
Abstract
Objective
Developmental Coordination Disorder (DCD) and Attention-Deficit/Hyperactivity Disorder (ADHD) persist into adulthood; however, little research exists to describe how adults with DCD and/or ADHD cope with their symptoms. Therefore, the purpose of this study was to investigate coping mechanisms reported by adults with DCD, ADHD, or both conditions. We expected there would be strategies specific to each condition and a broader scope of mechanisms reported by those with co-occurring DCD+ADHD.
Method
N = 161 participants completed the online survey, including n = 31 with DCD only, n = 116 with ADHD only, and n = 14 with DCD+ADHD.
Results
Most participants reported adaptive strategies. Of these, behavioral adaptations were most relevant to ADHD, while environmental modifications were common in DCD. Cognitive reframing and social support were similarly relevant to those with DCD and DCD+ADHD. Coping strategy categories were most uniform for the DCD+ADHD group.
Conclusions
Coping profiles highlight several noteworthy differences between DCD and ADHD which may be relevant for treatment.
Developmental Coordination Disorder (DCD) and Attention-Deficit/Hyperactivity Disorder (ADHD) are both neurodevelopmental disorders which are known to co-occur in up to 50% of cases (Blank et al., 2019). The two conditions have unique primary symptoms required for diagnosis; DCD involves developmental delays in learning and execution of fine and gross motor functions, while ADHD is characterized by general impulsivity, hyperactivity, and/or inattention (DSM-5: American Psychiatric Association, 2013). While DCD and ADHD are separate conditions, there are numerous overlaps in the mechanisms linked to their symptoms. For example, certain motor functions require simultaneous deployment of attention and motor coordination (e.g., riding a bike and avoiding incoming traffic at an intersection). Hyperactivity may also interrupt the control of fine movements, and has been shown to negatively impact children with DCD compared to typically developing controls (Harrowell et al., 2018). Furthermore, both executive functions in DCD and motor skills in ADHD were reported to be reduced compared to typically developing peers (Bernardi et al., 2015; Sartori et al., 2020; Tal Saban et al., 2014; Kaiser et al., 2015; Kurdziel et al., 2015). Such considerable overlap between the symptoms persists even if the co-occurrence of ADHD or DCD is accounted for and subsequently separated in analyses (e.g., Meachon et al., 2021).
While formerly thought to be disorders of childhood, it is now clear that both DCD and ADHD persist into adulthood (Blank et al., 2019, Tal Saban and Kirby, 2018).
Furthermore, both conditions can have negative psychological and social consequences in adulthood, including reduced wellbeing, lower mood, and increased depression and anxiety in many individuals with DCD (Draghi et al., 2019; Kirby et al., 2013; Omer et al., 2019; Mancini et al., 2019; Zwicker et al., 2018). In order to manage their symptoms into adulthood, those with DCD and/or ADHD develop sophisticated coping mechanisms (Wilmut, 2017; Kysow et al., 2017). It is possible that the overlaps in symptoms and psychosocial consequences of DCD and ADHD may promote the manifestation of similar coping mechanisms among adults. However, to date there are no studies which have examined coping mechanisms in adults with co-occurring DCD and ADHD, and there are few studies in general which address coping with DCD. Therefore, in the present study, we explore and compare coping mechanisms in adults with both DCD and ADHD for the first time. Understanding the strategies patients use could support improving the treatment process and treatment outcomes (Canela et al., 2017; Algorani and Gupta, 2020), as well as provide insights to individuals with DCD and/or ADHD who are searching for strategies to cope with their symptoms.
Coping with DCD and ADHD
Coping mechanisms may aid in the progression of symptom management before patients seek treatment (i.e., adaptive coping). However, dysfunctional coping (i.e., maladaptive coping) can be central to the maintenance of symptoms (e.g., avoidance in anxiety; Alpers, 2010). Therefore, understanding coping mechanisms is particularly important to build an effective treatment plan for patients, and can influence the progression of both physical and mental disorders (Algorani and Gupta, 2020).
Several studies have examined the coping mechanisms used to manage symptoms of adults with ADHD in particular (e.g. Kysow et al., 2017; Canela et al., 2017). Those with ADHD previously reported using coping mechanisms in the categories of social skills, organizational skills, attentional skills, motor skills, psychopharmacological methods, task adaptation, and avoidance (Canela et al., 2017; Kysow et al., 2017). One study compared adults with ADHD to typically developed adults in approaches to stressful situations and found those with ADHD were significantly more confrontative, used escape-avoidance more often, and practiced significantly less planful problem-solving (Young, 2005). On the other side, those with ADHD also used significantly more positive appraisal than typically developed adults in approaching stressful situations (Young, 2005).
Regarding those with DCD, one phenomenological study recorded the experiences of young adults with DCD during in-depth interviews, including the coping strategies they found helpful to manage symptoms (Missiuna et al., 2008). In symptom management, participants reported (1) using avoidance or withdrawing from activities, (2) finding an activity in which they could succeed, (3) using humor, (4) modifying the rules or their role in an activity, (5) and persevering through challenging activities (Missiuna et al., 2008).
It has been suggested that individuals with DCD compensate for their symptoms into adulthood despite numerous constraints from motor symptoms (Wilmut, 2017; Meachon et al., 2022b) and that similar methods may be employed in order to manage the symptoms of ADHD (Kysow et al., 2017). Evidence from brain-behavior comparisons showed such compensatory mechanisms may be performed the extent that symptoms may not be overtly observable in behavioral tasks in adults DCD and ADHD (e.g., Meachon et al., 2021).
Therefore, in order to better inform the treatment process for DCD and/or ADHD, it is important to improve the understanding of types of compensatory mechanisms used by adults with DCD and/or ADHD and the extent to which they overlap.
The psychological relevance of DCD and ADHD
Understanding how patients cope with symptoms in general (i.e., including primary and secondary symptoms) can provide an important holistic perspective for complex conditions such as DCD and ADHD. This is especially necessary for DCD given that there is a limited set of known effective treatments for patients (Smits-Engelsman et al., 2018) despite increasing evidence suggesting secondary anxiety and depression is common for those with DCD (Tamplain and Miller, 2020; Omer et al., 2019; Mancini et al., 2019; Kirby et al., 2013). At present, established treatment for DCD is primarily based around primary (motor) symptoms, and it is recommended to practice specific skills relevant to the patient (Blank et al., 2019; Smits-Engelsman et al., 2018). However, there is increasing evidence indicating that psychological therapy may be beneficial for individuals with DCD (Caçola et al., 2016) and an important push for more research on psychotherapy for DCD patients (Tamplain and Miller, 2020).
Conversely, effective evidence-based treatment approaches are better understood for ADHD. Aside from psychopharmacological approaches, psychotherapeutic options include cognitive-behavioral therapy (CBT), psychoeducation, and family and marital therapy (e.g., Kolar et al., 2008). However, there is still more research needed to address certain treatment approaches in ADHD, such as the relevance of motor skill training options given the relevance of motor symptoms in children with ADHD and undertreatment of these symptoms (Fliers et al., 2009), particularly in the case of co-occurring DCD and ADHD.
It is important to screen for DCD in cases of ADHD in research and clinical practice (Fliers et al., 2009). However, there is a lack of screening for DCD in studies of ADHD populations, and vice versa. Therefore, it is important to examine if motor skills are important in the profile of coping mechanisms for individuals with ADHD versus those with only DCD or co-occurring DCD and ADHD.
Current study
Beyond the phenomenological study by Missuna et al. (2008), to our knowledge, there are neither wide-scale studies to assess coping mechanism in adults with DCD, nor studies to compare and contrast the coping mechanisms relevant to DCD and/or ADHD. This motivated the present study, in which we collected open-ended responses and other information (see Questionnaires section) regarding coping with relevant symptoms in groups of adults with DCD, ADHD, or DCD + ADHD. We systematically classified responses to several theory-driven categories of adaptive or maladaptive coping strategies (see Appendix A), and provide insights for the varying patterns of responses in each group.
We expected that (1) there would be specific patterns of coping mechanisms for DCD compared to ADHD, and (2) that an increased amount of coping mechanisms would be used by the adults with DCD and ADHD compared to those with only DCD or ADHD.
Given the response-based approach to coping strategy classification, as well as the novelty of the present study focused on DCD and ADHD beyond childhood, we conducted several additional analyses with standardized instruments. This included comparisons between reported coping mechanisms and scores on DCD symptom and coping strategy questionnaires.
Method
Participants
A total of N = 197 adults with a reported symptoms Developmental Coordination Disorder (DCD), Attention-Deficit/Hyperactivity Disorder (ADHD), or both DCD and ADHD filled in some of the online survey in English or German. Of this total, n = 22 did not have a confirmed diagnosis of DCD or ADHD, and n = 14 participants left the open-ended questions incomplete, leaving a remaining N = 161 participants with a previous diagnosis of DCD and/or ADHD in the present study. Among them, n = 31 had a diagnosis of DCD, n = 116 had a diagnosis of ADHD, and an additional n = 14 were diagnosed with both ADHD and DCD.
There were n = 40 English-speaking and n = 121 German-speaking respondents. The age of participants ranged from 18 to 62 years old were (M = 35.1; SD = 11.3). Participants were 65.8% female, 31.7% male, and 2.5% non-binary, transgender, or other gender identities (unspecified).
Procedures
This study was linked to another survey testing the Adult Developmental Coordination Disorders/Dyspraxia Checklist (ADC; Kirby et al., 2010; Meachon et al., 2022a). Therefore, following virtually signed informed consent, all participants began by filling out the ADC, then demographic information, diagnostic history, and coping strategies they used to manage DCD and/or ADHD. More specifically, participants were asked the following questions: “Can you describe any compensation strategies or coping mechanisms you have developed to deal with the coordination issues or the symptoms of your [condition] in your daily life?” and “Can you describe any strategies or coping mechanisms you have developed that might have exaggerated your coordination issues or symptoms of your [condition]?”, where (condition) was DCD/Dyspraxia, or ADHD/ADD. Responses to these questions were given in open text fields for adaptive and maladaptive coping, respectively. Following this, participants completed the Brief COPE (Carver, 1997). The study was conducted online though the SoSciSurvey platform (soscisurvey.de) from March to December 2019 in English and German and was approved by the University of Mannheim ethics committee.
Questionnaires
To assess symptomatology relevant to DCD, the survey included the 40-item Adult Developmental Coordination Disorders/Dyspraxia Checklist (ADC; present study α
Data preparation and strategy classification
Classification of coping strategies and group counts.
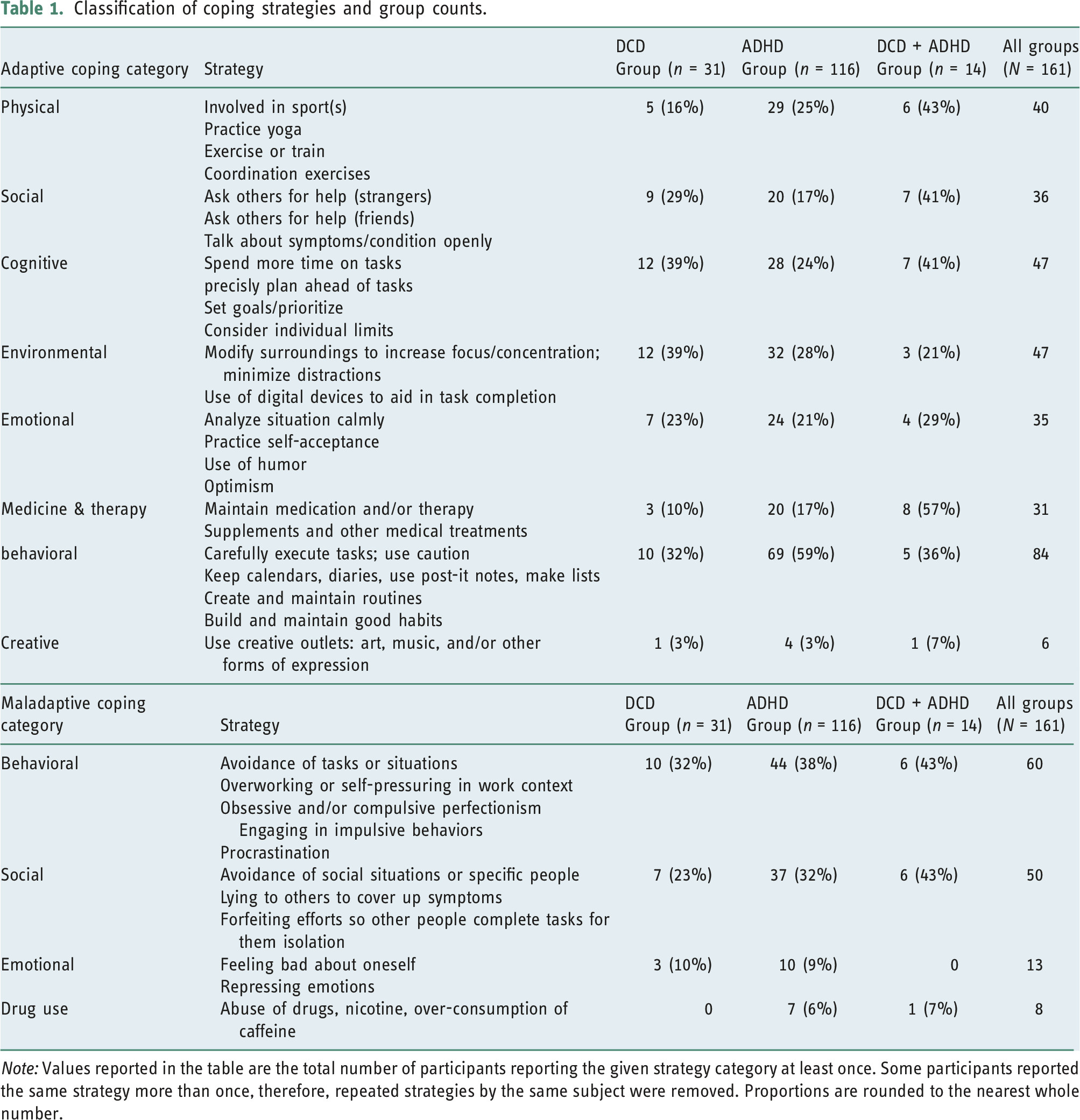
Note: Values reported in the table are the total number of participants reporting the given strategy category at least once. Some participants reported the same strategy more than once, therefore, repeated strategies by the same subject were removed. Proportions are rounded to the nearest whole number.
The German and English language groups were compared before concatenating the two datasets to determine if substantial differences existed based on language group. There were significantly more participants with DCD in the English-speaking subset; however, no other demographic characteristics were significantly different.
Results
Categorization of reported strategies
In general, participants reported an average of 1.2 adaptive (Range: 0–3) and 0.4 maladaptive strategies (Range: 0–3) for coping with DCD symptoms, and average of 1.4 adaptive (Range: 0–3) and 0.6 maladaptive coping strategies (Range: 0–3) for ADHD symptoms.
Several descriptive patterns in reported coping mechanisms existed between groups (see Figure 1). Participants with only ADHD most often reported using behavioral modification techniques to cope adaptively (59%), while those with only DCD and both DCD and ADHD most often reported coping adaptively through the use of cognitive reframing (39%, 43%, respectively). For maladaptive coping, all groups reported behavioral mechanisms (e.g., avoiding tasks) most often (DCD: 35%, ADHD: 39%, DCD + ADHD: 36%), and the DCD + ADHD group reported an equal proportion (36%) for maladaptive social behaviors (e.g., avoiding people or gatherings). See Figure 1 for proportions by group, across coping classifications. Proportions of adaptive and maladaptive coping strategies reported per group.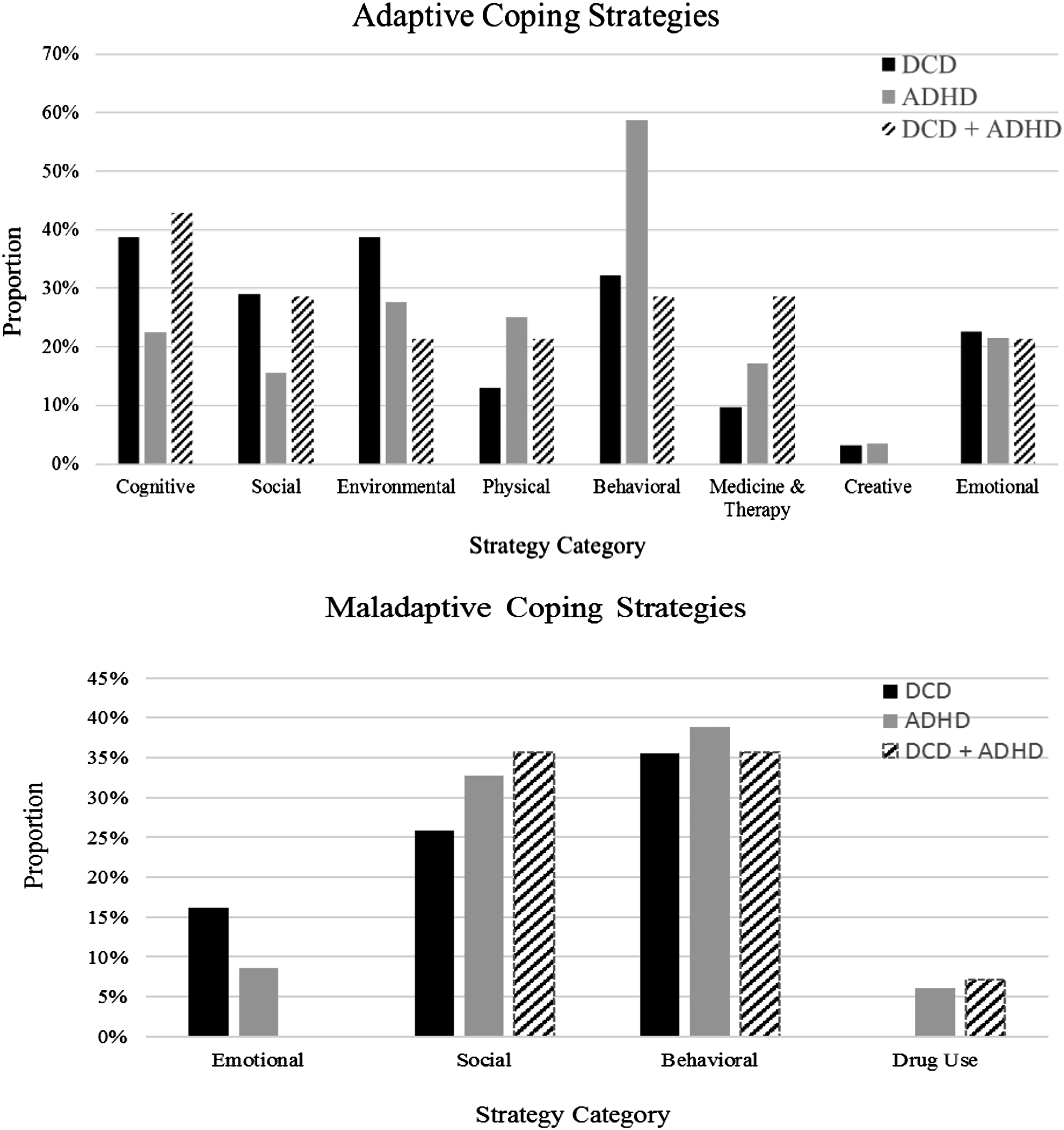
The type of adaptive strategies reported varied between groups for behavioral strategies [F (2, 79) = 3.45, p = 0.037] and strategies related to the use of medication or therapy [F(2, 24) = 4.97, p = 0.016]. Post hoc testing with Tukey’s LSD revealed the difference in behavioral strategies was driven by more behavioral strategies reported by the ADHD group (M = 1.65, SD = 0.80) compared to the DCD group (M = 1.10, SD = 0.32). However, the difference in medication/therapy use was driven by significantly higher reported use by the DCD + ADHD group (M = 1.75, SD = 0.50) compared to the ADHD (M = 1.15, SD = 0.37) and DCD (M = 1.0, SD = 0) groups. There were no significant differences between groups in the number of maladaptive strategies reported by participants.
Analyses with standardized scales
Questionnaire responses on the ADC and Brief COPE were compared to several aspects of the reported coping mechanisms. First, overall ADC scores correlated significantly with number of adaptive coping strategies participants reported for DCD symptoms [r(160) = 0.191, p = 0.015] while a significant and negative correlation was present for ADC scores and the amount of adaptive coping strategies listed for ADHD [r(154) = −0.232, p = 0.004]. Overall ADC scores correlated positively and significantly with Brief COPE scores in the dimensions of self-distraction (r = 0.234, p = 0.004), behavioral disengagement (r = 0.196, p = 0.015), and venting (r = 0.215, p = 0.008). There was a significant effect of group on overall ADC scores [F(2, 158) = 7.7, p = 0.001], with the DCD + ADHD group scoring the highest (M = 113.7, SD = 12.2), followed by the DCD group (M = 106.2, SD = 18.4), and the ADHD group (M = 96.9, SD = 18.3).
In addition, there was an effect of group on Brief COPE planning subscale scores [F(2, 150) = 5.38, p = 0.006]. Post hoc testing via Tukey’s LSD revealed this difference was primarily driven by a significant difference between planning subscale scores of the DCD (M = 5.04, SD = 1.89) and DCD + ADHD (M = 6.97, SD = 2.00) groups, such that the DCD + ADHD group scored significantly higher (p = 0.004).
Discussion
The present study revealed a wide variety of coping mechanisms were regularly used by participants to cope with DCD and/or ADHD, especially to cope adaptively. As we expected, there were several patterns in the reported coping mechanisms, where some were more common to DCD (e.g., cognitive, social, and environmental) and others to ADHD (e.g., behavioral). As we further expected, those in the DCD + ADHD group had especially varied coping mechanisms compared to the DCD or ADHD groups, potentially reflecting a wider breadth of compensatory strategies to manage a greater symptom load.
Differences in coping in DCD versus ADHD
There were several noteworthy trends in some of the various themes of reported coping mechanisms in the ADHD group. Interestingly, the highest proportion of a strategy type reported by any group was behavioral changes (e.g., making to-do lists, following routines) listed by participants with ADHD. This aligns with major components of several successful forms of therapy for ADHD, such as CBT (Kolar et al., 2008) and signals the substantial importance behavior-based strategies had for individuals with ADHD in this study. Otherwise, environmental changes, physical training, and emotional regulation were reported for more than 20% of participants with ADHD, signaling they might be relevant to some ADHD symptoms. In particular, physical training and motor therapy was noted to be relevant to ADHD, but underused (Fliers et al., 2009).
As for the DCD group, cognitive strategies and environmental modifications for adaptive coping were the most frequently reported categories of coping strategies. Among participants with DCD, there was only a small difference between rates of reported cognitive, environmental, social, behavioral, and emotional adaptive coping strategies. Given the frequently reported use of behavioral and cognitive strategies among those with DCD, the application of CBT for DCD patients should also be considered in treatment. Existing treatment for DCD is generally most substantially grounded in motor-based training, such as Cognitive Orientation to daily Occupational Performance (CO-OP; Sugden, 2007). While CO-OP is highly effective in supporting and facilitating motor learning and sources elements of CBT (Smits-Engelsman et al., 2013), it does not address concerns beyond motor skill acquisition and training. Even if symptoms initially stem from motor problems, they may manifest later as larger concerns (i.e., avoiding social situations) which necessitate interdisciplinary interventions. This may be especially important for overcoming maladaptive coping patterns in cognitive and behavioral realms. As demonstrated in this study, participants consistently reported maladaptive behaviors more often than any other form of maladaptive coping.
The use of adaptive social support by participants with DCD in the present study is encouraging, as teenagers and young adults with DCD can have self-reported feelings of strain in social relationships with peers, family, and friends based on their symptoms (Payne et al., 2013; Tal Saban and Kirby, 2019). Those with DCD who did report the use of social support often reported simply informing their peers, coworkers, or friends about having DCD was a productive way of coping. Social support may be particularly useful for those with DCD compared to ADHD given the limited psychologically based therapies (Tamplain and Miller, 2020) and lack of psychopharmacological interventions that can be used in treatment. The potential sources of social support and utility of disclosing one’s condition should be considered and discussed in treatment. At the same time, we acknowledge that this is not a trivial objective, as families can be affected by the symptoms of a loved one and may face related challenges (Weyers et al., 2019).
Notably, there were fewer reports of using physical, medicinal/therapeutic, or creative outlets to adaptively cope with symptoms in the DCD group compared to those in the ADHD or DCD + ADHD groups. It is possible that physical and therapeutic sources of coping are less relevant to DCD because motor symptoms are reduced by adulthood. For one, adults could have already completed one of the many effective motor-based therapies for DCD (Smits-Engelsman et al., 2013). It is also possible that individuals with DCD learn or teach themselves a variety of strategies to compensate for their motor difficulties over time (Wilmut, 2017), and as such, physical coping strategies are less relevant. The potentially reduced concerns in managing motor symptoms give way for treating lesser understood and undertreated secondary concerns of DCD (i.e., psychological; Meachon et al., 2022b) due to more options for effective physical training programs to manage DCD and learned compensation strategies for those with DCD (Wilmut, 2017). Psychotherapy could be useful in managing secondary symptoms of DCD (Caçola et al., 2016); however, more evidence is needed to determine the role and effectiveness of psychotherapy in treating DCD (Tamplain and Miller, 2020). As for those with ADHD, it is possible that motor symptoms remain untreated into adulthood (Fliers et al., 2009). Therefore, it is plausible that common motor skill interventions used for DCD may prove useful for those with ADHD as well.
Wider variety of coping mechanisms in co-occurring DCD and ADHD
Aside from creative outlets, the adaptive coping mechanisms reported by the DCD + ADHD groups were more uniform in distribution than the DCD or ADHD groups, reflecting a more widespread and less variable set of coping mechanism used. This could be reflective of a heightened symptom load, a pattern already observed in neural activity among those with both DCD and ADHD compared to just DCD or ADHD (e.g., Meachon et al., 2021). This could also be due to selection bias for participation as there was a small group size for those with both DCD and ADHD. Future studies should seek to replicate these results in larger groups and investigate the neural correlates related to coping mechanisms in DCD and ADHD versus only DCD or ADHD.
In addition, there was a significantly higher rate of reported use of medication and therapy in the DCD + ADHD group than the DCD or ADHD groups. As there are no medications proven to be effective for DCD, medication use is likely for management of ADHD symptoms, and potentially needed because of the increased symptom load of DCD and ADHD versus only ADHD. Interestingly, only participants in the ADHD or DCD + ADHD groups reported the use of drugs or caffeine as a maladaptive coping mechanism. While participants in the sample did not report having substance use disorders (SUDs) in their diagnostic history, there is a link between ADHD and SUDs and evidence of frequent substance use in other studies (e.g. Ohlmeier et al., 2011). To our knowledge, this link was not reported before with DCD, and the present study does not provide evidence of a link to be investigated further with substance use and DCD occurring alone. However, this link should be investigated further with ADHD patients, particularly among those with one or more co-occurring condition.
Similarities across all groups
Similar patterns were observed across all groups for some types of coping mechanisms. For one, the use of creative outlets was consistently the least common method reported among adaptive coping mechanisms. In the case of ADHD, unique profiles of creativity might exist even if underrepresented in terms of coping (White and Shah, 2011). This could be because explained by creativity as a means of expression with the arts (Andreasen, 2008), which is not necessarily linked to ADHD or DCD symptoms by participants in the present study.
Furthermore, emotional regulation strategies to cope with symptoms were similarly common across all groups. While it is unclear if such emotional regulation strategies are directly linked to managing the primary symptoms of DCD and/or ADHD or their secondary problems, there is evidence that internalizing symptoms are relevant to both disorders, especially in childhood (Mancini et al., 2019; Omer et al., 2019; Cairney et al., 2010). Future research should address the emotional regulation strategies sustained or developed across development for individuals with DCD and ADHD.
The most frequently reported maladaptive coping mechanisms were in behavioral and social realms for all groups. Many of these strategies were avoidance-based (of tasks or people), and align with findings previously reported among adults with ADHD (Canela et al., 2017; Kysow et al., 2017) and DCD (Missiuna et al., 2008). However, participants generally reported more adaptive strategies with greater variety than the reported maladaptive strategies. This may be because the nature of the word “coping” itself has a positive connotation (Skinner et al., 2003). It is equally possible that even a coping mechanism with negative consequences might outweigh dealing with symptoms of DCD and/or ADHD. The causal mechanisms surrounding maladaptive coping and symptoms of DCD and/or ADHD should be investigated in future research.
DCD symptom scale and the brief COPE scale
Beyond descriptive patterns of coping mechanisms, several interesting patterns were observed in relation to the ADC scores of participants in the current study. More specifically, increased intensity of DCD-relevant symptoms (i.e., higher ADC scores) related to more ways of productively coping with DCD. However, increased symptom severity of DCD was also related to decreased methods of adaptive coping strategies for ADHD, or vice versa. Despite the high overlap of symptoms between DCD and ADHD, it is possible that the coping mechanisms between these conditions are distinct. It is also possible that this result, instead, might be explained by underdiagnosis and undertreatment of DCD in the sample, which could be examined in a future study with an experimental design. Furthermore, while these correlations were significant, it should be noted they were of small magnitude. We argue they are meaningful results which describe the relationship between two distinct constructs: psychopathology versus behavioral responses in daily life and are important to examine in a replication study. Future studies should further consider examining the potential for undiagnosed DCD among those with ADHD, and participation in therapy in both groups.
Finally, Brief COPE scores were related to ADC scores in the domains of self-distraction, behavioral disengagement, and venting. Given that higher ADC scores generally indicate an increased presence and/or severity of DCD symptoms, it seems plausible that those with more pervasive symptoms could be reporting increased need to distract themselves, disengage, and vent in order to manage or avoid symptoms. Furthermore, coping by planning differed between the groups, where the DCD + ADHD group, indicated using planning significantly more than the DCD group. While additional investigations of the norms of the Brief COPE are needed, particularly in further comparisons of adults with ADHD versus control populations, this result aligns with the hypothesis that cognitive reframing and appraisal strategies are less commonly used by individuals with ADHD due to the symptoms of inattention (Young, 2005).
Limitations and future directions
There are several limitations of the present study which must be considered. First, the study was conducted in an online self-report format, and therefore, the coping strategies, diagnoses, and symptoms were examined non-experimentally. Despite the non-experimental design of this study and small sample sizes for some groups, a larger sample was recruited than possible in a lab study, thus increasing generalizability to several nationalities of adults with DCD and/or ADHD. This study also lays important groundwork to inform future research of the types of coping mechanisms used by those with DCD and/or ADHD. Although an examination of coping with (specific and unspecific) symptoms requires that samples are examined who actually do experience symptoms, future research should examine how these coping strategies generalize beyond coping with symptoms (e.g., Young, 2005). Such a perspective would then require comparisons with control groups. This would reveal, for example, whether the patient groups cope differently with attentional demands (daily distractions) or motor demands (learning new skills) than control participants.
In addition, the present study relied on participant recall for reported coping strategies.
Given the low averages of strategies reported, it is likely there were many strategies participants did not remember when completing the survey. Nonetheless, there was a wide variety of strategies reported across groups. Relatedly, it is likely the reported symptoms are those which are most relevant to individuals in managing daily DCD and/or ADHD. Of course, the frequency of some strategies may differ due to their availability (e.g., socioeconomic status and access to therapy). Future studies should not only study the self-selected coping strategies consider their effectiveness modifying responses to challenges and access to therapy.
Various therapeutic interventions should be examined for effectiveness among individuals with DCD in future research, with consideration of coping mechanisms used by the patient. It may be useful to consider the inclusion of interventions to treat anxiety or depression, for example, exposure to reduce anxiety and counter-avoidance used as dysfunctional coping (Alpers, 2010). Elements of these interventions may also be useful for supporting the development of healthy coping mechanisms for DCD and/or ADHD, as well as overcoming the common maladaptive coping strategies in these groups, that is, avoiding social situations or tasks.
Conclusions
It is important to understand coping mechanisms given the limited evidence for experiences among adults with DCD and ADHD. The present study identified several patterns in coping mechanisms used by all groups, including a greater number of reported adaptive strategies versus maladaptive strategies, as well as similar rates of reported use of emotional regulation and creative strategies across groups. There were several coping mechanisms that were more relevant to DCD, including environmental modifications and cognitive reframing, as well as those highly relevant to ADHD, including behavioral changes. Our findings attest to the symptomatic overlap but as well as uniqueness of the conditions. This information can be used to inform clinicians of several patterns to be aware of for adults with DCD versus ADHD, as well as combined DCD and ADHD. Furthermore, this study provides a foundation for future work regarding coping skills in adults with both DCD and ADHD. Overall, there is evidence that adults with DCD or ADHD have specific coping mechanisms, suggesting DCD and ADHD have unique symptoms.
Key findings
• Adults with DCD and ADHD have numerous, specific adaptive coping strategies • Maladaptive strategies were reported less often, and more uniformly across groups • Broader variability of coping strategies in DCD+ADHD may reflect wider symptom load • Behavioral strategies predominate in adults with ADHD; cognitive and environmental in those with DCD
What the study has added
The first study to examine coping strategies among adults with DCD, with comparisons to ADHD and DCD+ADHD groups. Results indicate necessity of multimodal support of adults with insights for treatment.
Footnotes
Acknowledgements
We would like to thank our participants for their time and effort completing our survey, as well as Annkathrin Schwier for her support in the recruitment process, and Julian Philipp Schaider for his efforts in data preparation. We would like to thank the Graduate School of Economics and Social Sciences at the University of Mannheim for their support in funding the present project.
Author’s note
Pilot data for this project was presented at the First Congress of the European Association of Clinical Psychology and Psychological Treatment in Dresden, Germany.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Graduate School of Economics and Social Sciences at the University of Mannheim through this affiliation of Emily Meachon.
Data availability statement
Ethics approval
Ethical approval for the present project was granted by the University of Mannheim Ethics Committee in 2018 and renewed in 2019.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.