
Abstract
Introduction:
The hospital environment can exacerbate symptoms of delirium; as such there is a move to promote early supported discharge for patients with delirium. However, the occupational therapy role and impact of intervention is not well known. Our study evaluated an occupational therapy delirium pathway facilitating early assessment, intervention and supported discharge to home compared with hospital-based care.
Method:
A before and after, observational study design. Data was collected regarding hospital use, patient function (Functional Independence Measure/Functional Assessment Measure) and the carer experience (Preparedness for Caregiving Scale).
Results:
Ninety patients (43 control and 47 intervention group patients) were recruited with a mean patient age of 82.8 years (SD 7.6). There was a significant difference in hospital re-presentations (n = 3 in the intervention group compared to n = 10 in the control group (p = 0.026)). Hospital length of stay did not significantly differ between the groups (p = 0.534). The mean score for the Preparedness for Caregiving Scale was 3.3 indicating that most carers felt ‘pretty well prepared’. However, patients continued to experience significant functional decline (p = 0.006).
Conclusion:
An occupational therapy delirium pathway reduced hospital re-presentations and could be implemented in clinical practice to better support patients recovering from delirium as they transition from hospital to home.
Introduction
Delirium is an acute cognitive impairment accompanied by fluctuating mental status, inattention and disorganised thought (Australian Commission on Safety and Quality in Health Care [ACSQHC], 2016; The National Institute for Health and Care Excellence [NICE], 2023). It is a significant clinical problem with a prevalence of 23% in acute hospital settings (Aung Thein et al., 2020; Bauernfreund et al., 2018). The hospital environment can exacerbate symptoms of delirium, leading to increased agitation, confusion, and disorientation (Chia et al., 2020). In more recent years, a hospital-in-the-home (HITH) model and early supported discharge has been proposed to replace extended hospital stays and promote early resolution of delirium symptoms (Chia et al., 2020). In this model, patients diagnosed with delirium are identified in hospital and as soon as they are medically stable, they are discharged into care at home earlier than the traditional hospital-based care for treating delirium (Chia et al., 2020).
Previous studies have found that carers were supportive of this model of care (Eeles et al., 2016) and that hospital length of stay (LOS) was reduced (Chia et al., 2020). A systematic review completed in 2021 identified the most effective single-component intervention to reduce delirium incidence was a HITH intervention (risk ratio = 0.29, 95% CI: 0.09–0.87) (Ukwuoma Ekeozor et al., 2021). Current evidence is supportive of discharging patients as early as possible to minimise the effects of the hospital environment for medically stable patients who have delirium (Chia et al., 2020; Eeles et al., 2016; Isaia et al., 2009). Early discharge programs are in demand to accommodate the increasing pressures on acute health services.
Occupational therapists assist patients with delirium through early assessment and identification of a change in a patient’s baseline cognitive function, facilitation of non-pharmacological interventions, discharge planning and supported post-discharge follow-up (Pozzi et al., 2020a; Strecker and Hitch, 2021; Tobar et al., 2017). Occupational therapy delirium management strategies have included cognitive stimulation and orientation, maintenance of functional independence, education of family or carer, bed and seating positioning, sleep hygiene, and modifying the physical environment with assistive equipment (Pozzi et al., 2020a). Previous occupational therapy studies have focused on the therapist role in different settings including intensive care units, (Álvarez et al., 2017; Tobar et al., 2017) rehabilitation (Pozzi et al., 2020a) and nursing homes (Pozzi et al., 2020b). Occupational therapy has been found to be effective in decreasing duration, incidence of delirium and improving discharge function for non-ventilated older patients in intensive care (Pozzi et al., 2020a).
The HITH model of delirium care is a potential alternative to the traditional hospital route for patients with delirium (Caplan, 2008), but further research is needed to ascertain effectiveness of interventions including occupational therapy (Pozzi et al., 2023). No other reviews have focused on occupational therapy as a single intervention, although occupational therapy services have been provided as part of other multidisciplinary post-discharge programs (Chia et al., 2020; Eeles et al., 2016). Chia et al. (2020) described a multidisciplinary HITH delirium pathway compared with hospital-based care. This included occupational therapy once per day post discharge. Eeles et al. (2016) also evaluated a supported discharge program utilising HITH. This included occupational therapy intervention consisting of a daily home safety and equipment check for 16 patients. The duration of these programs post discharge was approximately 4–5 days until patients were delirium-free. These programs did not explore services provided across the continuum of care from hospital to home.
Overall, the study purpose was to describe and evaluate an occupational therapy pathway supporting the facilitation of early assessment, intervention and supported follow-up for patients with delirium transitioning from the acute hospital setting to the home environment. The pathway commenced in the acute setting and continued into the home environment, providing rehabilitation and increasing safety post discharge. This research explored the benefits of occupational therapy for patients with delirium and elucidated details of optimal timing, dosage and intensity of intervention required to add value as patients move from acute care to home. Additionally, this research evaluated the impact of early discharge on carers and explored the needs of subgroups such as patients with dementia. It was hypothesised that pathway care would decrease hospital LOS and reduce re-presentations after discharge.
Method
Study design
This study utilised a before and after, observational quasi-experimental study design to examine the impact of an occupational therapy delirium pathway. The primary aim of the study was to evaluate the safety (hospital re-presentations and readmissions within 1 month of discharge) and efficiency (hospital LOS) of the occupational therapy delirium pathway compared with hospital-based usual care. Patients who received usual care were not provided with pathway care and did not receive a post-discharge occupational therapy home visit. Feedback regarding the service provided as part of the intervention was sought from carers. The secondary aim was to describe the pathway and its impact on a patient’s function and carer experience. Reporting adhered to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement for observational studies (Von Elm et al., 2008).
Setting and timeframes
The program was evaluated within a tertiary-level acute hospital in a metropolitan setting throughout 2019 and 2021. Retrospective data was collected for the control group from medical records and Allied Health System. Control group patients received occupational therapy between January and August 2019. They were provided with usual care and did not receive a post-discharge home visit. An occupational therapy delirium pathway was introduced in June 2020 and consecutive patients who received this service were recruited between June 2020 and April 2021. Patients were followed up for 1 month post hospital discharge.
Participants
The inclusion criteria consisted of patients with a diagnosis of delirium who were admitted to hospital. Patients on any hospital ward were eligible, that is, general medical, general surgical and geriatric wards. Patients were expected to return to community-dwelling post discharge with carer support and may or may not have had a pre-existing cognitive impairment. The diagnosis of delirium was confirmed based on initial delirium screening and consultant physician or geriatrician assessment. Patients with delirium were eligible for pathway care if they lived in their own home with a functionally capable care-giver available to provide 24 h support for a period of at least 2 weeks. They needed to have a reversible/identifiable delirium trigger addressed with treatment and were medically stable. Patients were excluded if they were medically unstable, from a residential care facility or at a palliative phase of care or did not have a suitable live-in carer for early discharge. Patients were recruited by a treating ward-based senior occupational therapist in the acute setting.
Control group
The control group received usual care following hospital guidelines for delirium management. All hospital inpatients received ward-based occupational therapy who provided intervention strategies including initial and functional assessments, inpatient rehabilitation including delirium management strategies such as orientation, optimising the physical environment, cognitive stimulation, equipment prescription and providing patient and carer education. Patients were not identified for early supported discharge and did not receive a home visit post discharge. The retrospective data for control patients meeting the inclusion criteria (n = 43) were extracted from a clinical database of 94 patients.
Intervention
The intervention consisted of an occupational therapy delirium pathway involving two phases; hospital ward-based intervention and a home visiting follow-up service (Table 1). The intervention was developed following a screen of the literature. This literature review identified five articles outlining non-pharmacological interventions delivered by occupational therapists completed in the hospital and/or home setting that reduced hospital LOS in patients with delirium, promoted early hospital discharge and recovery (Angel et al., 2016; Chia et al., 2020; Chong et al., 2014; Lundström et al., 2005; McKenzie and Joy, 2020).
Occupational therapy delirium pathway.
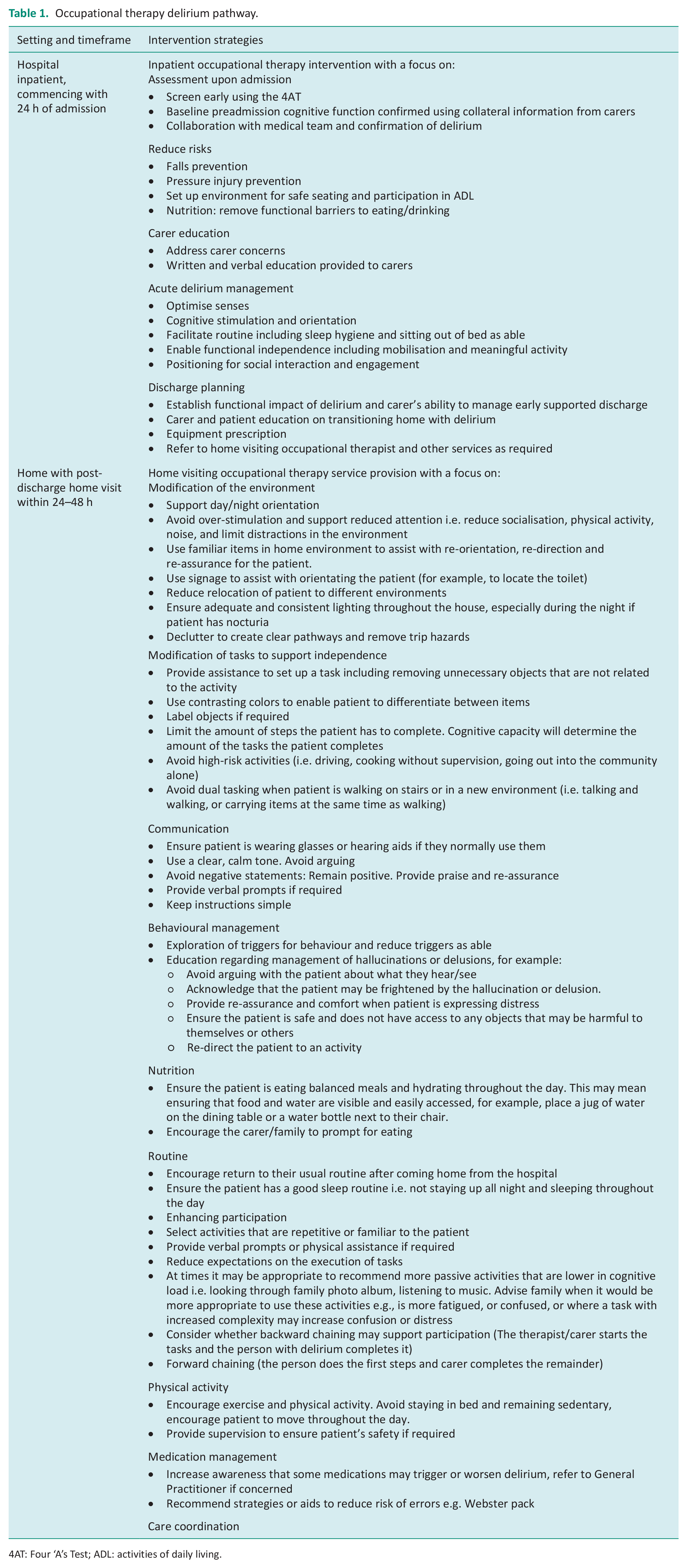
4AT: Four ‘A’s Test; ADL: activities of daily living.
All hospital inpatients continued to receive usual care including assessments and inpatient rehabilitation as outlined above. Assessment was enhanced with the introduction of the Four ‘A’s Test (4AT) (Bellelli et al., 2014). Additionally, functional and cognitive ability was measured with a modified Functional Independence Measure/Functional Assessment Measure (FIM/FAM) (Cournan, 2011; Hall et al., 1993; Harper et al., 2017).
Hospital education for carers was formalised. It included written and verbal education explaining delirium, causation factors, what to expect post discharge, signs of worsening delirium, i.e. increasing confusion, personality changes including agitation/aggression, anxiety or fearlessness and changes in alertness. It provided strategies for carers to support patients post discharge including communication tips, home safety, regaining routine, mobilisation and nutrition.
Post-discharge occupational therapy consultation was provided via the telephone within 24–48 h of discharge with a home visit scheduled as required within that time frame. A home visiting toolkit was developed to support treatment fidelity post discharge. Two senior occupational therapists were involved in the provision of intervention. Overall the service included an initial telephone screen, between one to three post-discharge home visits as clinically indicated, and between one to two follow-up telephone calls. Delirium resolution was based on patient and carer report regarding acuity of confusion and functional impact. The home visiting intervention had the following aims:
Management of safety and falls risks as a result of increased confusion or challenging behaviours
Providing education and strategies to build capacity in carers
Avoidance of patient functional decline
Prevention of hospital readmission
Home visiting intervention strategies addressed the following factors including communication, behaviour management, nutrition, routine, enhancing participation, physical activity, identifying the need for further medical management, environmental modification, task modification and care coordination. Upon discharge from occupational therapy, if required, patients may have been referred onto other services including the memory clinic, Rehabilitation in the Home (RITH) or for home care services.
Outcome measures
Patient-descriptive measures including primary diagnosis were recorded by the ward-based occupational therapist. Demographic data was collected upon hospital admission and included gender, age, living situation and home care service use. The Clinical Frailty Scale (CFS) (Rockwood et al., 2005) and the Charlson Comorbidity Index (CCI) (Charlson et al., 1987) were used as summative health measures. The 4AT (Bellelli et al., 2014) was utilised as a delirium screening measure and baseline cognitive characteristics were noted including a previous diagnosis of dementia.
The FIM/FAM (Cournan, 2011; Hall et al., 1993; Harper et al., 2017) determined functional and cognitive ability at three time points; hospital admission (pre-admission function), at hospital discharge and upon discharge from the home visiting service. This consisted of 13 items measuring cognition, activities of daily living (ADLs), transfers, and locomotion, each scored from complete dependence (1) to complete independence (7). A total score out of 91 was calculated indicative of burden of care. A lower score indicated a higher burden of care. All occupational therapists involved in scoring the FIM/FAM were provided with training to ensure competence and reliability.
Carers were invited to complete the Caregivers Preparedness for Caregiving Scale (Archbold et al., 1990) at patient discharge from hospital and at discharge from the occupational therapy home visiting service. Caregivers of patients with delirium provide practical and medical caregiving, support the patient emotionally and socially, as well as maintaining household chores (Alvariza et al., 2020). Carers were defined as any relative, friend, or family caregiver who had a significant relationship with, and provided any assistance to the patient (Alvariza et al., 2020). Preparedness for caregiving refers to how ready the caregivers perceive they are for the tasks related to the caregiving role, such as providing physical and emotional support and dealing with the stress of caregiving (Alvariza et al., 2020). This tool included eight questions with an associated scale of 0–4 where carers could indicate if they were ‘not at all prepared’ (0) to ‘very well prepared’ (4). Carers were also asked ‘is there anything specific you would like to be better prepared for?’
The primary outcome was the number of hospital re-presentations 1 month post discharge home. Secondary outcomes included time to readmission, hospital LOS, inpatient and home visiting occupational therapy treatment time, characteristics of treatment provided and the patient’s FIM/FAM. This data was extracted from local hospital computer systems by a research assistant blinded to group allocation.
As this was an observational study, a formal calculation was not appropriate as definitive effectiveness was not being assessed (Lancaster et al., 2004). Instead, a pragmatic sample size of n = 86 was adequate to estimate our quantitative outcomes dependent on data availability.
Statistical analysis
Summary descriptives include means and standard deviations or medians and interquartile ranges (IQR) for continuous data and frequency distributions for categorical data. The Kolmogorov-Smirnov test was used to assess continuous data for normality. Comparisons between groups for outcomes including hospital re-presentations and admissions utilised Mann-Whitney U tests or Chi squared tests for continuous and categorical data respectively. Kaplan-Meier survival curves were used to examine time to readmission, with groups compared using log rank tests. Paired t-tests were used to evaluate changes in the FIM/FAM score for the intervention group. All hypotheses were 2-sided and p-values <0.05 were considered significant. Stata version 17.0 (StataCorp, College Station, TX, USA) was used for data analysis.
Ethical considerations
This project underwent review and was assessed as of negligible risk (QA33952) by the Sir Charles Gairdner Osborne Park Health Care Group. Patients and their carers who participated in the intervention group provided verbal consent in line with approval. Consent was waived for the control group data which was extracted retrospectively. All data was deidentified and analysed in aggregate form.
Results
Overall 90 patients were recruited into the study consisting of 43 control and 47 intervention group patients. All prospective eligible patients in the intervention group were included during the recruitment timeframe. Follow-up data was available for all patients at 1 month post discharge from hospital, with no patients lost to follow-up.
The mean patient age was 82.8 years (SD 7.6) with 48% (n = 43) male. Sixty five percent (n = 59) of patients had delirium on admission with 27% (n = 24) of patients having a previous diagnosis of dementia. The mean CCI was 5.4 (SD 1.3). Thirty one percent (n = 28) of patients lived alone with 42% (n = 38) previously receiving formal in-home care services. Patient descriptors are outlined in Table 2 with no significant differences between the groups identified. Patients had an overall median hospital LOS of 8.5 days (IQR 4, 14). This did not significantly differ between the groups with a median of 7 days in the intervention group compared to 8 days in the control group (p = 0.534) (Table 3).
Baseline characteristics of occupational therapy delirium pathway intervention group compared to usual care controls.
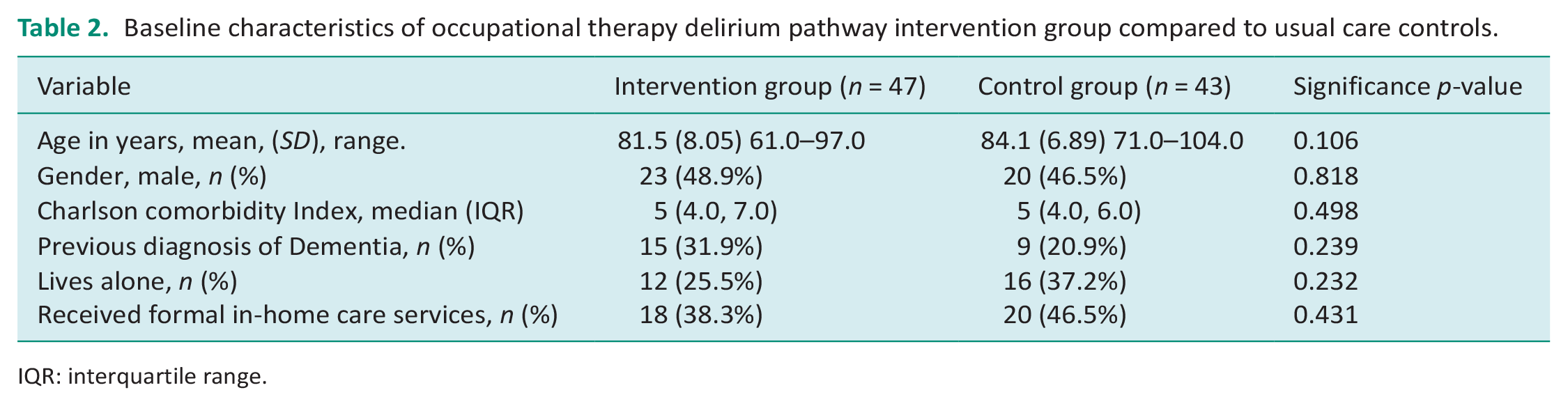
IQR: interquartile range.
Primary outcomes for the occupational therapy delirium pathway intervention group compared to usual care controls.
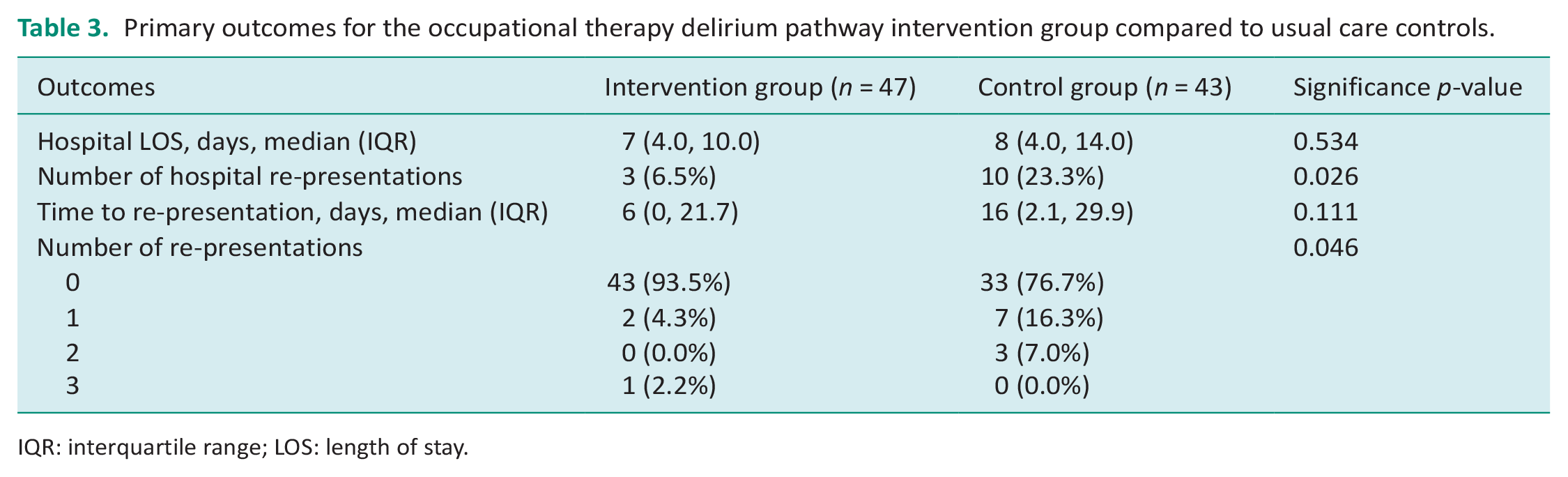
IQR: interquartile range; LOS: length of stay.
For the primary outcome there was a significant difference in hospital re-presentations. Three (6.5%) patients in the intervention group re-presented to hospital compared to 10 (23.3%) in the control group (p = 0.026). Three patients in the control group had more than one re-presentation compared to one in the control group (p = 0.046). There were four hospital delirium-related admissions in the intervention group and nine in the control group (p = 0.094). The median time to readmission was 6 days in the intervention group compared to 16 days in the control group (p = 0.111) (Supplemental Data, Figure 1). No significant factors were associated with hospital re-presentations including age (p = 0.293), previous diagnosis of dementia (p = 0.732), hospital LOS (p = 0.622), gender (p = 0.603), living status (p = 0.954) or preadmission function (p = 0.882).
The intervention group had a mean CFS of 5.5 (SD 1.1) indicating most patients had mild frailty and a 4AT score of 5.9 (SD 2.0) at initial assessment. Thirty four percent (n = 11) had fallen in the past 12 months. Inpatient occupational therapists spent a mean 292.0 min with patients (SD 258.2) diagnosed with delirium. This was not significantly different from the control group where patients received a mean of 298.0 min (SD 266.3) of inpatient therapy time (p = 0.915). Patients in the intervention group received an initial assessment (n = 44, 95.7%), functional assessments (n = 43, 93.5%), cognitive assessments (n = 30, 65.2%) and cognitive rehabilitation (n = 10, 21.7%) in the hospital setting.
Twenty one carers completed the Preparedness for Caregiving Scale (Archbold et al., 1990) upon hospital discharge. The majority of carers had a tertiary education (9.5% primary school education, 42.8% secondary school education and 47.6% tertiary education). The mean score for the Preparedness for Caregiving Scale was 3.3 indicating that the majority of carers felt ‘pretty well prepared’ at the time of patient discharge from inpatient hospital care. Qualitative comments from carers prior to patient discharge home included concerns about managing at night time, what to do if the patient deteriorates, how to track fluid/food intake and one carer reported that ‘more notice for discharge home was required’. The mean score for the Preparedness for Caregiving Scale remained stable at discharge from the occupational therapy home visiting service at 3.3 (SD 0.6).
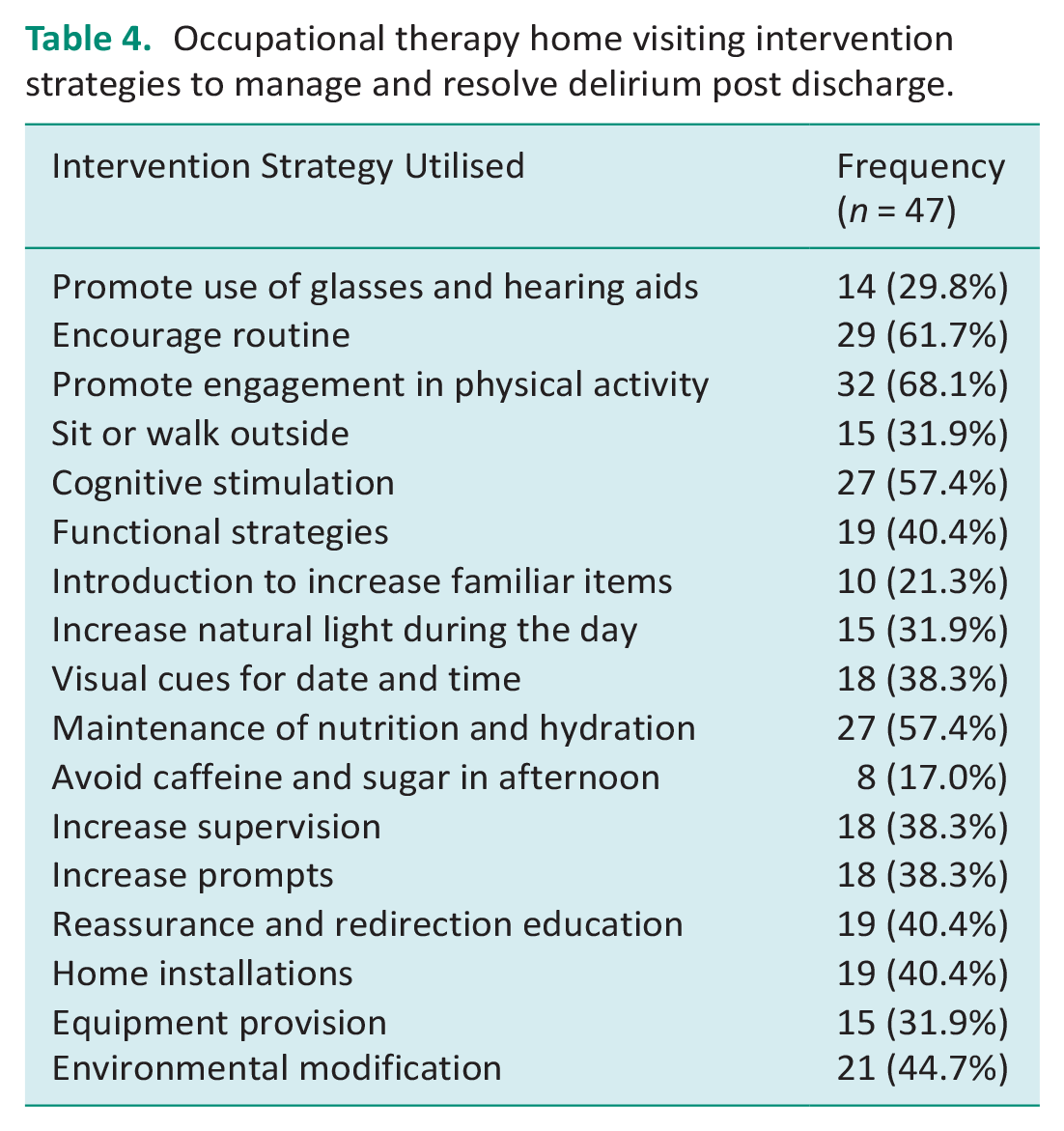
Patients received a median of 1 home visit and 2 telephone calls post discharge. The mean time spent with patients was 202.3 min at home. All patients received a home assessment and a variety of intervention strategies to support delirium reduction and resolution as per Table 4.
Occupational therapy home visiting intervention strategies to manage and resolve delirium post discharge.
The mean preadmission FIM/FAM was 64.2 (SD 17.3) which significantly dropped to 50.3 (SD 17.9) for patients with delirium assessed on the inpatient wards (p < 0.001). At discharge from the occupational therapy home visiting service the post-discharge FIM/FAM was 58.8 (SD 20.3) indicating that patients were continuing to experience a significant functional decline of 5.4 point from their original baseline measure (p = 0.006). On discharge from the occupational therapy home visiting service, 42% (n = 20) of patients in the intervention group received further referrals e.g. referral for home care services (n = 5) and referral to the day hospital memory clinic (n = 7).
Discussion and implications
This study has explored the impact of an occupational therapy delirium pathway to facilitate early assessment, intervention and supported discharge along a continuum of care from hospital to home. Pathway care did not result in earlier discharge from hospital; however, it significantly reduced hospital re-presentations.
In previous studies in the intervention groups, Chia et al. (2020) reported higher rates of 1 month re-presentations with 30% requiring readmission compared to 25% in the study by Eeles et al. (2016), and 6% in our study. Patients in these studies (10, 14) were slightly older and had higher levels of frailty (mean CFS of 6.0 compared to 5.5) and comorbidity (mean CCI of 6.0 compared to 5.4) with higher levels of premorbid dementia (Chia et al., 2020). Overall, the readmission rate in our study was substantially lower than others reported in the literature (Kennedy et al., 2014). Although patients in the intervention group did return to hospital earlier than those in the control group, possibly due to the receipt of regular health care input and earlier identification of need.
Hospital LOS was similar to others reported in the literature with patients in our intervention group staying a median of 7 days. Chia et al. (2020) reported a hospital LOS of 8 days in their intervention group and Eeles et al. (2016) reporting 10.8 days. Other research has highlighted that teams that focus on early supported discharge can reduce hospital LOS, reduce health care use post discharge and associated costs. In New Zealand, a supported discharge group’s costs were calculated at a mean NZ$10,836 (SD NZ$12,087) compared to NZ$16,943 (SD NZ$22,303) for usual care (Parsons et al., 2018). Pathway care with a focus on early supported discharge and a continuum of care from hospital to home could provide an effective means of discharging older people home earlier from hospital and can make a cost-effective contribution to managing increasing demand for hospital beds (Parsons et al., 2018).
This study has also highlighted the impact delirium has on a patient’s function from pre-admission to post-discharge. Functional decline was evident at discharge from the occupational therapy home visiting service with delirium resolution. Previous research has highlighted that partial and no recovery from delirium after hospital discharge can predict adverse events, including health care use and death, during the following 3 months (Cole et al., 2016; Elsamadicy et al., 2017). Delirium incidence is associated with future cognitive decline including an increased risk of dementia diagnosis (Bickel et al., 2008). At 6 month follow-up, mortality has been found to be significantly higher among patients who experienced delirium (Isaia et al., 2009). Moreover, patients have higher institutionalisation rates (Isaia et al., 2009). Future research would benefit from exploring functional changes in groups managed solely in hospital compared to those who received pathway care. Longer term functional and cognitive measurements would also be recommended.
Previous research has identified that caregiver involvement in providing interventions to patients with delirium in hospital reduces hospital LOS and may reduce duration of delirium (McKenzie and Joy, 2020). Caregiver involvement may also reduce family anxiety, can be provided relatively easily and has been deemed an acceptable mode of intervention by carers and staff (Eeles et al., 2016; McKenzie and Joy, 2020). McKenzie and Joy (2020) found that families reported increased confidence at home if involved in delirium management while patients were in hospital. Likewise to previous research, carers involved in this study were satisfied with the services provided and reported that they were prepared to support patients with delirium when transitioned to home.
The pathway promoted linkage between ward and home visiting staff with review of services provided at each stage reducing replication and ensuring a value add. Further research would benefit from engaging with consumers and therapists to determine where and when intervention adds value. Patients were provided with approximately 5 h of inpatient therapy and 3 h of therapy at home. Previous research (n = 400) has explored the use of enhanced occupational therapy discharge planning intervention that involved pre- and post-discharge home visits, goal setting, and follow-up (the HOME program) for older adults receiving acute care (Clemson et al., 2016). This resulted in twice as many occupational therapy recommendations as the in-hospital only consultation, but did not increase participation in ADL or participation in life tasks than in-hospital consultation alone (Clemson et al., 2016). It was not recommended that home visits be conducted routinely for all acutely hospitalised medical patients (Clemson et al., 2016). However, our research has demonstrated that for certain population groups, including patients with delirium, pathway care with supportive post-discharge follow-up may be beneficial.
There were only 15 patients with a previous diagnosis of dementia in the intervention group, with re-presentations not associated with a pre-existing diagnosis of dementia. As such we are unable to determine if this subgroup would be more likely to benefit from pathway care. Future research could identify target populations and also a cost analysis would be beneficial to review the cost benefits from the provision of this service.
Limitations
This was a non-randomised before and after study with several limitations including a single-centre design with control data collected retrospectively. Future research could consider a larger sample size and adverse events such as falls could be recorded. As the control group data was extracted retrospectively we were unable to determine the FIM/FAM for this group which would clarify functional changes in future research. Treating therapists completed outcome measures including the FIM/FAM and the Carer’s Preparation Scale. Primary outcomes including re-presentations and hospital LOS were extracted by a blinded research assistant. Only a subset of carers agreed to complete the Preparedness of Caregiving Scale at hospital discharge (n = 21) and at discharge from the home visiting service (n = 10) which could impact on the strength and generalisability of these results.
Conclusion
This study provides initial evidence of the benefit of using an occupational therapy delirium pathway for the management of patients with delirium when transitioning from acute hospital care to the home environment. This resulted in reduced hospital re-presentations in the following month post discharge. Carers reported feeling prepared and were satisfied with the service provided. Functional decline in older adults with delirium requires identification with risk factors addressed in order to return patients to pre-admission levels of function.
Key findings
An occupational therapy delirium pathway reduced hospital re-presentations after discharge.
Patients with delirium experience functional decline and require ongoing management strategies.
A delirium pathway did not increase inpatient therapy time, however requires outpatient resources.
What the study has added
An occupational therapy delirium pathway has been described and provides early intervention and care transition support reducing hospital re-presentations.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226231197010 – Supplemental material for An occupational therapy delirium pathway reduces hospital re-presentations in older adults with delirium: A before and after observational study
Supplemental material, sj-docx-1-bjo-10.1177_03080226231197010 for An occupational therapy delirium pathway reduces hospital re-presentations in older adults with delirium: A before and after observational study by Kristie J Harper, Kelly McAuliffe, Melinda Williamson, Angela Jacques, Kathryn Sainsbury and Deborah Edwards in British Journal of Occupational Therapy
Supplemental Material
sj-docx-2-bjo-10.1177_03080226231197010 – Supplemental material for An occupational therapy delirium pathway reduces hospital re-presentations in older adults with delirium: A before and after observational study
Supplemental material, sj-docx-2-bjo-10.1177_03080226231197010 for An occupational therapy delirium pathway reduces hospital re-presentations in older adults with delirium: A before and after observational study by Kristie J Harper, Kelly McAuliffe, Melinda Williamson, Angela Jacques, Kathryn Sainsbury and Deborah Edwards in British Journal of Occupational Therapy
Footnotes
Acknowledgements
Thank you to occupational therapy staff at Sir Charles Gairdner Hospital for supporting participant recruitment including Ms Siân Fitzgerald and Ms Rebecca Grant.
Research ethics
Ethical approval was granted by the Sir Charles Gairdner Osborne Park Health Care Group (QA33952) in 2020.
Consent
This project was deemed to be of negligible risk; as per the National Statement on Ethical Conduct in Human Research (5.1.22) (National Health and Medical Research Council, 2007). The control group was a retrospective medical records audit, and as such the requirement for informed consent was waived. Additionally, the patients and caregivers in the intervention group provided verbal informed consent.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in planning and progress of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
KH, KM, DE and KS researched literature and conceived the study. All authors were involved in protocol development and gaining ethical approval. KM, MW and KH supported the data collection. AJ and KH completed the data analysis. KH and MW wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.