
Abstract
Introduction:
This study aimed to investigate the effectiveness of modifying the home environment on falls in older adults with dementia.
Methods:
In this single-blind clinical trial study, 44 older adult patients with dementia who met the inclusion criteria, were included in the study and then randomly assigned to intervention (n = 22) and control (n = 22) groups using a balanced block randomization method. The intervention group received home modifications, while the control group did not receive any modifications. After intervention, The HOME Fall and Accident Screening Tool was used to assess falls. The ethics committee of Tehran University of Medical Sciences approved the study procedure (IR.TUMS.FNM.REC.1399.163) and this study was registered in the Iranian Registry of Clinical Trials with the code: IRCT20210106049950N1.
Results:
Comparing the mean fall risk scores between the two groups at the beginning of the study showed no significant difference in the risk of falling (p = 0.6). By contrast, at the end of the study, this difference became significant between groups (p < 0.001). This comparison in the control group at the beginning and end of the study indicated no significant difference (p = 0.32). However, it was significant in the intervention group at the beginning of the study and after modifications (p < 0.001).
Conclusion:
Modifications by applying changes and reforms to the home environment reduced the risk of falling in older adults with dementia.
Introduction
The World Health Organization defines dementia as a cognitive syndrome in which memory, thinking, behavior, and the ability to perform daily activities deteriorate. Furthermore, it is the fifth leading cause of death and a major public health concern. Approximately 50 million people worldwide have dementia, with nearly 60% living in low-income or middle-income countries, and the number is growing by nearly 10 million each year (World Health Organization, 2019). Older adults with cognitive impairment and dementia are at risk of falling and its consequences (Shaw, 2002). Dementia can increase the risk of falling by impairing judgment, walking, visual-spatial perception, and ability to recognize and avoid dangers (Van Doorn et al., 2003). The World Health Organization defines a fall as an event that results in a person coming to rest inadvertently on the ground (World Health Organization, 2018). Almost 60% of older adults who have fallen once in the past year have experienced falling at least once more (Goswami, 2017). The risk of falling in older adults with dementia in the community is 2–3 times higher (Yeni and Yilmaz, 2022). Serious injuries caused by falling include femur fracture, subdural bleeding and hematoma, bruises, sprained joints, muscle strain, death, psychological effects, fear of falling, loss of self-confidence, and limitations in performance (Mehraban et al., 2011). More than half of those with a history of falling experience another fall (Letts et al., 2010). The majority of falls occur in the home environment and during daily activities (Mortazavi et al., 2018). Neurologists recommend that the living environment of people with dementia should be modified. Necessary environmental adaptations should be made to improve everyday action performance, lifestyle, and quality of life (Giovannetti et al., 2007). Home modifications are a set of strategies that include modifying and renovating the home and building, using assistive devices, using visual cues and memory aids, rearranging or removing furniture and dangerous home appliances, and simplifying activities (Gitlin, 1998). With the increase in the aging population and the prevalence of chronic health conditions, the number of people affected by environmental barriers is expected to rise (WHO, 2011).
As the population of the elderly increases, it is important to pay more attention to elderly health concerns. Rehabilitation plays a prominent role in medical services for older adults (Maghsoudei, 2006). In many falls, environmental factors are important (Montero-Odasso et al., 2022), and most falls occur in the home environment and during daily activities. As people get older, they spend more time at home, and the activities they perform at home often lead to them falling (Karlsson et al., 2013). Modifying the home environment creates a safe and supportive environment for dementia patients and allows them to function at the highest possible level of independence (Sheldon and Teaford, 2002). Therefore, this study aimed to investigate the effectiveness of modifying the home environment on falls in older adults with dementia.
Materials and methods
Study design and participants
The statistical population of this single-blind clinical trial study was all older people with dementia in Tehran, Iran. In all, 44 older adults with dementia were recruited from hospitals affiliated with Tehran University of Medical Sciences (TUMS) in 2022–2023. The disease was diagnosed by a neurologist with experience in geriatric medicine. The inclusion criteria were as follows: older adults aged 65 and above with mild dementia symptoms; in other words, their Clinical Dementia Rating test (CDR) score for the individual was between 4.5 and 9, and they live at home. The following were considered as exclusion criteria: older adults with dementia who were residents of nursing homes or bedridden, older adults with a history of other neurological problems, orthopedic and rheumatology disorders, and acute psychiatric disorders based on the information in the medical history.
Sample size and random allocation
To determine the required sample size in this study, the value of type one error (alpha) was considered equal to 0.05 and the power of the study was 80%. A study by Gitlin et al. has investigated the elderly with dementia and estimated the average Instrumental Activity Daily Living (IADL) in the control group to be 5.8 (standard deviation 0.3) and in the intervention group to be 5.5 (standard deviation 0.6), we have considered the acceptable clinical difference between the two groups to be equal to 0.5 points, and using the following formula, the sample size is estimated to be 19 people for each group, with the possibility of dropping 22 people in each group and a total of 44 people:

Participants were then allocated to intervention and control groups using balanced block randomization with blocks of four and six. An epidemiologist conducted the randomization. Randomization, allocation, and concealment were conducted using an online site (www.sealedenvelope.com). As for the randomization method, an initial sequence of 44 random cases was generated using the block method, which included 22 intervention cases and 22 control cases. An epidemiologist kept a copy of a random sequence. The random sequence was kept secret from the home visitor, representing the concept of concealment in the random assignment process.
Study procedure
After completing the written consent form, demographic information including gender, age, type of dementia, fall history, and the number of falls was based on the observations and statements of caregivers of elderly people. The home visit and intervention were done by a senior occupational therapist trained to modify the home environment. In Iran, usual treatment includes routine occupational therapy interventions that do not include home modifications. The control group received the routine occupational therapy intervention without home modification. In the control group, until the end of the study, home modification was not implemented and they were only evaluated. If the participants in the control group were willing to do home modification, after finishing the study, home modification was done for them.
Intervention
Home modification interventions for older adults with dementia were carried out by a master’s degree student of occupational therapy who was trained to modify the home for the intervention group, and the participants in the control group did not receive any home modifications. The following home modifications were made for older adult patients with dementia who met the study’s inclusion criteria: modifications for access, including doors, handles, barriers, corridors, ramps, and barriers (Stark, 2004); modification of the edges of stairs inside and outside the house; checking and modifying the condition of flooring outside and inside the house, bathroom and toilet; checking the floor surfaces for slippage; ensuring that floor coverings (carpets, rugs) are securely fixed to the ground; modifying the night light so that it is easy to access from the bed; checking the lighting of the outdoor and indoor environment lights (rooms, corridor, bathroom, toilet, and kitchen) and outdoor paths, stairs and entrances at night, which have enough light; recommending that non-slip flooring be purchased for safe entry into the bathroom or bathtub and toilet space; installing handles on the bathroom door and beside the tub and shower; modifying the kitchen appliances for convenient and safe access; checking the railings of the internal and external stairs of the house; ensuring safe access for domestic animal care; recommending slippers and shoes that are perfectly suited to one’s feet (Mackenzie et al., 2000); removing clutter and crowding from home; checking necessary assistive devices; checking the arrangement of furniture and household items (Gitlin et al., 1999); recommending the placement of a chair in both the kitchen and bathroom; and modifying or removing the lower part of the door frame at the entrance to the bathroom or toilet. The protocol of this intervention has been approved by five faculty members of TUMS.
Assessment and tools
CDR was used to determine the severity of dementia. This test has 75 statements in 6 areas “Memory,” “Time and Spatial Orientation,” “Judgment and Problem Solving,” “Social Affairs,” “Home and Recreation,” and “Personal Affairs,” and the score of each area was determined based on answering a number of questions. Those with a score between 4.5 and 9 were considered to have mild dementia and were included in the study. CDR is one of the few tests that examine short-term and long-term memory and can be administered to literate and illiterate older adults. A study conducted by Sadeghi et al. (2012) qualitatively confirmed the face and content validity of the Persian version of this test and substantiated its reliability by calculating Cronbach’s alpha coefficient of 0.73 (Sadeghi et al., 2012).
The HOME Fall and Accident Screening Tool (HOME FAST) was used to assess falls. One and two months following the home visit, a re-evaluation was conducted with HOME FAST to follow up on the implementation of the modifications. Finally, after 3 months of the intervention, HOME FAST was used as an outcome measurement tool to determine the impact of the modifications. HOME FAST is designed as a fall screening and evaluation tool. It is primarily employed to identify older adults who live at home and are at risk of falling (Mackenzie et al., 2000). The absolute and relative correlation coefficients of the Persian version of the retest–test of this tool were 0.88 and 0.54, respectively, and the inter-examiner reliability was reported with absolute and relative correlation coefficients of 0.72 and 0.84. Its content validity is reported to be 76% (Maghfouri et al., 2013). Home FAST considers a score of 9 as an indication of a high risk of falling. The intervention should be prioritized for those with a score of 9 or higher or those with risk identified in six specific items (Mackenzie and Byles, 2018). This tool is the only tool that is valid and reliable in the Persian language and it is commonly used in all research in Iran. Two scoring styles have been proposed for the overall scoring of the CDR test. In the first style, the average scores of six areas are calculated, and based on the calculated average, a decision is made in relation to the person’s condition and level of dementia. In the second style, which was used by O’Bryant et al. in 2008, instead of using the average scores of the areas, the sum of their scores is used. He believes that the use of total scores instead of average scores is more useful than scoring in the form of average scores due to the easier calculation and reduction of the possibility of error in calculation, the wide range of scores, and the possibility of using more intervals for data interpretation and the possibility of better classification of the level of dementia (O’Bryant et al., 2008, 2010). In this study, the second style of scoring was used.
Data analysis
The Shapiro–Wilk test was used to check the normal distribution of the data. T-test and chi-square were used to detect the difference in demographic variables between the two groups. The t-test was employed to examine the differences between the control and intervention groups in terms of continuous variables. The level of statistical significance was considered p < 0.05 for all tests. The statistical analyses were conducted using Stata14 software. Since this was a blinded study, the statistical analyst was blind and unaware of how participants were allocated to groups. They were provided with coded data.
Results
As it was shown in Figure 1, in total 113 older patients with dementia were evaluated, of whom 44 met the inclusion criteria and randomly allocated into groups. Out of 69 excluded participants, 28 patients were excluded from the study due to their unwillingness to participate, and 41 patients did not meet the inclusion criteria. Four participants were lost to follow up and finally, 40 participants (intervention (n = 20) and control (n = 20)) completed the trial and were included in the analysis.
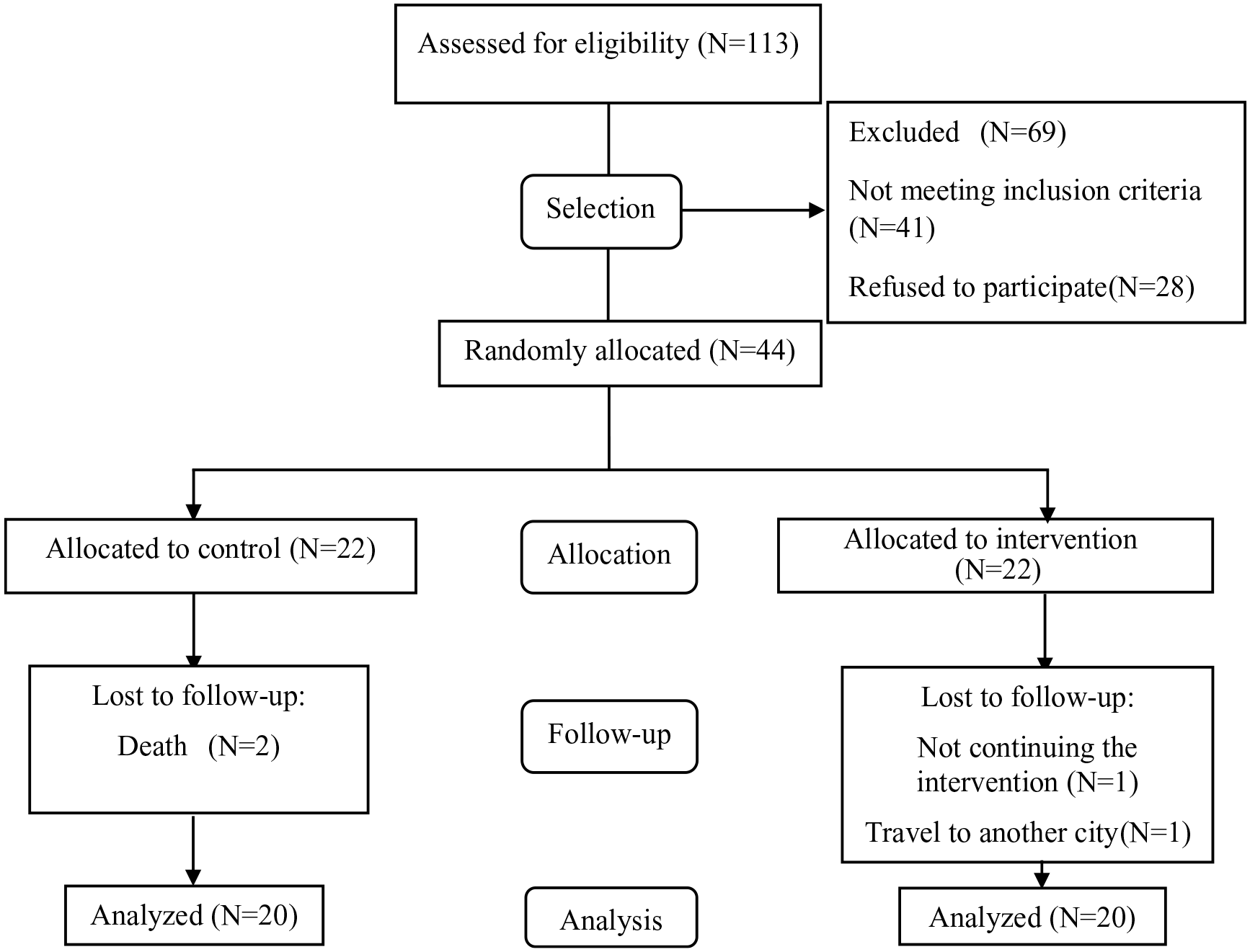
Tracking participants during the study (CONSORT chart).
Five men and 15 women were in the intervention group with a mean age of 77.6 ± 7.356, and 6 men and 14 women were in the control group with an average age of 77 ± 5.394. The p value of the independent t-test for the age and the CDR score between the intervention and control groups were p = 0.789 and p = 0.594, respectively. A chi-square test was performed between the two groups, revealing p = 0.723 for gender and p = 0.884 for the dementia types. As a result, the distribution of these variables was uniform across both groups, with no significant difference. Table 1 illustrates other demographic and clinical characteristics of the participants.
Demographic and clinical characteristics of study participants.
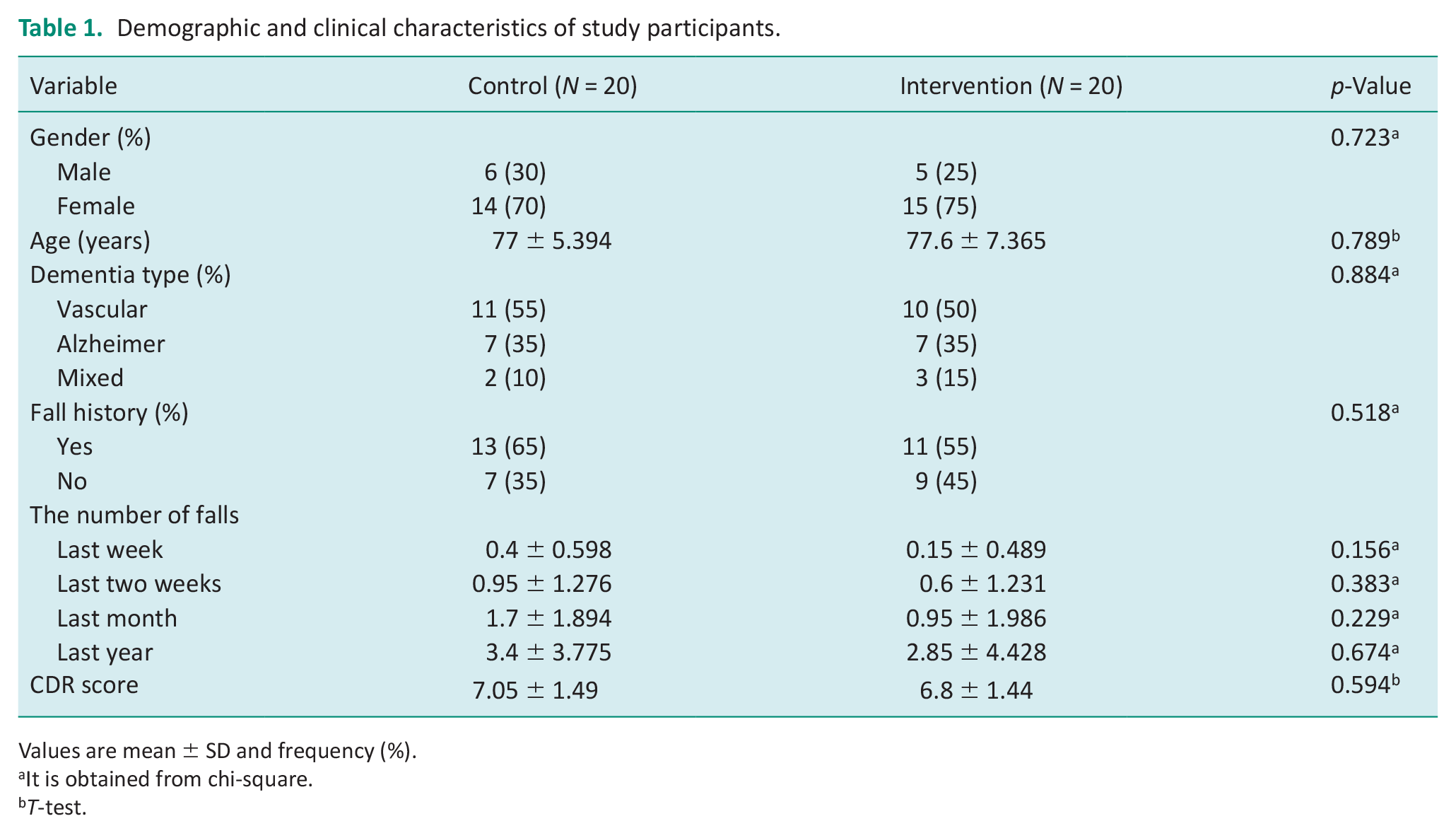
Values are mean ± SD and frequency (%).
It is obtained from chi-square.
T-test.
The frequency of each item from HOME FAST in the intervention group is given in Table 2. The tool contains 25 items (questions), and the responses for answering each question are YES, NO, and Not Applicable (N/A). A score of 0 is assigned to the YES response, a score of 1 to the NO response, and a score of 0 to the N/A response. The questions with NO response indicate that the environment does not have enough safety, the risk of falling is high, and that the environment needs to be modified. Home modification intervention included all the listed items for all 20 participants in the intervention group. In Table 2, only the information related to the intervention group was presented. The information related to the control group was not shown due to the number of NO responses for all items remained unchanged in the control group. In the intervention group, the item that needed the most modification was item 13, because all the people in this group did not have an accessible or sturdy grab rail in their shower or beside the bath. In the intervention group, the highest score change was related to item 4 and then item 13. Also, items 3, 11, 15–17, 19, 22, and 25 did not change.
The frequency of responses for each item on the HOME FAST in the intervention group.
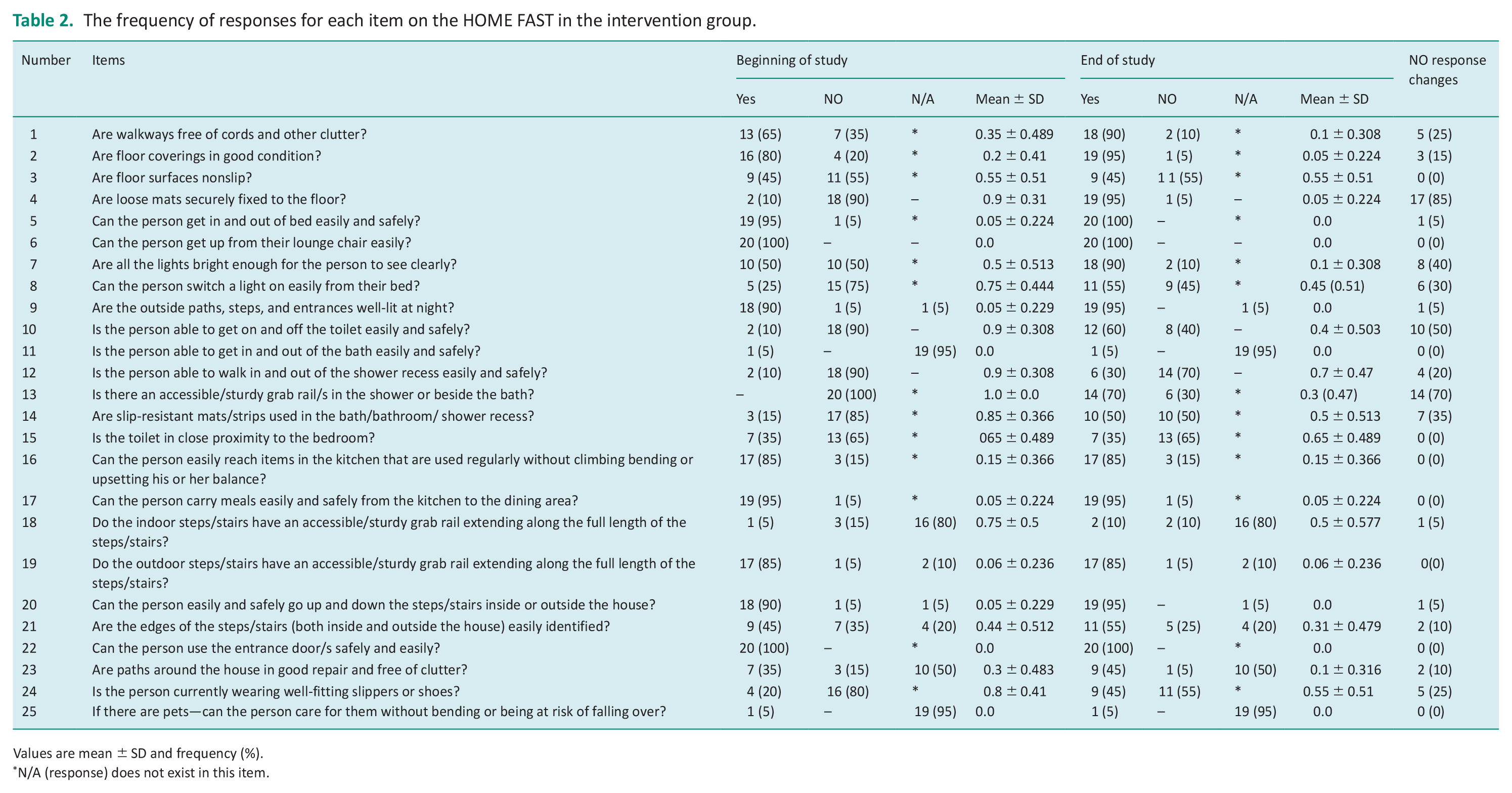
Values are mean ± SD and frequency (%).
N/A (response) does not exist in this item.
A Shapiro–Wilk test was used to investigate the normal distribution of the risk of falling data and the results showed that all data were normally distributed. The result of the two-sample t-test demonstrated that at the beginning of the study, there was no significant difference between the intervention and control groups in terms of falling risk scores (p = 0.6; Table 3). However, at the end of the study, the difference between the two groups was significant (p < 0.001). Therefore, home modifications for the intervention group reduce the risk of falling in older adults with dementia compared to the control group. The trend of changes in the fall risk score during the study is reported in Figure 2.
Comparison of fall risk scores in the intervention and control groups during the study based on HOME FAST data.
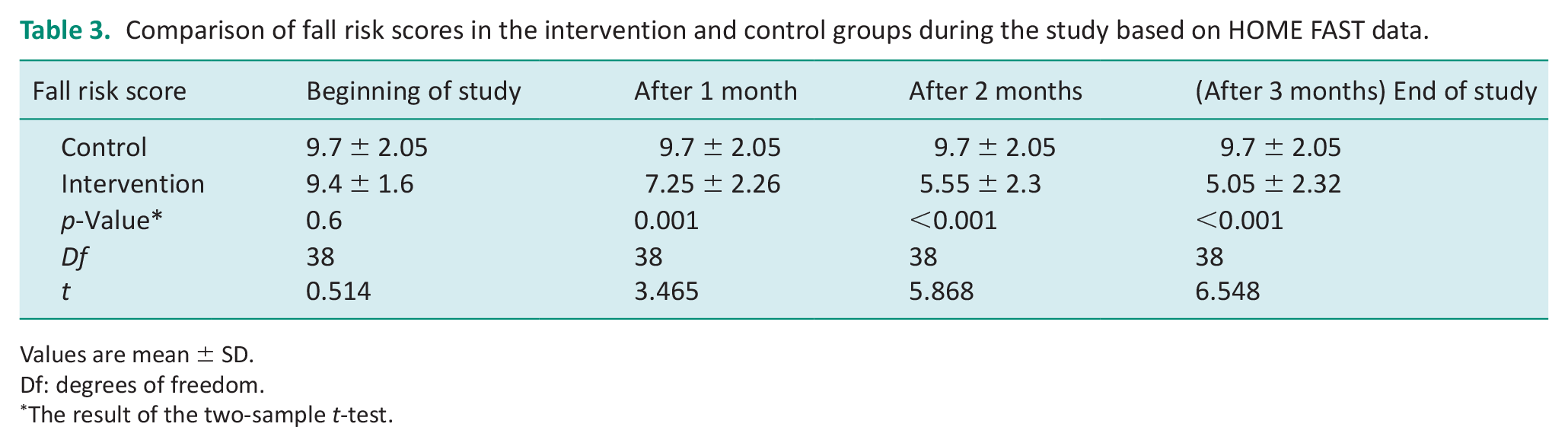
Values are mean ± SD.
Df: degrees of freedom.
The result of the two-sample t-test.
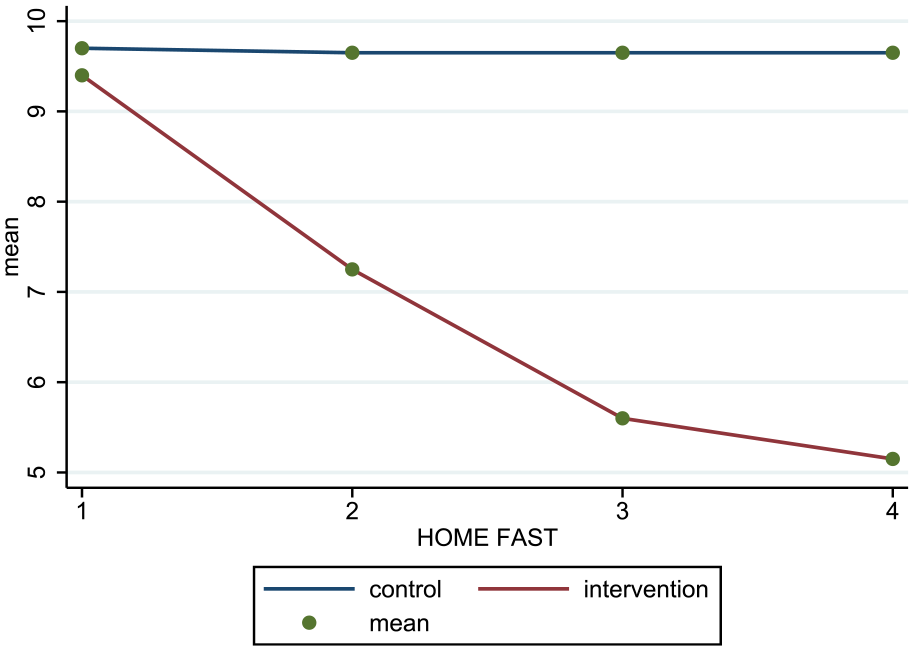
The trend of changes in the score of HOME FAST during the study in each group.
A paired t-test was used to investigate the effect of home modifications on the risk of falling at the beginning of the study and 3 months later in each group. The results are displayed in Table 4. The average fall risk score for the intervention group was 9.4 at the beginning of the study. It reached 5.05 3 months after the intervention. The decrease in score indicates that the risk of falling into the intervention group has decreased after implementing home modifications. The results of the paired t-test demonstrate that this decrease was significant (p < 0.001). The average fall risk score in the control group was 9.7 at the beginning of the study and remained unchanged after 3 months. Furthermore, the result of the paired t-test was not significant (p = 0.32).
Comparison of fall risk scores during the study in each group based on HOME FAST data.
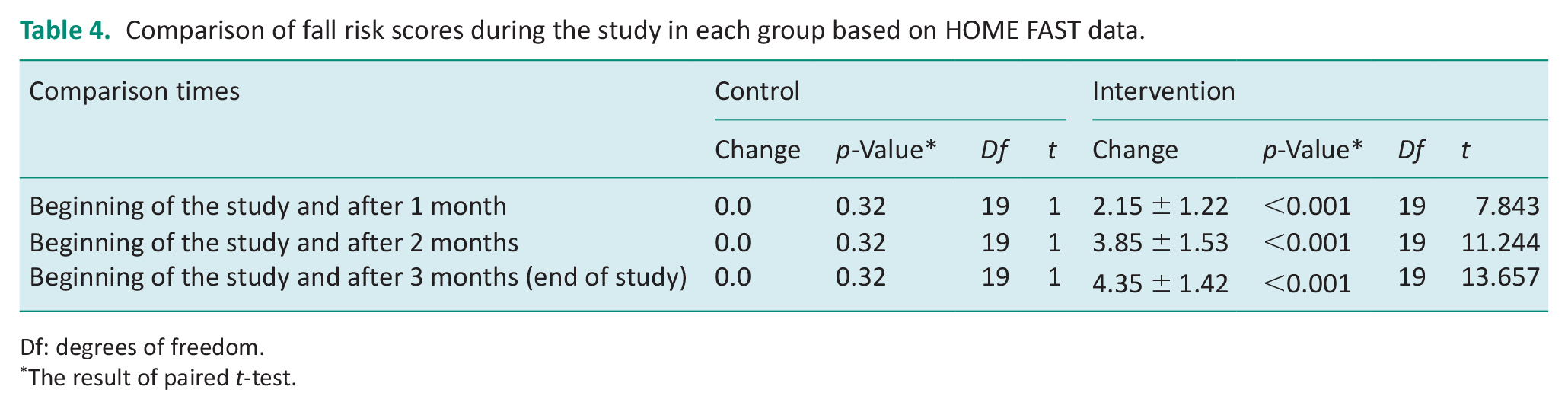
Df: degrees of freedom.
The result of paired t-test.
Discussion
Consequently, the present study examined the effectiveness of modifying the home environment on falls in older adults with dementia. Studies have reported that the most dangerous places to fall are the stairs in the building (Amiri et al., 2013) and the bathroom and toilet inside the house (Salarvand and Birjandi, 2009). Eighty-two percent of older people have had a history of falling at home. Bathrooms (19.6%), toilets (18%), bedrooms (18%), and living rooms (16%) are the most common places where falls occur (Na’emani et al., 2019). The present study incorporated these environments as part of its intervention program and carried out modifications in them. In HOME FAST, the items related to stairs are 18–21, bathroom 11–14, toilet 10, 14, 15, and bedroom 5. Table 2 summarizes NO response changes for each item which shows the effect of modification on each item. A decrease in the number of NO responses indicates a reduction in the risk of falling in these environments. Physical factors contributing to falls include poor ambient lighting and floors with slippery surfaces (Pahlevanian et al., 2020). There are modifications for brightness and slippery surfaces in the current study, which is indicated by the NO response changes in items 1–4 and 7–9. The interventions appear to have successfully identified physical risk factors for falling. Modifying them can reduce the risk of falling among older adults with dementia. Inappropriate socks, shoes, pajamas, or long pants have been identified as possible causes of falling (Salarvand and Birjandi, 2009; Schwartz et al., 2002). Among the interventions implemented in the current study was the prescription and recommendation of appropriate shoes or slippers. For those individuals for whom this modification has been implemented, there are fewer NO responses related to this item. The highest score change in HOME FAST was related to item 4 and then item 13. Accordingly, home modifications have had the greatest impact on floor coverings and accessible grab rails in the shower or beside the bath, resulting in a change in score in these two items.
The results of the present study demonstrated that modifying the home environment reduces the risk of falling in older people with dementia. Gitlin et al. (2006) examined the effects of modifying the environment and behavioral factors on community-dwelling older adults with functional impairments. They concluded that modifications reduced the risk of falling and household hazards (Gitlin et al., 2006). Their findings align with the present study. However, the present study did not implement modification for behavioral factors as an intervention. A study by Yeni et al. (2022) investigated the effect of home modification interventions led by nurses on family members of older adults with dementia living at home. The results showed that home modification interventions for older people with dementia reduce the number of falls (Yeni and Yilmaz, 2022). Similar to the present study, they found that home environment modifications led to fewer falls. Yeni et al.’s study was conducted under a nurse’s leadership which involved home modification interventions. In this study, however, home modification interventions were implemented by a trained occupational therapist. Moreover, their effect was assessed only on older people with dementia, not their family members. A study conducted in 2011 by Pighills et al. demonstrated that the evaluation and modification of the home environment to prevent falls in older adults does not affect the fear of falling 1 year after the evaluation. An occupational therapist’s evaluation of the home environment significantly reduced the rate of falls among people at risk, whereas its administration by a trained evaluator did not (Pighills et al., 2011). According to Cumming et al. (1999), home visits by an occupational therapist to a house exposed to environmental hazards and facilitating home modifications can reduce the risk of falling (Cumming et al., 1999). In a 2018 study by Maggi et al., it was demonstrated that modifying the home environment by an occupational therapist minimized the risk of falling among older adults (Maggi et al., 2018). Their findings are consistent with the present study demonstrating that modifications of the home environment implemented by the occupational therapist reduce the risk of falling in older adults. The results of the present study were consistent with the results of the above studies.
The causes of falls in older people are divided into two categories: internal and external factors. Internal factors include weakness of lower limb muscles, decreased balance, reduced mental ability, decreased sensory information, and slow motor response. External factors consist of using sleeping pills, environmental conditions such as low lighting in traffic areas, uneven surfaces, mobility of the support surface, slipping, and the presence of cumbersome tools and equipment on the commuting route (Park, 2017). The “multifactorial falls risk” framework considers the risk of a person falling as a consequence of the interaction of three factors, mobility, behavior, and physical environment (Clemson et al., 2004). In this conceptual framework, mobility refers to a person’s ability to perform movements, and risky behavior is defined as behaviors that increase the possibility of adverse physical consequences, such as falling. Poorly designed stairs, uneven ground, slippery surfaces, fall hazards, a lack of lighting, and a lack of handrails or grabrails are examples of unsafe physical environments. On the other hand, a safe environment poses no or minimal environmental risks and supports people with varying levels of mobility (Feldman and Chaudhury, 2008). As outlined in the multifactorial fall risk framework, the physical environment is one of the risk factors for falls, while environmental conditions are external factors. A significant relationship exists between the increased risk of falling and the home environment. The home environment is one of the physical environments playing an essential role in the risk of falling. It seems that by modifying and reforming the home environment, it is possible to make it safer and ultimately reduce the risk of falling.
In this study, one limitation was that it was conducted amid COVID-19 outbreaks and lockdown conditions, which made accessing older patients, collecting samples, and conducting home visits challenging. As another limitation of the study, only individuals with mild dementia could participate, whereas other stages of dementia were considered. Since dementia is progressive, strategies such as home modifications may need to be performed at higher levels and on a different scale during more advanced stages of the disease. As a result, the modifications for mild dementia differ from those for other severities of dementia. Future studies should examine older adults with other stages of dementia and under post-pandemic conditions of COVID-19 and compare their results with those presented in the present study.
Key findings
Item 13 needed the most modification because all the people in the intervention group did not have an accessible or sturdy grab rail in their shower or beside the bath.
The highest score change in the HOME FAST tool was related to item 4, which indicates that modifications have had the most impact on floor coverings.
Modifications by applying changes and reforms to the home environment reduced the risk of falling in older adults with dementia.
What the study has added
This study confirms the effect of home modifications on the risk of falling in older adults with dementia and emphasizes the importance of using it as a complementary intervention to other rehabilitation services.
Footnotes
Research ethics
The ethics committee of Tehran University of Medical Sciences confirmed the study procedure and the ethics code (Ethic number: IR.TUMS.FNM.REC.1399.163).
Consent
All participants signed an informed consent before entering the study.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
The authors’ responsibilities were as follows: HS and HD: contributed to the conception, design, and drafting of the manuscript; AA-H: contributed to the statistical analysis; HS, ANS, and ZV: contributed to data collection; and HS: contributed to the interpretation of the data and had primary responsibility for final content. All authors read and approved the final version of the manuscript.
Registration code for RCT
This study was registered on 2021-05-31 in the Iranian Registry of Clinical Trials (IRCT) with the code IRCT20210106049950N1. The participants voluntarily participated in this research, provided their verbal and written consent, and were free to withdraw at any time.