
Abstract
Introduction
While the Model of Human Occupation Screening Tool has undergone psychometric development and testing and is widely used in mental health practice, only a few small-scale studies to date have examined its use in clinical practice.
Method
A national survey was conducted with United Kingdom occupational therapists working in mental health settings to evaluate the use of the Model of Human Occupation Screening Tool. The survey included the modified version of the Usefulness, Satisfaction, and Ease of Use (USE) questionnaire and two open-ended questions. The latter were coded through inductive content analysis and all responses were analysed using Statistical Package for the Social Sciences software.
Results
n=105 questionnaires were analysed. The Model of Human Occupation Screening Tool was found to be a useful tool, with most therapists scoring it favourably on the usefulness (74.7%), ease of use (76.1%), ease of learning (81.2%) and satisfaction (80.6%) subscales. It was praised as a valuable outcome measure, guiding interventions and providing a comprehensive overview of assessed individuals. Time consumption, inaccessible terminology and lack of sensitivity to change were indicated as possible downfalls.
Conclusion
Therapists valued the Model of Human Occupation Screening Tool as an assessment tool, but more importance should be placed on training to overcome some of the limitations identified here. Also, its suitability to the setting in which it is used should be considered before implementation in practice.
Introduction
The Model of Human Occupation (MOHO) (Kielhofner, 2008; Taylor, 2017) has become a widely recognised model of practice within occupational therapy (Crist et al., 2000; Lee, 2010; McColl, 2015). The MOHO and its concepts and assessments have been subject to scientific scrutiny, have an extensive evidence-base (Lee, 2010) and are commonly used in practice, particularly in mental health settings (Ashby and Chandler, 2010; Lee, 2010; Parkinson et al., 2008).
The Model of Human Occupation Screening Tool (MOHOST) is an evaluation tool derived from the constructs of the MOHO. The MOHOST version 2.0 was created in the United Kingdom (UK) by Parkinson and colleagues (2006). It is designed to enable the therapist to gain an overview of an individual’s occupational functioning. It considers six domains: motivation for occupation, pattern of occupation, communication and interaction skills, process skills, motor skills and environment. Each domain contains four subscales and items are rated by the therapist on a FAIR scale, where F = facilitates, A = allows, I = inhibits and R = restricts the person’s occupational participation. Extensive rating criteria for each item are provided in the manual (Parkinson et al., 2006). Since its creation, the MOHOST has become widely used. It was translated into many languages (MOHO web, n.d.) and it has been found to be a valid and reliable tool that can be used with a range of client groups internationally, for example in the United States (US), UK, Japan, Brazil or Sweden (Cruz et al., 2019; Fan, 2014; Haglund, 2020; Kielhofner et al., 2010; Kramer et al., 2009; Shinohara et al., 2012).
Literature review
Despite its scope of use, only a few studies to date have examined the clinical use of the MOHOST. Parkinson et al. (2008) discussed the application of the MOHOST in an acute psychiatric setting where they outlined a pathway of how the assessment could be applied. A case presentation is used to demonstrate the use of the tool and comments were gathered from the occupational therapists who used the tool. Parkinson et al.’s (2008) paper is a service evaluation without research aims, method or an analytical strategy; therefore, the findings should be considered with caution. It should also be noted that the leading author is the main creator of the MOHOST and that possible difficulties when using the tool are not discussed. Nevertheless, the paper concluded that the MOHOST was quick to administer, unobtrusive when used repeatedly, and increased the profile and the understanding of the role of occupational therapists amongst multi-disciplinary team (MDT) members. A further paper that explored the use of the MOHOST also had some methodological limitations: Hawes and Houlder (2010) provided a practice analysis reflection on the use of the MOHOST in a community learning disability team. In the paper, Hawes and Houlder (2010) wrote that the aim of participants was to demonstrate the clinical effectiveness of evidence-based assessment without compromising professional autonomy. This suggests that the assumptions were drawn prior to the commencement of the study and the possible presence of demand characteristics (Orne, 1962). Therefore, and not surprisingly, it was concluded that the introduction of the MOHOST supported evidence-based interventions without compromising clinical flexibility (Hawes and Houlder, 2010). Additionally, the MOHOST was considered to be easy to use, applicable to the learning disability population and helpful in providing a framework to write reports (Hawes and Houlder, 2010). However, the study was preliminary, with no follow-up, used a small sample, and gave no information about how the data was gathered and analysed to provide the outcomes.
Smith and Mairs (2014) published a practice analysis of occupational therapists working in a community mental health team using the MOHOST and another MOHO assessment tool, the Occupational Circumstances Assessment Interview and Rating Scale (OCAIRS). Although they found that the MOHOST was the preferred assessment to use, four of the 10 therapists who took part did not complete any assessments. As the sample was small, this translated to 40% of therapists not utilising available assessments. However, the authors did not collect any data that could account for or explain this phenomenon (Smith and Mairs, 2014). A study by Wimpenny et al. (2010) may offer some explanation. Wimpenny et al. (2010) conducted participatory action research (n=15 on average involved at one time) focusing on implementing the MOHO into a community mental health team. Some of the initial difficulties identified by the authors in doing so included therapists’ lack of knowledge and confidence with the MOHO’s concepts or added pressure to already existing agendas (Wimpenny et al., 2010). However, after overcoming initial barriers, the authors concluded that the implementation of the MOHO concepts supported therapists’ occupation-focused practice, encouraged professional reflection and enhanced their professional profile (Wimpenny et al., 2010). Both of these studies were small-scale and conducted at one research site; therefore, further wide-scale research is needed to confirm the findings.
More recently, Haglund (2020) examined the utility of the Swedish version of the MOHOST. In the study, two groups of occupational therapists were compared: those who had undertaken training in using the MOHOST (a 2-day course) and those who were self-taught (using the manual), although this was not initially intended. Those who had attended the course rated their knowledge about the assessment more highly than did the self-taught group. Thirty-seven participants remained in the study after initial recruitment of 65 occupational therapists who used the Swedish version for at least 6 months, of whom 47 responded and 10 were excluded because they reported not using the assessment in practice (seven of those were self-taught). When asked about the advantages/disadvantages of the assessment, occupational therapists praised it for providing a good overview of the client, being flexible in terms of data gathering, support in structuring documentation and ease of application. The main disadvantage mentioned was the difficulty to ‘get into’ the assessment (although this was not explored further) and all the comments in this regard came from the self-taught group. Also, the need for too much depth to understand the client’s situation and the time-consuming nature of the assessment were mentioned as disadvantages. When asked about the clinical relevance of the tool, the majority of the occupational therapists praised it for providing guidance in determining future need for treatment/interventions. Also, supporting communication with external agencies and support in structuring reports was again mentioned as useful. However, four occupational therapists, all of whom belonged to the self-taught group, said that they would not use the assessment in the future. The more sceptical view of the assessment from the self-taught group is evident, and this may be due to the lack of appropriate training, but also, as the author mentioned, those who chose to invest in training and participation may not want to critique their own choices.
Overall, the literature supports that the MOHOST is valuable in practice. However, a range of possible limitations to current studies have been identified, including small sample sizes, lack of scientific method and bias. The frequent involvement of the creators of the MOHO and the MOHOST in studies raises the questions of objectivity and possible ‘experimenter effects’ (Rosenthal, 1976). The current study intended to address some of these issues by using a quantitative survey design with a large, non-related sample and conducted by independent researchers.
Aim
The aim of the study was to explore the usability of the MOHOST by occupational therapists working in mental health settings in the UK.
Method
Design
This study used a survey design (Sue and Ritter, 2012). Ethical approval was obtained from the Leeds Beckett Local Research Ethics Co-ordinator in January 2019 (Application Ref: 56443). The survey was conducted online using Qualtrics software (version: 06:2019; Qualtrics, 2019). The survey was anonymous, participant information and consent were embedded in the survey, and participants were required to read and confirm before proceeding to the questions. The right to withdraw and the mechanism of data withdrawal were explained to the participants in these sections.
Instrument
The online survey consisted of 18 questions. Initial questions enquired about demographics, followed by a modified version of the Usefulness, Satisfaction, Ease of Use (USE) questionnaire (Lund, 2001) and two open-ended questions that asked about the negative and positive aspects of using the MOHOST.
In the absence of a specific standardised measure of assessment tool use in practice, a modified USE questionnaire (Lund, 2001) was chosen to collect data. The original USE questionnaire consisted of four subscales measuring Usefulness, Satisfaction, Ease of Use and Ease of Learning and items are constructed with responses in a Likert-type format. (Lund, 2001). Permission and materials for the USE questionnaire were provided by its author Dr Lund via email correspondence. Lund’s (2001) paper has been cited nearly 800 times since its publication, and the scale has been found to be a reliable and valid measure of user experience (Chung and Sahari, 2015; Gao et al., 2018). Lund (2001) designed the questionnaire to be used for software, services and user support materials, but not exclusively, and it is non-proprietary (Gao et al., 2018). The questionnaire was modified for the purpose of this study; this included changing generic statements within the tool and making them relevant to occupational therapy practice, for example ‘It makes the things I want to accomplish easier to get done’ (original item) vs ‘It makes the things I want to accomplish with patients easier to get done’ (modified item). Two occupational therapists piloted the modified questionnaire to assess the clarity and face validity of the statements. In total there were three statements modified prior and one added to the questionnaire following the pilot.
Participants
The study inclusion criteria were that participants must be UK-based occupational therapists who were working in inpatient or community adult mental health settings and used the MOHOST in their practice. This purposive sample was recruited through the Royal College of Occupational Therapists Specialist Section Mental Health group, which acted as a gatekeeper on behalf of the researchers (researchers did not receive any information about the members, for example names, email addresses) and via social media groups (Research4OT, MH4OT). The survey remained live for 8 weeks. To enhance the response rate (Sue and Ritter, 2012), fortnightly reminders were sent to the social media groups during this period, and one reminder was sent via email to the Specialist Section.
Data analysis
The quantitative questionnaire data was transferred into the Statistical Package for the Social Sciences (SPSS, version 25) and was screened for errors and omissions to ensure data integrity. Descriptive statistics were then calculated, including totals (n) and percentages, as well as ranges, medians, means and standard deviations.
The open-ended questions were coded through inductive content analysis (Elo and Kyngas, 2008). This approach was chosen for the present study because it makes it possible to quantify qualitative data, and therefore enhanced the understanding of the responses gathered through the questionnaire (Vaismoradi et al., 2013). The development of the coding manual commenced with open coding. The researcher (KB) read through participants’ responses in order to become familiar with the data and identify the most frequently emerging categories. Subsequently, the researchers (KB, RB) reviewed the data and discussed and agreed the final list of categories (Elo and Kyngas, 2008; Elo et al., 2014). These processes have enhanced the trustworthiness of the research (Elo et al., 2014).
The coding manual included the categories related to the questions asked. Every category also included an ‘other’ variable when the answer was singular and did not match any of the identified categories. The categories identified were entered into SPSS to provide frequency tables of the number of therapists who had answered in accordance with the given category. The therapists usually provided one- to three-sentence answers; therefore, multiple categories could have been identified within one answer.
Results
In total, 145 surveys were returned. Following data cleansing, 40 surveys with only partial responses were excluded from further analysis, leaving 105 surveys to be analysed. Percentages (%) of the total responses as well as totals (n) are reported.
Demographics
Of the 105 participants, there were 96.2% (n = 101) females and 3.8% (n = 4) males; the mean age was 36.93 (SD = 10.07). Fifty-two of the participants (49.5%) worked in inpatient settings, 43.8% (n = 46) in community settings, 3.8% (n = 4) for a charity and 2.9% (n = 3) in other settings (two participants had worked in mixed settings, and one in a general hospital as a psychiatry liaison). Of the 105 participants, 84.8% (n = 89) of the occupational therapists worked for the National Health Service, 8.6% (n = 9) reported working privately, 5.7% (n = 6) for a charity and 1% (n = 1) for a local authority. The average length of practising as an occupational therapist was 5 years and 3 months. Out of the 105 occupational therapists, 66.7% (n = 70) recorded their MOHOST online, 28.6% recorded it on paper (n = 30), and 4.8% in other ways (n = 5; four therapists declared that they used both methods and one said that they recorded it as a Word document). The MOHOST was reported as a core assessment tool at their place of work by 73.3% (n = 77) occupational therapists, whilst 26.7% (n = 28) reported that this was not the case.
Questionnaire results
The questionnaire results for each of the subscales are presented separately below. Following the study’s completion, the reliability analysis evidenced a high level of internal reliability of the revised tool, with overall Cronbach’s alpha of .94, whilst the individual subscales scores were as follows: usefulness: Cronbach’s α = .91; ease of use: Cronbach’s α = .84; ease of learning: Cronbach’s α = .88 and satisfaction: Cronbach’s α = .94.
Usefulness subscale
Most of the therapists scored the MOHOST favourably on the usefulness subscale, with the majority of the respondents (74.3%) responding ‘somewhat agree’ to ‘strongly agree’ to the items of the subscale overall (see Table 1). The majority of the participants agreed that the MOHOST is productive and effective, and found it useful. They also indicated that it provides more control over the selection of other assessments to be used in practice, and that it is a useful outcome measure. The majority also agreed that it makes the things that they want to accomplish with the patients easier to achieve. The variable with the most dispersed scores was asking about whether the MOHOST saved time when used: although the majority agreed, 19% of the therapists responded neutrally, and 36% somewhat disagreed to strongly disagreed.
The modified USE questionnaire results.
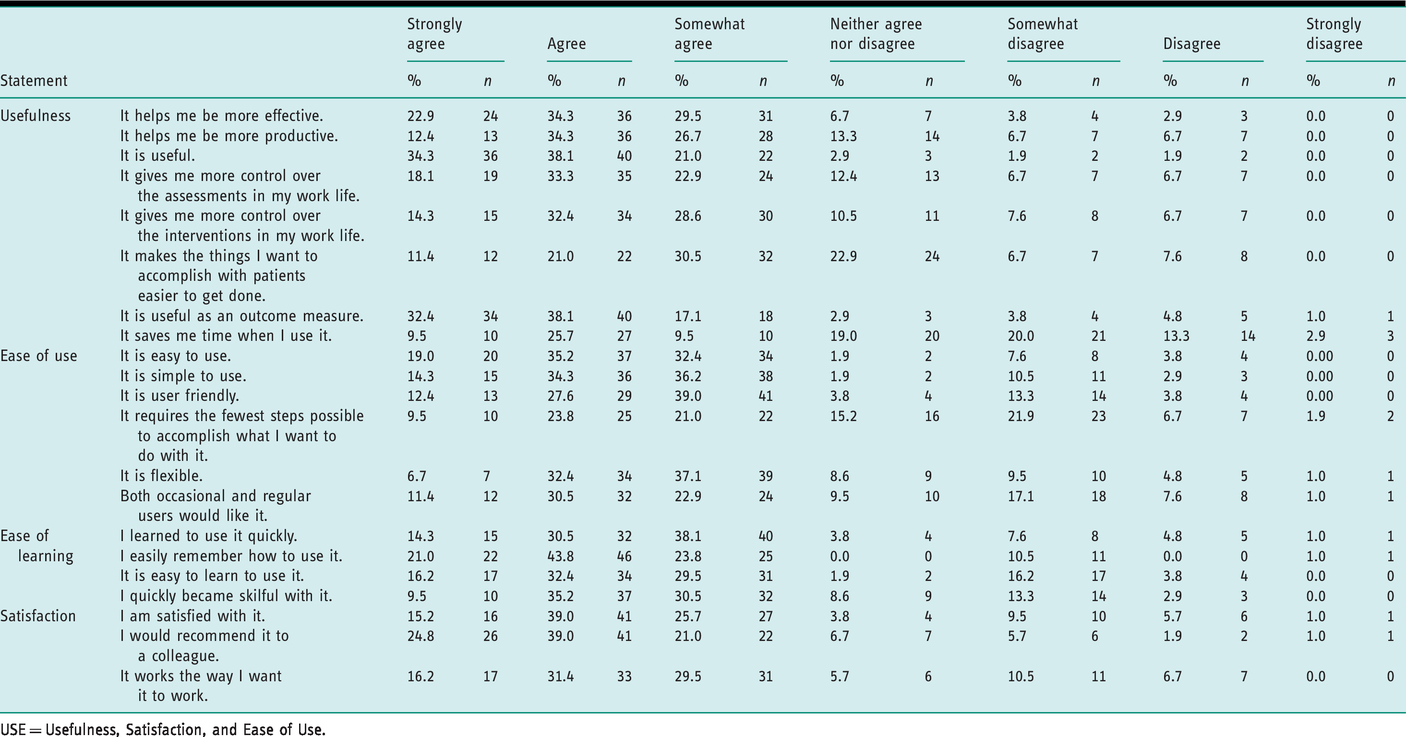
USE = Usefulness, Satisfaction, and Ease of Use.
Ease of use subscale
The majority of the therapists (74.2%) scored the MOHOST favourably on the ease of use subscale, with the majority responding ‘somewhat agree’ to ‘strongly agree’ to the items of the subscale overall. As presented in Table 1, there was an agreement that the MOHOST was easy and simple to use, flexible and user friendly. The greatest dispersal of the scores was on the items ‘It requires the fewest steps possible to accomplish what I want to do with it’ and ‘Both occasional and regular users would like it’.
Ease of learning subscale
The majority of the therapists scored the MOHOST favourably on the ease of learning subscale, with the majority of the respondents (81.2%) responding somewhat agree to strongly agree to the items of the subscale overall (see Table 1 for results). However, 19% of the therapists somewhat disagreed to disagreed on the ease of learning to use it.
Satisfaction subscale
Again, the majority (80.6%) of the therapists were satisfied with the MOHOST, responding ‘somewhat agree’ to ‘strongly agree’ to the items of the satisfaction subscale overall. As can be seen in Table 1, they indicated that they were satisfied with it, that they would recommend it to a colleague and that it works in a way that suits them. A small number of respondents disagreed with these items.
Content analysis results
The categories of variables identified from the open-ended questions via content analysis are presented in Tables 2 and 3. The tables include examples of extracts used to create the categories and the percentages of responses given.
Positive aspects when using the MOHOST.
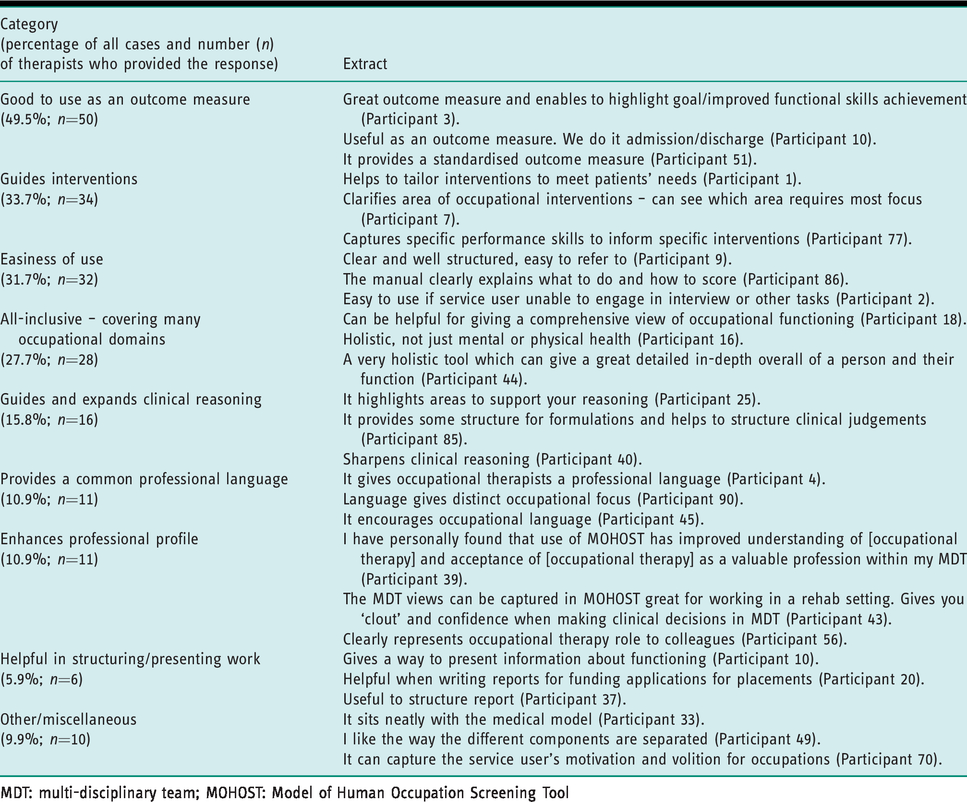
MDT: multi-disciplinary team; MOHOST: Model of Human Occupation Screening Tool
Negative aspects when using the MOHOST.
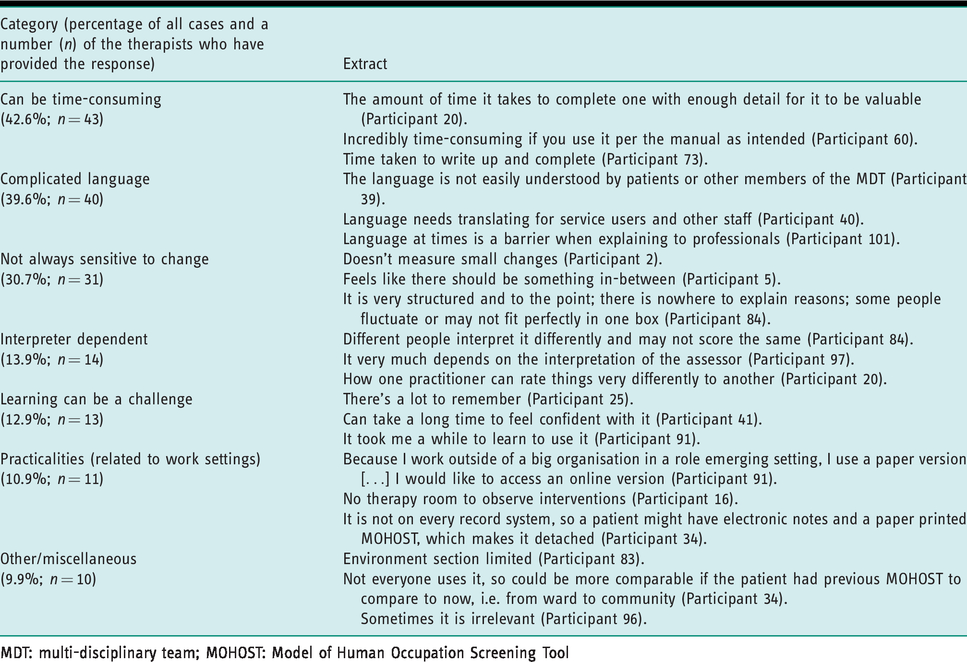
MDT: multi-disciplinary team; MOHOST: Model of Human Occupation Screening Tool
Table 2 shows the findings for the positive aspects of the MOHOST. Nearly half (49.5%, n = 50) of the therapists valued the MOHOST as an evidence-based outcome measure. Just over one-third (33.7%, n = 34) found that it helps to guide their interventions, with just under one-third (31.7%, n = 32) also expressing that it is easy to use. Over a quarter (27.7%, n = 28) stated that it is an all-inclusive tool which covers many areas of occupational domains. Guidance and development of clinical reasoning were also pointed out as advantages when using the MOHOST (15.8%, n = 16). Some therapists (10.9%, n = 11) appreciated the MOHOST’s use and encouragement of use of occupational therapy specific language and the enhancement of their professional profile through MOHOST use. A small number (5.9%, n = 6) also appreciated the MOHOST as helpful in structuring their written work.
Table 3 shows the findings for the negative aspects of the MOHOST. Over 40% (42.6%, n = 43) of the therapists criticised the MOHOST for being time-consuming. Over a third (39.6%, n = 40) found that the language used by the MOHOST is overly complicated; further, its sensitivity to change was deemed deficient by nearly one-third (30.7%, n = 31). Some therapists expressed their viewpoint that the MOHOST ratings can be assessor-dependent and thus subjective, and that learning about how to use the MOHOST can be challenging (13.9%, n = 14; 12.9%, n = 13 respectively). Some (10.9%, n = 11) expressed that the practicalities related to their work settings influence their attitude towards the MOHOST.
Discussion
This survey has explored the views of UK occupational therapists working in mental health settings on the usefulness, ease of use, ease of learning and satisfaction when using the MOHOST in their practice. The MOHOST is arguably the most widely used assessment tool in mental health occupational therapy practice in the UK. Its creation in collaboration with therapists has made it authentic for practice and it has a range of evidence that supports its psychometric properties. This study has found that in practice the MOHOST is useful, easy to use, flexible and valuable as an outcome measure. The participants of this study found the MOHOST language and time taken to use as limitations to the tool. These findings echo and build on existing studies and this study as addressed previous methodological limitations.
Most of the participants of this study worked within the UK National Health Service, where the MOHOST was often imposed as a core assessment tool; however, nearly a third of therapists in this study chose to use the MOHOST despite this not being the case. The majority of the therapists scored the MOHOST favourably on the modified usefulness scale. However, there were some items where the scores were more dispersed; the discussion of the main categories that have emerged from the content analysis about the positive and negative aspects of the MOHOST’s use may provide some understanding of this.
Although most of the participants scored the MOHOST favourably on the usefulness subscale, the majority disagreed with the item asking whether it saves them time when they use it. Similarly, the most prominent response in relation to the negative aspects of the MOHOST was that it is time-consuming. Parkinson et al. (2006) recognised that the assessment may be a relatively lengthy process (approximately four sessions), as the therapist’s knowledge about the client increases and the rapport is built (Parkinson et al., 2006). Furthermore, the MOHOST can be supported by shorter assessments, such as the Model of Human Occupation Screening Tool – Single Observation Form, or the Interest Checklist (Kielhofner, 2008; Parkinson et al., 2006). Therefore, the decision regarding which tool is most appropriate in a given time/situation may be due to the clinical judgement of the therapists. Nevertheless, if the MOHOST is the main assessment in their workplace, additional training or the suitability of the assessment in the first place should be discussed. Furthermore, investing time in the assessment process is often necessary, as it provides a client-centred performance context and evidence-base that is needed to assert the value of occupational therapists (Seymour et al., 2012).
The language of the MOHOST was identified as one of the negative aspects when communicating with the other MDT members or with the patients; for example, it was seen as being not easily understood or hard to translate to others. Although the use of conceptual models and assessments facilitates the use of occupational therapy language, this finding suggests that the idea of suppressing the use of occupational therapy language by the therapists is still relevant (Creek, 2009; Gillen and Greber, 2014). It may be that the language poses issues in translating it for others; however, occupational therapists were able to adapt many medical terms. Parkinson et al. (2006) acknowledged this matter in the past and changed some of the terminology to make it easier to translate to others; for example, ‘volition’ became ‘motivation for occupation’. Though Creek (2009) pointed out that occupational therapists may not describe what they do in occupational therapy terms for the fear of being laughed at or ignored by their colleagues, nonetheless, adapting the language of other disciplines, such as medicine, can lead to the loss of the essence of occupational therapy (Creek, 2009). In contrast, a small number of therapists in the current study praised the use of the distinctive occupational therapy language. Perhaps the notion of a shared language should be emphasised more within the discipline. It was found that the use of a shared language between different healthcare professions was associated with a better quality of care and improved job satisfaction, and one way to develop a shared language is through interprofessional education (Stühlinger et al., 2019).
Regarding the MOHOST’s sensitivity to detect small changes or any change at all revealed in this study, examples of patient groups were those with severe mental health issues, learning disabilities and dementia. A reason for this could be practice time restrictions that limit the ability to perform a comprehensive first assessment, which may influence the latter detection of change. This could also be related to the suitability of the assessment to the setting in which is conducted. Also, as the MOHOST highlights occupational deficits, its sensitivity when applied with learning disability clients was questioned by Hawes and Houlder (2010), who stated that work with this client group involves focusing on what they can do rather than what they cannot. This could also be relevant to its use with dementia patients. Hawes and Houlder (2010) suggested that a more in-depth analysis of the manual would be helpful if the difficulty of assigning the rating arose. Furthermore, the issue of the MOHOST detecting change in these populations has been acknowledged in the past by its creators (Parkinson et al., 2014). Recently, The Model of Human Occupation Explanatory Level Outcome Ratings (MOHO-ExpLOR) (Cooper et al., 2018; Parkinson et al., 2014) was created as an alternative assessment for those who may be severely impaired through long-term disabilities or cognitive deficits; thus, their level of future change is projected to continue at an explanatory level. This assessment is similar to the MOHOST as it is a therapist-rated tool in which the information can be gathered from several different sources, and it covers the majority of the MOHO concepts to gain an overview of occupational functioning. Thus, with minimal training, it may be a welcomed alternative by the therapists who currently use the MOHOST to work with such populations.
Although the MOHOST was criticised for its lack of sensitivity, the main factor that it was praised for was its usefulness as an outcome measure. Parkinson et al. (2006) designed the MOHOST with the idea of providing a simple outcome measure covering a range of occupational concepts as indicated by the MOHO. This finding confirms this notion, as well as previous study results (Fan, 2014; Fan et al., 2016; Kirsh et al., 2019). This is particularly important since there is a professional requirement for occupational therapists to be able to evidence the effectiveness of their interventions (Long et al., 2017). As described by Parkinson et al. (2008), the ability to unobtrusively repeat the assessment is particularly valued. This is often relevant to mental health patients, who may be suspicious and/or withdrawn in an acute stage of their illness (Davey, 2008; Parkinson et al., 2006).
The MOHOST was praised for its ability to guide therapists’ interventions and provide a comprehensive overview of an individual. This finding supports Parkinson et al.’s (2006) notion that the MOHOST’s ability to highlight areas for further assessment and/or interventions is central to its use as a screening tool and is in line with recent findings by Haglund (2020). This is to be achieved through equal distribution of the items per section in the assessment (Parkinson et al., 2006). This makes it possible to highlight the areas of occupational functioning that may require attention and provide an in-depth overview of an individual’s occupational functioning. Following this, the therapist is responsible for remaining client-centred and assessing the meaningfulness of interventions that could contribute to the improvement in identified areas of need. Furthermore, it was found that the interventions that use concepts of the models of practice, such as the MOHO and its associated assessments, can significantly improve the intervention outcomes in occupational performance and clients’ quality of life in comparison to not adapting any occupational models in practice (Shinohara et al., 2012).
The ease of its use was also indicated as a positive aspect of the assessment in the current study. As the MOHO and its concepts are widely used, this is not surprising (Lee et al., 2012). Additionally, the supporting manual available on how to conduct the assessment, social media support groups and training events all contribute to the familiarity and the ease of use of the assessment. Still, a small number of therapists have indicated that learning about the assessment can be challenging, and the scores on the ease of learning scale were somewhat dispersed. Also, participants in Haglund’s (2020) study who were self-taught criticised the assessment’s user-friendliness/accessibility, and some declined to use it in the future. However, it was found that with minimal training the therapist can use the tool effectively (Kramer et al., 2009). Nevertheless, as the MOHOST was identified by 73.3% of the therapists in this study as being the core assessment used in their work settings, the question is whether the responsibility for training should fall on the work setting (especially if it is imposed) or on the individual therapist as a part of their professional development. Previously, Wimpenny et al. (2010) found that the community of practice (clinicians working in collaboration with academic partners) was an effective way of facilitating practice development when implementing the MOHO concepts. Therefore, when possible, such collaborations could be organised to support individual practitioners as well as to allow for the exchange of ideas between the two parties.
Limitations
The study limitations should be noted. The demographic data revealed homogeneity in the respondents’ characteristics, with the majority being female and working within National Health Service settings. However, the sample was heterogeneous in other variables, such as age, length of work or the service base. It was not possible to ascertain the response rate, as there are no data available on the total number of mental health occupational therapists working in the UK. Thus, the generalisability of the findings should be considered with caution. Also, despite the qualitative data being examined by a second researcher (RB), it could not be classed as being coded by a separate coder. Nevertheless, no standard recommendations exist when encoding data through inductive content analysis (Elo et al., 2014). The researchers have followed the guidance of Elo et al. (2014), where one person was responsible for the analyses whilst another was overlooking the process cautiously, and any differences in categorisation were debated. Furthermore, due to the impartiality of the researchers and based on data about the sample that have been collected, it can be assumed that a broad picture of current UK practice and service provision has emerged through this enquiry.
Conclusion and implications
This was the first large-scale study where independent researchers examined the usefulness of the MOHOST amongst occupational therapists in the UK who work in mental health settings. It has confirmed previous notions of the positive aspects of the tool (Hawes and Houlder, 2010; Parkinson et al., 2008; Wimpenny et al., 2010). It has revealed a more in-depth understanding of the views of occupational therapists who use the MOHOST in practice. The MOHOST was found to be a useful tool for practice in terms of overall usefulness, as an outcome measure, guiding interventions, or providing a comprehensive overview of an individual. However, time consumption, inaccessible terminology and inability to detect a change in functioning were pointed out as its possible downfalls by over a third of the therapists.
As the MOHOST was found to be a useful assessment tool and to contribute to client-centred and evidence-based practice, it is suggested that training could address some of the negative aspects that have emerged from this enquiry. Additionally, it is recommended that the suitability of the assessment for the setting in which it is to be used should be carefully evaluated.
Key findings
Occupational therapists working in mental health services report that the MOHOST tool is useful, easy to use, and guides interventions and outcomes. The MOHOST may be limited by its language and time taken to administer and learn to use.
What the study has added
This national survey has increased knowledge of occupational therapists’ views when applying the MOHOST in their practice; it has confirmed several attributes of the tool identified in previous enquiries. It has also highlighted possible negative aspects when using the tool in practice and provided some thoughts/ideas on how to overcome these.
Footnotes
Acknowledgements
The authors would like to thank Dr Joanne Inman for her support and the occupational therapists who participated in the study.
Research ethics
Ethical approval was obtained from the Leeds Beckett Local Research Ethics Co-ordinator (Application Ref: 56443) on the 14 January 2019.
Consent
All participants gave informed consent, participant information and consent were embedded in the survey and participants were required to read and confirm their consent by clicking a box before proceeding to the rest of the survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Contributorship
Kinga Bugajska researched the literature, applied for ethical approval for the study and completed data analysis. Both authors contributed to the interpretation of data. Kinga Bugajska wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.