate this confidently. Although based on a critical review of 12 articles that included opinion pieces as well as research articles, Turner and Knight (2015) argued that without ownership of their unique values and beliefs, occupational therapy professional identity will be influenced by role blurring and likely to be undervalued, invisible to, or overinfluenced by other professions. Although not listed as one of the top 10 Royal College of Occupational Therapists’ research priorities (RCOT, 2021b), understanding professional identity is key in developing a strong evidence base for the profession, as occupational therapists need to understand ‘who they are’, as well as ‘what they do’ and ‘why’ to thrive (Monrouxe and Rees, 2017). The author, a United Kingdom (UK) registered occupational therapist with 20 years of NHS experience in acute and community physical health, had also struggled with their own professional identity at times during their career. The purpose of this study was, therefore, to explore how occupational therapists experience their professional identity and the implications that might have not only for the individual but for the occupational therapy profession to thrive.
Literature review
Professional identity is a term often used within the healthcare literature despite not being clearly defined or understood (Fitzgerald, 2020). Fitzgerald’s (2020) concept analysis recognised that professional identity was a conceptual term that combines: actions and behaviours (what one does); knowledge and skills (what one knows); values, beliefs and ethics (one’s personal moral standards and attitudes); context and socialisation (who one is and who one is not); as well as group and personal identity. The Academy of Medical Royal Colleges (2020) acknowledged that a diverse healthcare professional workforce has positive and negative implications for professional identity as individuals try and balance their own values and beliefs with that of their profession and their role. In western society, healthcare professionals often experience discord between how professional identity is defined, understood, formed, portrayed (often with stereotyped cultural images) and experienced in practice (Hallam, 2000; Monrouxe & Rees, 2017).
There is limited research that explores occupational therapy professional identity, with most focusing on the relationship between job satisfaction and burnout working in mental health or the emerging identity of students through practice placements (Ashby et al., 2016; Clarke et al., 2014, 2015, 2019; Derakhshanrad et al., 2021; Scanlan and Hazelton, 2019). Whitcombe’s (2013) qualitative research study exploring the relationship between problem-based learning and the professional identity of 20 occupational therapy students found that professional identity was formed through the development of professional values, beliefs and expert knowledge, whereas Boehm et al. (2015), argued that professional identity formulation was a lifelong process developed through time and experiences. Clarke et al. (2015) highlighted that, whilst the occupational therapists in her study developed an authentic sense of professional identity on their role-emerging placement, those participants who went on to work in a traditional medical role after graduating felt let down by the reality of practice where there was a lack of opportunity to be truly occupational, and client centred in their practice and led them to question the value of the occupational therapy profession and their identity in these roles. None of these studies are generalisable, but they do demonstrate discord in the formulation of professional identity and the importance of having a sense of being and belonging (Wilcock, 1999). Wilcock (1999) advocated that ‘doing’ is the participation and acquisition of skills needed for the role, ‘being’ helps the individual to reflect and discover who they are and ‘becoming’ is a process which allows the individual to move towards their ideal role, all of which are intertwined with a contextual element of ‘belonging’ (Wilcock, 1999). Hitch et al. (2014a, 2014b) have further explored and developed Wilcock’s (1999) framework, highlighting that all four components, ‘doing’, ‘being’, ‘becoming’ and ‘belonging’, are interconnected and interact with one another. Taylor (2022) agrees, adding that not only does one’s professional identity aligns with one’s occupational identity, but that this develops over time as ‘doing’, ‘being’, ‘becoming’ and ‘belonging’ are multifaceted, individual yet synergistic in nature. Therefore, professional identity is developed through ‘doing’ an occupational therapy role, and how this is perceived impacts on the individual’s sense of ‘being’ an occupational therapist and what they have to offer the profession. Professional identity is then created through belonging to the profession and building a community of practice. Any doubts or dilemmas about professional identity could be attributed to a discord between an individual’s ideal role and the reality of practice, the interconnectivity of ‘doing’, ‘being’, ‘becoming’ and ‘belonging’.
Walder et al.’s (2021) scoping review identified that occupational therapists need to have a clear ontology, access to professional support networks and a robust supervision framework to formulate their professional identity. Walder et al. (2021) reviewed 89 published research articles on occupational therapy professional identity; although the review acknowledges that these were analysed through a western lens and a third of these studies were conceptual or theoretical, and three were literature reviews and therefore not based on primary research. The review also identified that 22 of these studies focused generally on occupational therapy, and only one study, van Stormbroek and Buchanan (2016), focused on occupational therapists working specifically in community services. However, as van Stormbroek and Buchanan’s (2016) study was conducted in South Africa, this challenges its transferability to the UK. Sixteen of the reviewed studies by Walder et al. (2021) were based in the UK, and of these, only five were based on primary research by registered occupational therapists working in the UK.
Although occupational therapy focuses on the interaction between the person, the environment and their occupational participation and performance (RCOT, 2021a), services in the UK tend to commission occupational therapists to primarily focus on either the person’s physical health, mental health, or social care needs. Physical health describes conditions of the body, often an illness, injury, or health condition. Registered occupational therapists working in community physical health roles will usually see people at home following hospital discharge or to prevent an admission to hospital for their physical health. The occupational therapist is usually part of a multidisciplinary team. These occupational therapists are often employed through community health trusts, charities or independent practices.
Arguably, there is a gap in the literature that explores what is understood about the factors of working in a community physical health role and the impact working in this role has on registered occupational therapists’ professional identity which led to the research question ‘what are occupational therapists’ lived experiences of professional identity when working in physical health community roles in the UK?’
Method
Research design
To explore the lived experiences of occupational therapists’ professional identity, interpretative phenomenological analysis (IPA), a phenomenological research approach underpinned by hermeneutics, was adopted (Smith et al., 2019). IPA research is often referred to as double hermeneutic, as the ‘researcher is trying to make sense of the participant trying to make sense of what is happening to them’ (Smith et al., 2022: 3). Although IPA originates from psychology, it is now used within occupational therapy and other professions, as it allows the researcher to develop a deeper understanding of others’ experiences, facilitating reflections and changes in practice (Clarke, 2009). The experience of identity is a common theme explored in IPA research as it is a complex phenomenon which is difficult to define, but central to each individual (Smith et al., 2022). As suggested by Smith et al. (2022), the researcher used an idiographic approach to understand how each occupational therapist made sense of their unique experience of their professional identity, producing subjective but rich and detailed data, before identifying common themes and experiences across participants.
Participants
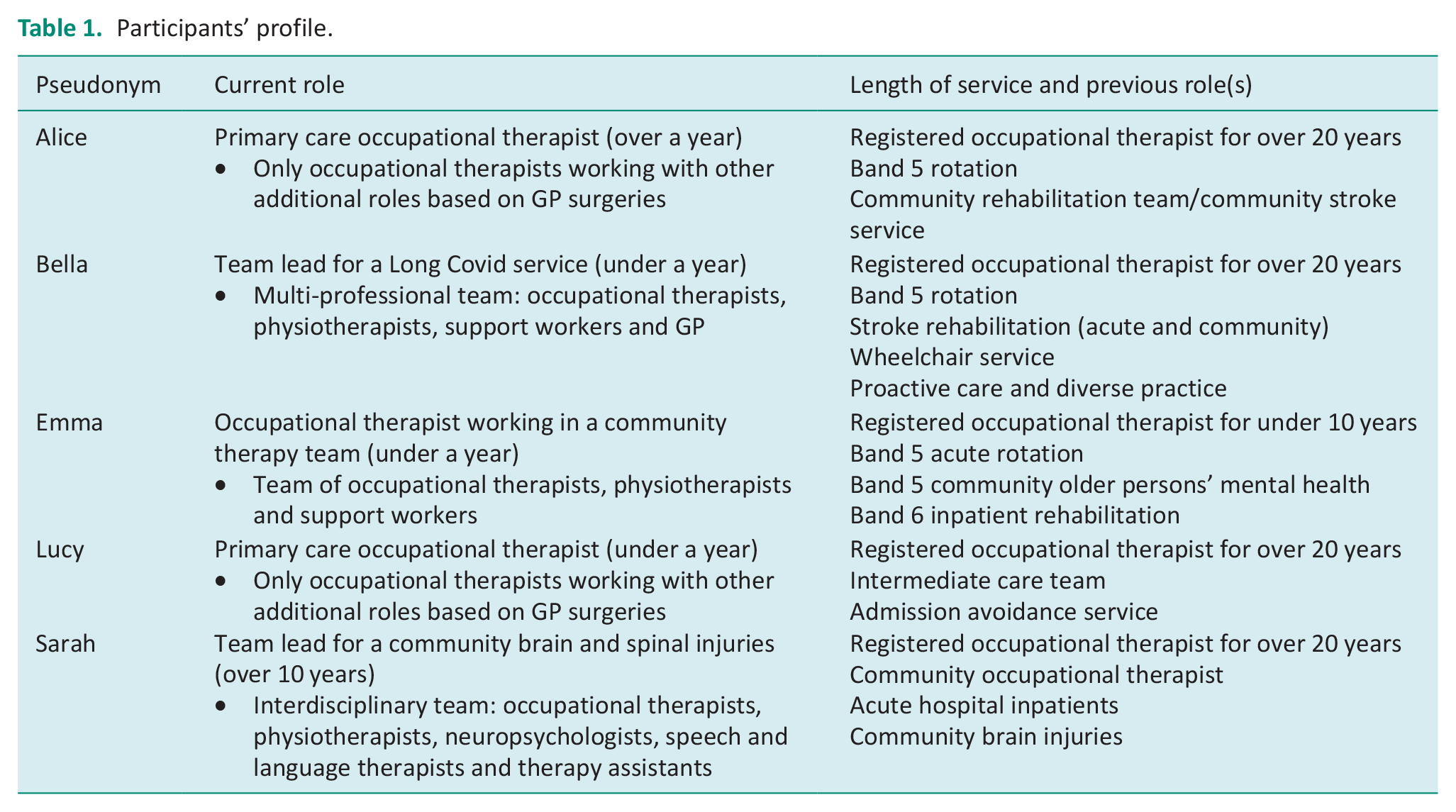
IPA studies use small sample sizes to enable a rich and deep understanding of each participant’s unique experience, thus allowing the researcher to focus on the depth rather than breadth of what is said (Pietkiewicz and Smith, 2014). Following ethical approval from the University of Brighton, five participants were recruited purposively via social media (using a recruitment poster on Twitter and Facebook). They all met the criteria of being registered occupational therapists working in the UK in a community physical health role. The exclusion criteria included those known to the researcher. All five were female occupational therapists. Signed consent forms were returned and informed consent was verbally re-confirmed at the interview. Pseudonyms have been used for all participants, and all identifiable data has been anonymised (Table 1).
Participants’ profile.
Data collection and analysis
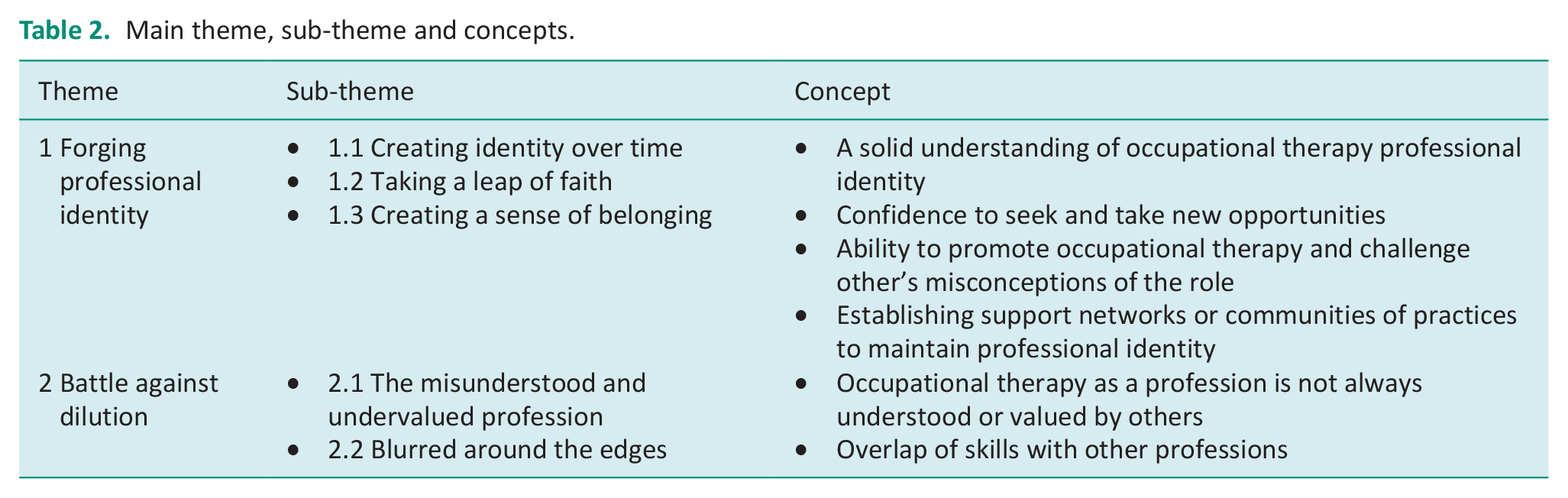
Individual in-depth interviews were conducted over MS Teams outside the participant’s and researcher’s normal working hours, at a mutually agreed time, and free from interruptions and distractions. Interviews are commonly used in IPA as they allow participants to speak freely and share their stories, producing rich and detailed accounts of their lived experiences (Smith et al., 2022). The researcher used a semi-structured interview guide that, whilst having some overarching questions, was led by the unique experiences of each participant and what was meaningful to them. This included non-leading open questions and prompts to assist participants in exploring their experiences in greater depth (Appendix 1). Participants answered all the questions, and there was no reason for the researcher to stop any interviews. Each interview lasted an average one hour and was recorded and transcribed through MS Teams. Smith et al.’s (2022) step-by-step guide to analysis was used for each participant. Once all five steps were completed for each transcript, the personal experiential themes were further analysed to develop group experiential themes (GETs; Table 2).
Main theme, sub-theme and concepts.
Rigour
The study followed the IPA process, and all stages were documented to ensure transparency and trustworthiness, as recommended by Smith et al. (2022). Before conducting the study, the primary researcher explored and acknowledged their own biases of having worked as an occupational therapist in a community physical health role in a reflexive notebook, which was used throughout the study. Reflexive journals allow qualitative researchers to continually remain reflexive and acknowledge how their own values, beliefs, biases and assumptions may impact all stages of the research process (Finlay, 2012). The primary researcher did not disclose their own experience of professional identity so as not to attribute bias to participant’s own experience, and therefore, only participants who were not known to the researcher were recruited for this study. As suggested by Nizza et al. (2021), to enhance the trustworthiness of the study, quotations are used to demonstrate that the researcher’s interpretations are grounded in participants’ individual experiences.
Findings
This paper presents the themes that emerged from the study (Table 2). The researcher acknowledges that the assigned quotes are transferable across themes, illustrating the difficulties of trying to compartmentalise individual’s experience and complex nature of professional identity and it also reflects the interconnectedness of doing, being, becoming and belonging.
Theme 1: Forging professional identity: focused on how participants felt they had built and cemented a solid understanding of what occupational therapy was and what professional identity meant to them. It highlighted that these solid foundations were built through time and experience, allowing participants to align the reality of practice with their ideal. It also identified that participants felt that their professional identities were reinforced and maintained through external support networks that created a sense of belonging by building a community of practice. It is divided into the following sub-themes:
1.1 Creating identity over time: This signified how, through time and experiences, participants had constructed a unique story of their professional identity, knowing who they were and who they were not. This was felt to be important in creating a clear, solid and strong sense of belonging as an occupational therapist.
Three participants identified that forging professional identity started from their undergraduate training. Emma talked about how having a clear professional identity was viewed as an important priority for her course and was instilled right from the start:
My Uni, they were very big on what OT is and started that right from the get-go
Conversely, Bella suggested that her training had left her with little confidence in her identity and like Lucy, it has been a battle with time and experience that allowed it to develop:
When I qualified, I was, I was awful . . . I’d so little confidence and academically I struggled . . . when I look back now . . . . all that experience I’ve gained and how much I’ve changed over the years (Bella) As a basic grade . . . I’d not had the experience, the day-to-day of trying to fight for your professional identity . . . you know 17/18 years on . . . I’m quite confident to say . . . I’m an OT (Lucy)
Participants all recognised that experience working in different roles and teams combined with the length of time they had been a registered occupational therapist was essential in developing their inner understanding of occupational therapy and construction of their professional identity, illustrated by Lucy’s phrase ‘experience under my belt’. This enabled Alice to set her professional boundaries and have clarity about what she could offer the team:
Having the experience and really understanding what OT means to me . . . I know what I feel my offer is, my core skills are. I know the extras I’m prepared to do . . . I also know what I’m not prepared to do.
Sarah depicted that her professional identity has been made secure and permanent through practising occupational therapy and increasing her confidence:
You grow in confidence the more you deliver what you see as being OT . . . the more you do it, the more you cement it
Participants all concurred that forging professional identity was influenced by their inner sense of occupational therapy as well as external and contextual factors. Emma suggested these were ‘where you work and the expectations of the service’ and Bella added how others ‘understood OT’. External factors had a strong influence on how devoted Sarah felt to her professional identity:
I think my identity feels like it stays the same, but my strength of how I feel that is seen by others or how attached to it I feel myself, can change from day to day
1.2 Taking a leap of faith: This sub-theme explored how all participants had stepped into the unknown, leaving the security of their existing roles for higher banded positions or new roles or areas of practice to try and match their ideal sense of occupational therapy to the reality of practice, carving their identity as part of their unique career journey. For Bella, managing change and having to be more visible and assertive when changing into more senior roles has not always been straightforward:
Put myself out there all the time . . . it’s really hard . . . it’s made me stronger . . . had to justify myself and think outside the box
Sarah was the only participant who articulated a clear vision of the area she wanted to practice in and actively sought out these opportunities. The development of her identity and confidence was attributed to being challenged in this role:
I think that helped me massively to figure out who I was as a therapist and who I wanted to be as a therapist . . . I mean the things I’ve done in this job; I could never have dreamed of.
Despite her initial reservations, Lucy was delighted that her confidence, self-belief and skills flourished through accepting her new role:
I’m really pleased I took that leap of faith . . . . I’m chuffed to bits what I’ve done so far.
1.3 Creating a sense of belonging: This identified that participants felt that security in their professional identity was maintained through peer support, networking and supervision, thus, building a community of practice. Reflection also provided participants with a sense of accomplishment, inclusion, respect and validation. Participants placed importance on collaboration and partnership, working to develop and belong to a shared team identity. A sense of belonging provided participants with the confidence and voice to promote the profession and challenge others’ beliefs.
Alice identified that her sense of belonging to the profession was bolstered by integral external influences. Her use of the word ‘army’ below suggests there have been a large number of people that have supported her with her identity development and together they could be perceived as some kind of force:
Army of OTs that I’ve had role modelling . . . OT learning sets . . . social media has been just fantastic . . . very much setting up or shoring up systems that support professional identity
Both Emma and Sarah described how their teams had given them permission, autonomy, confidence and the ability to speak up, and this had developed and sustained their identity and helped them promote the profession:
Expectations of the service . . . allow me to be an OT in comparison to other areas (Emma) Flexibility of the company to allow you to be able to go and develop that role rather than being dictated on (Sarah)
Bella agreed and recognised that she felt privileged that her team provided an alignment and recognition between her ideal and reality of practice:
I feel like everything’s come together, all the work I did . . . has come together into a service that actually nationally, it’s been recognised. . . that OTs are quite central . . . our team is full of OTs
All participants discussed the importance of peer supervision and their own clinical supervision to strengthen their identity. Other factors emphasised by participants included: social media, networking and conferences, professional leadership, in-service training, student practice placements and family and friends. Lucy also felt that her internal identity was enhanced through the visual identity of wearing a uniform, which helped create a sense of belonging and raise the profile of occupational therapy. The use of the phrase ‘my greens’ reflects how being an occupational therapist and having the green uniform felt part of her:
I’m back to my greens now and yeah, and it feels, it feels good to be able to promote it through uniform, through my RCOT badge . . . it gives me every opportunity to say this is what OTs do. . .
Rather than questioning their professional identity as occupational therapists, participants felt that different experiences had made them question whether the role they were doing was occupational therapy:
I don’t know whether I have questioned my identity, its more about questioning my role within the service (Alice)
Theme 2: Battle against dilution: This theme explored how all participants understood the discord between their ideal understanding of occupational therapy professional identity and the reality of what is expected or experienced in practice. It is divided into the following sub-themes:
2.1. The misunderstood and undervalued profession: this sub-theme explored the discrepancy between how occupational therapy is understood and valued by others compared to participants’ expectations.
All participants acknowledged the toughest challenge the profession faces is the ability to clearly articulate what occupational therapy is, as shown here by Emma and Bella:
I think that is one of the hardest questions in the world, can you explain what an OT does? (Emma) As OTs, we really struggle with it, because a lot of what we do is common sense (Bella)
A major concern and frustration shared by all participants was that the purpose of occupational therapy was not always perceived to be visible to the wider team and that there appeared to be a lack of value for their role; this is indicated by Lucy and Emma’s disappointment and potentially submissive attitude:
Take physiotherapy . . . it’s almost a given that people know what they do . . . I don’t even think the MDT saw me as an occupational therapist . . . in that team, I didn’t promote it (Lucy) I didn’t feel like anything that I was doing needed to be an OT (Emma)
Alice suggested that it was well known that GPs generally misunderstood the occupational therapy role, and other participants also felt resigned that this lack of understanding was a long-standing issue:
Seriously overestimated GPs understanding of the OT role (Alice). GPs ask for OT a lot which is rare from everywhere else I’ve worked (Emma)
All participants highlighted the requirement of being able to explain the role of occupational therapy through solid examples and knowing who you were speaking to and in what context. The significance of knowing your audience and ability to read the room was discussed by Alice:
You talk very differently about OT depending on your audience . . . it’s having that toolbox . . . how theoretical or non-theoretical you’re going to be . . . giving really concrete examples
2.2. Blurred around the edges: this sub-theme described how participants felt they had taken on parts of their occupational therapy identity that were not perceived as ‘pure’ but overlapped or were generic to other professionals.
All participants had the experience of working as part of an interdisciplinary or multidisciplinary team. They highlighted that there was often a challenging overlap between professional remits despite having clearly defined roles, as illustrated by Bella:
We tend to have different roles . . . but there is a lot of crossover
Although Alice articulated that she had developed a secure sense of her professional identity through her experience, her use of the phrase ‘blurred around the edges’ here suggests that it is still hard to know where her professional boundaries were, and her identity was not as clear as it could be:
I’ve been knocking around and I’ve been qualified for well over 20 years, so I have a very strong professional identity and that really helps. But what I would say is I’m blurred around the edges.
There was a consensus among all participants that if they were confident and competent in those interdisciplinary or ‘generic’ skills, and it benefited patient care, then they should use those skills. Lucy and Sarah appeared to have inner strength in their identity, being comfortable and not reliant on others knowing their title or being precious about their unique identity:
My identity was not diluted but I wasn’t known as an occupational therapist. . . there is a place for that if you wanted to have those generic skills, which I did (Lucy) We are the person’s rehab team, so it doesn’t matter what role we all have we are all there ultimately to work towards the client goals, not their therapy goals (Sarah)
Discussion
Participants all described themselves as having a strong sense of professional identity as an occupational therapist. When asked what they understood about the term professional identity, they referred to the values, beliefs, knowledge and skills of an occupational therapist and what makes occupational therapy different from other healthcare professionals, a similar understanding to Whitcombe (2013). However, as participants shared their stories, it revealed that they had a deeper understanding of professional identity that aligned with Fitzgerald’s (2020) conceptual explanation of the term. Participants showed an unconscious awareness that their personal identity and conceptual factors (internal and external) influenced and impacted their professional identity formulation. Like Fitzgerald (2020), they recognised that knowledge and skill acquisition was only one component of professional identity that is intertwined, influencing the formulation of professional identity, which builds on the findings of Whitcombe (2013). The participants’ understanding of their professional identity combines Fitzgerald’s (2020) conceptual explanation with that of Hansson et al. (2022) that their occupational therapy professional identity combines both internal and external factors of doing, being, becoming and belonging.
The length of time participants had been working as registered occupational therapists, their previous experience and the length of time they had been in their current community physical health role all varied. All participants attributed their inner security in their professional identity to their previous and current experiences. It was, therefore, over time, doing, being and becoming occupational therapists and experiencing different opportunities that they felt their professional identity had been cemented, creating a sense of belonging. This is aligned with the literature that states professional identity formulation is a lifelong process, meaning that knowledge, skills and competencies are developed over time and from different learning experiences (Boehm et al., 2015; Monrouxe and Rees, 2017; Fitzgerald, 2020). Whilst participants recognised that their experiences provided them with knowledge and skill acquisition that enhanced their confidence and self-belief, it was also responsible for them discovering who they were and wanted to be as occupational therapists. Monrouxe and Rees (2017) identified that for healthcare professionals to thrive in their chosen profession, they needed to have a clear sense of professional identity; this meant understanding ‘who they are’, as well as ‘what they do’ and ‘why’. Arguably, it is hard to distinguish whether participants felt that it was their current role as a community physical health occupational therapist that had provided them with a strong sense of their professional identity or whether it was in this role that they recognised that their inner ideal sense of identity aligned with their reality of practice. This reinforces Hitch et al.’s (2014a, 2014b) view, in their further development of Wilcock’s (1999) framework of ‘doing’, ‘being’, ‘becoming’ and ‘belonging’, that all of these components are interconnected and impact on each. As ‘occupational beings’, it is difficult to separate whether roles carried out in the past or present can be attributed to who one wants to become in the workplace (Hitch and Pepin, 2021; Taylor, 2022). Only one participant had a clear vision of the area of practice that she wanted to work in that aligned with her inner sense of professional identity, although whether this inner desire originated or was developed from personal or professional experience is unclear.
All participants identified at various points in their career, whilst doing, being and becoming occupational therapists, that they had experienced a lack of recognition as an occupational therapist. This does not appear to be necessarily unique to physical community roles, as the participants had all worked in different areas. However, the participants felt that the lack of recognition of the occupational therapy roles was due to the role being misunderstood or undervalued by others, which aligns with the literature (Turner, 2011; Drummond, 2010). Participants all felt that a lack of recognition of the occupational therapy role was a long-standing problem that was partly attributed to the difficulties in clearly articulating the occupational therapy role and its unique knowledge and skills, especially in generic multidisciplinary working, which the literature also indicated (Molineux, 2011; Turner, 2011; Turner and Knight, 2015). If, as Walder et al. (2021) stated, occupational therapy had clear ontology, this would arguably be resolved. However, it was through time and experience of doing and increased sense of their professional being that participants felt their inner confidence had developed and provided the knowledge and understanding to recognise their ideal role, thus creating a sense of belonging and enabled the setting of professional boundaries. This illustrates that participants’ professional identity was developing from ‘being’ an occupational therapist to ‘becoming’ the occupational therapist they wanted to be (Wilcock, 1999). It also appeared that participants felt they were able to know their audience, ‘read the room’ and challenge others’ perceptions by developing this inner confidence that time and experience had provided. It also seemed that this inner confidence and understanding of the profession provided the desire for participants to find and take the opportunities to develop themselves through new roles or areas of practice that aligned with their ideal, becoming the occupational therapist they want to be. This could lead to retention and recruitment in some areas of practice or create new occupational therapy positions in others (Clarke et al., 2015).
Although participants all felt that they had a strong sense of occupational therapy professional identity, they also felt the boundaries with other professions overlapped in community physical health roles. Turner and Knight (2015) argue that occupational therapists’ professional identity will be influenced by role blurring and is likely to make the profession feel undervalued or overinfluenced by other professions if occupational therapists do not have ownership of their unique values and beliefs. However, whilst the Academy of Medical Royal Colleges (2020) highlighted the importance of having clearly defined roles and responsibilities to formulate a professional identity, they acknowledged that professionals have multi-layered identities, especially when working as part of a team, which can enhance job satisfaction, professional relationship and patient care. Two participants in this research study appeared comfortable and not precious about their unique identity, which could be attributed to how time and experience had made them feel secure in their identity and that they had achieved a sense of belonging as part of the team and profession.
Whilst experience and time, doing and being, were key components attributed to becoming an occupational therapist, it was a sense of belonging to both the profession and team that appeared to allow participants to shore up their occupational therapy professional identity. This extends Wilcock’s (1999) occupational perspective of health concept a step further recognising that what you ‘do’, who you ‘are’, what you want to ‘become’ and how you feel you ‘belong’ are all interconnected and interdependent (Hitch et al., 2014a, 2014b). The framework of doing, being, becoming and becoming has illustrated the complex nature of forging occupational therapy professional identity. Arguably, it is the interconnected and interdependent experience of doing, being and becoming that starts professional identity development and the sense of belonging that maintains it. In this study, the participants highlighted that belonging to a community of practice providing partnership working, role modelling, peer supervision, in-service training, student education, networking, social media and conferences all helped to maintain a secure sense of their professional identity.
Limitations of the study
The researchers recognised that IPA is a subjective approach which explored how participants interpreted their lived experience of professional identity but not why that experience occurred. They also acknowledge that different researchers, using different lenses, could also interpret the same data differently (Tuffour, 2017). Although the study did not aim to be representative of the UK occupational therapy profession, all five of the participants were female. The author, therefore, recognises that therapists from outside the UK, other genders and work contexts may have a different experience, especially where their undergraduate training may be delivered very differently, and subsequent work roles, settings and respect for the occupational therapy role may be different. The findings were also influenced by the context of participant’s current role, the range of experience they had and the length of time they had been working. Recruiting through social media meant it was likely that only participants who have access to and used social media could have chosen to participate in this study. It is also likely that only participants who had an interest in the topic area or perceived themselves as having a strong sense of professional identity would have chosen to participate, rather than those struggling with their professional identity, although this would have added a different perspective.
Conclusion and recommendations
This paper suggests that time, experience, doing, being, becoming and sense of belonging to the profession and role are what formulated and cemented participants’ secure sense of professional identity in a community physical health role. It recognises that professional identity is unique to the individual as it is formed not only from knowledge and skill acquisition but through the interaction of an individual’s personal identity, their lived experience of different roles and socio-cultural factors. Therefore, occupational therapy students and newly registered occupational therapists require a range of opportunities to be able to forge their professional identity through ‘doing’ and ‘being’ and ‘becoming’, to create their sense of ‘belonging’ to the occupational therapy profession. If an individual does not have a wide range of experience, this could impact their sense of professional identity in a community physical health role. Types of practice placement are particularly important as role-emerging placements have been shown to enable students to develop a strong sense of their professional identity (Clarke et al., 2015). All occupational therapists need to have a clear understanding of the role of occupational therapy and the ability to articulate this in practice; otherwise, they are at risk of being overinfluenced and undervalued by others. To enhance the profile of the profession the Royal College of Occupational Therapists (2022) is engaging with higher education and with its members through social media to promote the value and diversity of the profession to others. However, there needs to be an awareness and recognition for students, higher education institutes and employers of the discord that currently and historically exists in some areas of clinical practice that may impact how occupational therapists align their ideal understanding of the profession with that of the reality of practice.
Practice educators and supervisors also need to have education and training on how to support and develop the professional identity of others. This includes the awareness that different experiences are all valuable in the construction of professional identity, and the creation of communities of practice will allow professional identity to be shored up. The study identified that peer supervision, role modelling, mentorship, reflective practice, problem-based learning, in-service training, networking and social media are all tools that can form the basis of a community of practice. This paper recommends the inclusion of these tools as key components of academia, practice placements and preceptorship within a structure for ongoing career development to ensure that professional identity formulation, development and maintenance are supported to allow each occupational therapist, role and team and ultimately the profession to thrive.
Further research is needed into occupational therapists’ lived experiences of their professional identity to have a richer understanding of how professional identity is understood, forged and experienced by occupational therapists in practice. To provide recommendations to support the development and maintenance of professional identity for others, a longitudinal study focusing on different stages of an occupational therapist’s career journey (e.g. commencing the course, during the course, when newly qualified and after five years), to explore how participants attribute meaning to their experiences and what factors supported or influenced their professional identity is needed.
Key findings
Articulating a clear definition of occupational therapy continues to be a difficulty for occupational therapists which appears to contribute to the long-standing misunderstanding of the role.
The framework of doing, being, becoming and belonging can be used to explore how professional identity is forged and maintained.
Professional identity seems to be formulated through experience and over time which allows occupational therapists to build their knowledge and skills, discover who they want to be as an occupational therapist and create a sense of belonging.
Building a community of practice appears to be a key component of occupational therapists shoring up and sustaining their professional identity.
What the has study added
Professional identity can be explored through the framework of doing, being, becoming and belonging. This adds to the current literature on the lived experience of community physical health occupational therapists in the UK, forging and sustaining their professional identity in practice.
Footnotes
Appendix 1 Interview questions
As IPA is about exploring in-depth participants’ lived experiences of their professional identity, these are some of the questions used in my research.
Acknowledgements
The authors thank participants who took part in this study for sharing their experiences.
Research ethics
Ethical approval 2022-9456 was obtained from the University of Brighton, School of Sport & Health Science Research Ethics and Integrity Committee.
Consent
Not applicable.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship and/or publication of this article.
Contributorship
This research was undertaken as part of MSc Advanced Occupational Therapy dissertation. Emily Rosalyn French researched literature, applied for ethical approval, recruited participants, completed data collection and analysis, and wrote up the results. Channine Clarke supervised the research throughout. Both authors then reviewed and edited the manuscript and approved the final version.