
Abstract
Introduction:
Myalgic encephalomyelitis/chronic fatigue syndrome affects an individual’s occupational participation. There is little understanding in Australia of occupational interventions for myalgic encephalomyelitis/chronic fatigue syndrome. This study explored how Australian adults with myalgic encephalomyelitis/chronic fatigue syndrome use their time and whether the National Institute of Health Activity Record can inform occupational interventions.
Method:
Using a convergent mixed method, nine participants completed the National Institute of Health Activity Record time diary and five survey questions exploring clinical utility and the impact of myalgic encephalomyelitis/chronic fatigue syndrome. Data analysis included descriptive statistics for time-use data and an inductive thematic analysis for survey responses.
Results/Findings:
Participants (aged 29–59 years) reported 58% of their time was spent awake and in recreation and leisure occupations. Quantitative data reflected no statistically significant change in participants’ symptoms, performance and motivation throughout the day. Six themes emerged from the qualitative data that highlighted participants’ experiences completing the National Institute of Health Activity Record and the impact of myalgic encephalomyelitis/chronic fatigue syndrome on their time-use.
Conclusion and Relevance:
The National Institute of Health Activity Record provided insights into a participant’s time-use, which could inform occupational interventions. Modifying the National Institute of Health Activity Record format would improve usability for participants and reduce time for completion. Discussing results and extending the data collection period may capture the impact and fluctuations of myalgic encephalomyelitis/chronic fatigue syndrome more accurately.
Keywords
Introduction
Myalgic Encephalomyelitis (ME) chronic fatigue syndrome (CFS) is a condition characterised by debilitating fatigue that rest cannot alleviate (Eaton-Fitch et al., 2020). Estimated to be prevalent in up to 22,050 Australians as of 2020 (Orji et al., 2022), individuals with ME/CFS can experience accompanying symptoms such as impaired cognition, muscle or joint pain and sleep disturbances that fluctuate unpredictably over months and years (Eaton-Fitch et al., 2020). People with ME/CFS experience remissions and relapses that significantly impact their physical, social-emotional and psychological well-being (Eaton-Fitch et al., 2020; Lowry and Pakenham, 2008). ME/CFS has been found to reduce a person’s quality of life by 50% (Eaton-Fitch et al., 2020; Taylor et al., 2010), and this long-standing disruption can adversely impact the person and their ability to engage in their occupations, resulting in a reduction in roles and social isolation (Bartlett et al., 2021; Hughes, 2009; Jason et al., 2012; Taylor et al., 2010).
Occupational therapists work with people with chronic health conditions to increase their participation in occupations they need, want, or are expected to do (Gray and Fossey, 2003; World Federation of Occupational Therapists, 2020). Occupations are everyday activities that enable health and well-being as they bring structure, meaning and purpose (Polatajko et al., 2013). However, too few or too many occupations can cause experiences of occupational deprivation or imbalance, diminishing a person’s health, well-being and quality of life (Bass, 2015; Kroksmark et al., 2006). Occupational deprivation is when circumstances beyond their control reduce a person’s choice and diversity of occupations, whereas occupational imbalance describes engagement that fails to meet an individual’s unique physical, social, mental or rest needs (Bass, 2015). Occupational therapists have the knowledge and skills to work with people who experience these deprivations and imbalances (Hughes, 2009).
Occupational therapists seeking to understand an individual and the impact of their illness on their occupational participation (such as occupational imbalance or deprivation) can utilise tools such as illness narratives and time diaries (Farnworth, 2003; Pemberton and Cox, 2015). Unpacking a person’s engagement in occupations, a person’s lived experience expressed through an illness narrative can allow occupational therapists to understand the subsequent impacts that their illness has on their health, well-being and quality of life (Gray and Fossey, 2003). Further, as time defines engagement in occupations and occupations give meaning to time (Pemberton and Cox, 2015), time diaries offer a way to assess and understand the complexities of a person’s occupational participation (Liedberg et al., 2009). Time diaries can provide a comprehensive profile of function, dysfunction and quality of life otherwise difficult to observe (Jason et al., 2009), as well as measure changes in occupational participation driven by intervention (Kroksmark et al., 2006; Taylor and Kielhofner, 2003). One such time diary is the National Institute of Health (NIH) Activity Record (ACTRE) (Gerber and Furst, 1992a).
The NIH ACTRE, first developed in 1987, is a valid self-administered time diary developed to measure the outcome of energy conservation programmes for individuals with chronic health conditions (Gerber and Furst, 1992a). Deemed a highly reliable tool (ICC = 0.88–1.00, α = 0.77; Quaresma et al., 2017), the NIH ACTRE assesses symptoms, performance and motivation and the impact on specific daily occupations (Gerber and Furst, 1992b). These occupations are self-care, preparation and planning, household activities, work, recreation and leisure, transportation, treatment, sleep and rest (defined as cessation of activities to restore energy; Bernhofer, 2016; Jason et al., 2009). Using concepts from the Model of Human Occupation, the NIH ACTRE details how chronic health conditions impact volition (motivation), habituation (habits), performance capacity (perception of their capacity) and how the environment influences a person’s engagement in occupations (Taylor and Kielhofner, 2017). In applying these principles, the NIH ACTRE attempts to provide clinicians with a measure of a person’s illness experiences via their time-use and can bring to light impacts on a person and areas for change. This can be implemented at various points during their long-term condition to measure progress (Gerber and Furst, 1992b; Taylor et al., 2010).
Purpose and aims
Given the impact of ME/CFS on a person’s participation, the NIH ACTRE could be utilised as a tool to understand the person’s time-use and measure change in response to occupational therapy interventions. Whilst the NIH ACTRE has been utilised with other chronic health conditions, there was no literature found relating to use with adults with ME/CFS. Therefore, the purpose of this study was to understand better the lived experience of time for adults with ME/CFS and whether the NIH ACTRE could be used to inform and measure occupational therapy intervention for this population. Thus, the two research questions were, ‘How do Australian adults with ME/CFS use their time?’ and ‘What implications does the use of the NIH ACTRE have for occupational therapy intervention?’
Methods
Design
This study used a convergent mixed methods research design to produce a descriptive study. A convergent mixed methods design is a comprehensive approach that integrates qualitative and quantitative data collection and analysis methods to provide rich information to explore a research topic and provide a nuanced understanding of the research question (Creswell and Plano-Clark, 2017).
Participants
Commencing April to June 2021, participant recruitment occurred. To recruit, an advertisement was posted on relevant Facebook support groups after permission to post was granted. When participants expressed an interest, they were invited to email the research team to confirm eligibility and receive a plain language statement to ensure an understanding of the logistics and requirements before consenting (e.g. right of withdrawal and confidentiality). Eligibility criteria for this included being an Australian resident, having a medical diagnosis of ME/CFS, being over 18 years old, and having adequate English language skills. Confirmation of participant’s diagnosis was received via the consent form, where participants self-reported that they had a medical diagnosis of ME/CFS. To ensure that comorbidities were excluded, those who expressed an interest were screened through simple questioning via email if they had any other diagnoses. If they expressed they had other diagnoses that contributed to additional fatigue (i.e. fibromyalgia and cancer), they were excluded. In total, nine adults, 7 females and two males, with a reported diagnosis of ME/CFS aged 29–59 years and varying durations of diagnosis (4–33 years), were recruited from across Australia using a non-probability convenience sample method.
Instrumentation
Two individuals with ME/CFS piloted the instruments. They suggested amendments to clarify questions and improve instructions, format and usability of the NIH ACTRE and the online Qualtrics survey. Participants who provided consent were emailed an Excel spreadsheet version of the NIH ACTRE and a link to the survey to ask about their experience of completing the time diary. Both instruments gave instructions to guide participants on how to complete the tools. Participants were asked to complete the NIH ACTRE and to upload their time diary at the end of the survey approximately within 3 weeks of receipt. They were then directed to complete the survey questions. The authors of the NIH ACTRE provided permission to use the diary, and the Australian Catholic University (ACU) Human Research Ethics Committee granted the necessary ethical approval (2020-226EAP).
National Institute of Health Activity Record (NIH ACTRE)
The NIH ACTRE collected quantitative data whilst additional cells were added to capture demographic information: participants’ names, ages, genders, post-codes, living status and duration since diagnosis. Participants were asked to complete the NIH ACTRE in the AM and PM, indicating what they did during each 30-minute time block for two 24-hour periods. It also asked them to self-report using a 4-point Likert rating for symptoms, performance and motivation. To gather information on the participant’s symptoms, ‘pain’, ‘fatigue’ and ‘activity-related fatigue’ scored from not at all (1) to a lot (4) (Gerber and Furst, 1992a). Similarly, a participant’s performance was explored via ‘difficulty with activity’ and was scored from very difficult (1) to not difficult (4) (Gerber and Furst, 1992a). Lastly, ‘how well done’, ‘meaningful’ and ‘enjoyment’ addressed participant’s motivation (Gerber and Furst, 1992a). These topics were scored from very poorly (1) to well (4), from not meaningful (1) to very meaningful (4), and from not at all (1) to a lot (4) (Gerber and Furst, 1992a).
Usability of the time diary
The online Qualtrics survey allowed participants the opportunity to provide open-text responses (Qualtrics, 2021) to comment on the time diary questions, instructions, format and usability. The survey consisted of five open-ended questions which were designed by the research team for this study to explore:
(1) How would you describe the changes in the way you spend your time since being diagnosed with ME/CFS?
(2) What was your experience with using the activity record for this research project?
(3) Can you identify any aspect of the activity record that was helpful/positive?
(4) Can you identify any aspect of the activity record that was unhelpful/negative?
(5) How well do you think the activity record reflects the impact of ME/CFS on how you spend your time?
Data collection was concurrent recruitment.
Data analysis
The quantitative data was analysed using Microsoft Excel and the Statistical Package for the Social Sciences (SPSS) Version 27 (IBM, 2021). The Shapiro–Wilk test determined that the data was non-normally distributed; therefore, frequency distributions, percentages and medians were used to review the occupational categories and their symptoms, performance and motivation (Khatun, 2021; Laerd Statistics, 2018b). A non-parametric Friedman test then determined whether symptoms, performance and motivation changed across the morning, afternoon and evening (Laerd Statistics, 2018a). Finally, Holm’s step-down procedure set a corrected significance level (ranging from 0.005 to 0.05) for each question to control Type 1 error rates due to the assessment of multiple hypotheses (Holm, 1979).
An inductive thematic approach was used to analyse the qualitative data regarding participants’ time-use and usability of the NIH ACTRE (Nowell et al., 2017). Completing the thematic analysis involved all researchers and consisted of a six-step process: familiarisation, coding, generating themes, reviewing themes and defining and naming themes (Braun and Clarke, 2019). First, researchers familiarised themselves with the data and developed initial codes independently before coming together to collaboratively agree on 46 different codes. The research team further discussed these 46 codes across a series of meetings to group similar codes into themes. In discovering repeated patterns of meaning and grouping similarities, themes were reviewed and then finalised into six themes. During this process, researchers established theme trustworthiness through prolonged data engagement, well-organised archives, documenting discussions, vetting of themes and obtaining consensus before concluding analysis (Braun and Clarke, 2019; Nowell et al., 2017).
Results
Participants
Nine participants submitted an NIH ACTRE and completed a Qualtrics survey response. Of these nine, seven were females and two were males. All participants, aged between 29 and 54, lived within a metropolitan area but varied in age and duration since receiving their diagnosis of ME/CFS (Table 1). The results are presented and discussed below using pseudonyms. Unfortunately, two participants did not provide their names when submitting the NIH ACTRE with their Qualtrics survey, and therefore, Unknown 1 and Unknown 2 are used when reporting their comments.
Demographic data.
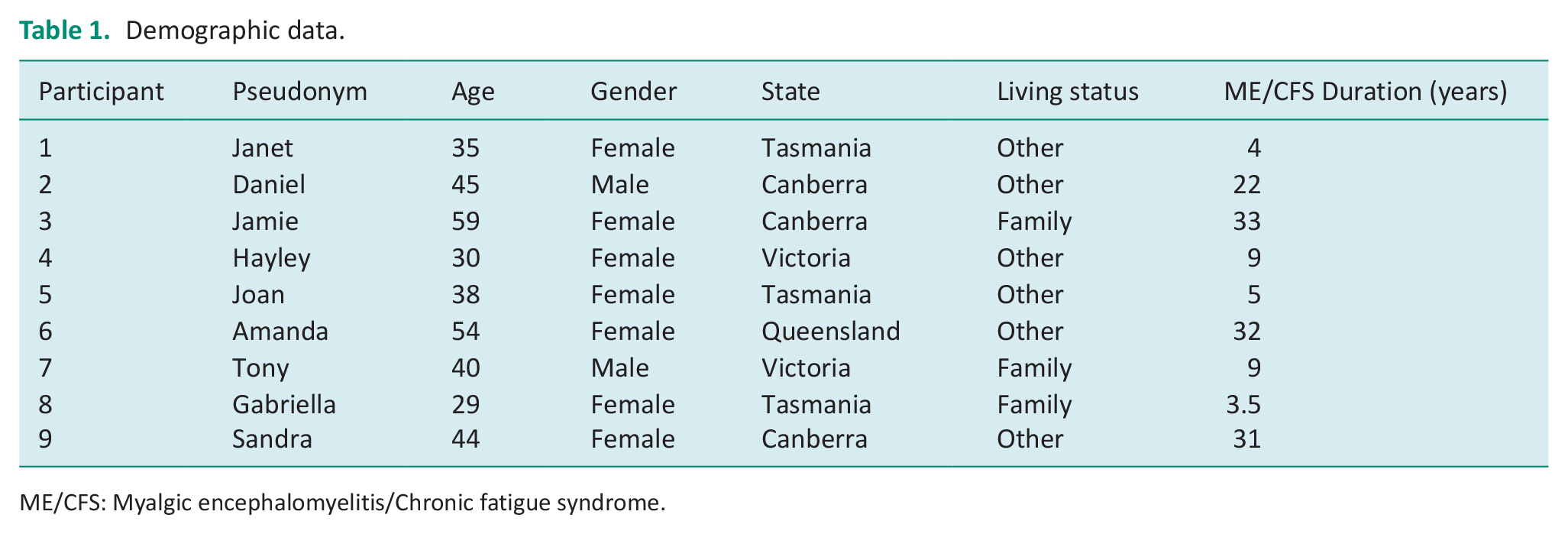
ME/CFS: Myalgic encephalomyelitis/Chronic fatigue syndrome.
Quantitative results
The statistical outcomes relevant to the NIH ACTRE data are shown below. The non-parametric tests revealed that the grouped participant data were not statistically significant across the sample’s symptoms, performance and motivation over the morning, afternoon and evening.
Symptoms
Pain
There was no significant change across the day (x2(2) = 1.62, p = 0.45) but large individual variation in pain symptoms was reported. Some participants reported having pain 100% of the time, whereas others experienced pain 0% of the time across the day (Table 2). Whilst some participants experienced more pain over a day, this did not seem to impact the time they spent resting (Figure 1).
Participant’s symptoms and performance across the day.
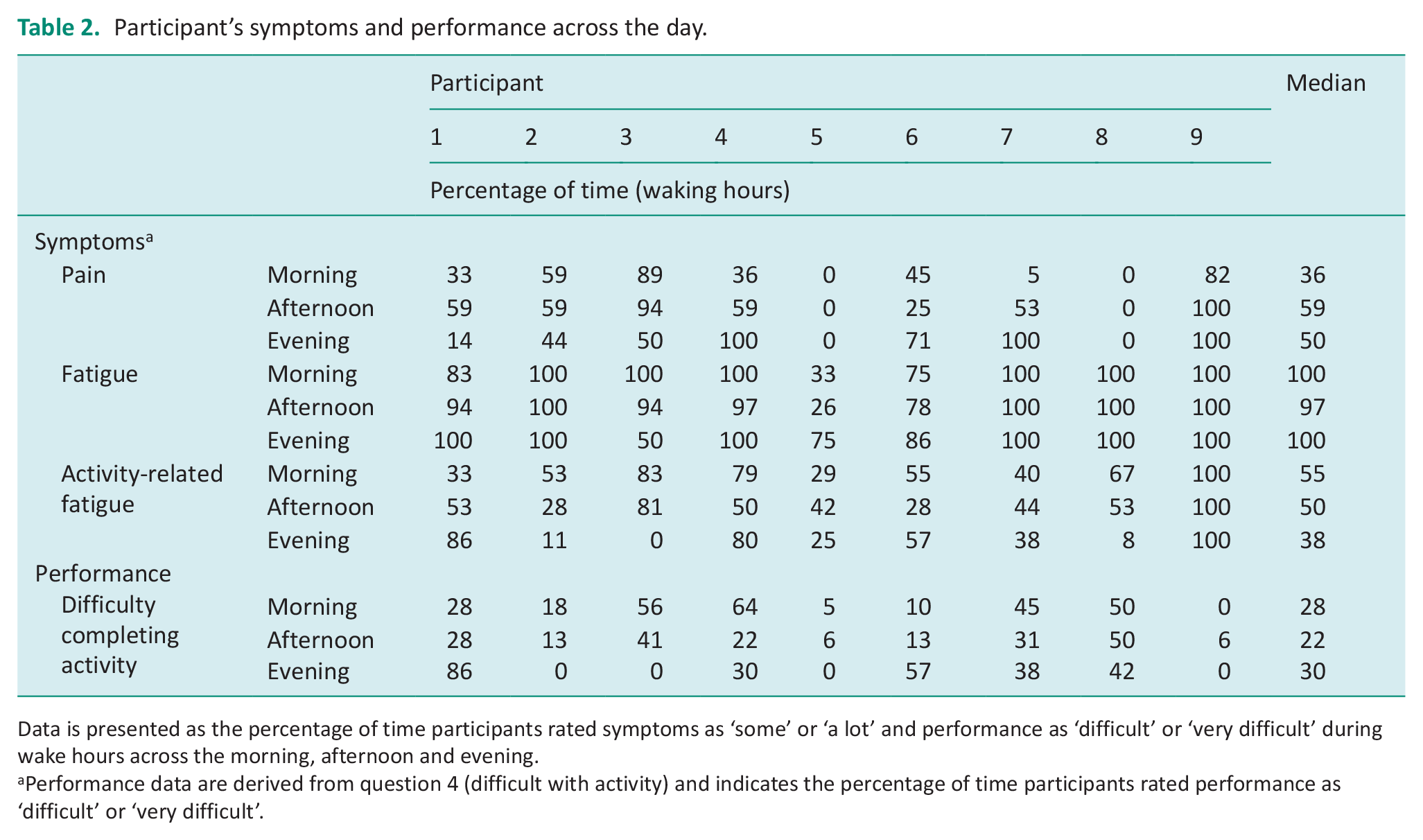
Data is presented as the percentage of time participants rated symptoms as ‘some’ or ‘a lot’ and performance as ‘difficult’ or ‘very difficult’ during wake hours across the morning, afternoon and evening.
Performance data are derived from question 4 (difficult with activity) and indicates the percentage of time participants rated performance as ‘difficult’ or ‘very difficult’.
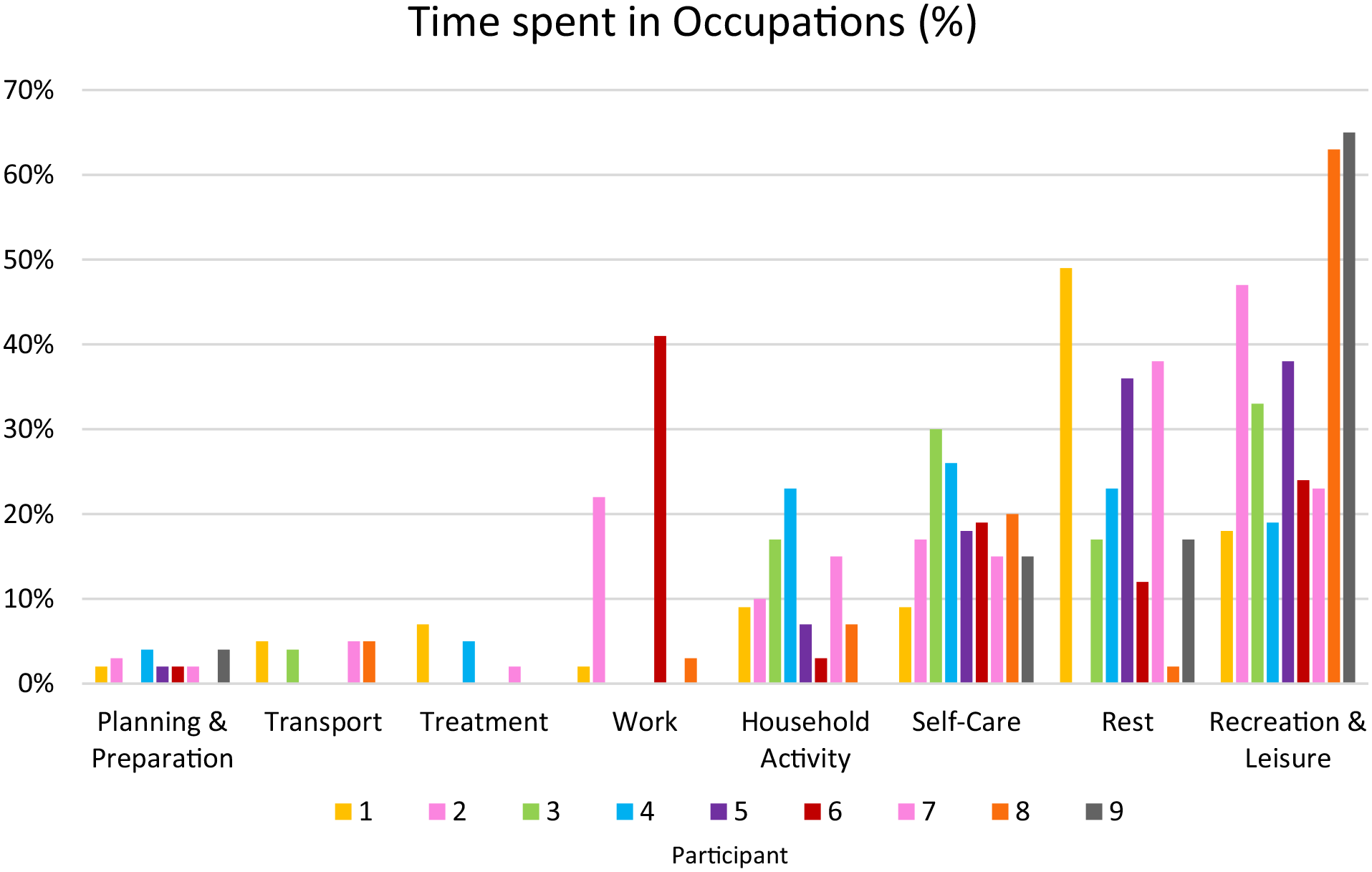
Participant’s time spent in different occupations.
Fatigue
For most participants, there was no significant change in fatigue across the day (x2(2) = 2.21, p = 0.33), with participants (n = 8) reporting consistently high levels of fatigue 90–100% of the time (Table 2).
Activity-related fatigue
Activity-related fatigue results indicated no significant change across the whole day (x2(2) = 1.0, p = 0.61), but there were large individual variations occurring in the morning and evening (Table 2). Activities that required more exerted energy, such as showering, meal preparation, shopping, household activities and socialising, appeared to cause the greatest activity-related fatigue.
Performance
Difficulty completing activity
There was no significant change in difficulty completing activities across the day (x2(2) = 1.52, p = 0.47). Most participants recorded few activities to be difficult, and thus, little individual variation occurred (Table 2). Like activity-related fatigue, activities that required more exerted energy were reported to be the most difficult to complete.
Motivation
Perceived performance
Participants perceived performance of activity did not significantly change over the day for activities done well (x2(2) = 0.74, p = 0.69) or poorly (x2(2) = 1.54, p = 0.46). For activities done well, there was little individual variation for the morning and afternoon. However, in the evening, a large individual variation was identifiable. Two participants could have influenced this variation as they reported completing activities poorly more than 88% of the time (Table 3).
Participant’s motivation across the day.
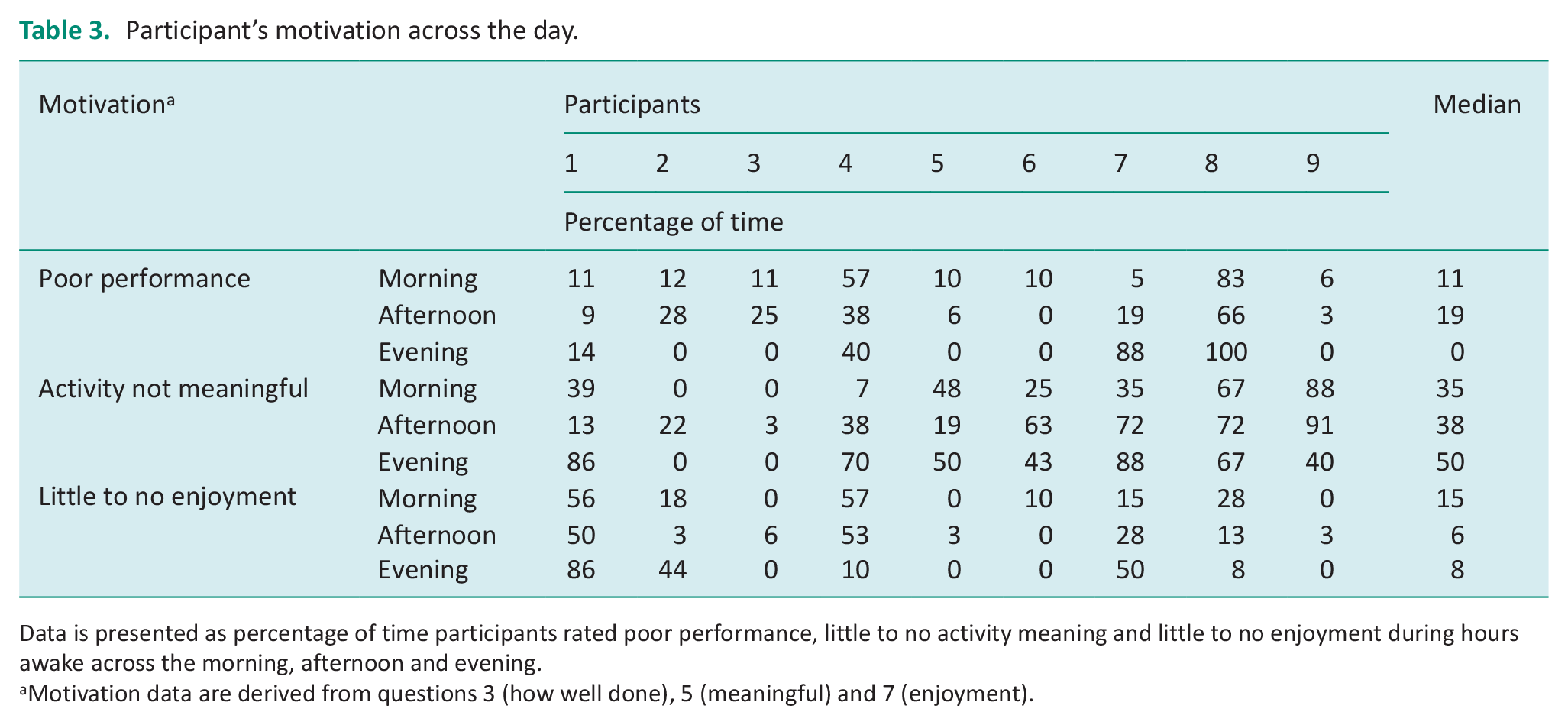
Data is presented as percentage of time participants rated poor performance, little to no activity meaning and little to no enjoyment during hours awake across the morning, afternoon and evening.
Motivation data are derived from questions 3 (how well done), 5 (meaningful) and 7 (enjoyment).
Activity’s Meaning
There was no significant change across the day for whether activities were considered meaningful (x2(2) = 3.82, p = 0.15) or not meaningful (x2(2) = 3.82, p = 0.15) and for both meaningful and not meaningful, large individual variation occurred (Table 3). Meaningful activities took up 50%–65% of participant’s time and were associated with purposeful self-care, work and household activities. Non-meaningful activities comprised 25%–50% of their time and constituted rest, recreation, leisure and planning activities.
Enjoyment of Activity
There was no significant change across the day between participants activity-related enjoyment (x2(2) = 0.26, p = 0.88) and activities that were not enjoyable (x2(2) = 0.19, p = 0.91). Little variation amongst scores occurred for enjoyable activities as, on average, participants reported greater time spent in these activities (Table 3). For activities that were not enjoyable, there was a large individual variation for the evening (Table 3). However, participant one reported their activities to be 86% unenjoyable, potentially influencing this variation as this was greater than other participants.
Occupations
The two 24-hour periods are separated into time spent awake and time spent asleep.
Time spent: Awake
Across the 2 days, participants spent an average of 58% of their time awake. Within this time, participants recorded their time spent across eight occupational categories. On average, participants spent 2% on planning and preparation, 2% on transporting, 2% on treatment, 8% on working, 10% on household activities, 19% on self-care, 22% on resting and 37% on recreation and leisure (Figure 1). For time spent in recreation and leisure activities, 12–65% of these activities were seated activities and included reading, crafts, watching TV/Netflix, video games, or engaging with social media. Participants’ active recreational activities only accounted for 0–11% of activities, including shopping, baking and walking.
Time spent: Asleep
Across the 2 days, participants spent an average of 42% of their time asleep. Seven participants recorded that they started sleeping between 8:00 pm and 10:00 pm, and two participants between 11:00 pm and 12:00 am. All participants reported waking between 7:00 am and 9:00 am. As the time-use information was not recorded over consecutive days, approximate sleep duration per night was not captured.
Qualitative results
The six themes developed from the qualitative data are explored below.
Theme 1: Increased awareness
Most participants reported that completing the NIH ACTRE provided insight into their time- use and offered a better understanding of the meaning behind their activities.
I don’t generally consider whether . . . activities are important to me, so it was nice to consider that and realise that some of them are (Hayley). . . .I realised that extended time using TV as a means to relax was rendering blocks of time ‘meaningless’ (Amanda).
Theme 2: Completing the time diary spreadsheet
Participants expressed a range of perspectives about completing the NIH ACTRE, with most reflecting the experience was:
Time-consuming . . . (Sandra). . . .intensive and hard to complete. . . (Janet).
Participants also shared ideas that could be utilised to improve the NIH ACTRE.
. . .a bit difficult as I didn’t purely do one thing each half hour (Joan). . . .would have liked space to provide clarifying comments. . . [as] life with ME/CFS is far more nuanced than the activity record allows for. . . (Sandra).
Theme 3: Only a snapshot in time
Many participants expressed that capturing 2 days of time-use provided only a small insight/snapshot of how they spend their time.
. . .there’s not enough demonstrative evidence of my condition (Unknown 1). ME/CFS fluctuates, so this was just a snapshot in time. . . (Joan).
Theme 4: Impact on relationships
The changes in a person’s time-use were reported to have resulted in changes in their relationships with family and friends.
Lost many friends . . . [and] my mum . . . became my carer (Janet). a lot less socialising (Joan).
Theme 5: Loss and missing out
ME/CFS has resulted in changed lifestyles for many participants, resulting in a loss of meaningful activities and purpose and an inability to achieve life goals.
From busy working, studying, volunteering, exercising, socializing, gardening, out of the house most of the time, to 95% housebound, lots of naps, no work, no study, no volunteering, minimal socializing, no exercise, needing help with chores (Unknown 2). . . .had to let go of many activities I once loved to do (Jamie).
Theme 6: Adapting lifestyle
Because of ME/CFS, participants reported a need to adapt their time-use, resulting in a lowering of their expectations for participation.
Over time, I adapted my life to my dwindling energy levels . . . (Hayley). I have continually had to lower my expectations and live within my current capabilities (Jamie).
Discussion
This study investigated how occupational therapists could utilise the NIH ACTRE to inform intervention for adults living with ME/CFS in Australia to understand how people with ME/CFS experience their time and what the benefits and limitations of using the NIH ACTRE may be for this purpose.
Understanding participants time-use
The experience of ME/CFS impacts time-use, and as a result, participants experience occupational deprivation that is detrimental to their health and well-being (Bass, 2015). Participants reported that ME/CFS significantly reduced their ability to participate in meaningful activities such as work, study, volunteering, exercise and socialising. Furthermore, all participants reported high fatigue levels, causing them to adapt their lifestyle by changing their habits, roles, interests and values that once formed their identity and purpose. Consequently, the participant’s time-use information from the NIH ACTRE confirmed that ME/CFS has inhibited and reduced their choices and ability to participate in occupations they consider meaningful (Bass, 2015; Baum et al., 2015).
Participants also experienced an imbalance in their time-use and participation in occupations (Bass, 2015), disrupting and changing their lifestyles, with more time spent in sedentary recreation and leisure activities. Whilst participants still engaged in some meaningful, productive and active leisure occupations, the increased energy expenditure limited their subsequent engagement, and often, long rest periods followed. This insight into their time-use caused participants to report dissatisfaction with how they spent their time and supported previous research on how a decrease in self-belief (personal causation), mood, motivation (volition), functional capacity and relationships adversely impact their participation and occupational engagement (Pemberton and Cox, 2015; Taylor et al., 2010). Subsequently, the participants’ quality of life was adversely impacted as their engagement in occupations failed to meet their physical, social, mental and rest needs (Bass, 2015).
Using the NIH ACTRE
Exploring participants’ experiences completing the NIH ACTRE highlighted benefits relevant to collecting time-use information. Participants reported that they found it insightful to review their time-use and reflect on whether the activities were meaningful or enjoyable. This insight may bring about change by highlighting patterns of a participant’s habits, interests, motivation and possible experiences of occupational deprivation or imbalance (Bass, 2015; Kroksmark et al., 2006). Use of the NIH ACTRE could identify opportunities for self-management of change. Occupational therapists could also facilitate opportunities to explore a person’s time-use and, as a result, enable people to be more self-directed and in control of their health management options. Furthermore, the NIH ACTRE accurately reflected participants’ time-use over the 2 days, and despite being cognitively draining for some, it was considered a productive exercise. Thus, participants found the NIH ACTRE a valuable tool to gain awareness about their time-use and, when used with an occupational therapist, could inform interventions for people with ME/CFS by means of adapting occupations and the environment.
Participants also identified disadvantages to the use of the NIH ACTRE. The main limitation was that they felt it did not capture the fluctuating nature of ME/CFS. For participants with ME/CFS they expressed that symptoms are not consistent every day, and therefore, the short period for the time diary did not accurately represent ME/CFS (Eaton-Fitch et al., 2020). So, snapshots of time were merely representative of two separate days. The collection of two separate days also prevented a clear understanding of a participant’s sleep, which would have been of value as the literature suggests that people with ME/CFS often experience sleep disturbances (Eaton-Fitch et al., 2020). The extent of the fluctuations was also not adequately captured by the Likert rating, as participants mentioned that the 1–4 ratings did not seem large enough to capture variances in symptoms, performance and motivation. Participants also reported completing multiple activities within the 30-minute time frames, which may not have accurately reflected the actual percentage of time spent in different occupations. Finally, the complexity of completing the NIH ACTRE for participants who experience impaired cognition meant that completing the time diary was cognitively demanding, arduous and time-consuming for most. Consequently, adaptions to the structure and format of delivering the NIH ACTRE should be considered by occupational therapists to address the above limitations. This could be supported by considering what current non-standardised diaries are being used and how they support information gathering.
Understanding time-use to inform interventions
Combining a person’s illness narrative with the NIH ACTRE could better assist occupational therapists in developing and measuring change in response to interventions for people with ME/CFS. Whilst the NIH ACTRE seeks to quantify the meaning and enjoyment of activities, a person’s illness narrative can provide greater understanding of the time-use information. The benefits of obtaining a person’s illness narrative are demonstrated in the varying themes of ‘Impact on Relationships’ and ‘Loss and Missing Out’, where participants described how ME/CFS impacts had influenced their participation in occupations. Bartlett et al. (2021) further evidenced the value of a person’s narrative as it demonstrated ME/CFS causation of occupational disruption. Therefore, by gaining a better understanding of the person and what they need/want/choose to do and the impact ME/CFS has for them, the combination of the NIH ACTRE and illness narrative could become useful tools. This holistic picture of a person’s occupational participation could enable occupational therapists to work with people to better support them in achieving occupational balance through interventions that adapt to their occupations and environment.
These findings raise an important issue around interpreting what constitutes ‘rest’, as this varied widely amongst the participants. For example, many participants used extended blocks of sedentary recreational activities (e.g. Netflix) to rest, though using these activities to rest is not in keeping with its definition of ceasing activities to restore energy (Bernhofer, 2016). As fatigue is a key symptom that impacts occupations, it is important to ensure that rest is seen as ceasing activity rather than seated activity. Therefore, there may be value in occupational therapists having conversations with people living with ME/CFS to discuss what rest is, the value and purpose of resting, the value of being and feelings surrounding this and how this compares to a person’s perspective of rest (Nurit and Michal, 2003). These discussions could lead to potential interventions, such as energy conservation (Hughes, 2009; Rubal and Iwanenko, 2004).
Limitations
Results from this study should be generalised with caution. When applying findings to the ME/CFS population, the diverse nature of ME/CFS limits the homogeneity in experiences. Therefore, whilst a small sample size was appropriate for this study, it may affect the applicability of results. Furthermore, potential selection bias could have occurred when choosing Facebook support groups for recruitment. Another limitation is that researchers did not seek formal medical evidence of participants’ diagnosis of ME/CFS. As ME/CFS diagnoses use different criteria, it would have been difficult for participants to prove their diagnosis, making the consent and registration process too cumbersome and, therefore, potentially detrimental to the trust between researchers and participants (Hughes, 2009). The utilisation of this tool with a Likert rating scale of 1-4 is another limitation, as it didn’t identify the changes and fluctuating levels of fatigue and pain due to its condensed nature. This was evidenced by a large portion of participants scoring 4/4 (100% of the time) for both pain and fatigue. Finally, methodological factors were constrained by the NIH ACTRE needing clear conceptual definitions, resulting in confusion between the daily activities reported, namely, rest and recreational activities. The self-report nature of time diaries also limited the study as parallel activities (Liedberg et al., 2009), demands associated with completing the tool, recall bias (Jowsey et al., 2014) and social desirability responses (Andrews et al., 2018) could have influenced the information gathered.
Implications for occupational therapy practice
Occupational therapists have an extensive skill set that enables engagement in occupations and enables individuals with ME/CFS to adequately use their time to better their well-being. This study alludes to ME/CFS strongly influencing occupational imbalance, deprivation and changes to identity, suggesting a poorer quality of life. What can we, as occupational therapists, do? We could unpack their use of time, using tools such as the NIH ACTRE, and, in combination with their narrative, create a comprehensive profile of a person’s occupational participation. Maximising the data collection before intervention would be essential through tailoring the NIH ACTRE to increase clinical utility and usability, such as creating a larger Likert rating scale or adding areas for open answers. Once an understanding of the person’s time-use is gained, occupational therapists can then use their understanding of the person’s time-use, environment, occupations and person-related factors to provide appropriate, person-based occupational interventions.
Conclusion
Overall, the NIH ACTRE may be helpful for occupational therapists when working with adults living with ME/CFS but would require revision to improve its clinical utility. However, the NIH ACTRE does provide a baseline for understanding a person’s time-use and can be used to identify occupational deprivations or imbalances. Occupational therapists can use these patterns in occupations, time-use, roles and habits to inform and guide interventions and goal setting. Time diaries, either standardised such as the NIH ACTRE or non-standardised, in combination with the person’s narrative, could be used to create a comprehensive profile of a person’s occupational participation. This type of tool could be used by occupational therapists to collaboratively work towards improved engagement in occupations and better quality of life for adults with ME/CFS.
Key findings
ME/CFS decreases a person’s quality of life and occupational participation.
A person’s narrative and NIH ACTRE provide a greater understanding of their occupational participation and health and well-being.
What the study has added
The study contributes to the occupational therapy evidence base regarding the significant relationship between time-use and person’s health and well-being for those with ME/CFS and how to explore this.
Footnotes
Acknowledgements
The authors would like to acknowledge the Facebook support group facilitators who assisted with the recruitment and thank those who participated in this study. We would also like to thank Richard Johnston for his guidance on the quantitative data.
Research ethics
The authors of the NIH ACTRE provided permission to use the diary, and the Australian Catholic University (ACU) Human Research Ethics Committee granted the necessary ethical approval (2020-226EAP).
Consent
Participants who participated in this study provided informed consent to participate via a written document to which within this study, their information has been de-identified.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in the conduct of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
JH conceptualised the question whilst RR researched literature. All authors were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. RR wrote the drafts of the manuscript and all authors reviewed and edited the manuscript and approved the final version of the manuscript.