
Abstract
Introduction
Canadian occupational therapists are employed as case managers on assertive community treatment (ACT) teams to support community living for individuals with severe and persistent mental illnesses. In this position, occupational therapists act primarily as generalists, typically attending appointments with clients, supervising medication adherence, supporting basic living needs, and managing client crises. Occupational therapists may also provide psychotherapy and coping skill groups, as well as profession-specific practices, such as skills training. Exploring how ACT occupational therapists describe their perceived ideal practice may support transformation in long-standing, occupational therapy practices on ACT teams.
Method
This qualitative, interpretive description study involved 11 Canadian ACT team occupational therapists in one individual, semi-structured in-depth interview using an interview guide containing open-ended questions. Interview transcripts were analyzed to identify themes pertaining to therapists’ descriptions of their perceived ideal occupational therapy practice on ACT teams.
Results
Three themes emerged: (a) Engaging in practice “with intention”; (b) Finding the space for occupational therapy practice; and (c) Supporting clients in their recovery to find their best occupational self.
Conclusions
The findings highlight practice possibilities for occupational therapist working on ACT teams and provide a foundation for advocating for better use of specific occupational therapy practices within community mental health settings.
Keywords
Introduction
Mental illness is one of the leading causes of disability in the world and can significantly impact an individual’s ability to engage in meaningful activities and participate in their communities (Vos et al., 2017). Occupational therapists are experts in enabling occupational performance and engagement and have practiced in mental health recovery in Canada since the early 1900s through interventions focused on return to work, psychotherapeutic techniques, and behavioral reactivation (Cowl and Hale, 2005; Moll et al., 2013, 2018). Many occupational therapists working in Canadian community mental health settings are part of assertive community treatment (ACT) teams. These multidisciplinary teams follow the ACT model to support individuals living in the community with severe and persistent mental illnesses and prevent potential costs from repeated hospitalization. This model focuses on preventing re-hospitalizations and holds a medical-based approach (Egan et al., 2010; Krupa et al., 2002). Currently, the practice of occupational therapists on ACT teams draws from domains outside of occupational therapy, such as case management, and predominantly involves supporting clients with attending medical appointments, managing medications, and refraining from using illicit drugs. While the Canadian occupational therapy profession has developed a strong occupation-centered perspective, the multidisciplinary scope of the occupational therapy role on ACT teams has remained stagnant (Drake and Deegan, 2008; Krupa et al., 2002; Stein and Test, 1980). Subsequently, this study presents the findings of a study exploring Canadian mental health occupational therapists' perceptions of “ideal practice” on ACT teams.
Literature review
Since the 1960s, deinstitutionalization has afforded individuals with severe and persistent mental illnesses the possibility of living in the community and has reduced costs from repeated hospitalization (Nakhost et al., 2017). ACT, created in response to deinstitutionalization, is a model of service delivery that provides treatment and support to individuals with continuous high service needs (Egan et al., 2010). The goal of ACT is to ensure that these individuals receive services needed to remain in the community and function optimally with the highest possible quality of life (Drake, 1998). The robust literature on ACT’s effectiveness, including reductions in hospitalizations and improvements in quality of life, has led this model to be adopted internationally (Bond and Drake, 2015; Svensson et al., 2018).
The disciplinary paradigm in which occupational therapy is embedded acknowledges the importance of performance and engagement in meaningful activities to support participation and quality of life. The core values of the practice are rooted in client-centeredness and occupation-centered approaches. As such, occupational therapists have a unique scope of practice that adds value within community mental health settings (Krupa et al., 2002) and is one of the professions to fulfill the rehabilitation requirements on ACT teams in Ontario (Ontario Ministry of Health, 2004). Since the ACT model is characterized by interdependence and sharing of roles and responsibilities across all team members, occupational therapists practice as case managers and engage in the role of a generalist mental health worker in addition to providing some profession-specific services (Krupa et al., 2002). Many studies recognize the distinct and unique contribution occupational therapy offers to community mental health practice, demonstrating the need for occupational therapists to practice in this domain. However, the ACT model poses a few challenges for occupational therapists. Its medical-based approach causes difficulties for occupational therapists in delivering collaborative, occupation-centered care consistently due to the prioritization of symptom management (Egan et al., 2010). In addition, the allocation of ACT staffing resources has left many teams with only one occupational therapist to fulfill the rehabilitation mandate of the service delivery model. The lack of a rehabilitation-lens representation poses an additional challenge for occupational therapists to integrate their professional values into practice (Krupa et al., 2002).
Study purpose and research question
There is a paucity of literature describing occupational therapy’s scope within the ACT model (Egan et al., 2010). Most of this literature investigates ACT team members’ perspectives on the barriers, facilitators, and effectiveness of implementing the ACT model, leaving a void in understanding the possibilities for practice change for occupational therapists working within the ACT model (Egan et al., 2010; Krupa et al., 2002, 2004). As such, this study aims to initiate a discussion of the ideal occupational therapy practice from the perspective of occupational therapists working on ACT teams. The research question for this study is “What do occupational therapists working on ACT teams in Ontario, Canada, perceive as their ideal practice?
Method
An interpretive descriptive qualitative design (Sandelowski, 2000) was used for this study to support the systematic inquiry and understanding of a phenomenon through individual perspectives within a specific social context (Portney and Watkins, 2015). The design was selected to capture the contextual and unique nature of each occupational therapist’s perspectives while elucidating the shared realities of similar workplace experiences within ACT teams in Ontario, Canada. Moreover, this design captures themes and patterns through subjective perceptions to generate an interpretive description (Thorne et al., 2004) that can be applied to inform an understanding of future community occupational therapy practice. As the primary purpose of this study is to explore the Canadian mental health occupational therapists' ideal occupational therapy practice on ACT teams, an interpretive descriptive design was deemed the most appropriate.
Participants and recruitment
Following ethics approval by the Health Sciences Research Ethics Board of the University of Toronto, purposive sampling was used to recruit participants. Using the authors’ professional networks, occupational therapists were recruited through occupational therapy contacts within hospitals, healthcare systems, and community health organizations with ACT teams. These contacts were asked to forward the study information to eligible occupational therapists. Interested participants contacted the researchers directly through email, and the researchers provided them with a letter of information and a consent form and informed them of the study’s purpose, time commitment, details around confidentiality, and potential risks and benefits of participation. If participants indicated continued interest, they were asked to sign and return the consent form prior to the interview. Snowball sampling was also used as some interested participants referred contacts from their own networks.
Participant demographics.
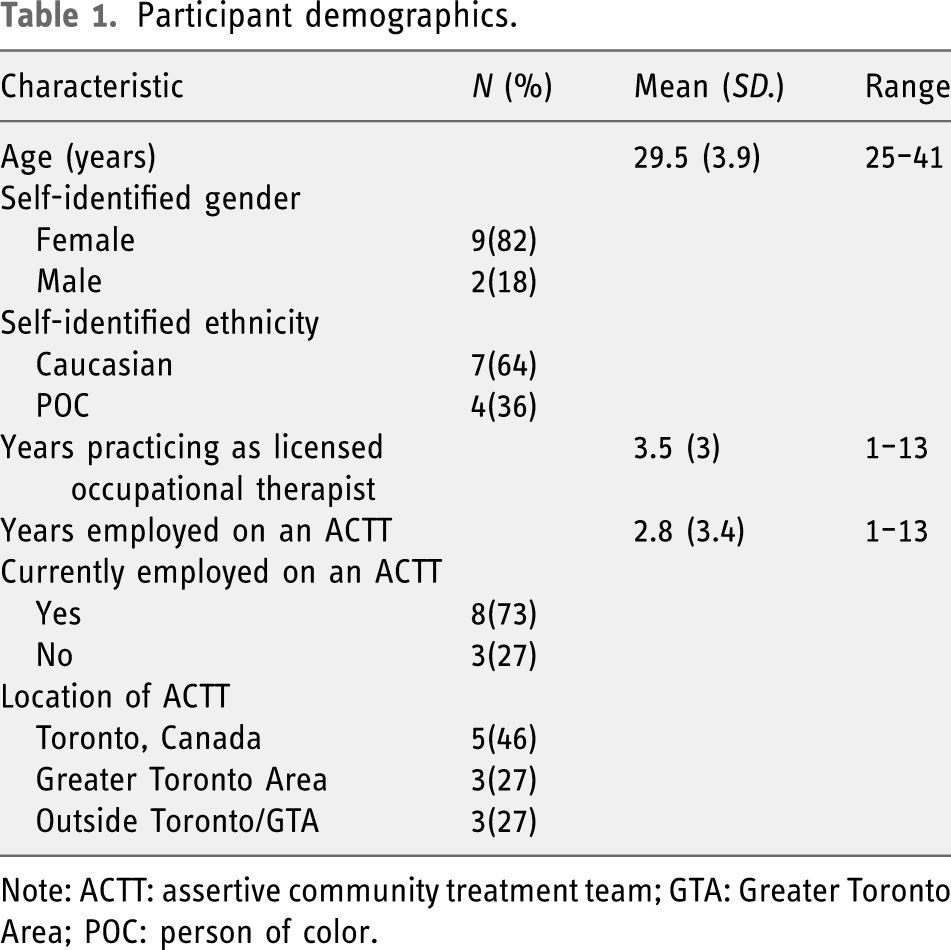
Note: ACTT: assertive community treatment team; GTA: Greater Toronto Area; POC: person of color.
Data collection
In line with an interpretive descriptive study design, data were collected using individual interviews. Demographic information and written informed consent were collected prior to the interview. Individual semi-structured interviews, lasting between 46 and 72 min, were conducted through video conference by two occupational therapy student researchers, trained and supervised by a faculty researcher. The interviews followed an interview guide comprised of open-ended questions and probes to promote rich discussions and further exploration of ideas. The interview guide was constructed by the three researchers to address the specific research question and was trialed by the two student researchers with two community mental health occupational therapists with between 5 and 10 years of experience, prior to commencing study the interviews. Both occupational therapists and the faculty supervisor provided feedback to the students on their interview technique and questioning, as well as suggestions for modifying the interview guide; examples of topics from the final interview guide were (a) practice background; (b) current work on the ACT team (current work tasks, feelings about current work, and general experience on team); (c) current applications of occupational therapy scope of practice (i.e., client-centeredness and occupation-based practice); and (d) vision of ideal practice on ACT team. As is typical with an interpretivist paradigm, the interview guide was modified as the interviews and preliminary analyses progressed to gain a more complete understanding of the emerging themes. All interviews were digitally audio-recorded and transcribed verbatim. All interviews were de-identified and assigned a code (P1 to P11), and the demographic information was aggregated to maintain confidentiality.
Data analysis
Following Braun and Clarke’s (2006) guide and consistent with the interpretivist paradigm, thematic analysis was used to analyze the qualitative data gathered from the in-depth interviews. This method allowed the researchers to identify what was common around topic discussions and make sense of these commonalities. Data collection and analysis occurred simultaneously and iteratively; the transcripts were independently reviewed and checked by the first two authors for accuracy through reading them multiple times and writing memos. Additionally, the first two authors independently coded the transcripts to uncover similar concepts, create categories, and formulate themes. No new themes emerged during the analysis of the 10th interview; an 11th and final interview was completed to ensure saturation. Once the initial themes were identified and defined, the entire research team reviewed and challenged the themes multiple times to arrive at a final consensus.
Trustworthiness
Following an interpretive descriptive analytic process, multiple strategies were used to enhance the trustworthiness of the analysis. An audit trail was kept throughout the study to maintain procedural dependability, ensure analytic transparency, and allow a pathway for others to follow. The audit trail included reflexive journaling, memo notes to record new ideas during the coding process, and decisions made during the review meetings, which supported confirmability of the research. The research team used personal journals to document their positionality before, during, and after data analysis. The transferability of the study was increased through purposive sampling, including the inclusion of current and former ACT occupational therapists, and rich descriptions of the participants’ perspectives.
Findings
This study explored ACT occupational therapists’ perspectives for ideal occupational therapy practice. Three themes emerged that convey the perspectives of 11 Canadian occupational therapists on ACT teams: (a) Engaging in practice “with intention”; (b) Finding the space for occupational therapy practice; and (c) Supporting clients in their recovery to find their best occupational self. All participants in this study were assigned a code (P1 to P11)
Engaging in practice “with intention”
Occupational therapists in this study described their ideal practice as engaging in practice “with intention.” Practicing with intention is defined as occurring when occupational therapists work with clients to set occupational goals and provide consistent support to enable their clients to achieve their goals throughout the complete practice process, including administering assessments, planning treatment, and carrying out interventions. One participant captured this theme broadly: I want to go visit with intention. I wish I was able to spend more time with clients that have OT [occupational therapy] goals but unfortunately that’s not the ACT model because we have to regularly rotate staff … I find that some visits are very unintentional, it’s just having coffee, talking about day-to-day activities. (P3)
This participant highlighted how as ACT case managers, occupational therapists are mandated to make rotational visits with all the clients on the team’s caseload, regardless of whether the client has an occupational goal. Thus, occupational therapists are often unable to achieve consistent follow through across the complete practice process. As such, participants expressed their frustration with having to make visits without an intention. I do the assessment and I could have as much time as I want with that—that’s good—but then I would make recommendations and it’s not necessarily me who would follow up those recommendations. It would be the team or the community partners for instance for cooking assessment; the recommendation might be a graded intervention plan to help gradually increase someone’s independence with cooking … It would be nice if I could do more of the carrying out of the plan … But it’s not really realistic. It’s kind of a shared thing among the team … Maybe you want to have a really precise plan with a gradually fading of supports, but you know, someone will [not] follow your instructions 100%. (P4)
Several participants alluded to practicing “with intention” as seeing clients more consistently to support them in progressing with their goals. If I can see people more, and more consistently so for example sometimes I’ll set a goal with a person and then I won’t see them for a month and a half … And the next time I see them their goals got lost. (P11)
Although many participants expressed challenges in practicing with intention, identified as inconsistent visits and the inability to follow-through on clients’ goals, others discussed advocating for the capacity to follow-up with client goals and practice consistently with intention. Specifically, one participant advocated for practice change so that she could see clients more often. When you see a client once a month, there’s no consistency there. So I was really able to advocate for consistency, where I would see the client based on how I felt and [what] the client felt they needed … I wouldn’t be on that rotation of seeing clients [who didn’t have occupational therapy] goals. (P2)
One participant discussed scheduling in advance as a strategy to work more consistently with clients with occupational therapy goals: If I was doing treatment with the client then I would try to schedule myself in advance to say I’m going with someone to the job, gym, to meet with an employment counsellor, or we’re working on exposure or whatever it is. I would try to schedule myself to go and see that person. (P11)
Finding the space for occupational therapy practice
Occupational therapy has a broad scope of practice that emphasizes the relationship among people, their environments, and their occupations. The participants spoke of wanting to have the space to carry out occupational therapy practice as a part of their ideal practice, beyond the dominant focus on case management. This theme is defined as reconfiguring their time and physical spaces to be able to engage in occupation-centered practice. P3 clearly conveyed this wish: “I wish that I was doing more OT [occupational therapy] things rather than case manager kind of things.” Similarly, P1 discussed “It’s like I don’t have time to do my OT stuff.” Participants found that by taking on a case manager role, they had insufficient space to work on client goals and other occupational therapy–specific practice. As P5 described in her ideal occupation-based practice: I really like doing behavioral scheduling so how can we build someone a nice routine. Like it might not be the same routine as the next person, the routine might just be getting up at the same time and trying to take a shower and going for a walk … It’s kind of my style of OT [occupational therapy].
However, she found that practicing within scope was often elusive within the context of the ACT model: I’m so busy delivering medication that the person I wanted to see to work on employment, that gets pushed to the side because that’s less important than the people who need their medication because they’re going to become unwell so that takes priority over the thing that maybe that person could have improved if I worked a little bit more on their employment goal but now I don’t have time for that kind of thing. (P5)
While most of the participants expressed needing more space for occupational therapy practice, a few felt that they were able to find this space through advocating for the profession and having supportive managers. P2 stated being able to find space for occupational therapy practice by, being very assertive on my team, and saying no that’s not what I do, I will not do that, … But I can do this, right? So given that’s not what I do, here is the education on what I do and here’s what can happen and giving clear goals and focusing on that.
As such, being an assertive advocate for the occupational therapy profession was a facilitator in finding space for occupational therapy practice. P3 also advocated for the profession through leading an “in-service on what OTs do” and felt “that really helped give [my colleagues] a view on what exactly we did.”
Although many participants articulated their ideal practice as finding the space for more occupational therapy practice, the role-blending of the case management model added further challenges. As P10 stated, The ACT team here, it’s very focused on generic duties, a lot of case worker roles, delivering medications to clients, assisting with transportation. It has been an ongoing struggle for me to make more of an effort to be more occupational therapy (OT) specific instead of generalist.
To address this, P11 stated “I think if the OT [occupational therapy] role had like a definition” as one of her strategies for finding space for ideal practice.
Finding the space for occupational therapy practice also included physical space. P8 explained that with “the lack of an office space conducive to providing an environment for socializing and the geographical barriers … There’s no room for us to host a group” (P8). P10 expressed using communal spaces in the community to run groups by building “a great partnership with the health unit, we run [groups] there because they have great spaces” (P10).
Many participants articulated specific occupational therapy practice that they would want to implement on ACT teams. P1 stated that he would like to focus on occupation and do more assessments related to activities of daily living (ADL). Most participants expressed interest in running more groups, including budgeting, social skills, and exercise groups. Overall, participants felt that providing space for occupational therapy practice would allow for occupation-centered enablement, thereby enhancing clients’ best occupational self.
Supporting clients in their recovery to find their best occupational self
In addition to finding the space for occupational therapy practice, the participants spoke of using this space to support their client’s recovery through working with them to discover their best occupational self. The participants described this process as enabling clients to imagine and dream of the “best version” of their “self,” and using it as the foundation to guide clients in their recovery journey. P5 stated, It [is] definitely like leading with the question of “what’s the best version of your life” as a way to gauge what they see for themselves for the future, and if they have their ideal life, what would that look like.
The notion of supporting clients to dream and define the “best version” of their occupational self is grounded in client-centeredness. Four participants defined this term as meeting the clients “where they are at” (P2, P7, P8, P11), focusing on the client’s values and self-identified occupational goals, and “being respectful and looking at the client as the expert in their care” (P10). In addition, helping clients find the “best version” of their “self” was consistent with a recovery perspective, which holds the core principle that recovery is unique to each client’s journey. As P2 stated, It goes back to being client-centered. I didn’t like the idea that this is the client, and this is where they are at, and this is what it’s going to be, you can’t change that. I just didn’t buy it … I think that it is possible for people to change, to grow, to recover, and that does not mean everyone is going to look the same. Recovery is going to look different for everyone.
Ultimately, the participants voiced that they wanted clients to find the “best version” of their occupational self through engagement in meaningful occupations and to ensure that their clients’ overall quality of life is being enhanced through living in the community. As P9 stated, I think an ideal OT [occupational therapy] practice is about really focusing on the value of a person’s health and well-being. Striving for quality of life, ensuring that they’re engaging in meaningful activities that really make them feel their quality of life is being met and really working on how we’re able to provide them support so they continue to stay in the community.
Furthermore, the participants expressed that working with clients in the community to uncover their capabilities, develop their skills, and facilitate opportunities to enhance their participation are ways for occupational therapists to support their clients’ recovery. P6 stated that she would like, “a lot more involvement with recreational programming, a lot more time spent in the community and a lot more ADL skill building.” Additionally, P11 highlighted the importance of helping clients uncover their current capabilities: “Let’s foster some independence and mastery and make you feel good about some of the skills you have. You have capabilities.” Participants felt that it was important to enhance client participation and uncover their capabilities in supporting their clients’ recovery.
Beyond learning and uncovering skills, participants felt that establishing supportive relationships with family members and caregivers was integral to a clients’ recovery journey. P4 expressed having relationships as closely linked to a client’s occupational success and occupational therapy practice: “You are helping families that are supporting their loved ones and then [the clients are] better able to carry out their occupations.” P2 created a caregiver support group that covered various topics, including stigma related to schizophrenia and bipolar disorder, and “felt that as a result of the group, families better interacted with their loved ones.”
If occupational therapists were given the space for occupational therapy practice, they used this space to support client’s recovery and help them find their best occupational self. This ideal practice involved taking a collaborative, client-centered approach to working with clients in the community on skill development and acquisition, participation and engagement, as well as providing support and education for their caregivers. Ultimately, the participants felt that their perceived ideal occupational therapy practice on ACT teams was helping clients find their best occupational self.
Discussion
This study explored the perceived ideal practice of Canadian occupational therapists regardless of the known barriers and challenges on ACT teams. Overall, the participants conveyed their desire to always practice with intention across the complete practice process, by finding spaces to demonstrate the full potential of occupational therapy practice to enable the clients’ recovery journey toward finding their best occupational self.
The participants described their ideal practice as engaging in practice “with intention,” which they defined as setting and working on goals with clients through the complete practice process consistently to achieve the clients’ occupational goals. However, participants often experienced role-blurring due to the prioritization of case management tasks over profession-specific service and were not able to engage with many clients as occupational therapists following initial assessments. Similarly, the literature highlights role-blurring for occupational therapists in community mental health with other healthcare professionals (Culverhouse and Bibby, 2008; Lloyd and King, 2001). In a study about professional resilience, participants spoke about how the pressure to take on nonoccupational therapy tasks, such as psychotherapy, within their mental health practice “diluted” their occupation-based skills, diminishing their perceived professional identity as occupational therapists (Ashby et al., 2013). In the current study, the participants were required to supervise medication adherence and transport clients to appointments—tasks guided by the dominant medical-based approach—as part of their case manager role, which always displaced their rehabilitation and recovery mandate as an occupational therapist on the team. ACT occupational therapists typically undertake many generic case management tasks, including medicine compliance, bloodwork, and housing. Such responsibilities can take priority over occupational therapy practice and undermine the traditional professional practice scope of occupational therapists (Brown et al., 2000; Horghagen et al., 2020), preventing practice “with intention.” Although the ACT model provides a unique opportunity for occupational therapists to engage individuals with severe and persistent mental illnesses, a well-known criticism is its focus on the immediate medical needs and a lack of consideration for a “formal component of rehabilitation” (Lauriello et al., 1999: 1412). Pettican and Bryant (2007) further argue that “working entirely generically will not best serve service users or the future development of the occupational therapy profession” (pp. 144–145).
The participants in this study described their ideal practice as having the space, including time and physical spaces, to provide more occupational therapy services to their clients and to achieve a more occupation-centered practice. Occupation-centered practice is defined as “adopting a profession-specific perspective—a world view of occupation and what it means to be an occupational being—where occupation is placed in the center and ensures that what we do is linked to the core paradigm of occupational therapy” (Fisher, 2013: 167). The participants perceived that their practice would be occupation-centered if they were able to implement more profession-specific evaluations and interventions. Many participants spoke about using groups as a means for occupation-centered practice as they provide an inclusive and nurturing space for occupational enablement (Lloyd et al., 2007; Sundsteigen et al., 2009).
Consistent with the literature, the current underrepresentation of the rehabilitation and recovery perspectives on ACT teams and the lack of balance between mental health generalists and specialists (i.e., occupational therapy; Horghagen et al., 2020) limit the development of occupation-centered practices in mental health (Krupa et al., 2002). Although occupational therapists in mental health contexts may face challenges in articulating their scope of practice (COT, 2007), the participants in this study were able to capture the potential of using their occupational lens and professional expertise on ACT teams. A study by Arntzen et al. (2019) identified four ideal types of occupational therapists practicing in community-based practice (not including mental health). Their participants spoke of “the innovator” as the “preferred” type, who would work to move away from performing generic tasks or tasks requested by other professionals to practicing professional autonomy. As with the current study, participants reported working on developing new programs and following through with client-centered goals and working on daily living skills (Arntzen et al.). Innovators used education, practice innovation, and client advocacy to find the time and physical spaces for occupation-centered practice.
The participants articulated that, ultimately, having the space for occupational therapy practice would enable them to support their clients’ recovery to find their best occupational self. The 2008 United Nations Convention on the Rights of Persons with Disabilities specifies rights for all persons living with a disability, including “the right to live in the community, participation and inclusion, education, health, employment, and social protection.” All participants strongly believed that their ideal practice would endeavor to support their clients’ right to create their best life living and participating in the community. However, they all experienced challenges with implementing their values in their practice. While the ACT model has evolved to include more recovery-oriented practices, these practices have low implementation (Odden et al., 2019). Research highlights that service providers on ACT teams experience difficulties in implementing specific key elements of rehabilitation, community integration, and recovery mandated by the ACT model (Krupa et al., 2004). Similarly, the participants in this current study envisioned their ideal practice as supporting clients in reaching their best occupational self through community integration, skills development and acquisition, and caregiver support groups; however, most participants were challenged to reach this ideal.
Implications for occupational therapy practice
The findings of this study emphasize the importance for occupational therapists, especially those hired into dual case-manager/occupational therapist positions, to explicitly define their unique scope of practice within the ACT model, beyond case management, as one focused on occupation-centered rehabilitation, community integration, and recovery. Although most participants felt that institutional and programmatic barriers limited their capacity to engage in practice “with intention,” they also highlighted ways that they were able to enact their ideal and unique scope of practice through education and client advocacy efforts within their teams with the aim of expanding the possibilities of their practice to better enable their clients’ occupational performance and engagement (Dhillon et al., 2010). Occupational therapists can provide educational sessions for their ACT teams on the scope of occupational therapy. They can also advocate for specific changes in scheduling and caseload by arriving early and being the first to speak up in team meetings to ensure that they are able to meet with the clients they feel will benefit the most from specific occupation-based services. For some clients, advocating for them to remain on an occupational therapist’s caseload can support follow through and attainment of the client’s goals.
In their study, Krupa et al. (2004) found that ACT practitioners were astonished by their clients’ limited family support and lack of opportunities for involvement in organized social and leisure occupations. The participants of our study felt that occupational therapists are well-positioned to address these client needs by creating educational support groups for caregivers and families and occupation-based groups for clients located within community spaces. Occupational therapist can lead client groups focused on teaching specific skills and strategies, such as cooking, budgeting, and social skills, with individual sessions supporting community integration through developing leisure and social occupations, as well as return to school and finding employment (Doroud et al., 2015; Wimpenny et al., 2014).
Limitations and future research
A limitation of this study is that 73% of the participants were recruited from Toronto and the Greater Toronto Area in Ontario, Canada. Given that the purpose of this study was to explore the ideal practice on ACT teams through the perspectives of Ontario-based occupational therapists, future studies should involve more participants beyond Toronto, Ontario, and eventually within different areas across Canada. Most participants were newer graduates with an average of 2.8 years of experience (refer to Table 1); only one participant had over 10 years of experience. Although the participants shared a range of perspectives, as this is the first study to the researchers’ knowledge that explores occupational therapists’ perspectives of ideal practice on ACT teams, future research should identify occupational therapists’ tasks, both within case management and in relation to rehabilitation and recovery, as well as age range and length of practice on ACT teams via survey methodology. Additional perspectives can be gathered by engaging a broader representation of ACT experiences using focus groups. Focus groups would support the creation of a shared understanding of ideal practice, which could lead to deeper and richer data (Thomas et al., 1995). Additionally, integrating individual interview and focus group data would support data triangulation and a deeper exploration of participants’ perspectives on ideal practice to enhance study credibility. More exploration is required to understand the full breath of ACT occupational therapists’ perspectives on ideal practice, and how this knowledge can be integrated into the ACT model.
Future research could also explore whether other health and social service professionals experience perceived or actual constraints on their ability to implement profession-specific practices. Systemic pressures within the health and social services toward reducing costs may lead to constraints on many profession’s ability to perform within their scope of practice.
Conclusion
This study adds to the current literature by exploring occupational therapists’ perspectives of ideal occupational therapy practice on ACT teams. The participants conveyed their desire to find space to practice with intention across the complete practice process to enable clients’ recovery journey toward finding their best occupational self. The ACT occupational therapists who participated in this study were often unable to fulfill their rehabilitation and recovery mandates as most of their time was devoted to case management duties. Role-blending on the ACT teams continually challenged their ability to use their unique skill set and enact their professional values to work with clients to enable occupational change; however, most found some way to introduce their profession-specific skills into their ACT practice. By generating knowledge of the potential for community mental health practice for occupational therapists, the findings of this study provide an initial perspective of how ACT teams can better integrate occupational therapists’ specialized skills to support clients’ recovery.
Key findings
Occupational therapists on assertive community treatment (ACT) teams perceive ideal practice as having space for profession-specific, occupation-centered practice. ACT occupational therapists’ case management duties impede their intentional practice.
What the study has added
This study provides an initial understanding of the practice possibilities for occupational therapists working on ACT teams and a foundation for advocating for profession-specific occupational therapy practice.
Footnotes
Acknowledgements
The authors would like to thank all the occupational therapists who participated in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research ethics
Ethics approval was obtained from the Health Sciences Research Ethics Board of the University of Toronto #38748–2020.