
Abstract
Introduction:
Relatives are important when older adults return home after a hospital stay. The aim of this study was to describe close relatives’ perspectives of the everyday activities of older adults who are repeatedly readmitted to hospital and discharged to home.
Methods:
A semi-structured interview was performed to collect data from twenty relatives (aged 45–82 years). Data were analysed using a deductive qualitative content analysis based on the results of a previous study within this field.
Results:
The overall theme ‘In need of support to manage an unpredictable everyday life’ shows that the older adults often needed support in everyday activities. In the two categories ‘Difficulties in dealing with an unstable day’ and ‘Managing an unstable day’ and the 10 subcategories, close relatives described that the older adults needed support in various ways from relatives or other individuals. Close contact was important for how everyday activities worked at home and in maintaining social contacts and contact with healthcare.
Conclusion:
It was found that social needs, such as social contacts/activities, are just as important to assess at discharge as medical and functional needs.
Keywords
Introduction
Rationale
A safe and coherent discharge from hospital to home is dependent on collaboration between different healthcare providers (Goncalves-Bradley et al., 2022; Henke et al., 2017; Socialdepartementet [Ministry of Social Affairs] 2017) and on communication and coordination with relatives (Goncalves-Bradley et al., 2022; Hautsalo et al., 2013). Discharge planning at hospital also seems to prevent readmission (Goncalves-Bradley et al., 2022; Henke et al., 2017). Close relatives play an important role when older adults return home after a hospital stay because they often provide day-to-day attendance and give support after discharge (Hvalvik and Reierson, 2015; Johansson and Schön, 2017; Jorgensen et al., 2021; Nyborg et al., 2017). In order to ensure a safe discharge home, the participation of relatives is often required. This is of particular importance when the older adults have complex health conditions and the home situation is thus assumed to be fragile. The close relatives’ perspectives can therefore add to existing knowledge on the everyday activities of older adults who are repeatedly readmitted to hospital.
Literature review
An ageing population will require various services to support everyday activities, healthy aging and age-friendly environments (World Health Organization, 2020). The initial period at home after a hospital stay is especially challenging for older adults and their close relatives because the home environment can be highly demanding due to worsened health and decreased ability in everyday activities (Dyrstad et al., 2015; Rocca et al., 2021; Rustad et al., 2017; Uscatescu et al., 2014). Older adults with a lower socioeconomic status also seem to be more likely to be affected by chronic illnesses and functional limitations in everyday activities (Lampert and Hoebel, 2019). From an occupational therapy perspective, limitations in everyday activities such as eating, mobility and personal hygiene have proven to be risk factors for readmission (Magdelijns et al., 2016). However, few studies have investigated everyday activities in this group of older adults (Nielsen et al., 2018) and from the perspective of their relatives. For example, we need to know if there are barriers related to the older adults’ ability that need to be overcome, but also how meaningful activities can still be performed in order to support everyday activities and healthier ageing.
Previous studies concerning older readmitted adults have shown that everyday activities are important as older adults try to maintain activities despite an unpredictable everyday life (Dilworth et al., 2012; Jonsson et al., 2020; Uscatescu et al., 2014). Close relatives often meet them on a regular basis, and their perspective is of value for supporting this group in order to promote a safe life at home (Dilworth et al., 2012; Jonsson et al., 2020). Relatives, most of whom are women (Johansson and Schön, 2017), cooperate with different healthcare professionals (Digby and Bloomer, 2014; Jakobsen et al., 2019), and a lack of collaboration among healthcare professionals and relatives can lead to an increased burden among the relatives (Bökberg et al., 2014). Moreover, relatives are in need of support to meet challenges during the care transition of the older adult (Jakobsen and Vik, 2019; Rustad et al., 2017) and to prevent their own depressive symptoms and to avoid the risk for social isolation (Behm et al., 2018; Digby and Bloomer, 2014; Hautsalo et al., 2013).
Method
Research design
A qualitative design with individual semi-structured interviews with a close relative were chosen in order to obtain the close relatives’ perspective of the everyday activities of the older (75 years or older) repeatedly readmitted person. A deductive qualitative content analysis was conducted using a template-organizing style (Crabtree and Miller, 1999; Kibiswa, 2019). Everyday activities in this study include all kinds of activities that take place in a person’s everyday life, such as personal activities of daily living (PADL), homemaking and leisure (Boyt Schell and Gillen, 2019). The older readmitted person is referred to as ‘older adult’ in the following text.
Participants and recruitment
The criteria for inclusion were persons being a close relative of an older adult (75 years and older) who was readmitted to a medical ward for the third time within a period of 12 months. This definition was earlier used by the National Board of Healthcare in Sweden (Socialstyrelsen [The National Board of Health and Welfare], 2021) when describing repeated hospital admissions in older adults. The older adults were assessed as ready for discharge within 1–5 days from admission to hospital. The exclusion criteria were older readmitted adults having a hospital stay >5 days because these older adults were assessed as being medically instable. A close relative was identified by the older adult as someone they have a close relationship with, that is, a husband/wife, cohabiting/non-co-habiting partner, child, sibling, close friend, neighbour or a legal representative. The participants in the study also had to be able to understand Swedish because the interviews were conducted in Swedish. The interviews were transcribed verbatim and the analyses were made in Swedish. The selected quotes were translated into English by an authorized translator. When including participants, we strived for a uniform distribution regarding gender among the close relatives in order to capture a variety of experiences.
The older adults had received care at a university hospital in central Sweden. They were asked by an occupational therapist if they allowed a close relative to be contacted upon discharge from the hospital. The occupational therapist who made the request did not treat the patient during the hospital stay. The occupational therapist received information on the inclusion criteria from the first author and selected eligible older adults from the patient roster on a daily basis (Monday–Friday). If an interest in participating was indicated by the older adult, the close relative was contacted by telephone and given verbal and written information about the study by the first author. A written consent was obtained by the first author if the close relative accepted to participate in the study. None of the researchers had a previous relation with the participants.
Data collection
Semi-structured interviews were conducted by the first author between September 2018 and March 2019. The first author is an occupational therapist and at the time a PhD student. Her daily professional practice is within acute medical care, and her previous research experience concerns older readmitted adults at hospital and at home. At the time of the data collection, the first author was not working clinically.
The interview guide used in this study was adapted from a previously constructed interview guide used for interviewing older, repeatedly readmitted adults on how they experienced everyday activities after discharge (Jonsson et al., 2020). The interview guide was tested in one pilot interview in the study by Jonsson et al. (2020).The content of the questions was the same as in the study by Jonsson et al. (2020), but the questions were rephrased in order to match the target group of this study (Appendix 1).
Questions were asked concerning how they experienced the older adult’s everyday activities.
Examples of open-ended questions from the interview guide were:
Can you describe what an ordinary day looks like for × right after he/she came home from hospital?
Follow-up questions were asked to gather further information.
● What is he/she able to do?
● What is he/she not able to do?
● What support does he/she need to perform activities?
A total of 20 participants were included. The interviews took place about 2 weeks after discharge and were conducted in the participants’ homes (n = 12), at their work place (n = 4), or in an office at the hospital (n = 4) as chosen by the participants. The interviews lasted between 23 and 75 minutes with an average length of 48 minutes and were digitally recorded.
Data analysis
Data were analysed with a deductive approach using a template-organizing style (Crabtree and Miller, 1999; Kibiswa, 2019). In the template-organizing style the template can be constructed in three different ways, namely based on theoretical perspectives, on prior research involving initial categories, or on a preliminary scanning of the text (Crabtree and Miller, 1999; Kibiswa, 2019). In this study, the template-organizing style was employed according to prior research (Jonsson et al., 2020). The analysis started with a word-for-word transcription of each interview by two trained medical secretaries that was then transferred to the NVivo 11 Pro. NVivo was used as a management tool (Edlundh and McDougall, 2017). In the first step, the first and last author read the transcripts several times in order to obtain an overall sense of the material as a whole. In the second step, the categories and subcategories from the result of the older readmitted adults’ experience of everyday activities (Jonsson et al., 2020) were used as templates, and information of significance with respect to this study was coded into them.
In the third step, information that could not be coded into one of the categories or subcategories was coded as ‘additional information’. This was later refined and resulted in three new subcategories. In the fourth step, the categories and subcategories were examined by the four researchers for ways in which they could be grouped into a theme. During the analytical process, the coding was discussed among all the researchers. In the final analysis, the first author reviewed each interview and the coding of the data in order to ensure, check and verify the coding process. Finally, an agreement upon the content and the identified theme, categories and subcategories was reached with the co-authors.
Trustworthiness
The credibility in this study was confirmed through the continuous engagement with the data by the first and last author. To assess the dependability of the data, the individual semi-structured interviews were listened to and carefully read by the first author. In order to increase conformability, the process of including the participants, analysing the data and presenting the results were continuously discussed by the research team, which is a form of triangulation (Hadi and Jose Closs, 2016). Further, transferability was increased when no new information emerged in the data from the participants, which was discussed by the research team.
Ethics
This study was conducted in accordance with the ethical principles for medical research involving human subjects in line with the Declaration of Helsinki. The Regional Ethical Review Board in (Uppsala) (Ref.no 2014/261/1) approved the study.
Results
Twenty participants (17 women and 3 men) were included in the study, including nine wives, five daughters, three sons, one non-cohabiting partner, one sister and one niece, with an age range of 45–85 years. The contact with the older adult varied from daily contacts, visits or phone calls to having a visit or a phone call once a week. Ten of the participants (nine wives and one adult child) were living together with the older adult.
According to the close relatives, the main reasons for the older adults seeking acute care were shortness of breath, dizziness, nausea, chest pain and eating problems. Ten of the older adults had safety alarm, nine had mobility services, five homecare services and four homecare nursing. Further, three older adults participated in day care and the most commonly used assistive device was a walker.
The overarching theme was ‘To be in need of support while managing an unpredictable everyday life’, which depicted the different dimensions that affect the performance of everyday activities by the older adult after discharge. A close contact with relatives, or sometimes healthcare professionals, was important for the ways an older adult could perform different activities after discharge. The theme, the two categories, and the ten subcategories are presented in Table 1.
Summary of the results with exemplifying quotes, 10 subcategories, 2 categories and one theme.
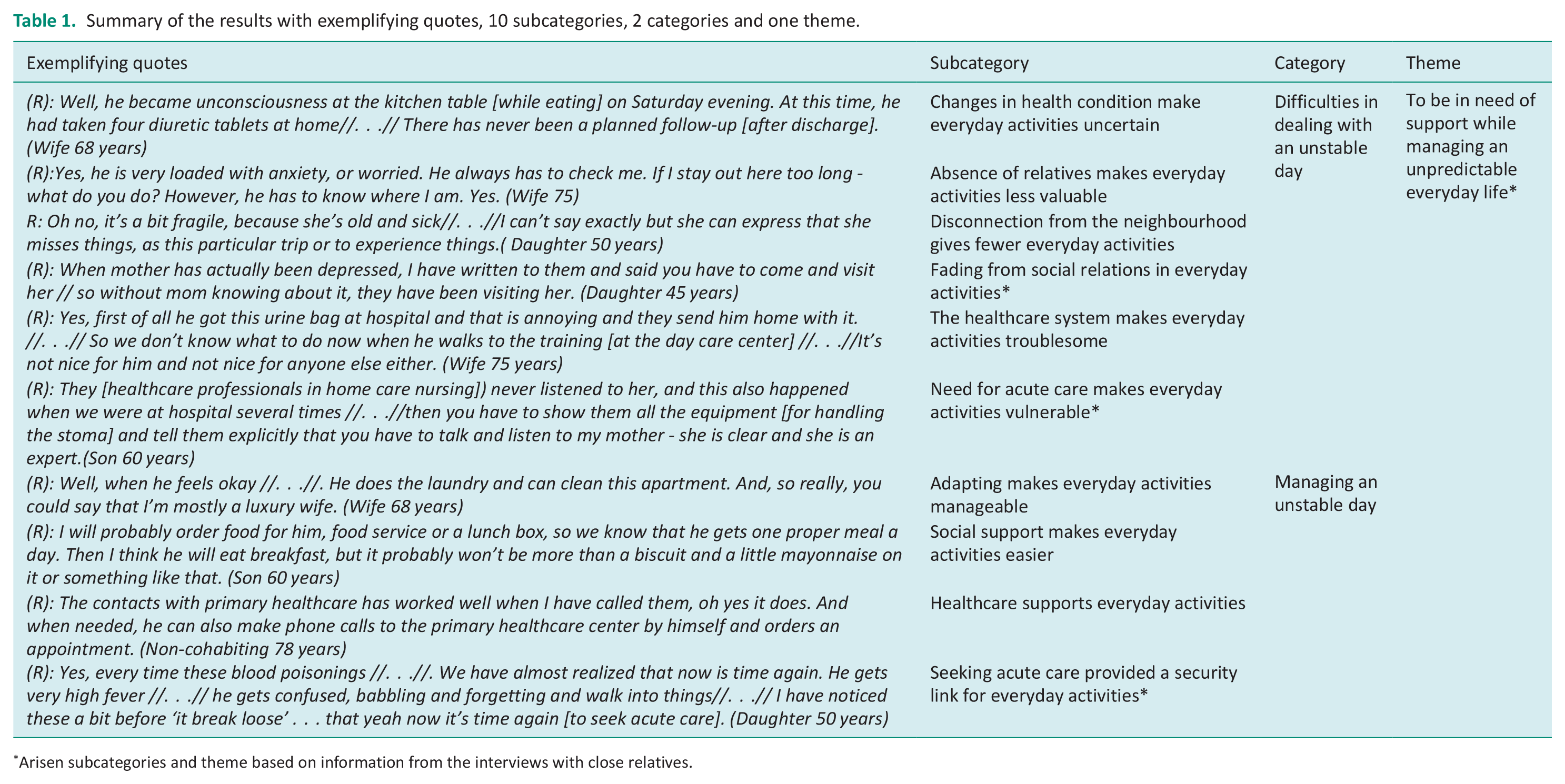
Arisen subcategories and theme based on information from the interviews with close relatives.
Difficulties in dealing with an unstable day
In this category, the participants described difficulties the older adults had in performing everyday activities at home and in engaging in social activities as well as frustration with the healthcare system. This category contained the subcategories of ‘Changes in health condition make everyday activities uncertain’, ‘Absence of relatives makes everyday activities less valuable’, ‘Disconnection from the neighbourhood gives fewer everyday activities’, ‘Fading from social relations in everyday activities’, ‘The healthcare system makes everyday activities troublesome’, and ‘Need for acute care makes everyday activities vulnerable’ (Table 1).
Changes in health condition make everyday activities uncertain
The participants indicated that changing health and medical conditions created uncertainty for the older adult at home. Conditions such as breathlessness, nausea, fatigue and balance difficulties could create uncertainty and also imply that some of the older adults did not have the ability to carry out their everyday activities. This uncertainty also created some worries in everyday life for both the participant and the older adult.
Participant (R): Oh, both X and I might think if we have planned a trip or something. I hope that nothing will happen, you know. There is a tension, or what to say. There is a concern in that. However, at the same time you can say that we have not been able to say that there is something triggering. Because this can appear when it is just calm. (Wife 69 years)
The participants also described that a mental condition could affect the initiative of the older adult and could contribute to uncertainty as to whether activities such as cooking, shopping and gardening could be done.
(R): Well, a basic problem is that X thinks he should do things but he does not and he has been very energetic. //. . . //. I don’t know how many times he has said, ‘I have to get out to the garage and get it done’, but he doesn’t. It’s not that he does not want to, but he feels bad and he just can’t seem to make it happen. (Wife 73 years)
Absence of relatives makes everyday activities less valuable
In some of the descriptions from the participants, broken contacts or loss of family members had negatively affected the performance of the everyday activities at home. This could limit the older adult when carrying out activities such as planning for meals, walking and travelling. The loss of a family member could cause irritation in the close relationship between the older adult and the participant. One participant described how the loss of a daughter of her husband from an earlier relationship appeared to affect the ability and initiative to perform activities for the older adult at home.
(R): One daughter died. Moreover, they had no contact. I would say that is a big part in my husband’s illness, or at least in his mind. . . . Actually, this pretty much affects our everyday life. (Wife 73 years)
Disconnection from the neighbourhood gives fewer everyday activities
Some participants described that the older adult could have difficulties participating in social activities. Others described how medical devices, such as urine bags, were not always adapted to the needs of the older adult, which could be barriers to outings or participating in social day care. Sometimes an altered medical condition involved a physical change for the older adult. This could cause difficulties in participating in activities outside the home, in turn causing a reduced level of everyday activities in general.
(R): He usually attends day care two days a week. Nevertheless, he doesn’t really want to participate there either because he cannot talk or eat properly. He thinks it is very embarrassing, he is not used to it. He feels insulted. //. . .// so he is very much alone now. (Son 50 years)
Fading from social relations in everyday activities
According to the participants, the older adults were not always capable of maintaining activities that included social relations inside and outside the home. The older adults could be described as fading from the communication related to different social relations or activities, for example, going on outings or visiting friends. One participant expressed it like this:
(R): The social relations and keeping contacts [with friends or family members] are important. He has sometimes refused . . . He almost turns away from it. (Wife 75 years)
This could create a distance in the communication between the older adult and the participant and affect some of the activities at home. From the perspective of the participants, this meant that the older adult was not always aware that the participant was trying to keep up various everyday activities and social relations and to keep things as normal as possible.
The healthcare system makes everyday activities troublesome
There were participants who indicated failings and faults in the care after the hospital stay. From the perspective of the participants, this could affect the activity performance and safety at home for the older adult. For example, it could be difficult for the older adult to get in contact with and get information from a healthcare centre when purchasing medical devices or medicines. The use of digital technology related to care, or travelling with a mobility service, could be a challenge for the older adult. In summary, the participants expressed some frustration on behalf of the older adult related to how he/she was able to manage different activities after discharge.
(R): He uses bag-dispensed drugs and he wonders if this can be sent to his home instead. So, I have called. . . . Nobody knows and I’ve called the pharmacy. They have no idea. (Son 50 years)
Need for acute care makes everyday activities vulnerable
According to the participants, activities such as mobility and food intake were affected due to an altered medical condition (chest pain, dizziness, etc.), and this could lead to a need for acute care. At the hospital, the participants described how there could be difficulties for the older adult to receive and to communicate information to relatives during their stay.
(R): No, he telephoned by himself. He called me when he was at the hospital and then he came home late the next day. I was going to visit him . . . but he was already home. //. . .//He was just dropped off at home, and after that he was just sitting here. (Wife 80 years)
The participants described how the older adult could not always absorb the information that was given at discharge from hospital, which could contribute to new upcoming needs at home. For example, these situations included whether the older adult was able to take his or her medications, but also how consequences such as low endurance and balance difficulties affected the ability to perform everyday activities for the older adult after the hospital stay. The participants described this as an incomplete follow-up-care for the older adult because the communication had been interrupted or failed.
Managing an unstable day
In this category, the participants described that, in order to maintain ability and performance at home, direct or indirect personal support from family members or the healthcare system was important. This category contained the subcategories ‘Adapting makes everyday activities manageable’, ‘Social support makes everyday activities easier’, ‘Healthcare supports everyday activities’, and ‘Seeking acute care provides a security link for everyday activities’ (Table 1).
Adapting makes everyday activities manageable
Trying to maintain performance in everyday activities at home was considered to be important for the older adult from the perspective of the participants. Several of the older adults were independent when performing personal care at home after discharge from hospital. However, many participants said that the older adults often had adapted their activity repertoire by doing fewer activities both indoors and outdoors. It appeared that the older adults performed specific self-care activities, although these required strength, carefulness and endurance. One participant described how his mother had made adjustments to be able to take care of her stoma with precision both during the day and at night.
(R): Well . . . she draws herself every third hour. The morning, first, is about six o’clock for her. She takes her medicines with some high-calorie nutritional drink. Then she goes to bed again and wakes up again about nine, and then she usually eats her breakfast, some of it already prepared at six o’clock, takes her medicines, and handles her stoma. There are many things for her to do. She is BUSY. (Son 60 years)
Social support makes everyday activities easier
The description from the participants indicated that some of the older adults were dependent on social support in different ways for the performance of everyday activities. Some of the older adults had to be attended to more often and were given more instructions or help than before. For example, participants described older adults who sometimes needed direct and practical support or had to be instructed while changing clothes, taking the right medicine at the right time, booking appointments, or using digital technology.
(R): I have been thinking a lot, it is probably the same with all the old ones, with (phone) calling and then choosing one, two, and three. He has a problem with managing this without getting angry. Therefore, I take care of everything like that, phone calls, bills and things. He does not know how to do them. (Wife 68 years)
The participants claimed that close emotional contacts were important for the older adults when life became more difficult. Being closely related to another person seemed to create opportunities to express emotions and meaning for the older adult’s routines and performance. According to the participants, the older adult could express frustration or discomfort in a situation and the participant could give verbal support, make a phone call, or do ‘face time’.
(R): . . . However, after he started living alone, we make a phone call almost every day. . . I think it’s loneliness, and when you get pain and are not able to be so physically active, he expresses panic, anxiety, and sometimes anger. . . (Daughter 50 years)
Healthcare supports everyday activities
According to the descriptions of the participants, the healthcare system gave the older adults appropriate support at home after the hospital visit. They described, for example, how the older adults had been given more support at home related to fall risk or received day care or were planned to be supported by a local mobile health care team. Thus, the participants argued that the older adult appeared to be able to maintain some performance and routines or could have a safer home environment despite a poorer health condition.
(R): The meeting today was reserved for this (planning). From today, they will now be able to give fluid infusion at home. Previously, we had to take an ambulance to the emergency ward, and in recent weeks we have been there three times maybe. (Son 60 years)
Seeking acute care provides a security link for everyday activities
According to the participants, the decision to seek acute care was often made by the older adult together with a relative. The participants described an older adult with severe symptoms, such as shortness of breath or infections related to circulatory or respiratory organs, which could affect the older adult’s everyday activities, such as food intake and mobility, including falls inside and outside the home.
(R): That’s the only thing he has been seeking acute care for. He is feeling so bad, and he is dehydrated. Therefore, we have stayed at home shorter and shorter periods because we have noticed it becomes a vicious circle. Everyday life just doesn’t work. . .Because then he needs some fluid intravenously and such things. (Wife 69 years)
Some participants described how the older adults, due to changed medical conditions, felt safer at hospital than at home. In the participants’ opinion, the hospital stay gave the older adult the support they needed to maintain activity performance in everyday activities at home. The hospital stays contributed to recovery and made the older adults maintain ability and perform activities as shopping, cooking, biking or taking a walk after discharge.
Discussion
In this study, the perspectives of close relatives showed that the older adults’ everyday lives were vulnerable. The older adults often needed medical, physical and social support in order to maintain their everyday activities at home. According to the close relatives, the previously readmitted older adult was not always able to perform everyday activities or was ill-prepared for life at home when discharged.
One result in this study is the close relative’s experience concerning the older adults’ need for adaptation of their activity performance. These adaptions supported the older adult in maintaining different activities after discharge. Health problems such as breathlessness, dizziness and feelings of weakness were mentioned as unpredictable and could force some of the older adults to be more sedentary instead of doing activities they had previously been able to manage. Also, eating problems and nausea along with a reduction in endurance were mentioned by close relatives as barriers to the performance of everyday activities at home. These results are consistent with previous studies (Dilworth et al., 2012; Jonsson et al., 2020; Vat et al., 2015) that showed that various health problems in this group of older adults contributed to difficulties when adapting to everyday activities at home.
According to the descriptions of the close relatives and previous studies (Dilworth et al., 2012; Jonsson et al., 2020), feelings of preparedness and a need for support, for instance, with medicines and PADL (eating/drinking, toileting, mobility etc.), have to be assessed and integrated into the discharge process to prevent further readmission. Healthy ageing involves improving opportunities for activity, health, participation and security in order to enhance well-being and quality of life (World Health Organization, 2020). In order to prepare for a safer life at home, the results from our study and from experiences of older repeatedly readmitted adults (Jonsson et al., 2020) indicate that altered activity performance in, for example, eating, taking medicines, or mobility should be in focus at follow-up in order to prevent readmission and to promote healthy ageing. For example, the development of senior-centre programmes and health-promotion strategies that aim to support functional ability could be of value and may promote a healthier ageing (Nuwere et al., 2022) in this group of older adults.
Performing follow-up interventions with continuity at home has also been shown to be associated with fewer rapid readmissions (Benzo et al., 2016). A barrier to continuity of follow-up interventions at home can be a lack of available resources in the community setting. Despite this, and in light of the results in this study, occupational therapists and other healthcare professionals have to assess not only activity performance, but also how previously readmitted older adults are prepared for a safe life at home. Moreover, the older adults’ functional ability was described as reduced with respect to everyday activities at home. In order to support their ability at home and to promote healthier ageing, occupational therapists have to be aware of older adults with repeated readmissions to hospital. To prevent readmission, follow-up visits and phone calls from a care coordinator in primary healthcare might also provide further support related to safety, health problems and PADL (Benzo et al., 2016).
The results of the present study show from the perspective of a close relative that older adults often need social support in order to perform everyday activities. Adults with several social contacts are less likely to report loneliness (Dahlberg et al., 2018), and therefore social relations, such as contact with family members, relatives and friends, are important to maintain. These aspects are also mentioned in the studies by Dilworth et al. (2012) and Jonsson et al. (2020). In these studies, loneliness or social isolation were shown to have a negative impact on the performance of everyday activities. Broken social contacts with other family members, as mentioned in our study, could have a negative impact on the initiative to engage in different everyday activities. As described by close relatives, participating in different social activities and maintaining an everyday life could be problematic. When people age and experience health problems, the need for social support may increase and social activities may change. According to the close relatives, the initiative of the older adult and the ability to maintain social relations were seen as important facilitators in maintaining everyday activities at home. This aspect has been raised by Lees (2013), who questioned how different healthcare professionals were able to identify older adults with a reduced initiative, fragile social support and involuntary loneliness at home. Therefore, social support must be given more attention along with medical and functional needs at discharge and at follow-up in order to provide good and safe care at home. Therefore, occupational therapists should, together with the assessments and interventions of functional ability in everyday activities at home, provide suitable interventions such as referral to social day care in order to prevent involuntary loneliness.
Another result of this study is that communication between different actors may be deficient. In our interviews, the close relatives sometimes experienced that they received insufficient information regarding the medical and physical conditions of the older readmitted adults at discharge. This can lead to a lack of understanding because patients’ own insights might be limited. Healthcare professionals could, on the other hand, have too much credence in the older adult’s description of their ability (Dilworth et al., 2012; Uscatescu et al., 2014). The short hospital stay may contribute to a lack of person-centred care for this group and may lead to unmet individual needs for care. The short hospital stays may also result in a lack of sharing information about practical care issues between healthcare providers, the older readmitted adults, and their close relatives. This was also seen in studies by Dilworth et al. (2012), Jones (2016), and Hestevik et al. (2019) who observed that older adults admitted to a hospital and their relatives often had insufficient or contradictory information at discharge. In the present study, the older adult was also mentioned as too rapidly discharged, which affected the performance of everyday activities at home. This calls for better awareness, communication and follow-ups after discharge. A structured communication between healthcare providers and a better coordination of care at home may increase the possibility to recover at home (Goncalves-Bradley et al., 2022).
Early involvement of relatives could also be useful for adjustment of different activities at home. However, the close relatives in this study also described that healthcare had met the needs of the older adult in some aspects. One example of this was when seeking emergency care repeatedly due to dehydration or shortness of breath after discharge. These repeated ‘life-saving’ contacts with the hospital were later met with continuity of interventions, such as support from a local mobile healthcare team. This intervention indicated that the risk for readmission was decreased for some of the older adults in this group. Continuity of follow-ups seems to be necessary in order to prevent readmission (Benzo et al., 2016; Hestevik et al., 2019). In addition, continuity, such as contact with a mobile healthcare team and having medical support at home, may prevent readmission in older adults with chronic conditions (Facchinetti et al., 2020), but further studies are needed.
Strengths and limitations
The present study has both limitations and strengths. The results in this study may be limited by the fact that healthcare systems can differ between countries and in the care of older adults at home.
At inclusion, the first 15 recruited close relatives were mostly women, which is not surprising as the majority of caregivers are women (Johansson and Schön, 2017). However, another five participants were recruited and in that second phase of recruitment two more men were included. In the second phase of recruitment, no new information emerged as similar patterns of experiences were found. The interviews with the participants contributed to a variation and richness of data. The interviews were recorded, listened to, transcribed and read through several times, which strengthened the credibility and confirmability of the study (Lincoln and Guba, 1985).
The data in this study were analysed using a deductive qualitative approach comprising a template-organizing style(Crabtree and Miller, 1999; Kibiswa, 2019). According to Crabtree & Miller (1999) and Kibiswa (2019), the deductive qualitative content analysis can be performed in different ways. In this study, we chose to use the template-organizing style (Crabtree and Miller, 1999). The deductive research approach explores a known theory or phenomenon and tests if that theory or phenomenon is valid in the given circumstances (Crabtree and Miller, 1999). However, coding data from predetermined categorization may have biased the exploratory nature of qualitative methods. Even if the data is analysed using predetermined codes in a published study, the information of the everyday activities of this group of older adults using ‘the lens’ from close relatives could both validate and complement some findings presented in the previous study (Jonsson et al., 2020). The three new subcategories that emerged from the data have contributed to additional knowledge and understanding regarding this group of older adults and are seen to strengthen the trustworthiness (Lincoln and Guba, 1985) of the results in this study. A limitation may be that we have not used member checking in this study. Not using member checking in qualitative research has previously been described as problematic when the research team did not have multiple contacts with the participants (Thomas, 2016), which was the case in this study. On the other hand, the participants in this study did not have a relation to those older adults who participated in the previous study by Jonsson et al. (2020), which is seen to strengthen the transferability of the results in this study. In order to clarify and enable transferability of the findings of this group of older adults in this study, some characteristics of both the participants and the older readmitted adults are described. All authors were involved in the analysis process in order to confirm the study’s credibility and confirmability (Lincoln and Guba, 1985).
Conclusion
The perspectives from close relatives have contributed to additional knowledge about everyday activities of older readmitted adults discharged to home. The close contact with a relative was important for how the performance of everyday activities worked at home as well as for maintaining social activities in order ‘to keep life as normal as possible’. Social contacts and social activities may therefore be just as important as the medical and functional needs at home for the older adult in order to prevent or delay readmission.
Key findings
Close contact with relatives was important for the ability to perform everyday activities after discharge.
Older readmitted adults were not always capable of maintaining social activities at home.
What the study has added
Healthcare and social care need to identify whether or not older readmitted adults need additional support at home.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226231191366 – Supplemental material for Close relatives’ perspectives of everyday activities at home for older adults repeatedly readmitted to hospital: A qualitative study
Supplemental material, sj-docx-1-bjo-10.1177_03080226231191366 for Close relatives’ perspectives of everyday activities at home for older adults repeatedly readmitted to hospital: A qualitative study by Marie Jönsson, Marie Holmefur, Peter Appelros and Carin Fredriksson in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors would like to thank the twenty participants in the study. The authors gratefully acknowledge this support.
Research ethics
The Regional Ethical Review Board in Uppsala (Ref.no 2014/361/1) approved the study.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Consent
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Region Örebro County.
Contributorship
All authors declare that this manuscript is original and has been read and approved by all authors. We confirm that all authors fulfil the authorship requirements and are listed in the correct order. We confirm that we have given due consideration to the protection of intellectual property associated with this work and that all necessary contact information for the corresponding author has been provided and is accurate.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.