
Abstract
Introduction
People with severe mental health problems often struggle to manage everyday tasks such as personal hygiene, housework, shopping, cooking and budgeting. These functional problems result in self-neglect and are associated with specific cognitive impairments and poor outcomes. Despite their importance, little guidance is available for practitioners in how to address these problems.
Method
We conducted a systematic review of the research literature published since 1990 on the effectiveness of interventions that aim to assist people with severe mental health problems to manage their personal self-care. We searched six major electronic databases and followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidance in the conduct of the review and reporting of results.
Results
Our search identified 2808 papers of which only eight met our inclusion criteria. The included papers comprised six randomised controlled trials and two ‘pre-post’ studies reporting on evaluations of five different interventions. We used narrative synthesis to summarise our findings. The strongest evidence was for cognitive adaptation training, comprising environmental supports provided in the home that address the functional problems arising from specific cognitive impairments.
Conclusion
The paucity of research into interventions to assist personal self-care for people with severe mental health problems is surprising. More research in this area is urgently needed.
Introduction
Alongside symptoms such as hallucinations and delusions, people with severe mental health problems, such as schizophrenia, schizoaffective disorder and bipolar disorder, often struggle to manage everyday tasks. These activities of daily living (ADL) include attending to personal self-care, laundry, housework, shopping, cooking and budgeting (Velligan et al., 1997). These functional problems have been shown to be associated with specific cognitive impairments affecting attention, executive functioning, verbal fluency, learning and memory (Depp et al., 2012; Green, 1996). It has been estimated that approximately 80% of people with psychosis and approximately 60% of those with affective psychosis experience cognitive deficits which often persist even when positive symptoms have resolved or reduced (McCleery, 2019).
Two recent national studies of services working with people with severe mental health problems in England identified that self-neglect is a common problem among this group, affecting 49% of those in inpatient mental health rehabilitation wards (Killaspy et al., 2013) and 57% of those living in supported accommodation in the community (Killaspy et al., 2016). Activities of personal self-care include regular bathing/showering, dental hygiene, hair washing and combing, nail care and shaving/depilation. Other forms of personal self-care, beyond personal hygiene, are also essential to avoid self-neglect, such as attending to laundry, wearing appropriate clothing, cleaning, shopping and preparing food to maintain an adequate diet. Impaired ADL functioning has been shown to be associated with increased inpatient admissions, costs of care, mortality risk and poorer quality of life (Hayes et al., 2012; Mlinac and Feng, 2016). Qualitative research has also identified attending to personal care as an important facilitator of community participation for people with schizophrenia, helping with confidence and motivation (Chugg and Craik, 2002). Conversely, not attending to personal care has been reported as an impediment to leaving the house (Andonian, 2010).
Despite the evidence that self-neglect is highly prevalent among people with severe mental health problems and is associated with negative consequences, little seems to be known about how to address it. We therefore conducted a systematic review of the published literature to investigate the evidence regarding the effectiveness of interventions that aim to improve personal self-care in adults with severe mental health problems.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed in the conduct and reporting of this review (Moher et al., 2009).
Search strategy
A systematic literature search was conducted using the following six electronic bibliographic databases: MEDLINE, PubMed, Embase, PsycINFO, Applied Social Sciences Index and Abstracts (ASSIA) and Cochrane Central Register of Controlled Trials (CENTRAL). The search was limited to peer-reviewed journal articles published in English from 1990 to 1 September 2019, and the search was updated in March 2020. This date range was chosen on the basis that relevant studies would have been completed since the ‘deinstitutionalisation’ era of the 1990s. The search strategy employed relevant terms derived from medical subject headings (MeSH), Emtree thesaurus, PsycINFO thesaurus and ASSIA thesaurus, that were adapted for each database and related to the concepts ‘mental health’, ‘mental disorders’, ‘mental illness’ AND ‘self-care’, OR ‘self-management’ OR ‘personal self-care’ OR ‘personal hygiene’ OR ‘activities of daily living’ OR ‘everyday functioning’ AND ‘psychiatric rehabilitation’ OR ‘occupational therapy’ OR ‘intervention’ OR ‘approach’ OR ‘training’ OR ‘program’ AND ‘functional performance’ OR ‘everyday function’ OR ‘daily function’ OR ‘functional status’ OR ‘functional capacity’ OR ‘community function’ OR ‘social function’ OR ‘living skills’. Additional relevant papers were identified through hand searching reference lists of the eligible studies selected from the database searches.
Study selection criteria
Participants
Eligible studies were those that recruited adults aged 18 years or over in which at least 50% of the study sample had a primary diagnosis of a severe mental health problem (schizophrenia, schizoaffective disorder, or bipolar affective disorder).
Interventions
Studies were included if the intervention being evaluated aimed to improve participants’ ability to perform ADL relating to personal self-care. This included any of the following: grooming (bathing/showering, brushing teeth, washing hair, nail care, etc.); choosing appropriate clothing; doing laundry; food shopping and cooking; housework/cleaning.
Outcome measures
We also included studies in which the primary outcome of interest was improvement in participants’ functioning in ADL including personal self-care, assessed using a validated self-rated, clinician-rated, or informant-rated measure.
Study designs
Eligible studies were those that were designed to assess the effectiveness of the intervention; randomised controlled trials (RCTs), non-RCTs, pre-post studies and case–control studies.
Publication type
Only studies that had been peer reviewed before publication were included.
Screening and study selection
Database search results were merged and de-duplicated using the reference management software ‘Endnote X9’. Manuscript titles and abstracts were screened independently by two reviewers against the inclusion criteria. The two reviewers then compared their lists of included studies and discrepancies were resolved through discussion to reach consensus. Full texts of the included studies were then retrieved and reassessed for eligibility.
Data extraction
Data extraction was conducted by HTW using an Excel spreadsheet with items adapted from the Cochrane Effective Practice and Organisation of Care Review Group data collection checklist including: general study information (author, year of publication, title); study design and objectives; participants and setting (characteristics/eligibility criteria, location of care (inpatient/community), country); methods (unit of allocation (if randomised) or selection process (non-randomised), unit of analysis, power calculation, statistical methods); intervention (purpose, timing, recipient, deliverer, format); description of comparison intervention; outcomes (main outcome measure/s, timing of initial and any further follow-up assessments); results (main outcome/s, subgroup, time point, or adjusted sub-analyses and management of missing data).
Quality assessment
Quality assessment was conducted after data extraction to reduce reporting bias. RCTs were assessed using the risk of bias 2 tool (‘Rob 2’), which measures five domains of potential bias arising from: randomisation of participants; assignment to interventions; missing outcome data; measurement of outcome; and selection of reported result (Sterne et al., 2019). The overall risk of bias is judged as ‘low’, ‘some concerns’, or ‘high’ using a specified algorithm. Non-randomised studies were assessed using the ROBINS-I tool (Sterne et al., 2016) which also generates an overall judgement, based on the following: confounding; selection of participants; classification of interventions; missing data; measurement of outcomes; and selection of results. The overall risk of bias is rated as ‘low’, ‘moderate’, ‘serious’ or ‘critical’ (if ‘critical’ the study is considered too problematic to provide any useful evidence). Domains can also be reported as having ‘no information’ on which to base a judgement. Two reviewers independently assessed bias for all included studies (HTW and MB) with any discrepancy discussed and resolved by a third reviewer (HK).
Data synthesis
A meta-analysis was not feasible due to heterogeneity of interventions and outcomes. A narrative approach was therefore employed to synthesise findings. Narrative synthesis relies on the use of words and text to summarise and explain findings including: a preliminary synthesis to identify patterns of findings across included studies; exploring whether effects of interventions varied according to study populations and types of intervention; identifying factors that might have influenced the results within individual studies and explaining different findings between studies; developing a theoretical framework for the intervention effects to provide further interpretations on findings; assessment of the robustness of synthesis based on the strength of evidence; discussion of the generalisability of conclusions to wider populations and contexts (Popay et al., 2006).
Results
The search results are presented in the PRISMA flow diagram in Figure 1. In total, 2775 papers were identified from the database searches and 33 additional manuscripts were identified from hand searching, reporting on 2807 individual studies. After screening abstracts and titles, 171 papers were included in full-text screening. Of these, 51 were excluded because they reported on studies that evaluated interventions where the focus on personal self-care could not be differentiated from other aspects of ADL; 32 recruited a sample that did not meet our inclusion criteria; 26 were not peer-reviewed; 21 did not report any outcome for ADL relating to personal self-care; 14 were not studies of effectiveness; 10 used ineligible study designs; nine had not published any results.
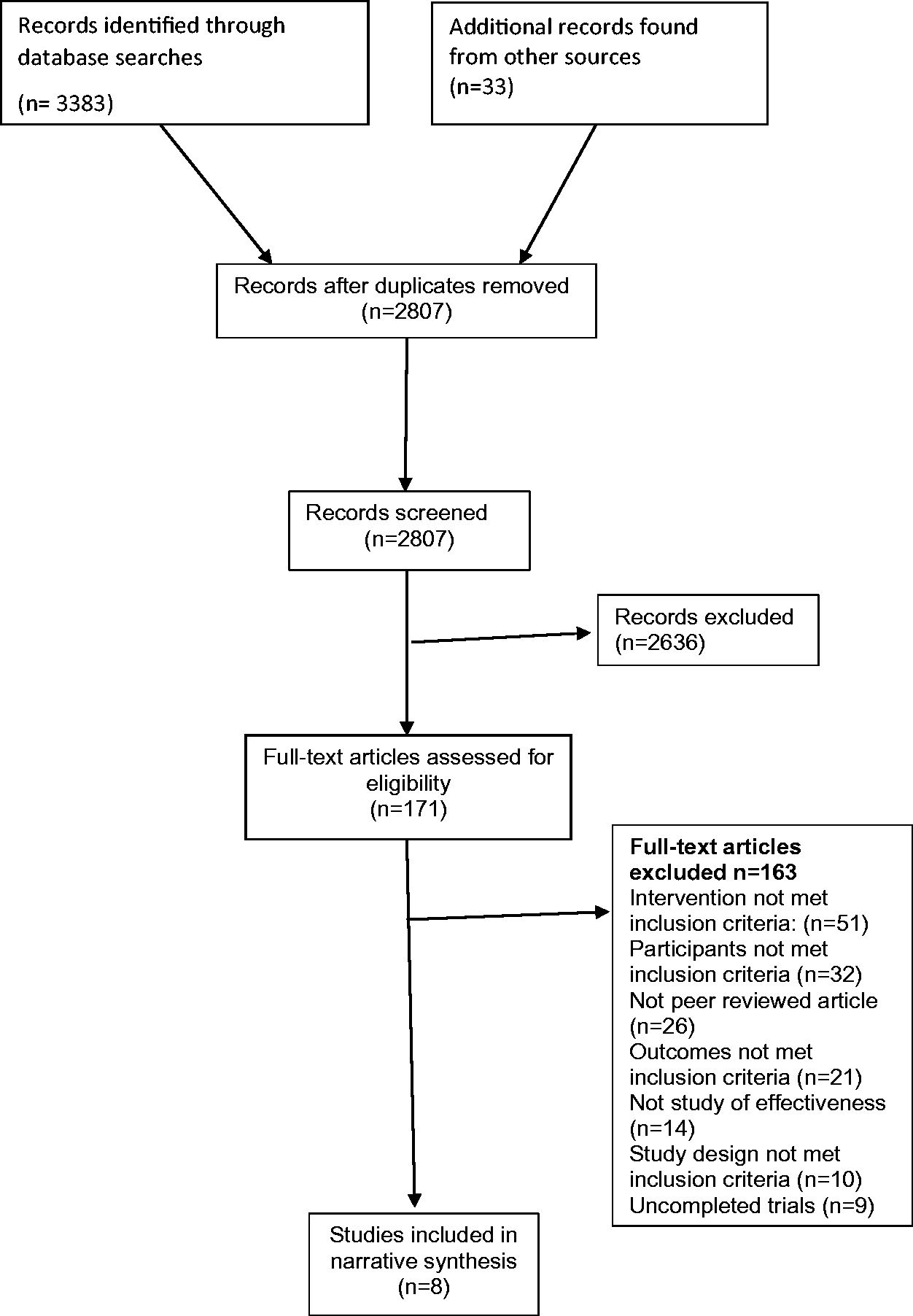
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
The final synthesis included eight papers reporting on eight studies evaluating five different interventions. Of these eight papers, six reported results from RCTs and two reported results from pre-post studies.
Table 1 summarises the characteristics of the eight included studies. Six were conducted in the United States (US), one in Spain and one in Japan. Five studies took place in community settings and three in inpatient settings. The year of publication ranged from 1991 to 2014.
Characteristics of included studies.
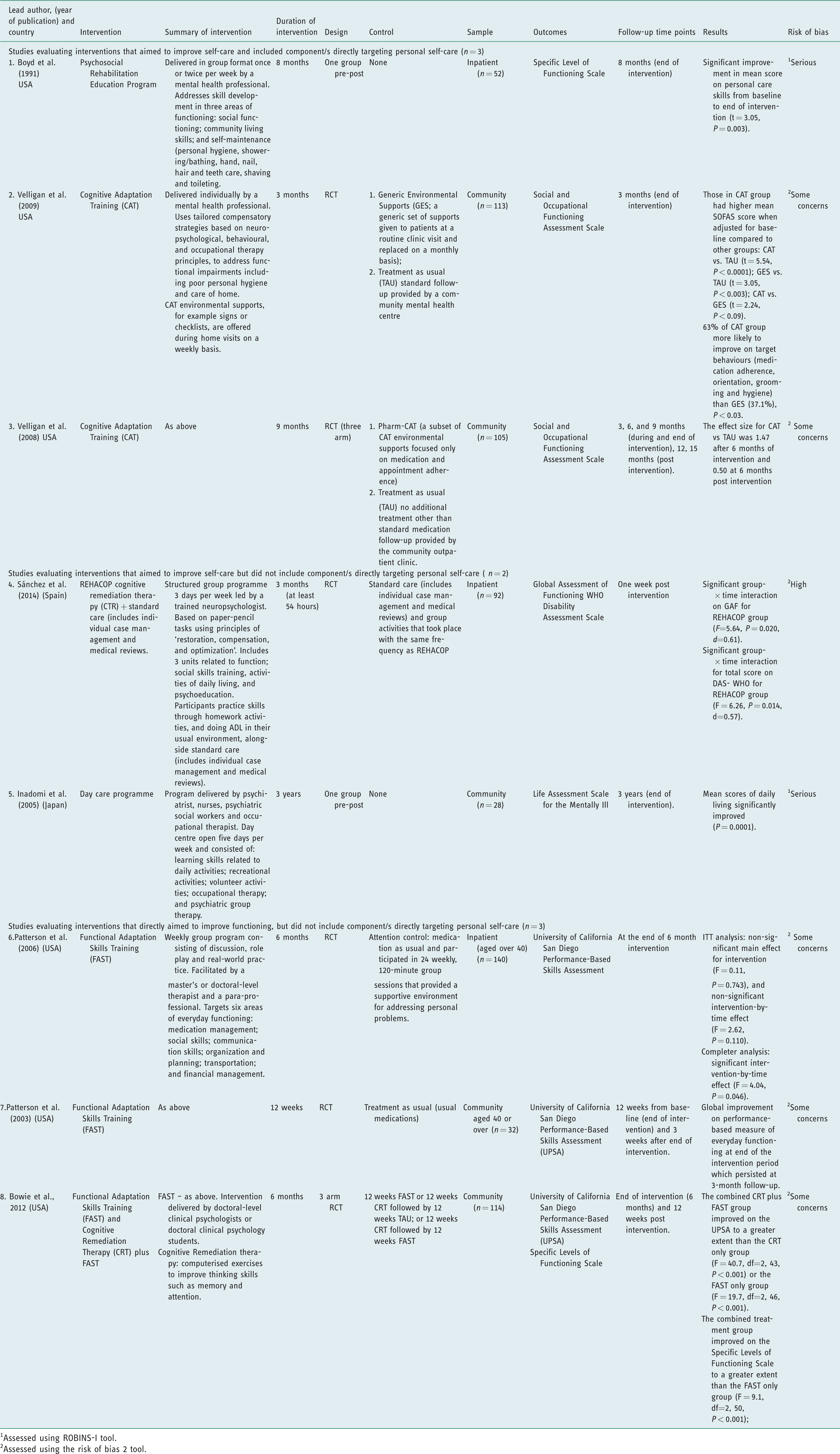
1Assessed using ROBINS-I tool.
2Assessed using the risk of bias 2 tool.
Risk of bias
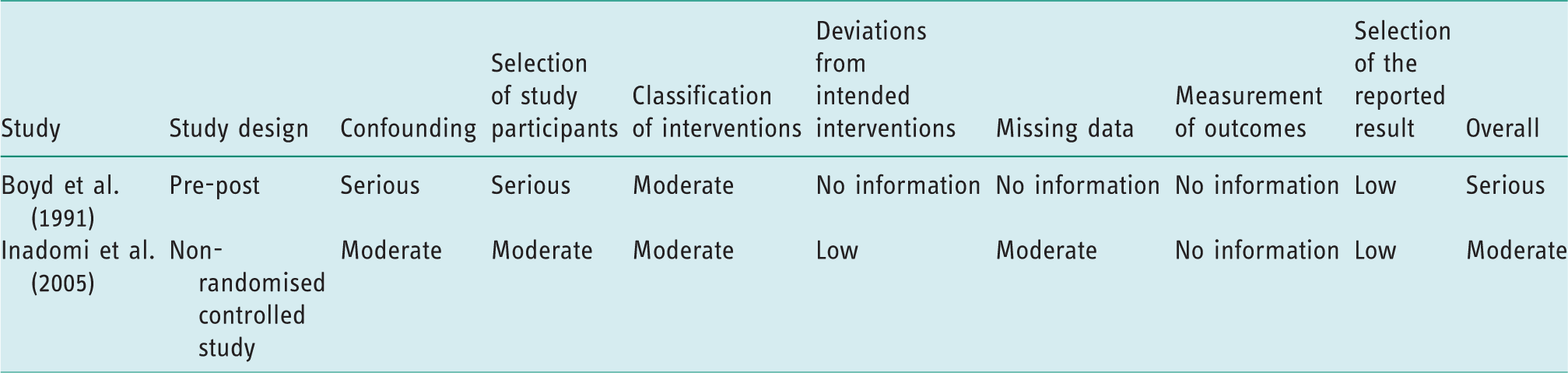
Table 2 summarises the risk of bias for included studies reporting on RCTs. Five of the six were assessed as having ‘some concerns’ (Bowie et al., 2012; Patterson et al., 2003, 2006; Velligan et al., 2008, 2009) and one was assessed as being at ‘high’ risk of bias (Sánchez et al., 2014). Table 3 summarises the risk of bias for the pre-post studies; both were assessed as being at ‘serious’ risk of bias (Boyd et al., 1991; Inadomi et al., 2005).
Risk of bias assessment using the RoB-2 tool for randomised trials.
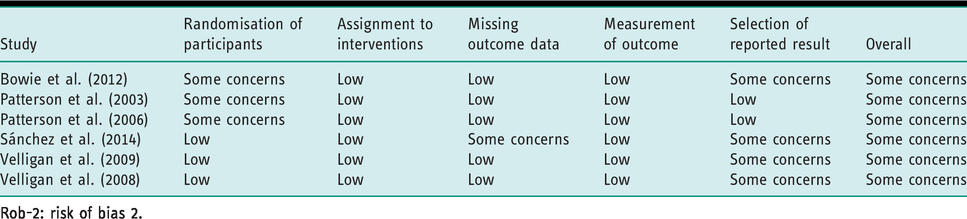
Rob-2: risk of bias 2.
Risk of bias assessment using ROBINS-I tool for non-randomised studies.
Interventions
No studies reported evaluations of interventions that focused solely on improving personal self-care as defined for this review. For descriptive purposes we grouped the interventions as follows: those that directly aimed to improve personal self-care and included a personal self-care component (n = 2); those that aimed to improve ADL but included no specific content relating to personal self-care (n = 2); those that aimed to improve functioning, but included no specific content relating to personal self-care (n = 1).
Of the two interventions that included a component that directly aimed to improve personal self-care, one was described as a group psychosocial rehabilitation education programme conducted in an inpatient setting (Boyd et al., 1991). The intervention consisted of three components to improve functioning: social functioning; community living skills; self-maintenance. The self-maintenance component included modules on showering/bathing, hand and nail care, dental hygiene, hair care, shaving and toileting. The intervention was evaluated using a pre-post study and participants’ scores on the self-care domain of the primary outcome measure were reported to improve significantly. However, the study was assessed as having a serious risk of bias. The second intervention that directly aimed to improve personal self-care was cognitive adaptation training (CAT), delivered one to one in community settings (Velligan et al., 2008, 2009). The intervention used individualised environmental supports to compensate for the cognitive impairments associated with severe mental health problems that impact negatively on functioning. These included signs and checklists, personal care supplies and simple storage systems to help the person organise their belongings. These environmental supports aim to prompt and facilitate personal self-care; for example, reminding the person to attend to grooming and other routine tasks such as taking medication and doing laundry. Beyond personal self-care, the intervention also aimed to facilitate engagement in community-based activities. The two RCTs evaluating CAT identified in this review found it to be associated with higher scores on a measure of social and occupational functioning compared to a treatment as usual control group (Velligan et al., 2008) and an attention control (Velligan et al., 2009). As with three of the four other RCTs we identified for this review, both of the RCTs assessing CAT were assessed as having ‘some concerns’ with regard to the risk of bias.
One of the two studies evaluating an intervention that aimed to improve ADL but had no specific content targeting self-care, was described as a day care programme for people living in the community (Inadomi et al., 2005). That study was conducted in Japan and the intervention comprised a 5 day a week programme that aimed to help participants gain ADL skills and to engage in community-based leisure activities. It included social skills training, artistic activities (creative arts and handicrafts), ‘occupational therapy’ (not defined) and ‘psychiatric group therapy’ (not defined). The programme was evaluated in a small pre-post study and was reported to have benefits on a measure of daily living skills, but it was assessed as having a serious risk of bias. The second study we identified that evaluated an intervention that aimed to help participants improve in ADL and other areas of function, was a RCT conducted in an inpatient setting in Spain (Sánchez et al., 2014). The intervention was described as a multidimensional remediation programme that included cognitive remediation therapy (CRT) with a specific emphasis on the implementation of ADL skills in the person’s ‘real environment’. The intervention was more effective than standard care in improving functioning, but there was no difference in relation to self-care management. In addition, the study was assessed as having a high risk of bias.
The fifth of the five interventions we identified in this review, functional adaptation skills training (FAST), aimed to improve functioning but did not specifically target personal self-care. The intervention was delivered as a group intervention for people aged over 40 years, and aimed to facilitate independent living skills such as planning and organisation of daily activities, financial management, medication management and transportation. Three RCTs were identified that evaluated this intervention, one conducted in an inpatient setting (Patterson et al., 2006) and two in community settings (Bowie et al., 2012; Patterson et al. 2003). In the inpatient trial, FAST was compared with an attention control. It was not found to be effective in an intention-to-treat analysis on the primary outcome of the performance of everyday living skills, but there was a trend towards effectiveness for those who completed at least a quarter of the programme. The initial RCT evaluating FAST in a community setting reported it to be effective on the same measure of performance-based everyday living skills compared to treatment as usual (Patterson et al., 2003). A subsequent community-based RCT (Bowie et al., 2012) found that combining FAST with CRT was more effective than providing FAST alone.
Narrative synthesis
Preliminary synthesis of findings from across studies
All eight studies we identified reported positive findings on measures of functioning. However, the interventions were not all well described and none targeted personal self-care solely. The three studies that included personal self-care within the focus of the intervention under evaluation reported positive outcomes on their chosen measure of self-care. One of these was a low quality, pre-post design study conducted in an inpatient setting (Boyd et al., 1991), while the other two were RCTs of reasonable quality that evaluated CAT delivered in the person’s home (Velligan et al., 2008, 2009). The two studies that evaluated interventions that included a focus on ADL but not specifically personal care, were both of low quality. One was a pre-post study conducted in the community (Inadomi et al., 2005) and one was a low quality trial based in an inpatient setting (Sánchez et al., 2014). The pre-post study reported the intervention to have a positive impact on daily living skills (Inadomi et al., 2005); the trial reported no significant difference in self-care management skills between intervention and control groups (Sánchez et al., 2014). The three remaining studies were RCTs of reasonable quality that evaluated the FAST intervention, one based in an inpatient setting (Patterson et al., 2006) and two in the community (Bowie et al., 2012; Patterson et al., 2003). While this intervention did not specifically focus on ADL or personal self-care, sustained improvement in household skills was reported when combined with CRT in one of the community-based trials (Bowie et al., 2012). In summary, our review identified few relevant studies but the strongest evidence was for CAT provided to people in their own home. There was also evidence that the FAST intervention may be effective in improving skills relevant to personal self-care, particularly when combined with cognitive remediation but this intervention did not specifically target personal self-care.
Variation in effects of interventions on different subgroups and factors that might explain different findings between studies
All the studies focused on people with severe mental health problems and evaluated structured programmes. However, the three studies showing the strongest evidence for specific interventions were based in the community rather than inpatient settings (CAT: Velligan et al., 2008; FAST: Bowie et al., 2012). This could be interpreted as meaning that individuals who are more advanced in their recovery and are able to live in a community setting benefit more from specific interventions that aim to improve personal self-care than those who still require inpatient treatment.
Theoretical framework for the intervention effects
All eight studies reported positive findings for the intervention studied being associated with improvements in functioning. While the format and content of the five different interventions evaluated by these eight studies varied, as did the quality of the studies, this finding suggests that interventions that specifically focus on function are beneficial for people with severe mental health problems. The strongest evidence we found was for two separate interventions, one of which employed compensatory environmental supports that specifically addressed the practical implications of the cognitive deficits leading to poor personal self-care (CAT), whereas the other intervention had a more general focus on functioning (FAST), which was effective in improving personal self-care when combined with an initial CRT programme. It therefore appears that interventions are more likely to benefit personal self-care if they address the cognitive impairments associated with severe mental health problems either directly (CRT) or indirectly (CAT). While it is already known that CRT leads to improved cognition, it follows that a subsequent structured programme such as FAST can build on this through practical ‘real-world’ activities that improve functioning. This mechanism of action seems likely as it is akin to existing evidence for the effectiveness of combining cognitive remediation with supported employment (Van Duin et al., 2019). However, the mechanism of action for compensatory environmental approaches such as CAT is unclear; it could be that it leads to improvements in cognition that benefit an individual’s functional abilities, or simply provide practical ‘aides’ that bypass the cognitive impediment altogether. The studies we identified in this review cannot help answer this.
Strength of the evidence
The intervention evaluated by Boyd et al. (1991) and CAT (Velligan et al., 2008, 2009) were most closely aligned with the aims of our review in terms of targeting personal self-care, but the Boyd study was of low quality. The trials of CAT (Velligan et al., 2008, 2009) were of reasonable quality. Both studies that evaluated interventions that focused on ADL more generally were of low quality (Inadomi et al., 2005; Sánchez et al., 2014). There was reasonably good evidence that the FAST intervention was associated with sustained gains in skills relevant to personal self-care, particularly when combined with cognitive remediation (Bowie et al., 2012).
Generalisability of the findings
The three trials which produced the strongest evidence for the effectiveness of specific interventions associated with improvements in personal self-care (Bowie et al., 2012; Velligan et al., 2008, 2009) were all conducted in the US and results may therefore not generalise to other settings.
Discussion and implications
We believe this to be the first systematic review of the published literature reporting on the effectiveness of interventions that aimed to improve personal self-care for people with severe mental health problems. Interestingly, although self-neglect is an important problem for this group, the majority of studies our search identified did not include any focus on personal self-care. We identified no studies that evaluated an intervention that specifically targeted this aspect of functioning alone. We identified three studies, evaluating two interventions, that included personal self-care as one aspect of an intervention that aimed to improve the person’s functioning (Boyd et al., 1991; Velligan et al., 2008, 2009). We identified a further five papers evaluating three interventions that were not described as having any specific focus on personal self-care, but included it within a broader conceptualisation of ADL (Bowie et al., 2012; Inadomi et al., 2005; Patterson et al., 2003, 2006; Sánchez et al., 2014).
The study by Boyd et al. (1991) evaluated an intervention that included a clear focus on personal self-care, alongside two other aspect of functioning, but it was almost 30 years old and of low quality. The results are therefore of questionable relevance to contemporary practice. The strongest evidence came from the other two studies that included a personal self-care element in the intervention. Both were conducted by the same group and evaluated CAT, an intervention that provides individually tailored environmental strategies to compensate for the cognitive impairments associated with severe mental health problems in order to address specific functional impairments (Velligan et al., 2008, 2009). This differs from CRT which aims to address specific cognitive impairments directly. Although these two trials were of reasonable quality and the results were generally positive, the findings have not been replicated in a subsequent trial carried out in Denmark in which CAT was combined with assertive community treatment (ACT), an intensive model of community-based case management for people with severe mental health problems. However, the patient group in the Danish trial is likely to have been more functionally impaired than in the original US studies as ACT targets those with more complex problems (Hansen et al., 2012). The trial was also underpowered. We are aware of an encouraging pilot study and current RCT of CAT being conducted in The Netherlands which will help to inform the evidence for the efficacy of this approach (Quee et al., 2014). Of note, neither the Danish nor the Dutch studies were identified by our literature search as neither included in their description of the CAT intervention terms that we used to identify studies targeting personal self-care. However, the description of the original CAT intervention includes its potential to provide strategies to assist with personal self-care when relevant (Velligan et al., 2008).
This highlights a problem with the term ‘self-care’, a rather vague concept that extends beyond practical daily living skills into the realm of emotional self-regulation and the promotion of wellbeing. To address this, we chose search terms that were specific to personal self-care and agreed these in advance. We also conducted hand searches of the references of included studies to minimise the chance of missing relevant studies. Nevertheless, we may not have identified studies that did not mention personal self-care (or related terms) in the study title, abstract or description of the intervention. This may explain why we found so few studies, although it seems unlikely that an intervention that aims to improve personal self-care, whether directly or indirectly, would not be described as such. Alternatively, the low number of studies we identified may reflect an area which is under-researched, or where there is publication bias secondary to negative findings.
Another possible explanation is that contemporary mental health practitioners and services may not consider personal self-care as a relevant area for research. Prior to deinstitutionalisation, people with severe mental health problems often resided in long-term hospitals where basic needs such as meals, laundry and a clean environment were provided, mitigating the risk of self-neglect (Gunstone, 2003). As mental health services moved to more of a community-based care model, the degree to which some people struggled with ADL became more evident (Abelha et al., 2006). One would expect therefore an increasing interest in research into interventions that aim to enable personal self-care. However, a number of factors may have inhibited this. Contemporary mental health services, rightly, aim to provide a recovery-orientated approach in which practitioners and service users discuss and agree together the aims of the treatment and support. It may be that this collaborative approach is failing to identify personal self-care as an important recovery goal. Service users and practitioners may be embarrassed to raise it or fail to identify it as a problem, particularly if meetings take place in an office environment, as signs of self-neglect that are evident in the person’s home may not be obvious when they attend an appointment at a community team base or outpatient department. Even if practitioners are aware of the issue and are not embarrassed by it, they may feel that it is intrusive or inappropriate to raise it when trying to foster a collaborative and empowering relationship with their client; in other words, they may not know how to raise the topic in a sensitive manner, or it may be that they choose not to raise it as they do not know how to help to address it.
Occupational therapists have specific expertise in working with people to improve their ADL skills. However, there are few mental health occupational therapy researchers and the evaluation of complex interventions based on mental health occupational therapy through trials and other robust study designs is at a relatively early stage of development. In recent years, researchers in this field have tended to focus on interventions to help people achieve balance in their activities in order to promote wellbeing rather than on developing interventions to assist people to manage ADL (Edgelow and Krupa, 2011; Eklund et al., 2017).
It appears that focusing on personal self-care may be ‘out of fashion’. This seems both surprising and problematic. Being able to manage one’s personal self-care is a fundamental life skill which is usually acquired in childhood. It impacts on how others perceive us and informs the initial impression we make in any social situation. Poor personal care has obvious negative consequences in terms of building friendships and intimate relationships, on our chances of success at interviews for work or courses and, when very severe, on even being allowed into shops to buy essentials. Poor self-care is also highly stigmatising, and should be assessed and addressed as part of a holistic, recovery-orientated approach to treatment and support for people with severe mental health problems. Currently, we lack evidence to guide practitioners in how to do this.
Our review identified one trial that used a cognitive remediation intervention that included ADL as one of three areas of function targeted. While the intervention was not found to be effective at improving self-care, global functioning was greater than for controls at follow-up (Sánchez et al., 2014). Similarly, one of the three trials we identified that evaluated the FAST intervention found it to be more effective in improving functioning when combined with CRT, and improvements in community and household activities and work skills were sustained 6 months after the intervention period (Bowie et al., 2012). There is recent good evidence that the benefits of CRT on cognitive impairments only translate to functional improvement when it is incorporated into real-life settings where skills can be practised and developed as part of the therapy, although, to date, such studies have tended to focus on improving work and social skills rather than self-care (Van Duin et al., 2019). Our findings suggest that combining cognitive remediation with programmes that aim to improve ADL may be synergistic. However, a very recent, small, three arm trial, that was published after our updated literature search, found no advantage for combination therapy comprising CAT plus cognitive remediation over CAT alone, although both were superior to treatment as usual control (Kidd et al., 2020). That trial recruited people at an early stage of psychosis and the results may therefore not be generalisable to people with longer term and more complex psychosis.
These studies help our understanding of the kinds of complex interventions that are feasible and acceptable to people with severe mental health problems, but further studies of interventions such as CAT and FAST are needed to inform their efficacy in addressing personal self-care, singly or in combination with CRT. It seems highly likely that a variety of complex interventions will be needed to tailor support to individuals’ needs and preferences. What is clear is that there is an urgent need for more research in this important area.
Key findings
More research is needed to develop personal self-care interventions for people with severe mental illness. CAT appears promising and combining ADL skills promotion with cognitive remediation may help.
What the study has added
Very little research has been conducted that can inform the interventions required to support people with severe mental health problems develop the fundamental skills required to manage their personal self-care.
Footnotes
Acknowledgements
The author(s) would like to thank and acknowledge Noel Wong for independently reviewing the initial list of publication titles and abstracts.
Research ethics
Research ethics approval was not required for this systematic review.
Consent
No consent was required as this paper reports on the results of a systematic review of previously published literature.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Contributorship
The study was designed by HK and PMcP. The literature search and data extraction were carried out by HTW with supervision by HK and PMcP. MB and HK drafted the manuscript with input and review by all authors prior to submission.