
Abstract
Introduction:
COVID-19-related restrictions resulted in changes to time use and occupational participation, impacting individual and collective well-being. This study addressed a knowledge gap concerning the adaptive process during periods of occupational disruption. We explored the experience of occupational disruption and how people managed disruption during the COVID-19 pandemic.
Methods:
We used a qualitative descriptive approach and interviewed 18 participants of a larger survey study of time use during the COVID-19 pandemic undertaken around a medium-sized city in Canada. Transcript analysis was conducted inductively using conventional content analysis.
Findings:
Two overarching themes were constructed during data analysis: The Disruption Experience and Adopting New Habits and Routines. In the face of disruption, participants described a sense of loss and disconnection, and challenges with time management. Establishing new habits and routines required new learning associated with increased time and flexibility, connecting with others and health and wellness.
Conclusion:
During changing pandemic restrictions, participants expressed a sense of loss, disconnection and time management challenges associated with occupational disruptions, but also described ways they adapted, improving their health and well-being. Strategies identified through this work may be used to enhance adaptation during disruptions. Future research should explore differences in adaptation, among more diverse populations.
Introduction
The COVID-19 pandemic has led to unprecedented changes worldwide, with over six hundred million confirmed cases worldwide and over six million deaths as of 16 December 2022 (World Health Organization, 2022). To minimize the transmission of COVID-19, many countries implemented transmission prevention strategies such as lockdowns, mask-wearing and physical distancing. These restrictions resulted in changes to time use and participation in occupations (Kamalakannan and Chakraborty, 2020, Sangster Jokic and Jokic-Begic, 2022). Clark (2020) described occupations as being organized through habits (automatic behaviours) and routines (established sequences of procedures describing occupations that contribute to identity, purpose and structure in daily life). Thus, pandemic-related changes in occupational participation resulted in disruptions to habits, routines and occupations that can negatively impact on sense of meaning, identity and physical and mental health. Understanding how people experienced these disruptions and how they adapted will build on our current understanding of time use and occupation (Pemberton and Cox, 2011), assist occupational therapists to support occupational participation in times of crisis, and help inform health service planning in preparation for similar future crises (Sangster et al., 2022).
Several studies demonstrate the impact of the COVID-19 pandemic on occupational participation of populations across the globe (e.g. Quiroga-Garza et al., 2021; Tujit et al., 2021). For example, with schools closed, parents were expected to home-school their children and work full-time (Lippke et al., 2021; Quiroga-Garza et al., 2021), which increased stress associated with childcare (Adams et al., 2021). In a study in India, Deshpande (2020) reported increased time spent by men on household chores, likely related to job loss. Meanwhile, working from home allowed some people more time for personal activities due to the lack of need to commute (Lee and Tipoe, 2021). The types of leisure activities also changed, with less time spent outside the house (walking, shopping, caregiving, or meeting friends (Tsouros et al., 2021)), and more time spent watching TV, consuming online media and playing online games (Lee and Tipoe, 2021; Wagner et al., 2021). Changes made to routines and occupations because of the pandemic led to increased feelings of isolation, loneliness and psychological distress (Aknin et al., 2022; Best et al., 2021; Siew et al., 2021).
Other studies contribute to the knowledge of how people adapted during the COVID-19 pandemic. For example, in a survey of adults in Belgium, respondents reported adapting their activities by changing the manner of participation, changing the environment and searching for comparable activities that provided the same purpose or meaning (Cruyt et al., 2021). Findings from a U.S. study found that while resilience was low overall during the pandemic, those who went outside more often, exercised more, slept better, perceived more social support and prayed more often were more resilient, that is they were better able to withstand and adapt positively to adversity (Killgore et al., 2020). Luck et al. (2022) explored the experiences of individuals living with chronic diseases in managing their health during the pandemic. Participants reported increased focus on occupations related to maintaining health and well-being but were impeded by feelings of vulnerability to poor outcomes if they caught COVID-19 and environmental barriers. A study of community-dwelling adults in Singapore during the pandemic found some participants had improved coping through seeking social support, occupational adaptation, adhering to hygiene and distancing measures and developing stress management strategies (Lee et al., 2022). Younger and middle-aged adults were more successful than older adults in using technology to these ends (Lee et al., 2022). Studies of older adults early on in the pandemic, (Carlsson et al., 2022; Rotenberg et al., 2021) and those living in low-income housing (Aubin et al., 2022) note experiences of disruption to daily activities with adapting through a supportive social network, use of technology for connecting with others, creating structure through activities at home, creating enjoyable moments and focussing on the positive.
While the above research provides important information on how people spent their time and adapted to disruptions in occupational participation during COVID-19 restrictions, more in-depth information on the process of adapting to occupational disruptions among different populations and in different contexts (e.g. locations, stages of the pandemic) is needed to provide a more fulsome understanding to inform future practice and policy in times of crisis. The purpose of this research was to explore individuals’ experiences of occupational disruption, that is, the temporary inability to participate in necessary or meaningful occupations due to external factors (Townsend and Polatajko, 2007), and ways in which they managed these disruptions during a 6-month period of re-occurring lockdowns in the pandemic in the region surrounding a medium-sized city (between 100,000 and 500,000 people) of Canada.
Methods
We used a descriptive qualitative approach (Neergaard et al., 2009) to explore the experiences of people with varying levels of well-being in managing occupational disruption during pandemic restrictions. This approach was appropriate as we sought a comprehensive description of an event or phenomenon with minimal interpretation and did not seek to apply theory. Qualitative description stays close to the data and lacks the in-depth conceptual description and interpretation provided by interpretive methods (Neergaard et al., 2009; Sandelowski, 2000).
Sampling and recruitment
We purposively invited participants who took part in a longitudinal survey study that used time use diary methods to examine activity patterns and well-being (Kessler et al., 2022). In the larger study, 185 adult participants were recruited through community and educational organizations in a medium-sized city and the surrounding area in Ontario, Canada and through social media. Adult age (18 or older) was the only inclusion criterion to participate. We planned to recruit 24 participants to ensure a sample that included a broad range of experience and was likely to attain data saturation (Hennink and Kaiser, 2022). We sought to build a sample that included people of different ages who represented a range of well-being scores. We invited participants with low and high well-being scores and moved towards middle scores, while also considering age, to recruit the target number. We initially sought to also include diversity with respect to gender and race/ethnicity, but the lack of diversity in the original sample on these variables did not allow for this.
Well-being has been defined as the combination of feeling good (e.g. happy, content, engaged, confident) and functioning effectively (e.g. having a sense of control and purpose and experiencing positive relationships; Huppert, 2009). Therefore, a composite well-being score was created by combining scores from the original survey that included the stress and emotions subscales of the CoRonavIruS Health Impact Survey (Nikolaidis et al., 2021), and the Satisfaction with Life Scale (Diener et al., 1985). Scoring direction was converted on one measure such that lower scores consistently represented better well-being and measures were given equal weightage (Moreau and Wiebels, 2021). Selected participants were contacted by e-mail. Eighteen participants consented and completed the interview.
Data collection
Data were collected using a 60 to 90-minute, semi-structured interview that expanded on the participant’s most recently completed time use diary from the survey study. The diary captured all activities and their duration over the course of 1 day. To explore how people experienced disruptions and how they adapted, qualitative interview questions focused on the purpose of each activity, how activities were accomplished, the participant’s sense of choice versus obligation related to the activities, and specific constraints on the activities. We also asked participants about how well they felt they were managing changes to their time use during the pandemic. Interviews were not completed immediately following survey completion; therefore, the Research Assistant (LA) reviewed the completed diaries with participants and used it as a guide to provide structure. Interviews were conducted by phone or videoconference per the participant’s preference and were recorded and transcribed verbatim. Interviews took place from February to July 2021. Contextually, lockdown restrictions in the region were lifted at the end of February/early March 2021, were reinstated in April, and started to lift again in June 2021.
Data analysis
Analysis explored the changes to occupational participation experienced by participants, choices made, including reasons for these choices, and the impact of choices on well-being. Occupational participation was defined as taking part in ‘valued occupations within meaningful relationships and contexts’ (Egan and Restall, 2022, p. 15). Conventional content analysis (Hsieh and Shannon, 2005) was used to code and categorize data and NVivo software (QSR International Pty Ltd., 2018) supported the analysis. To begin, three coders (EB, JM, DK) independently coded a transcript and discussed key emerging ideas that formed the preliminary codes. Next, two coders (EB, JM) coded two additional transcripts independently, followed by a meeting of the three original coders to establish the coding framework. Both primary coders analyzed the remaining interviews with periodic consistency checks. Finally, codes were iteratively grouped into overarching and sub-themes by the three coders.
Ethics approval was obtained through Queen’s University Health Sciences & Affiliated Teaching Hospitals Research Ethics Board ID#: REH-770-20 in August 2020. used throughout the article.] All participants were sent an information sheet and provided informed verbal consent documented by the research assistant to take part in the interviews. They were assigned pseudonyms for reporting of findings. Participants were offered a $25CAD gift card as a token of appreciation for their time.
Findings
Eighteen participants (1 male and 17 female) took part in the qualitative interviews (see Table 1). All participants self-identified as White except two (Angela and Tegan). Five participants were retired, eight were working full-time, two were post-secondary students, and three were not working. Participants reported income ranging from less than $25,000 up to a maximum of $199,999. Seven participants reported no chronic health conditions while eleven reported between one and three conditions. The most reported health conditions were mental health conditions (n = 4), arthritis (n = 3), heart disease (n = 2) and asthma (n = 2). Other conditions were stroke, spinal cord injury, epilepsy and migraines. The mean well-being score was 51.4 with a range of 30–82 (scale range was 0–100).
Participant demographic characteristics.
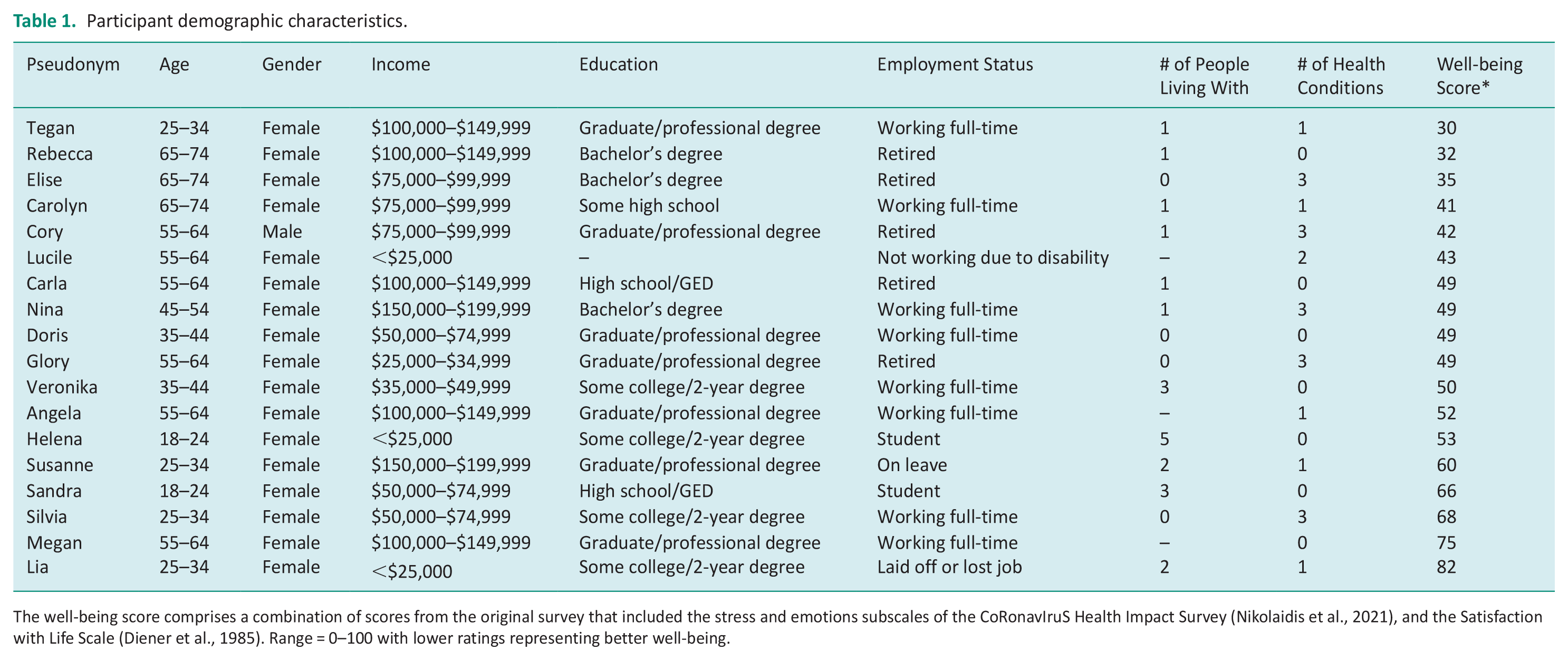
The well-being score comprises a combination of scores from the original survey that included the stress and emotions subscales of the CoRonavIruS Health Impact Survey (Nikolaidis et al., 2021), and the Satisfaction with Life Scale (Diener et al., 1985). Range = 0–100 with lower ratings representing better well-being.
Two overarching themes resulted from data analysis: The Disruption Experience and Adopting New Habits and Routines (See Figure 1). Participants spoke about disruptions to their activities and daily routines including leisure, productivity and health-related activities. These disruptions were experienced in a variety of ways that negatively impacted well-being. However, throughout their dialogues, participants also spoke about changes to their habits and routines that promoted wellness. Adopting new habits and routines reflected an overarching way of adapting to the pandemic restrictions. The overarching themes and sub-themes are presented below with supporting quotes. Data saturation was achieved as no new codes were identified during the final interview analyses.
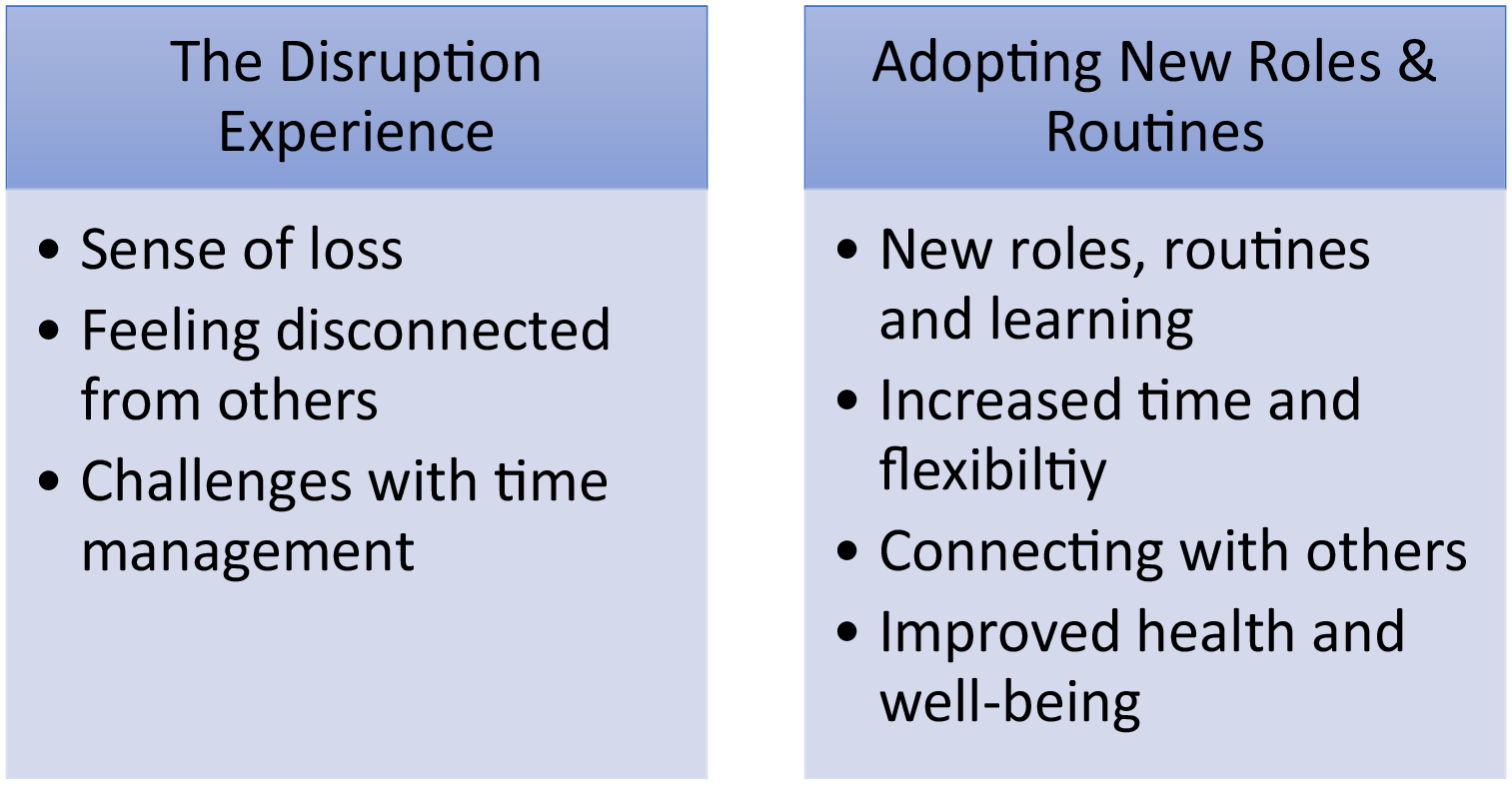
Overarching themes and sub-themes.
The disruption experience
Disruption of habits and routines due to pandemic restrictions was prominent in participants’ daily lives. The experience of disruption was associated with three major impacts on the well-being of participants: a sense of loss, feeling disconnected from others and challenges with time management.
Sense of loss
Participants spoke about disruptions to active exercise, physical activities and other types of leisure activities, as well as disrupted work and health services. These disruptions were seen as impacting enjoyment, motivation and in some cases, health and well-being.
Most people shared frustrations associated with losing activities that held personal meaning. Lia reported ‘I was finally going to an NHL game and that got shut down. So, it was just like loss after loss after loss and like completely shut down’. Doris talked about missing the ability to travel, ‘I love travelling and just visiting new cultures, new places. . .’ Some participants experienced loss of work activities which in turn led to income loss and stress. Lia reported that in ‘the span of two days, I lost one job and another job was put on hold’. Several participants discussed how volunteer opportunities were discontinued.
Participants sought ways to adapt to new forms of occupation to fill the void of these losses. For example, some roles and activities were shifted to an online platform. This helped to continue engagement, but many noted how the meaning or the joy in the experience had changed. For example, Lucile, who volunteered with local hospitals, students and other organizations noted, ‘I like to see people. I like the human contact and its bigger and better understanding if you’re face to face’. Silvia described her decreased enjoyment and motivation with exercise, ‘I’d rather be out playing a sport with others, I just find it more enjoyable. . . it doesn’t feel like exercise, you’re just having fun with friends’. Nina noted ‘[I] lost that engagement that I used to get from in-person events’. Often, occupations were lost due to social isolation and could not be fully replaced. Carolyn, for example, shared that adapting to changes and having to stay home wasn’t easy and emphasized the difficulty in ‘finding things that gave me pleasure in the house’.
Occupational disruptions impacted some participants’ activities that supported health and well-being. For example, Megan shared the challenges she was experiencing with her health:
It’s been difficult . . . I’ve gained 15 pounds . . . I’m sore, I’m tired. I’m stiff, I have arthritis and if I do yoga and swim I have no problems with my arthritis, but now . . .I don’t have the energy. . . . so I’m not as productive at work.
Glory shared that she missed her in-person, group mental health support meetings and her sessions with her therapist which also promoted social interaction.
Feeling disconnected from others
Disruptions to in-person interactions with a transition to communicating virtually led to some participants feeling decreased connection with others, and a lack of support. Susanne noted, ‘The main [challenge] was feeling so disconnected from our families and our social circle’. The change was particularly frustrating for activities that had typically been done in parallel or in collaboration with others, such that socialization was central to the meaning experienced in an activity. Glory, who had been part of a knitting group with older adults, shared, ‘A lot of the elderly, they don’t really like to do a lot on Zoom’. She noted that she did not meet as often with her friends on-line and missed in-person meetings where ‘we eat together, we [have] coffee, we just have so much fun’. Working from home also led to loss of social interactions. Doris noted, ‘The hard part I think with working from home is that disconnect’.
The lack of connection also reduced the quality and effectiveness of activities. Helena, a student, noted a lack of connection with and support from people in her academic programme, ‘it’s not the same talking and trying to get to know someone texting them or doing Facebook messages. I also don’t have the same kind of academic support from my peers’. Susanne shared a lack of tangible support from her family as she went through a pregnancy and having a baby during the pandemic. She explained, ‘It was challenging because it was almost like we had to put up barriers to our family. And, typically, it would have been like, yeah, hold the baby or please take the baby for an hour’.
Challenges with time management
Disrupted habits and routine led to challenges managing time and activities, particularly related to working from home and managing time spent on social media. Participants identified increased procrastination, lack of structure and increased stress and anxiety related to these time management challenges. Silvia shared, ‘At home, because I’m not going out and doing as much as I usually would, I procrastinate even more than normal’. Other participants identified that the lack of structured time led to increased work stress. Veronika explained,
When I’m at work, I have my lunch break and my recess breaks, so I always had those to socialize and relax and so being at home obviously you don’t like get an hour away during the day, so that was more stressful.
Doris described a lack of structure and increased stress associated with working in a constantly changing environment: ‘I like lists, I like to plan, I don’t like triaging or being reactive and that was something we did a lot at the beginning of COVID’.
Many participants discussed concerns related to spending more time on social media and watching TV or streaming services. Megan shared her concern about being ‘addicted’ to watching shows on streaming services and noted, ‘I spend way more time on social media now’. Nina shared, ‘it’s hard for me to control it [spending time on social media] once I get started. . .I consciously have to shut it off’. She noted that she was ‘becoming a little compulsive about what’s going on and like scanning, scanning, scanning for anything COVID’, which began to increase her anxiety levels and negatively affected her sleep.
Adopting new habits and routines
Although participants identified disruptions to habits and routines, they all found ways to adapt through adopting new habits and routines. These new practices included new routines, roles and learning and were associated with increased time and flexibility, connecting with others and improved health and wellness.
New routines, roles and learning
Participants spoke about the positive impact of the pandemic on their day-to-day lives through the establishment of new routines and roles, and the integrations of new learning. New routines and roles led to more consistency, enjoyment, feelings of contributing and learning.
Doris described how establishing new routines took effort but led to more consistency with her days, ‘Just kind of getting back into a little bit of a routine of actually making breakfast, having lunches at home . . . Now kind of forcing myself into that habit again of cooking, going for walks, that sort of thing’. Nina shared that she is now ‘on that regular schedule of I usually get up before my alarm goes off because I’m more well rested and I get to bed at a fairly common hour now where before it was all over the place’. Carolyn noted increased enjoyment from her routine of regularly walking to and from work each day. Susanne reported establishing a routine of ‘just spending our time going outside . . . .’
Some participants adopted new roles, including new domestic roles (e.g. cooking and house cleaning), and volunteering, that provided a sense of contributing. Cory mentioned the positive changes associated with taking over cooking and cleaning roles since the pandemic because he was home and his wife worked full-time. In his words,
I was able to cook dinner and then I was starting to do housecleaning and look after the housework in general, whatever it entails. And I’m very happy to do it, she’s working full time and I’m happy to help out in her place.
Angela spoke about adopting new virtual volunteer roles calling older adults and helping children with homework.
New routines and roles required new learning. Doris shared her appreciation for the new learning associated with the shift in technology use, ‘I love learning new technologies. I think coming up with ways [that] are flexible for people’s schedules and you still get the same content and productivity have been helpful’. Elise spoke about her new learning related to using Facebook, ‘I started posting a few general things, you know, a joke or a clever saying. . . then I started adding a few personal comments about my personal life and found that that invoked a lot of conversation on Facebook with friends’. Nina shared her new learning related to cooking ‘I’ve been buying a lot more cookbooks. [. .] So more time to experiment and try new things’. Sandra described new insights regarding learning strategies for studying, ‘I’ve learned to be able to differentiate between passive and active learning, which is a positive. So, I know when I go back to in-person . . . I’ve learned from this year of school how to do it [reading] actively’.
Increased time and flexibility
Participants reported having a sense of increased time and flexibility that allowed them to take more time for meals, housework, and family, and to be creative. The increased flexibility and sense of time resulted in participants feeling like their life activities were experienced at a more relaxed pace. Glory explained that working from home was ‘more relaxing in the sense that I’m not rushing to meetings’. According to Carolyn, ‘the sense of urgency has been reduced’ since the beginning of the pandemic. Megan shared that she does more cooking and meal preparation ‘because I have time’. Sandra noted, ‘I find I am purposefully taking breaks. . . I’m going to eat my food and not work at the same time and take a minute, relax, breathe’. Veronika shared the productivity benefits associated with time gained through working from home: ‘I have more time to keep the house clean and cook better meals and spend more time with the kids’.
Time flexibility also allowed for more creativity and the opportunity to think about doing different things. Angela shared that she enjoyed being ‘more creative in my kitchen’. Glory used wool spinning and knitting as a creative outlet. She noted ‘It is a great way to focus because I have a lot of problems with memory and concentration’. Projects such as needlework were something that Rebecca described as an enjoyable ‘meditative process’ that gave her a ‘liberating effect’. Elise shared, ‘I am able to read a lot more than normal. I was able to explore and develop new interests’. Lia commented, ‘I was able to, like, do a deep dive and kind of figure out what I actually like doing. And what I think I’m good at and stuff like that’.
Connecting with others
While many challenges with social interactions were associated with pandemic-related changes, several participants reported an increased connection with others through adopting new routines, roles and learning. These connections included increased social interactions, quality time with family and more time spent with pets.
Angela mentioned increased social interactions with friends: ‘Interesting enough, some [friends] I’m seeing more often, like zooming more often than I would in person’. Some participants noted that technology expanded opportunities for connections. For example, Glory shared her experience with Alcoholics Anonymous (AA) stating, ‘there [were] like a million AA Zoom meetings, you can be on it 24/7 if you wanted to’. Tegan also reported easier access to online programming. She described how she ‘created a really big community. . . that I didn’t have before’. Elise found that joining an online group allowed her to stay in touch better than ever with other seniors within her community. She noted, ‘I became more social than normal’. Veronika shared her experience with online dating. She stated, ‘[The experience was] actually really fun just to, like, talk to people’.
For some participants, the pandemic led to an increased connection with family. Susanne discussed the positive change of an increased family focus, ‘We’re not rushing around doing all sorts of social things on the weekend. So, we’re focusing on making dinner or going for a walk as a family. So, it’s a net positive . . . that we’re rebuilding our social connections’. Glory commented, ‘I’m not that close to my family. But since the pandemic, we’ve been playing Euchre online once a week. And we also have a family Zoom meeting once a week’. Tegan noted the importance of spending her lunch breaks, while working from home, with her partner and dogs.
Other participants discussed the importance of spending more time with their pets, as well as family and friends. For example, Glory noted that to make up for the loss of social interactions during the pandemic, she really began to interact with other people at the dog park.
Improved health and wellness
Participants noted that new ways of engaging in activities positively impacted their health and well-being. Benefits included increased access to various wellness programmes offered virtually, increased physical activity including walking and working out from home, and spending more time in nature.
From a physical activity standpoint, Helena noted that although her motivation for working out and dancing decreased at the beginning of the pandemic, she began to slowly reintroduce ‘working out or doing yoga partially to feel better, and then also to make it easier for me to fall asleep’. Other participants shared that walking and moving their bodies helped with both their physical and mental health. Nina noted, ‘If I have to miss my run in the morning [. . .] I don’t feel great for the rest of the day . . . It gives me a good kick start, like an adrenaline rush’.
Although some participants missed having access to local gyms, others enjoyed working out from home or via virtual means. Angela shared, ‘I exercise with two other colleagues virtually. So we meet 6–7 days a week for 40 minutes. And we exercise, we do yoga, or we do fitness splendour, one of those online ones’. Tegan, who connected to a virtual fitness community for dancing, shared:
There was a whole world out there we never knew existed. Nobody was online, you’d go to the studio in your hometown and be part of the community there and that would be your whole community. But now, . . . I have taken lessons, from people on the other side of the world.
Setting up a home gym was also a solution for some participants. For example, Rebecca shared that she and her partner bought a Peloton bike to help them stay in shape during the winter lockdown season when they could no longer bike outdoors. She felt this was a positive solution since she ‘never liked going to the gym’.
Spending more time in nature during COVID-19 was a therapeutic and enjoyable health and wellness activity mentioned by participants. Rebecca shared that being in nature, either by herself, with her partner, or surrounded by others was ‘very therapeutic’. Glory also commented, ‘We go hiking through the trails in the woods and that helps me a lot connecting with the outdoors and seeing my dog happy’.
Discussion
This study provides a unique perspective on how people in a small city in Canada and the surrounding area experienced and adapted to disruptions in habits, routines and occupational participation in a period of re-occurring lockdowns during the COVID-19 pandemic. Participants reported a variety of disruptions to habits, routines and occupations that were associated with the experience of loss, disconnection from others and challenges with time management. However, participants at all levels of well-being described ways they adapted to these disruptions through adopting new habits and routines.
Participants experienced disruptions to work, social and recreational activities that were associated with a sense of loss including loss of volunteer and paid work, loss of access to supports and services, loss of structure and routine and loss of enjoyment. Disruptions also led to feeling disconnected from family, friends and colleagues and to challenges with time management. These experiences resulted in increased stress and anxiety. Similar experiences and challenges related to disruptions in habits and routines experienced by participants in our study have been reported in other studies. Disconnection from others, increased stress and anxiety, negative health impacts and increased social media use have been reported by other researchers, and linked to negative impacts on overall well-being (Best et al., 2021; Brooks et al., 2020; Cruyt et al., 2021; Droit-Volet et al., 2020; Lee et al., 2022; Petzold et al., 2020; Şentürk, et al., 2021), In particular, a qualitative study of older adults reported occupational disruption that led to adoption of new less meaningful activities, and the experience of threat to independence and fluctuating mood (Rotenberg et al., 2021). Together, these studies document how mental heath and well-being can be impacted when restrictions limiting occupations and social connections are imposed.
An important aspect of the current study is that it adds to our understanding of ways in which people adapted to occupational disruptions during the pandemic. Participants described adopting new routines and roles that were associated with enjoyment, new learning, increased time and flexibility, creativity, connecting with friends, family and pets and increased health and wellness. Participants made efforts to establish consistency in their day-to-day lives through their new routines and roles. This was facilitated by a relaxed pace where there was time for creativity and connecting with important others and pets. In this way, findings support the relationship between occupational dimension of balance and rhythm and well-being (Pemberton and Cox, 2015).
Health and wellness were facilitated through access to on-line programmes and services, engagement in physical activity, and taking time to be in nature. These results are consistent with other studies that reported eating and lifestyle changes (Di Renzo et al., 2020); finding new ways of doing and creating structure (Carlsson et al., 2022; and coping through seeking social support, and occupational adaptation (Lee et al., 2022). Likewise, in a study of older adults living in low-income housing, a supportive social network, access to technologies and a positive attitude seemed to promote occupational adaptation (Aubin et al., 2022).
Participants in our study adopted habits, routines and occupations, including creative and physical activities, that provided meaning during pandemic restrictions. Creative activities may assist with coping, distraction, or enjoyment (Kapoor and Kaufman, 2020), while taking time to be outside in nature, exercising and connecting with others may promote resilience (Killgore et al., 2020). Killgore et al. (2020) also noted factors of sleep and prayer that were not specifically identified in our study.
These findings build on and add new insights to previous studies that primarily used survey methods. Contrary to our findings, Cruyt et al. (2021) found that participants did not modify in-house activities such as self and family care, cooking and household chores during the COVID-19 lockdown. However, participants in that study did adapt to activities performed outside the home such as sports, training and working and social activities. These were performed in a different environment or manner or were replaced with a different activity with a similar purpose or meaning (Cruyt et al., 2021). A study of on-line workers in the United States (US) that examined the tendency towards ‘silver lining’ thinking found that participants adapted by identifying benefits including having more time with family and friends, experiencing life at a slower pace, and focusing on physical health (Kowalski, et al., 2022). A German study found that while over 50% of participants reported psychological distress, anxiety and depression during COVID-19; use of strategies such as maintaining a healthy lifestyle and social contacts and accessing information on where to get medical treatment seemed to help (Petzold et al., 2020).
The current study adds an in-depth perspective on the experience of individuals who were going through a period of uncertainty where pandemic restrictions were being lifted and re-instated. These findings align with several studies from other countries and support the need for occupational therapists and other practitioners to consider measures to enhance social supports and promote adaptation to habits, routines and occupations to enhance well-being during times of crisis.
Limitations
This was a qualitative study of participants with limited diversity in one region of Canada. All study participants, except one, were women; most reported income over $75,000CAD and only three reported income less than $35,000CAD, and all but two identified as White. While we sought to include diverse participants in this study, we were limited by the characteristics of the larger study. Therefore, findings may not be similar in persons of other racial and socio-cultural backgrounds or those living in other regions. As well, member checking was not done, which may limit trustworthiness of findings.
Conclusion
Participants expressed a sense of loss, disconnection and time management challenges associated with occupational disruptions during a period of reoccurring COVID-19 lockdowns, However, they also described ways they adapted, improving their health and well-being. Adopting new habits, routines and roles provided enjoyment, new learning, increased time and flexibility, creativity and social connection. Occupational therapists and other providers can draw upon the strategies identified through this work to enhance individual adaptation during times of lockdown and social restrictions. Future studies are needed to better understand differences in adaptation for specific populations, particularly those in vulnerable sub-groups.
Key findings
Occupational disruption impacted well-being through feelings of loss, social disconnection and challenges with time management.
New habits, routines, and roles provided enjoyment, learning, flexibility, creativity, and social connection.
What the study has added
This study adds to the knowledge of ways in which occupational therapists can support well-being during times of occupational disruption through promoting establishment of habits, routines, and roles that contribute to enjoyment, learning, creativity and social connection.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226241232815 – Supplemental material for Adopting new habits and routines in response to COVID-19 lockdown disruptions: A qualitative study
Supplemental material, sj-docx-1-bjo-10.1177_03080226241232815 for Adopting new habits and routines in response to COVID-19 lockdown disruptions: A qualitative study by Dorothy Kessler, Emma Boudreau, Jennifer Maitland, Rosemary Lysaght, Mary Ann McColl, Libby Alexander, Clarke Wilson, Beata Batorowicz, Vincent DePaul and Catherine Donnelly in British Journal of Occupational Therapy
Footnotes
Research ethics
Ethics approval was obtained through Queen’s University Health Sciences & Affiliated Teaching Hospitals Research Ethics Board, ID # REH-770-20 in August 2020.
Consent
All participants provided informed consent verbally (as per an approved Research Ethics Board protocol) to take part in the interviews and were assigned pseudonyms for reporting of findings.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, public involvement in the research was included in planning (data collection) and progress (recruitment) of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the Social Sciences and Humanities Research Council of Canada; under Grant 1008-2020-0142.
Contributorship
DK, RL, MAM, SG, CW, BB, VDP, and CD conceived the study and developed the protocol. DK, EB, and JM were involved in researching literature and data analysis. LA was involved in gaining ethical approval, patient recruitment, and data collection. DK, EB, and JM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.