
Abstract
Introduction:
People with complex physical disabilities unable to change their position independently are at risk of developing postural deformities and secondary complications. 24-hour posture management is needed to protect body structure. With inconsistencies in current service provision, this research aimed to scope the evidence for a 24-hour posture management approach.
Method:
A scoping review was conducted using four health and social science databases. Inclusion and exclusion criteria were applied; further papers were included through citation chaining.
Results:
The evidence for 24-hour posture management was often low quality due to the complications of completing robust research studies in this complex specialty. However, many professionals in the field agree that a 24-hour approach to postural care is essential.
Conclusion:
There is a need for clear national policy and guidance relating to postural care and scope for development of dedicated posture management services. Current NHS service provision is variable and inconsistent. Lack of postural care is a safeguarding and human rights issue. Specialist training and research in postural care within the Occupational Therapy profession is required to raise awareness of the role Occupational Therapists can play in preventing postural deformities and other secondary complications through providing good postural care.
Introduction
For people with complex physical and sensory disabilities, who are unable to independently change their body position, posture and positioning become a very important issue. Their body structures are influenced by both postural alignment and the forces of gravity, which in turn affect body functions and the ability to participate in everyday activities. Posture is defined as the alignment of body segments relative to each other (Casey et al., 2020; Stinson et al., 2021). If an individual adopts an asymmetrical position, is not able to independently change position and is submitted to the forces of gravity they can develop secondary complications such as tissue damage, muscle contractures, pain and discomfort, constipation and infections (Pope, 2007); characteristics which are typically not a direct consequence of the diagnosed impairment (Pope, 2007). Often the body structures distort because of an inability to change position and an asymmetric posture, coupled with the influence of gravitational forces, which compress and restrict the function of the internal organs. If left uncorrected, this can lead to further health and participation complications and even premature death (Changing our Lives, 2018; Clayton et al., 2017).
To reduce the negative effects of gravity and avoid the development of such complications, ‘24-hour posture management’ is regarded as necessary (Hill and Goldsmith, 2010) by many therapists. Farley et al. (2003) define 24-hour postural management as utilisation of a range of interventions to reduce postural asymmetry and improve function, and includes all lying, sitting and standing positions that occur within any 24-hour period. Assessment of posture throughout the day and night needs to be examined within a multi-disciplinary framework to ensure appropriate provision of postural advice and supports (Castle et al., 2014; Hill and Goldsmith, 2009; Wright et al., 2010) that match the needs of both the individual and their caregivers. Techniques include the use of lying supports, standing supports and specialised seating (Agustsson and Jonsdottir, 2018) to sustain comfort and symmetry across multiple orientations that a person can spend significant lengths of time over a 24-hour period. If posture is not examined collectively in each orientation of sitting, lying and standing, it can be counterproductive to the provision of postural supports in only one orientation.
From an Occupational Therapy perspective, taking a ‘whole-person approach’ to support both mental and physical health and wellbeing is essential to enable individuals the opportunity to achieve their full potential (RCOT, 2019). Therefore, it is important for the profession to consider posture management as a pre-requisite (Agustsson and Jonsdottir, 2018) and fundamental to occupational performance. For example, if an individual is unable to maintain sitting balance because their trunk is not stable, their arms will naturally seek to provide the stability required; leaving their hands unavailable to engage in task performance. They may uneconomically use energy attempting to maintain an upright position, rather than engaging in an activity. Optimal postural care often relies on therapists’ knowledge and experience (Humphreys and Pountney, 2006; Pountney et al., 2002) leading to a postcode lottery of expertise, funding and timely provision of appropriate 24-hour postural management intervention.
In the United Kingdom, NHS provision of postural management assistive technology is ad hoc due to complicated and fragmented commissioning procedures and funding across varying models of postural management services (Aldersea, 1999; Darzi, 2018). Integration of these services as well as a joined-up approach to commissioning has long been recommended to improve efficiency and cost-effectiveness of equipment provision for posture management (Aldersea, 1999). Today, wheelchair services are well-established at meeting mobility and postural needs within wheeled mobility, but often there is no consideration given to the remainder of the 24-hour period, including no provision for static seating. Often, persons who need specialist static seating provision outside of a wheelchair, or who do not meet the criteria for a wheelchair, will fall into a gap in service provision with their needs going unmet. In these instances, individuals and families are left to purchase static seating independently, which can often lead to expensive mistakes of purchasing ill-fitting or inappropriate seating (Collins, 2001).
There is growing evidence that supports the notion that positioning in lying has a direct relationship on the success of postural alignment in sitting. Many individuals spend short periods of time in a wheelchair that has been custom made for their complex needs and frequently have no provision to address their postural needs outside of the wheelchair. There is often no funding for alternative seating or lying supports. Provision is patchy and inconsistent throughout the UK; it is not typically coordinated to ensure that postural supports work in harmony to cover the whole 24-hour period.
Failure to provide appropriate wheelchair seating and static seating leads to individuals being unable to reach their occupational potential and often not able to participate in life as an equal citizen (Gowran, 2013). At this point, posture management provision becomes an issue of safeguarding and human rights as it is seen as ‘a pre-requisite for survival and personal mobility’ (Gowran et al., 2020: 9). Therefore, the primary objective of this study is to examine the evidence for 24-hour posture management. Secondary objectives were to explore the current provision of postural care and consider recommendations that can improve postural management practice within the Occupational Therapy profession in the UK.
Method
A scoping review methodology was used to synthesise the breadth of available literature and study designs employed. This method of scoping an emerging topic area that is broad, ensures that all available literature is included, including policy as well as intervention and exploratory research papers. Munn et al. (2018) suggested that scoping reviews offer a different technique for scrutinising theories and could therefore be more beneficial for practice development. As the aim of this study is to explore the use and merits of 24-hour posture management to inform practice, it is more appropriate to adopt a scoping method that captures rationale from across a range of sources.
Further, Anderson et al. (2008) stated that scoping studies are a crucial research methodology for guiding policy makers and can provide the opportunity to develop further research, policy and evidence-based practice (Colquhoun et al., 2014). Global literature was included since this is an emerging topic with patchy provision in the UK. It was felt there could be potential learning from the international community for implementing 24-hour posture management that might be relevant to the development of recommendations for enhanced practice within the UK.
This scoping review was structured using the PRISMA (Preferred Reporting Items for Systematic review and Meta Analyses) guidelines. The concept of posture management continues to evolve, so published research studies, policies, clinical frameworks and emerging unpublished studies and reports were included in the search. The literature review conducted by Farley et al. (2003) was used as the starting point for this review examining the evidence since 2003 for posture management interventions.
Relevant scientific literature was identified using four electronic databases: CINAHL, Psych INFO, Web of Science, and Medline covering the range of scientific literature published in educational, medical, psychological and social sciences journals. An initial search of PubMed was used to test out the preliminary search terms. A PICO framework was used to identify a list of 33 keywords based on the authors’ (LO and JC) experience of the field relating to posture and types of posture management devices, such as ‘custom moulded seating’. An additional 21 keywords describing postural deformities, such as ‘contracture’ and ‘hip subluxation’ were also identified (Table 1).
PICO framework.
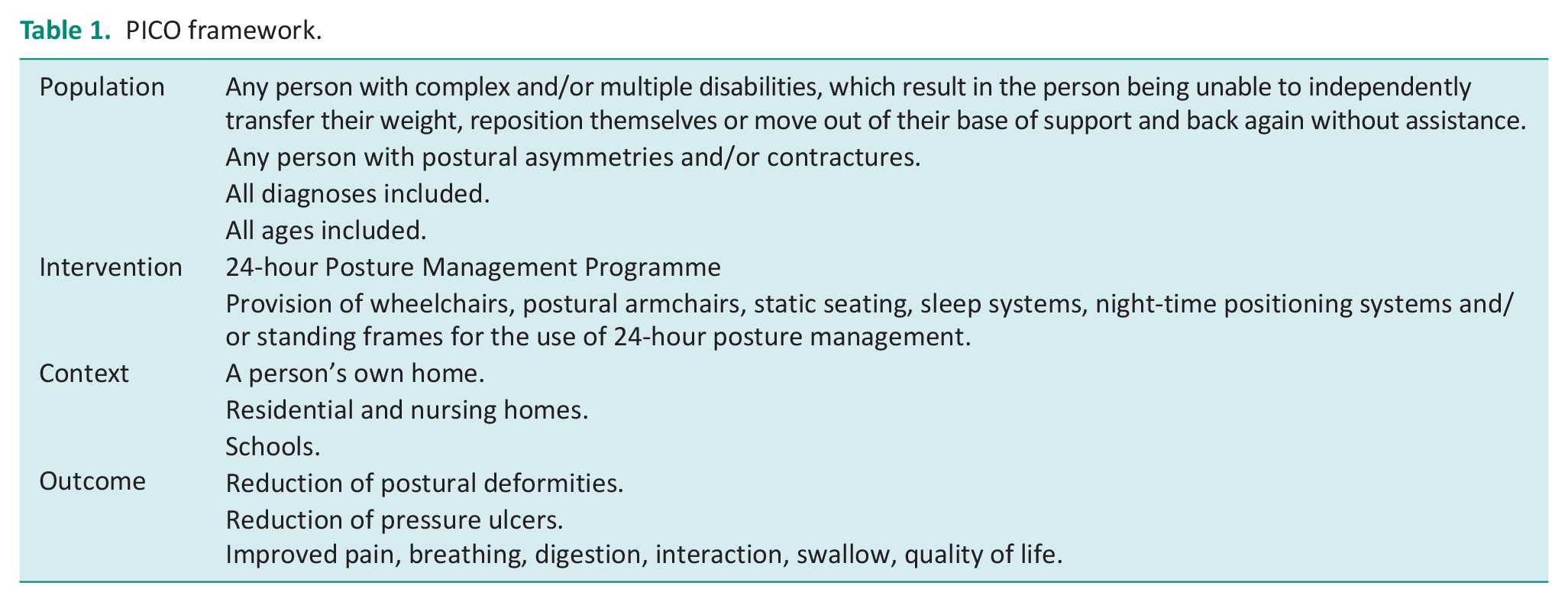
Each of the keywords listed under ‘posture management’ were searched using the Boolean operator ‘OR’ to capture all possible terms; this yielded 101,434 hits. These were then searched in association with the keywords against ‘postural deformities’ using the Boolean operator ‘AND’, yielding a total of 4387 hits. The Boolean phrase ‘AND’ was used to combine the search results, resulting in only five papers. Therefore, it was decided to remove the second column of postural deformity terms and widen the search by concentrating on the posture management keywords; using the disability and diagnosis terms did not enhance the search strategy. As it is an emerging topic, scoping the breadth of the literature, including such refined terms narrowed the search results. Research that is completed on this topic is catalogued using the main heading of postural terms, rather than being diagnosis-specific. This also ensured that there was no bias towards one particular diagnosis, as postural deformity can affect anyone who is unable to move their position independently and is not determined by their medical diagnosis.
However, with a result of over 100,000 papers, this needed to be refined. In consultation with the health librarians all generic terms such as ‘chair’ and ‘position*’ were removed as these were felt to be too broad. Papers not relevant to the research question were excluded. The final search terms were ‘posture management’, ‘night-time positioning’, ‘seating assessment’ and ‘postural seating’; these were truncated to include similar terms such as ‘posture’ and ‘postural’. The grey literature was retrieved via a Google search engine using the search terms and names of known authors in the field. They were then reviewed and scanned in the same way as the retrieved published peer-reviewed literature and the same inclusion/exclusion criteria were applied.
Titles and abstracts were independently reviewed by two authors (LO and JC), then full texts obtained if the abstract appeared relevant or if it seemed unclear. The following inclusion and exclusion criteria were applied to focus the search into meaningful results.
Inclusion
Scientific and grey literature relating to 24-hour posture management
Literature relating to use of wheelchairs, specialised seating, night-time positioning and standing frame use within the context of 24-hour posture management
Literature worldwide
Written in English language only
Dated from 2003 to 2019
Exclusion
Non-English language literature
Dated pre-2003
Literature detailing product testing or development
Literature relating to wheelchairs, specialist seating, night-time positioning and standing frames specifically, without applying the context of 24-hour posture management.
As the papers from each database were reviewed, so too were their reference lists; a method referred to as ‘citation chaining’ (Greenhalgh, 2010). Typically, a scoping review does not critically appraise the evidence presented (Colquhoun et al., 2010; Peters et al., 2015). However, it was felt necessary to comment on the strength of the research available to demonstrate the challenges of conducting research in this field, and to consider the reasons for this and hence the importance of considering other types of literature.
The papers were read multiple times and the primary author was fully immersed in the literature. A simple categorisation system by Wallace and Wray (2006), cited in Aveyard (2014) was used to categorise the literature type and then an interpretive phenomenological approach was used to identify common themes arising across all of the literature.
(Wallace and Wray, 2006 cited in Aveyard, 2014: 44).
Results
A total of 268 papers were retrieved, with 44 meeting the inclusion criteria. Of these, half were centred around a view of 24-hour posture management, or posture management in general, 10 were focused on lying postures and night-time positioning, 8 on sitting posture and seating assessment and 4 on standing programmes (see Figure 1).
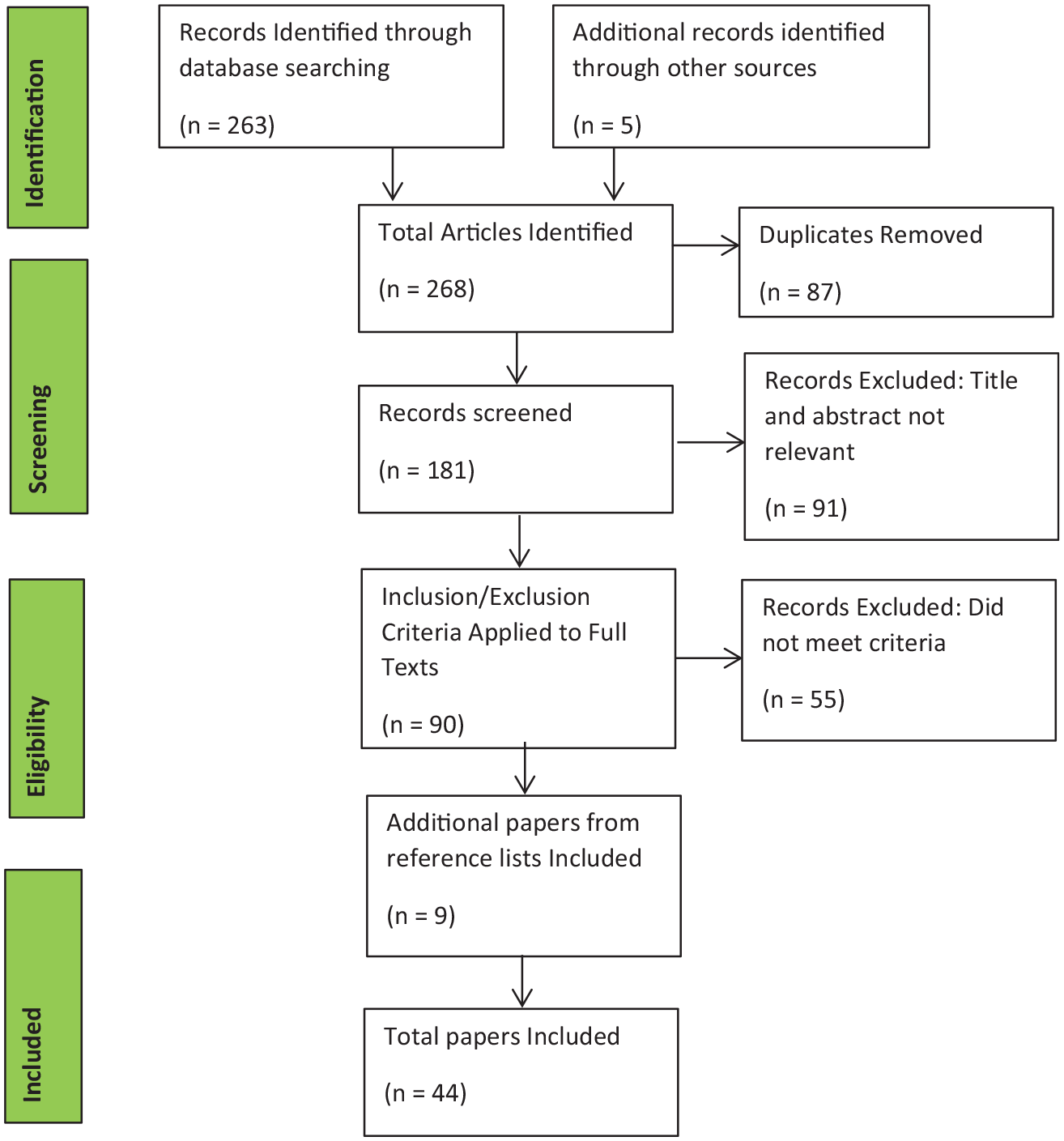
PRISMA Diagram showing search results.
Types of papers
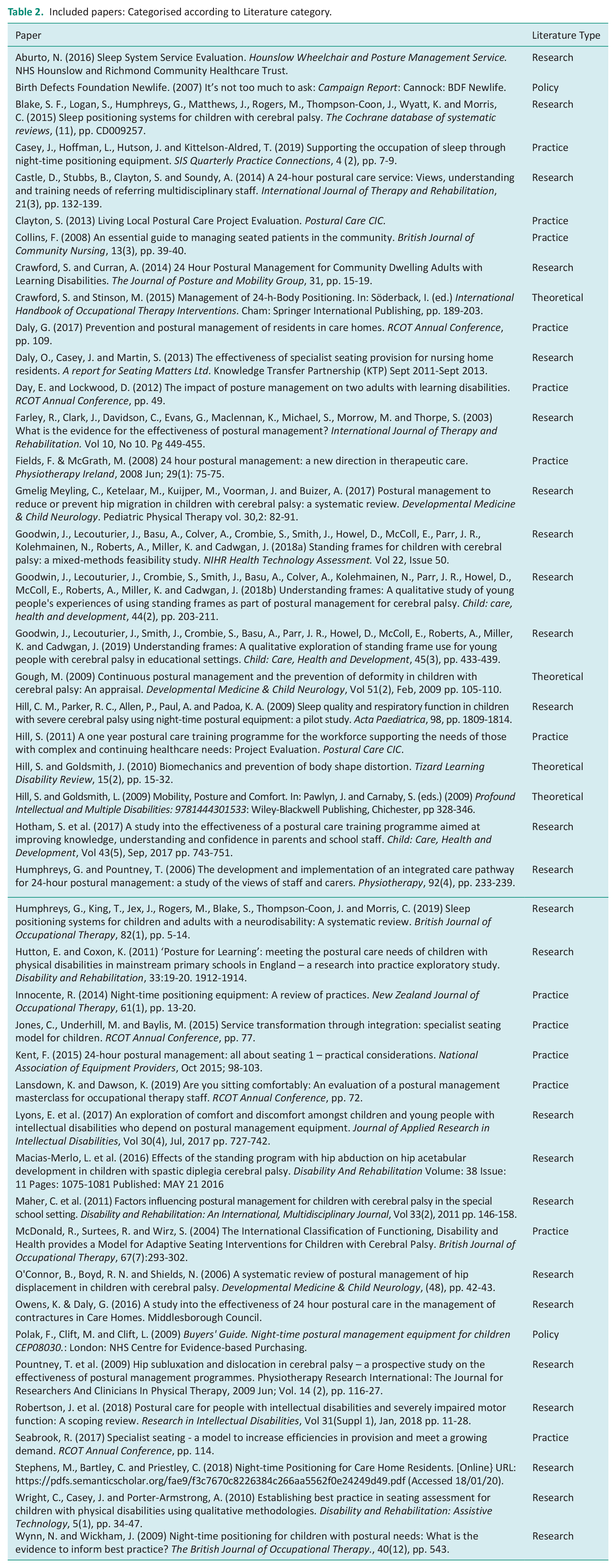
Of the 44 papers included, 4 were classified as theoretical literature, 25 as research literature, 13 as practice literature, and 2 as policy literature. See Table 2.
Included papers: Categorised according to Literature category.
Study design
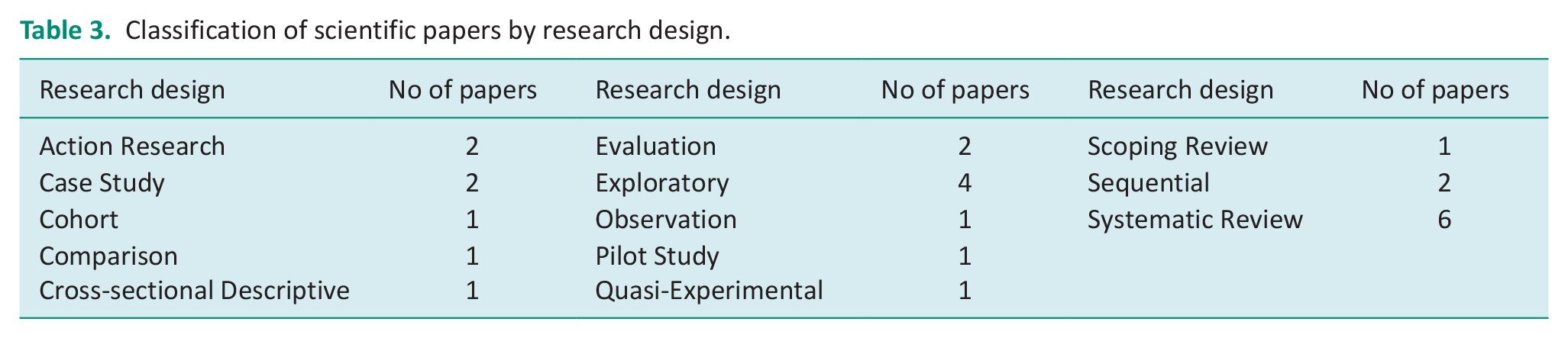
There were no RCTs and only one quasi-experimental design amongst the included research papers, supporting the view these research methodologies are not appropriate for this population and clinical field (see Table 3).
Classification of scientific papers by research design.
Most papers were systematic literature reviews, concluding that the research available was weak in design and of low quality (Blake et al., 2015; Gmelig Meyling et al., 2017; Humphreys et al., 2019; O’Connor et al., 2006) and stipulated that further research was recommended such as development of a consensus statement of expert opinion and regular publishing of case studies from clinical practice (Farley et al., 2003; Wynn and Wickham, 2009).
Whilst the evidence body is small, it is growing and does appear to support 24-hour posture management (Wynn and Wickham, 2009). The systematic review by Blake et al. (2015) also noted that many papers included in their review were not indexed on electronic databases and were retrieved through directly contacting manufacturers and authors, illustrating that literature on this topic is hard to locate. An explanation for this may be due to strict submission criteria and that many journals will not publish research with lower levels of research design.
Of the 13 papers classified as practice literature, 6 were conference abstracts of presentations given by clinicians working within the posture management field. Half of those directly stated that Occupational Therapists have a direct role in assessing and delivering posture management (Daly, 2017; Day and Lockwood, 2012; Lansdown and Dawson, 2019). Whilst the other half presented their own development of multidisciplinary working towards a posture management service in their geographical area (Fields and McGrath, 2008; Jones et al., 2015; Seabrook, 2017). Four of the practice papers were from clinicians writing to review an area of their practice or providing their own guidance from experience within the field (Casey et al., 2019; Collins, 2008; Innocente, 2014; McDonald et al., 2004). The remaining three were projects from the specialist interest groups National Association of Equipment Providers and Postural Care CIC, exploring relevant evidence, policy and guidelines, then making recommendations for future service provision (Clayton, 2013; Hill, 2011; Kent, 2015).
This demonstrates that clinicians on the front line have recognised a need for postural management and are beginning to implement interventions and seek out an evidence base for this. In addition, this suggests that they are searching for policy or guidance to steer them and to share their findings with peers, indicating that posture management is a tangible issue that is increasingly part of standard Occupational Therapy practice.
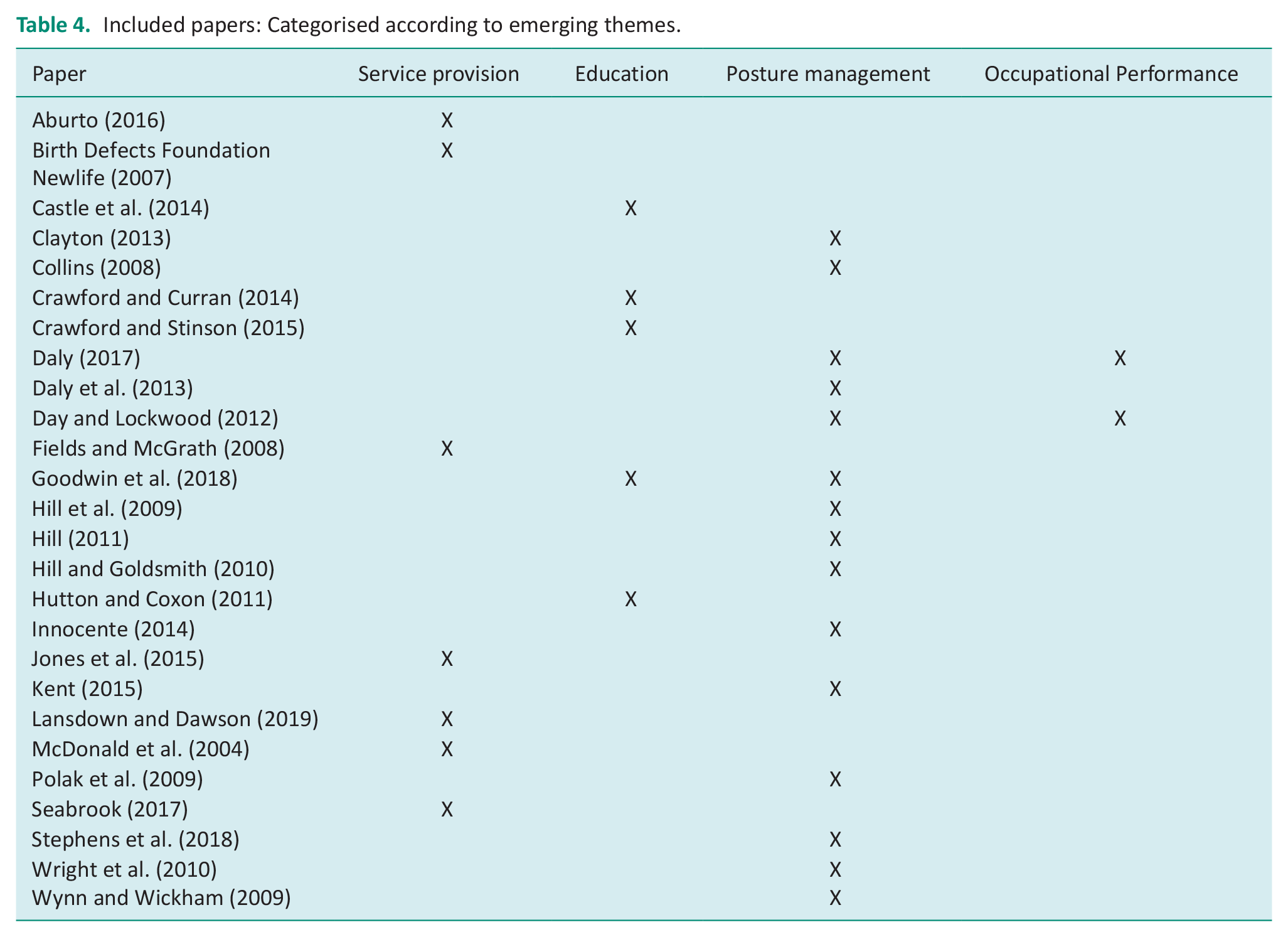
The team discussed the themes and further analysis condensed these into four over-arching themes which were then linked back to the primary objective (see Table 4):
Education on posture management
Posture management across the three primary positions
Impact on occupational performance and participation
Service provision
Included papers: Categorised according to emerging themes.
Education on posture management
Literature identified similar definitions of posture management as the use of a range of techniques that can be used to preserve body shape to prevent secondary complications, promoting a symmetrical body shape and enhance function and participation, whilst recognising that its use is mainly directed at individuals who are unable to change their position independently (Castle et al., 2014; Crawford and Curran, 2014; Crawford and Stinson, 2015). These benefits to health and wellbeing will have an impact on the individual’s quality of life.
There was also a clear, defined need for 24-hour posture management, recognising that many of the secondary complications that can occur due to lack of posture management are avoidable and therefore, clinicians have a duty of care to prevent their development (Castle et al., 2014).
In addition, there is a need for further training for healthcare professionals in prescribing postural care techniques and associated devices as well as for families and carers at how best to apply those techniques and devices. Castle et al. (2014) found that most staff within the multidisciplinary team had no understanding of the need for postural management and they did not have any assessment tool for identifying need. Instilling staff and family knowledge and understanding of the need for posture management and the benefits it can produce, will help to alleviate any fear or anxieties of not applying postural supports appropriately and reduce the risk of causing harm (Goodwin et al., 2019; Hutton and Coxon, 2011).
Posture management across the three primary positions
Impact on occupational performance and participation
It is recognised that provision of appropriate postural seating can increase participation in activities through improving the accessibility and awareness of the environment, as well as enabling individuals to be more functional in a better supported position (Daly, 2017). The involvement of Occupational Therapists in the provision of seating offers a distinctive approach in how positioning affects a person’s ability to participate (Day and Lockwood, 2012). Sleep is often overlooked as an occupation, plus having good sleep can have additional positive benefits to daytime occupational engagement.
Service provision
McDonald et al. (2004) referred to the Audit Commission (2000) report ‘Fully Equipped’ as emphasising poor strategic and operational methods for delivery of mobility services. The disbanding of healthcare services has subsequently resulted in a postcode lottery of service provision, with much confusion not only amongst members of the public, but also health and social care professionals about where and what funding is provided, and often with insufficient budgets allocated (Birth Defects Foundation Newlife, 2007). The lack of providing adequate individualised postural support devices, whether it is an armchair, night-time positioning system or a standing frame can lead to more complex postural deformities developing and therefore ultimately present a higher cost, requiring more specialised care and equipment for long-term care plans, which could be prevented. Also, adopting a pro-active intervention at the outset would often reduce the likelihood of the individual having pain and developing preventable secondary complications (Daly, 2017). The numbers of people requiring posture management equipment are a relatively small proportion of an overall clinical group. However, their needs are more complex and therefore use a greater proportion of the limited resources (Aburto, 2016). It could be assumed that if their postural needs were addressed early before they deteriorate and become non-reducible requiring complex care, more resources would be available to share. On a positive note, dedicated posture management services are starting to emerge in different areas across the UK (Aburto, 2016; Crawford and Curran, 2014; Fields and McGrath, 2008; Robertson et al., 2018; Seabrook, 2017). Further, several clinicians are now presenting on this topic at conferences (Daly, 2017; Day and Lockwood, 2012; Fields and McGrath, 2008; Jones et al., 2015; Lansdown and Dawson, 2019; Seabrook, 2017), which shows there is some innovation of service development across the professional field. With wheelchair services in much of the UK often being tendered to private providers, competition for contracts could be an opportunity to drive pioneering service provision to offer an advantage over competitors (Daly et al., 2013). This could present an opportunity for posture management to become embedded into wheelchair services and enable a more rounded and coordinated 24-hour postural management approach to be adopted.
Discussion and recommendations
There currently is no global interest group or platform for influencing postural care on a wider scale. Therefore, initial recommendations are tailored to improve the provision of postural care within UK practice. Many papers identify a lack of robust evidence for posture management techniques and interventions, all recognising there was a lack of randomised control trials (RCTs). Although often perceived as the ‘gold standard’ of research design, complex rehabilitation does not easily lend itself to RCTs. It would be unethical to withhold posture management interventions when the harmful effect of gravity on body-structures is well recognised. Further, blinding of the researchers on whether postural supports are used or not would be difficult depending upon the type of outcome measures employed; thereby making it very difficult to have a treatment group versus control group. Much of the literature cited in this scoping review is based on specialist clinical knowledge and expertise gained from real-life experience of working with the complex population who require posture management.
There are multiple authors from this field with similar conclusions; namely that 24-hour posture management can prevent the development of secondary complications, pressure ulcer development and improve health and wellbeing outcomes so that people are able to engage in occupation to live a more meaningful and comfortable life. Considering Humphreys et al.’s (2019) conclusions, a consensus of expert opinion on the subject would be beneficial to drive this agenda forwards into development of policy to guide assessment of need and provision of intervention. Therefore, it is recommended that a consensus paper on 24-hour posture management is produced, leading to development of national policy and guidance for Clinicians, individuals and their carers in the delivery of postural care for all people that have complex physical needs and who are at risk to the effects of gravity on their posture. It is important to recognise that this is an issue that does not only affect one client group and this work presents an opportunity to guide the creation and delivery of postural care services for all who need it. At present, there are guidelines around pressure ulcer prevention (NICE, 2014) and spasticity management in under 19’s (NICE, 2012) but these do not go far enough to recognise that habitual asymmetric postures can affect any person with complex physical disabilities, all age groups, all positions, and those unable to change their position independently.
Funding is a key barrier for preventing access to postural care. According to the Human Rights Act (1998), everyone has a ‘right to life’ and the secondary complications caused by poor posture management have been presented as a cause of premature death. Therefore, access to postural management services is a human right. The Audit Commission (2002: 4) stated that commissioning was a real problem for the provision of equipment and that ‘service commissioners and providers generally have no idea about the underlying level of demand for equipment services. Unmet need represents a major cause of social exclusion’. This is reflected in the findings from the Birth Defects Foundation Newlife (2007) campaign report; and in the Guidance for Postural Care and People with Learning Disabilities, Public Health England (2018), it is stated ‘It is recommended that clinical commissioning groups should ensure they commission expert, preventative services including proactive postural care support’. It has been reported that current service provision is patchy and inconsistent. With postural care being so devolved and postural supports for the three orientations of lying, sitting and standing being provided in isolation, or not at all, the current provision falls far short of the joined-up service that is advocated. To address this, development of a dedicated posture management service where all postural care needs and equipment is assessed for and provided as part of a holistic, 24-hour approach is recommended. This provides an opportunity to reduce duplication and ensure that all prescribed devices and recommendations work collectively.
For postural care to be recognised and delivered appropriately, it is proposed that universities in the UK and Ireland must include posture management training for undergraduate students and that training is multidisciplinary (Collins, 2012, cited in Kent, 2015). Additionally, training is required for families and carers of people who need postural care to ensure they are competent and confident to transfer and position the individual using the equipment so that it is used effectively and does not cause more harm (Blake et al., 2015; Hill et al., 2009; Polak et al., 2009). Posture management equipment is often very expensive and therefore, not investing in training families and carers in how to use it effectively, is a waste of resources and can have a negative effect for the individual through insufficient or incorrect posture management (Polak et al., 2009).
A limitation of this scoping review could be the exclusion of standing for which there is already an extensive body of published literature, particularly within physiotherapy. The authors recognise that standing is a vital strand of 24-hour postural care programmes and it is important that physiotherapy colleagues are part of the overall pathway. Another limitation is, there was no analysis on the complexity of postural supports used. For example, night-time positioning did not differentiate between using simple off-the-shelf pillows and wedges or a custom-moulded system. It was also acknowledged that none of the literature explored the perspective of the person using the assistive devices, although some did comment on the carer’s perspective.
As highlighted by Blake et al. (2015), it is important to be mindful when reviewing literature in this field of any potential bias and ethical concerns regarding objectivity when manufacturers may have sponsored research or provided assistive technology devices.
Conclusion
A scoping review was conducted to examine the evidence for 24-hour posture management, which is regarded as necessary to reduce the effects of postural asymmetries and gravity on people that are unable to change their position independently and prevent the development of postural deformities and pressure ulcers. Whilst the evidence for 24-hour posture management may not be considered robust or of sufficient research quality, there is evidence none-the-less that holds weight and is valuable in guiding future practice. There are clear health and wellbeing benefits from the provision of 24-hour posture management for people who are unable to change their position independently.
Current NHS service provision for posture management and commissioning is weak and insufficient. The resulting postcode lottery of service provision is inadequate (Birth Defects Foundation Newlife, 2007) and failure to provide adequate posture management can be considered a safeguarding issue and a breach of human rights (Gowran, 2020). Therefore, to advance the posture management agenda, we urgently need to develop national guidance and a posture care pathway informing future practice. There are opportunities for the development of a dedicated posture management service through the expansion of current wheelchair services to include the provision of night-time positioning equipment, standing frames and postural static seating.
Key findings
Current NHS provision of posture management is inadequate, resulting in unmet needs.
Research in this field is challenging; subsequently, greater credibility should be attributed to specialist expertise.
National guidelines are needed.
What the study has added
This review identifies the need for best-practice clinical guidelines on 24-hour posture management; scope for dedicated posture management services and increased training throughout the Occupational Therapy profession on 24-hour postural management intervention.
Footnotes
Acknowledgements
The primary author expresses sincere gratitude to Millbrook Healthcare and to the Oxford Brookes Healthcare Librarians.
Authors’ note
Jackie Casey is now affiliated with Advanced Occupational Therapist Practitioner, Regional Wheelchair: Training, Research & Service Development, Belfast Health & Social Care Trust, Belfast, Northern Ireland; Discipline Occupational Therapy, Faculty of Education and Health Sciences, School of Allied Health, Health Research Institute, Health Implementation Science and Technology, University of Limerick, Limerick, Ireland.
Research ethics
Ethics approval was not required for this study.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted as part of an MSc, which was funded by Millbrook Healthcare.
Contributorship
LO researched literature and conceived the study. LO and JC developed search strategy. LO completed literature analysis. LO wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.