
Abstract
Introduction
Adults with spinal cord injuries are living longer than previously, and a majority are living in ordinary housing in the community. Housing accessibility is important for maintaining independent occupational performance for this population, but knowledge in this area is insufficient. We investigated housing adaptations and current accessibility problems among older adults with long-standing (>10 years) spinal cord injuries.
Method
Data from home visits among 122 older adults with spinal cord injuries in Sweden were used. Housing adaptations and environmental barriers were descriptively analysed.
Findings
Kitchens, entrances, and hygiene areas were common locations for housing adaptations and environmental barriers that generated accessibility problems. The most common adaptations were ramps, wheelchair-accessible stovetops, and ceiling-lifts. Wall-mounted cupboards and high shelves (kitchen), inaccessible storage areas (outside the dwelling), and a lack of grab bars (hygiene area) generated the most accessibility problems.
Conclusion
Despite housing adaptations, there are considerable accessibility problems in the dwellings of older adults with long-standing spinal cord injuries in Sweden, indicating that long-term follow-up of the housing situation of this population is necessary. Focusing on accessible housing as a prerequisite for occupational performance is at the core of occupational therapy, deserving attention on the individual as well as the societal level.
Keywords
Introduction
Adults with spinal cord injury (SCI) are living longer than previously due to improvements in acute care and rehabilitation (Groah et al., 2012), and most of this population are living in ordinary housing in the community. SCI is a well-documented condition, and there are several ongoing large-scale studies aiming to capture different aspects of the experiences of those living with SCI (Gross-Hemmi et al., 2017; Post et al., 2011; van der Woude et al., 2013). However, research focusing on older adults with SCI and the physical environments where they live is scarce. Specifically, knowledge about the housing adaptations and accessibility problems of older adults with SCI from a long-term perspective is virtually non-existent.
The home environment is known to become a vital factor for independence with increasing age (Mahler et al., 2014). Based on research on ageing and health influenced by occupational therapy perspectives (Iwarsson, 2004), there is evidence that accessible housing environments support health (Iwarsson et al., 2016). Recent evidence from the Scandinavian context shows that home-based occupational therapy including housing adaptations improves older adults’ occupational performance (Nielsen et al., 2019), which is an important aspect of health.
The term housing adaptation is often used interchangeably with home modification, although home modifications include a wider range of interventions, such as assistive technologies and training in activities of daily living (ADL). The types of housing adaptations that can be undertaken often depend on the national legislative framework as well as the housing standards and building traditions. In many countries no public grants are provided, with the result that clients and their family members must pay for such interventions themselves or take out private insurance to cover the costs. Applying the Swedish definition, the term ‘housing adaptation’ refers to a specific facet of the broader concept of home modifications, limited to alterations of the housing environment (SFS, 2018: 222). A housing adaptation is tailored to facilitate the performance of daily activities for the individual in the home (Fänge, 2004), is restricted to the removal of environmental barriers in the dwelling and its close exterior surroundings, and is regulated in Sweden under specific legislation (SFS, 2018: 222). The municipalities in Sweden have financial and administrative responsibility for housing adaptation grants. A grant application can be submitted once a housing adaptation is initiated by the client, a family member, or health professional (predominantly an occupational therapist). According to the responsible national authority (Boverket, 2016), the most common housing adaptation measures undertaken to improve accessibility are the elimination of thresholds, installation of grab bars, installation of ramps, installation of stove guards, and adaptation of bathrooms.
With a focus on occupational performance as the primary outcome of interventions, occupational therapy theories embrace the complex interaction between person, environment, and occupation (Townsend and Polatajko, 2007). Unpacking this complexity of occupational therapy interventions that focus on the home environment as an arena for occupational performance, previous research illustrates that new knowledge useful for practice can be gained by concentrating specifically on the person–environment (P–E) relationship (see for example Pettersson et al., 2018). Accessibility is a facet of P–E fit (Lawton and Nahemow, 1973), denoting the relationship between the capacity of the individual and the demands generated by the environment (Iwarsson and Ståhl, 2003). Accessibility problems arise when the demands of the physical environment exceed the capacity of the individual and make it difficult for the individual to perform basic tasks, such as moving around between rooms in the home, reaching and manipulating equipment in the kitchen or bathroom, etc. With reduced functional capacity, the individual is more sensitive to the demands of the environment. For instance, an environment where controls are placed very high or very low, or where doors are heavy and difficult to open, results in environmental press on the individual. Accordingly, accessibility in the sense of a P–E fit relationship is a prerequisite for occupational performance. P–E fit implies that the consequences of functional limitations (for a definition, see Nagi, 1991) in terms of accessibility problems can be essentially reduced by lowering the environmental demands in relation to the functional capacity of the individual. In the context of housing this can be achieved through housing adaptations, for example by removing physical environmental barriers and/or installing assistive equipment/technology (Boverket, 2016). Internationally, such measures are common facets of occupational therapy interventions, but when it comes to research, a range of disciplines are involved in studies in this field of inquiry (see for example Stark et al., 2017). Accordingly, the theoretical underpinnings of different studies go beyond those of occupational therapy.
Functional limitations do increase with age and generate increasing accessibility problems even if the physical environment does not change. When it comes to people with specific functional limitations, such as those arising following SCI, there is evidence of premature ageing (Frontera and Mollett, 2017; Holtz and Levi, 2006). Age-related physical decline can also have disproportionately negative consequences, as the body’s reserve capacity may have been used to a great extent in the initial stage of recovery at the time of injury (Holtz and Levi, 2006; Savic and Charlifue, 2015). Thus, individuals with SCI may experience age-related decline and its consequences earlier than the general population (Kemp et al., 2004; Thompson and Yakura, 2001). Considering a previous study targeting a different population (very old people in the general population) (Granbom et al., 2016b), accessibility did not improve when very old adults moved to dwellings with fewer environmental barriers, due to functional decline over time. The environmental press decreased, but so did the individuals’ functional capacity, resulting in persisting accessibility problems. That is, P–E fit is a non-static relation; therefore, although a housing adaptation is based on the functional capacity of the individual implemented at the time of an expressed need for adaptation, P–E fit changes over time. As there are no studies targeting P–E fit over time among the ageing SCI population, there is no knowledge about changes over time.
Among older adults in general, there is evidence of the efficacy of home modifications for improving functioning, reducing the risk of falls, and reducing demand on caregivers (Stark et al., 2017). The results from studies in different countries capture a variety of aspects of the consequences of SCI (Gross-Hemmi et al., 2017; Post et al., 2011; van der Woude et al., 2013), although the impact of the physical environment, as is the case for housing accessibility, is given little attention. Moreover, long-term follow-up of housing adaptations is rare (Malmgren-Fänge et al., 2013), which is a concern considering the anticipated change in P–E fit as people age. As community-living people with SCI typically receive housing adaptation soon after their injury, their housing situation after many years living with SCI is largely unknown, both with regard to housing adaptations and accessibility issues.
The purpose of this study was to investigate housing adaptations and current accessibility problems among older adults in Sweden living with SCI for more than 10 years. Specific aims were to map, by housing section (areas of the home), the most common housing adaptations and the environmental barriers that generated accessibility problems for this group despite the presence of housing adaptations.
Method
Design
The present study utilised selected cross-sectional baseline data from the Swedish Aging with Spinal Cord Injury Study (SASCIS) (Jörgensen et al., 2016). SASCIS is a longitudinal study focusing on people aged 50 years or older, at least 10 years post SCI. The overarching aim of SASCIS is to deepen the understanding of ageing with long-standing (>10 years) SCI in Sweden by increasing the knowledge of personal and environmental factors affecting daily life and health. For further details, see Jörgensen et al. (2016).
Sample
In all, 123 participants were included in the SASCIS, but for the present study one participant was excluded due to missing housing accessibility data (n = 122; mean age = 63 years; 71% men). To describe the diversity of the sample in terms of functional limitations, the participants were classified according to the SCI severity categories of the American Spinal Injury Association Impairment Scale (AIS) (Kirshblum et al., 2011). That is, the sample was categorised into three SCI severity groups: tetraplegia AIS A–C (n = 22; 15 AIS A, four AIS B, and three AIS C); paraplegia AIS A–C (n = 41; 23 AIS A, 8 AIS B, and 10 AIS C); and all AIS D (n = 59). The vast majority of the participants (77%) lived in dwellings with housing adaptations. About half of the participants (51%) lived alone. Details are provided in Table 1.
Socio-demographics and housing situation among individuals with long-standing spinal cord injuries, n = 122.
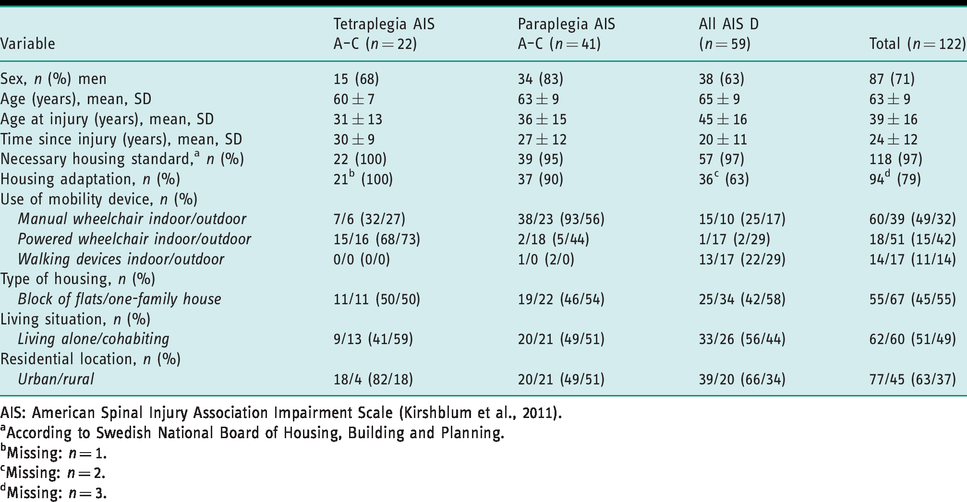
AIS: American Spinal Injury Association Impairment Scale (Kirshblum et al., 2011).
aAccording to Swedish National Board of Housing, Building and Planning.
bMissing: n = 1.
cMissing: n = 2.
dMissing: n = 3.
Data collection and dataset
The SASCIS data were collected at home visits conducted jointly by a registered occupational therapist (LN, first author) and a licensed physician (S Jörgensen). A set of self-administered instruments were mailed to the participants prior to the home visit and were reviewed and collected during the visit. The visits included structured interviews based on a study-specific questionnaire, which was complemented with well-established and validated generic and SCI-specific instruments. Information on the SCI and socio-demographic data was retrieved from medical records (Jörgensen et al., 2016).
The subset of baseline data from the SASCIS used in this study only included socio-demographics, housing accessibility, and complementary field notes. Housing accessibility data were collected with the Housing Enabler instrument (HE) (Iwarsson et al., 2012) by the first author (LN) during all of the visits. To ensure reliability, all data collectors using the HE in research projects are required to take a training course and practise data collection with the instrument. Data on housing adaptations were not included in the study-specific questionnaire; however, detailed field notes based on observations, including photo documentation of typical features, were taken during the home visits to complement the housing accessibility assessment. The field notes contained detailed descriptions of housing adaptations (including location), perceived assessment challenges, and the use of mobility devices. The details and extent of the field notes were considered adequate and of good quality by the research team. Because the field notes resulted in valuable information, all housing adaptations and mobility devices recorded were coded and added to the SASCIS dataset (Norin et al., 2019). The coding of the field notes was first done by LN and then verified by the team of authors through consensus discussions.
The Housing Enabler instrument
The Housing Enabler (Iwarsson et al., 2012) is a research-based instrument that yields a quantitative measure of P–E fit. The HE can be used reliably, validly, and systematically by professionals and addresses accessibility in ordinary housing (Iwarsson et al., 2012). The instrument has been used in large studies of ageing populations in several countries (Iwarsson et al., 2007). The HE consists of two parts: the personal component and the environmental component. The personal component, assessed through interviews and observation, includes a dichotomous assessment of functional limitations and dependence on mobility devices (walking devices and/or wheelchair), resulting in a functional profile. The environmental component comprises the housing section’s exterior surroundings (28 items), entrances (46 items), and indoor environment (kitchen, laundry, bathroom, bedroom, supplementary facilities, and indoors in general) (87 items), containing 161 items in all. The environmental barriers are dichotomously assessed by on-site observation and recorded as present/not present. An accessibility problem score is generated through a computerised scoring matrix juxtaposing the functional profile with the environmental barriers present. In each intersection of the matrix, there are predefined severity scores (0 = no problem, 1=potential problem, 2 = problem, 3 = severe problem, 4=impossibility) that are summed up to a total accessibility problem score (range=0–1844; higher scores indicate more problems). In the absence of functional limitations, the score is zero regardless of the number of environmental barriers present.
Results from a previous methodological study of the HE (Norin et al., 2019) showed that the presence of certain housing adaptations and mobility devices used to compensate for environmental barriers in ways not covered by the HE may hamper the reliability and validity of the instrument. Hence, in this study the accessibility problem scores were adjusted to reflect whether potential accessibility problems had been resolved by housing adaptations or mobility devices. For instance, if light switches were placed too high (recorded as an environmental barrier in the HE) for a person in a wheelchair, the score was adjusted to not indicate an accessibility problem if the switches had been adapted to be operated by remote control.
Descriptive data analyses
The presence of housing adaptations and environmental barriers generating accessibility problems in the sample was described and mapped by housing section based on the HE (Iwarsson et al., 2012) and the housing standards applied in Sweden (exterior surroundings, entrance, kitchen, laundry, bathroom, bedroom, supplementary facilities, and indoors in general).
In this study, the accessibility problem scores generated by single environmental barriers were used for the descriptive analyses (Norin et al., 2017). For each of the 161 environmental barriers in the HE an average accessibility problem score was computed, ranging from 0 to 35. To produce a ranking list of the environmental barriers according to the magnitude of accessibility problems they generated, they were sorted in descending order based on these average scores.
The HE software, Veten & Skapen HB and Slaug Enabling Development, Lund and Staffanstorp, Sweden, and the SAS software, SAS Institute Inc., Cary, NC USA, version 9.4, were used for the analyses.
Results
Location of housing adaptations by housing section
Seven of the 15 most common housing adaptations were located in the kitchen, and three at both the entrance and in the bathroom (Table 2). Housing adaptations were frequent at entrances (found at 42% of the dwellings with housing adaptations), in kitchens (31%), and in bathrooms (25%). Ramps at entrances were by far the most common housing adaptation, with an occurrence of 24%, followed by wheelchair-accessible stovetops (14%) and ceiling-lifts in bedrooms (13%) (Table 2; Figure 1).
The 15 most common housing adaptations and their location in the dwelling, n=122.
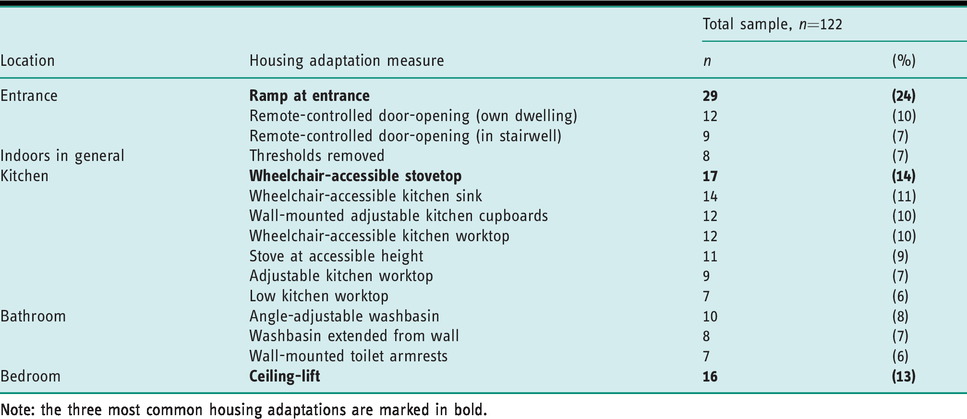
Note: the three most common housing adaptations are marked in bold.

The three most common housing adaptations.
Environmental barriers generating accessibility problems
The investigation of environmental barriers that generated accessibility problems identified the entrance as the most common location, with four barriers, followed by the kitchen with three barriers, while the other locations shared third place with two barriers each (Table 3). The four environmental barriers at the entrance collectively generated an accessibility problem score of 20.8, the three barriers in the kitchen 20.7, and the two barriers in the bathroom generated 11.4 (Table 3). Wall-mounted cupboards and shelves placed high in the kitchen represented the single environmental barrier that generated the most accessibility problems, with an average accessibility problem score of 10.8, inaccessible supplementary storage areas outside the dwelling were ranked second (6.3), and lack of grab-bar in bathroom ranked third (6.0). Controls in inaccessible positions (window and door fittings, locks, switches, etc.) were a recurrent problem in the kitchen (96% of the dwellings), bathroom (86% of the dwellings), and indoors in general (87% of the dwellings), see Table 3.
The 15 environmental barriers generating most accessibility problems, n=122.
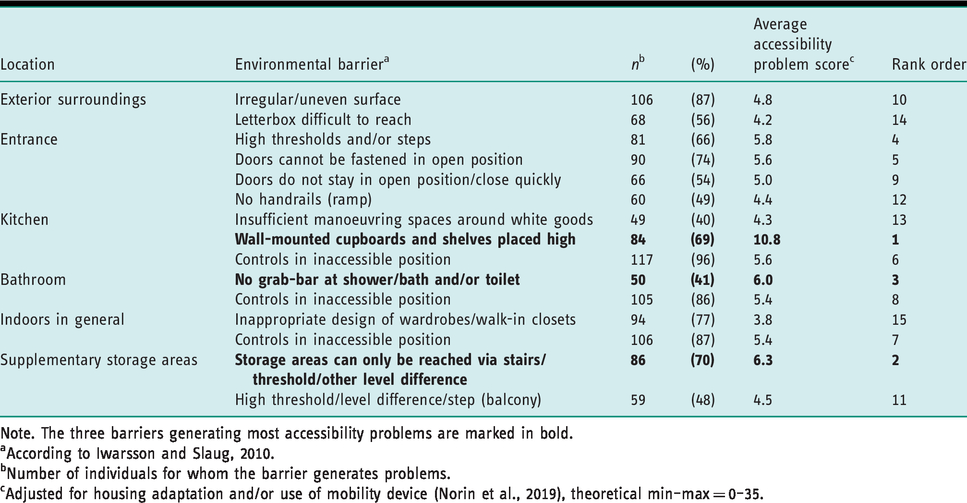
Note. The three barriers generating most accessibility problems are marked in bold.
aAccording to Iwarsson and Slaug, 2010.
bNumber of individuals for whom the barrier generates problems.
cAdjusted for housing adaptation and/or use of mobility device (Norin et al., 2019), theoretical min–max = 0–35.
Discussion
In this study, which was focused on older adults with long-standing SCI, we mapped the most common housing adaptations and current accessibility problems by housing section. The housing sections where housing adaptations were most common were also those where most accessibility problems were located. That is, adaptations were predominately located at entrances and in kitchens, followed by bathrooms. Environmental barriers in terms of level differences and inaccessible positions of objects (letterbox, cupboards, shelves) or functions (for example different types of controls) were common throughout the dwellings. This was despite the fact that several of the most common housing adaptations recorded addressed such problems (ramp, wall-mounted adjustable kitchen cupboards, remote-controlled door-opening, etc.). These contradictory results indicate that these challenging areas need careful attention in occupational therapy practice. To ensure that all environmental barriers that have the potential to generate accessibility problems are addressed, closer attention should be paid to the wide range of design features present in entrances, kitchens, and bathrooms.
People ageing with disability may experience that they, to age on equal terms with others, are more dependent on health care resources, societal services, and accessible environments. On the other hand, they may be better prepared for age-related challenges, as they have developed skills to adapt and strategies to compensate for physical decline (Molton and Yorkston, 2017). Still, the interaction with the surrounding physical and social environment considerably impacts the degree of disability among people with SCI (Molton and Jensen, 2010), which is in line with the notion of P–E fit (Lawton and Nahemow, 1973) as well as the theories and practice models of occupational therapy (see for example Townsend and Polatajko, 2007). Importantly, because individual needs related to housing change as people age, the results of our study highlight that occupational therapists should be more aware of potential changes for their clients in the future and factor these into the housing adaptations they suggest. Moreover, housing adaptation services should include follow-ups for people ageing with SCI to identify accessibility problems that appear in the long-term perspective.
The fact that housing adaptations and environmental barriers occurred in the same section of the dwelling is noteworthy. That is, even where environmental adaptations had been put in place, accessibility problems remained, and this was common throughout the dwelling. For example, four of the common kitchen adaptations concerned the accessible positioning of objects/controls such as adjustable or low-placed wall-mounted cupboards, yet wall-mounted cupboards/shelves that were placed high represented the environmental barrier that generated the most accessibility problems (Table 2). The results for bathrooms were similar. While these findings relate to a Swedish context, they may very well be applicable on the international level. Our interpretation is that, over time, the conditions people with SCI live under gradually change, and there is a need for greater focus on person-centred long-term follow-ups of housing accessibility.
Keeping in mind that the HE instrument targets accessibility as a professionally assessed construct (Iwarsson and Ståhl, 2003), it should be noted that more than 7% of the participants in a previous SCI study (Hertig-Godeschalk et al., 2018) indicated that kitchen accessibility could be unnecessary if another family member performed the kitchen chores. This means that a housing adaptation may not be initiated if the individual activity repertoire does not include such tasks, which is in line with client-centred occupational therapy. Our results highlight the importance of aspects not investigated in the present study, such as activity patterns and perceptions of usability, which are central features relating to individual occupational performance within the context of the home.
Environmental barriers, such as uneven surfaces and high thresholds, were common and generated accessibility problems. These environmental barriers were mainly found at entrances and in supplementary storage areas often located in communal areas in multi-dwelling blocks. In Sweden, a housing adaptation is an individually granted intervention where the individual owns the adaptation and, in most cases, is entitled to bring it with him/her in case of relocation. Hence, accessibility problems in communal areas can be a challenge to address considering that other people also use the building. For example, automatic door-opening and ramps in multi-family dwellings made up more than 11% of the housing adaptation grants in Sweden in 2015 (Boverket, 2016). This issue highlights the need for universally designed (Mace, 1985; Preiser and Smith, 2010) housing that accommodates the needs of the population at large, rather than directing public funding to individually tailored housing adaptations (Pettersson et al., 2018). The fact that the inaccessible positioning of objects (for example letterboxes) or functions (controls, cupboards, shelves) were recurrent environmental barriers in all housing sections is worth noting. Given that this affected practically the entire sample (see Table 3), the extent and frequency suggest that existing housing design standards and traditions do not accommodate the needs of people with the functional profiles of our sample. As previous research has demonstrated that the evidence for the use of current housing standards to prevent accessibility problems among people with functional limitations is insufficient (Helle et al., 2014), these findings support the need to revisit current housing standards and direct the focus towards universal design.
The most common housing adaptations in the study (see Table 2) differ slightly from the most common housing adaptations among the general population in Sweden (threshold elimination, mounted grab-bar, ramp installation, stove guard installation, bathroom adaptation) (Boverket, 2016). Requiring a wheelchair-accessible stovetop and a ceiling-lift in the bedroom is consistent with the complex functional limitations and restricted mobility that people with SCI have, including the need to use a wheelchair. The most common housing adaptations undertaken among the general population reflect typical consequences of age-related functional decline, such as reduced mobility and memory problems. While age-related functional decline develops over time, thus allowing the individual to adjust occupational performance gradually, an SCI results in an abrupt change in body functions and activity performance. The characteristics of SCI-related functional limitations and the sudden changes in functioning at a younger age most likely explain the differences in common housing adaptations. The differences between older adults in general and those with a long-standing SCI represent valuable knowledge that can be applied in the provision of person-centred occupational therapy based on current as well as future individual needs.
Implications for occupational therapy research and practice
Over the years, it has been identified that housing adaptation is an area in need of expanded research (see for example Stark et al., 2017). In a literature review, Boniface et al. (2013) found that occupational therapists increasingly provide rehabilitation and reablement services, including housing adaptations. Many occupational therapy interventions are carried out in the home environment, where an awareness of common challenging housing sections, housing adaptations, and environmental barriers is vital information. The challenging sections are well known, while the most common housing adaptations among the sample in the present study differ from those for the older population in general, which is new knowledge. The fact that accessibility problems in one section of the dwelling may repeat themselves in another section highlights the value of seeing the whole dwelling as one unit when evaluating occupational performance, and thus not focusing on just a specific section. Our study points to the need for adopting a comprehensive approach that takes person–environment–task transactions and implications for occupational performance into account. Not only for occupational therapists in Sweden but worldwide, it is crucial to provide guidance towards client-centred solutions, fulfilling the needs of the individual.
Based on experiences gained from individual cases aggregated to the group and population levels, occupational therapists can provide expert knowledge and become agents for societal change. While hitherto a largely neglected public health issue (Granbom et al., 2016a), the complexity of P–E fit as a prerequisite for occupational performance and the diversity of needs of different population groups deserve explicit attention in housing policy and housing provision. Skills for enabling societal change are different from the competencies used for enabling individual change (Townsend and Polatajko, 2007) within traditional occupational therapy practice, but facts based on valid data such as those generated by the present study can assist practitioners in such novel endeavours.
Limitations
As this is a cross-sectional study, there is no information regarding functional limitations, accessibility, and/or changes in environmental barriers over time, which is a limitation that merits further attention. As housing adaptations were not specifically targeted by the data collection for SASCIS but emerged as an important aspect in the present study, there is important information lacking on when a housing adaptation was performed and how it was financed and implemented (grant or private), and the results should be interpreted with this in mind.
The HE has some limitations when used for individual assessments in clinical practice in populations where extensive housing adaptations and use of mobility devices are frequent (Norin et al., 2019). We took these limitations into account in the present study, even though the effect of the limitations is insignificant for results on the group level. Despite limitations on the individual level, using a well-established, research-based, internationally available instrument to assess housing accessibility is a strength that enhances the possibility of similar studies on the population level in other contexts.
The concepts of accessibility and usability are often used interchangeably, although they do differ (Iwarsson and Ståhl, 2003). Accessibility is objective in nature, while usability is a self-perceived phenomenon that adds personal experiences to the P–E relation and thus relates to the individual repertoire of occupations. Consequently, when targeting objective housing accessibility based on national legislation and guidelines, the HE is not suitable for measuring the effects of a housing adaptation intervention because the data collected do not convey anything about individual perceptions related to P–E fit and occupational performance. Investigating usability and other perceived aspects of housing would add valuable knowledge to the housing situation of older adults with long-standing SCI and deserves attention in further research.
Conclusion
Despite the presence of housing adaptations in most of the cases included in the present study, there are considerable accessibility problems in the dwellings of older people with long-standing SCI in Sweden, regardless of the comprehensive national welfare system and high housing standards. The results indicate that long-term follow-up of the housing accessibility situation of people with SCI is necessary. Focusing on accessible housing as a prerequisite for occupational performance is at the core of occupational therapy, and deserves attention on the individual as well as the societal level. Further research focusing on how individuals with SCI perceive their housing situation and the usability of their dwellings would be useful for deepening the knowledge and understanding of what challenges they face as they age and what to focus on to improve their long-term housing situation.
Key findings
Despite housing adaptations addressing common environmental barriers, substantial accessibility problems were found. Kitchens, entrances, and bathrooms are common locations for both housing adaptations and environmental barriers that generate accessibility problems.
What the study has added
The results contribute to the understanding of the environmental challenges faced by older adults with long-standing SCI and point to the importance of long-term follow-ups by occupational therapists.
Footnotes
Acknowledgements
The authors wish to thank all participants. The authors are grateful to S Jörgensen, MD, PhD, for collaboration during the data collection and Professor J Lexell, MD, PhD (PI for SASCIS), for collaboration in the overall project.
Research ethics
Ethical approval was obtained from the Regional Ethical Review Board in Lund (No.2010/692).
Consent
All participants were given oral and written information about the study and informed of their right to withdraw at any time. Written informed consent to be visited and interviewed for the study was obtained from all participants before starting the data collection.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to research, authorship, and/or publication of this article: S Iwarsson and B Slaug are the copyright holders and owners of the Housing Enabler (HE) instrument and software, which are provided as commercial products. The other authors have no competing interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by the Swedish Research Council, King Gustav V and Queen Victoria’s Freemason Foundation, and the Ribbingska Foundation in Lund. The study was accomplished within the context of the Centre for Ageing and Supportive Environments (CASE), Lund University, financed by the Swedish Research Council for Health, Working Life and Welfare (Forte). The first author was supported by the Swedish National Graduate School for Competitive Science on Ageing and Health (SWEAH), financed by the Swedish Research Council.
Contributorship
L Norin was one of the two data collectors in the Swedish Aging with Spinal Cord Injury Study (SASCIS) and conducted the HE assessments, contributed fieldnotes, set up the database, and performed the quality controls. All authors were involved in the design of the study and the iterative analysis process, with L Norin as the main contributor. She was responsible for drafting the manuscript, with all co-authors actively contributing to the development and editing of the manuscript towards submission. S Iwarsson and B Slaug performed the major revision of the original submission. All authors reviewed and approved the final version of the manuscript.